
New Approaches in Joints Pain - Cloud Object Storage ... · New Approaches in Joints Pain ......
89
LUBLIN 2013 New Approaches in Joints Pain Tennis Elbow edited by Karolina Janikowska, Katarzyna Chomiuk
Transcript of New Approaches in Joints Pain - Cloud Object Storage ... · New Approaches in Joints Pain ......

LUBLIN 2013
New Approaches in Joints Pain
Tennis Elbow
edited by Karolina Janikowska, Katarzyna Chomiuk

1
Reviewer: Ewa Kołodziej, CPT
Edited by: Karolina Janikowska, Katarzyna Chomiuk
Copyright © 2013 Karolina Janikowska. All rights reserved.
Published by Medunio 2013, Lubartowska 38/19, Lublin
Photo: Michał Wroński
ISBN : 978-83-938086-0-1
First edition

2
CONTENTS
The influence of the physical therapy on pain and elbow function in
patients with lateral epicondylitis .......................................................... 3
The role of Mulligan Therapy Concept in treatment of "tennis elbow"
symptoms ............................................................................................. 20
The review of the mobilization with movement techniques in
management of tennis elbow ............................................................... 35
Effects of Kinesio® taping in patients with symptoms of lateral
epicondylalgia ...................................................................................... 43
Review of the musculofascial Kinesio® taping applications for the
lateral epicondylalgia – part 1 ............................................................. 59
Review of the musculofascial Kinesio® taping applications for the
lateral epicondylalgia – part 2 ............................................................. 66
Kinesio® taping application for elbow pain ....................................... 76

3
Karolina Janikowska, Joanna Fidut
The influence of the physical therapy on pain and elbow function in patients with lateral epicondylitis
Background
Lateral epicondylitis is one of the most common cause of elbow pain related to the pathology
of the muscle extensor carpi radialis brevis [1,2]. In every population it can affect from from 1
to 3 % of active working people[3]. It can impaired the function of the dominating hand in
men and women [1,4]. The disorder is often defined as the repetitive strain injury of the
muscles attached to the lateral epicondylitis [5]. Previous studies pointed the tennis elbow as
the type of tendinitis what suggested the presence of the acute inflammatory process. Current
research investigating the absence of inflammatory marker in patients with tennis elbow
indicating the term “tendinosis” or “tendinopathy” as more appropriate to reflect the chronic
process [6,7]. The basic symptom of the tennis elbow is pain localized in the area of the
lateral epicondyle aggravating with hand grips and resistance applied to the muscles of the
forearm during the wrist extension[8].
The conservative therapy is based on use of ultrasound, cryotherapy, heat, electrical and laser
stimulation or extracorporeal shock wave therapy [9-15]. The other possible treatment is
based of pharmacological preparates e.g. non- steroidal anti-inflammatory drugs (NSAID),
corticosteroids prepared for the injections in the area of the lateral epicondyle [16-19].
Modern therapies focus on the botulinum toxin type A injections in improving the healing of
the tendons attached to the lateral epicondyle [20,21]. Another type of injections performed in
this area is use of the platelet-rich plasma extracted from the patient’s own blood and the
effect of the autologos growth factors [22,23]. The physical therapy seems to be still more
accessible for the patient and less invasive than even very promising biological treatment.
4
Aim of the study
The aim of the was to assess the influence of physical therapy set based on ultrasound, laser
and hydromassage stimulation on pain and the functional status of the patients with lateral
epicondylalgia.
Material and methods
The study was conducted on group of 28 patients (19 men and 9 women) diagnosed with
lateral epicondylalgia who suffered for at least three months and failed to the conventional
therapy. The exclusion criteria for the study was: previous injury of the elbow in anamnesis,
structural changes in the area of the elbow, osteoarthritis of the elbow, receiving any therapy
for lateral epicondylitis during last 4 weeks, cervical spine changes and symptoms of
radiculopathy, skin changes, allergy observed after tape application, inflammation in the
elbow area and general contraindication for each of the physical therapy method.
During the study the patients underwent physical examination of the upper limbs.
The standardized questionnaires e.g. Quick DASH (Disability of the Arm, Shoulder and
Hand) and PRTEE (Patients’ Related Tennis Elbow Examination) were used to assess the
functionality in this condition. To determinate the severity of the pain the visual-analog scale
(VAS) was applied.
DASH and Quick DASH
The Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure is 30-item, self-
report questionnaire developed to measure physical function and symptoms in patients with
musculoskeletal dysfunctions of the upper limb. It was released in 1996 [24]. This tool was
designed by the Institute for Work & Health and the American Academy of Orthopaedic
Surgeons (AAOS) and supported by the American Association for Hand Surgery, the
American Orthopaedic Society for Sports Medicine, the American Shoulder & Elbow
Surgeons, the American Society for Surgery of the Hand, the Arthroscopy Association of
North America and the American Society of Plastic and Reconstructive Surgeons [25]. The
QuickDASH is a shortened version of the DASH Outcome Measure. Instead of 30 items, the
QuickDASH based on 11 items to measure functionality and symptoms of patients with any
musculoskeletal disorders of the upper limb. Scoring is divided into the two components: the
disability/symptom section, consisting of 11 items, scored 1-5 and the optional high
performance sport/music or work modules with 4 items, scored 1-5. To calculate the score at
5
least 10 of the 11 items must be completed. Bacause this tool was developed to measure the
disability, the scaling was ranked from 0 indicating least disability to 100 indicating most
disability. The researcher should be aware of the direction of the scales [26]. This tool
included also two optional modules intended to assess symptoms and function in athletes,
performing artists and high degree physical performance workers. Both instruments are valid,
reliable and responsive and can be used for clinical and research purpose [26,27]. The tools
are characterized by rating of intra-class correlation coefficient on 0.94 and Cronbach’s alpha
also on. 0.94 [28].
The Patient-rated Tennis Elbow Evaluation (PRTEE)
This instrument enables quantitative rating by the patient of pain and functional impairment
associated with lateral epicondylitis, commonly called “tennis elbow”. PRTEE is an
instrument that has been developed specifically for use with this disorder, and is increasingly
being included in research, especially randomized controlled trials.
The questionnaire consist of a 15-item, with five addressing pain and ten concerned with
functional impairment. Each of the item are rated with use of 0 – 10 numerical scale to assess
the average pain or difficulty they have faced over the previous week during various activities
that usually cause pain in tennis elbow. In this system the pain and function are weighted
equally in the total score [29,30]. Higher scores present greater severity and the maximum
score is 100. Major advantages of this instrument are its simplicity, shortness and specificity
to lateral epicondylitis [31,32]. The characteristic of the test is based on recent study used a
four-week test-retest period and calculated Intraclass Correlation Coefficient values of 0.81
for the pain sub-score and 0.76 for the total score. In another studies the Cronbach's alpha
coefficients were high for both the pain and function sub-scales (0.84 and 0.93, respectively)
[33,34].
Pain assessment - Visual-analog scale (VAS)
Visual-analog scale is a psychometric response scale which can be used in questionnaires.
This measurement instrument can be used for subjective characteristics or attitudes that are
impossible to measure directly. Pain assessed in VAS scale is a unidimensional measure of
pain intensity. Respondents express their level of agreement to a statement by pointing a
position along a continuous line between two end-points on a 100-mm long horizontal line.
Usually it takes less than 1 minute to complete the measure [35,36]. Scoring on VAS is
determined by measuring with ruler the distance (mm) on the 10-cm line between the “no

6
pain” anchor and the patient’s mark, providing a range of scores from 0–100. According to
the research, the visual analogue scales have superior metrical characteristics than discrete
scales, therefore a wider range of statistical methods can be applied to the measured
parameters [37,38]. The characteristic of the instrument is based on calculated intraclass
correlation coefficients (ICC) on 0.97 for acute pain and Cronbach’s alpha varies depending
on the studies from 0.79 to 0.91 [39,40].
The pain was assessed as a total feeling, during the wrist extension, during palpation the area
of the lateral epicondyle, during the hand grip, during stretch of extensor carpi radialis brevis
(ECRB) muscle and during movements of elbow.
Therapy process
All procedures where performed by one certified physical therapy practitioner with used of
original devices dedicated to the method. The application were performed during 10 days.
Examples of the pain localization, physical examination and physical therapy are presented on
the figures (Fig. 1-9 ).
Data collection and analysis
Patients underwent the examination and fulfilled the questionnaires at the beginning of the
therapy and after completing it. The data collected were taken into the statistical analysis and
present in the results. All data were expressed by mean ±standard deviation. The normality of
the data distribution was estimated with use of Shapiro-Wilk test. The Wilcoxon rank-sum
test was used for comparison of the two related groups of the data. The alfa significance level
was set at 0.05. P value of less than 0.05 will be considered to indicate statistical significance.
Statistical analyses was performed with use of Statistica 10.0 software (StatSoft).
Results
The study group consist of 28 patients (19 men and 9 women). The mean age of the patients
was 42,8 ± 7,6 years. None of the patient were tennis player or professional athlete. The
occupation of the patients was mostly in office or physical work in agriculture. Most difficult
and painful activity were associated with the hand grip and the palpation of the lateral
epicondyle. In all patients the elbow of the dominating hand was affected. All patients were
underwent the set of conventional physical therapy and still have symptoms seriously
impairing their daily
7
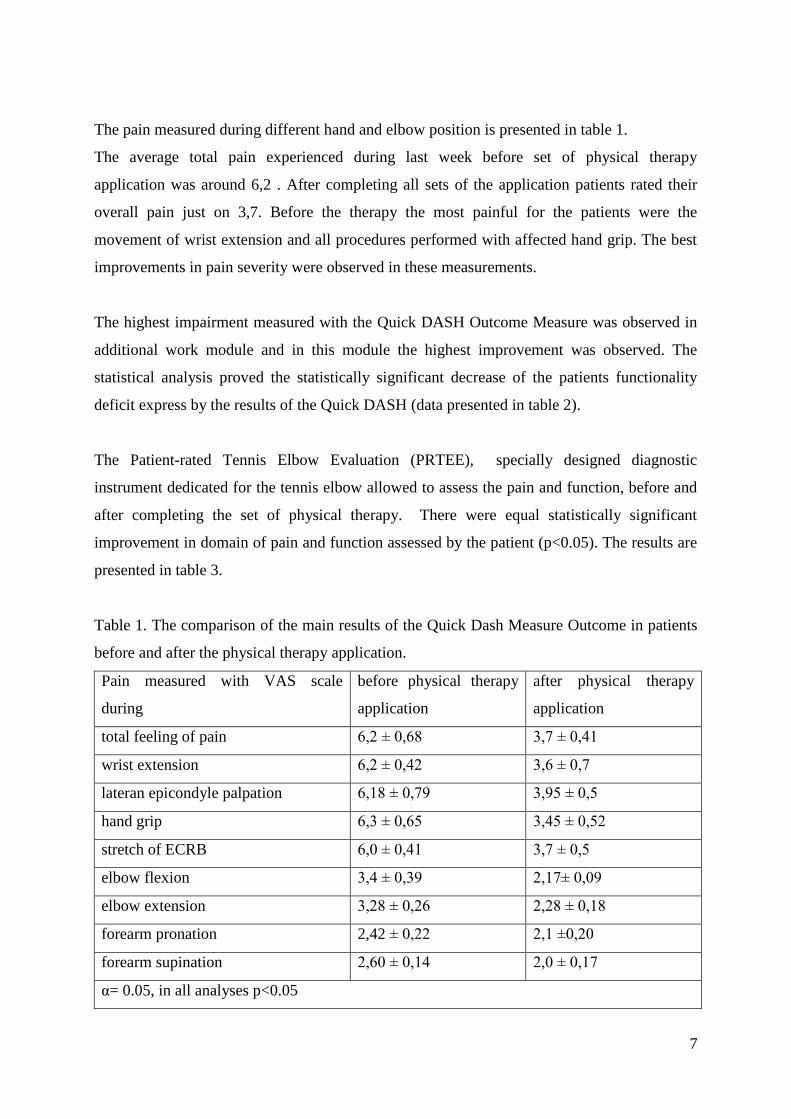
The pain measured during different hand and elbow position is presented in table 1.
The average total pain experienced during last week before set of physical therapy
application was around 6,2 . After completing all sets of the application patients rated their
overall pain just on 3,7. Before the therapy the most painful for the patients were the
movement of wrist extension and all procedures performed with affected hand grip. The best
improvements in pain severity were observed in these measurements.
The highest impairment measured with the Quick DASH Outcome Measure was observed in
additional work module and in this module the highest improvement was observed. The
statistical analysis proved the statistically significant decrease of the patients functionality
deficit express by the results of the Quick DASH (data presented in table 2).
The Patient-rated Tennis Elbow Evaluation (PRTEE), specially designed diagnostic
instrument dedicated for the tennis elbow allowed to assess the pain and function, before and
after completing the set of physical therapy. There were equal statistically significant
improvement in domain of pain and function assessed by the patient (p<0.05). The results are
presented in table 3.
Table 1. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after the physical therapy application.
Pain measured with VAS scale
during
before physical therapy
application
after physical therapy
application
total feeling of pain 6,2 ± 0,68 3,7 ± 0,41
wrist extension 6,2 ± 0,42 3,6 ± 0,7
lateran epicondyle palpation 6,18 ± 0,79 3,95 ± 0,5
hand grip 6,3 ± 0,65 3,45 ± 0,52
stretch of ECRB 6,0 ± 0,41 3,7 ± 0,5
elbow flexion 3,4 ± 0,39 2,17± 0,09
elbow extension 3,28 ± 0,26 2,28 ± 0,18
forearm pronation 2,42 ± 0,22 2,1 ±0,20
forearm supination 2,60 ± 0,14 2,0 ± 0,17
α= 0.05, in all analyses p<0.05

8
Table 2. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after physical therapy application.
Main module-
Restriction Index
Additional module-
work
Additional module-
sport
Before
physical therapy
application
0,70 ± 0,12 0,80 ± 0,14 0,76 ± 0,18
After
physical therapy
application
0,34 ± 0,08 0,32 ± 0,04 0,52 ± 0,20
The mean
improvement
0,36 0,52 0,24
α= 0.05, in all analyses p<0.05
Table 3. The comparison of the pain, function and total results of the Patient-rated Tennis
Elbow Evaluation (PRTEE) fulfilled by patients before and after physical therapy
application.
Pain PRTEE
Function
PRTEE Total PRTEE
Before
physical therapy
application
0,76 ± 0,12 0,72 ± 0,16 0,74 ± 0,14
After
physical therapy
application
0,30 ± 0,2 0,26 ± 0,08 0,28 ± 0,05
The mean
improvement
0,46 0,46 0,46
α= 0.05, in all analyses p<0.05

9
Discussion
The study showed that application of the physical therapy can significantly reduce the pain
occurring during the wrist extension and hand grip. There are several studies presenting
different physical therapy methods and its role. Dingemanse and Randsdorp in their
literature review found the potential effectiveness of ultrasound and laser light but pointed
the need of high-quality RCTs examining different intensities and on long-term follow-up
results [41 ]. According to the Oken and Kahraman a brace has a shorter beneficial effect
than ultrasound and laser therapy in reducing pain, and that laser therapy is more effective
than the brace and ultrasound treatment in improving grip strength [42].Barr and Cerrisola
showed that corticosteroid injections are effective at short-term follow-up, and
physiotherapeutic interventions are effective at intermediate- and long-term follow-up [43]. In
studies comparing the steroid injections and physical therapy was observed that physical
therapy does not have significant effect on symptoms in patients receiving steroids injections
[44].
The research limitation
The limitation of the study is small group of the patients included who underwent whole
process of the examination and full set of physical therapy methods application, therefore the
study can be underpowered. Another limitation is the lack of the control group included into
the process of randomization. To exactly determine the effect of combination of ultrasound,
laser light and hydro massage application in patients with symptoms of tennis elbow there is a
need of randomized controlled trial what was pointed also in other studies.
Conclusions
Combination of the laser light, ultrasound and hydro massage applied for the elbow seems to
be effective as supportive therapy of patients with lateral epicondylitis. It leads to decrease of
the severity of the pain, improve patients functionality assessed with standardized
questionnaires .

10
Fig. 1. The lateral view of the left elbow model. The lateral epicondyle matched with three red
places for muscle attachement.
Fig. 2. Painful area matched with the cross.

11
Fig. 3. Painful area of the lateral epicondyle during palpation.
Fig. 4. Examination of the elbow movements – forearm pronation.

12
Fig. 5. Examination of the elbow movements – forearm supination.
Fig.6. Application of the laser light for the lateral epicondyle.

13
Fig. 7. Application of the ultrasound for the lateral epicondyle.
Fig. 8. Application of the hydro massage for the upper limb.

14
Fig. 9. Application of the magnetic field for the lateral epicondyle.

15
Summary
Background:
Lateral epicondylitis is a condition characterized by the pain in a region of the lateral
epicondylus of humerus, weakness of the forearm muscles, grips forces and general
dysfunctions of upper extremity. The standard management of the lateral epicondylitis
consists of physical therapy methods, pharmacological treatment, immobilization and surgical
techniques.
Aim of the study :
The aim of the study was to estimate the symptoms reduction and the improvement of the
functionality of upper limb after ultrasound, laser light and hydro massage application in
patients with "tennis elbow" symptoms.
Material and methods:
The study group consisted of 28 patients with tennis elbow treated with the physical therapy
methods. All procedures were performed by certified physical therapy specialist with certified
devices. The VAS, PRTEE scales and Quick DASH questionnaires were used to assess the
effectiveness of this management. The range of motion, the pain free grip strength and the
maximal strength of the grip was tested at the beginning and the end of the therapy. The data
collected were analyzed with use of Statistica 10.0 software. The significance level of 0.05 (α
= 5%) was adopted.
Results:
The significant reduction of pain in the lateral epicondylus region measured in VAS scale and
values of the PRTEE and Quick DASH questionnaire were observed in the study group. The
pain during the hand grip and the wrist, elbow movements were significantly improvement in
group of patients treated with combination of laser light, ultrasound and
hydromassage(p<0.05).
Conclusions:
Combination of the laser light, ultrasound and hydro massage can be an effective method in
decreasing symptoms of "tennis elbow", mostly the pain and hand grip.

16
References
1. Norris C. Sports injuriesddiagnosis and management. 3rd ed. Butterworth Heinemann;
2005. p. 412e7.
2. Greenbaum B, Hammura J. Extensor carpi radialis brevis: an anatomical analysis of its
origin. J Bone Joint Surg Br 1999;81:926e9.
3. Hong Q, Durand M, Loisel P. Treatment of lateral epicondylitis: where is the evidence?
Joint Bone Spine 2004;71: 369e73.
4. Waseem M, Nuhmani S, Ram CS, Sachin Y. Lateral epicondylitis: a review of the
literature.
J Back Musculoskelet Rehabil. 2012;25(2):131-42.
5. Boyer MI, Hastings H. Lateral tennis elbow: “Is there any science out there?”. J Shoulder
Elbow Surg 1999;8:481e91.
6. Nirschl R.P., Ashman E.S., Elbow tendinopathy: Tennis elbow. Clin Sports Med. 2003;
22(4):813–836.
7. Stasinopoulos D, Johnson MI, ‘Lateral elbow tendinopathy’ is the most appropriate
diagnostic term for the condition commonly referred-to as lateral epicondylitis. Med
Hypotheses. 2006; 67(6):1400–1402.
8 . Van Hofwegen C, Baker CL 3rd, Baker CL Jr. Epicondylitis in the athlete's elbow. Sports
Med. 2010 Oct;29(4):577-97.
9. Faro F, Wolf JM. Lateral epicondylitis: review and current concepts. J Hand Surg Am.
2007 Oct;32(8):1271-9.
10. Haker EHK, Lundeberg TCM. Lateral epicondylalgia report of noneffective midlaser
treatment. Arch Phys Med Rehabil 1991; 72:984e8.
11. Lundeberg T, Abrahamsson P, Haker E. A comparative study of continuous ultrasound,
placebo ultrasound and rest in epicondylalgia. Scand J Rehabil Med 1988;20:99e101.
12. Bisset L, Paungmali A, Vicenzino BA. Systematic review and meta-analysis of clinical
trials on physical interventions for lateral epicondylalgia. Br J Sports Med 2005;39:411e22
13. Halle J, Franklin R, Karalfa B. Comparison of four treatment approaches for lateral
epicondylitis of the elbow. J Orthop Sports Phys Ther 1986;8:62e9.
14. Simunovic Z, Trobonjaca T, Trobonjaca Z. Treatment of medial and lateral
epicondylitisdtennis and golfer’s elbowdwith low level laser therapy. Laser Med Surg
1998;16:145e51.
15 Rompe JD, Hopf C, Kullmer K, Heine J, Burger R. Analgesic effect of extracorporeal
shock wave therapy on chronic tennis elbow. J Bone Joint Surg 1996;78:233e7.

17
16. Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, et al. Non-steroidal anti-
inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database
Syst Rev 2001;(4). CD003686.
17. Assendelft W, Green S, Buchbinder R, Struijs P, Smidt N. Extracts from concise clinical
evidence: tennis elbow. BMJ; 2003:327e9.
18. Assendelft WJJ, Hay EM, Adshead R, Bouter LM. Corticosteroid injections for lateral
epicondylitis: a systematic overview. Br J Gen Pract 1996;46:209e16.
19. Price R, Sinclair H, Heinrich I, Gibson T. Local injection treatment of tennis elbow:
hydrocortisone, tiamcinolone and lignocaine compared. Br J Rheumatol 1991;30:39e44.
20. Espandar R, Heidari P, Rasouli MR, Saadat S, Farzan M, et al. Use of anatomic
measurement to guide injection of botulinum toxin for the management of chronic lateral
epicondylitis: a randomized controlled trial. CMAJ. 2010 May 18;182(8):768-73.
21. Placzek R, Drescher W, Deuretzbacher G, Hempfing A, Meiss AL. Treatment of chronic
radial epicondylitis with botulinum toxin A. A double-blind, placebo-controlled, randomized
multicenter study. J Bone Joint Surg Am. 2007 Feb;89(2):255-60.
22. Thanasas C, Papadimitriou G, Charalambidis C, Paraskevopoulos I, Papanikolaou A.
Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow
epicondylitis: a randomized controlled clinical trial. Am J Sports Med. 2011 Oct;39(10):2130-
4.
23. Mishra AK, Skrepnik AV, Edwards SG, Jones GL, Sampson S et all. Platelet-Rich
Plasma Significantly Improves Clinical Outcomes in Patients With Chronic Tennis Elbow: A
Double-Blind, Prospective, Multicenter, Controlled Trial of 230 Patients. Am J Sports Med
July 3, 2013.
24. Hudak P, Amadio PC, Bombardier C, and the Upper Extremity Collaborative Group.
Development of an Upper Extremity Outcome Measure: The DASH (Disabilities of the Arm,
Shoulder, and Hand). American Journal of Industrial Medicine 1996; 29:602-608.
25. http://www.dash.iwh.on.ca/ access 26.07.2013r.
26. Beaton DE, Davis AM, Hudak P, McConnell S. The DASH (Disabilities of the Arm,
Shoulder and Hand) outcome measure: What do we know about it now? British Journal of
Hand Therapy 2001a; 6(4):109-118.
27. Kennedy CA, Beaton DE, Solway S, McConnell S, Bombardier C. Disabilities of the
Arm, Shoulder and Hand (DASH). The DASH and QuickDASH Outcome Measure User’s
Manual, Third Edition. Toronto, Ontario: Institute for Work & Health, 2011.
18
28. Beaton DE, Wright JG, Katz JN, and the Upper Extremity Collaborative Group.
Development of the QuickDASH: Comparison of three item-reduction approaches. Journal of
Bone and Joint Surgery 2005a; 87A(5):1038-1046.
29. MacDermid, J. Update: The Patient-rated Forearm Evaluation Questionnaire is now the
Patient-rated Tennis Elbow Evaluation. J Hand Ther, 2005. 18(4): p. 407-10.
30. MacDermid, J. The Patient-Rated Tennis Elbow Evaluation (PRTEE) User Manual. 2007,
School of Rehabilitation Science, McMaster University: Hamilton, Canada.
31. Rompe, J.D., T.J. Overend, and J.C. MacDermid, Validation of the Patient-rated Tennis
Elbow Evaluation Questionnaire. J Hand Ther, 2007. 20(1): p. 3-10; quiz 11.
32. D'Vaz, A.P., A.J. Ostor, C.A. Speed, et al. Pulsed low-intensity ultrasound therapy for
chronic lateral epicondylitis: a randomized controlled trial. Rheumatology (Oxford), 2006.
45(5): p. 566-70.
33.Chung, B. and J.P. Wiley. Validity, responsiveness and reliability of the Patient-Rated
Tennis Elbow Evaluation. Hand Therap, 2010. 15(3): p. 62-68.
34. Nilsson P, Baigi P, Marklund P, Månsson J. Cross-cultural adaptation and determination
of the reliability and validity of PRTEE-S (Patientskattad Utvärdering av Tennisarmbåge), a
questionnaire for patients with lateral epicondylalgia, in a Swedish population. BMC
Musculoskelet Disord. 2008; 9: 79.
35. Reips UD, Funke F. "Interval level measurement with visual analogue scales in Internet-
based research: VAS Generator." doi:10.3758/BRM.40.3.699
36. Grant S, Aitchison T, Henderson E, Christie J, Zare S, et al. A comparison of the
reproducibility and the sensitivity to change of visual analogue scales, Borg scales, and Likert
scales in normal subjects during submaximal exercise. Chest. 116(5):1208-17.
37. McCaffery M, Pasero C. Pain: Clinical Manual, St. Louis, 1999, P. 16.
38. Bijur PE, Silver W, Gallagher J. Reliability of the Visual Analog Scale for Measurement
of Acute Pain. Academic Emergency Medicine Volume 8, Issue 12, pages 1153–1157,
December 2001.
39. McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a
critical review. Psychol Med 1988;18:1007–19.
40. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison
of six methods. Pain 1986;27:117–26.
41. Dingemanse R, Randsdorp M, Koes BW, Huisstede BM. Evidence for the effectiveness of
electrophysical modalities for treatment of medial and lateral epicondylitis: a systematic
review. Br J Sports Med. 2013 Jan 18.
19
42. Oken O, Kahraman Y, Ayhan F, Canpolat S, Yorgancioglu ZR, Oken OF. The short-term
efficacy of laser, brace, and ultrasound treatment in lateral epicondylitis: a prospective,
randomized, controlled trial. J Hand Ther. 2008 Jan-Mar;21(1):63-7; quiz 68.
43. Barr S, Cerisola FL, Blanchard V. Effectiveness of corticosteroid injections compared
with physiotherapeutic interventions for lateral epicondylitis: a systematic review.
Physiotherapy. 2009 Dec;95(4):251-65. doi: 10.1016/j.physio.2009.05.002. Epub 2009 Jul 24.
44. Coombes BK, Bisset L, Brooks P, Khan A, Vicenzino B. Effect of corticosteroid
injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral
epicondylalgia: a randomized controlled trial. JAMA. 2013 Feb 6;309(5):461-9. doi:
10.1001/jama.2013.129.

20
Karolina Janikowska, Joanna Fidut
The role of Mulligan Therapy Concept in treatment of "tennis elbow" symptoms
Background
Tennis elbow is a common name for lateral epicondylitis (LE). This condition is based on
tendinitis of the extensor carpi radialis brevis muscle [1,2]. Depending on the study it can
affect from 1 to 3 % of the population [3]. The incidence of the lateral epicondylitis is equally
distributed among both genders, but mostly affects the dominant upper limb [1,4 ].
The repetitive strain injury is described as the most common cause of the lateral epicondylitis
[5]. In historical approach the tennis elbow was included in the type of tendinitis and
suggested the presence of the acute inflammatory process. According to the research
investigating the absence of inflammatory marker in patients with tennis elbow the term
“tendinosis” or “tendinopathy” is more appropriate to reflect the chronicity of the condition
[6,7]. Pain localized in the area of the lateral epicondyle of the elbow is most common
symptom of the tennis elbow and aggravates with hand grips and resistance applied to the
muscles of the forearm responsible for wrist extension. [8]. The conservative physical therapy
is based on use of ultrasound, cryotherapy, heat, electrical and laser stimulation or
extracorporeal shock wave therapy [9-15]. The conventional therapy include the
pharmacological preparates e.g. non- steroidal anti-inflammatory drugs (NSAID),
corticosteroids prepared for the injections in the area of the lateral epicondyle [16-19].
Modern therapies focus on the botulinum toxin type A injections in improving the healing of
the tendons attached to the lateral epicondyle [20,21]. Another type of injections performed in
this area is use of the platelet-rich plasma extracted from the patient’s own blood and the
effect of the autologos growth factors [22,23]. The physical therapy is still more accessible for
the patient and less invasive than even very promising biological treatment but require new
approach focusing on the core of the patients problem. One of the new ideas in manual
therapy is mobilization with movement according the Brian Mulligan Concept. The
techniques include a sustained lateral glide to the elbow joint with concurrent physiological
21
movement and allows to correct the faulty position of the elbow joint that can causa the
tennis elbow symptoms [24,25].
Aim of the study
The aim of the was to assess the influence of the manual therapy based on mobilization with
movement according to the Brain Mulligan Concept on pain and the functional status of the
patients with lateral epicondylalgia.
Material and methods
The study was conducted on group of patients (14 men and 5 women) diagnosed with lateral
epicondylalgia who suffered for at least three months and failed to the conventional therapy.
The exclusion criteria for the study was: previous injury of the elbow in anamnesis, structural
changes in the area of the elbow, osteoarthritis of the elbow, receiving any therapy for lateral
epicondylitis during last 4 weeks, cervical spine changes and symptoms of radiculopathy,
osteoporosis, inflammation in the elbow area.
During the study the patients underwent physical examination of the upper limbs.
The standardized questionnaries e.g. Quick DASH (Disability of the Arm, Shoulder and
Hand) and PRTEE (Patients’ Related Tennis Elbow Examination) were used to assess the
functionality in this condition. To determinate the severity of the pain the visual-analog scale
(VAS) was applied.
DASH and Quick DASH
The Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure is 30-item, self-
report questionnaire developed to measure physical function and symptoms in patients with
musculoskeletal dysfunctions of the upper limb. It was released in 1996 [26]. This tool was
designed by the Institute for Work & Health and the American Academy of Orthopaedic
Surgeons (AAOS) and supported by the American Association for Hand Surgery, the
American Orthopaedic Society for Sports Medicine, the American Shoulder & Elbow
Surgeons, the American Society for Surgery of the Hand, the Arthroscopy Association of
North America and the American Society of Plastic and Reconstructive Surgeons [27]. The
QuickDASH is a shortened version of the DASH Outcome Measure. Instead of 30 items, the
QuickDASH based on 11 items to measure functionality and symptoms of patients with any
musculoskeletal disorders of the upper limb.Scoring is divided into the two components: the
disability/symptom section, consisting of 11 items, scored 1-5 and the optional high

22
performance sport/music or work modules with 4 items, scored 1-5. To calculate the score at
least 10 of the 11 items must be completed. Bacause this tool was developed to measure the
disability, the scaling was ranked from 0 indicating least disability to 100 indicating most
disability. The researcher should be aware of the direction of the scales [27]. This tool
included also two optional modules intended to assess symptoms and function in athletes,
performing artists and high degree physical performance workers. Both instruments are valid,
reliable and responsive and can be used for clinical and research purpose [28,29]. The tools
are characterized by rating of intra-class correlation coefficient on 0.94 and Cronbach’s alpha
also on. 0.94 [30].
The Patient-rated Tennis Elbow Evaluation (PRTEE)
This instrument enables quantitative rating by the patient of pain and functional impairment
associated with lateral epicondylitis, commonly called “tennis elbow”. PRTEE is an
instrument that has been developed specifically for use with this disorder, and is increasingly
being included in research, especially randomized controlled trials. The questionnaire consist
of a 15-item, with five addressing pain and ten concerned with functional impairment. Each of
the item are rated with use of 0 – 10 numerical scale to assess the average pain or difficulty
they have faced over the previous week during various activities that usually cause pain in
tennis elbow. In this system the pain and function are weighted equally in the total score
[31,32]. Higher scores present greater severity and the maximum score is 100. Major
advantages of this instrument are its simplicity, shortness and specificity to lateral
epicondylitis [33,34]. The characteristic of the test is based on recent study used a four-week
test-retest period and calculated Intraclass Correlation Coefficient values of 0.81 for the pain
sub-score and 0.76 for the total score. In another studies the Cronbach's alpha coefficients
were high for both the pain and function sub-scales (0.84 and 0.93, respectively) [35,36].
Pain assessment - Visual-analog scale (VAS)
Visual-analog scale is a psychometric response scale which can be used in questionnaires.
This measurement instrument can be used for subjective characteristics or attitudes that are
impossible to measure directly. Pain assessed in VAS scale is a unidimensional measure of
pain intensity. Respondents express their level of agreement to a statement by pointing a
position along a continuous line between two end-points on a 100-mm long horizontal line.
Usually it takes less than 1 minute to complete the measure [37,38]. Scoring on VAS is

23
determined by measuring with ruler the distance (mm) on the 10-cm line between the “no
pain” anchor and the patient’s mark, providing a range of scores from 0–100.
According to the research, the visual analogue scales have superior metrical characteristics
than discrete scales, therefore a wider range of statistical methods can be applied to the
measured parameters [39,40]. The characteristic of the instrument is based on calculated
intraclass correlation coefficients (ICC) on 0.97 for acute pain and Cronbach’s alpha varies
depending on the studies from 0.79 to 0.91 [41,42].
The pain was assessed as a total feeling, during the wrist extension, during palpation the area
of the lateral epicondyle, during the hand grip, during stretch of extensor carpi radialis brevis
(ECRB) muscle and during movements of elbow.
Therapy process
All procedures where performed by one certified in Mulligan Therapy practitioner with used
of original belt for mobilization. The whole therapy was divided into 6 sets with 2-3 days of
break between sets. All patients were instructed to practice some exercises related to the
therapy at home. The process of the diagnosis and the therapy is presented on pictures (Fig. 1-
4).
Data collection and analysis
Patients underwent the examination and fulfilled the questionarries at the beginning of the
therapy and after completing it. The data collected were taken into the statistical analysis and
present in the results. All data were expressed by mean ±standard deviation. The normality of
the data distribution was estimated with use of Shapiro-Wilk test. The Wilcoxon rank-sum
test was used for comparison of the two related groups of the data. The alfa significance level
was set at 0.05. P value of less than 0.05 will be considered to indicate statistical significance.
Statistical analyses was performed with use of Statistica 10.0 software (StatSoft).
Results
The study group consist of 19 patients, 14 men and 5 women. The mean age of the patients
was 35,57 ± 5,7 years. None of the patient were tennis player or professional athlete. The
occupation of the patients was mostly in office or physical work in agriculture. Most difficult
and painful activity were associated with the hand grip. In all patients the elbow of the
dominating hand was affected. All patients were underwent the set of conventional physical
therapy and still have symptoms seriously impairing their daily
24
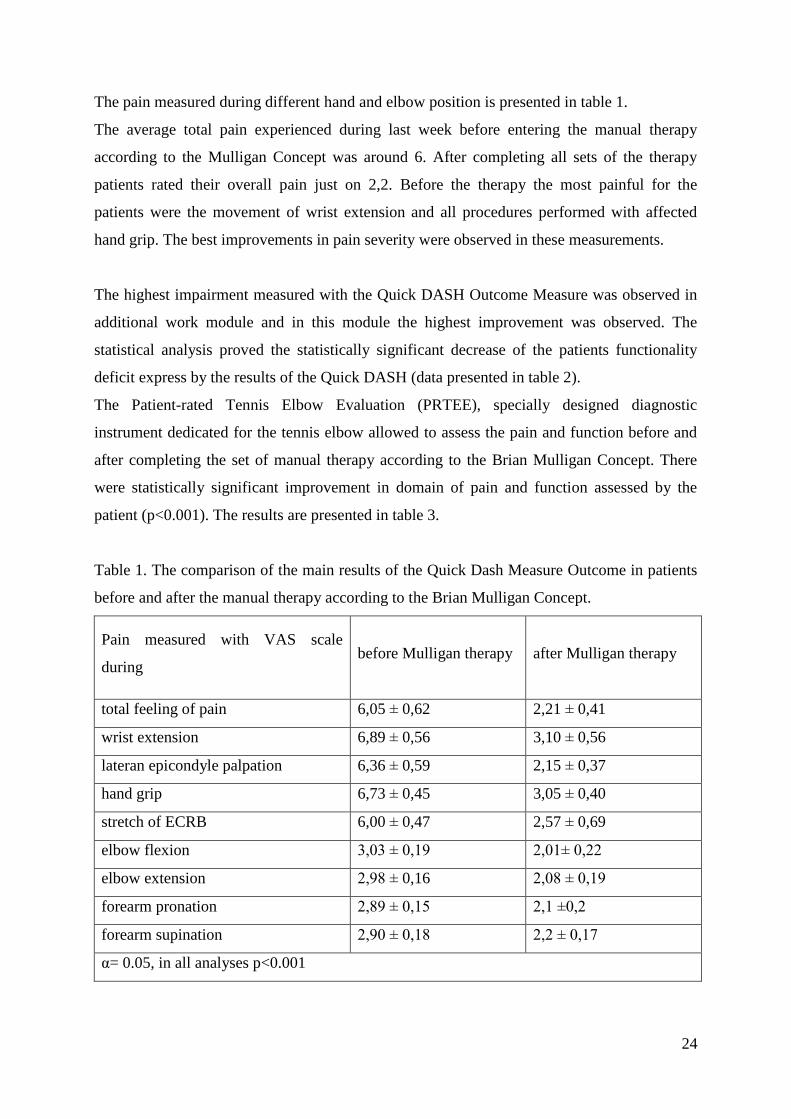
The pain measured during different hand and elbow position is presented in table 1.
The average total pain experienced during last week before entering the manual therapy
according to the Mulligan Concept was around 6. After completing all sets of the therapy
patients rated their overall pain just on 2,2. Before the therapy the most painful for the
patients were the movement of wrist extension and all procedures performed with affected
hand grip. The best improvements in pain severity were observed in these measurements.
The highest impairment measured with the Quick DASH Outcome Measure was observed in
additional work module and in this module the highest improvement was observed. The
statistical analysis proved the statistically significant decrease of the patients functionality
deficit express by the results of the Quick DASH (data presented in table 2).
The Patient-rated Tennis Elbow Evaluation (PRTEE), specially designed diagnostic
instrument dedicated for the tennis elbow allowed to assess the pain and function before and
after completing the set of manual therapy according to the Brian Mulligan Concept. There
were statistically significant improvement in domain of pain and function assessed by the
patient (p<0.001). The results are presented in table 3.
Table 1. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after the manual therapy according to the Brian Mulligan Concept.
Pain measured with VAS scale
during before Mulligan therapy
after Mulligan therapy
total feeling of pain 6,05 ± 0,62 2,21 ± 0,41
wrist extension 6,89 ± 0,56 3,10 ± 0,56
lateran epicondyle palpation 6,36 ± 0,59 2,15 ± 0,37
hand grip 6,73 ± 0,45 3,05 ± 0,40
stretch of ECRB 6,00 ± 0,47 2,57 ± 0,69
elbow flexion 3,03 ± 0,19 2,01± 0,22
elbow extension 2,98 ± 0,16 2,08 ± 0,19
forearm pronation 2,89 ± 0,15 2,1 ±0,2
forearm supination 2,90 ± 0,18 2,2 ± 0,17
α= 0.05, in all analyses p<0.001

25
Table 2. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after the manual therapy according to the Brian Mulligan Concept.
Main module-
Restriction Index
Additional module-
work
Additional module-
sport
Before
Mulligan Therapy
0,72 ± 0,11 0,81 ± 0,13 0,81 ± 0,14
After
Mulligan Therapy
0,1 ± 0,02 0,12 ± 0,03 0,60 ± 0,12
The mean
improvement
0,61 0,69 0,21
α= 0.05, in all analyses p<0.001
Table 3. The comparison of the pain, function and total results of the Patient-rated Tennis
Elbow Evaluation (PRTEE) fulfilled by patients before and after the manual therapy
according to the Brian Mulligan Concept.
Pain PRTEE
Function
PRTEE Total PRTEE
Before
Mulligan Therapy
0,8 ± 0,12 0,76 ± 0,16 0,78 ± 0,14
After
Mulligan Therapy
0,16 ± 0,08 0,14 ± 0,02 0,15 ± 0,05
The mean
improvement
0,64 0,62 0,63
α= 0.05, in all analyses p<0.001
Discussion
In our study we observed the male domination. Similarly to the other observation the elbow of
the dominated hand was affected [1,4]. We observed the statistically significant decrease of
the pain measured in all situations reported in the table 1. and expressed with visual analog
scale. Previous studies indicated the effectiveness of the mobilization with movement
especially in fields of pain reduction and improving the hand grip using the same measure
tools [43]. Geetu and Miller in their papers also prove the role of application these techniques

26
in enhancing the functional performance according to the Mulligan Concept [44, 45,46].
There are nine randomized controlled trials pointing the effectiveness of the mobilization with
movement in pain reduction [47]. According to some research mobilization with movement
for the elbow was capable of inducing physiological effects similar to those reported for some
forms of spinal manipulation [48]. Mulligan Concept of the manual therapy allows to
increase the patients pain free range of motion of the elbow and wrist [49,50,51]. The use of
this techniques seems to be effective even in high performance patients e.g. rock climbers
[52].
The research limitation
The limitation of the study is small group of the patients included who underwent whole
process of the examination and all sets of mobilizations with movement of Brian Mulligan
Manual Therapy Concept, therefore the study can be underpowered. Another limitation is the
lack of the control group included into the process of randomization. To exactly determine the
effect of mobilization with movement in Mulligan Therapy in patients with symptoms of
tennis elbow
Conclusions
The mobilization with movement according to the Brian Mulligan Manual Therapy Concept
seems to be effective as supportive therapy of patients with lateral epicondylitis. It leads to
decrease of the severity of the pain, improve patients functionality assessed with standardized
questionnaires .

27
Fig. 1. Mobilization with movement.
Fig. 2. Mobilization with movement in elbow flexion.

28
Fig. 3. Assessment of the origin of the elbow pain.
Fig. 4. Automobilization with therapeutic belt.

29
Fig. 5. The painful area of the lateral epicondyle matched with cross.

30
Summary
Background:
"Tennis elbow" is a condition characterized by the pain in a region of the lateral epicondylus
of humerus, weakness and dysfunctions of upper extremity. The standard management offers
methods of pharmacological and physical therapy, immobilization or surgical techniques.
Recently manual therapy is more often applied in this condition especially with techniques of
Mulligan Therapy Concept, which is a modern and still not well known method.
Aim of the study:
The aim of the study was to estimate the symptoms reduction after manual therapy applied
according to Mulligan Therapy Concept in patients with lateral epicondylitis.
Material and methods:
The group consisted of 19 patients with tennis elbow symptoms treated with the Mulligan
Therapy Concept. The mobilizations with movement with the use of mobilization belt were
applied on affected elbow during the 6 sessions of therapy. All procedures were performed by
certified Mulligan Therapy Concept practitioner. The VAS, PRTEE scales and Quick DASH
questionnaires were used to asses the effectiveness of this management.
Results:
The significant reduction of pain in the lateral epicondyle region and values of the PRTEE
and Quick DASH Outcome Measure were observed.
Conclusion:
Manual therapy including the mobilization with movement according to the Mulligan Therapy
Concept is a promising method in decreasing symptoms of "tennis elbow", especially the
pain, especially during the hand grip and patients’ functionality.

31
References
1. Norris C. Sports injuriesddiagnosis and management. 3rd ed. Butterworth Heinemann;
2005. p. 412e7.
2. Greenbaum B, Hammura J. Extensor carpi radialis brevis: an anatomical analysis of its
origin. J Bone Joint Surg Br 1999;81:926e9.
3. Hong Q, Durand M, Loisel P. Treatment of lateral epicondylitis: where is the evidence?
Joint Bone Spine 2004;71: 369e73.
4. LaFreniere JG. Tennis elbow: evaluation, treatment, and prevention. Phys Ther
1979;59:742e6.
5. Boyer MI, Hastings H. Lateral tennis elbow: “Is there any science out there?”. J Shoulder
Elbow Surg 1999;8:481e91.
6. Nirschl R.P., Ashman E.S., Elbow tendinopathy: Tennis elbow. Clin Sports Med. 2003;
22(4):813–836.
7. Stasinopoulos D, Johnson MI, ‘Lateral elbow tendinopathy’ is the most appropriate
diagnostic term for the condition commonly referred-to as lateral epicondylitis. Med
Hypotheses. 2006; 67(6):1400–1402.
8 . Van Hofwegen C, Baker CL 3rd, Baker CL Jr. Epicondylitis in the athlete's elbow. Sports
Med. 2010 Oct;29(4):577-97.
9. Kamien M. A rational management of tennis elbow. Sports Med 1990;9:173e91.
10. Haker EHK, Lundeberg TCM. Lateral epicondylalgia report of noneffective midlaser
treatment. Arch Phys Med Rehabil 1991; 72:984e8.
11. Lundeberg T, Abrahamsson P, Haker E. A comparative study of continuous ultrasound,
placebo ultrasound and rest in epicondylalgia. Scand J Rehabil Med 1988;20:99e101.
12. Bisset L, Paungmali A, Vicenzino BA. Systematic review and meta-analysis of clinical
trials on physical interventions for lateral epicondylalgia. Br J Sports Med 2005;39:411e22
13. Halle J, Franklin R, Karalfa B. Comparison of four treatment approaches for lateral
epicondylitis of the elbow. J Orthop Sports Phys Ther 1986;8:62e9.
14. Simunovic Z, Trobonjaca T, Trobonjaca Z. Treatment of medial and lateral
epicondylitisdtennis and golfer’s elbowdwith low level laser therapy. Laser Med Surg
1998;16:145e51.
15 Rompe JD, Hopf C, Kullmer K, Heine J, Burger R. Analgesic effect of extracorporeal
shock wave therapy on chronic tennis elbow. J Bone Joint Surg 1996;78:233e7.
32
16. Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, et al. Non-steroidal anti-
inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database
Syst Rev 2001;(4). CD003686.
17. Assendelft W, Green S, Buchbinder R, Struijs P, Smidt N. Extracts from concise clinical
evidence: tennis elbow. BMJ; 2003:327e9.
18. Assendelft WJJ, Hay EM, Adshead R, Bouter LM. Corticosteroid injections for lateral
epicondylitis: a systematic overview. Br J Gen Pract 1996;46:209e16.
19. Price R, Sinclair H, Heinrich I, Gibson T. Local injection treatment of tennis elbow:
hydrocortisone, tiamcinolone and lignocaine compared. Br J Rheumatol 1991;30:39e44.
20. Espandar R, Heidari P, Rasouli MR, Saadat S, Farzan M, et al. Use of anatomic
measurement to guide injection of botulinum toxin for the management of chronic lateral
epicondylitis: a randomized controlled trial. CMAJ. 2010 May 18;182(8):768-73.
21. Placzek R, Drescher W, Deuretzbacher G, Hempfing A, Meiss AL. Treatment of chronic
radial epicondylitis with botulinum toxin A. A double-blind, placebo-controlled, randomized
multicenter study. J Bone Joint Surg Am. 2007 Feb;89(2):255-60.
22. Thanasas C, Papadimitriou G, Charalambidis C, Paraskevopoulos I, Papanikolaou A.
Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow
epicondylitis: a randomized controlled clinical trial. Am J Sports Med. 2011 Oct;39(10):2130-
4.
23. Mishra AK, Skrepnik AV, Edwards SG, Jones GL, Sampson S et all. Platelet-Rich
Plasma Significantly Improves Clinical Outcomes in Patients With Chronic Tennis Elbow: A
Double-Blind, Prospective, Multicenter, Controlled Trial of 230 Patients. Am J Sports Med
July 3, 2013.
24. Mulligan BR. Mobilisation with movement. J Man Manip Ther 1993;1(4):154e6.
25. Miller J. Mulligan concept e management of tennis elbow. Can Physiother Assoc Ortho
Div Rev; 2000 May/June:45e6.
26. Hudak P, Amadio PC, Bombardier C, and the Upper Extremity Collaborative Group.
Development of an Upper Extremity Outcome Measure: The DASH (Disabilities of the Arm,
Shoulder, and Hand). American Journal of Industrial Medicine 1996; 29:602-608.
27. http://www.dash.iwh.on.ca/ access 26.07.2013r.
28. Beaton DE, Davis AM, Hudak P, McConnell S. The DASH (Disabilities of the Arm,
Shoulder and Hand) outcome measure: What do we know about it now? British Journal of
Hand Therapy 2001a; 6(4):109-118.
33
29. Kennedy CA, Beaton DE, Solway S, McConnell S, Bombardier C. Disabilities of the
Arm, Shoulder and Hand (DASH). The DASH and QuickDASH Outcome Measure User’s
Manual, Third Edition. Toronto, Ontario: Institute for Work & Health, 2011.
30. Beaton DE, Wright JG, Katz JN, and the Upper Extremity Collaborative Group.
Development of the QuickDASH: Comparison of three item-reduction approaches. Journal of
Bone and Joint Surgery 2005a; 87A(5):1038-1046.
31. MacDermid, J. Update: The Patient-rated Forearm Evaluation Questionnaire is now the
Patient-rated Tennis Elbow Evaluation. J Hand Ther, 2005. 18(4): p. 407-10.
32. MacDermid, J. The Patient-Rated Tennis Elbow Evaluation (PRTEE) User Manual. 2007,
School of Rehabilitation Science, McMaster University: Hamilton, Canada.
33 Rompe, J.D., T.J. Overend, and J.C. MacDermid, Validation of the Patient-rated Tennis
Elbow Evaluation Questionnaire. J Hand Ther, 2007. 20(1): p. 3-10; quiz 11.
34 D'Vaz, A.P., A.J. Ostor, C.A. Speed, et al. Pulsed low-intensity ultrasound therapy for
chronic lateral epicondylitis: a randomized controlled trial. Rheumatology (Oxford), 2006.
45(5): p. 566-70.
35.Chung, B. and J.P. Wiley. Validity, responsiveness and reliability of the Patient-Rated
Tennis Elbow Evaluation. Hand Therap, 2010. 15(3): p. 62-68.
36. Nilsson P, Baigi P, Marklund P, Månsson J. Cross-cultural adaptation and determination
of the reliability and validity of PRTEE-S (Patientskattad Utvärdering av Tennisarmbåge), a
questionnaire for patients with lateral epicondylalgia, in a Swedish population. BMC
Musculoskelet Disord. 2008; 9: 79.
37. Reips UD, Funke F. "Interval level measurement with visual analogue scales in Internet-
based research: VAS Generator." doi:10.3758/BRM.40.3.699
38. Grant S, Aitchison T, Henderson E, Christie J, Zare S, et al. A comparison of the
reproducibility and the sensitivity to change of visual analogue scales, Borg scales, and Likert
scales in normal subjects during submaximal exercise. Chest. 116(5):1208-17.
39. McCaffery M, Pasero C. Pain: Clinical Manual, St. Louis, 1999, P. 16.
40. Bijur PE, Silver W, Gallagher J. Reliability of the Visual Analog Scale for Measurement
of Acute Pain. Academic Emergency Medicine Volume 8, Issue 12, pages 1153–1157,
December 2001.
41. McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales:
a critical review. Psychol Med 1988;18:1007–19.
42. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a
comparison of six methods. Pain 1986;27:117–26.

34
43. Amro A, Diener I, Bdair W, Hameda IM, et all. The effects of Mulligan mobilisation with
movement and taping techniques on pain, grip strength, and function in patients with lateral
epicondylitis. Hong Kong Physiotherapy Journal (2010) 28, 19e23.
44. Geetu M, Deepak G. Effectiveness of movement with mobilization compared with
manipulation of wrist in case of lateral epicondylitis. Indian J Physiother Occup Ther 2008;2.
45. Miller J. Mulligan concept e management of tennis elbow. Can Physiother Assoc Ortho
Div Rev; 2000 May/June:45e6.
46. Mulligan BR. Mobilisation with movement. J Man Manip Ther1993;1(4):154e6.
47. Heiser R, O'Brien VH, Schwartz DA. The use of joint mobilization to improve clinical
outcomes in hand therapy: A systematic review of the literature. J Hand Ther. 2013 Sep 14.
48 Heiser R, O'Brien VH, Schwartz DA. The use of joint mobilization to improve clinical
outcomes in hand therapy: A systematic review of the literature. J Hand Ther. 2013 Sep 14
49. Abbott JH. Mobilization with movement applied to the elbow affects shoulder range of
movement in subjects with lateral epicondylalgia. Man Ther. 2001 Aug;6(3):170-7.
50. Herd CR, Meserve BB. A systematic review of the effectiveness of manipulative therapy
in treating lateral epicondylalgia. J Man Manip Ther. 2008;16(4):225-37.
51. Slater H, Arendt-Nielsen L, Wright A, Graven-Nielsen T. Effects of a manual therapy
technique in experimental lateral epicondylalgia. Man Ther. 2006 May;11(2):107-17.
52. González-Iglesias J, Cleland JA, del Rosario Gutierrez-Vega M, Fernández-de-las-Peñas
C. Multimodal management of lateral epicondylalgia in rock climbers: a prospective case
series. J Manipulative Physiol Ther. 2011 Nov;34(9):635-42.

35
Joanna Fidut, Karolina Janikowska
The review of the mobilization with movement techniques in management of tennis elbow
Brain Mulligan Mobilization with Movement Concept
The Mulligan Concept is an integrative part of practice of many current manual therapist.
Author of this method Brain Mulligan built his techniques on the principles of manual therapy
proposed by Kaltenborn and focused on restoration the physiological movement of the joints.
It consists of the Sustained Natural Apophyseal Glides (SNAG's) applied for the spine and
MWMs for the extremities.
The principles of the Mulligan Concept are based on the painless motion and therapy. The
therapist should first identify the signs described by Maitland and including for example loss
of joint movement, pain occurring during movement, pain related to the resisted wrist
extension. Therapy include accessory glide performed parallel or perpendicular to the joint
plane. The therapist need to find the correct plane and grade of mobilization to not recreated
the patient’s pain. The success of the therapy is confirmed by significant comparable sign
indicating no pain. Another element of the concept is the passive overpressure applied at the
end of the range, again causing no pain for the patient. The self-treatment is possible with use
of these mobilization with movement techniques.
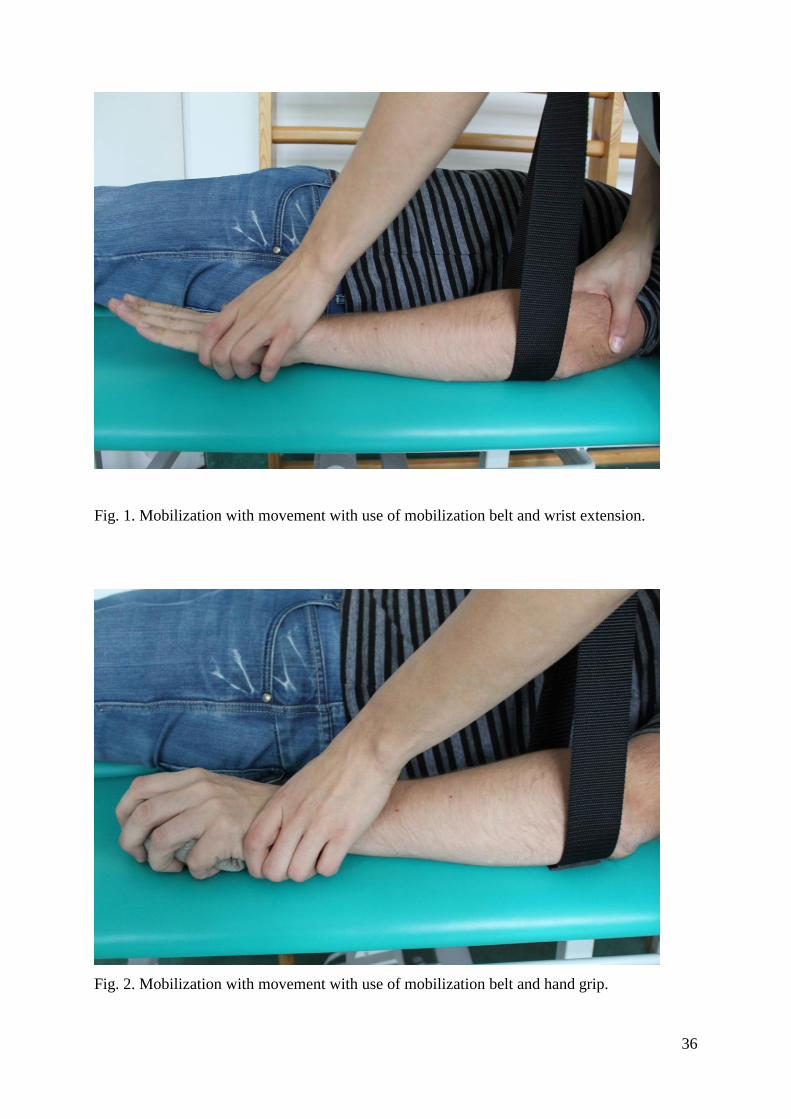
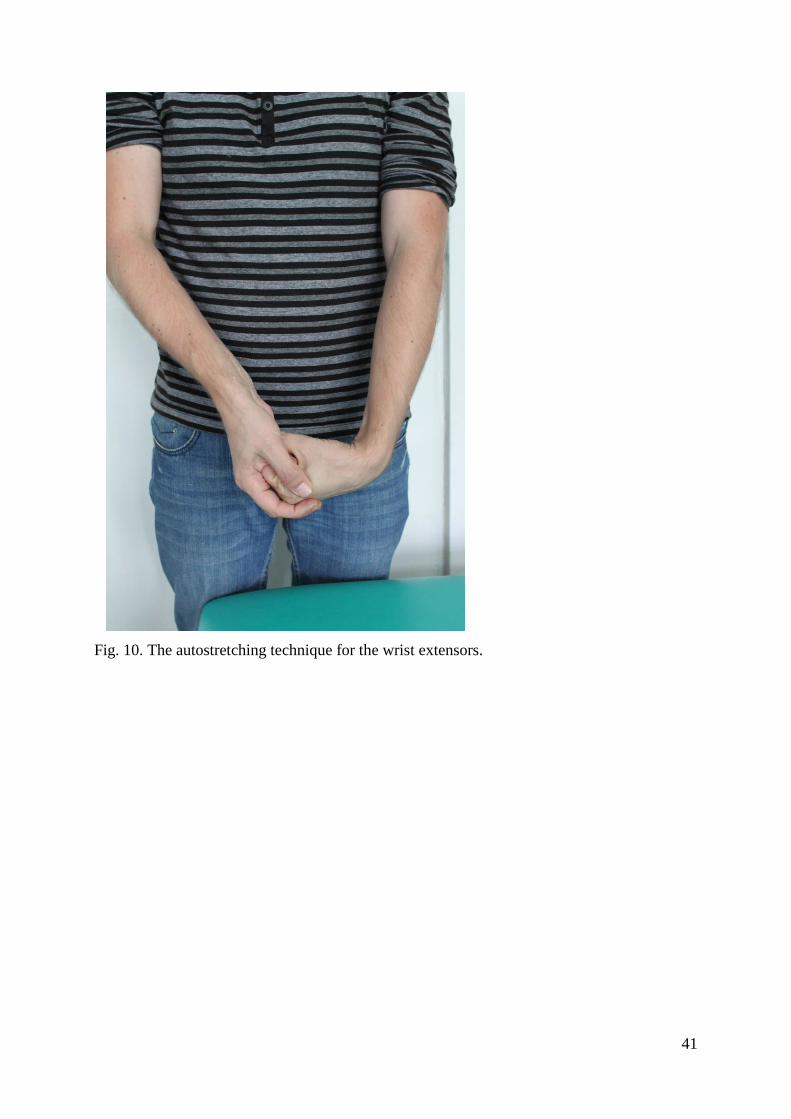
The aim of this paper is to review and present most common techniques of Brian Mulligan
Concept used in lateral epicondylitis therapy (Fig. 1-10).
36
Fig. 1. Mobilization with movement with use of mobilization belt and wrist extension.
Fig. 2. Mobilization with movement with use of mobilization belt and hand grip.

37
Fig. 3. Mobilization with movement with use of mobilization belt and hand grip in elbow
flexion and forearm supination.
Fig. 4. Mobilization with movement in wrist extension with force applied to the hand.

38
Fig. 5. Automobilization of the elbow with use of the wall in wrist extension and hand grip.
Fig. 6. Mobilization with movement and patients motion of flexed wrist.

39
Fig. 7. Mobilization with movement and patients motion to wrist extension.
Fig. 8. Mobilization with movement with passive overpressure.

40
Fig. 9. Mobilization with movement with passive overpressure applied to the elbow.
41
Fig. 10. The autostretching technique for the wrist extensors.

42
References:
1. Mulligan, BR. Manual Therapy ‘NAGS’, ‘SNAGS’, ‘MWMS’ etc. (6th Ed), Orthopedic
Physical Therapy Products, 2010.
2. Mulligan, BR. Self Treatments for Back, Neck, and Limbs, A new approach (2nd Edition).
Orthopedic Physical Therapy Products, 2006.
3. Vicenzino B, Hing W, Rivett D, Hall T. Mobilisation with Movement: The art and the
science by Bill Vicenzino, Wayne Hing, Darren Rivett and Toby Hall, and forewords written
by Brian Mulligan and Professor Gwedolen Jull. Churchill Livingstone, Australia, 2011.
4. Mulligan BR. Manual Therapy, "NAGS", "SNAGS", "MWMS: etc. Plane View Press
Wellington. 1995.
5. Mulligan BR. Mobilizations with Movement (MWMS), Journal of Manual and
Manipulative Therapy, Vol. 1, No. 4, 1993.
6 Vincenzino, B., Wright, A. Effects of a Novel Manipulative Physiotherapy Technique on
Tennis Elbow, A single Case Study, Manual Therapy, 1,1995.
7. Wilson E. The Mulligan Concept: NAGS, SNAGS, and mobilisations with movement.
Journal of Bodywork and Movement Therapies 5(2): 81–89.

43
Karolina Janikowska, Joanna Fidut
Effects of Kinesio taping in patients with symptoms of lateral epicondylalgia
Background
Lateral epicondylitis is one of the most common cause of elbow pain related to the pathology
of the muscle extensor carpi radialis brevis [1,2]. In every population it can affect from from 1
to 3 % of active working people[3]. It can impaired the function of the dominating hand in
men and women [1,4 ]. The disorder is often defined as the repetitive strain injury of the
muscles attached to the lateral epicondylitis [5]. Previous studies pointed the tennis elbow as
the type of tendinitis what suggested the presence of the acute inflammatory process. Current
research investigating the absence of inflammatory marker in patients with tennis elbow
indicating the term “tendinosis” or “tendinopathy” as more appropriate to reflect the chronic
process [6,7]. The basic symptom of the tennis elbow is pain localized in the area of the
lateral epicondyle aggravating with hand grips and resistance applied to the muscles of the
forearm during the wrist extension[8].
The conservative therapy is based on use of ultrasound, cryotherapy, heat, electrical and laser
stimulation or extracorporeal shock wave therapy [9-15]. The other possible treatment is
based of pharmacological preparates e.g. non- steroidal anti-inflammatory drugs (NSAID),
corticosteroids prepared for the injections in the area of the lateral epicondyle [16-19].
Modern therapies focus on the botulinum toxin type A injections in improving the healing of
the tendons attached to the lateral epicondyle [20,21]. Another type of injections performed in
this area is use of the platelet-rich plasma extracted from the patient’s own blood and the
effect of the autologos growth factors [22,23]. The physical therapy seems to be still more
accessible for the patient and less invasive than even very promising biological treatment but
require new approach and techniques focusing on the core of the patients problem. One of the
new ideas in manual Kinesio® taping developed by Kenzo Kase. The concept is based on
application of the special elastic tapes to the skin, over and around muscles in order to assist
and give support or to prevent over-contraction. Kinesio® Taping affects also the activation
of the neurological system, the circulatory system and improve healing of overcontracted
muscles [24,25].
Aim of the study
44
The aim of the was to assess the influence of the manual Kinesio® taping application on pain
and the functional status of the patients with lateral epicondylalgia.
Material and methods
The study was conducted on group of patients (15 men and 8 women) diagnosed with lateral
epicondylalgia who suffered for at least three months and failed to the conventional therapy.
The exclusion criteria for the study was: previous injury of the elbow in anamnesis, structural
changes in the area of the elbow, osteoarthritis of the elbow, receiving any therapy for lateral
epicondylitis during last 4 weeks, cervical spine changes and symptoms of radiculopathy, skin
changes, allergy observed after tape application, inflammation in the elbow area.
During the study the patients underwent physical examination of the upper limbs.
The standardized questionnaires e.g. Quick DASH (Disability of the Arm, Shoulder and
Hand) and PRTEE (Patients’ Related Tennis Elbow Examination) were used to assess the
functionality in this condition. To determinate the severity of the pain the visual-analog scale
(VAS) was applied.
DASH and Quick DASH
The Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure is 30-item, self-
report questionnaire developed to measure physical function and symptoms in patients with
musculoskeletal dysfunctions of the upper limb. It was released in 1996 [26]. This tool was
designed by the Institute for Work & Health and the American Academy of Orthopaedic
Surgeons (AAOS) and supported by the American Association for Hand Surgery, the
American Orthopaedic Society for Sports Medicine, the American Shoulder & Elbow
Surgeons, the American Society for Surgery of the Hand, the Arthroscopy Association of
North America and the American Society of Plastic and Reconstructive Surgeons [27]. The
QuickDASH is a shortened version of the DASH Outcome Measure. Instead of 30 items, the
QuickDASH based on 11 items to measure functionality and symptoms of patients with any
musculoskeletal disorders of the upper limb. Scoring is divided into the two components: the
disability/symptom section, consisting of 11 items, scored 1-5 and the optional high
performance sport/music or work modules with 4 items, scored 1-5. To calculate the score at
least 10 of the 11 items must be completed. Bacause this tool was developed to measure the
disability, the scaling was ranked from 0 indicating least disability to 100 indicating most
disability. The researcher should be aware of the direction of the scales [27]. This tool

45
included also two optional modules intended to assess symptoms and function in athletes,
performing artists and high degree physical performance workers. Both instruments are valid,
reliable and responsive and can be used for clinical and research purpose [28,29]. The tools
are characterized by rating of intra-class correlation coefficient on 0.94 and Cronbach’s alpha
also on. 0.94 [30].
The Patient-rated Tennis Elbow Evaluation (PRTEE)
This instrument enables quantitative rating by the patient of pain and functional impairment
associated with lateral epicondylitis, commonly called “tennis elbow”. PRTEE is an
instrument that has been developed specifically for use with this disorder, and is increasingly
being included in research, especially randomized controlled trials.
The questionnaire consist of a 15-item, with five addressing pain and ten concerned with
functional impairment. Each of the item are rated with use of 0 – 10 numerical scale to assess
the average pain or difficulty they have faced over the previous week during various activities
that usually cause pain in tennis elbow. In this system the pain and function are weighted
equally in the total score [31,32]. Higher scores present greater severity and the maximum
score is 100. Major advantages of this instrument are its simplicity, shortness and specificity
to lateral epicondylitis [33,34]. The characteristic of the test is based on recent study used a
four-week test-retest period and calculated Intraclass Correlation Coefficient values of 0.81
for the pain sub-score and 0.76 for the total score. In another studies the Cronbach's alpha
coefficients were high for both the pain and function sub-scales (0.84 and 0.93, respectively)
[35,36].
Pain assessment - Visual-analog scale (VAS)
Visual-analog scale is a psychometric response scale which can be used in questionnaires.
This measurement instrument can be used for subjective characteristics or attitudes that are
impossible to measure directly. Pain assessed in VAS scale is a unidimensional measure of
pain intensity. Respondents express their level of agreement to a statement by pointing a
position along a continuous line between two end-points on a 100-mm long horizontal line.
Usually it takes less than 1 minute to complete the measure [37,38]. Scoring on VAS is
determined by measuring with ruler the distance (mm) on the 10-cm line between the “no
pain” anchor and the patient’s mark, providing a range of scores from 0–100. According to
the research, the visual analogue scales have superior metrical characteristics than discrete
scales, therefore a wider range of statistical methods can be applied to the measured
46
parameters [39,40]. The characteristic of the instrument is based on calculated intraclass
correlation coefficients (ICC) on 0.97 for acute pain and Cronbach’s alpha varies depending
on the studies from 0.79 to 0.91 [41,42].
The pain was assessed as a total feeling, during the wrist extension, during palpation the area
of the lateral epicondyle, during the hand grip, during stretch of extensor carpi radialis brevis
(ECRB) muscle and during movements of elbow.
Therapy process
All procedures where performed by one certified in Kinesio® Taping Method practitioner
with used of original Kinesio® Tex Gold tape for application. The application were perfomed
during 4 weeks. All patients were instructed to deal with the applied tape at home. The
process of the diagnosis and the Kinesio® Tex Gold tape application is presented on pictures
(Fig. 1-7).
Data collection and analysis
Patients underwent the examination and fulfilled the questionnaires at the beginning of the
therapy and after completing it. The data collected were taken into the statistical analysis and
present in the results. All data were expressed by mean ±standard deviation. The normality of
the data distribution was estimated with use of Shapiro-Wilk test. The Wilcoxon rank-sum
test was used for comparison of the two related groups of the data. The alfa significance level
was set at 0.05. P value of less than 0.05 will be considered to indicate statistical significance.
Statistical analyses was performed with use of Statistica 10.0 software (StatSoft).
Results
The study group consist of 23 patients, 15 men and 8 women. The mean age of the patients
was 38,8 ± 4,6 years. None of the patient were tennis player or professional athlete. The
occupation of the patients was mostly in office or physical work in agriculture. Most difficult
and painful activity were associated with the hand grip and the palpation of the lateral
epicondyle. In all patients the elbow of the dominating hand was affected. All patients were
underwent the set of conventional physical therapy and still have symptoms seriously
impairing their daily
The pain measured during different hand and elbow position is presented in table 1.

47
The average total pain experienced during last week before entering Kinesio®taping
application was around 5,5. After completing all sets of the application patients rated their
overall pain just on 3,5. Before the therapy the most painful for the patients were the
movement of wrist extension and all procedures performed with affected hand grip. The best
improvements in pain severity were observed in these measurements.
The highest impairment measured with the Quick DASH Outcome Measure was observed in
additional work module and in this module the highest improvement was observed. The
statistical analysis proved the statistically significant decrease of the patients functionality
deficit express by the results of the Quick DASH (data presented in table 2).
The Patient-rated Tennis Elbow Evaluation (PRTEE), specially designed diagnostic
instrument dedicated for the tennis elbow allowed to assess the pain and function, before and
after completing the set of Kinesio®taping application There were equal statistically
significant improvement in domain of pain and function assessed by the patient (p<0.01). The
results are presented in table 3.
Table 1. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after the Kinesio® taping application.
Pain measured with VAS scale
during
before Kinesio®taping
application
after Kinesio®taping
application
total feeling of pain 5,5 ± 0,7 3,5 ± 0,51
wrist extension 6,2 ± 0,52 3,3 ± 0,6
lateran epicondyle palpation 6,06 ± 0,49 3,75 ± 0,57
hand grip 6,13 ± 0,55 3,55 ± 0,50
stretch of ECRB 6,10 ± 0,51 3,07 ± 0,65
elbow flexion 3,43 ± 0,29 2,21± 0,21
elbow extension 3,48 ± 0,46 2,38 ± 0,2
forearm pronation 2,92 ± 0,19 2,3 ±0,22
forearm supination 2,80 ± 0,12 2,1 ± 0,18
α= 0.05, in all analyses p<0.01

48
Table 2. The comparison of the main results of the Quick Dash Measure Outcome in patients
before and after the Kinesio®taping application.
Main module-
Restriction Index
Additional module-
work
Additional module-
sport
Before
Kinesio®taping
application
0,70 ± 0,10 0,80 ± 0,12 0,78 ± 0,16
After
Kinesio®taping
application
0,14 ± 0,04 0,18 ± 0,02 0,62 ± 0,1
The mean
improvement
0,54 0,62 0,16
α= 0.05, in all analyses p<0.01
Table 3. The comparison of the pain, function and total results of the Patient-rated Tennis
Elbow Evaluation (PRTEE) fulfilled by patients before and after Kinesio®taping application.
Pain PRTEE
Function
PRTEE Total PRTEE
Before
Kinesio®taping
application
0,78 ± 0,14 0,74 ± 0,16 0,76 ± 0,15
After
Kinesio®taping
application
0,20 ± 0,1 0,16 ± 0,04 0,18 ± 0,07
The mean
improvement
0,58 0,58 0,58
α= 0.05, in all analyses p<0.01

49
Discussion
The study showed that application of the Kinesio® Tex Gold tape can significantly reduce the
pain occurring during the wrist extension and hand grip. The experimental study of Liu and
Chen with use of ultrasound proved the role of these application in enlarging muscle motion
[25]. The research of the Chang and Wang suggest that application of the Kinesiot® taping
and placebo-taping have the same effect on pain conditions and wrist flexor stenght [43].
Vicenzino and Brooksbank in their research pointed the improvement in pain-free grips
strength after Kinesio® taping application significantly higher than in control and placebo
groups [44]. The literature about the Kinesio®taping application and its role in lateral
epicondylitis improvement is very limited and based mostly on the application proposed by
the developer of the method [45].
The research limitation
The limitation of the study is small group of the patients included who underwent whole
process of the examination and all sets of Kinesio®taping application, therefore the study can
be underpowered. Another limitation is the lack of the control group included into the process
of randomization. To exactly determine the effect of mobilization Kinesio®taping application
in patients with symptoms of tennis elbow there is a need of randomized controlled trial.
Conclusions
Kinesio®taping application seems to be effective as supportive therapy of patients with lateral
epicondylitis. It leads to decrease of the severity of the pain, improve patients functionality
assessed with standardized questionnaires .

50
Fig.1. Application starts with placing the middle of the one short stripe over the most painful
area with 50% stretch.
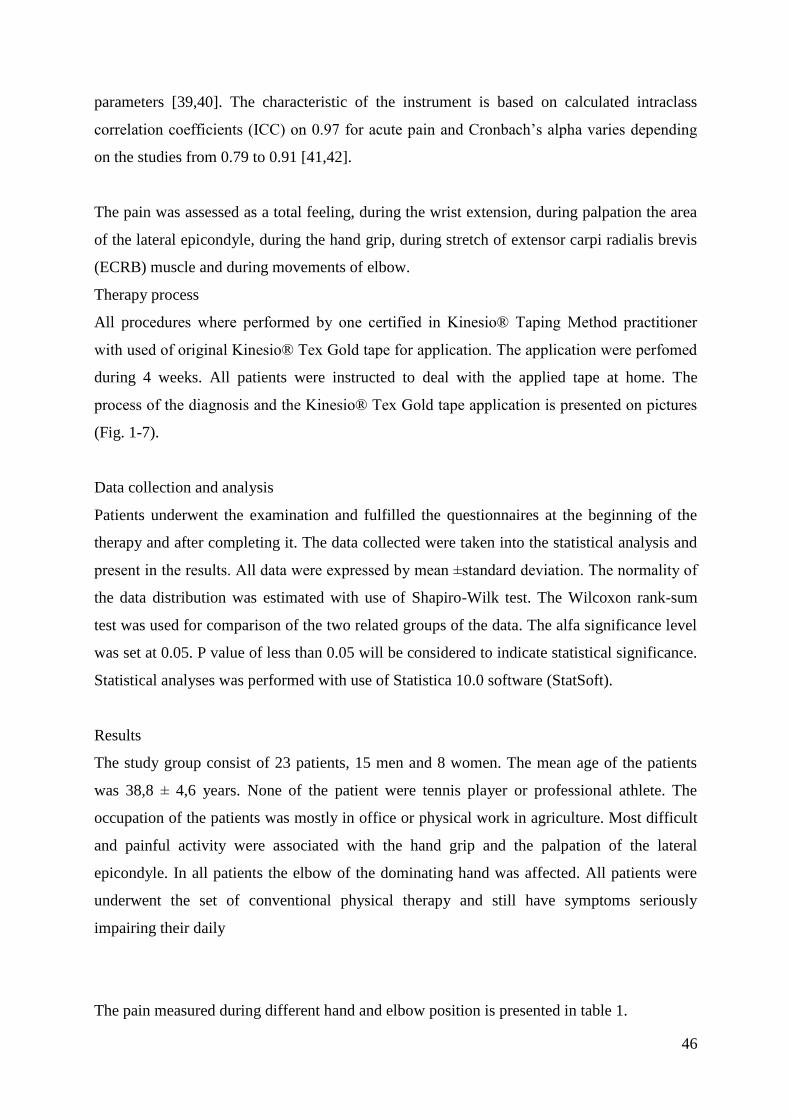
Fig.2. Endings of the one short stripe over the most painful area are placed with no tension.

51
Fig.3 The second short stripe of the tape is placed with 50% tension in the middle and should
cross the previous stripe in the most painful area of the elbow.
Fig.4 Endings of the second short stripe over the most painful area are also placed with no
tension.

52
Fig.5. Basis of the third long stripe is placed with no tension over the elbow on the lateral part
of arm.
Fig.6. The tape is placed over the most painful area of the elbow and along with the forearm
muscles with 25 % tension.

53
Fig.7. Finished application of the Kinesio ® Tex Gold tapes. The stripe is applicated on the
forearm with no tension.

54
Summary
Background:
"Tennis elbow" is a condition characterized by the pain in a region of the lateral epicondylus
of humerus, weakness of the forearm muscles, grips forces and general dysfunctions of upper
extremity. The standard management of the lateral epicondylitis consists of physical therapy
methods, pharmacological treatment, immobilization and surgical techniques. Recently the
Kinesio® taping method is more often applied in patients with symptoms of this condition.
The elastic properties of Kinesio® Tex Tape applied according to the Kinesio® Taping
Method can enhance the function of muscle fibers and decrease the pain.
Aim of the study :
The aim of the study was to estimate the symptoms reduction and the improvement of the
functionality of upper limb after Kinesio®taping application in patients with "tennis elbow"
symptoms.
Material and methods:
The study group consisted of 23 patients with tennis elbow treated with the physical therapy
methods and Kinesio® taping applications. All procedures were performed by certified
physiotherapist and Kinesio taping practitioner with use of Kinesio® Tex tape. The VAS,
PRTEE scales and Quick DASH questionnaires were used to assess the effectiveness of this
management. The range of motion, the pain free grip strength and the maximal strength of the
grip was tested at the beginning and the end of the therapy. The data collected were analyzed
with use of Statistica 10.0 software. The significance level of 0.05 (α = 5%) was adopted.
Results:
The significant reduction of pain in the lateral epicondylus region measured in VAS scale and
values of the PRTEE and Quick DASH questionnaire were observed in the study group. The
pain during the hand grip and the wrist, elbow movements were significantly improvement in
group of patients treated with application of the Kinesio® Tex Gold tapes (p<0.05).
Conclusions:
Kinesio® taping is a promising and effective method in decreasing symptoms of "tennis
elbow", mostly the pain and hand grip.

55
References
1. Norris C. Sports injuriesddiagnosis and management. 3rd ed. Butterworth Heinemann;
2005. p. 412e7.
2. Greenbaum B, Hammura J. Extensor carpi radialis brevis: an anatomical analysis of its
origin. J Bone Joint Surg Br 1999;81:926e9.
3. Hong Q, Durand M, Loisel P. Treatment of lateral epicondylitis: where is the evidence?
Joint Bone Spine 2004;71: 369e73.
4. LaFreniere JG. Tennis elbow: evaluation, treatment, and prevention. Phys Ther
1979;59:742e6.
5. Boyer MI, Hastings H. Lateral tennis elbow: “Is there any science out there?”. J Shoulder
Elbow Surg 1999;8:481e91.
6. Nirschl R.P., Ashman E.S., Elbow tendinopathy: Tennis elbow. Clin Sports Med. 2003;
22(4):813–836.
7. Stasinopoulos D, Johnson MI, ‘Lateral elbow tendinopathy’ is the most appropriate
diagnostic term for the condition commonly referred-to as lateral epicondylitis. Med
Hypotheses. 2006; 67(6):1400–1402.
8 . Van Hofwegen C, Baker CL 3rd, Baker CL Jr. Epicondylitis in the athlete's elbow. Sports
Med. 2010 Oct;29(4):577-97.
9. Kamien M. A rational management of tennis elbow. Sports Med 1990;9:173e91.
10. Haker EHK, Lundeberg TCM. Lateral epicondylalgia report of noneffective midlaser
treatment. Arch Phys Med Rehabil 1991; 72:984e8.
11. Lundeberg T, Abrahamsson P, Haker E. A comparative study of continuous ultrasound,
placebo ultrasound and rest in epicondylalgia. Scand J Rehabil Med 1988;20:99e101.
12. Bisset L, Paungmali A, Vicenzino BA. Systematic review and meta-analysis of clinical
trials on physical interventions for lateral epicondylalgia. Br J Sports Med 2005;39:411e22
13. Halle J, Franklin R, Karalfa B. Comparison of four treatment approaches for lateral
epicondylitis of the elbow. J Orthop Sports Phys Ther 1986;8:62e9.
14. Simunovic Z, Trobonjaca T, Trobonjaca Z. Treatment of medial and lateral
epicondylitisdtennis and golfer’s elbowdwith low level laser therapy. Laser Med Surg
1998;16:145e51.
15 Rompe JD, Hopf C, Kullmer K, Heine J, Burger R. Analgesic effect of extracorporeal
shock wave therapy on chronic tennis elbow. J Bone Joint Surg 1996;78:233e7.
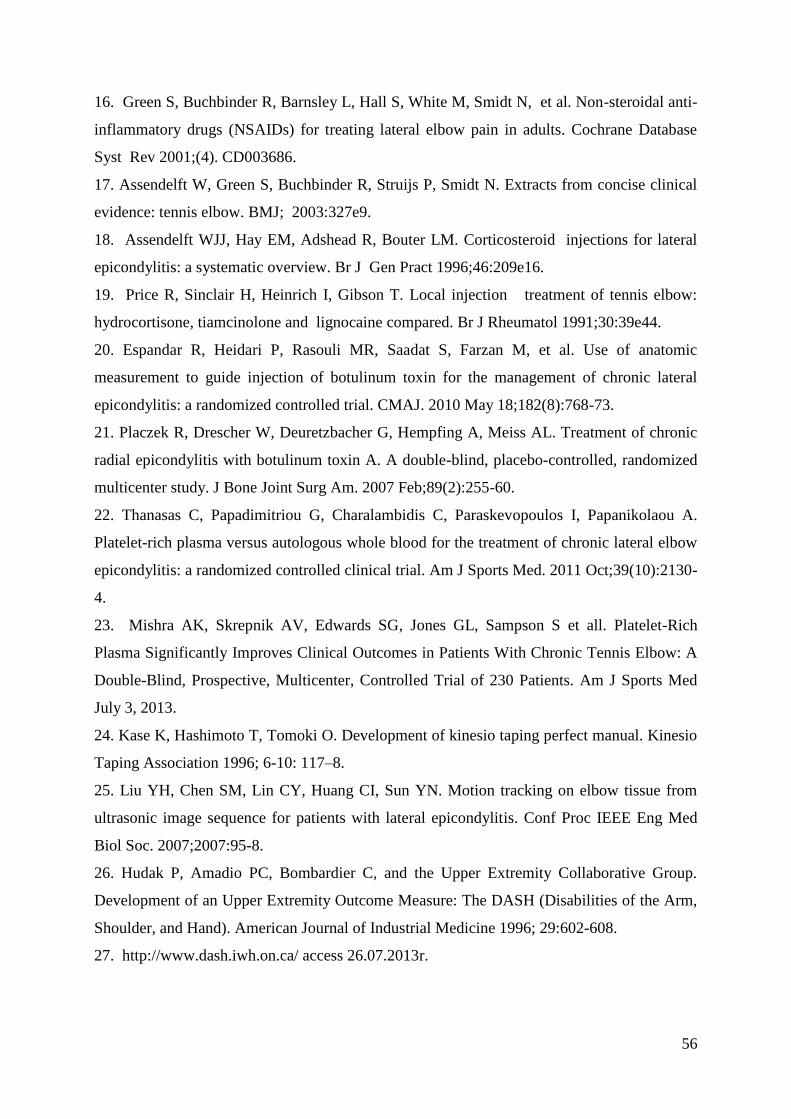
56
16. Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, et al. Non-steroidal anti-
inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database
Syst Rev 2001;(4). CD003686.
17. Assendelft W, Green S, Buchbinder R, Struijs P, Smidt N. Extracts from concise clinical
evidence: tennis elbow. BMJ; 2003:327e9.
18. Assendelft WJJ, Hay EM, Adshead R, Bouter LM. Corticosteroid injections for lateral
epicondylitis: a systematic overview. Br J Gen Pract 1996;46:209e16.
19. Price R, Sinclair H, Heinrich I, Gibson T. Local injection treatment of tennis elbow:
hydrocortisone, tiamcinolone and lignocaine compared. Br J Rheumatol 1991;30:39e44.
20. Espandar R, Heidari P, Rasouli MR, Saadat S, Farzan M, et al. Use of anatomic
measurement to guide injection of botulinum toxin for the management of chronic lateral
epicondylitis: a randomized controlled trial. CMAJ. 2010 May 18;182(8):768-73.
21. Placzek R, Drescher W, Deuretzbacher G, Hempfing A, Meiss AL. Treatment of chronic
radial epicondylitis with botulinum toxin A. A double-blind, placebo-controlled, randomized
multicenter study. J Bone Joint Surg Am. 2007 Feb;89(2):255-60.
22. Thanasas C, Papadimitriou G, Charalambidis C, Paraskevopoulos I, Papanikolaou A.
Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow
epicondylitis: a randomized controlled clinical trial. Am J Sports Med. 2011 Oct;39(10):2130-
4.
23. Mishra AK, Skrepnik AV, Edwards SG, Jones GL, Sampson S et all. Platelet-Rich
Plasma Significantly Improves Clinical Outcomes in Patients With Chronic Tennis Elbow: A
Double-Blind, Prospective, Multicenter, Controlled Trial of 230 Patients. Am J Sports Med
July 3, 2013.
24. Kase K, Hashimoto T, Tomoki O. Development of kinesio taping perfect manual. Kinesio
Taping Association 1996; 6-10: 117–8.
25. Liu YH, Chen SM, Lin CY, Huang CI, Sun YN. Motion tracking on elbow tissue from
ultrasonic image sequence for patients with lateral epicondylitis. Conf Proc IEEE Eng Med
Biol Soc. 2007;2007:95-8.
26. Hudak P, Amadio PC, Bombardier C, and the Upper Extremity Collaborative Group.
Development of an Upper Extremity Outcome Measure: The DASH (Disabilities of the Arm,
Shoulder, and Hand). American Journal of Industrial Medicine 1996; 29:602-608.
27. http://www.dash.iwh.on.ca/ access 26.07.2013r.

57
28. Beaton DE, Davis AM, Hudak P, McConnell S. The DASH (Disabilities of the Arm,
Shoulder and Hand) outcome measure: What do we know about it now? British Journal of
Hand Therapy 2001a; 6(4):109-118.
29. Kennedy CA, Beaton DE, Solway S, McConnell S, Bombardier C. Disabilities of the
Arm, Shoulder and Hand (DASH). The DASH and QuickDASH Outcome Measure User’s
Manual, Third Edition. Toronto, Ontario: Institute for Work & Health, 2011.
30. Beaton DE, Wright JG, Katz JN, and the Upper Extremity Collaborative Group.
Development of the QuickDASH: Comparison of three item-reduction approaches. Journal of
Bone and Joint Surgery 2005a; 87A(5):1038-1046.
31. MacDermid, J. Update: The Patient-rated Forearm Evaluation Questionnaire is now the
Patient-rated Tennis Elbow Evaluation. J Hand Ther, 2005. 18(4): p. 407-10.
32. MacDermid, J. The Patient-Rated Tennis Elbow Evaluation (PRTEE) User Manual. 2007,
School of Rehabilitation Science, McMaster University: Hamilton, Canada.
33 Rompe, J.D., T.J. Overend, and J.C. MacDermid, Validation of the Patient-rated Tennis
Elbow Evaluation Questionnaire. J Hand Ther, 2007. 20(1): p. 3-10; quiz 11.
34 D'Vaz, A.P., A.J. Ostor, C.A. Speed, et al. Pulsed low-intensity ultrasound therapy for
chronic lateral epicondylitis: a randomized controlled trial. Rheumatology (Oxford), 2006.
45(5): p. 566-70.
35.Chung, B. and J.P. Wiley. Validity, responsiveness and reliability of the Patient-Rated
Tennis Elbow Evaluation. Hand Therap, 2010. 15(3): p. 62-68.
36. Nilsson P, Baigi P, Marklund P, Månsson J. Cross-cultural adaptation and determination
of the reliability and validity of PRTEE-S (Patientskattad Utvärdering av Tennisarmbåge), a
questionnaire for patients with lateral epicondylalgia, in a Swedish population. BMC
Musculoskelet Disord. 2008; 9: 79.
37. Reips UD, Funke F. "Interval level measurement with visual analogue scales in Internet-
based research: VAS Generator." doi:10.3758/BRM.40.3.699
38. Grant S, Aitchison T, Henderson E, Christie J, Zare S, et al. A comparison of the
reproducibility and the sensitivity to change of visual analogue scales, Borg scales, and Likert
scales in normal subjects during submaximal exercise. Chest. 116(5):1208-17.
39. McCaffery M, Pasero C. Pain: Clinical Manual, St. Louis, 1999, P. 16.
40. Bijur PE, Silver W, Gallagher J. Reliability of the Visual Analog Scale for Measurement
of Acute Pain. Academic Emergency Medicine Volume 8, Issue 12, pages 1153–1157,
December 2001.

58
41. McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a
critical review. Psychol Med 1988;18:1007–19.
42. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison
of six methods. Pain 1986;27:117–26.
43. Chang HY, Wang CH, Chou KY, Cheng SC. Could forearm Kinesio Taping improve
strength, force sense, and pain in baseball pitchers with medial epicondylitis? Clin J Sport
Med. 2012 Jul;22(4):327-33.
44. Vicenzino B, Brooksbank J, Minto J, Offord S, Paungmali A. Initial effects of elbow
taping on pain-free grip strength and pressure pain threshold. J Orthop Sports Phys Ther. 2003
Jul;33(7):400-7.
45. Kase K, Wallis J. The latest kinesio taping method. Ski-J 2002.

59
Joanna Fidut, Katarzyna Chomiuk, Karolina Janikowska
Review of the musculofascial Kinesio® taping applications for the lateral epicondylalgia – part 1
Background
Kinesio® taping was developed by Kenzo Kase in early 1970’. The concept is based on
application of the special elastic tapes to the skin, over and around muscles in order to assist
and give support or to prevent over-contraction. Kinesio® Taping affects also the activation
of the neurological system, the circulatory system and improve healing of overcontracted
muscles. Kinesio Taping is currently being used by therapists to modify muscle tone, move
lymphatic fluids, correct movement patterns, and improve body posture. The Kinesio®
Taping Method is a unique method of applying Kinesio® Tex Tape in a specific manner to
create change in the tissue under the applied tape. The experimental study of Liu and Chen
with use of ultrasound proved the role of these application in enlarging muscle motion. The
research of the Chang and Wang suggest that application of the Kinesiot® taping and
placebo-taping have the same effect on pain conditions and wrist flexor stenght. Vicenzino
and Brooksbank in their research pointed the improvement in pain-free grips strength after
Kinesio® taping application significantly higher than in control and placebo groups. The
literature about the Kinesio®taping application and its role in lateral epicondylitis
improvement is very limited and based mostly on the application proposed by the developer
of the method.
Muscular and fascial Kinesio®taping application (Fig. 1-10.)
Description and preparation of the Kinesio® Tex Gold tape.
The application is based on three parts of the tape. One part (black on Fig. 1) is a one short
strip prepared for the direct application over the most painful area. Second tape (black on Fig.
1) is for the same purpose. Third tape (blue on Fig.3) is a long strip prepared to be placed
from arm to the forearm. The endings of the tapes should be rounded. All application are
performed with use of Kinesio® Tex Gold tapes.

60
Fig.1. Kinesio® Tex Gold tapes cut for before the application. Initial preparation is important
and strips of kinesiology tape are cut so the ends are rounded.
Fig.2. Application starts with placing the middle of the one short stripe over the most painful
area with 50% stretch.
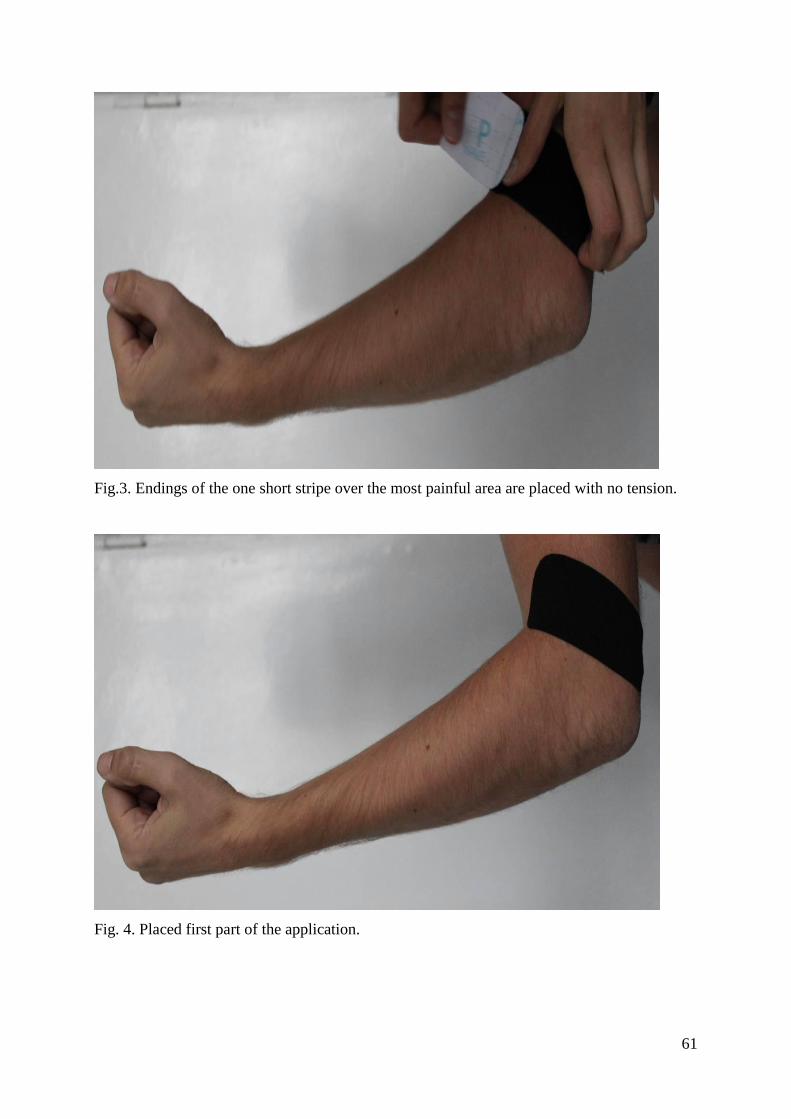
61
Fig.3. Endings of the one short stripe over the most painful area are placed with no tension.
Fig. 4. Placed first part of the application.

62
Fig.5. The second short stripe of the tape is placed with 50% tension in the middle and should
cross the previous stripe in the most painful area of the elbow.
Fig.6. Endings of the second short stripe over the most painful area are also placed with no
tension.

63
Fig.7. Basis of the third long stripe is placed with no tension over the elbow on the lateral part
of arm.
Fig.8. The tape is placed over the most painful area of the elbow and along with the forearm
muscles with 25 % tension.

64
Fig.9. The stripe is applicated on the forearm with no tension.
Fig.10. Finished application of the Kinesio ® Tex Gold tapes.

65
References:
Kase K, Wallis J. The latest kinesio taping method. Ski-J 2002.
Kase K, Hashimoto T, Tomoki O. Development of kinesio taping perfect manual. Kinesio
Taping Association 1996; 6-10: 117–8.
Kinesio Taping Perfect Manual by Kinesio Taping Association, 2Ed.
llustrated Kinesio Taping manual, 4th Ed.
Clinical Kinesio Taping - DVD.
Kase K, Wallis J. Clinical Therapeutic Applications of the Kinesio Taping Method 3rd
Edition, Ski-J 2003.

66
Joanna Fidut, Katarzyna Chomiuk, Karolina Janikowska
Review of the musculofascial Kinesio® taping applications for the lateral epicondylalgia – part 2
Background
Kinesio® taping was developed by Kenzo Kase in early 1970’. The concept is based on
application of the special elastic tapes to the skin, over and around muscles in order to assist
and give support or to prevent over-contraction. Kinesio® Taping affects also the activation
of the neurological system, the circulatory system and improve healing of overcontracted
muscles. Kinesio Taping is currently being used by therapists to modify muscle tone, move
lymphatic fluids, correct movement patterns, and improve body posture. The Kinesio®
Taping Method is a unique method of applying Kinesio® Tex Tape in a specific manner to
create change in the tissue under the applied tape. The experimental study of Liu and Chen
with use of ultrasound proved the role of these application in enlarging muscle motion. The
research of the Chang and Wang suggest that application of the Kinesiot® taping and
placebo-taping have the same effect on pain conditions and wrist flexor stenght. Vicenzino
and Brooksbank in their research pointed the improvement in pain-free grips strength after
Kinesio® taping application significantly higher than in control and placebo groups. The
literature about the Kinesio®taping application and its role in lateral epicondylitis
improvement is very limited and based mostly on the application proposed by the developer
of the method.
Muscular and fascial Kinesio®taping application (Fig. 1-7.)
Description and preparation of the Kinesio® Tex Gold tape.
The application is based on two parts. One tape (black on Fig. 1) is a one long strip prepared
for the muscle application. Second tape (blue on Fig. 1) is dedicated for the fascia application
and divided into two strips from the basis. The endings of the tapes should be rounded. All
application are performed with use of Kinesio® Tex Gold tapes.

67
Fig.1. Kinesio® Tex Gold tapes cut for before the application. Initial preparation is important
and strips of kinesiology tape are cut so the ends are rounded.
Fig.2. Placing the basis of muscle application on dorsal surface of the wrist with no tension.
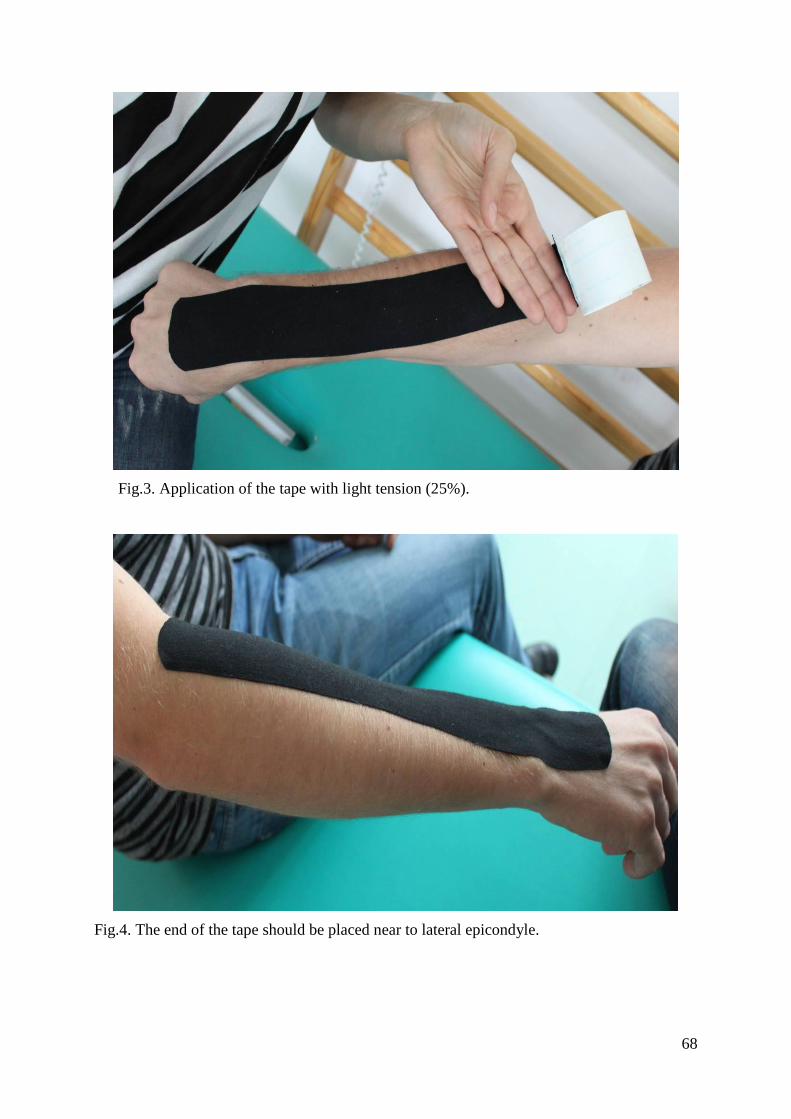
68
Fig.3. Application of the tape with light tension (25%).
Fig.4. The end of the tape should be placed near to lateral epicondyle.

69
Fig.5. Basis placed with no stretch and application of the strips with 75% stretch from
posterior area of the elbow.
Fig.6. Placing the end of the tape with no tension close to the medial epicondyle of the right
elbow.
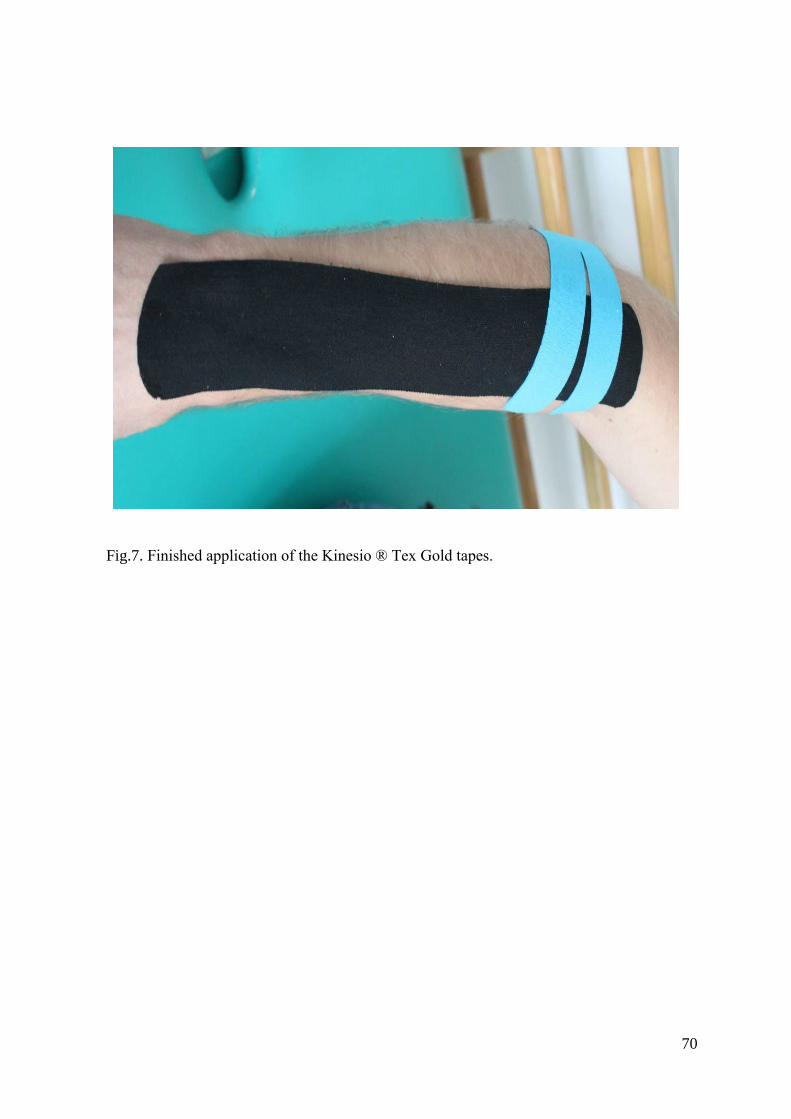
70
Fig.7. Finished application of the Kinesio ® Tex Gold tapes.

71
Muscular and fascial Kinesio®taping application (Fig. 8-15.)
Description and preparation of the Kinesio® Tex Gold tape.
The application is based on two parts. One tape (black on Fig. 1.) cut vertically to the basis is
prepared for the muscle application. Second strip of the tape (pink on Fig. 2.) is dedicated for
the fascia application. The endings of the tapes should be rounded. All application are
performed with use of Kinesio® Tex Gold tapes.
Fig.8. Kinesio® Tex Gold tapes cut for before the application.

72
Fig.9. Placing the basis of muscle application with no tension over the elbow.
Fig.10. Application of the upper and lower strip with light tension (50%).

73
Fig.11. Placing the end of strip on the dorsal surface of the forearm with no tension.
Fig.12. Placing the basis of the tape with no tension below the lateral epicondyle of the elbow.

74
Fig.13. Application of the tape with 75% stretch from posterior to anterior area of the elbow.
Fig.14. Placing the end of the tape with no tension close to the medial epicondyle of the
elbow.

75
Fig.15. Finished application of the Kinesio ® Tex Gold tapes.
References:
Kase K, Wallis J. The latest kinesio taping method. Ski-J 2002.
Kase K, Hashimoto T, Tomoki O. Development of kinesio taping perfect manual. Kinesio
Taping Association 1996; 6-10: 117–8.
Kinesio Taping Perfect Manual by Kinesio Taping Association, 2Ed.
llustrated Kinesio Taping manual, 4th Ed.
Clinical Kinesio Taping - DVD.
Kase K, Wallis J. Clinical Therapeutic Applications of the Kinesio Taping Method 3rd
Edition, Ski-J 2003.
76
Joanna Fidut, Katarzyna Chomiuk, Karolina Janikowska
Kinesio® taping application for elbow pain
Background
Kinesio® taping was developed by Kenzo Kase in early 1970’. The concept is based on
application of the special elastic tapes to the skin, over and around muscles in order to assist
and give support or to prevent over-contraction. Kinesio® Taping affects also the activation
of the neurological system, the circulatory system and improve healing of overcontracted
muscles. Kinesio Taping is currently being used by therapists to modify muscle tone, move
lymphatic fluids, correct movement patterns, and improve body posture. The Kinesio®
Taping Method is a unique method of applying Kinesio® Tex Tape in a specific manner to
create change in the tissue under the applied tape. The experimental study of Liu and Chen
with use of ultrasound proved the role of these application in enlarging muscle motion. The
research of the Chang and Wang suggest that application of the Kinesiot® taping and
placebo-taping have the same effect on pain conditions and wrist flexor stenght. Vicenzino
and Brooksbank in their research pointed the improvement in pain-free grips strength after
Kinesio® taping application significantly higher than in control and placebo groups. The
literature about the Kinesio®taping application and its role in lateral epicondylitis
improvement is very limited and based mostly on the application proposed by the developer
of the method.
Fascial Kinesio®taping application for lateral epicondylalgia (Fig. 1-7).
Description and preparation of the Kinesio® Tex Gold tape.
Application
The application is based on two parts. One tape (black on Fig. 1) is a one short strip prepared
for the fascial application. Second tape (pink on Fig. 1.) is also dedicated for the fascia
application. The endings of the tapes should be rounded. All application are performed with
use of Kinesio® Tex Gold tapes.

77
Fig.1. the Kinesio® Tex Gold tapes cut for before the application.

78
Fig.2. Placing the basis of muscle application on medial surface of the elbow with no tension.
Fig.3. Application of the tape with 75% stretch over the painful lateral epicondyle of the
elbow.
Fig.4. Placing the end of strip with no tension.

79
Fig.5. Basis of the second tape placed with no tension just below the black stripe.
Fig. 6. Application of the second strip with 75% stretch from the medial to the lateral area of
the elbow.

80
Fig.7. Finished fascial application of the Kinesio ® Tex Gold tapes.
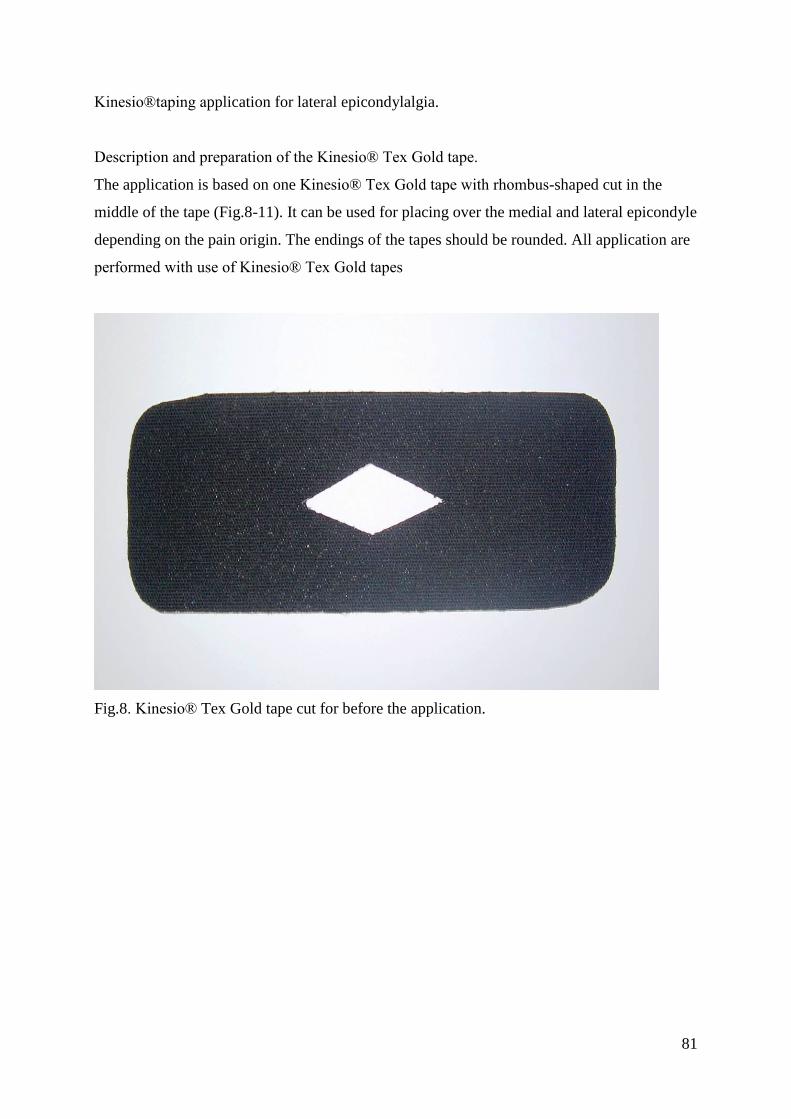
81
Kinesio®taping application for lateral epicondylalgia.
Description and preparation of the Kinesio® Tex Gold tape.
The application is based on one Kinesio® Tex Gold tape with rhombus-shaped cut in the
middle of the tape (Fig.8-11). It can be used for placing over the medial and lateral epicondyle
depending on the pain origin. The endings of the tapes should be rounded. All application are
performed with use of Kinesio® Tex Gold tapes
Fig.8. Kinesio® Tex Gold tape cut for before the application.

82
Fig.9. Placing the basis of muscle application on lateral surface of the elbow with 50%
tension.
Fig.10. Application of the tape with no tension.

83
Fig.11. Finished application of the Kinesio® Tex Gold tape around the area of painful lateral
epicondyle.

84
Muscular Kinesio®taping application for lateral epicondylalgia (Fig.11-16)
Description and preparation of the Kinesio® Tex Gold tape.
The application is based one long stripe of the Kinesio® Tex Gold tape (Fig. 11) prepared for
the muscle application. The proximal part has two rhombus-shaped holes dedicated for II and
III finger. The endings of the tapes should be rounded. All application are performed with use
of Kinesio® Tex Gold tapes.
Fig.11. Kinesio® Tex Gold tapes cut for before the application. Initial preparation is
important and strips of kinesiology tape are cut so the ends are rounded.

85
Fig.12. Placing the proximal part of tape on the II and III finger with no tension.
Fig.13. Placing the basis of the proximal part of tape on the palmar side of the hand.

86
Fig.14. Application of the stripe on the dorsal part of the hand.
Fig.15. Application of the rest of the stripe on forearm along to the extensor muscles with
25% tension.

87
Fig.16. Finished application of the Kinesio ® Tex Gold tapes. The end of the tape should be
placed near to lateral epicondyle with no stretch.
References:
Kase K, Wallis J. The latest kinesio taping method. Ski-J 2002.
Kase K, Hashimoto T, Tomoki O. Development of kinesio taping perfect manual. Kinesio
Taping Association 1996; 6-10: 117–8.
Kinesio Taping Perfect Manual by Kinesio Taping Association, 2Ed.
llustrated Kinesio Taping manual, 4th Ed.
Clinical Kinesio Taping - DVD.
Kase K, Wallis J. Clinical Therapeutic Applications of the Kinesio Taping Method 3rd
Edition, Ski-J 2003.

88









![Elbow Pain - Welcome To | HealthSharehealthshare.org.uk/HS_leaflets/Elbow_Pain.pdf[ 3 ] Elbow Pain Lateral epicondylitis What is lateral epicondylitis? This is often referred to as](https://static.fdocuments.us/doc/165x107/5ac8bc037f8b9a51678c93c8/elbow-pain-welcome-to-he-3-elbow-pain-lateral-epicondylitis-what-is-lateral.jpg)








