Neuroscience and “real world” practice: music as a therapeutic resource for children in zones of...
8
Ann. N.Y. Acad. Sci. ISSN 0077-8923 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES Issue: The Neurosciences and Music IV: Learning and Memory Neuroscience and “real world” practice: music as a therapeutic resource for children in zones of conflict Nigel Osborne Institute for Music in Human and Social Development (IMHSD), Reid School of Music, University of Edinburgh, Edinburgh, United Kingdom Address for correspondence: Prof. Nigel Osborne, IMHSD, Reid School of Music, University of Edinburgh, Alison House, Nicolson Square, Edinburgh EH8 9DF, United Kingdom. [email protected] Recent developments in music neuroscience are considered a source for reflection on, and evaluation and development of, musical therapeutic practice in the field, in particular, in relation to traumatized children and postconflict societies. Music neuroscience research is related to practice within a broad biopsychosocial framework. Here, examples are detailed of work from North Uganda, Palestine, and South Thailand. Keywords: music; therapy; PTSD Introduction It may be premature to speak of an applied music neuroscience, but the fruits of music neuroscience research have already begun to play a role in re- flection on practice in areas such as music educa- tion, community music, music therapy, and music medicine. An area of work that overlaps with all of these disciplines is the use of music as an in- tervention to support children in zones of conflict and postconflict. 1 Although one of the principal concerns for such children is posttraumatic stress disorder (PTSD), and the most commonly used diagnostic criteria are psychiatric (expo- sure to trauma, traumatic recall, avoidance, and hyperarousal—DSM-IV), 2 the symptoms of trauma are spread over a much wider range of human ex- perience, and the potential usefulness of music is probably best considered from the perspective of a broad biopsychosocial framework (Fig. 1). This short paper records three anecdotes of work in the field from key areas of the frame- work and discusses how reflection on practice, and in some cases practice itself, can be influenced by the results of research in the neuroscience of music. Biological concerns Peter Oloya is one of East Africa’s finest sculptors, regards Damien Hirst as a major influence, and was recently artist-in-residence for Pangolin Editions near Stroud in the United Kingdom. His origins are in a small village—Lemo Bongolewich—near Kitgum in North Uganda. His childhood, however, was overshadowed by the bloody conflict between Joseph Kony’s Lord’s Resistance Army (LRA) and the Uganda People’s Defence Force (UPDF). Between 1987 and 2007 the Luo-speaking Acholi people of North Uganda found themselves between a rock and a hard place, facing murder, rape, abductions, eth- nic cleansing, and the forced recruitment of child militias and prostitutes. It was this life experience that prompted Peter, now 33 years old, to create a nongovernmental or- ganization (NGO) in Kitgum—AFOCOD (Art for Community Development)—using art to support the welfare of communities and children. Some of his volunteers are themselves former child soldiers. In an interview in AfricanColours, 3 he describes his background: Art is my reason for living, in fact it has given a structure to my whole life. I have lived through war doi: 10.1111/j.1749-6632.2012.06473.x Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c 2012 New York Academy of Sciences. 69
-
Upload
nigel-osborne -
Category
Documents
-
view
212 -
download
0
Transcript of Neuroscience and “real world” practice: music as a therapeutic resource for children in zones of...

Ann. N.Y. Acad. Sci. ISSN 0077-8923
ANNALS OF THE NEW YORK ACADEMY OF SCIENCESIssue: The Neurosciences and Music IV: Learning and Memory
Neuroscience and “real world” practice: music as atherapeutic resource for children in zones of conflict
Nigel OsborneInstitute for Music in Human and Social Development (IMHSD), Reid School of Music, University of Edinburgh, Edinburgh,United Kingdom
Address for correspondence: Prof. Nigel Osborne, IMHSD, Reid School of Music, University of Edinburgh, Alison House,Nicolson Square, Edinburgh EH8 9DF, United Kingdom. [email protected]
Recent developments in music neuroscience are considered a source for reflection on, and evaluation and developmentof, musical therapeutic practice in the field, in particular, in relation to traumatized children and postconflict societies.Music neuroscience research is related to practice within a broad biopsychosocial framework. Here, examples aredetailed of work from North Uganda, Palestine, and South Thailand.
Keywords: music; therapy; PTSD
Introduction
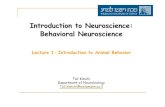
It may be premature to speak of an applied musicneuroscience, but the fruits of music neuroscienceresearch have already begun to play a role in re-flection on practice in areas such as music educa-tion, community music, music therapy, and musicmedicine. An area of work that overlaps with allof these disciplines is the use of music as an in-tervention to support children in zones of conflictand postconflict.1 Although one of the principalconcerns for such children is posttraumatic stressdisorder (PTSD), and the most commonlyused diagnostic criteria are psychiatric (expo-sure to trauma, traumatic recall, avoidance, andhyperarousal—DSM-IV),2 the symptoms of traumaare spread over a much wider range of human ex-perience, and the potential usefulness of music isprobably best considered from the perspective of abroad biopsychosocial framework (Fig. 1).
This short paper records three anecdotes ofwork in the field from key areas of the frame-work and discusses how reflection on practice, andin some cases practice itself, can be influencedby the results of research in the neuroscience ofmusic.
Biological concerns
Peter Oloya is one of East Africa’s finest sculptors,regards Damien Hirst as a major influence, and wasrecently artist-in-residence for Pangolin Editionsnear Stroud in the United Kingdom. His originsare in a small village—Lemo Bongolewich—nearKitgum in North Uganda. His childhood, however,was overshadowed by the bloody conflict betweenJoseph Kony’s Lord’s Resistance Army (LRA) and theUganda People’s Defence Force (UPDF). Between1987 and 2007 the Luo-speaking Acholi people ofNorth Uganda found themselves between a rock anda hard place, facing murder, rape, abductions, eth-nic cleansing, and the forced recruitment of childmilitias and prostitutes.
It was this life experience that prompted Peter,now 33 years old, to create a nongovernmental or-ganization (NGO) in Kitgum—AFOCOD (Art forCommunity Development)—using art to supportthe welfare of communities and children. Some ofhis volunteers are themselves former child soldiers.In an interview in AfricanColours,3 he describes hisbackground:
Art is my reason for living, in fact it has given astructure to my whole life. I have lived through war
doi: 10.1111/j.1749-6632.2012.06473.xAnn. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences. 69

Music as a therapeutic resource Osborne
Figure 1. Proposed biopsychosocial framework for our under-standing of music as a therapeutic resource.
and experienced death throughout my early years,and I used art as a kind of therapy to help get methrough those difficult times. In fact, it continuesto help me to this very day. Most of the childrenand youths who come to us are traumatised butour training really helps with their healing process.Helping to bring some kind of normality to young,innocent lives is very important to me because theyare the future and will one day help to bring peaceto the country.
It is March 2007 and Peter has invited me toKitgum to help develop musical aspects of theAFOCOD program. He believes that there is a “vis-ceral,” physical/mental engagement in music mak-ing that has an important contribution to make tothe welfare of his children. We travel to Ayoma IDPcamp, which lies north of Kitgum, toward the Sudanborder and the “dry lands” where militias still roam.Ayoma is a densely packed maze of mud-and-wattlehuts and dusty narrow passageways where childrenin torn clothes play with improvised toys of tin andcardboard. International NGOs have provided a fewbare administrative and community buildings, andit is in a space by the community center that wedecide to hold our first music workshop.
The children arrive, around 40 of them, followedby the usual gathering of curious adults. There isa specific atmosphere and feeling among groups oftraumatized children that is much the same every-where. Here, it takes the form of a restless numbness,and maybe a little fear. But I am confident I can en-gage the children, and I begin to play North Ugandandances with my colleagues Robert and Hakim from
the Uganda Dance Academy: first gentle rhythmsand slow tempi, then faster and more vigorous mu-sic. We encourage the children to move, to clap,and to sing. We play and dance joyfully and ener-getically, almost to the point of clowning. It is notlong before the transformation has taken place, andthe children are laughing, smiling, and joining inenthusiastically. We are particularly keen that theyuse their voices, breathe well, and move fluently; wewant them to be both energized and relaxed. It is atransformation that never fails and normally leadsto requests, from both children and their caretakers,for our work to continue.
I have written elsewhere about the biologicalsymptoms of PTSD and how music may help chil-dren deal with these problems.1 Although we donot “apply” neuroscience in our work, we can usethe research findings to help relate and connect ourknowledge of the symptoms of trauma to our expe-rience of the intervention in the field.
For example, there is a significant amount of re-search literature on how trauma can affect the heart,in terms of increased heart rate, blood pressure,and cardiac arrhythmias.4–10 This may be consid-ered alongside research from neuroscience and re-lated disciplines that indicate that music may af-fect and help regulate the autonomic nervous sys-tem and related behaviors of the heart.11–20 Finally,practitioners have anecdotal evidence from the fieldthat their work may have a modest effect in helpingregulate children’s hearts and autonomic nervoussystems (e.g., from discussion with general practi-tioners, treating traumatized children at the Centrefor Children with Special Needs, Mostar, Bosnia,and Herzegovina).
Similarly, there is a small body of evidence sug-gesting that PTSD, and stress in general, affect anddysregulate breathing and respiratory sinus arrhyth-mia.21–24 This evidence may be related to researchfindings that music may affect and help regulate au-tomatic breathing and sinus arrhythmia.25–27 Vocalmusic is of course directly and accountably interac-tive with conscious breathing,28 and there is expe-rience from the field of successful work supportingand improving children’s breathing through singing(e.g., once again, in work with children in Bosniaand Herzegovina).1
PTSD is associated with dysregulation of move-ment repertoires, including both hyperactivity andextreme sluggishness.29–32 The music neuroscience
70 Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences.

Osborne Music as a therapeutic resource
literature is rich in research on music and itsrelationship with the premotor and motor cortices,and by inference, its ability to “make us” or to “helpus” move.33 Evidence from the field, based on sim-ple observation of changing movement repertoires,and my own experiences working with children withADHD in Scottish special education, suggests thatmusic may help traumatized children regulate theirmovements.1,33
Finally, there is a large body of evidence thatPTSD dysregulates systems for dealing with stressand relaxation, and in particular, the hypothalamic–pituitary–adrenal (HPA) axis (e.g., Refs. 34–37). Ev-idence from music neuroscience and endocrinologysuggests that music may help modulate and reg-ulate these systems (e.g., Refs. 38, 39). This cor-relates well with anecdotal evidence—mostly ob-servation of children’s behavior—from parents andcaregivers conveyed in personal communicationsfrom the field.1
Psychobiological and psychologicalconcerns
It is November 2007, and we drive out to the Pales-tinian West Bank town of Nablus to the southeast,past the Jami’ Al-Kabir Mosque to the Balata refugeecamp. I am traveling with colleagues from the Pales-tinian Union of Social Workers and Psychologists(PUSWP) and with Sheena Boyle from the char-ity Children of Amal. Our objective is to supporta program of therapeutic and educational work forchildren and to offer training to young social work-ers in our methods. During a previous workshopvisit, journalist Donald Macintyre accompanied usand filed the following story.40
The Reid Professor of Music at EdinburghUniversity. . .. is somehow managing simultane-ously to play the guitar, dance, and conduct aclass of 30 children in their lusty performance ofa West African folk song. . . The electricity broughtto this room would be surprising enough even ifit was not happening in the heart of the WestBank’s most populous—and most problematic—Palestinian refugee camp, scene of some of the worstbloodshed during the past six years of conflict.
This is Balata, a stronghold of armed militancy andthe target of at times almost daily Israeli incursions,where 150 Palestinians have been killed since theintifada began six years ago. It is also one of the mostdensely populated places on earth, home to 30,000
civilians who live in less than two square kilometresof cement-block housing packed so closely togetherthat fat people cannot squeeze into some of the alleysbetween them.
He first asks the children to join him in singing amelodic African chant, increasing the volume andthen reducing it to a whisper. Then he has themclap in time. Then he introduces them, still clap-ping, to the rhythm, then, with his guitar, to thetune, and then finally—for those that need it—to thewords of an old Arab song: “Aya Zeyn al-Abidin/IrWrd, Ir Wrd/Imfetah Baynil/Besatin” [“Zeyn alAbidin, you are like a rose that blooms in thegarden.”]
“I have loved Arabic music for a long time, longerthan you!” he tells the children through the inter-preter Assim Eshtaya, 27, a school counsellor inNablus. “I won’t say more, but longer. The notes inthe song we learnt come from a very old traditionalArab scale.” He plays the notes on his guitar. “NowI have a proposal. Would you like to create a newsong with Arabic music?” And so, with ProfessorOsborne allowing the children to decide the wordsof the song. . . and then to choose the melody, noteby note, the song comes into being: “Dear friends,friends for ever, friends for ever,” the whole groupsings in Arabic.
Certainly, the Balata community leaders seem de-lighted with the success of the project. Mrs. Boyle’sJuly training sessions involved 90 children in threeNablus refugee camps—with others having to beturned away. “During the month, the results wereclear for everyone to see,” said Shaer Badawi of Bal-ata’s Yafa centre. “The children were happier.”
On this visit I am keen to widen opportuni-ties for expression and emotional communication.Back in the PUSWP headquarters in Nablus, I runtraining workshops for social workers involvingsimple musical/emotional games: we sit in a cir-cle, half with loud, “angry” instruments (djembes,bongos, and cowbells) and half with gentle sounds(metal chimes, shakers, and crotales). A volunteerin the middle activates the different sound worldsby moving back and forth through the circle—achance to play safely with extremes of aggressiveand caressing sound. I introduce blindfold journeysthrough forests of musical trees, and we invent thesounds of imaginary animals to communicate inthe space—what are these animals, why do theymake this sound, what do they feel, what do theywant to say? Most important of all, we work on
Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences. 71

Music as a therapeutic resource Osborne
co-improvisation—person-to-person exchanges ofmusical empathy, one of the core techniques of clin-ical music therapy—adapted here for more generalprofessional use.
For practitioners, one of the most useful modelsfor reflecting on and developing the psychologicaland psychobiological aspects of the work has beenthe theory of communicative musicality.41 The the-ory has its origins, in part, in the neurosciences andrelated disciplines. Its basis is intersubjectivity in thephenomenological sense,42 and it is promising that aneuroscience of intersubjectivity has recently begunto emerge.43–45
The empirical foundations of communicativemusicality lie in the study of mother–infant vocalcommunication,46–55 which has revealed the rich-ness and significance of the responses of infants—irrespective of culture—to the “prosodic” utterancesof mothers: the sharing of time and intention, emo-tional communication, sympathy, and movement.Research in the affective neuroscience of musicopens up the possibility that this prosodic com-munication may be linked to the activation of avariety of cortical and subcortical neural and neu-roendocrine systems.56–69
The theory of communicative musicality, and itsassociated music neuroscience research, offers toworkers in the field a measure of reassurance (e.g.,confirmation that changes observed in children mayindeed have a basis in science), an opportunity forreflection, and the chance to advance practice. Thetheory further implies that through intersubjec-tivity, empathy, common “musical” emotions, andtheir neural substrates, musical activity may affectthe state of mind and body of those who take part init. From this corpus of literature and personal expe-rience, it is reasonable to propose that children withsymptoms of avoidance, numbing, or hyperarousal(DSM-IV2), or associated feelings of detachment,estrangement, anger, fear, lack of trust, distress, orsimply unhappiness, may indeed (as they and theircarers so often tell us) find a measure of physicaland mental release in joyful shared experiences ofmusical expression.
Psychosocial, social, and biosocialconcerns
It is late June 2010, and I travel to Thailand witha small group of students from Edinburgh to work
on placement with colleagues from Silpakorn Uni-versity, Bangkok. Anothai Nitibhon is a composerand community musician who completed her doc-torate with us at the University of Edinburgh andreturned to Thailand to found a new compositiondepartment and community music course at Sil-pakorn. I am impressed by the way their work hasbeen embraced enthusiastically by communities inmany different parts of Thailand.
Our destination is the South, and the narrow stripof Thai territory that runs between the Myanmar(Burma) border and the South China Sea down tothe Kra Isthmus. These are the districts of PrachuapKhiri Khan, Chumphon, and Ranong, which havebecome in some ways a “no man’s land.” The Britishcolonial period left large populations of ethnic Thaitrapped in Burma, where they have become a signif-icant minority with limited human rights. Over theyears, there has been a slow seepage of populationacross the border to Thailand. There are now about4,700 displaced Burmese Thai in the region, granted“leniency” to live in Thailand, but with no citizen-ship, rights, health care, employment protection, orpermission to travel out of the region. Our project isto try—at their invitation—to help give the youngpeople a voice.
Our first stop is Klong Loi, a small village thatsurvives in dignified poverty, a bitter sweet par-adise, surrounded by banana trees, long kong,and abruptly rising hillsides of tropical forest.Rachel Bradley, a postgraduate student from Ed-inburgh, takes up the story in her paper “No man’sband” (R. Bradley, Univ. of Edinburgh, in prep.).
In the community hall, a large open concrete plat-form with a stage and a roof supported by pillarsto allow the breeze to blow in from the moun-tains, a group of teenagers (dressed like teenagerseverywhere) congregates for the project. Onlookersgather as the group begins warm up games, dancesand songs. The young people participate with ap-prehension at first, but quickly come to speak, laughand gain confidence.. . .
They are invited to talk about their lives in the dis-placed community. They describe what they wouldlike to say to other teenagers living legally in Thai-land, and many speak of what they would like to bewhen they are older. . .a painter, teacher, Thai boxer,tour guide, rapper, husband.
Inspired by these conversations they split intosmaller groups to compose songs with the support
72 Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences.

Osborne Music as a therapeutic resource
of the student volunteers and their respective instru-ments. Participants are offered notes to choose from(from the traditional scales of Thai music); they as-semble the notes of the melody one by one.. . .
The songs are a fascinating mixture of styles, in-cluding traditional, folk, pop, and rap. Interestingly,all melodies scrupulously respect the contours ofthe five tones of the Thai language—low, mid, high,falling, or rising—a discipline now lost in muchThai popular music. The words of the songs aretouching, more a gentle cri de coeur than agitationpropaganda.
. . .. Many times we have been hurtFelt confused and don’t know where to turnLike the long kong fruit we come and we goAnd give the long kong branch to showThat we would like to be its friendBut now we just don’t see an endSo if some day you think about usWe are here, still waiting for you.
The workshop culminates in performances in thevillage and the local school. Our objectives here areto offer the children a positive, collective musicalexperience; an opportunity to build creativity, self-respect, and a sense of identity; and the chance totell their story and to use the social power of mu-sic to raise awareness of their situation in a widerworld.
There are many areas of psychosocial and socialintervention among both postconflict and displacedpopulations where music has proven to be an agentof change.70–72 Its potential usefulness in the psy-chosocial domain begins with relaxation, joy, andtrust and progresses to individual creativity, self-expression, self-belief, and self-respect. At the sociallevel, music may be effective in facilitating socialcommunication, collective creativity, and, as in thecase of Klong Loi, the expression of social iden-tity. In situations where populations have been di-vided by conflict, for example, in postwar Bosnia–Hercegovina, music and the creative arts mayprovide a mutually acceptable meeting point innormality. It is rarely possible to “reconcile” peo-ple. But music making is a safe place for people to“be” together and rebuild trust how and when theychoose. In postconflict areas, music has been ef-fective beyond the biopsychosocial paradigm in thedomains of politics and economics, as, for exam-ple, the music-based social reconstruction programin Srebrenica, or new arts-based economic initia-
tives in East Africa (e.g., the work of the RuwenzoriFoundation in Uganda).
All of this may seem very far from the world ofmusic neuroscience; certainly there has been littlecrossover so far into postconflict social intervention.Yet, social neuroscience is a dynamically expand-ing field,73–80 and an overlap of research interestswith music neuroscience has already occurred—forexample, in the neuroscience of intersubjectivity(see above), and in the work of Overy and Molnar–Szakacs, whose shared affective motion experience(SAME) model of emotional responses to music81,82
proposes a shared, deep apprehension, beyond sim-ple hearing, of the human, expressive origins of mu-sical sound. Their suggested co-occurence of motor,emotional, and social responses to music certainlyhelps to explain the power and importance of groupwork in our activities with traumatized children.This leads the way back around the biopsychoso-cial circle, through issues of synchronization (e.g.,in joy in making music and movement together), tothe biosocial and biological starting points of thisframework.
It seems clear that the circle itself may representa continuity, synergy, and synchronicity of biologi-cal, psychological, and social concerns active in po-tentially therapeutic, rehabilitational, and sociallyreparative musical processes.
Conflicts of interest
The author declares no conflicts of interest.
References
1. Osborne, N. 2009. Music for children in zones of conflictand post-conflict: a psychobiological approach. In Com-municative Musicality. S. Malloch & C. Trevarthen, Eds.:331–356. Oxford University Press. New York.
2. American Psychiatric Association. 1994. Diagnostic and Sta-tistical Manual of Mental Disorders. 4th Ed. APA. Washing-ton, DC.
3. AfricanColours. 2008. Art saved my life - PeterOloya. URL http://www.africancolours.com/african-art-news/38/uganda/art saved my life - peter oloya.htm [ac-cessed on 9 February 2012].
4. Cohen, H., M. Kotler, M.A. Matar, et al. 1998. Analysis ofheart rate variability in posttraumatic stress disorder pa-tients in response to a trauma-related reminder. Biol. Psy-chiatry 44: 1054–1059.
5. Cohen, H., J. Benjamin, A.B. Geva, et al. 2000. Autonomicdysregulation in panic disorder and in post-traumatic stressdisorder: application of power spectrum analysis of heartrate variability at rest and in response to recollection oftrauma or panic attacks. Psychiatry Res. 96: 1–13
Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences. 73

Music as a therapeutic resource Osborne
6. Buckley, T.C. & D.G. Kaloupek. 2001. A meta-analytic ex-amination of basal cardiovascular activity in posttraumaticstress disorder. Psychosom. Med. 63: 585–594.
7. Beckham, J.C., S.R. Vrana, J.C. Barefoot, et al. 2002.Magnitude and duration of cardiovascular responsesto anger in Vietnam veterans with and without post-traumatic stress disorder. J. Consult. Clin. Psychol. 70:228–234.
8. Forneris, C.A., M.I. Butterfield & H.B. Bosworth. 2004.Physiological arousal among women veterans with andwithout posttraumatic stress disorder. Mil. Med. 169: 307–312.
9. Buckley, T.C., D. Holohan, J.L. Greif, et al. 2004. Twenty-four-hour ambulatory assessment of heart rate and bloodpressure in chronic PTSD and non-PTSD veterans. J.Trauma. Stress 17: 163–171.
10. Kibler, J.L. & J.A. Lyons. 2004. Perceived coping ability me-diates the relationship between PTSD severity and heart raterecovery in veterans. J. Trauma. Stress 17: 23–29.
11. Updike, P.A. & D.M. Charles. 1987. Music Rx: physiologicaland emotional responses to taped music programs of preop-erative patients awaiting plastic surgery. Ann. Plast. Surg. 19:29–33.
12. Iwanaga, M. & M. Tsukamoto. 1997. Effects of excitative andsedative music on subjective and physiological relaxation.Percept. Mot. Skills 85: 287–296.
13. Byers, J.F. & K.A. Smyth. 1997. Effect of a musical inter-vention on noise annoyance, heart rate, and blood pres-sure in cardiac surgery patients. Am. J. Crit. Care 6: 183–191.
14. Gerra, G., A. Zaimovic, D. Franchini, et al. 1998. Neuroen-docrine responses of healthy volunteers to ‘techno-music’:relationships with personality traits and emotional state.Int. J. Psychophysiol. 28: 99–111
15. Cardigan, M.E., N.A. Caruso, S.M. Haldeman, et al. 2001.The effects of music on cardiac patients on bed rest. Prog.Cardiovasc. Nurs. 16: 5–13.
16. Knight, W.E. & N.S. Rickard. 2001. Relaxing music preventsstress-induced increases in subjective anxiety, systolic bloodpressure and heart rate in healthy males and females. J. MusicTher. 38: 254–272.
17. Aragon, D., C. Farris & J.F. Byers. 2002. The effects of harpmusic in vascular and thoracic surgical patients. Altern.Ther. Health Med. 8: 52–54, 56–60.
18. Mok, E. & K.Y. Wong. 2003. Effects of music on patientanxiety. AORN J. 77: 396–397, 401–406, 409–410.
19. Lee, O.K., Y.F. Chung, M.F. Chan & W.M. Chan. 2005. Musicand its effect on the physiological responses and anxietylevels of patients receiving mechanical ventilation: a pilotstudy. J. Clin. Nurs. 14: 609–620.
20. Iwanaga, M., A. Kobayashi, C. Kawasaki. 2005. Heart ratevariability with repetitive exposure to music. Biol. Psychol.70: 61–66.
21. Sahar, T., A.Y. Shalev & S.W. Porges. 2001. Vagal modulationof responses to mental challenge in posttraumatic stressdisorder. Biol. Psychiatry 49: 637–643.
22. Donker, G.A., C.J. Yzermans, P. Spreeuwenberg & J. Van derZee. 2002. Symptom attribution after a plane crash: com-parison between self-reported symptoms and GP records.Brit. J. Gen. Pract. 52: 917–922.
23. Sack, M., J.W. Hopper & F. Lamprecht. 2004. Low respira-tory sinus arrhythmia and prolonged psychophysiologicalarousal in posttraumatic stress disorder: heart rate dynam-ics and individual differences in arousal regulation. Biol.Psychiatry 55: 284–290.
24. Nixon, R.D. & R.A. Bryant. 2005. Induced arousal and re-experiencing in acute stress disorder. J. Anxiety Disord. 19:587–594.
25. Fried, R. 1990. Integrating music in breathing training andrelaxation: I. Background, rationale and relevant elements.Biofeedback Self Regul. 15: 161–169.
26. Fried, R. 1990. Integrating music in breathing training andrelaxation: II. Applications. Biofeedback Self Regul. 15: 171–177.
27. Bernardi, L., C. Porta & P. Sleight. 2006. Cardiovascular,cerebrovascular and respiratory changes induced by differ-ent types of music in musicians and non-musicians: theimportance of silence. Heart 92: 445–452.
28. McCoy, S.J. 2004. Your Voice: An Inside View—MultimediaVoice Science and Pedagogy. Inside View. Delaware, OH.
29. Yule, W. 1994. Posttraumatic Stress Disorder. Plenum. NewYork.
30. Brent, D.A., J.A. Perper, G. Moritz, et al. 1995. Posttraumaticstress disorder in peers of adolescent suicide victims: pre-disposing factors and phenomenology. J. Am. Acad. ChildAdolesc. Psychiatry 34: 209–215.
31. Famularo, R., T. Fenton, R. Kinscherff & M. Augustyn. 1996.Psychiatric comorbidity in childhood post traumatic stressdisorder. Child Abuse Negl. 20: 953–961.
32. Adler, L.A., M. Kunz, H.C. Chua, et al. 2004. Attention-deficit/hyperactivity disorder in adult patients with post-traumatic stress disorder (PTSD): is ADHD a vulnerabilityfactor? J. Atten. Disord. 8: 11–16.
33. Osborne, N. 2009. Towards a chronobiology of musicalrhythm. In Communicative Musicality. S. Malloch & C.Trevarthen, Eds.: 545–564. Oxford University Press.New York.
34. Goenjian, A.K., R. Yehuda, R.S. Pynoos, et al. 1996. Basalcortisol, dexamethasone suppression of cortisol and MHPGin adolescents after the 1988 earthquake in Armenia. Am. J.Psychiatry 153: 929–934.
35. Yehuda, R. 2000. Neuroendocrinology. In Post-TraumaticStress Disorder, Diagnosis, Management and Treatment . D.Nutt, J.R.T. Davidson & J. Zohar, Eds.: 1–260. MartinDunitz. London.
36. Rasmusson, A.M., M. Vythilingam & C.A. Morgan. 2003.The neuroendocrinology of posttraumatic stress disorder:new directions. CNS Spectr. 8: 651–656, 665–667.
37. Delahanty, D.L., N.R. Nugent, N.C. Christopher & M.Walsh. 2005. Initial urinary epinephrine and cortisol lev-els predict acute PTSD symptoms in child trauma victims.Psychoneuroendocrinology 30: 121–128.
38. Miluk-Kolasa, B., Z. Obminski, R. Stupnicki & L. Golec.1994. Effects of music treatment on salivary cortisol in pa-tients exposed to pre-surgical stress. Exp. Clin. Endocrinol.102: 118–120.
39. Uedo, N., H. Ishikawa, K. Morimoto, et al. 2004. Reductionin salivary cortisol level by music therapy during colono-scopic examination. Hepato-Gastroenterology 51: 451–453.
74 Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences.

Osborne Music as a therapeutic resource
40. Macintyre, D. 2006. Music therapy: the pied piper of Balata.The Independent (UK), October 30, 2006.
41. Malloch, S. & C. Trevarthen, Eds. 2009. CommunicativeMusicality. Oxford University Press. New York.
42. Trevarthen, C. & K.J. Aitken. 2001. Infant intersubjectivity:research, theory and clinical applications. J. Child Psychol.Psychiatry 42: 3–48.
43. Dumas, G., J. Nadel, R. Soussignan, et al. 2010. Inter-brain sychronization during social interaction. PloS ONE 5:e12166.
44. Redcay, E., D. Dodell-Feder, M.J. Pearroe, et al. 2010.Live face-to-face Interaction during fMRI: a new toolfor social cognitive neuroscience. Neuro Image 50: 1639–1647.
45. Guionnet, S., J. Nadel, E. Bertasi, et al. 2011. Reciprocalimitation: toward a neural basis of social interaction. Cereb.Cortex22: 917–918.
46. Stern, D.N. 1974. Mother and infant at play: the dyadicinteraction involving facial, vocal and gaze behaviours. InThe Effect of the Infant on its Caregiver. M. Lewis & L.A.Rosenblum, Eds.: 187–213. Wiley. New York.
47. Alegria, J. & E. Noirot. 1978. Neonate orientation be-haviour towards the human voice. Early Hum. Dev. 1: 291–312.
48. Bullowa, M., Ed. 1979. Before Speech: The Beginning of Hu-man Communication. Cambridge University Press. Cam-bridge, UK.
49. DeCasper, A.J. & W.P. Fifer. 1980. Of human bonding:newborns prefer their mothers’ voices. Science 208: 1174–1176.
50. Fernald, A. 1985. Four-month-old infants prefer to listen tomotherese. Infant Behav. Dev. 8: 181–195.
51. Papousek, M. 1987. Models and messages in the melodiesof maternal speech in tonal and non-tonal languages. Abstr.Soc. Res. Child Dev. 6: 407.
52. Trehub, S.E. 1987. Infants’ perception of musical patterns.Percept. Psychophys. 41: 635–641.
53. Papousek, M. 1992. Early ontogeny of vocal communica-tion in parent-infant interactions. In Nonverbal Vocal Com-munication, Comparative and Developmental Approaches.H. Papousek, U. Jurgens & M. Papousek, Eds.: 230–261.Cambridge University Press. Cambridge, UK.
54. Masataka, N. 1993. Relation between pitch contour ofprelinguistic vocalisations and communicative functions inJapanese infants. Infant Behav. Dev. 16: 397–401.
55. Kuhl, P.K., J.E. Andruski, I.A. Chistovich, et al. 1997. Cross-language analysis of phonetic units in language addressedto infants. Science 277: 684–686.
56. Goldstein, A. 1980. Thrills in response to music and otherstimuli. Physiol. Psychol. 3: 126–129.
57. Panksepp, J. 1998. The periconscious substrates of con-sciousness. Affective states and evolutionary origins of theSELF. J. Conscious. Stud. 5: 566–582.
58. Blood, A.J., R.J. Zatorre, P. Bermudez & A.C. Evans. 1999.Emotional responses to pleasant and unpleasant music cor-relate with activity in paralimbic regions. Nature Neurosci.2: 322–327.
59. Pratt, R.R. & D.E. Grocke, Eds. 1999. MusicMedicine – MusicMedicine and Music Therapy: Expanding Horizons. Vol. 3.MMB Music. St. Louis, MO.
60. Blood, A.J. & R.J. Zatorre. 2001. Intensely pleasurable re-sponses to music correlate with activity in brain regionsimplicated in reward and emotion. Proc. Natl. Acad. Sci.USA 98: 11818–11823.
61. Kreuz, G., S. Bongard, S. Rohrmann, et al. 2004. Effectsof choir singing or listening on secretory immunoglobulinA, cortisol, and emotional state. J. Behav. Med. 27: 623–635.
62. Stefano, G.B., W. Zhu, P. Cadet, et al. 2004. Music altersconstitutively expressed opiate and cytokine processes inlisteners. Med. Sci. Monit. 10: MS18–MS27.
63. Menon, V. & D.J. Levitin. 2005. The rewards of musiclistening: response and physiological connectivity of themesolimbic system. Neuro Image 28: 175–184.
64. Craig, D.G. 2005. An exploratory study of changesduring chills induced by music. Musicae Scientiae 9:273–287.
65. Alcaro, A., R. Huber & J. Panksepp. 2007. Behavioral func-tions of the mesolimbic dopaminergic system: an affec-tive neuroethological perspective. Brain Res. Rev. 56: 283–321.
66. Klockars, M. & M. Peltomaa. 2007. Music Meets Medicine.Acta Gyllenbergiana VII . The Signe and Ane GyllenbergFoundation. Helsinki, Finland.
67. Grewe, O., E. Magel, R. Kopiez & E. Altenmuller. 2007.Listening to music as a re-creative process: physiological,psychological, and psychoacoustical correlates of chills andstrong emotions. Music Percept. 24: 297–314.
68. Guhn, M., A. Hamm & M. Zentner. 2007. Physiologicaland musico-acoustic correlates of the chill response. MusicPercept. 24: 170–180.
69. Panksepp, J. & C. Trevarthen. 2009. The neuroscience ofemotion in music. In Communicative Musicality. S. Malloch,C. Trevarthen, Eds.: 105–146. Oxford University Press. NewYork.
70. Urbain, O., Ed. 2007. Music and Conflict Transformation:Harmonies and Dissonances in Geopoilitics. I.B. Tauris.London.
71. O’Connell, J. & S.E.-S. Castelo-Branco. 2010. Music andConflict . University of Illinois Press. Champaign, IL.
72. Robertson, C. 2010. Music and conflict transformation inBosnia: constructing and reconstructing the normal. MusicArts Action 2: 2.
73. Cacioppo, J.T. 2002. Social neuroscience: understanding thepieces fosters understanding the whole and vice versa. Am.Psychologist 57: 819–831.
74. Brune, M., H. Ribbert & W. Schiefenhovel. 2003. TheSocial Brain: Evolution and Pathology. Wiley & Sons.Hoboken, NJ.
75. Cacioppo, J. T. & G.G. Berntson. 2004. Social Neuroscience:Key Readings. Psychology Press. East Sussex, UK.
76. Wolpert, D. & C. Frith. 2004. The Neuroscience of SocialInteractions: Decoding, Influencing, and Imitating the Actionsof Others. Oxford University Press. New York.
77. Cozolino, L. 2006. The Neuroscience of Human Relation-ships: Attachment and the Developing Social Brain. W. W.Norton. New York.
78. de Haan, M. & M.R. Gunnar. 2009. Handbook of De-velopmental Social Neuroscience. Guilford Press. NewYork.
Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences. 75

Music as a therapeutic resource Osborne
79. Decety, J. & W. Ickes. 2009. The Social Neuroscience of Em-pathy. MIT Press. Cambridge, MA.
80. Decety, J. & J.T. Cacioppo. 2011. Handbook of Social Neuro-science. Oxford University Press. New York.
81. Molnar-Szakacs, I. & K. Overy. 2006. Music and mirror neu-
rons: from motion to ‘e’motion. Soc. Cogn. Affect. Neurosci.1: 235–241.
82. Overy, K. & I. Molnar-Szakacs. 2009. Being together intime: musical experience and the mirror neuron system.Music Percept. 26: 489–504.
76 Ann. N.Y. Acad. Sci. 1252 (2012) 69–76 c© 2012 New York Academy of Sciences.