New Approaches to Myeloid Disorders in Blood and...
69
New Approaches to Myeloid Disorders in Blood and Bone Marrow Kathryn Foucar, MD [email protected] July 2013 Colorado Society for Clinical Pathologists
Transcript of New Approaches to Myeloid Disorders in Blood and...

New Approaches to
Myeloid Disorders in
Blood and Bone
Marrow
Kathryn Foucar, MD
July 2013
Colorado Society
for Clinical
Pathologists

How to get from
2
to
and
Avoid
becoming

Goals • Master use of conventional
“tools” to sub-categorize myeloid
neoplasms; reorganize clues to
specific myeloid neoplasms
• Embrace the ever-expanding role
of molecular genetics in both
diagnosis and prognosis 3

4
Clinician to Pathologist
“What genetic tests do I
need to order in this case?”
“What do these results
mean?”

5
Old Expectations/Tools of the Trade
Good Old Days
Document and classify advanced disease
Tools of the Trade
Clinicopathologic correlation > 150yrs
Autopsy > 120yrs
Romanosky/cytochem stains ~ 100 – 120 yrs ago
Cytogenetics (1960) ~ 50yrs
Immunophenotype ~ 25 – 30 yrs

6
New Expectations/Tools of the Trade Today
• Provide comprehensive assessment of neoplasm
including molecular/genetic features
• Provide comprehensive prognostic factors
• Determine optimal treatment
• Predict risk of therapy
• Detect and quantify minimal residual disease
Tools of the Trade
• All traditional “tools”
• 8+ color Flow cytometry
• Molecular/genomic “tools” including Next
Generation Sequencing

Maintain all
“Good Old Days”
skills and
Expand Diagnostic
“Horizons” 7

Encode 2012
8

In the world of
Myeloid Neoplasms,
CML has always lead
the way
9

Battle
between
Bennett
and
Virchow
Leukemia First Described in 1845
10

Clinico-Pathologic
Correlation
Blood:
Buffy Coat
CML:
WBC > 900,000
WBC’s
11

Unstained
130 years ago 150 years ago 12

1960
13
Nowell and Hungerford
Philadelphia Chromosome

Courtesy J. Anastasi
1973
14

15
Courtesy J. Anastasi David Baltimore, 1980’s
1980’s; different groups

Ph1: reciprocal translocation
BCR-ABL1 fusion gene
1982-1985
Translocation results in
constitutive tyrosine kinase
activity CML 16

CML
•1st genetically defined
leukemia
•Must document BCR-ABL1
fusion gene for diagnosis
17

Source: Kalidas, et al.
NEJM 2001; 286:895-898
Leukemogenic
Effects of
Constitutive Non-
Receptor Tyrosine
Kinase Activation
18

Source: Kalidas, et al. NEJM 2001;286:895-898
Therapy to Block Tyrosine Kinase Activity (1987-1998 )
19

Blast-Phase in CML: 1983-present
Source: Hehlmann, R. How I treat CML blast crisis. Blood 2012;120:737.
20

Who 2008 Myeloid Neoplasm
• Myeloproliferative (MPN) (11)
• Myelodysplasia (MDS (8)
• MDS/MPN (4)
• Acute myeloid leukemia (24)
• Myeloid neoplasm with eos and
PDGFRA, etc (3) 21

Myeloid Neoplasms
• 4 broad categories
• Typical blood and BM features
• Systemic approach
• CBC clues, blast %, dysplasia,
megakaryocytes, degree of
maturation 22

Comparison of blood features
MDS MPN AML
23

MDS CML AML
Comparison of bone marrow features 24

25
Usual Features of Myeloid Neoplasms (at diagnosis)
Disorder Bld
Counts
BM
Cellularity
%
BM
Blasts
Maturation Morphol ↑
Spl/L
MPN ↑↑ Nl - ↑↑↑ Nl Present Nl
(megas)
Yes
MDS ↓↓ ↑ (usu) Nl –
19%
Present Dyspl. No
MDS/
MPN
↑, ↓ ↑↑ Nl –
19%
Present Dyspl. Yes
AML ↑, ↓ ↓ - ↑↑ (usu) 20% Minimal
(usu)
Dyspl.
(usu)
No
(usu)

26
Diagnosis requires integration of
• Clinical (e.g. spleen size)
• Hematologic (sequential CBC data)
• Other laboratory data (e.g. LDH)
• Morphologic (blood and bone marrow)
• Genetic features
Disorders are characterized by
• Uncontrolled cell proliferation (usually multiple lineages)
• Intact maturation (mature cells predominate)
Myeloproliferative Neoplasms

27 Erythrocytosis, thrombocytosis
74 yr-old Female Hgb 17 Hct 51% Plt 950,000

28 BM aspirate: ↑ cell, ↑ megakaryocytes
74 yr-old Female Hgb 17 Hct 51% Plt 950,000

29 BM biopsy: megs, dilated sinuses, EMH
74 yr-old Female Hgb 17 Hct 51% Plt 950,000

Likely Diagnosis?
P vera
30

31
71b22

32
71b26
Bone marrow core: osteosclerosis

33
•60b29, 62b33 inset
BM: pleomorphic megas; Bld: LER

Likely Diagnosis?
Primary
myelofibrosis
(PMF) (Or: Post polycythemic PV-history is key!)
34

What additional tests
are needed?
•JAK2 mutation analysis
including Exon 12
•Exclude BCR-ABL1
•Possible karyotype 35

36
Janus Kinases in Cytokine Signal Transduction
Source: Goldman,
J. NEJM 352;17,2005
Receptor
tyrosine kinase
negative
transmembrane
receptors
include EPO,
TPO, G-CSF
receptors

37
Why Does Excess, Unregulated Cell
Production Occur?
CML
Ph1 t(9;22) results in BCR-ABL1 fusion gene
with constitutive tyrosine kinase activity
Other MPN
Point mutation in regulatory region of JAK2
results in constitutive tyrosine kinase activity

38
MPN: Key Tips
• Recognize blood clues
• Molecular genetic assessment
essential (BCR-ABL1, JAK2)
• Assess for mast cell infiltrates
• Recognize features of disease
progression

Myelodysplasia
• Ineffective HP results in cytopenias
despite hypercellular BM
• Hallmark of cytopenias with
dysplasia
• Variable % blasts in blood and BM
• Dysplasia may involve 1, 2, or 3 HP
lineages 39

40 Neutropenia; assess qual/quant all lineages

Elderly Patient with
Unexplained Cytopenia(s)
• Common problem
• All the usual causes of anemia excluded
• Must distinguish MDS from non-
neoplastic
• Low grade MDS very challenging
–Minimal (so-so) dysplasia
–Normal cytogenetics 41

Blood Features in MDS
42 Blasts < 20% Dysplasia

Bone Marrow Aspirate in MDS
43 Megakaryocyte abnormalities; small, pawn ball

MDS – Look Alike • Zinc induces
copper
deficiency
• Cytopenias
• Vacuoles
• Normalizes
when zinc
discontinued
44

MDS: Key Tips
• Exclude lookalikes
• Low grade MDS dx of exclusion
• Count blasts in blood and BM
• Assess architecture
• Conventional cytogenetics key
(better than FISH)
• Exclude low blast count AML 45

Acute Myeloid Leukemia
• Many molecular genetic subtypes
• Key AML-defining genotypes
• Usual threshold 20% blasts
in blood and BM (exceptions)
46

Blasts and Immature Myeloid
Elements
• Myeloblasts
• Promyelocytes*
• Monoblasts
• Promonocytes
• Erythroblasts†
• Megakaryoblasts
47
* Blast equivalent in some AML’s † Not typically included in blast % except for acute erythroid leukemia

Myeloid Blasts

49
Acute megakaryoblastic leukemia

50 Acute megakaryoblastic leukemia

51
NSE
AMoL, t(9;11)(p22;q23)
Forward Scatter
Sid
e S
catt
er
CD45
Sid
e S
catt
er
Sid
e S
catt
er
CD45 CD14 CD4
CD
8
CD45
HL
A-D
R

AML with multilineage dysplasia 52

AML: Morphologic Classification*
*Source: J Clin Oncol 21:256, 2003
Years from Start of Therapy
53

Acute Promyelocytic Leukemia t(15;17)(q22;q11-12)
Clinical: Constant rate over lifetime Profound thrombocytopenia; coagulopathy Medical emergency!
54
Morphology: Major: Hypergranular promyelocytes (low WBC) Microgranular: 1) folded nuclei (high WBC) 2) inconspicuous granules Little, if any, maturation beyond promyelocyte
Cytogenetics/ Molecular:
t(15;17) PML/RARα fusion gene
IP: My antigen + , HLA/DR - , CD34 -, MPO+, High side scatter!
Outcome: Manage coagulopathy; favorable risk

APL with t(15;17) - Note cells rare in blood 55

Elevated WBC: Microgranular APL; looks Monocytic 56

WHO 2001: Acute Myeloid Leukemia
57
I. AML with recurrent cytogenetic abnormalities
• AML with t(8;21) (AML1/ETO)
• AML with inv(16) (CBFβ/MYH11)
• APL with t(15;17) (PML/RARα)
• AML with 11q23 (MLL) abnormalities
II. AML with multilineage dysplasia
III. Therapy – related AML/MDS: 2 types
IV. AML, NOS (lineage based)
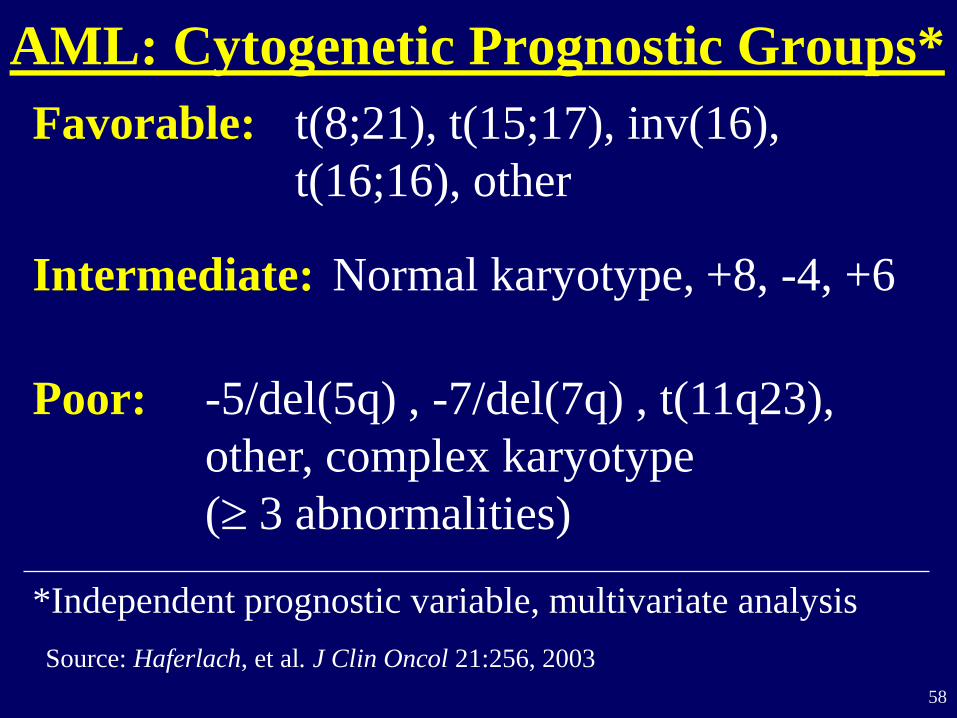
AML: Cytogenetic Prognostic Groups*
Favorable: t(8;21), t(15;17), inv(16),
t(16;16), other
Intermediate: Normal karyotype, +8, -4, +6
Poor: -5/del(5q) , -7/del(7q) , t(11q23),
other, complex karyotype
( 3 abnormalities)
*Independent prognostic variable, multivariate analysis
Source: Haferlach, et al. J Clin Oncol 21:256, 2003
58

59
AML: Overall Survival by Karyotype*
Years from Start of Therapy
*Source: J Clin Oncol 21:256, 2003
P < 0.0001

AML Classification: Biologic Groups
2001 2008
AML with
recurrent genetic
abnormalities
4 types 9 types
t(1;22), NPM1, CEBPA,
inv(3), t(6;9)
AML with MDS-
related changes
AML after MDS AML after MDS, MDS/MPN
AML with multi. dysplasia
AML with MDS karyotypes
Therapy-related
AML
Alkylating Agent
Topo II inhibitor
T-AML, MDS, MPN
T-AML with balanced tx
T-AML w/o translocations
Down Syndrome None Transient abnormal
myelopoiesis, other
leukemias 60

AML: Overall Survival
Source: Grimwade, Hematology 2009 61

Combined Cytogenetic and Molecular
Stratification
Favorable
t(8;21), inv(16), t(15;17)
Mutated NPM1 without FLT3
Mutated CEBPA (normal CC)
Intermediate-1
(normal CC)
Mutated NPM1 and FLT3-ITD
Wild-type NPM1 with /without FLT3-ITD
Intermediate-2
t(9;11); other cytogenetics
Adverse inv(3), t(6;9), other MLL, -5, del (5q,) -7,
complex
62

63

AML: Class I and Class II Mutations
Class I Mutations
(Proliferation)
Class II Mutations
(Impaired differentiation)
FLT3 PML-RARA
KIT RUNX1-RUNX1T1
RAS CBFB-MYH11
PTPN11 MLL fusions
JAK2 CEBPA
* The mechanism of leukemogenesis for NPM1
mutations remains somewhat unclear 64

65
Source: NEJM 366(12):1079-89, 2012
400 cases; patients <60 massive parallel sequencing

Acute Myeloid Leukemia
Source: Patel, et al. NEJM 366:1079, 2012
Gene Overall
Frequency (%)
FLT3 (ITD, TKD) 37 (30, 7)
NPM1 29
DNMT3A 23
NRAS 10
CEBPA 9
TET2 8
WT1 8
IDH2 8
IDH1 7
KIT 6
RUNX1 5
MLL-PTD 5
ASXL1 3
PHF6 3
KRAS 2
PTEN 2
TP53 2
HRAS 0
EZH2 0
A Total Cohort

67 Source: Patel, et al. NEJM 366:1079, 2012

68 Source: NEJM 366(12):1079-89, 2012

• Dramatic expansion of
realm of pathology
expertise
• Dramatic pace of new
discoveries
• “Survival of the fittest” 69