
New Changes in JCI 5th Edition Hospital Standards by Dr.Mahboob Khan Phd
85
New Changes In JCI 5 th Edition Hospital Standards Dr.Mahboob Ali Khan MHA,CPHQ,Phd Harvard Renowned Healthcare Quality Consultant, 1
-
Upload
drmahboob-khan-mhaphdpmp -
Category
Healthcare
-
view
1.865 -
download
3
Transcript of New Changes in JCI 5th Edition Hospital Standards by Dr.Mahboob Khan Phd
New Changes In
JCI 5th
Edition Hospital Standards
Dr.Mahboob Ali Khan MHA,CPHQ,Phd Harvard
Renowned Healthcare Quality Consultant,
1

5th Edition Update Overview
• Global healthcare has changed in many ways
over the last 3 years of the 4th Edition and
will continue to change • Standards ensure hospital care not only
reflects up to date practice but also help
hospitals prepare for a different future • Change means that improving quality and
patient safety will always be a work in progress
with continuous advances but no end point • Some of these changes in global healthcare
stimulated revisions to the JCI standards
2










What Is New In This 5th
Edition
• Many changes • Continuous readiness & compliance
of JCI accredited hospitals is
emphasized by conducting
unannounced as well as announced
surveys by JCI. • All of the significant changes are listed
in a table at the beginning of each of
patient-centered and organization
management- centered chapters
• Nearly, all of the 4th
edition text has
been edited for clarity in the 5th
edition • The total number of standards has
been reduced by more than 10%
& MEs by more than 5%

What Is New In This
• New standards and established standards
deemed by the field as more difficult to
meet are supported with evidence-based
references • References of various types are cited in the
text of the standard's intent and are listed at
the end of the applicable standard chapter • A new Section, “ Accreditation Participation
Requirements” (APR) has been added.
16

What Is New In This 5th
Edition
• Standards requiring a written policy or
procedure are indicated by a icon after the
standard text . In previous editions, each
required policy or procedure was specified in
its own ME. In this edition, all policies and
procedures will be scored together at MOI.9
and MOI.9.1.
• Examples that better illustrate compliance
are provided in most standards' intents • JCI’s policies and procedures are
summarized and moved from the front of the
manual to their current location on page 253.
Starting in late 2013, JCI policies will be
published on JCI’s public website.

What Is New In This 5th
Edition
• The Medical Professional Education
(MPE) and Human Subjects Research
Programs (HRP) standards for
Academic Medical Center Hospitals
are now included in this manual. • The “Management of Information”
(MOI) chapter has been changed from
“Management of Communication and
Information” (MCI) in the 4th
edition. • Widespread wording changes for clarity,
including frequently substituting the term
program for plan or process
18

Accreditation Participation
Requirements (APR)
19

APR Chapter
New Chapter
It is about how compliance will be evaluated
APRs are not scored like standards during the on-site
survey; hospitals are considered either compliant or not
compliant with the APR
Most of APR requirements have been moved from many
4th
edition documents
The consequence of non-compliance 20

APR Chapter Standards
• APR.1 – timely submission of data and information • APR.2 – accurate and complete information • APR.3 – reporting changes in hospital profile • APR.4- Hospital permits on site review of compliance or
verification of concerns or regulatory sanctions (at ANY TIME) • APR.5- Hospital allows JCI to request/review results and reports
of external evaluations from publicly recognized bodies • APR.6- Hospital allows observations by JCI Board members and
JCI staff
21

APR Chapter Standards
• APR.7- The selection and use of the Library of Measures
is integrated into the hospital’s measurement priorities • APR.8 – The hospital accurately represents
its accreditation status and program • APR.9 – Any hospital staff member can report concerns
about safety or quality of care without retaliatory action • APR.10 – translation and interpretation services
are provided by licensed translation and
interpretation professionals 22

APR Chapter
• APR.11 – The hospital notifies the public it serves about
how to contact its hospital management and JCI to report
concerns about patient safety and quality of care • APR.12 - The hospital is required to provide patient care
in an environment that poses no risk of an immediate
threat to patient safety, public health or staff safety
23

Joint Commission Patient Centered
International 5th
Standards
Edition Hospital
IPSG, ACC,
Standards
PFR & AOP
Major Changes in the IPSG,
ACC, PFR, and AOP Chapters
24

Major Changes in the IPSG, ACC,
PFR, and AOP Chapters
• Focus on highlights, not all changes • Clearer and more comprehensive intent
statements, with more examples • New decision rule #5 for IPSG’s
25

IPSG
International Patient Safety
Goals
26

IPSG Major Changes
Emphasizes the need for more
focused compliance on 3
distinct communication-related
areas
Highlights reporting of critical
results of diagnostic tests as an
important communication issue
Introduces a new requirement
for effective handovers of
patient care within the hospital-
NEW STANDARD IPSG.2.2
27

IPSG Major Changes
Clarify expectations for
high-alert medications &
concentrated electrolytes
Clarifies the purpose and
content of the preoperative
verification process & the
approach for the time-out
procedure
28

IPSG Major Changes
Clarifies the need to address
fall risk assessment and
reassessment in both inpatients
& outpatients
Raises requirements for
addressing falls to include
locations and situations at high
risk for falls
29

ACC
Access to Care and
Continuity of Care
30

ACC Major Changes
Adds a new requirement for hospitals to
manage the flow of patients throughout
the hospital NEW STANDARD
ACC.2.2.1
Separates the AMA requirements
according to two conditions:
• Leaving Against Medical Advice with
notification: full D/C summary is required • Leaving Against Medical Advice without
notification
31
New standard to require mechanism to manage patient
flow throughout the organization including:
32

PFR
Patient and Family Rights
33

PFR Major Changes
added a new requirement for informing patients and
families of the tests & treatments that require a
separate informed consent
Informed Consent must be in a manner/language that
patient understands (NEW) & must have uniform
recording requirement (NEW)
Informed Consent to be obtained before high risk
procedures or treatments & before admission for
inpatient care
34

PFR Major Changes
Further emphasized the need
to ensure patient & family
rights regarding organ & tissue
donation
Clarify requirements regarding
organ & tissue procurement 35

AOP
Assessment of Patients
36
AOP Major Changes
- Patient assessment and documentation
must be more patient centric - Patient and family participation in
decisions more critical - Patient record and out‐patient summaries are essential communication tools
- Patient and family education at
many points in care process
37
AOP Major Changes
Establishes a NEW STANDARD to
emphasize the need to reduce special
risks for laboratory staff related to
infection control & biohazards
Adds a NEW STANDARD to detail
requirements for reference (contract)
laboratories used by the hospital
Introduces a NEW STANDARD specific
to blood bank and transfusion services

Joint Commission
Patient Centered
Standards
International 5th
Edition Hospital
COP, ASC, MMU
Standards
& PFE
Major Changes in the COP,
ASC, MMU, and PFE Chapters
39 Edits by PVO, Sept 23 2013

COP
Care of Patients
40

COP Major Changes
Emphasizing the need for uniform
process for prescribing patient
orders
Adds new requirement: the person
requesting, and the reason for
requesting, the procedure or
treatment are documented in the
patient’s record
Clearly identify expectations for the
care of high-risk patients in the
hospital
41
COP Major Changes
Introduces new requirement for staff
training to recognize & respond to
changes in a patient’s condition
NEW STANDARD
Adds new requirement to emphasize
the need for resuscitation services to
be available & consistent throughout
the hospital NEW STANDARD
COP.3.2
Adds ME to emphasize the need for
timely distribution of food and
honoring special requests 42
COP Major Changes
Adds a requirement on communication
with patients regarding potential pain from
planned treatments, procedures, or
examinations
Introduces several standards to
emphasize the need for safety & quality of
organ and tissue transplant services
NEW STANDARDS COP.8- COP.9.3
43

ASC
Anesthesia and Surgical Care
44

ASC Major Changes
Adds a description of sedation &
anesthesia
Emphasizes the importance of
standardization, qualification of
practitioners, and professional
practice guidelines as they relate to
procedural sedation
Adds a new requirement for discussing
the risks, benefits, and alternatives of
procedural sedation with the patient,
family, and other decision makers
NEW STANDARD ASC.3.3
45

ASC Major Changes
Adds text to include documentation of the
anesthesia agent, dose, and anesthetic
technique in the patient’s anesthesia
record
Emphasizes the need for postoperative
analgesia education
Adds clarification that monitoring
needs to be consistent with
professional practice guidelines
Clarifies that the patient’s assessment
should also be used to guide the
identification of significant findings during
monitoring
46

ASC Major Changes
Better detail requirements of
surgery documentation in the
patient’s record
Adds text to expand on what is
included in postsurgical plan of
care
Adds a new requirement regarding
the special considerations needed
in planning surgical care that
involves the implanting of medical
devices
NEW STANDARD ASC.7.4
47

MMU
Medication Management and Use
48

MMU Major Changes
• Emphasizes the need for proper storage
of medications inside and outside of the
pharmacy • Introduces concept that hospitals should
define standards of practice for a safe
and clean dispensing environment • Required elements for prescriptions
are separated from the processes for
problematic or special types of
prescriptions • New requirements for auditing by
hospital to determine the accuracy
and completeness of prescriptions 49

MMU Major Changes
Recognizes two reviews of
the prescriptions • Review 1 - Review
of appropriateness • Review 2 - Review of
medication against order
Identifies that properly trained staff
other than pharmacists may
perform the medication review for
appropriateness & specifies that the
requirement applies when the
pharmacy is open or closed
50

PFE
Patient and Family Education
51

PFE Major Changes
• Chapter now contains standards relating
to general education principle • Specific education has been moved to
chapters where education applies
Compliance with PFE Chapter
Uniform documentation and staffknowledge
Patient and Staff interview and Medical
records review
• Compliance issues: Staff and patient lack of knowledge
No evidence of documentation
or training
• 52

Joint Commission
Organization
Management
International 5th
Standards
Edition Hospital
Standards QPS, PCI, &
GLD
Major Changes in the QPS, PCI,
and GLD Chapters
53

QPS
Quality Improvement and
Patient Safety
54

QPS Major Changes
QPS.1 - Qualified leader of quality
program NEW STANDARD
• Selection of the right individual to
lead program • Selection of the right staff for
program functions • Coordination of quality across
the organization • Implementation of a staff training program • Regular communication to hospital
staff about quality issues
55

QPS Major Changes
QPS.2 – Support and coordination
of quality within the hospital
NEW STANDARD
• Quality program supports
the selection of measures • The program has a supportive
function for department/service and
hospital wide measure priorities • Program integrates event reporting
systems, safety culture measures
and others to facilitate an
integrated approach • Tracks progress
56
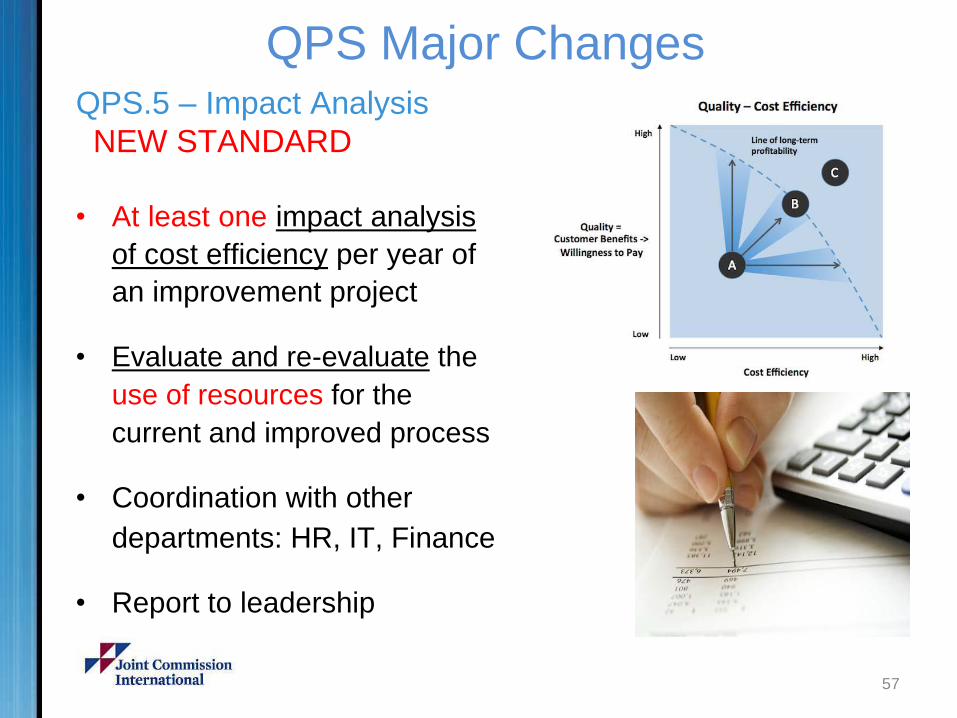
QPS Major Changes
QPS.5 – Impact Analysis
NEW STANDARD
• At least one impact analysis
of cost efficiency per year of
an improvement project • Evaluate and re-evaluate the
use of resources for the
current and improved process • Coordination with other
departments: HR, IT, Finance • Report to leadership
57

QPS Major Changes
QPS.7 – Managing Sentinel Events
• Sentinel event definition has
been expanded to include:
• Death of a full term infant • Transmission of a chronic or
fatal disease – blood, blood
products, or transplant • Rape, assault, homicide
– while on site at hospital • Reporting requirement change-
completion time of Root Cause
Analysis within 45 days from
date of the event 58

PCI
Prevention and Control
of Infections
59

PCI Major Changes
Emphasize the need for hospitals to
track infection risks and trends in an
effort to reduce risks within the hospital
• Use a risk-based approach to
identify epidemiologically important
infection prevention strategies and
focus on infection prevention. • Consider clinical practice guidelines,
and antibiotic stewardship • Annual assessment of the program
60

PCI Major Changes
Clarifies further requirements
for safe handling and disposal
of sharps and needles
Increases the emphasis on
reducing the risk of infections
associated with the operations
of food services
Addresses reporting to and
taking action on reports from
public health agencies
61

PCI Major Changes
Clarifies further that the infection
prevention and control program is
staffed according to hospital size,
level of risk, and the program’s
complexity & scope
Emphasizes that program
strategies should cross all levels
of the hospital
Emphasizes the importance of
mechanical and engineering
controls in minimizing infection risk
62

PCI Major Changes
concentrate on programs
integration of infection prevention
and control program with the
hospital quality program
A new emphasis on the measure
selection and measurement based
on the hospital wide and
department/service specific priorities
Requires reporting the data and
recommendations to the
leadership on a quarterly basis
63

PCI Major Changes
A new requirement on
theenvironmental cleaning of
contaminated isolation rooms NEW
Focuses in the management of
sudden influx of patients with
contagious diseases and
airborne infection when negative
rooms are not available NEW
64

GLD
Governance, Leadership and
Direction
65

Governance, Leadership and Direction (GLD) Overview
66

GLD Major Changes
Leadership role in communication
• Clear and consistent
communication is a responsibility
of leadership • Process, effectiveness and content • Measure of “effectiveness”
of communication
67

GLD Major Changes
Leadership reports to staff and governance
• Develop and implement a quality program
and select leadership for the program
• Quarterly report to governance • Six month review of sentinel events • Progress communicated to staff • Review minutes: governance, senior
leadership, and quality departments • “Sustainability of Improvements”
68

GLD Major Changes
Leadership sets hospital wide improvements
• Focus on measurement for system
improvement • Focus on research and education when
present • Focus on full compliance with IPSGs • Evaluate the impact of Improvement
69

GLD Major Changes
NEW STANDARD to emphasize the
need to protect patients and staff from
contaminated, fake, and diverted drugs,
medical technology, and supplies
NEW STANDARD for hospital leadership
to create, implement, support, monitor, and
take action to improve a culture of safety
70
GLD Major Changes
NEW STANDARDS applicable to hospitals that
conduct human subjects research but do not
meet the eligibility criteria for Academic
Medical Center Hospital accreditation
- NEW STANDARD to emphasize the need for
department/ service quality improvement
activities to be used in the ongoing
professional practice reviews of physicians and
the annual performance evaluations of nursing
and other health professionals staff
71

Joint Commission
Organization
Management
International 5th
Standards
Edition Hospital
Standards FMS, SQE, &
MOI
Major Changes in the FMS,
SQE, and MOI Chapters
72 Edits by PVO, Sept 23 2013

FMS
Facility Management and Safety
73

FMS Major Changes
Emphasize the distinctions
formanagingall aspects of the
hazardous materials and waste program;
References the WHO list of
hazardous materials and waste categories
Program for control and disposal
Explanation of content of MSDS
(Material Safety Data Sheets)
Immediate availability of the MSDS to
manage spills
74

FMS Major Changes
Medical technology’s term
introduced (formerly
medical equipment)
Includes all fixed and portable
medical equipment used for
diagnosis, treatment, monitoring
and direct care of individuals
New requirement for testing of
alternative water and electricity
sources quarterly (NEW)
New requirement for determination
of on-site fuel storage needs related
to emergency power (NEW)
75

FMS.9 – Utility Systems
NEW STANDARD
• Expanded to all utilities • A program for effective and efficient
operation • Inventory of utilities
system defined • Written inspection, maintenance
activities, inspecting and testing
intervals defined • Criteria from manufacturers
maintenance and testing
requirements • Labeling of utility system controls
introduced 76

SQE
Staff Qualifications and Education
77

SQE Major Changes
• Total rewrite of some standards to add
clarity with terminology explained • New Measurable Elements and wording
changes, consolidation of other Measurable
Elements • Flow of standards now is more like natural
process
• Identifies the need for more rigorous
vaccinations program for staff (NEW) • Acknowledges that violence in the workplace has
become an increasingly common problem in
health care organizations (NEW) 78

SQE Major Changes
New, more complete
explanations for key terms:
credentials medical staff verification appointment reappointment
Revise the requirement for primary source verification for initial surveys (new time frame)
Clarifies requirements
for determining medical
staff membership
79

SQE Major Changes
Clarify requirements regarding the
privilege delineation process for medical
staff members
Provides definition of key terms &
expectations to clarify requirements
for monitoring and evaluation of
medical staff
Emphasize the need to document and
take action on findings that affect the
appointment or privileges of medical
staff members (new)
Separates out and clarifies
requirements for reappointment and
renewal of clinical privileges of medical
staff members based on ongoing
monitoring and evaluation 80

MOI
Management of Information
81
MOI Major Changes
• New language in the standards, intent
and MEs
• Need to assess, test, evaluate health
information technology (HIT) systems
before and after implementation
• Evaluate HIT systems for usability,
effectiveness and patient safety
• Stakeholders participate in selection,
implementation and evaluation of
HIT system 82

MOI Major Changes
• Written guidelines on documents,
policies, procedures, and plans
managed to a consistent manner
• Standardized formats of similar
documents • Evidence found when
documents reviewed
83

MOI Major Changes
MOI.9.1 – Consistency across the organization in
policy management
NEW STANDARD
• Ensuring proper implementation of policies,
procedures, plans that guide clinical and
nonclinical practices
• P
When this symbol is found a document is expected
• All are scored together at this standard – one
score for the hospital - not at each location • Tracking, training, knowledge and
implementation are expected
84

5th
Edition JCI Hospital Standards Manual
Challenging
Achievable
Focused on the safety and quality of patient care
BEST WISHES From Dr.Mahboob Khan Phd
85


















