
New biologics for the treatment of atherosclerosis and the...
64
New biologics for the treatment of atherosclerosis and the safety thereof Derick Raal FCP(SA), FRCP, FRCPC, Cert Endo, MMED, PHD Head, Division of Endocrinology & Metabolism Director, Carbohydrate and Lipid Metabolism Research Unit Faculty of Health Sciences, University of the Witwatersrand
Transcript of New biologics for the treatment of atherosclerosis and the...

New biologics for the treatment
of atherosclerosis and the
safety thereof
Derick RaalFCP(SA), FRCP, FRCPC, Cert Endo, MMED, PHD
Head, Division of Endocrinology & Metabolism
Director, Carbohydrate and Lipid Metabolism Research Unit
Faculty of Health Sciences, University of the Witwatersrand
Presenter Disclosure Information
Frederick J. Raal
FCP(SA), FRCP, FRCPC, Cert Endo, MMed(Wits), PhD
Professor Raal has received research grants, honoraria, or consulting fees for
professional input and/or delivered lectures from Pfizer Pharmaceuticals, Merck,
Sanofi, Regeneron, Amgen and The Medicines Company.

Decline in deaths from cardiovascular disease in relation to scientific advances
Nagel. N Eng J Med 2012;366:54-63
600
500
400
300
200
100
0
1950 1960 1970 1980 1990 2000 2010 2020
Year
De
ath
s p
er
10
0 0
00
po
pu
latio
n
1954First
open-heart procedure(Gibbon)
1972NHBPEP
1961Risk
factors defined
1958Coronary
arteriography developed
(Sones)
1962Firstβ-blocker developed (Black)
1969First
description of CABG
(Favolaro)
1976First HMG
CoA reductase inhibitor
described (Endo)
1961Coronary care unit
developed (Julian) 1979
Coronary angioplasty developed (Grunfeld)
1976First
implantable cardioverter defibrillator developed (Mirowski)
1985 TIMI 1
1983 CASS
1986 GISSI andISIS-Z
1985 NCEP
2002 ALLHAT
1993 Superiority of
primary PCI vs fibrinolysis in
acute MI noted
2002 Efficacy of
drug-eluting vs bare-metal
stents determined
1992 SAVE
2007 Benefit of
cardiac resin-chronization
therapy in heart failure
demonstrated
2009 Deep gene sequencing for responsiveness to CV drugs performed
2009 Genomwide association in early onset MI described
2009 Left ventricular assist device as destination therapy in advanced heart failure shown to be effective

Cardiovascular disease
is the leading cause
of death worldwide
1 in every 2.4 deaths
> 17 million people worldwide every year
Murray CJL, Lopez AD, eds.The Global Burden of Disease; Boston: Harvard School of Public Health;1996

Atherosclerosis
Hypertension Smoking
Obesity Diabetesmellitus
DYSLIPIDAEMIA

Cholesterol, particularly
LDL- cholesterol is the pivotal risk factor
for atherosclerosis

Relative concentration of ApoB containing lipoproteins in normolipidaemic individuals
LDL
VLDL
IDL remnants
Lipoprotein(a)
Ference et al. Eur Heart J 2017;38:2459-2472

LDL/HDL
Current smoking
Diabetes
Hypertension
Abdominal obesity
Psychosocial
Fruit & veg daily
Exercise
Alcohol intake
Odds Ratio
3.25
2.87
2.37
1.91
1.62
2.57
0.70
0.86
0.91
INTERHEART: Nine modifiable risk factors
predict 90% of acute myocardial infarction
N = 30 000
(262 sites across
52 countries)
Salim Yusuf Lancet 2004;364: 937-52

50%
40%
30%
20%
10%
0%
-10%
40%
50%
30%
20%
10%
0%
-10%
Pro
po
rtio
na
l re
du
ction in e
ve
nt ra
te (
SE
)
0.5 1.5 2
0.5 1 1.5 2
1
Major vascular events
Major coronary events
For every 1 mmol/L reduction in
LDL cholesterol there is :
a) a 21 -24 % reduction in major
CAD or vascular events
b) a 12% reduction in overall
mortality
CTT Collaborators Lancet 2005;366:1267-99; n=90000
CTT Collaborators Lancet 2010;376:1670-81; n=170000
Relation between proportional
reduction in incidence of major
CAD and vascular events and
mean absolute reduction in
LDL cholesterol at 1 year
N= 170 000 subjects from 26 statin trials

80
60
40
20
0
Va
scu
lar
eve
nt fo
r p
rim
ary
en
dp
oin
t (p
er
10
00
pe
rson
ye
ars
)
75
64
28
19
25
15
77
68
27 26
75
64
27
21
Those with diabetes but no CVDallocated to placebo
Those with diabetes & CVDallocated to statin
Those with diabetes & CVDallocated to placebo
Those with diabetes but no CVDallocated to statin
HPS CARDS ASPEN CTTC
RRR with statin (%) 18 33 37 18 3 20 27
RRR with statin(events/1000 person years) 14 9 9 14 1 15 7
Residual risk despite statin(events/1000 person years) 64 19 15 66 26 61 21
With CVD No CVD No CVD With CVD With CVDNo CVD No CVD
STATINS ARE EFFECTIVE IN CAD PREVENTION BUT
DO NOT ELIMINATE THE RISK
“Residual Risk”
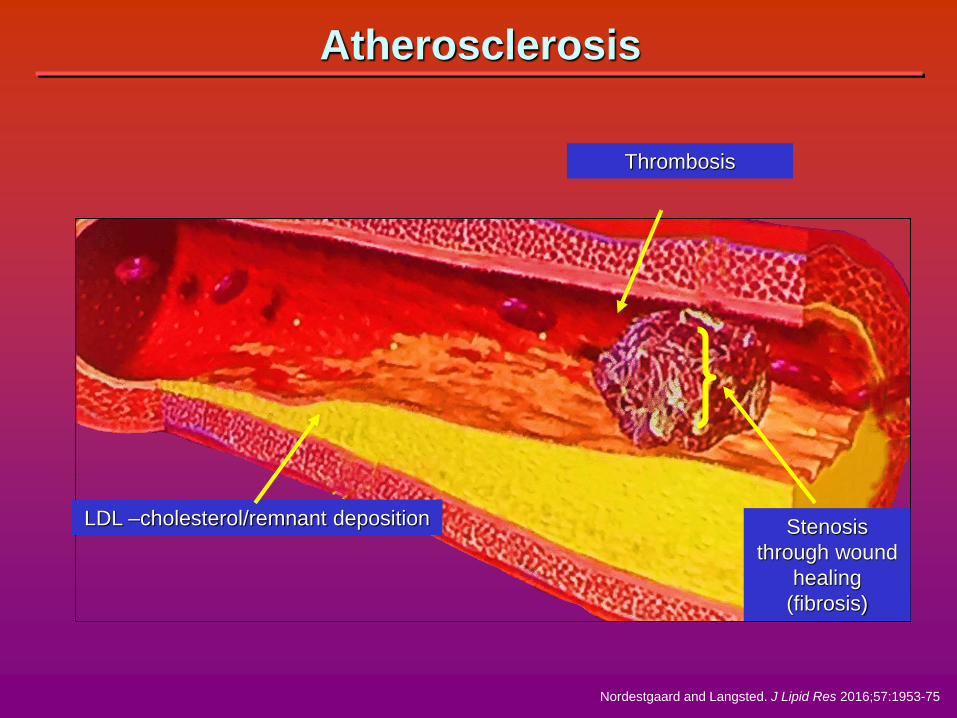
LDL –cholesterol/remnant deposition
Nordestgaard and Langsted. J Lipid Res 2016;57:1953-75
Stenosis
through wound
healing
(fibrosis)
Thrombosis
Atherosclerosis
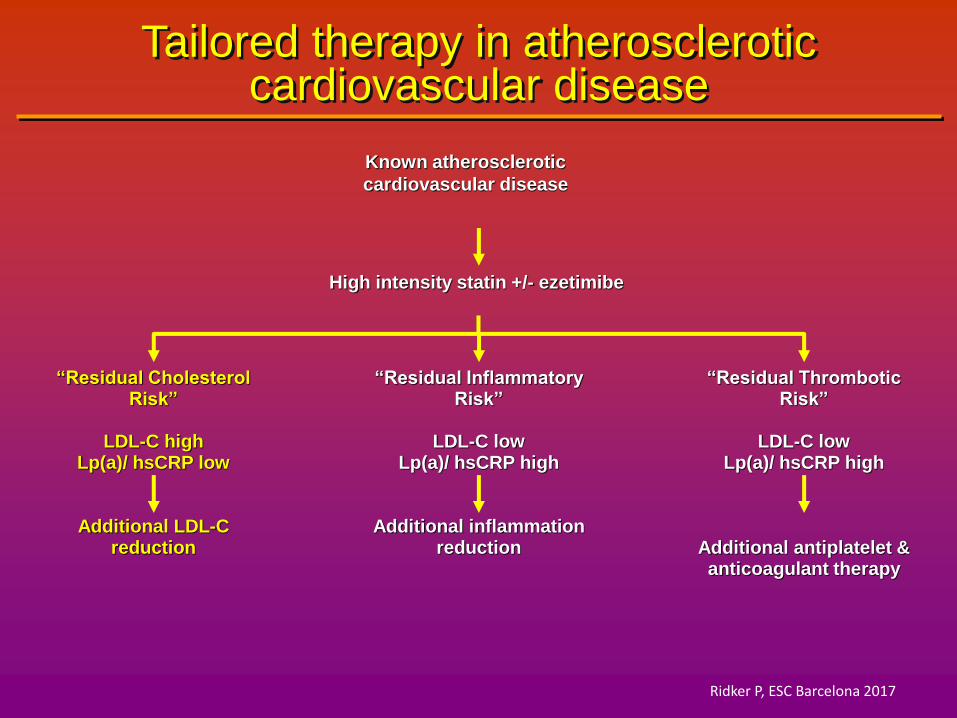
Tailored therapy in atherosclerotic cardiovascular disease
Known atherosclerotic
cardiovascular disease
High intensity statin +/- ezetimibe
“Residual Cholesterol Risk”
LDL-C highLp(a)/ hsCRP low
Additional LDL-C reduction
“Residual Inflammatory Risk”
LDL-C lowLp(a)/ hsCRP high
Additional inflammation reduction
“Residual Thrombotic Risk”
LDL-C lowLp(a)/ hsCRP high
Additional antiplatelet & anticoagulant therapy
Ridker P, ESC Barcelona 2017

15
10
5
-50%
10-20%
5-10%
55 - 70 %
reduction
In LDL-C
LDL-C
mmol/L
Reduction in LDL-C in FH with combination lipid-lowering therapy
Adapted from Nordestgaard B.G. et al. Eur Heart J 2013;34:3478-3490 and Hovingh G.K et al. Eur Heart J 2013;34, 962–971

100
80
60
40
20
01 2 3 4 65 7 8 9 10
LDL-C target
(mmol/L)
Att
ain
men
t o
f ta
rget
(%)
N=1249
Proportion of FH patients on LDL-C targets for different treatment goals
Pijlman AH, Atherosclerosis 2010;209:189-94
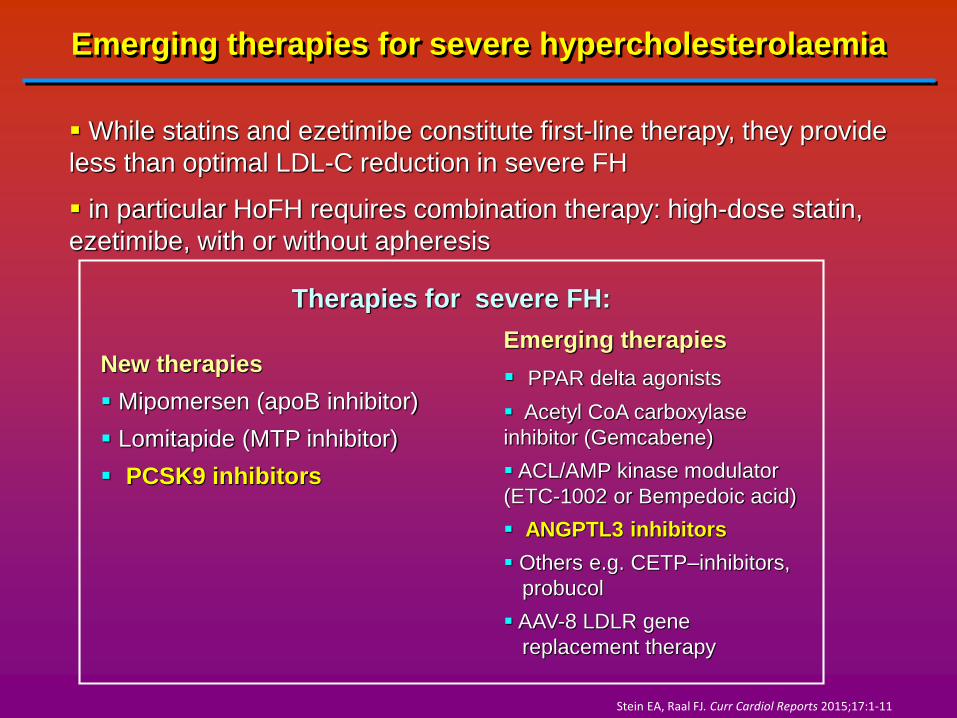
Emerging therapies for severe hypercholesterolaemia
While statins and ezetimibe constitute first-line therapy, they provide
less than optimal LDL-C reduction in severe FH
in particular HoFH requires combination therapy: high-dose statin,
ezetimibe, with or without apheresis
Emerging therapies
PPAR delta agonists
Acetyl CoA carboxylase
inhibitor (Gemcabene)
ACL/AMP kinase modulator
(ETC-1002 or Bempedoic acid)
ANGPTL3 inhibitors
Others e.g. CETP–inhibitors,
probucol
AAV-8 LDLR gene
replacement therapy
New therapies
Mipomersen (apoB inhibitor)
Lomitapide (MTP inhibitor)
PCSK9 inhibitors
Therapies for severe FH:
Stein EA, Raal FJ. Curr Cardiol Reports 2015;17:1-11
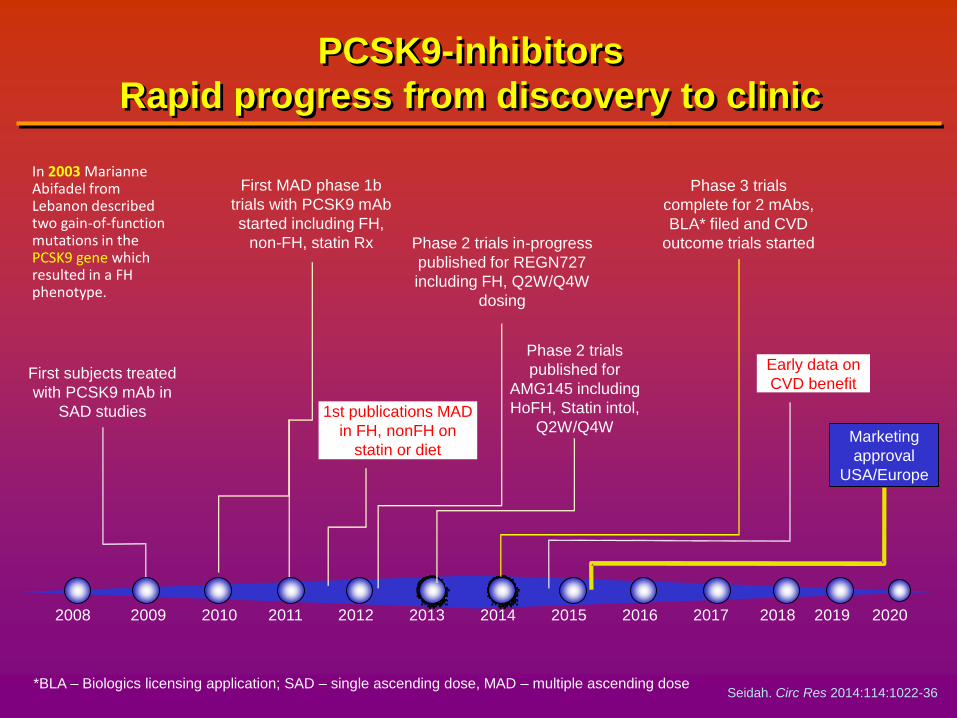
PCSK9-inhibitors
Rapid progress from discovery to clinic
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
First subjects treated
with PCSK9 mAb in
SAD studies
*BLA – Biologics licensing application; SAD – single ascending dose, MAD – multiple ascending dose
First MAD phase 1b
trials with PCSK9 mAb
started including FH,
non-FH, statin Rx Phase 2 trials in-progress
published for REGN727
including FH, Q2W/Q4W
dosing
Phase 2 trials
published for
AMG145 including
HoFH, Statin intol,
Q2W/Q4W
Phase 3 trials
complete for 2 mAbs,
BLA* filed and CVD
outcome trials started
1st publications MAD
in FH, nonFH on
statin or diet
Early data on
CVD benefit
Marketing
approval
USA/Europe
Seidah. Circ Res 2014:114:1022-36
In 2003 Marianne Abifadel from Lebanon described two gain-of-function mutations in the PCSK9 gene which resulted in a FH phenotype.

Modified from Bergeron et al. Circulation. 2015;132:1648-66
Pharmaceutical approaches targeting PCSK9
Approach
mAbs
Mimetic peptides
Adnectin
siRNA
Small molecules
Advantages
Highly selective
Less dosing frequencies
No serious adverse reactions
Highly selective
Easier production than mAbs
Selective
Easier & less costly production than mAbs
Highly selective
Oral administration
Low cost
Disadvantages
IV or subcutaneous
admin.
High cost
Short shelf life
Injection administration
Short half-life
IV or subcutaneous administration
Less selective
Greater likelihood of side effects
Compound
Alirocumab/ REGN7272/ SAR236553
Evolocumab/ AMG145
SX-PCK9
EGF-A peptide
BMS-962476
Inclisiran/ ALN-PCS (IV)
ALN-PCSsc (sub)
SBC-1 & SBC-1
Development stage
FDA approved July 24, 2015
Preclinical
Preclinical
Phase I completed
Phase I completed
Phase II recruiting
Preclinical completed
Company
Sanofi/Regeneron
Serometrix
Merck & Co
BMS-Adnexus
Alnylam Pharmaceuticals;
Medicines Company
Shifa Biomedical Corp
FDA approved Aug 27, 2015
Amgen
Pfizer/Genetech
Genentech/Roche
Development stopped in Nov 2016
Phase II
Bococizumab/ RN-316/ PFO4950615
RG7652(MPSK3169A)
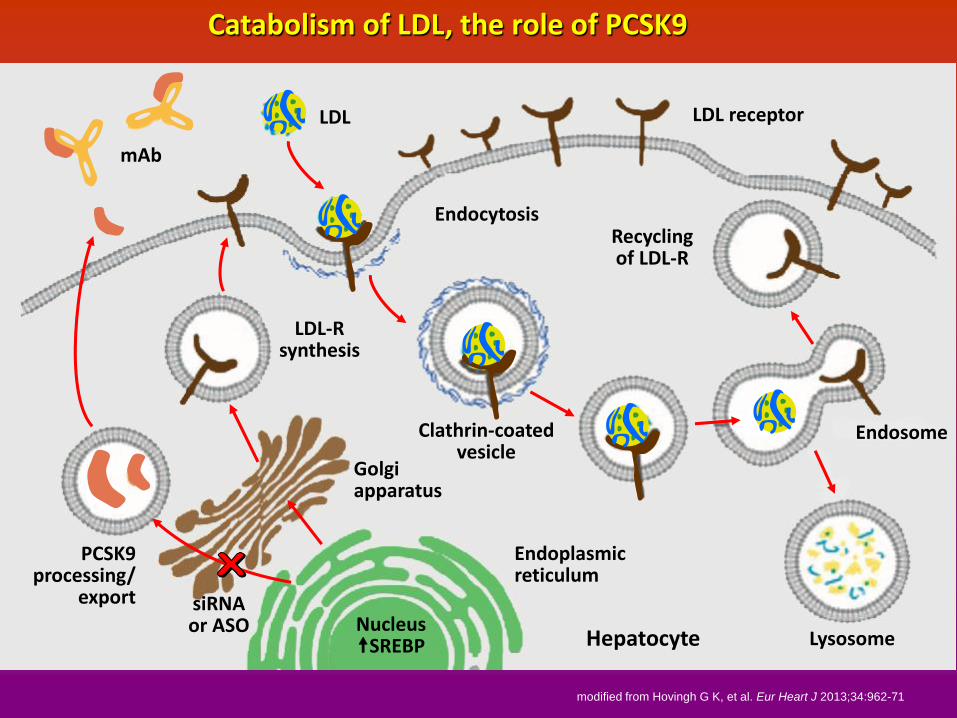
LDL
EndocytosisRecycling of LDL-R
LDL receptor
mAb
LDL-R synthesis
Clathrin-coated vesicle
Endoplasmic reticulum
Nucleus SREBP Hepatocyte Lysosome
Endosome
Golgi apparatus
PCSK9 processing/
export siRNA or ASO
modified from Hovingh G K, et al. Eur Heart J 2013;34:962-71
Catabolism of LDL, the role of PCSK9
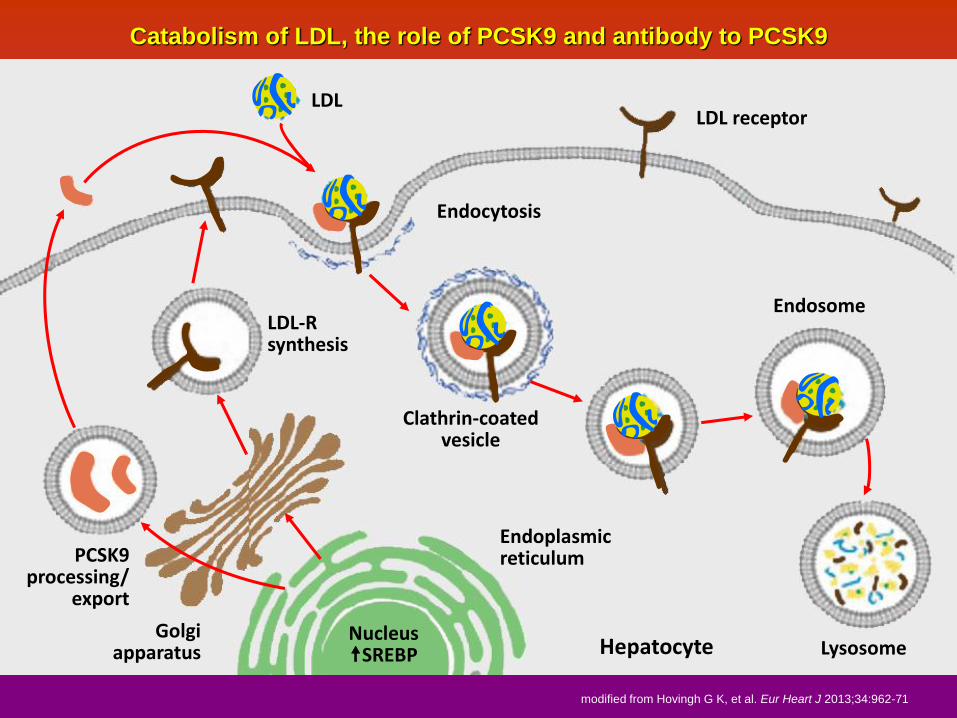
LDL
Endocytosis
LDL receptor
Endosome
Lysosome
Clathrin-coated vesicle
Hepatocyte
LDL-R synthesis
Endoplasmic reticulum
Nucleus SREBP
Golgi apparatus
PCSK9 processing/
export
Catabolism of LDL, the role of PCSK9 and antibody to PCSK9
modified from Hovingh G K, et al. Eur Heart J 2013;34:962-71

Stein E. N Engl J Med 2012;366:1108-18
Mean percent change from baseline in LDL-C values among healthy volunteers in single-dose studies
Subcutaneous administration of Alirocumab
-60
-50
-40
-30
-20
-10
0
10
20
-70
Me
an
ch
an
ge f
rom
ba
se
lin
e in
LD
L-C
(%
)
85 106
Study Day
Placebo 50 mg 100 mg 150 mg 250 mg
8443292215118421

PCSK9 Inhibitor CVD Outcomes Trials
www.clinicaltrials.gov (accessed September 6, 2017)
Sponsor
Trial
Sample size
Patients
Statin
LDL-C (mmol/L)
PCSK9i Dosing
Endpoint
Recruitment status
Completion
Evolocumab
Amgen
FOURIER
27,500
MI, stroke or PAD
Atorva ≥20 mg or equiv
≥1.8
Q2W or Q4W
Completed June 2015
ACC 2017
1º: CV death, MI stroke, revasc. or hosp for UA
Key 2º: CV death, MI or stroke
Alirocumab
Sanofi / Regeneron
ODYSSEY outcomes
17,000
4052 wks post-ACS
Evid.-based med Rx
≥1.8
Q2W
Completed Dec 2015
2017/2018
CHD death, MI, ischaemic stroke, or hospital for UA
Bococizumab
Pfizer
SPIRE I SPIRE II
17,000 9,000
High risk of CV event
Lipid-lowering Rx
1.8-2.6 ≥2.6
Q2W
Discontinued
2017/2018
CV death, MI, stroke, or urgent revasc.
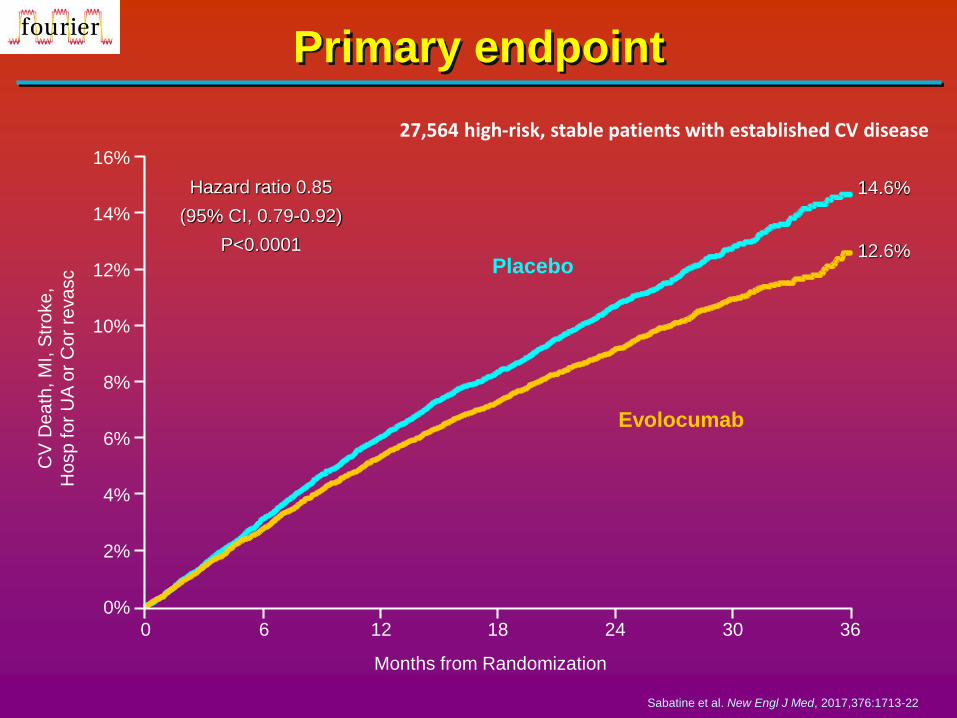
CV
De
ath
, M
I, S
tro
ke
,
Ho
sp
fo
r U
A o
r C
or
reva
sc
Primary endpoint
Evolocumab
Placebo
Hazard ratio 0.85
(95% CI, 0.79-0.92)
P<0.0001 12.6%
14.6%
0%
2%
4%
6%
8%
10%
12%
14%
16%
Months from Randomization
0 6 12 18 24 30 36
27,564 high-risk, stable patients with established CV disease
Sabatine et al. New Engl J Med, 2017,376:1713-22

0
Study Day
28 56
0
50
500
100
300
400
200
14 70 8442
LDL-C
Me
an C
han
ge (%
)
0
150
350
450
250
Total AMG 145 (evolocumab)
Free PCSK9
LDL-C
Fre
e P
CSK
9 c
on
cen
trat
ion
(n
g/m
L)Fr
ee
evo
locu
mab
co
nce
ntr
atio
n (
ng
/mL
x 0
.01
)
Pharmacokinetics and pharmacodynamics of
evolocumab: changes in PCSK9 and LDL-C levels
in response to evolocumab
Stein EA & Raal FJ Annu. Rev. Med. 2014. 65:417–31.
160
140
120
100
80
60
40
20
0
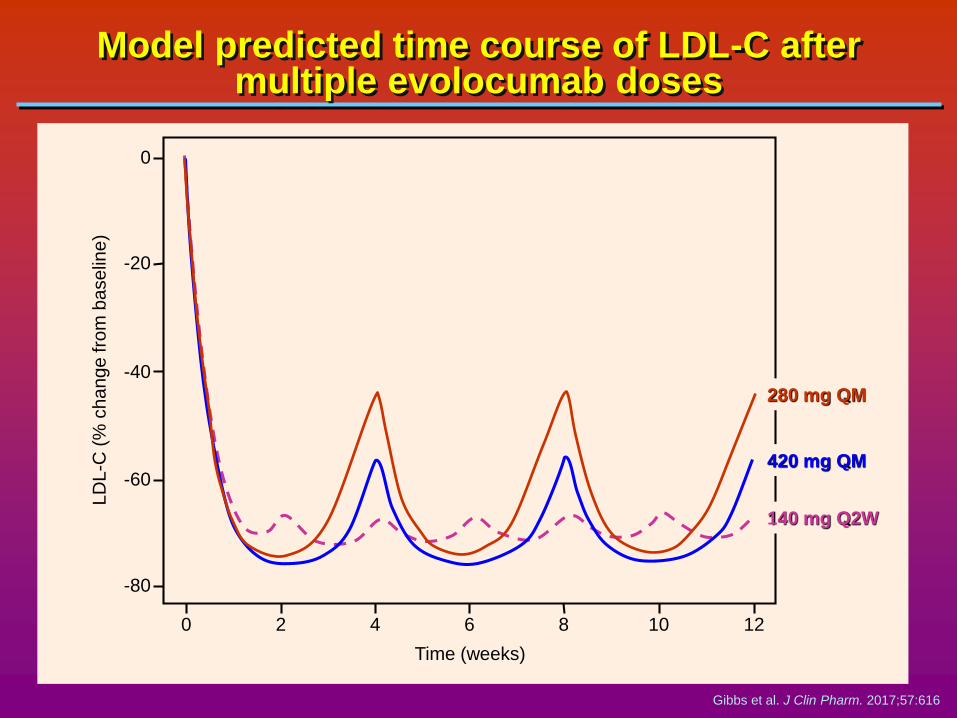
Model predicted time course of LDL-C after multiple evolocumab doses
Gibbs et al. J Clin Pharm. 2017;57:616
0
-20
-40
-60
-80
LD
L-C
(%
ch
an
ge
fro
m b
ase
line
)
0 2 4 6 8 10 12
Time (weeks)
280 mg QM
420 mg QM
140 mg Q2W

Whitehead et al. Nat Rev Drug Discov 2009;8:129-38
Small interfering RNA (siRNA) targeted to PCSK9: Mechanism of action
Long DNAsiRNA
Cytoplasm
Deer
AGO2
RISC
RISC assembly
Target mRNA recognition
Cleaved sense strand
Target mRNA cleavageRecycled RISC-siRNA
activated complex
Sense strand
Antisense strand
Target mRNA
5’ 3’GalNAc
GalNAc
GalNAc
Hepatic ASP
receptor
INCLISIRAN

Change in LDL-Cholesterol level in single-dose cohorts with Inclisiran
Fitzgerald K et al. N Engl J Med. 2017;376:41-51
160 180140120100806040200-80
-60
-40
-20
0
Days after dose
Me
an
ch
an
ge
fro
m b
ase
line
(%
)
Cohort
Placebo (n=6)
Inclisiran, 25 mg (n=3)
Inclisiran, 100 mg (n=3)
Inclisiran, 300 mg (n=3)
Inclisiran, 500 mg (n=3)
Inclisiran, 800 mg (n=6)

Ray et al. New Engl J Med 2017;376:1430-40
Inter-individual LDL-C lowering response to Inclisiran
Phase 2 Study
2.07
1.55
1.04
0.52
0
-0.52
-1.04
-1.55
-2.07
-2.59
-3.11
-3.63
-4.15
Cha
nge
fro
m b
ase
line in L
DL
-C (
mm
ol/L
)
2.07
1.55
1.04
0.52
0
-0.52
-1.04
-1.55
-2.07
-2.59
-3.11
-3.63
-4.15
Cha
nge
fro
m b
ase
line in L
DL
-C (
mm
ol/L
)Mean 1.66 mmol/L
Placebo group at day 180 Two-dose 300 mg Inclisiran group at day 180

LDL levels in FHFrom a lethal disorder to a manageable dyslipidaemia
Adapted from Kastelein JJP. Nat Rev Cardiol. 2014;11:629-631
11.7
10.4
9.1
7.8
6.5
5.2
3.9
2.6
1.3
0No
therapySimva 40 mg
Atorva 80 mg
Simva 40 mg
Simva 80 mg
Statin +Eze 10 mg
+ PCSK9-inhibitor
LD
L-C
levels
(m
mol/L)
Firstsynvinolin study
ASAP ENHANCE
RUTHERFORDODYSSEY I & II
TESLA, TAUSSIG
1986 2016

Tailored therapy in atherosclerotic cardiovascular disease
Known atherosclerotic
cardiovascular disease
High intensity statin +/- ezetimibe
“Residual Cholesterol Risk”
LDL-C highLp(a)/ hsCRP low
Additional LDL-C reduction
“Residual Inflammatory Risk”
LDL-C lowLp(a)/ hsCRP high
Additional inflammation reduction
“Residual Thrombotic Risk”
LDL-C lowLp(a)/ hsCRP high
Additional antiplatelet & anticoagulant therapy
Ridker PM, Eur Heart J 2016;37:1720-22
IMPROVE-IT: Ezetimibe 6% RR
FOURIER/SPIRE: PCSK9 inhibition Q2W 15% RRR
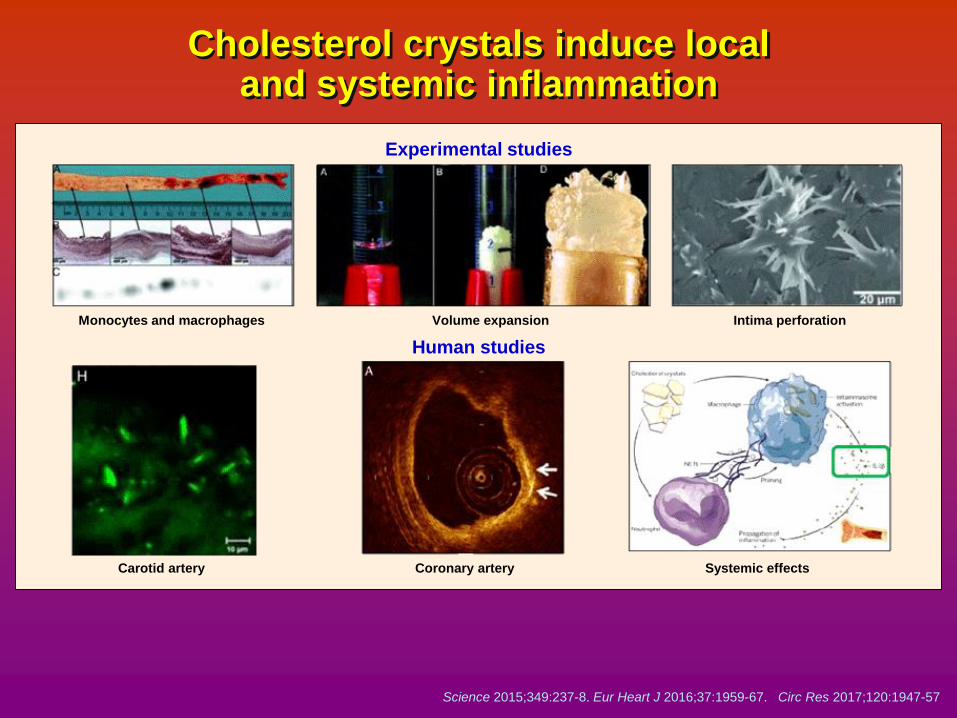
Science 2015;349:237-8. Eur Heart J 2016;37:1959-67. Circ Res 2017;120:1947-57
Cholesterol crystals induce local and systemic inflammation
Experimental studies
Human studies
Monocytes and macrophages Volume expansion Intima perforation
Carotid artery Coronary artery Systemic effects

Ridker PM et al, Circulation 2012;126:2739-2748
Activation of inflammasome - “clinical utility”
NLRP3inflammasome
IL-1β
TNF
IL-6
hsCRP
target
converter
distributor
biomarker

Ridker PM et al, Circulation 2012;126:2739-2748
CANTOS: dose-dependent effects on inflammatory biomarkers and lipids (38 months)
10
0
-10
-20
-30
-40
-50
-60
-70
hsC
RP
10
0
-10
LD
C
10
0
-10
HD
C
10
0
-10
TG
30 6 9 2412 36 48Months
Pa
tie
nt ch
an
ge
fro
m b
ase
line
(m
ed
ian)
Placebo SC q 3 nth
Canakinumab 50mg SC q 3 mth
Canakinumab 150mg SC q 3 mth
Canakinumab 300mg SC q 3 mth
Placebo Canakinumab 50 Canakinumab 150 Canakinumab 300

Ridker PM et al, New Engl J Med 2017;377:1119-31
CANTOS: greater risk reduction among those with greater hsCRP reduction (MACE+)
0.25
0.20
0.15
0.10
0.05
0.000 1 2 3 4 5
Follow-up years
Cu
mu
lative
in
cid
en
ce (
%)
HR 0.73
95% CI 0.63-0.83
p = 0.0001
Placebo
Canakinumab (on treatment hsCRP < median)
Canakinumab (on treatment hsCRP ≥ median)
for those with reductions
in hsCRP ≥median at 3
mths (1.8 mg/dL)
HR
1.0
0.95
0.73
(95% CI)
(referent)
(0.84-1.08)
(0.63-0.83)
P
(referent)
0.47
0.0001

CANTOS: additional outcomes (per 100 person years of exposure)
Adverse eventPlacebo
(N=3347)
50 mg
(N=2170
150 mg
(N=2284)
300 mg
(N=2263) P
Canakinumab SC q 3 months
* P-value for combined Canakinumab doses vs. placebo
Ridker PM et al, New Engl J Med 2017;377:1119-31
Any SAE
Leukopenia
Any infection
Fatal infection
Injection site reaction
Any malignancy
Fatal malignancy
Arthritis
Osteoarthritis
Gout
ALT >2x normal
Bilirubin >2x normal
12.0
0.24
2.86
0.18
0.23
1.88
0.64
3.32
1.67
0.80
1.4
0.8
11.4
0.30
3.03
0.31
0.27
1.75
0.55
2.15
1.21
0.43
1.9
1.0
11.7
0.37
3.13
0.28
0.28
1.69
0.50
2.17
1.12
0.35
1.9
0.7
12.3
0.52
3.25
0.34
0.30
1.72
0.31
2.47
1.30
0.37
2.0
0.7
0.43
0.002
0.12
0.9/0.02*
0.49
0.31
0.0007
0.002
0.04
0.0001
0.19
0.34

Tailored therapy in atherosclerotic cardiovascular disease
Known atherosclerotic
cardiovascular disease
High intensity statin +/- ezetimibe
“Residual Cholesterol Risk”
LDL-C highLp(a)/ hsCRP low
Additional LDL-C reduction
“Residual Inflammatory Risk”
LDL-C lowLp(a)/ hsCRP high
Additional inflammation reduction
“Residual Thrombotic Risk”
LDL-C lowLp(a)/ hsCRP high
Additional antiplatelet & anticoagulant therapy
Ridker PM, Eur Heart J 2016;37:1720-22
IMPROVE-IT: Ezetimibe 6% RR
FOURIER/SPIRE: PCSK9 inhibition Q2W 15% RRR
CANTOS
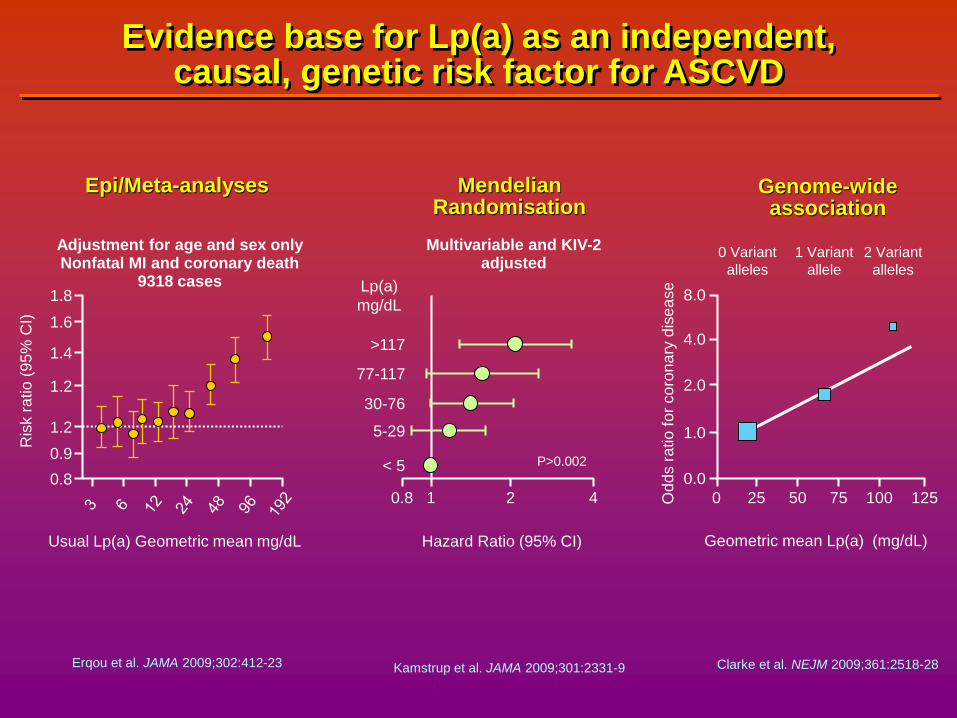
Evidence base for Lp(a) as an independent, causal, genetic risk factor for ASCVD
1.8
1.6
1.4
1.2
1.2
0.9
0.8
Usual Lp(a) Geometric mean mg/dL
Ris
k r
atio
(95
% C
I)
Adjustment for age and sex onlyNonfatal MI and coronary death
9318 cases
0.8 1 2 4
Hazard Ratio (95% CI)
P>0.002
Lp(a)
mg/dL
>117
77-117
30-76
5-29
< 5
Multivariable and KIV-2 adjusted
Epi/Meta-analyses Mendelian Randomisation
0 25 50 75 100 125
0.0
1.0
2.0
4.0
8.0
Geometric mean Lp(a) (mg/dL)
Od
ds r
atio
fo
r co
ron
ary
dis
ea
se
0 Variant
alleles
1 Variant
allele
2 Variant
alleles
Genome-wide association
Erqou et al. JAMA 2009;302:412-23 Kamstrup et al. JAMA 2009;301:2331-9 Clarke et al. NEJM 2009;361:2518-28

Helgadottir A. Nat Genet 2016;48:634-39
0.8
0.8
1.0
1.1
1.2
1.3
APOE LDLR
APOE
LPA
Non-HDL cholesterol effect of the minor allele
(mmol/L)
CA
D O
R
Lp(a) has ¼ effect of LDL-cholesterol on ASCVD risk but the effect
is 3 fold greater per mmol/L cholesterol

Comparison of cumulative effects of Lp(a) and LDL-C on CVD
50%
40%
30%
20%
10%
0%
0 20 40 60 80 100 120
Absolute lowering of Lp(a) (mg/dL)
Red
uctio
n in
CH
D r
isk
Genetic estimates
Observational estimates
Trial estimates (predicted)
50%
40%
30%
20%
10%
0%
0 0.3 0.3 0.5 1.0
Absolute lowering of LDL-C (mmol/L)
Red
uctio
n in C
HD
ris
k
Genetic estimates
Observational estimates
Trial estimates
Exome. CHD consortium 2017, in press

Changes in Lp(a) and LDL-C with equivalent effects on CVD
1.0 mmol/L lifetime lower LDL-C
50% reduction in lifetime risk of CHD
90 – 100 mg/dL lifetime lower Lp(a)
Reconciles epidemiologic and Mendellan randomisation studies
Explains failure of lowering Lp(a) in niacin, CETP and PCSK9 randomised trials
Informs the optimal design of RCTs for potent Lp(a) lowering agents
Ference B et al. Exome. CHD consortium 2017, in press

Viney et al. ACC 2016
Phase 2 IONIS-APO(a)Rx Study - mean change in Lp(a) in placebo and patients with Lp(a) 50-175 mg/dL and >175 mg/dL
30
0
-20
-40
-60
-80
1 190
Treatment period (days)
Fasting L
p(a
), m
ean %
change fro
m
ba
se
line
(±
SE
M)
16212085/99/ET
7857432915
Placebo
Cohort A
(> 175 mg/dL)
Cohort B
(50-175 mg/dl)

ATHEROSCLEROSIS
“chronic inflammatory fibroproliferative
process which is excessive and in its
excess, this protective response has
become a disease state.”
Russell Ross; New Engl J Med 1999;340:115-126

75th Percentile of CAC score in women (A) and men (B) across populations
700
600
500
400
300
200
100
045 50 55 60 65 70 75 80 85
Age (years)
45 50 55 60 65 70 75 80 85
Age (years)
75
thP
erc
en
tile
CA
C s
co
re
1800
1600
1400
1400
1000
800
600
400
200
0Tsimane
US women (UIC)
US women (MAHI)
US white women (MESA)
Korean women
US black women (MESA)
European women (HNR)
US Hispanic women (MESA)
US Chinese women (MESA)
Japanese women
Tsimane women
US men (MAHI)
US men (UIC))
US white men (MESA)
US black men (MESA)
US Hispanic men (MESA)
European men (HNR)
Korean men
US Chinese men (MESA)
Japanese men
Tsimane men
Tsimane
A B
Kaplan H, et al. Lancet 2017;389:1730-39

CAC scores by age for US MESA and Tsimane populations
100
90
80
70
60
50
40
30
20
10
0
Pro
po
rtio
n o
f in
div
idu
als
(%
)
0%
40-44 45-54 55-64 65-74 75-84
Age group (years)
1%
6%2%
17%
8%
34%
36%
8%
19%
51%
65%72%
83%
92%
55%
75%
Tsimane
CAC = 0
MESA
CAC = 0
MESA
CAC >100
Tsimane
CAC >100
Kaplan H et al. Lancet 2017;389:1730-39
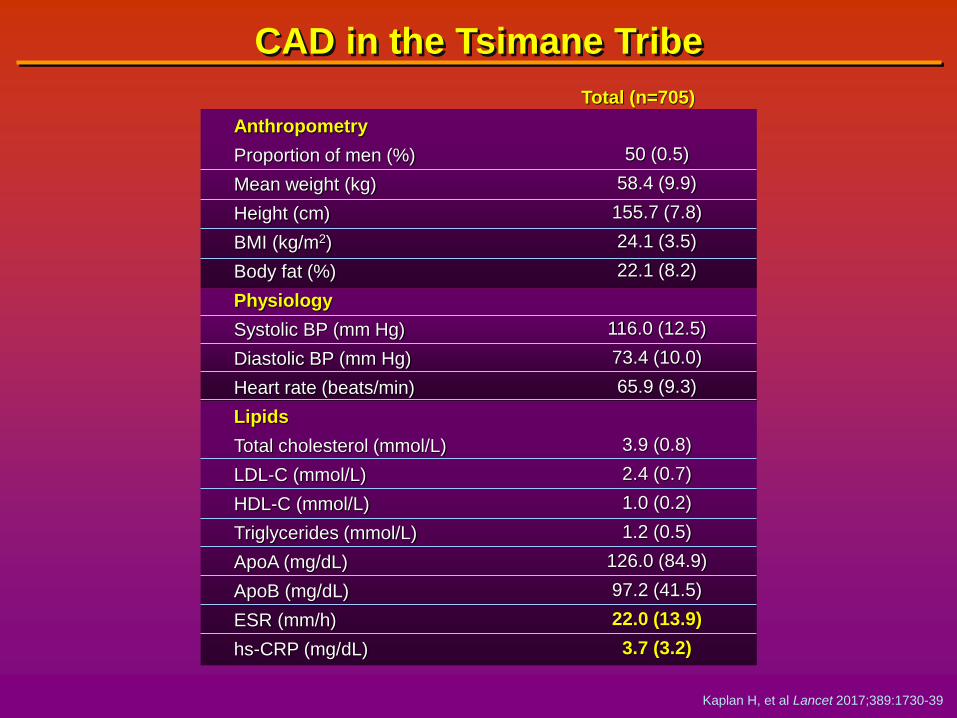
CAD in the Tsimane Tribe
Kaplan H, et al Lancet 2017;389:1730-39
Total (n=705)
Anthropometry
Proportion of men (%)
Mean weight (kg)
Height (cm)
BMI (kg/m2)
Body fat (%)
Physiology
Systolic BP (mm Hg)
Diastolic BP (mm Hg)
Heart rate (beats/min)
Lipids
Total cholesterol (mmol/L)
LDL-C (mmol/L)
HDL-C (mmol/L)
Triglycerides (mmol/L)
ApoA (mg/dL)
ApoB (mg/dL)
ESR (mm/h)
hs-CRP (mg/dL)
50 (0.5)
58.4 (9.9)
155.7 (7.8)
24.1 (3.5)
22.1 (8.2)
116.0 (12.5)
73.4 (10.0)
65.9 (9.3)
3.9 (0.8)
2.4 (0.7)
1.0 (0.2)
1.2 (0.5)
126.0 (84.9)
97.2 (41.5)
22.0 (13.9)
3.7 (3.2)

Tuberculosis is also a disease that has
a strong inflammatory component
It is associated with :-
• Influx of macrophages and T cells
• high levels of inflammatory cytokines
• elevated CRP
However treatment of this “inflammatory disease” is
the elimination of Mycobacterium tuberculosis, the root
cause

Likewise, in atherosclerosis, inflammation
is a consequence of LDL retention in the
sub-endothelial space, not the cause
The most successful treatment of
atherothrombotic vascular disease in humans is
therefore to address the root cause,
namely LDL-cholesterol!
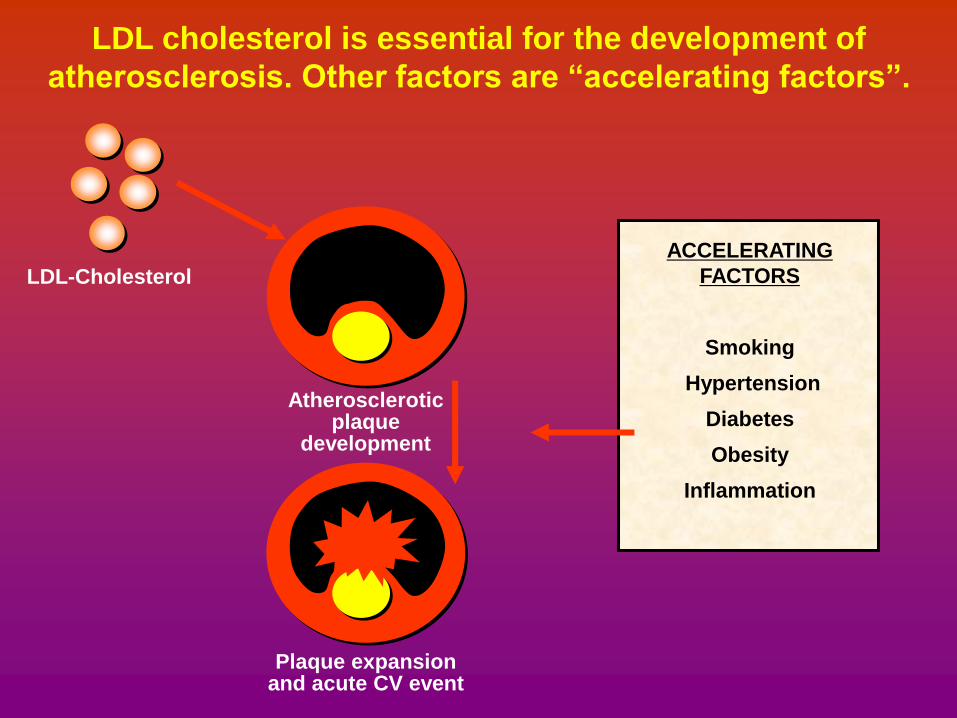
LDL-Cholesterol
Atherosclerotic plaque
development
Plaque expansion and acute CV event
ACCELERATING
FACTORS
Smoking
Hypertension
Diabetes
Obesity
Inflammation
LDL cholesterol is essential for the development of
atherosclerosis. Other factors are “accelerating factors”.

Can we go too low?
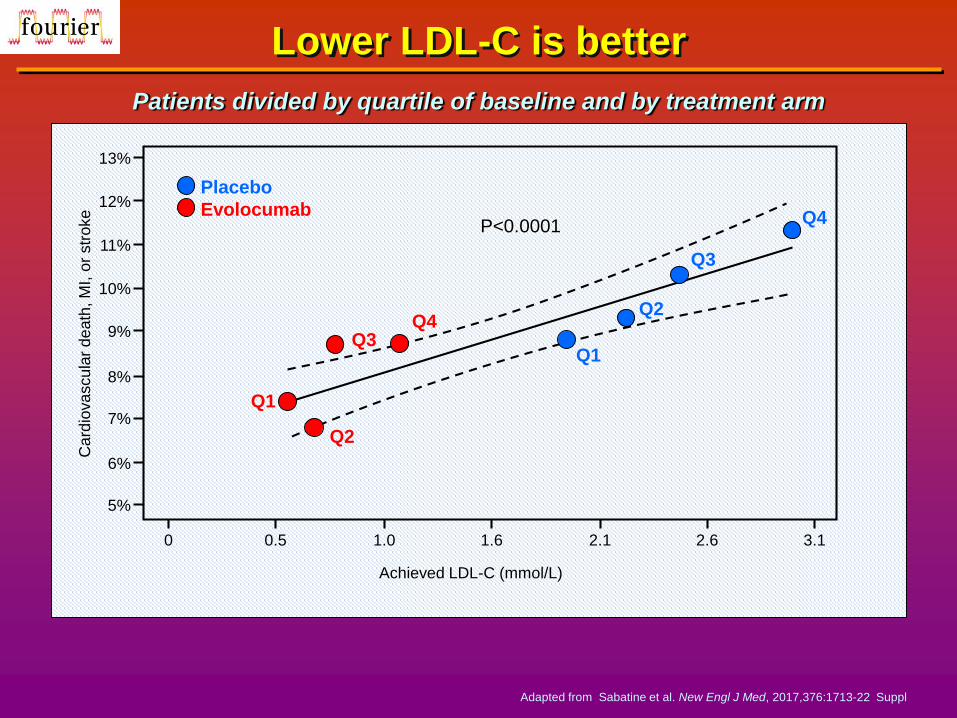
Lower LDL-C is better
12%
11%
10%
9%
8%
7%
6%
5%
13%
0 0.5 1.0 1.6 2.1 2.6 3.1
Achieved LDL-C (mmol/L)
Card
iova
scu
lar
de
ath
, M
I, o
r str
oke
P<0.0001
Patients divided by quartile of baseline and by treatment arm
Q3
Q1
Q2
Q4
Q1
Q2
Q3
Q4
Placebo
Evolocumab
Adapted from Sabatine et al. New Engl J Med, 2017,376:1713-22 Suppl
Clinical Efficacy and Safety of Achieving Very Low LDL Levels with the
PCSK9 Inhibitor Evolocumab in theFOURIER Outcomes Trial
RP Giugliano, TR Pedersen, AV Keech,
PS Seever, JG Park, and MS Sabatine, for the
FOURIER Steering Committee & Investigators
Presented at ESC, Barcelona, August 2017
Published in the Lancet 2017 ;390;1962-1971
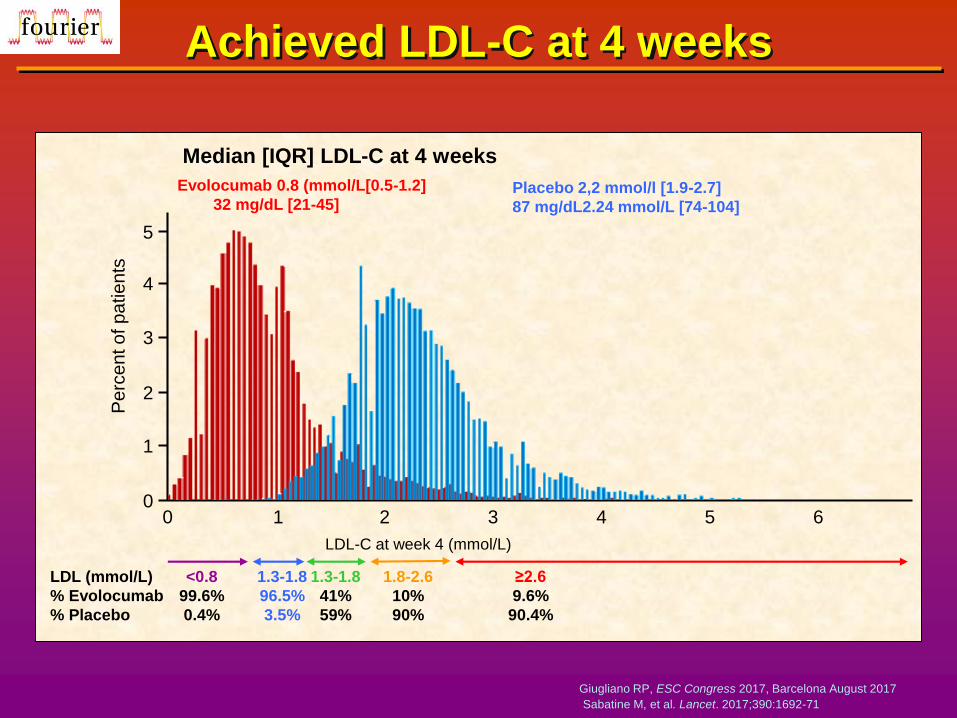
Achieved LDL-C at 4 weeks
Giugliano RP, ESC Congress 2017, Barcelona August 2017
Sabatine M, et al. Lancet. 2017;390:1692-71
4
5
2
1
0
3
Pe
rce
nt o
f p
atie
nts
0 1 2 4 5 6
≥2.6
9.6%
90.4%
1.8-2.6
10%
90%
1.3-1.8
41%
59%
1.3-1.8
96.5%
3.5%
<0.8
99.6%
0.4%
LDL-C at week 4 (mmol/L)
3
LDL (mmol/L)
% Evolocumab
% Placebo
Evolocumab 0.8 (mmol/L[0.5-1.2]
32 mg/dL [21-45]Placebo 2,2 mmol/l [1.9-2.7]
87 mg/dL2.24 mmol/L [74-104]
Median [IQR] LDL-C at 4 weeks

LDL-C over time
4
3
1
00 24 48 72 96 120 144 168
4 12
2
Weeks after randomisation
Mean L
DL
-C (
mm
ol/L)
Giugliano RP, ESC Congress 2017, Barcelona August 2017
Sabatine M, et al. Lancet. 2017;390:1692-71
LDL-C at 4 weeks in mmol/L
<0.5 0.5-1.3 1.3-1.8 1.8-2.6 ≥2.6
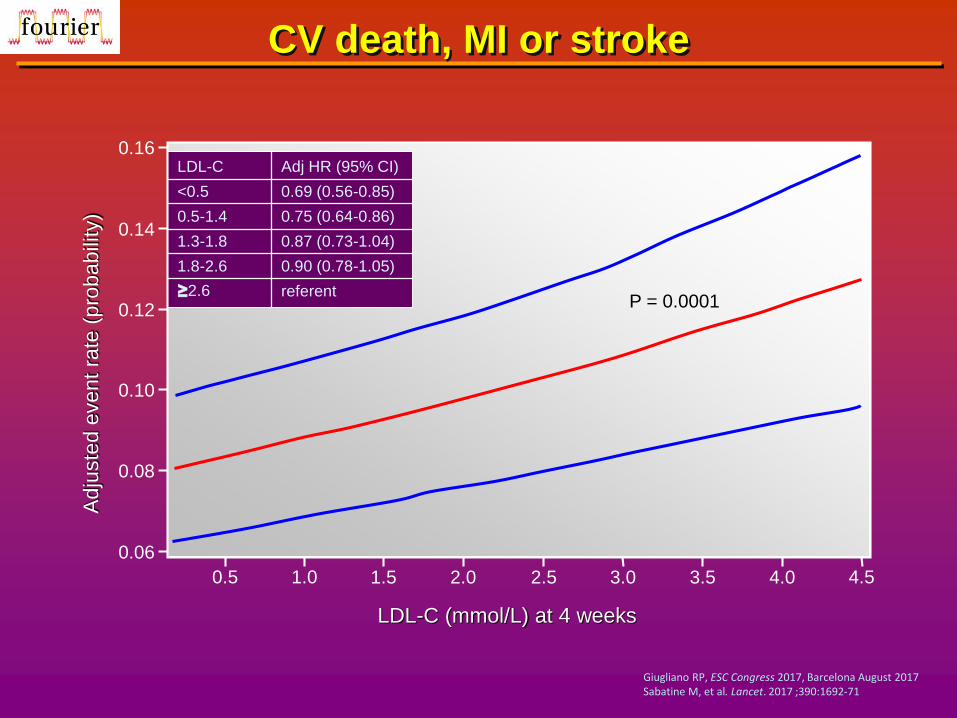
CV death, MI or stroke
0.16
0.14
0.12
0.10
0.08
0.06
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
LDL-C (mmol/L) at 4 weeks
4.5
LDL-C
<0.5
0.5-1.4
1.3-1.8
1.8-2.6
≥2.6
Adj HR (95% CI)
0.69 (0.56-0.85)
0.75 (0.64-0.86)
0.87 (0.73-1.04)
0.90 (0.78-1.05)
referentP = 0.0001
Adju
ste
d e
vent
rate
(pro
babili
ty)
Giugliano RP, ESC Congress 2017, Barcelona August 2017Sabatine M, et al. Lancet. 2017 ;390:1692-71
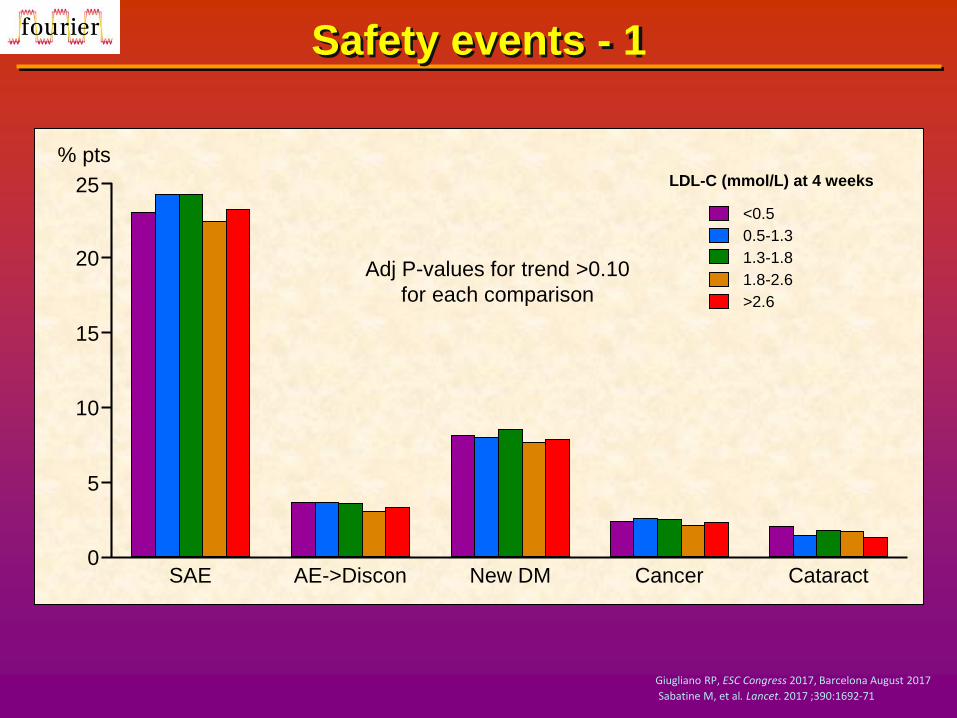
Safety events - 1
25
20
15
10
5
0
% pts
SAE AE->Discon New DM Cancer Cataract
Adj P-values for trend >0.10
for each comparison
LDL-C (mmol/L) at 4 weeks
<0.5
0.5-1.3
1.3-1.8
1.8-2.6
>2.6
Giugliano RP, ESC Congress 2017, Barcelona August 2017
Sabatine M, et al. Lancet. 2017 ;390:1692-71

Safety events - 2
LDL-C (mmol/L) at 4 weeks
<0.5
0.5-1.3
1.3-1.8
1.8-2.6
>2.6
10
5
% pts
0Neurocog AST/ALT CK Non-CV death Hemor stroke
Giugliano RP, ESC Congress 2017, Barcelona August 2017
Sabatine M, et al. Lancet. 2017 ;390:1692-71
Does reducing LDL cholesterol to low and very low levels have safety concerns?
In Fourier, reduction of LDL-C with evolocumab to a median of 0.78
mmol/L, with nearly 6,000 patients <0.65 mmol/L and 2500 patients
below 0.5 mmol/L, was not associated with any major safety concerns
such as haemorrhagic stroke, cognitive impairment or cataracts
Safety and benefit data for very low LDL-C based on increased LDL
clearance via upregulation of the LDL receptor (statins, ezetimibe and
PCSK9 inhibition) suggest eliminating a lower limit for LDL-cholesterol
Based on current evidence the real safety concern is under treatment
of LDL-C, not too low LDL-C!

A quarter of a century of treating LDL-C
5.18
4.66
4.15
3.63
3.11
2.59
2.07
1.55
1.04
0.52
01994 1996-2002 1994-2005 2015 2017
LD
L-C
(m
mo
l/L
)
High is bad
Lower is better
Even lower is even better
Lowest is best
Average is not good
Giugliano RP, ESC Congress 2017, Barcelona August 2017

Goldstein & Brown. Science 1996, 272:629

Cholesterol year score and the threshold for CHD
Concept of lifetime cumulative LDL-C exposure
and vascular risk
Adapted from Horton et al. J Lipid Res. 2009;50:S172-S177
1 20 40 60 80
Age (years)
Cum
ula
tive L
DL e
xposure
High RiskHeFHHoFH Mod. Risk
Statins, ezetimibe
plus PCSK9
inhibition
Ference B. Eur Heart J 2017;38:2459-72
The mean age at the time of
randomization in the statin
trials was 63 years

Comparative CHD risk reduction of earlier and later LDL-C lowering
Ference et al. JACC 2012;25: 2631-9
1.0 mmol/L
0.5 mmol/L
0.25 mmol/L
0.125 mmol/L
Genetic studies
Statin trials
Genetic studies
Statin trials
Genetic studies
Statin trials
Genetic studies
Statin trials
0.46 (0.41-9.51)
0.76 (0.74-0.78)
0.67 (0.64-0.72)
0.87 (0.86-0.88)
0.82 (0.80-0.85)
0.93 (0.93-0.94)
0.91 (0.89-0.92)
0.96 (0.96-0.97)
8.4x10-19
8.4x10-19
8.4x10-19
8.4x10-19
0.40 0.50 0.50 0.70 0.80 0.90 1.0
Lower LDL-C
Meta-analysis
312,321
169,138
212,321
169,138
312,321
169,138
312,321
169,138
Sample size (N)
OR (95% CI) P diff.

Lauf U, Ference B. Eur Heart J 2017, in press
Expected lifetime risk reduction with 50% reduction in LDL-C beginning in early adulthood
Baseline LDL-Cmmol/L
6.5
5.0
4.0
3.5
3.0
2.5
LDL-C mmol/Lafter 50% reduction
3.25
2.5
2.0
1.75
1.5
1.25
RR for CHDa
0.08
0.14
0.21
0.26
0.31
0.38
Relative reduction in lifetime risk
92%
86%
79%
64%
69%
62%
a Based on an expected 54% reduction in lifetime risk of ASCVD per mmol/L reduction in LDL-C
Importance of Early Treatment
10 80
Age (years)
40
Age of
intervention
Age at which clinical
horizon is reached

Biologics including PCSK9 inhibitors are very promising, and potentially the most effective, approach to further reducing LDL-cholesterol, the cause of atherosclerosis
Two large CVD outcome trials are completed or soon to be completed with the Amgen (evolocumab) and Sanofi (alirocumab) monoclonal antibodies and no significant adverse effects have emerged so far
“Residual risk” may well be the result of treating “too little, too late”
Earlier intervention and more aggressive LDL-cholesterol reduction is pivotal for effective treatment and prevention of atherosclerosis
Conclusions


















