Neuropsychological performance predicts clinical recovery in bipolar patients
8
Brief report Neuropsychological performance predicts clinical recovery in bipolar patients Staci A. Gruber ⁎ , Isabelle M. Rosso, Deborah Yurgelun-Todd Cognitive Neuroimaging Laboratory, Brain Imaging Center, McLean Hospital, and Department of Psychiatry, Harvard Medical School, 115 Mill Street, Belmont, MA 02478, USA Received 6 October 2006; received in revised form 30 March 2007; accepted 18 April 2007 Available online 23 May 2007 Abstract Background: Although a number of investigations have reported cognitive deficits in patients with bipolar disorder, relatively few have focused on the relationship between these impairments and clinical outcome. Methods: In order to help clarify the pattern of and extent to which cognitive deficits are present at the onset of illness and their relationship to outcome, we examined 26 bipolar patients during their first hospitalization and 20 psychiatrically healthy control subjects. All subjects completed tests of frontal/executive control, psychomotor speed and memory function at baseline and self- reports of clinical recovery (time to recover in days) at 12 months post study enrollment. Results: At baseline, first episode bipolar patients demonstrated greater deficits relative to control subjects on neurocognitive measures, and a significant association was detected between time to recover and performance on a measure of frontal/executive function (interference condition of the Stroop; p = .05; derived interference: p = .04). A trend towards significance was also demonstrated between time to clinical recovery and verbal fluency ( p = .06). Conclusions: These findings indicate that neuropsychological deficits are seen early in the course of bipolar disorder, prior to the effects of multiple or prolonged episodes, and may be associated with clinical outcome. Future studies are needed to determine whether changes in inhibitory processing or other cognitive function predict clinical outcome or are associated with treatment response. © 2007 Elsevier B.V. All rights reserved. Keywords: Bipolar; Neurocognition; Recovery; Inhibitory function; Stroop 1. Introduction Bipolar disorder has been associated with significant and often persistent impairment in cognitive function (Altshuler, 1993) however, the relationship of these cognitive deficits to clinical outcome has not been well documented. Several investigations have reported cognitive deficits which are suggestive of impairments in executive function, attention, memory and psycho- motor speed (Gourovitch et al., 1999; Dupont et al., 1995), yet relatively little research has focused on how these deficits relate to course of illness. It has been hypothesized that the cognitive deficits present in patients with bipolar disorder are due to residual effects caused by repeated or prolonged affective episodes, however, it is possible that these functional changes represent core features of the illness (Nordenson et al., 2004). Moreover, some studies have reported a progressive decline in cognitive performance over time while others have not, raising the question of whether these deficits are present at the onset of the illness (Altshuler, 1993). Several Journal of Affective Disorders 105 (2008) 253 – 260 www.elsevier.com/locate/jad ⁎ Corresponding author. Tel.: +1 617 855 2762; fax: +1 617 855 3713. E-mail address: [email protected] (S.A. Gruber). 0165-0327/$ - see front matter © 2007 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2007.04.014
-
Upload
staci-a-gruber -
Category
Documents
-
view
219 -
download
0
Transcript of Neuropsychological performance predicts clinical recovery in bipolar patients

Journal of Affective Disorders 105 (2008) 253–260www.elsevier.com/locate/jad
Brief report
Neuropsychological performance predicts clinical recovery inbipolar patients
Staci A. Gruber ⁎, Isabelle M. Rosso, Deborah Yurgelun-Todd
Cognitive Neuroimaging Laboratory, Brain Imaging Center, McLean Hospital, and Department of Psychiatry, Harvard Medical School,115 Mill Street, Belmont, MA 02478, USA
Received 6 October 2006; received in revised form 30 March 2007; accepted 18 April 2007Available online 23 May 2007
Abstract
Background: Although a number of investigations have reported cognitive deficits in patients with bipolar disorder, relatively fewhave focused on the relationship between these impairments and clinical outcome.Methods: In order to help clarify the pattern of and extent to which cognitive deficits are present at the onset of illness and theirrelationship to outcome, we examined 26 bipolar patients during their first hospitalization and 20 psychiatrically healthy controlsubjects. All subjects completed tests of frontal/executive control, psychomotor speed and memory function at baseline and self-reports of clinical recovery (time to recover in days) at 12 months post study enrollment.Results: At baseline, first episode bipolar patients demonstrated greater deficits relative to control subjects on neurocognitivemeasures, and a significant association was detected between time to recover and performance on a measure of frontal/executivefunction (interference condition of the Stroop; p=.05; derived interference: p=.04). A trend towards significance was alsodemonstrated between time to clinical recovery and verbal fluency ( p=.06).Conclusions: These findings indicate that neuropsychological deficits are seen early in the course of bipolar disorder, prior to theeffects ofmultiple or prolonged episodes, andmay be associatedwith clinical outcome. Future studies are needed to determinewhetherchanges in inhibitory processing or other cognitive function predict clinical outcome or are associated with treatment response.© 2007 Elsevier B.V. All rights reserved.
Keywords: Bipolar; Neurocognition; Recovery; Inhibitory function; Stroop
1. Introduction
Bipolar disorder has been associated with significantand often persistent impairment in cognitive function(Altshuler, 1993) however, the relationship of thesecognitive deficits to clinical outcome has not been welldocumented. Several investigations have reportedcognitive deficits which are suggestive of impairmentsin executive function, attention, memory and psycho-
⁎ Corresponding author. Tel.: +1 617 855 2762; fax: +1 617 855 3713.E-mail address: [email protected] (S.A. Gruber).
0165-0327/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jad.2007.04.014
motor speed (Gourovitch et al., 1999; Dupont et al.,1995), yet relatively little research has focused on howthese deficits relate to course of illness. It has beenhypothesized that the cognitive deficits present in patientswith bipolar disorder are due to residual effects caused byrepeated or prolonged affective episodes, however, it ispossible that these functional changes represent corefeatures of the illness (Nordenson et al., 2004). Moreover,some studies have reported a progressive decline incognitive performance over time while others have not,raising the question of whether these deficits are presentat the onset of the illness (Altshuler, 1993). Several

254 S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
investigations have reported that bipolar patients with amore severe course of illness and higher numbers ofaffective episodes experience greater cognitive decre-ments (van Gorp et al., 1998; Kessing, 1998; Denicoffet al., 1999), and that specific variables including age ofonset, duration of illness and number of hospitalizationsare associated with this neurocognitive profile. Given theimportance of understanding the relationship betweenclinical symptoms and cognition to assess the potentiallypredictive value of cognitive variables with regard tofunctional recovery, recent studies have begun to ex-amine neuropsychological performance of bipolar pa-tients at variable points in their illness.
In an investigation by Rubinsztein et al. (2000),investigators compared the performance of 14 bipolarpatients in full or partial remission to that of 12 healthycontrol subjects on a battery of neurocognitive tests,which included a pattern and spatial recognition task, adelayed matching to sample task, and the One TouchTower of London task, a spatial problem solving task(Elliott et al., 1996). Euthymic bipolar patients per-formed significantly worse on both the pattern andspatial recognition tasks as compared to controls andmade more errors on the delayed matching to sampletask. Performance was significantly correlated with totalnumber of months of hospitalization, underscoring theimportance of examining the associations betweenclinico-demographic factors and neurocognitive vari-ables. In a study designed to assess the relationshipbetween course of illness and neurocognitive function,Denicoff et al. (1999) examined 49 bipolar outpatientsusing a battery of tests, which included measures ofinhibitory function (Stroop), verbal fluency (ControlledOral Word Association Test [COWAT]), verbal learningand memory (California Verbal Learning Test [CVLT]),attention/vigilance (Continuous Performance Test[CPT]), psychomotor speed (Grooved Pegboard), exec-utive function (Wisconsin Card Sorting Test [WCST])and visual scanning/set maintenance (Letter Cancella-tion Test [LCT]). The authors reported that duration ofsymptoms was significantly predictive of the number ofperseverative responses on the CVLT, total response timeand number correct on the CPT, and performance on theLCT. Similarly, Zubieta et al. (2001) observed a negativecorrelation between executive function as measured bytheWCST, and the number of past affective episodes andhospitalizations due to mania in bipolar I subjects. In astudy by Lebowitz et al. (2001) bipolar patients with ahistory of multiple manic episodes generated signifi-cantly fewer words on a phonemic fluency task andmademore errors on phonemic and semantic verbal fluencytasks than patients experiencing their first manic episode
and healthy controls. Other investigations have reportedinverse correlations between sustained attention andnumber of affective episodes and hospitalizations (Clarket al., 2001). Psychomotor speed has also been shown tobe associated with number of past depressive episodes(MacQueen et al., 2001). In a study of euthymic bipolarpatients, El-Badri et al. reported that the while totalnumber of affective episodes was significantly related tocognitive impairment in multiple domains, no significantassociation was detected between cognitive performanceand duration of illness or age of onset (El-Badri et al.,2001). In a recent study by Frangou et al. (2005),remitted bipolar patients showed impairment on a rangeof tasks requiring executive function relative to controlsubjects and found that duration of illness predicted lossof inhibitory control (Frangou et al., 2005). Finally,Nehra et al. examined cognitive performance in a groupof euthymic bipolar patients following their first episoderelative to euthymic multiple episode bipolar patientsand control subjects (Nehra et al., 2006). While the studyreported that overall, first episode patients performedmore poorly than multiple episode patients or controls,multiple episode patients demonstrated significantlyworse performance on a subtest of executive functions,specifically perseverative errors on the WCST task, thaneither of the other two groups. Further, multiple episodepatients also achieved lower overall scores on a memoryscale than the other groups, raising the question ofprogressive cognitive impairment with repeated clinicalepisodes.
These investigations indicate a significant relation-ship between neurocognitive impairments and clinicalvariables, including frequency of affective episodes andnumber of hospitalizations. No study thus far has ex-amined patients during their first hospitalization todocument prospectively the relationship between neu-rocognitive performance and recovery. We examinedbipolar patients during their first hospitalization, andhypothesized that compared to normal control subjects,even after becoming clinically stable, these patientswould show deficits on neuropsychological tests sen-sitive to executive function. Further, it was hypothesizedthat that deficits in cognitive performance would bepredictive of clinical recovery, therefore, we examinedthe extent to which performance on these measures wasrelated to rehospitalization status and time to recover (indays) at 12 months post study enrollment.
2. Methods
Forty six subjects were enrolled in this neuropsy-chological protocol which included 26 patients admitted

255S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
to McLean Hospital for their first episode of bipolardisorder and 20 non-psychiatric control subjects,matched for age, sex, handedness and parental socio-economic status (SES), recruited from the community.All subjects completed a structured clinical interview(SCID-P) to ensure accurate diagnoses as well asclinical rating scales to characterize the phase of theirillness. These were administered by an experiencedclinical interviewer with an established good inter-raterreliability (kappa N .90). Control subjects were free ofAxis I pathologies and had no first degree relatives withany Axis I diagnosis. All subjects were native Englishspeakers, and had no history of head trauma, alcohol orsubstance dependence. A neurocognitive test battery,which included tests of frontal/executive control wasadministered to each study subject, and for the bipolarpatients, within 1 week of admission. All subjectssigned an Informed Consent form approved by theMcLean Hospital Institutional Review Board.
The neuropsychological tests were chosen becausethey are standard, well-known measures which can beadministered and scored reliably, and have provensensitive to frontal-lobe dysfunction (Lezak, 2004).The Stroop Color–Word Test (Stroop, 1935) measuresthe ability to inhibit inappropriate responses and resistinterference and includes three sections (color naming,word reading and interference). The task is designed toestablish competing response tendencies within thestudy subject and to assess the subjects' ability tosuppress the interfering stimuli (Comalli et al., 1962;Lezak, 2004). The Trail Making Test is a visualconceptual and visuomotor tracking task and involvesfirst connecting consecutively numbered circles on onework sheet (Part A) and then connecting the samenumber of consecutively numbered and lettered circleson another work sheet by alternating between the twosequences (Part B). Trails B is the more sensitive of thetwo tests, particularly to frontal-lobe dysfunction, asscores on this section are indicative of the subject'sability to shift sets and process concurrent stimuli(Reitan, 1958; Lezak, 2004). The Wisconsin CardSorting Test assesses a person's ability to form abstractconcepts, utilize feedback, and to shift and maintain set.In the Controlled Oral Word Association (FAS) test,subjects are asked to generate as many different words aspossible that begin with a particular letter during a 1 minperiod. Three letters are used in succession (F, A, S); thetotal number of words generated for all three letterscomprises the verbal fluency score. Finally, subjectscompleted the Vocabulary subtest of the Wechsler AdultIntelligence Scale-Revised (WAIS-R) as a measureof general intellectual ability (Wechsler, 1981). The
Vocabulary subtest has been identified as the single bestmeasure of both verbal and general mental ability(Lezak, 2004; Spreen and Strauss, 1991). All testswere administered by a trained psychometrician blind tosubjects' diagnostic group.
At the time of neuropsychological evaluation, firsthospitalized bipolar patients had received no more than2 weeks of pharmacologic treatment, and most wereseen within 1 week of entering the hospital. All subjectsagreed to be enrolled in a naturalistic, longitudinal studywhich required patients to be evaluated at monthly in-tervals. At 12 months post study enrollment, first epi-sode patients completed a second clinical interview (toconfirm diagnosis) and provide information regardingclinical state and recovery.
2.1. Statistical analyses
We examined differences in neuropsychologicalfunctioning between bipolar patients and healthycontrols using one-tailed Student's t-tests (as thedirection of the group differences were hypothesized apriori); to account for multiple comparisons we used aBonferroni adjusted significance level, one-tailed, of.005. Neuropsychological test scores found to differsignificantly between the groups were entered asdependent variables in analyses of covariance (ANCO-VAs) that included age, sex and education as covariates.Finally, to examine the association of neuropsycholog-ical functioning and clinical outcome (time to recovery),we used Spearman's Rho correlations. Variables thatdeparted significantly from a Gaussian distribution werelog-transformed.
3. Results
Demographic characteristics for the study subjectsare listed in Table 1. The study groups were matched forparental socioeconomic status, age and sex, however,bipolar patients completed slightly fewer years of edu-cation compared to control subjects (14.0 vs. 15.8,p=.01). With regard to estimated intellectual function,bipolar patients performed in the high average range(VIQ=108.4) while normal controls achieved scores inthe superior range (VIQ=120.9), yielding a significantbetween-group difference (p= .02). Given that pa-tients were evaluated within the first 2 weeks of theirhospitalization, and that scores may reflect elements ofthe current clinical state, a correction for VIQ was notincluded in the current data. Additionally, the primaryoutcome variable in this study is the relationship be-tween neurocognitive performance and recovery within

Table 2Neuropsychological measures of executive functioning in first episodebipolar patients and healthy controls
Frontal-executive task
Bipolar patientsN=26 mean±SD
Healthy subjectsN=20 mean±SD
p-value⁎
(t-test)
Trail making (seconds)Trails, PartA 44.0±14.2 32.5±9.8 .003Trails, Part B 64.8±28.1 44.7±14.1 .005Trails B–A 21.1±19.1 12.3±8.9 .48
Stroop Color–Word Test (seconds)Color naming 69.4±15.0 56.7±9.6 .002Word reading 48.1±9.7 43.6±6.6 .09Interference 120.4±32.4 100.8±22.7 .02Derived interference 51.0±21.5 44.1±17.6 .29
Wisconsin Card Sorting TestTotal categories 7.0±1.7 8.7±1.3 b .001Total perseverations 17.2±11.4 7.1±5.1 b .001
Verbal fluencyTotal words 40.1±10.0 47.3±13.6 .05
⁎p-values are one-tailed; those that remained significant afterBonferroni correction are printed in bold.
Table 1Demographic and clinical features in first episode bipolar patients andhealthy comparison subjects (mean±SD or N(%))
Variable Healthy controls(N=20)
Bipolar patients(N=26)
Age (years) 25.3±4.7 24.4±5.5Sex (male) 15 (75) 19 (73)Education 15.8±2.1 14.0±2.3⁎
Handedness (right) 19 (95) 24 (92)Estimated VIQ 120.9±16.3 108.7±18.2⁎
Age of onset (years) – 23.8±5.0Duration of illness (days) – 26.2 ±2.9
⁎pb .05.
256 S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
the patient cohort, which would not be affected by abetween-group correction for IQ.
Table 2 shows the results of the t-tests of groupdifferences. First hospitalized bipolar patients demon-strated significantly poorer performance on Trail MakingTest, Part A, a test of psychomotor speed, than controlsubjects (p=.003). Patients also performed more poorlythan controls on the Trail Making Test Part B, which hasan additional requirement of maintaining and shifting ofmental set (p=.005). Both these group differences sur-vived Bonferroni correction. Subtraction of the time tocomplete Trails A from the time to complete Trails Bwas calculated to examine the latency effect of shiftingset. This score was not significantly different betweengroups.
On the Stroop Color–Word Test, bipolar patientsperformed significantly slower on all three conditions(Color Naming, Word Reading, and Interference) relativeto control subjects, although only the group difference inColor Naming remained significant after Bonferronicorrection (p=.002). To better isolate inhibitory capacityfrom psychomotor speed, we also calculated a derivedinterference score (Interference score minus ColorNaming score), but this score did not differ significantlybetween groups. On the Wisconsin Card Sorting Test(WCST), a test of abstraction and the ability to shiftmental set, first hospitalized patients achieved fewer totalcategories than control subjects, a difference that was stillsignificant with Bonferroni correction (pb .001). Interest-ingly, after a clarification of the rules, no significant dif-ferences were detected between the groups, indicatingthat first hospitalized patients were able to utilize feed-back to improve their performance. Total number of per-severations on the WCST also differed between thegroups, with first hospitalized bipolar subjects makingsignificantly more errors than control subjects at theadjusted Bonferroni level (pb .001).
To examine potential confounds of demographicvariables on the above group differences, we conductedANCOVAs predicting each of the five neuropsycholog-ical test scores that survived Bonferroni correction, withsex, age and education as covariates. None of thesedemographic variables were significantly associated withStroop Color Naming, total categories on theWCST, totalperseverations on the WCST, or time to complete TrailsA or B.
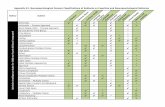
For the analyses examining neuropsychologicalfunctioning in relation to clinical outcome, “time torecovery” was defined as the number of days requiredfor the patient to return to a baseline level of function,which was assessed using self-report data collected at12 months post study enrollment. At the one year postdischarge time point, bipolar patients completed com-prehensive clinical follow-up interviews in the labora-tory or by telephone. As shown in Fig. 1, a significantassociation was detected between time to recovery andthe score on the Interference condition of the Stroop test(rs= .48; p=.05), as well as for the derived Interferencescore (rs= .51; p=.04). A strong but not statisticallysignificant negative correlation was found betweenrecovery and the verbal fluency score (rs =− .47;p=.06). Finally, age at onset and length of illness werenot significantly correlated with time to recovery, norwere they significantly associated with the Stroop scores.Thus, the correlations between time to recovery and

Fig. 1. Time to recovery was defined as the number of days required for the patient to return to a baseline of function, which was assesed via self-report collected at 12 month post study enrollment. A significant association was detected between time to recovery and the score on the interferencecondition of the Stroop test ( p = .05), as well as for the derived interference measure (CICN:p = .04). All data has been log transformed.
257S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
Stroop variables were not accounted for by these in-dicators of illness severity.
4. Discussion
As hypothesized, bipolar patients experiencing theirfirst hospitalization demonstrated a significant relation-ship between neuropsychological performance and timeto recovery. Consistent with previous reports, bipolarpatients performed more poorly on frontal/executivetasks when compared to healthy control subjects. Per-formance on tasks which require abstraction, executivecontrol, inhibition, or shifting of mental set appeared tobe altered early in the course of the illness in thesepatients, consistent with theories of anomalous prefron-tal function (Yurgelun-Todd et al., 2000; Nordensonet al., 2004; Yurgelun-Todd and Ross, 2006). Resultsfrom this investigation demonstrate that patients whoperformed better on the interference condition of theStroop test, a task requiring active inhibition of anoverlearned tendency, required fewer days to return to abaseline level of function as defined by patients' self-report. In fact, a significant association was also de-tected for the derived interference condition and time torecovery. The derived score is designed to control for thepotential effects of psychomotor slowing, thus provid-ing a precise measure of inhibitory capacity, therefore,these findings indicate that more efficient processing oftasks requiring executive function is related to a de-crease in time to recovery.
Performance on the Stroop interference condition,measured both by CI and CI-CN, is a process previously
shown to be mediated, at least in part, by the anteriorcingulate cortex (ACC) (Carter et al., 1995; Gruberet al., 2004), and was significantly associated with timeto recovery. These results complement recent neuroima-ging studies of bipolar patients which report alterationsin frontal regions (Drevets et al., 1997; Blumberg et al.,1999). Structural MR studies have reported alterationsof subregion specific prefrontal volume in bipolar pa-tients (Lopez-Larson et al., 2002) and a number offunctional imaging investigations have reported reduc-tions of frontal activity during cognitive challenge tasks(Blumberg et al., 2000; Yurgelun-Todd et al., 2000;Adler et al., 2004; Strakowski et al., 2005). One recentstructural MR study examined gray and white mattervolumes of subregions of the ACC and performance ontests of executive function, which included the TrailMaking Test and the Wisconsin Card Sorting Test, inbipolar patients and healthy subjects. Consistent withfindings from the current investigation, the authors ofthat study reported poorer performance in bipolar pa-tients relative to controls on tasks requiring executivefunction. Further, a significant interaction was detectedbetween groups for the relationship between ACC grayand white matter volume and prediction of task per-formance, suggesting a different contribution for theseregions in patients and control subjects.
While the precise role of the ACC and the dor-solateral prefrontal cortex (DLPFC) in bipolar disorderare not clear, both regions have been shown to be com-ponents of a neural network which plays a critical role inthe completion of tasks requiring self monitoring andinhibition, functions often noted to be altered in bipolar

258 S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
patients (Gruber et al., 2004; Christodoulou et al.,2006). In one recent functional magnetic resonanceimaging (fMRI) investigation, bipolar patients demon-strated significantly reduced signal intensity within asubregion of the anterior cingulate cortex which accom-panied an increase in the dorsolateral prefrontal cortexrelative to control subjects during the performance of theinterference condition of the Stroop test (Gruber et al.,2004). The alterations in cingulate activation noted inpatients with bipolar disorder may be reflective of anabnormality of the anterior cingulate itself, or inappro-priate modulation of the cingulate by other interactivebrain regions including theDLPFC.One possibility is thatpatients with bipolar disorder have an inherent disruptionof the frontal network, which supports inhibitory func-tions (Mayberg et al., 1997). This functional changewould be consistent with clinical observations in bipolardisorder (Clark et al., 2001; Sax et al., 1999), as bipolarpatients have difficulty staying on task and maintainingmental focus. The current findings would suggest thatbipolar patients who demonstrate the strongest inhibitorycontrol are also the most likely to demonstrate shortertimes to return to baseline levels of functioning.
Studies have begun to characterize the relationshipbetween clinical symptoms and cognitive function inorder to assess the predictive value of cognitive var-iables in terms of functional recovery. A number ofinvestigations have identified a relationship betweencognitive performance and number of past affectiveepisodes and hospitalizations, suggesting that deficits inrecall and recognition are associated with a longer du-ration of bipolar illness and a history of affective, par-ticularly manic, episodes (Deckersbach et al., 2004;Cavanagh et al., 2002; Donaldson et al., 2003).Recently, Martinez-Aran et al. (2004) identified apositive correlation between bipolar patients' perfor-mance on all measures of the CVLT and their GlobalAssessment of Functioning (GAF) scores. Poor GAFscores were also associated with more perseverativeerrors on the WCST, reduced psychomotor speed, im-paired verbal fluency, and deficits in delayed logical andvisual recall. All measures of the CVLT except forrecognition were inversely correlated with duration ofillness and total number of hospitalizations, manic epi-sodes, and suicide attempts suggesting a significantrelationship between verbal memory performance andthe course of bipolar illness. In the current investigation,the patient population was evaluated early in the courseof illness, and had no prior history of hospitalizations,underscoring the likelihood that differences noted be-tween the groups are independent of treatment effects orthe result of course of illness.
Several factors should be considered in interpretingthe study findings. This investigation focused on therelationship between neurocognitive performance andtime to recovery or outcome, as defined by the numberof days required for the patient to return to a baselinelevel of function following their initial hospitalization.Given that many subjects were not rehospitalized withinthe first 12 months, this measure was based on patients'self-report of clinical state and their determination of“return to baseline” levels of function. Self-report mea-sures rely on patients' ability to be good and truthfulhistorians, which may be a confounding variable in thisstudy (Sainfort et al., 1996). It is of note, however, thatsubjects were enrolled in a longitudinal study and werecontacted at several points during the investigation.Subjects were therefore “used to” thinking about theirown clinical state and were able to determine thenumber of days to feeling better. Further, since subjectswere contacted at multiple time points, it is likely thattheir reporting remained consistent, and for subjectswho were rehospitalized, the number of days was cal-culated based on hospital records. An additional con-sideration of the current investigation is the fact thatsome subjects were taking pharmacotherapeutic agentsat the time of initial testing, which differed per indi-vidual. All testing was completed within 2 weeks ofmedication treatment, and in most cases, within a singleweek of being in the hospital. Although we cannoteliminate the possibility that some medication effectswere present, it is probable that pharmacotherapy wouldhave only hindered their cognitive performance as theywere in the earliest stages of treatment; the relationshipto outcome would likely have remained the same. Infact, the majority of subjects remained on the sametherapeutic regime at their “recovery” point, althoughsome of the dosages may have been altered. Thus, it isexpected that any potential effect of medication wouldhave remained throughout the investigation and notaffected the relationship between cognitive performanceand outcome. The significant between-group differencefor VIQ is likely due to the fact that scores are an esti-mate, based on a single measure of the WAIS-R battery,and that control subjects, matched for patient age andsocioeconomic status, were largely comprised of healthyindividuals from the community, many of whom werefrom local colleges and universities. While the VIQ iscommonly used to estimate IQ, patients' scores werelikely slightly reduced relative to premorbid levels,given their recent inpatient admission. Nevertheless, therelationship between Stroop performance and time torecovery is a within-patient analysis, which remainsunaffected by a between-group difference in VIQ.

259S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
In summary, the findings from the current investi-gation suggest an association between baselineinhibitory capacity, as measured by the Stroop test, andtime to recovery in first episode bipolar patients. Neitherage at onset or length of illness were significantly cor-related with time to recovery, or performance on theStroop; the relationship between time to recovery andStroop performance was not accounted for by these in-dicators of illness severity. These neuropsychologicalmeasures may be associated with dysfunction in frontalregions, particularly the anterior cingulate cortex. Further-more, the neuropsychological deficits were seen in patientsearly in the course of the illness, prior to the potentialneurotoxic effects of repeated affective episodes, oralterations secondary to chronic treatment with pharma-cologic agents. Future studies are needed to determinewhether changes in inhibitory processing or other cog-nitive function predict clinical outcome or are associatedwith treatment response.
Role of funding sourceFunding for this study was provided in part by an NIMH grant
(MH-069840) awarded to Dr. Yurgelun-Todd. The NIMH had nofurther role in study design, collection of data, analyses or interpretationof data, or in the decision to submit this manuscript for publication.
Conflict of interest
All authors declare that they have no conflict of interest with regardto the submitted manuscript.
Acknowledgement
The authors kindly thank Ms. Alexandra McCaffreywho assisted with the preparation of this manuscript.
References
Adler, C.M., Holland, S.K., Schmithorst, V., Tuchfarber, M.J.,Strakowski, S.M., 2004. Changes in neuronal activation in patientswith bipolar disorder during performance of a working memorytask. Bipolar Disord. 6 (6), 540–549.
Altshuler, L.L., 1993. Bipolar disorder: are repeated episodes associatedwith neuroanatomic and cognitive changes? Biol. Psychiatry. 33 (8–9),563–565.
Blumberg, H.P., Stern, E., Ricketts, S.,Martinez, D., deAsis, J.,White, T.,Epstein, J., Isenberg, N., McBride, P.A., Kemperman, I., Emmerich,S., Dhawan, V., Eidelberg, D., Kocsis, J.H., Silbersweig, D.A., 1999.Rostral and orbital prefrontal cortex dysfunction in the manic state ofbipolar disorder. Am.J. Psychiatry. 156 (12), 1986–1988.
Blumberg, H.P., Stern, E., Martinez, D., Ricketts, S., de Asis, J.,White, T., Epstein, J., McBride, P.A., Eidelberg, D., Kocsis, J.H.,Silbersweig, D.A., 2000. Increased anterior cingulate and caudateactivity in bipolar mania. Biol. Psychiatry 48 (11), 1045–1052.
Carter, C.S., Mintun, M., Cohen, J.D., 1995. Interference and fa-cilitation effects during selective attention: an H215O PETstudy ofStroop task performance. Neuroimage 2 (4), 264–272.
Cavanagh, J.T., Van Beck, M., Muir, W., Blackwood, D.H., 2002.Case-control study of neurocognitive function in euthymic patientswith bipolar disorder: an association with mania. Br. J. Psychiatry180, 320–326.
Christodoulou, T., Lewis, M., Ploubidis, G.B., Frangou, S., 2006. Therelationship of impulsivity to response inhibition and decision-making in remitted patients with bipolar disorder. Eur. Psychiatry21 (4), 270–273.
Clark, L., Iversen, S.D., Goodwin, G.M., 2001. A neuropsychologicalinvestigation of prefrontal cortex involvement in acute mania.Am. J. Psychiatry 158 (10), 1605–1611.
Comalli Jr., P.E., Wapner, S., Werner, H., 1962. Interference effectsof Stroop Color–Word Test in childhood, adulthood, and aging.J. Genet. Psychol. 100, 47–53.
Deckersbach, T., Savage, C.R., Reilly-Harrington, N., Clark, L.,Sachs, G., Rauch, S.L., 2004. Episodic memory impairment inbipolar disorder and obsessive-compulsive disorder: the role ofmemory strategies. Bipolar Disord. 6 (3), 233–244.
Denicoff, K.D., Ali, S.O., Mirsky, A.F., Smith-Jackson, E.E.,Leverich, G.S., Duncan, C.C., Connell, E.G., Post, R.M., 1999.Relationship between prior course of illness and neuropsycholog-ical functioning in patients with bipolar disorder. J. Affect. Disord.56 (1), 67–73.
Donaldson, S., Goldstein, L.H., Landau, S., Raymont, V., Frangou, S.,2003. The Maudsley Bipolar Disorder Project: the effect ofmedication, family history, and duration of illness on IQ andmemory in bipolar I disorder. J. Clin. Psychiatry 64 (1), 86–93.
Drevets, W.C., Price, J.L., Simpson Jr., J.R., Todd, R.D., Reich, T.,Vannier, M., Raichle, M.E., 1997. Subgenual prefrontal cortexabnormalities in mood disorders. Nature 386 (6627), 824–827.
Dupont, R.M., Jernigan, T.L., Heindel, W., Butters, N., Shafer, K.,Wilson, T., Hesselink, J., Gillin, J.C., 1995. Magnetic resonanceimaging and mood disorders. Localization of white matter andother subcortical abnormalities. Arch. Gen. Psychiatry 52 (9),747–755.
El-Badri, S.M., Ashton, C.H., Moore, P.B., Marsh, V.R., Ferrier, I.N.,2001. Electrophysiological and cognitive function in youngeuthymic patients with bipolar affective disorder. Bipolar Disord.3 (2), 79–87.
Elliott, R., Sahakian, B.J., McKay, A.P., Herrod, J.J., Robbins, T.W.,Paykel, E.S., 1996. Neuropsychological impairments in unipolardepression: the influence of perceived failure on subsequentperformance. Psychol. Med. 26 (5), 975–989.
Frangou, S., Donaldson, S., Hadjulis, M., Landau, S., Goldstein, L.H.,2005. The Maudsley Bipolar Disorder Project: executive dysfunc-tion in bipolar disorder I and its clinical correlates. Biol. Psychiatry58 (11), 859–864.
Gourovitch, M.L., Torrey, E.F., Gold, J.M., Randolph, C., Weinberger,D.R., Goldberg, T.E., 1999. Neuropsychological performance ofmonozygotic twins discordant for bipolar disorder. Biol. Psychi-atry. 45 (5), 639–646.
Gruber, S.A., Rogowska, J., Yurgelun-Todd, D.A., 2004. Decreasedactivation of the anterior cingulate in bipolar patients: an fMRIstudy. J. Affect. Disord. 82 (2), 191–201.
Kessing, L.V., 1998. Cognitive impairment in the euthymic phase ofaffective disorder. Psychol. Med. 28 (5), 1027–1038.
Lebowitz, B.K., Shear, P.K., Steed, M.A., Strakowski, S.M., 2001.Verbal fluency in mania: relationship to number of manicepisodes. Neuropsychiatry Neuropsychol. Behav. Neurol. 14 (3),177–182.
Lezak, M., 2004. Neuropsychological Assessment, 4th Ed. OxfordUniversity Press, New York.

260 S.A. Gruber et al. / Journal of Affective Disorders 105 (2008) 253–260
Lopez-Larson, M.P., DelBello, M.P., Zimmerman, M.E., Schwiers,M.L., Strakowski, S.M., 2002. Regional prefrontal gray and whitematter abnormalities in bipolar disorder. Biol. Psychiatry 52 (2),93–100.
MacQueen, G.M., Young, L.T., Galway, T.M., Joffe, R.T., 2001.Backward masking task performance in stable, euthymic out-patients with bipolar disorder. Psychol. Med. 31 (7), 1269–1277.
Martinez-Aran, A.,Vieta, E., Colom, F., Torrent, C., Sanchez-Moreno, J.,Reinares, M., Benabarre, A., Goikolea, J.M., Brugue, E., Daban, C.,Salamero, M., 2004. Cognitive impairment in euthymic bipolarpatients: implications for clinical and functional outcome. BipolarDisord. 6 (3), 224–232.
Mayberg, H.S., Brannan, S.K., Mahurin, R.K., Jerabek, P.A., Brickman,J.S., Tekell, J.L., Silva, J.A.,McGinnis, S., Glass, T.G.,Martin, C.C.,Fox, P.T., 1997. Cingulate function in depression: a potentialpredictor of treatment response. Neuroreport 8 (4), 1057–1061.
Nehra, R., Chakrabarti, S., Pradhan, B.K., Khehra, N., 2006. Com-parison of cognitive functions between first and multi-episodebipolar affective disorders. J. Affect. Disord. 93, 185–192.
Nordenson, B., Gruber, S.A., Yurgelun-todd, D., 2004. Neurocogni-tion in bipolar disorder: a review of the current research. Curr.Psychos. Therap. Reports 2, 147–152.
Reitan, R.M., 1958. The Validity of the Trail Making Test as anindicator of organic brain damage. Percept. Mot. Skills 8, 271–276.
Rubinsztein, J.S., Michael, A., Paykel, E.S., Sahakian, B.J., 2000.Cognitive impairment in remission in bipolar affective disorder.Psychol. Med. 30 (5), 1025–1036.
Sainfort, F., Becker, M., Diamond, R., 1996. Judgments of quality oflife of individuals with severe mental disorders: patient self-reportversus provider perspectives. Am. J. Psychiatry 153 (4), 497–502.
Sax, K.W., Strakowski, S.M., Zimmerman, M.E., DelBello, M.P.,Keck Jr., P.E., Hawkins, J.M., 1999. Frontosubcortical neuroanat-omy and the continuous performance test in mania. Am. J. Psy-chiatry 156 (1), 139–141.
Spreen, O., Strauss, E., 1991. A Compendium of NeuropsychologicalTests: Administration, Norms and Commentary. Oxford UniversityPress, New York.
Strakowski, S.M., Adler, C.M., Holland, S.K., Mills, N.P., DelBello,M.P., Eliassen, J.C., 2005. Abnormal FMRI brain activation ineuthymic bipolar disorder patients during a counting Stroopinterference task. Am. J. Psychiatry 162 (9), 1697–1705.
Stroop, J., 1935. Studies of interference in serial verbal reactions.J. Exp. Psychol. 18, 643–662.
van Gorp, W.G., Altshuler, L., Theberge, D.C., Wilkins, J., Dixon, W.,1998. Cognitive impairment in euthymic bipolar patients with andwithout prior alcohol dependence. A preliminary study. Arch. Gen.Psychiatry 55 (1), 41–46.
Wechsler, D., 1981. Wechsler Adult Intelligence Scale — Revised.The Psychological Corporation, New York.
Yurgelun-Todd, D.A., Ross, A.J., 2006. Functional magnetic reso-nance imaging studies in bipolar disorder. CNS Spectr. 11 (4),287–297.
Yurgelun-Todd, D.A., Gruber, S.A., Kanayama, G., Killgore, W.D.,Baird, A.A., Young, A.D., 2000. fMRI during affect discriminationin bipolar affective disorder. Bipolar Disord. 2 (3 Pt 2), 237–248.
Zubieta, J.K., Huguelet, P., O'Neil, R.L., Giordani, B.J., 2001.Cognitive function in euthymic bipolar I disorder. Psychiatry Res.102 (1), 9–20.