NEUROPARASITIC INFECTIONS basis, diagnosis and limitations
85
NEUROPARASITIC INFECTIONS basis, diagnosis and limitations Dr.T.V.Rao MD
-
Upload
drtv-rao -
Category
Health & Medicine
-
view
224 -
download
2
Transcript of NEUROPARASITIC INFECTIONS basis, diagnosis and limitations

NEUROPARASITIC INFECTIONS
basis, diagnosis and limitations
Dr.T.V.Rao MD


How Parasites Enter Blood Brain Barrier
• Some intracellular and extracellular parasites can traverse the BBB during the course of infection and cause neurological disturbances and/or damage which are at times fatal. The means by which parasites cross the BBB and how the immune system controls the parasites within the brain are still unclear.

Methods to Diagnose Infections
• Methods for the diagnosis of infectious diseases have stagnated in the last 20–30 years. Few major advances in clinical diagnostic testing have been made since the introduction of PCR, although new technologies are being investigated.

Are we Practising Older Methods
•Many tests that form the backbone of the “modern” microbiology laboratory are based on very old and labour-intensive technologies such as microscopy for malaria or many parsites

Parasitic Infections Migrating from Developing Nations to Developed Nations
•Parasitic infections of the CNS, previously restricted mainly to people living in developing countries, are becoming increasingly more prevalent throughout the world. With the advent of increasing global travel,

Immune suppression changes the Adoptability of Infections
•Potent immunosuppression, and HIV infection, parasitic infections will likely become even more commonplace.

Overall familiarity is Important to Evaluate the Matters
•Basic familiarity with common pathogens can make diagnosis more expeditious and efficient. For the clinician confronted with a patient with suspected parasitic infection, additional assistance with diagnostic evaluation

Beginning of Career to Learn and Practice of parasitology at Mansa General hospital Zambia

Is it easy to Diagnose Parasitic Infections of Nervous system ?
•Parasitic infection of the nervous system can produce a variety of symptoms and signs. Because symptoms of infection are often mild or nonspecific, diagnosis can be difficult.

Be familiar with Epidemiology and Radiology
• Familiarity with basic epidemiological characteristics and distinguishing radiographic findings can increase the likelihood of detection and proper treatment of parasitic infection of the nervous system.

We are still using the Microscope as a Traditional tool in Diagnosis
•The primary tests currently used to diagnose many parasitic diseases have changed little since the development of the microscope in the 15th century by Antonie van Leeuwenhoek. Furthermore, most of the current tests cannot distinguish between past, , latent, acute, and reactivated infections.

Diagnostic Methods in Parasitology are Complex
If we wish sensitivity and specificity • The methods currently in use
range from rather simple, easily managed and routine techniques to the extremely complex cutting edge technologies of modern molecular biology and high-throughput miniaturised methods usually done as part of thesis and research work and rarely for diagnostic work

Newer Serological Assays • Firstly, a number of newer
serology-based assays that are highly specific and sensitive have emerged, such as the Falcon assay screening test ELISA (FAST-ELISA) , Dot-ELISA rapid antigen detection system (RDTS) , and luciferase immunoprecipitation system (LIPS).

Emerging Molecular methods
• Secondly, molecular-based approaches such as loop-mediated isothermal amplification (LAMP) , real-time polymerase chain reaction and Luminex have shown a high potential for use in parasite diagnosis with increased specificity and sensitivity.

Parasites Infections of the Central Nervous System
•Toxoplasma gondii associated with congenital defects and AIDS
•African trypanosomes African sleeping sickness
•Plasmodium falciparum cerebral malaria
•Endamoeba histolytic rare invasion of the brain
•Free-living amebae rare cases

MALARIA

Malaria Continues to be a Emergency in many countries
• Malaria should be considered a potential medical emergency and should be treated accordingly. Delay in diagnosis and treatment is a leading cause of death in malaria patients in Many Countries

Peripheral Blood Smear a Great tool
• Clinicians seeing a malaria patient may forget to consider malaria among the potential diagnoses and not order the needed diagnostic tests. Laboratories may lack experience with malaria and fail to detect parasites when examining blood smears under the microscope

Making a Smear is Most Important Part of Microscopy

Microscopic Diagnosis• Malaria parasites can be
identified by examining under the microscope a drop of the patient's blood, spread out as a "blood smear" on a microscope slide. Prior to examination, the specimen is stained (most often with the Giemsa stain) to give the parasites a distinctive appearance. This technique remains the gold standard for laboratory confirmation of malaria.

Appearance of P.vivax and P. falciparum

Malaria Diagnosis is a Emergency

Clinical examination a collaborating point
•Cerebral malaria, with abnormal behaviour, impairment of consciousness, seizures, coma, or other neurologic abnormalities

Antigen Detection• Various test kits are available to
detect antigens derived from malaria parasites. Such immunologic ("immunochromatographic") tests most often use a dipstick or cassette format, and provide results in 2-15 minutes. These "Rapid Diagnostic Tests" (RDTs) offer a useful alternative to microscopy in situations where reliable microscopic diagnosis is not available.

HRP2 levels predict likelihood of cerebral malaria in African children
• . While only about 1% of Plasmodium falciparum infections progress to cerebral malaria, mortality occurs in 10–20% of affected patients. plasma concentrations of the Plasmodium protein HRP2 (histidine rich protein 2) can predict the odds of developing cerebral malaria in Malawian children. Their data show that mean plasma HRP2 concentrations were significantly higher in the children who developed cerebral malaria than the ones with uncomplicated malaria.

QBC SYSTEM CANNOT DIFFERENTIATE Species

No Single Test is Perfect
•Current evidence indicates that no single method for the diagnosis of malaria is perfect nor can any one of them be a stand-alone accurate and effective diagnostic criterion . Accurate and effective malaria diagnosis should thus involve a rational approach to each patient with suspected malaria employing both symptoms/signs-based and laboratory-based malaria diagnostic methods.

Emerging methods at even Smaller Clinks
• The prioritizing of any of the malaria diagnostic methods, at all times, should be influenced by various factors including malaria endemicity, transmission pattern, the urgency of the diagnosis, the experience of the health worker, effectiveness of the health care system, and available budget resources.

Rapid Diagnostic Tests
• RDTs do not require laboratory equipment and are all based on the same principle and detect malaria antigen in blood flowing along a membrane containing specific anti- malaria antibodies . Most of the available RDTs are P. falciparum protein specific (either histidine rich protein II -HRP-II or lactase dehydrogenase-LDH) while some RDTs detect P. falciparum and other Plasmodium proteins such as aldolase or pan-malaria pLDH.

Rapid diagnostic tests proving useful
• Several studies have reported the performance of RDTs to be excellent. Inarguably, RDTs are enhancing the benefits of parasite-based diagnosis of malaria though not without problems or limitations

Molecular Malaria laboratory diagnostic tests• Molecular malaria techniques
such as PCR on blood or, more recently, even on saliva samples devised in Zambia by (Mharakurwa et al), the loop-mediated isothermal amplification (LAMP), microarray, mass spectrometry (MS), and flow cytometry (FCM) assay techniques are all new developments mainly utilized in research settings than during routine patient care.

Serology• Serology detects antibodies
against malaria parasites, using either indirect immunofluorescence (IFA) or enzyme-linked immunosorbent assay (ELISA). Serology does not detect current infection but rather measures past exposure.

Rapid Tests •RDTs currently available
in the market are quite a few and include brands such as O p t i M A L , P a r a c h e c k , I C T, p a r a - s i g h t - F, parascreen, and SD Bioline.

Artefacts

Free Living Amoebic Infections
PARASITIC MENINGITIS

Free Living Amoeba • Naegleria fowleri and
Acanthamoeba spp., are commonly found in lakes, swimming pools, tap water, and heating and air conditioning units. While only one species of Naegleria, N. fowleri, is known to infect humans An additional agent of human disease, Balamuthia mandrillaris, is a related free-living amoeba that is morphologically similar to Acanthamoeba in tissue sections in light microscopy.

Diagnostic Findings• In Naegleria infections, the
diagnosis can be made by microscopic examination of cerebrospinal fluid (CSF). A wet mount may detect motile trophozoites, and a Giemsa-stained smear will show trophozoites with typical morphology. Confocal microscopy or cultivation of the causal organism, and its identification by direct immunofluorescent antibody, may also prove useful.

Naegleria fowleri/Primary Amoebic Meningo encephalitis
• Early symptoms include severe, throbbing headache, fever, nausea, and vomiting.Most patients have a history of swimming or bathing in stagnant water.
• Meningismus is common, and some patients present with seizures or coma. Differentiation between PAM and bacterial meningitis can be difficult but is crucial given the rapid progression of N. fowlerii infection.

Wet mounts are beneficial
• Organisms are not visualized with Gram’s stain because amoebas are killed during the fixation process.
• CSF wet mount should be performed to look for trophozoites. Giemsa staining of CSF may also be useful. In the past,

Acanthamoeba• In Acanthamoeba infections,
the diagnosis can be made from microscopic examination of stained smears of biopsy specimens (brain tissue, skin, cornea) or of corneal scrapings, which may detect trophozoites and cysts

Acanthamoeba histolytica and Balamuthiamandrillaris/Granulomatous Amoebic
•CNS infection by A. histolytica is uncommon in immunocompetent hosts. In contrast to A. histolytica, B. mandrillaris causes infection inimmunocompetent and immunosuppressed hosts with equal frequency

Corneal scrapings
•Definitive diagnosis can be obtained by demonstration of trophozoites or cysts of A. histolytica on stained smears of biopsy specimens or corneal scrapings

Immunofluorescence studies
• Direct IFA tests can be useful. Differentiation between B. mandrillaris and A. histolytica infection requires immunofluorescence studies. Examination of contact lenses from patients with keratitis can reveal A. histolytica

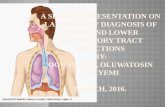
1Trophozoite of N. fowleri in CSF, stained with haematoxylin and eosin 2Trophozoite of N. fowleri in CSF, stained with haematoxylin and eosin

1Cyst of Acanthamoeba sp. from brain tissue, stained with haematoxylin and eosin
2Trophozoites of Acanthamoeba sp. in a corneal scraping, stained with H&E.

Real-Time PCR
• A real-time PCR was developed at CDC for identification of Acanthamoeba spp., Naegleria fowleri, and Balamuthia mandrillaris in clinical samples.1 This assay uses distinct primers and TaqMan probes for the simultaneous identification of these three parasites

Toxoplasmosis

Cerebral toxoplasmosis : Centre for Disease Control (CDC) criteria for diagnosis
•Recent onset of focal neurological abnormality consistent with intracranial disease or reduced consciousness•Evidence from brain imaging of a lesion (CT or MRI)•Positive serum antibody to T. gondii or response to treatment

Diagnosis of toxoplasmosis
•Diagnosis of toxoplasmosis is rarely made through the detection or recovery of organisms, but relies heavily on serological procedures. Parasites can be detected in biopsied specimens, buffy coat cells, or cerebral spinal fluid. These materials can also be used to inoculated mice or tissue culture cells. However, detecting tachyzoites from these materials is difficult.. Therefore, serologic tests are recommended for diagnosis

IgM and Toxoplasmosis
• Acute infections are characterized by high IgM titres and/or a significant increase in total antibody titre in a sample taken two weeks later. The serology may also correlate with the acute stage symptoms in some individuals.

Diagnostic tests for Toxoplasma
•Sabin-Feldman dye test (DT)•Enzyme immunoassay for T. gondii specific IgM (EIA)• Immunsorbent agglutination assay (ISAGA)•Enzyme immunoassay for IgG avidity• Isolation and culture of parasite •Direct detection by microscopy and PCR

Persons with ocular disease• Eye disease (most
frequently retinochoroiditis) from Toxoplasma infection can result from congenital infection or infection after birth by any of the modes of transmission discussed on the epidemiology and risk factors page.

Persons with compromised immune systems
•Persons with compromised immune systems may experience severe symptoms if they are infected with Toxoplasma while immune suppressed.

Serology •In the second situation, a second specimen should be drawn and both specimens submitted together to a reference lab which employs a different IgM testing system for confirmation. Prior to initiation of patient management for acute toxoplasmosis, all IgG/IgM positives should be submitted to a reference lab for IgG avidity testing.

Diagnosis• The diagnosis of toxoplasmosis is
typically made by serologic testing. A test that measures immunoglobulin G (IgG) is used to determine if a person has been infected. If it is necessary to try to estimate the time of infection, which is of particular importance for pregnant women, a test which measures immunoglobulin M (IgM) is also used along with other tests such as an avidity test.

Diagnosis by staining methods
• Diagnosis can be made by direct observation of the parasite in stained tissue sections, cerebrospinal fluid (CSF), or other biopsy material. These techniques are used less frequently because of the difficulty of obtaining these specimens.

:
Cysticercosis

Cysticercosis • This infection is caused by pork
tapeworm larvae (see Tapeworm Infection). It is the most common parasitic infection in the Western Hemisphere. After people eat food contaminated with cysticercuseggs, secretions in the stomach cause the eggs to hatch into larvae. The larvae enter the bloodstream and are distributed to all parts of the body, including the brain

MRI AND CT SCNNING CONTINUES TO BE MAIN IN STAY IN DIAGNOSIS
•Magnetic resonance imaging (MRI) or computed tomography (CT) can often show the cysts. But blood tests and a spinal tap (lumbar puncture) to obtain a sample of cerebrospinal fluid are often needed to confirm the diagnosis.

PRIMARY EXAMINATIONS
• Infection with adult T. solium worms can usually be diagnosed by microscopic examination of stool samples and identification of eggs and/or proglottids. However, T. solium eggs are present in ≤ 50% of stool samples from patients with cysticercosis.

CDC standarsises the Immunoblot Testing
• The CDC's immunoblot assay (using a serum specimen) is highly specific and more sensitive than other enzyme immunoassays (particularly when > 2 CNS lesions are present; sensitivity is lower when only a single cyst is present).

Immunoblot assay • CDC's immunoblot assay with
purified Taenia solium antigens has been acknowledged by the World Health Organization and the Pan American Health Organization as the immunodiagnostic test of choice for confirming a clinical and radiologic presumptive diagnosis of neurocysticercosis.

We mainly Dependent on
• There are two available serologic tests to detect cysticercosis, the enzyme-linked immunoelectrotransfer blot or EITB, and commercial enzyme-linked immunoassays.

Antigen Detection
• Tests that detect circulating cysticercal antigens in serum and CSF have been developed and may prove to be most useful to follow response to therapy in in subarachnoid and ventricular forms of neurocysticercosis. Antigen levels drop quickly in cured NCC patients, so serum antigen monitoring is useful for assessing treatment and determining of clinical cases.

Antigen Detection Methods lack sensitivity
•Antigen detection testing is not as sensitive as antibody detection and should not be used to diagnose neurocysticercosis

Molecular Detection•PCR tests have been developed to detect T. solium DNA in CSF but these are not widely used for clinical laboratory diagnosis of neurocysticercosis.

Schistosomiasis (Bilharzia)• EPIDEMIOLOGY—Schistosomiasis
occurs in up to 300 million people worldwide each year and is caused by five species of blood flukes (digenetic trematodes): Schistosoma mansoni, S.haematobium, S. japonicum, S. intercalculatum, and S. mekongi.62 CNS involvement has beenreportedwith three of the five species: S. mansoni, S. haematobium, S. japonicum

Neurological involvement • Neurological involvement usually
appears weeks ormonths after initial infection when eggs migrate through the vascular system to the brain orspinal cord; symptoms may result from mass effect of the egg itself or from granulomaformation around the egg. Because the parasite likely enters the CNS via Batson’s plexus,the spinal cord and posterior fossa are the most common sites of involvement

DIAGNOSIS• Definitive diagnosis of CNS
schistosomiasis is obtained by identification ofan egg in biopsy tissue. Detection of schistosomal eggs in stool or urine confirms the diagnosisof schistosomiasis.14 Stool examination is more sensitive for S. mansoni and S. japonicum,and examination of urine is best for S. hematobium.

Echinococcus (Hydatid Disease)

Echinococcus (Hydatid Disease) CESTODES
• Hydatid infection often remains undetected until cyst enlargement produces symptoms. The cyst can cause more severe symptoms if it ruptures or becomes super-infected. Central nervous system (CNS) involvement complicates 2 and 5% of infections with E. granulosis and E. multilocularis, respectively.1,3

DIAGNOSIS• Diagnosis of E. granulosus infection
can be confirmed by serum indirect hemagglutination (IHA), indirect fluorescent antibody (IFA), or enzyme-linked immunosorbent assay (ELISA), with assay sensitivity rates ranging from 50 to 60% in patients with pulmonary cysts to 98% in patients with hepatic cysts.9 Serum assays to detect E. multilocularis are more sensitive than assays for E. granulosis and are not cross-reactive

NEUROIMAGING• ontrast-enhanced computerized
tomography (CT) of the brain is usually sufficient for evaluation, but magnetic resonance imaging (MRI) is warranted if surgical intervention is planned. CT demonstrates cysts of various sizes, sometimes in grapelike clusters.13 Chronic disease may develop a granulomatous appearance

Serum indirect hemagglutination (IHA),
• Diagnosis of E.granulosus infection can be confirmed by serum indirect hemagglutination (IHA), indirectfluorescent antibody (IFA), or enzyme-linked immunosorbent assay (ELISA), with assaysensitivity rates ranging from 50 to 60% in patients with pulmonary cysts to 98% in patientswith hepatic cysts.9 Serum assays to detect E. multilocularis are more sensitive than assaysfor E. granulosis and are not cross-reactive.

CDC Helps in Diagnosis of Parasitic Infections

I wish many use this Facility
• The modern generation of Microbiologists can use digital imaging technology of parasitic infections with Web site developed and maintained by CDC's Division of Parasitic Diseases and Malaria (DPDM)

CDC Helps with Tele diagnosis of PaasiticInfection
• DPDx is a unique online educational resource that includes visual depictions of parasite lifecycles, a reference library of free images of parasites, and guidance on proper laboratory techniques for diagnostic parasitology. But it is much more than a Web site.

1Encysted larvae of Trichinella sp. in muscle tissue, 2 Babesia and Falciparum

Diagnostic Assistance functionA Diagnostic Assistance function, in which laboratory and other health professionals can ask questions and/or send digital images of specimens for expedited review and consultation with DPDxstaff. This assistance is free of charge.

Why we Stand Today In Diagnosis
• In spite of many Advances in Medical profession the Parasitology suffers much lacunae in diagnosis for optimal treatment, great reason being lack of human dedication in the matters concerned, and lack of evaluation of skills in matters of diagnostic talents in postgraduate examinations, and above all non-availability of advancing technologies

The Great Question hunts many of us, If we are true to our Job
Are we really diagnosing the
Parasitic Infections?

Say
OR NO•

What Can be Done? • Speciality of Parasitology
hangs between the domains of Microbiology and Pathologists. However it needs more inputs and coordination of Vetenary sciences and Zoology Professionals.