NEUROLOGY CASE CONFERENCE Subsection D2 NEUROLOGY CASE CONFERENCE Subsection D2 Rivera. Rivere....
165
NEUROLOGY CASE CONFERENCE Subsection D2 Rivera. Rivere. Robosa. Rodas. Rodriguez. Rogelio. Roque. Ruanto. Sabalvaro. Salac. Salazar, J. Salazar, R. Salcedo. Saldana. Sales. Salonga. San Diego. San Pedro. Sanez. Sanidad. Santos, E. Santos, J.
-
Upload
madlyn-austin -
Category
Documents
-
view
220 -
download
2
Transcript of NEUROLOGY CASE CONFERENCE Subsection D2 NEUROLOGY CASE CONFERENCE Subsection D2 Rivera. Rivere....

NEUROLOGY CASE CONFERENCESubsection D2Rivera. Rivere. Robosa. Rodas. Rodriguez. Rogelio. Roque. Ruanto. Sabalvaro. Salac. Salazar, J. Salazar, R. Salcedo. Saldana. Sales. Salonga. San Diego. San Pedro. Sanez. Sanidad. Santos, E. Santos, J.

CASE 2.1

Case 2.1
A 10 year-old girl was brought by her mother for a consult because of poor academic performance. School teachers often observed her to be absent minded described as recurrent but brief periods of blank staring and inattention. This was accompanied by eye blinking, reflex scratching of her head, lip smacking and chewing movements which all lasts for a few seconds. These would occur many times a day and after each attack, the patient would resume his usual activity.

Missing Data
First episode or onset of symptoms Presence or absence of fever, loose
bowel movement, vomiting Previous school performance Family History

Salient Features
10 year old girl Poor academic performance Absent minded
Recurrent, brief periods of blank staring and inattention
Accompanied by eye blinking, reflex scratching of her head, lip smacking and chewing movements
Occurs many times a day

Differential Diagnosis
Neonates(<1month
)
Infants and
Children(>1
month-<12yrs.)
Adolescents
12-18yrs.
Young Adults
18-35yrs.

Differential Diagnosis
Probable Cause Type
Infants and Children(>1 month-<12yrs.)
Febrile seizureGenetic disorders (metanolic, degenerative, primary epilepsy syndromes)CNS infectionDevelopmental disordersTraumaIdiopathic
Complex partial seizuresGeneralized Seizures: •Atonic Seizures•Absence (petit mal)Epilepsy Syndromes•JME•Lennox-Gastaut •MTLE

TYPES
Complex Partial
Ictal phase: sudden behavioral arrest or motionless stare
Automatisms:Chewing, lip smacking, swallowing, “picking” movements of hands
Seconds – an hourImpaired recollection or motionless stare
AtonicBriefly impaired consciousness
Quick head drop or nodding movement
1 to 2 secondsNo post-ictal confusion
JME
Bilateral myoclonic seizures;single or repetetiveConsciousness is preserved
Myoclonic seizures frequent in the morningProvoked by sleep deprivation
One-third have absence seizures
Lennox-Gastaut
•Multiple seizure types•Impaired cognitive function
Associated with CNS disease, devt. Abnormalities, perinatal hypoxia/ischemia, trauma, infection
Impaired cognitive syndrome
MTLE
AuraBehavioral arrest/stare
Complex automatismsUnilateral posturing
Postictal disorientation, memory loss dysphasia
Absence (petit-mal)
Sudden, brief lapses of consciousness, “daydreaming”
No loss of postural controlRapid blinking, chewing movements.Can occur hundred times a day
Lasts for secondsNo postictal confusionDecline in school performance

Clinical Impression:Absence Seizure

Absence Seizure
• A type of generalized seizure, lasting for several seconds to minutes and may occur several times a day.
Reference: Segan, S. (2009). Absence Seizures. American Academy of Neurology and American Epilepsy Society.
• Children with idiopathic generalized epilepsies may present with a history of staring spells, but infrequent absence seizures may not be diagnosed until a generalized tonic-clonic seizure has occurred.

Absence Seizure
• Other symptoms, such as behavioral problems may be the presenting complaint.– Although the brief attacks are unrecognized, the
lapses of awareness interfere with attention.
• Decline in school performance may be an indication of the onset or breakthrough of absence seizures.
• In symptomatic generalized epilepsies, atypical absence seizures often occur in the setting of developmental delay or mental retardation.
Reference: Segan, S. (2009). Absence Seizures. American Academy of Neurology and American Epilepsy Society.

Absence Seizure
On clinical examination, typical absence seizures appear as: Brief staring spells
Patients have no warning phase, and if engaged in gross motor activity, such as walking, they may stop and stand motionless or they may continue to walk.
Unresponsive during the seizure Children have no memory of what happened
during the attack; they are generally unaware that a seizure has occurred.
Reference: Segan, S. (2009). Absence Seizures. American Academy of Neurology and American Epilepsy Society.

Pathophysiology
• The pathophysiology of absence seizures is not fully understood.
• Abnormal oscillatory rhythms are believed to develop in thalamocortical pathways.
– This involves GABA-B–mediated inhibition alternating with glutamate-mediated excitation.
– GABA-B inhibition appears to be altered in absence seizures.
– Enhanced burst firing in selected corticothalamic networks may increase GABA-B receptor activation in the thalamus, leading to generalized spike-wave activity.
Reference: Segan, S. (2009). Absence Seizures. American Academy of Neurology and American Epilepsy Society.

Absence Seizure vs Complex Partial Seizure
• An absence seizures can sometimes be confused with a complex partial seizure but each type has its own distinctive features:– Absence seizures :• Never preceded by an aura• Are of briefer duration – seconds rather than
minutes• Begin frequently and end abruptly• The absence attack is always associated with the
strikingly typical EEG abnormality of spike and slow wave discharges, usually at a frequency of 3Hz which occur can occur interictally and ictally and are often provoked by hyperventilation.

Absence Seizures
Absence Seizures
In childhood absence epilepsy, seizures are frequent and brief, lasting just a few seconds (pyknoleptic). Some children can have many such seizures per day. In other epilepsies, particularly those with an older age of onset, the seizures can last several seconds to minutes and may occur only a few times a day (nonpyknoleptic or spanioleptic absence seizures).

The etiology of idiopathic epilepsies with age-related onset is genetic. About 15-40% of patients with these epilepsies have a family history of epilepsy; overall concordance in monozygotic twins is 74% with a 100% concordance during the peak age of phenotypic expression. Family members may have other forms of idiopathic or genetic epilepsy (eg, febrile convulsions, generalized tonic-clonic seizures.

Typical Absence Seizures
Sudden onset of impaired movements
Staring episodes or "absence spells" Accompanied by other motor,
behavioral or autonomic phenomena
May interfere with school function and learning
Reference: Pediatric Epilepsy: Diagnosis and Therapy: John M. Pellock,Blaise F. D. Bourgeois
Atypical Absence Seizure
Less abrupt onset and cessation More pronounced changes in tone and
longer duration Usually begins before 5 years of age Associated with other generalized
seizure types and mental retardation
Reference: Pediatric Epilepsy: Diagnosis and Therapy: John M. Pellock,Blaise F. D. Bourgeois

Diagnostic Work-up
Electroencephalography (EEG)
The only diagnostic test for absence seizures
Ambulatory EEG monitoring over 24 hours may be useful to quantitate the number of seizures per day and their most likely times of occurrence.

EEG: Typical Absence
Findings in typical absence seizures include the following: Background activity is normal.
In syndromes with frequent absence seizures, such as childhood absence epilepsy, a routine awake recording is often pathognomonic.
In syndromes with less frequent absence seizures (juvenile absence epilepsy or juvenile myoclonic epilepsy), an awake recording may be normal; a sleep or sleep-deprived recording may be needed.
Typical absence seizures have generalized 3-Hz spike-and-wave complexes.

EEG: Typical Absence

EEG: Typical Absence
The onset and ending of these seizures are abrupt; no postictal EEG slowing is noted.
Hyperventilation often provokes these seizures and should be a routine part of all EEGs in children.
EEG video monitoring demonstrates that clinical seizure manifestations may lag behind the start of ictal EEG activity; bursts lasting less than 3 seconds are usually clinically silent.
During the absence seizure, rhythmic eye blinks and mild clonic jerks may be present. As a seizure progresses, automatisms may be seen.
Clinical and EEG features may vary considerably in different children.
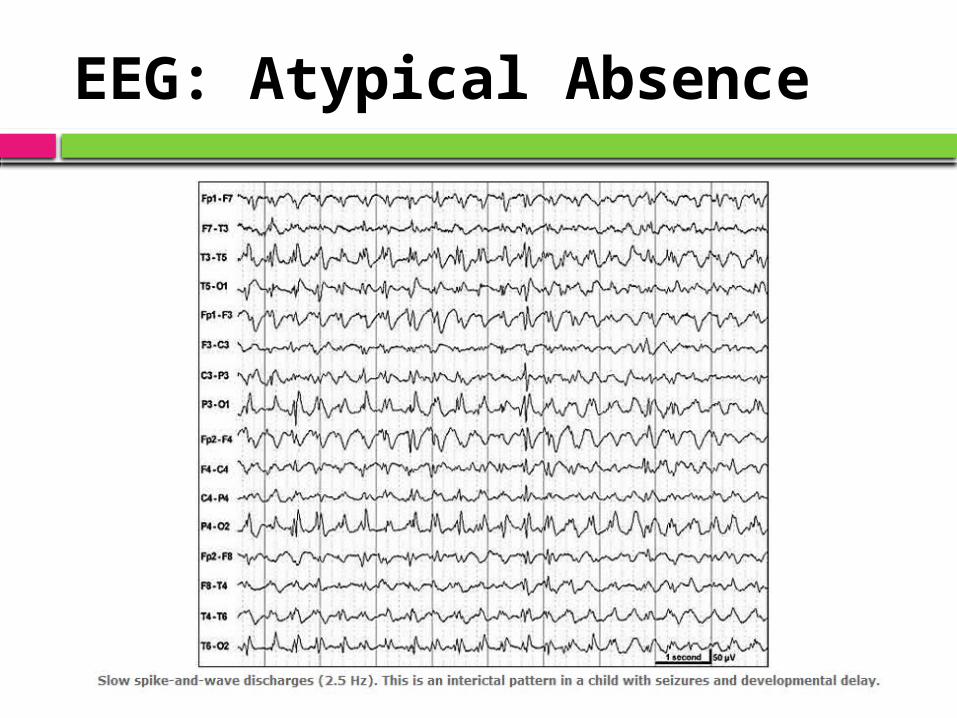
EEG: Atypical Absence
Findings in atypical absence seizures include the following: Background activity is often abnormal,
reflecting the diffuse or multifocal underlying encephalopathy of symptomatic generalized epilepsy.
Seizures are characterized by slow spike-and-wave paroxysms, classically 2.5 Hz.
EEG: Atypical Absence

EEG: Atypical Absence
• The onset may be difficult to discern, and postictal EEG slowing may be noted.
• The clinical correlation of generalized spike-and-wave complexes with clinical seizures is not as clear-cut as in typical absence seizures.
• EEG-video monitoring can show a more varied alteration of consciousness than in typical absence seizures. If the patient has underlying mental retardation, discerning changes in mental status also may be more difficult in atypical absence.
• Changes in postural tone, most noticeably head nods, are common.

Laboratory Studies
Laboratory tests for: Metabolic abnormalities Toxic or drug ingestion Blood levels of electrolytes, glucose, calcium,
magnesium Hepatic or renal disease
If a clear history of the episodic nature of the attacks is obtained, then the EEG can be diagnostic and laboratory tests may not be necessary.

Imaging Studies
Neuroimaging is not indicated if the typical clinical pattern is present.
Neuroimaging findings are normal in idiopathic epilepsies by definition.
Often ordered if a child presents with a generalized tonic-clonic seizure, to rule out significant structural causes of seizures.
If imaging is performed, MRI is preferred to CT scanning. MRI is more sensitive for certain anatomic abnormalities.

Treatment

Treatment
DEPENDS on the underlying cause
Metabolic : correctionStructural abnormality: seizure
control + consider surgeryTumorVascular
Idiopathic : seizure control

Treatment
Diagnosis and Classification of seizure disorder
Choose Anti-epileptic drug of choice
Main Goal: Adequate seizure control
Monitoring of response
(seizure-free) and side effects
Therapeutic Monitoring
Drug Interactions

Principles of Treatment
Individualized treatment Selection of specific drug for initial therapy is based
on specific clinical seizure type. Monotherapy is preferred. Dose is increased gradually. Enough time for steady state to be reached must be
allowed. Prompt substitution when serious adverse reaction
develops. If poor seizure control-gradually withdraw first drug
while replacing with second drug of choice for seizure type (should not be stopped abruptly).
Treatment failures may be due to poor compliance or misdiagnosis.
Continue treatment to achieve minimum seizure-free period of 3-5 years.
References: Katzung Basic and Clinical Pharmacology, 9th ed. The Treatment of Epilepsy, 3rd ed.

Absence Seizures
• Ethosuximide is the drug of choice for typical absence seizure
• Valproic Acid is the drug of choice for atypical absence seizure.
• Used only when treatment tolerance or failure appear with Ethosuximide
• Wide spectrum AED

Anti Epileptic Drug
Glutamate Antagonis
t
GABA agonist
Na channel blocker
Ca channel blocker
Phenobarbital *
Phenytoin *
Carbamazepine *
Valproic Acid * *
Gabapentin *
Topiramate * * * *
Oxcarbazepine * *
Ethosuximide *
Lamotrigine * *

Ethosuximide
Primary indication: First-line or adjunctive therapy of generalized absence seizures
Mechanisms of action: Inhibition of neuronal T-type calcium channels in the thalamus (Type III AED)
Usual preparations: Capsules: 250 mg; syrup: 250 mg/5 mL
Usual dosages: Initial: 250 mg (adults); 10–15 mg/kg/day (children)
Maintenance: 750–1500 mg/day (adults); 15–40 mg/kg/day (children)
Dosing frequency: 2–3 times/day Significant drug interactions:
Ethosuximide levels are reduced by co-medication with carbamazepine, phenytoin, phenobarbital and rifampicin.
Valproic acid may exert synergistic effects with ethosuximide in patients refractory to either drug given alone, and may have variable and inconsistent effects on ethosuximide levels. Serum valproic acid levels may be decreased by ethosuximide. Ethosuximide levels are increased by isoniazid.
References: Katzung Basic and Clinical Pharmacology, 9th ed. The Treatment of Epilepsy, 3rd ed.

Ethosuximide
Serum level monitoring: usually optimized based on clinical and EEG response.
Main advantages: Well-established treatment for absence epilepsy without the risk of hepatic toxicity carried by valproic acid
Main disadvantages: Adverse effects common. Unlike valproic acid, ethosuximide does not protect against generalized tonic–clonic seizures
Common/important adverse effects: Gastrointestinal symptoms, drowsiness, ataxia, diplopia, headache, dizziness, hiccoughs, sedation, behavioural disturbances, acute psychotic reactions, extrapyramidal symptoms, blood dyscrasias, rash, lupus-like syndrome, other severe idiosyncratic reactions.
References: Katzung Basic and Clinical Pharmacology, 9th ed. The Treatment of Epilepsy, 3rd ed.

Valproic Acid
Primary indications: First line for atypical absence seizures. First-line therapy of idiopathic generalized epilepsies. First-line or adjunctive therapy of cryptogenic or symptomatic generalized epilepsies. Valuable but not generally first-line therapy for partialseizures
Mechanisms of action: Increases brain GABA activity by increasing activity of glutamic acid decarboxylase, inhibition of GABA transaminase, inhibition of succinic semialdehyde dehydrogenase
Usual dosages: Initial: 400–500 mg/day (adults); 15 mg/kg/day (children)
Maintenance: 500–2500 mg/day (adults); 20–40 mg/day (children under 20 kg); 20–30 mg/kg/day (children over 20 kg)
Dosing frequency: 2-3 times a day Serum level monitoring: Dosage usually can be adjusted on the
basis of clinical response, but monitoring serum valproic acid levels may be useful in selected cases.
References: Katzung Basic and Clinical Pharmacology, 9th ed. The Treatment of Epilepsy, 3rd ed.
Valproic Acid
Significant drug interactions : Enzyme-inducing drugs and imipenem antibiotics reduce serum valproic acid levels. Felbamate, stiripentol, isoniazid and other drugs may increase valproic acid levels. Valproic acid inhibits the metabolism of a number of drugs, most notably phenobarbital, lamotrigine and rufinamide. Valproic acid displaces phenytoin from plasma protein binding sites and may inhibit phenytoin metabolism at the same time
Common/important adverse effects: Tremor, sedation, asthenia, encephalopathy, extrapyramidal symptoms, nausea, vomiting, hyperammonemia, weight gain, polycystic ovary syndrome, hair loss, platelet and coagulation disorders, liver toxicity, pancreatitis, teratogenic effects (including spina bifida)
Main advantages: Unsurpassed efficacy in most generalized epilepsy syndromes. Broad spectrum efficacy in different seizure types
Main disadvantages: Weight gain, severe liver toxicity (particularly in children), teratogenicity
References: Katzung Basic and Clinical Pharmacology, 9th ed. The Treatment of Epilepsy, 3rd ed.

Other Modalities
Surgical Management– Surgical excision of epileptic foci in simple and
complex partial epilepsies that have not responded to intensive and prolonged medical therapy may be beneficial for some.
Regulation of Physical and Mental Activity– Precipitating factors need to be modified and
stressed to the patient.– Moderate amount of physical exercise can
also be advised.– Psychosocial difficulties need to be identified
and addressed early.Reference: The Treatment of Epilepsy, 3rd ed.
Other Modalities
Ketogenic Diet– biochemical alteration both in the blood and
in the brain– possible GABA-mimetic effects of ketosis
given the structural similarities of GABA, -hydroybutyrate and acetoacetate
Vagal Nerve Stimulation– vagal stimulation produces its effects are
unclear and it is done through attachment of electrodes to the vagus nerve at the left carotid bifurcation
Reference: The Treatment of Epilepsy, 3rd ed.
Management
American Academy of Neurology Guidelines on CESSATION OF TREATMENT
Stopping the treatment may be considered when:
The patient has been seizure-free for 2 to 5 years.
The patient has a single type of seizure. The patient has no abnormalities on neurologic
examination and has a normal IQ. The patient’s electroencephalogram (EEG) has
become normal.
CASE 2.2
CASE 2.2
A 17 year-old male had an excellent antiepileptic drug control of his generalized tonic-clonic seizures for the past 3 years. Work up done showed an abnormal EEG patterns consistent with generalized type of seizures and a normal cranial CT scan.

Missing Data
Initial presentation of the patient when diagnosis was established
Family history History of trauma, loss of consciousness, severe
headache Precipitating factors
Fever, stress, fatigue, sleep deprivation, drug abuse, alcohol Prodromal symptoms
Mood changes, sleep disturbances, lightheadedness, anxiety, irritability, difficulty concentrating
Compliance to anti-epileptic medications Frequency, duration and presentation of the patient
during the recent attack

Salient Features
17 year-old Male 3 year history of generalized tonic-clonic
seizures- controlled Abnormal EEG patterns consistent with
generalized type of seizures Normal cranial CT scan

Clinical Impression:Generalized Tonic Clonic Seizures, controlled

Generalized Seizures
Paroxysmal discharges occurring in both hemispheres
Reference: Rohkamm, Color Atlas of Neurology © 2004 Thieme
Convulsive
• Generalized tonic clonic
Nonconvulsive
• Myoclonic• Tonic or
Atonic• Absence

Generalized Seizures
CAUSES
Reference: Rohkamm, Color Atlas of Neurology © 2004 Thieme
Genetic
• Predisposition• Hereditary diseases
associated with epilepsies:• Tuberous sclerosis, • Sturge–Weber
syndrome• Mitochondrial
encephalopathies• Sphingolipidoses
Acquired
•Focal – possibly with secondary generalization•Bilateral •Diffuse – primary generalized epilepsies•The causes include developmental disorders, pyridoxine deficiency, hippocampal sclerosis, brain tumors, head trauma, cerebrovascular disturbances, alcohol, drug abuse, medications, and CNS infections.
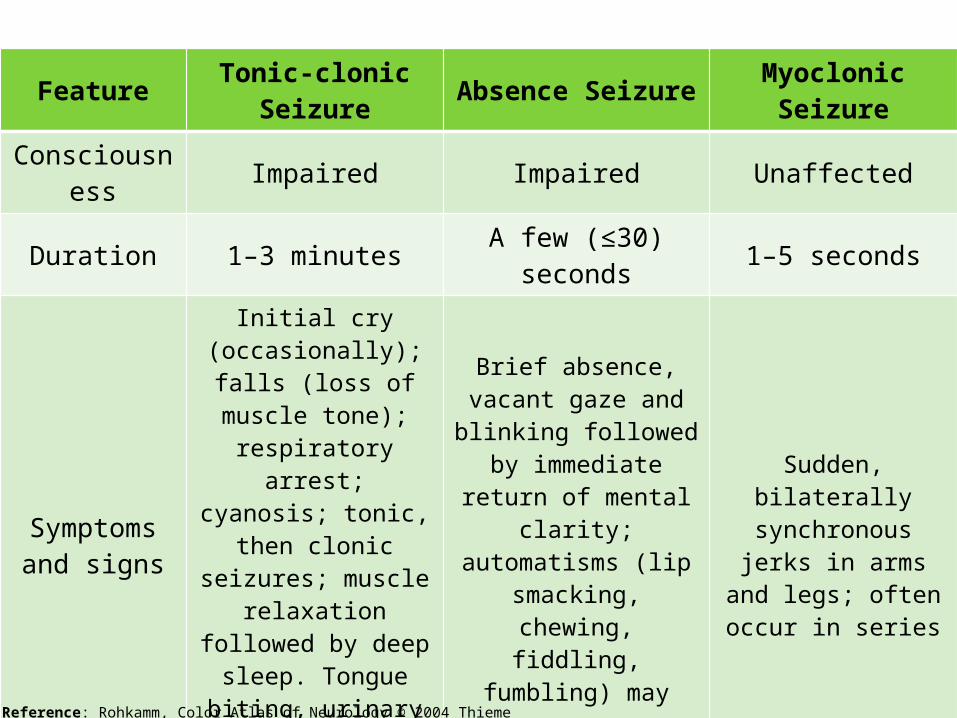
FeatureTonic-clonic
SeizureAbsence Seizure
Myoclonic Seizure
Consciousness Impaired Impaired Unaffected
Duration 1–3 minutesA few (≤30)
seconds 1–5 seconds
Symptoms and signs
Initial cry (occasionally); falls
(loss of muscle tone); respiratory arrest; cyanosis; tonic, then clonic seizures; muscle
relaxation followed by deep sleep. Tongue biting,
urinaryand fecal
incontinence
Brief absence, vacant gaze and
blinking followed by immediate return of
mental clarity; automatisms (lip
smacking, chewing, fiddling, fumbling)
may occur
Sudden, bilaterally synchronous jerks in arms and legs;
often occur in series
Age group Any ageChildren and adolescents
Children andadolescents
Ictal EEGOften obscured
by muscle artifacts
Bilateral regular 3 (2–4) Hz spike
waves
Polyspike waves, spike waves, or sharp and slow
waves
Reference: Rohkamm, Color Atlas of Neurology © 2004 Thieme

Myoclonic
Reference: Rohkamm, Color Atlas of Neurology © 2004 Thieme
Absence

Generalized Tonic-Clonic Seizure
A seizure involving the entire body. It is also called a grand mal seizure.
Usually involves muscle rigidity, violent muscle contractions, and loss of consciousness
They may occur in people of any age, as a single episode, or as part of a repeated, chronic condition (epilepsy).
Internationally, as in the United States, only a small proportion of seizures are generalized tonic-clonic seizures (20-25%).

Generalized Tonic-Clonic Seizure
Pathophysiology Thought to be initiated by 3 different
mechanisms: Abnormal response of hyperexcitable cortex to
initially normal thalamic input Primary subcortical trigger Abnormal cortical innervation from subcortical
structures A seizure results from a paroxysmal high-
voltage electrical discharge of susceptible neurons within an epileptogenic focus. These neurons are known to be hyperexcitable and, for unknown reasons, remain in a state of partial depolarization.

Generalized Tonic-Clonic Seizure
Pathophysiology GABA-ergic and hyperpolarized neurons
surrounding the epileptogenic focus inhibit the epileptogenic neurons.
At times, when the epileptogenic neurons overcome the surrounding inhibitory influence, the seizure discharge spreads to neighboring cortical structures and then to subcortical and brainstem structures.

Generalized Tonic-Clonic Seizure
Pathophysiology Brainstem structures involved:
Lateral geniculate body – produces a generalized tonic-clonic seizure when kindled in the cat
Ascending pathways through the mamillary bodies and anterior thalamus
Substantia nigra – includes a nigrotectal GABA-ergic projection and locus ceruleus
Phases: Tonic, Clonic, Post-ictal Tonic Phase - spread of excitability to subcortical,
thalamic, brainstem, and spinal cord structures Clonic phase – discontinuous bursts of electrical
activity brought about by the interruption of the tonic phase by an inhibitory impulse which starts from the thalamus

Generalized Tonic-Clonic Seizure
Tonic & Clonic Phases• Loss of consciousness or
fainting – 30 sec to 5 mins.• General muscle contraction
and rigidity (tonic phase) – 15-20 sec.
• Violent rhythmic muscle contraction and relaxation (clonic phase) – 1-2 mins.
• Biting the cheek/tongue, clenched teeth/jaw
• Incontinence• Stopped breathing or difficulty
breathing during seizure• Cyanosis
Post-ictal Phase
•Normal breathing•Sleepiness – 1 hr or longer•Loss of memory (amnesia) regarding events surrounding the seizure episode•Headache•Drowsiness •Confusion, temporary and mild•Weakness for up to 24 - 48 hours following seizure (Todd's paralysis)

Initial Diagnostic Evaluation CBC Blood chemistries Liver and thyroid function tests EEG Imaging study of the brain, preferably
MRI Video/EEG or prolonged EEG monitoring Other forms: cardiac stress tests, Holter
monitor, tilt-table testing, sleep studies

EEG
Initial Phase
•Movement artifacts obscure the EEG tracing.•(+) repetitive spikes or spike-wave discharges lasting a few seconds, followed by an approximately 10-s period of 10-Hz spikes.
Clonic Phase
•Spikes become mixed with slow waves •Then, EEG slowly assumes a polyspike-and-wave pattern.
Post-ictal Phase
•Nearly flat for a variable time•Brain waves then gradually resume their pre-seizure pattern.

Treatment

Choices of Antiepileptic Drugs by Type of Adult Seizure Disorders
SEIZURE TYPE INITIAL CHOICE SECOND LINE
Tonic-clonicCarbamazepine, valproate,
phenytoin
Lamotrigine, oxcarbazepine
Myoclonic ValproateTopiramate,
levetiracetam, zonisamide
PartialCarbamazepine,
phenytoin
Valproate, lamotrigine,
oxcarbazepine, levetiracetam
Absence ValproateEthosuximide,
lamotrigine
Unclassifiable Valproate Lamotrigine
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

General Principles of Treatment
The use of antiepileptic drugs is the most important factor of treatment.
Establish the diagnosis and rule out underlying pathology.
Classify seizure type, using EEG and clinical criteria. Because of the long half-lives of phenytoin,
phenobarbital, and ethosuximide, these drugs need be taken only once daily.
Valproate and carbamazepine have shorter half-lives, and their administration should be spaced during the day.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

General Principles of Treatment
Serum-protein binding characteristics of antiepileptic drugs and the interactions among these drugs and between antiepileptic and other drugs should be considered.
Initially, only one drug should be used and the dosage increased until sustained therapeutic levels have been attained.
If the first drug does not control seizures, a different one should be tried, but frequent shifting of drugs is not advisable.
In changing medication, the dosage of the new drug should be increased gradually to an optimum level while the dosage of the old drug is gradually decreased; the sudden withdrawal of a drug may lead to an increase in seizure frequency or status epilepticus.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.
General Principles of Treatment
Phenytoin, carbamazepine, and valproate are representative of antiepileptic drugs and are more or less equally effective in the treatment of both generalized and partial seizures.
Phenytoin and carbamazepine act by blocking sodium channels, thus preventing abnormal neuronal firing and seizure spread.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.
Phenytoin
Pediatric Dosage: 4-7 mg/kg Adult Dosage: 300-400 mg/day Oral, IM or IV Idiosyncratic phenytoin hypersensitivity: rash, fever,
lymphadenopathy, eosinophilia and other blood dyscrasias, and polyarteritis
Overdose: ataxia, diplopia, stupor, hirsutism, hypertrophy of gums, coarsening of facial features
Chronic use may be associated with peripheral neuropathy, some form of cerebellar degeneration.
Phenytoin should not be used with: disulfiram, chloramphenicol, sulfamethizole, phenylbutazone, or cyclosphosphamide
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Carbamazepine
Pediatric Dosage: 20-30 mg/kg Adult Dosage: 600-1200 mg/day This drug causes same effects with
phenytoin, but to a slightly lesser degree.
Mild leukopenia is common; pancytopenia, hyponatremia, diabetes insipidus are rare.
Oxcarbazepine, a more recently introduced analogue or carbamazepine, has fewer side effects, especially marrow toxicity.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Valproate
Pediatric Dosage: 30-60 mg/kg Adult Dosage: 1000-3000 mg/day All preparations are hepatotoxic. There has been evidence of weight gain
during the first months of therapy with valproate.
Menstrual irregularities and PCOS may appear in young women taking the drug.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Phenobarbital
Pediatric Dosage: 3-5 mg/kg Adult Dosage: 90-200 mg/day Still highly effective, but has many toxic
effects: drowsiness, mental dullness, nystagmus, staggering
Phenobarbital and primidone may provoke behavioral problems in retarded children.
It is still used to advantage as an adjunctive anticonvulsant and as a primary therapy in infantile seizures.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Lamotrigine
Pediatric Dosage: 0.5 mg/kg Adult Dosage: 300-500 mg/day Lamotrigine closely resembles phenytoin in its
antiseizure activity but has different features relating to toxicity.
It selectively blocks the slow sodium channels, thereby preventing the release of the excitatory neurotransmitters glutamate and aspartate.
It is effective as a first-line and adjunctive drug for generalized and focal seizures.
It does not provoke weight gain and ovarian problems.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Discontinuation of Anticonvulsants
Withdrawal of anticonvulsant drugs may be undertaken in patients who have been free of seizures for a prolonged period.
If the EEG tracing is abnormal by way of showing paroxysmal activity, it is generally better to continue treatment.
Callaghan et al. In patients who had been seizure-free during 2 years of
treatment with a single drug, 1/3 relapsed after discontinuation of the drug.
This relapse rate was much the same in adults and children and whether the drug was reduced over a period of weeks or months.
Relapse rate was lower in patients with absence and generalized onset seizures than in patients with complex partial seizures and secondary generalization.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Discontinuation of Anticonvulsants
Specchio et al. After 2 years on a single anticonvulsant
during which no seizures had occurred, the rate of relapse was 40% 2.5 years later and 50% at 5 years after discontinuation.
This compared to a seizure recurrence rate of 20% for patients remaining on medication.
A longer seizure-free period is associated with a lesser rate of relapse.
Reference: Adams and Victor’s Principles of Neurology, 9th Edition.

Prognosis
With treatment, seizures are eliminated in one-third of patients with epileptic seizures, and frequency of seizures is reduced by > 50% in another one-third. About 60% of patients whose seizures are well-controlled by drugs can eventually stop the drugs and remain seizure-free.
Sudden unexplained death in epilepsy (SUDEP) is a rare complication of unknown cause.
Reference: http://www.merck.com/mmpe/sec16/ch214/ch214a.html

CASE 2.3

CASE 2.3
An 11 month-old male infant was rushed to the hospital because of first-onset and single episode of generalized seizure.
The infant was noted to be coughing with nasal catarrh for the last 5 days. Hours before the seizure episode, his temperature was taken to be 38.9C. Perinatal and postnatal histories were unremarkable.
The father admitted to be having the same episodes when he was still around 5 years old during the height of his fever. Neurological examination was normal.

Salient Features
11 months old Male
Recent URI
Spike in body temp
38.9 °C
(+)Family history
Normal Neuro Exam

Missing Data
Duration of the seizure episode If there are other accompanying
symptoms such as vomiting, loss of consciousness, urinating or soiling himself.
Recent vaccination (DTP or MMR)

Clinical Impression:Febrile Seizure

Differential Diagnosis

DIFFERENTIAL DIAGNOSIS1. Meningitis2. Encephalitis3. Epilepsy

MENINGITIS
An inflammation of the membranes (meninges) and cerebrospinal fluid surrounding the brain and spinal cord, usually due to the spread of an infection.
The swelling associated with meningitis often triggers the "hallmark" symptoms of this condition, including headache, fever and a stiff neck.

MENINGITIS
• Most cases of meningitis are caused by a viral infection, but bacterial and fungal infections also can lead to meningitis.– Bacterial infections are the most damaging,
identifying the source of the infection is an important part of developing a treatment plan.
• Depending on the cause of the infection, meningitis can resolve on its own in a couple of weeks — or it can be a life-threatening emergency.

Acute Bacterial Meningitis
Usually occurs when bacteria enter the bloodstream and migrate to the brain and spinal cord.
Can directly invade the meninges, as a result of an ear or sinus infection or a skull fracture.

Acute Bacterial Meningitis
– Streptococcus pneumoniae• Most common cause of bacterial meningitis in
infants and young children in the United States.
– Neisseria meningitidis• Another leading cause of bacterial meningitis.• It commonly occurs when bacteria from an upper
respiratory infection enter your bloodstream.• Highly contagious and may cause local epidemics
in college dormitories and boarding schools and on military bases.

Acute Bacterial Meningitis
– Haemophilus influenzae• Before the 1990s, Haemophilus influenzae type b (Hib)
bacterium was the leading cause of bacterial meningitis. • Hib vaccines —routine childhood immunization
– Greatly reduced the number of cases of this type of meningitis
• It tends to follow an upper respiratory infection, ear infection (otitis media) or sinusitis.
– Listeria monocytogenes• These bacteria can be found almost anywhere — in soil, in
dust and in foods that have become contaminated– Soft cheeses, hot dogs and luncheon meats
• Most healthy people exposed to listeria don't become ill– Pregnant women, newborns and older adults tend to be more
susceptible.
• Listeria can cross the placental barrier, and infections in late pregnancy may cause a baby to be stillborn or die shortly after birth.
MENINGITIS
• Viral meningitis– Usually mild and often clears on its own within two
weeks– A group of common viruses known as enteroviruses are
responsible for about 90 percent of viral meningitis in the United States
– Most common signs and symptoms: Rash, sore throat, joint aches and headache
– “Worst headache I've ever had”
• Chronic meningitis– Ongoing (chronic) forms of meningitis occur when slow-
growing organisms invade the membranes and fluid surrounding the brain
– Although acute meningitis strikes suddenly, chronic meningitis develops over four weeks or more
– Signs and symptoms: Headaches, fever, vomiting and mental cloudiness
– Rare

MENINGITIS
• Fungal meningitis– Relatively uncommon – Cryptococcal meningitis
• Fungal form of the disease that affects people with immune deficiencies, such as AIDS
– Life-threatening if not treated with an antifungal medication
• Other Causes– Meningitis can also result from noninfectious
causes, such as drug allergies, some types of cancer and inflammatory diseases such as lupus.

Reference: Harrison’s Principles of Internal Medicine, 17th Edition.

CASE• II month old male infant• First onset and single
episode of generalized seizure
• coughing with nasal catarrh for the last 5 days
• T = 38.9C• Perinatal and postnatal
histories were unremarkable• The father admitted to be
having the same episodes when he was still around 5 years old during the height of his fever
• Neurological examination was normal
MENINGITIS
•History of infection•Classic triad of fever, headache, and nuchal rigidity•(+) Kernig's sign and Brudzinski's sign•Decreased level of consciousness occurs in >75% of patients and can vary from lethargy to coma•Nausea, vomiting, and photophobia are also common complaints•Seizures•Raised ICP •Reduced level of consciousness, papilledema, dilated poorly reactive pupils

ENCEPHALITIS
• “Inflammation of the brain," it usually refers to brain inflammation resulting from a viral infection.– Primary encephalitis
• Involves direct viral infection of the brain and spinal cord– Secondary encephalitis
• A viral infection first occurs elsewhere in the body and then travels to the brain
• In contrast to viral meningitis, where the infectious process and associated inflammatory response are limited largely to the meninges, in encephalitis the brain parenchyma is also involved.
ENCEPHALITIS
• It can be caused by:– Bacterial infection
• Spreads directly to the brain (primary encephalitis)• Bacterial meningitis
– A complication of a current infectious disease • Syphilis (secondary encephalitis)
– Parasitic or protozoal infestations• Can also cause encephalitis in people with compromised
immune systems• Such as toxoplasmosis, malaria, or primary amoebic
meningoencephalitis– Lyme disease and/or Bartonella henselae may also
cause encephalitis

CASE• II month old male infant• First onset and single
episode of generalized seizure
• Coughing with nasal catarrh for the last 5 days
• T = 38.9C• Perinatal and postnatal
histories were unremarkable• The father admitted to be
having the same episodes when he was still around 5 years old during the height of his fever
• Neurological examination was normal.
ENCEPHALITIS
• History of infection• Fever, headache and nuchal
rigidity• (+) Kernig’s and
Brudzinski’s sign• Photophobia and seizures• Altered level of
consciousness• Evidence of either focal or
diffuse neurologic signs and symptoms• Focal findings are aphasia,
ataxia, upper or lower motor neuron patterns of weakness, involuntary movements and cranial nerve deficits
• Hallucinations, agitation, personality change, behavioral disorders, and, at times, a frankly psychotic state

EPILEPSY
Classified as a disorder of at least two unprovoked recurrent seizures.
More common in young and old, plateau at 2nd – 4th decades of life
In children (0-14 years old)congenital> trauma=infection>CVA=tumor

EPILEPSY
Genetic Predispostion The direct result of a known or presumed
genetic defect in which seizures are the core symptom of the disorder. Examples include childhood absence epilepsy,
autosomal dominant nocturnal frontal lobe epilepsy, and Dravet syndrome.

EPILEPSY
Epileptic Seizures No sexual predisposition, may occur at any
age. Loss of consciousness is common. Onset is usually abrupt and may have a
short aura. Vocalization is present during automatism.

Dravet’s Syndrome
Severe myoclonic epilepsy of infancy (SMEI)
Generalized epilepsy syndrome Onset is in the first year of life. Peaks at about 5 months of age with
febrile hemiclonic or generalized status epilepticus.
Boys are twice as often affected as girls. Prognosis is poor.
Most cases are sporadic. Family history of epilepsy and febrile
convulsions is present in around 25 percent of the cases.
Known causative genes are the sodium channel α subunit genes SCN1A and SCN2A, an associated β subunit SCN1B, and a GABAA receptor γ subunit gene, GABRG2.
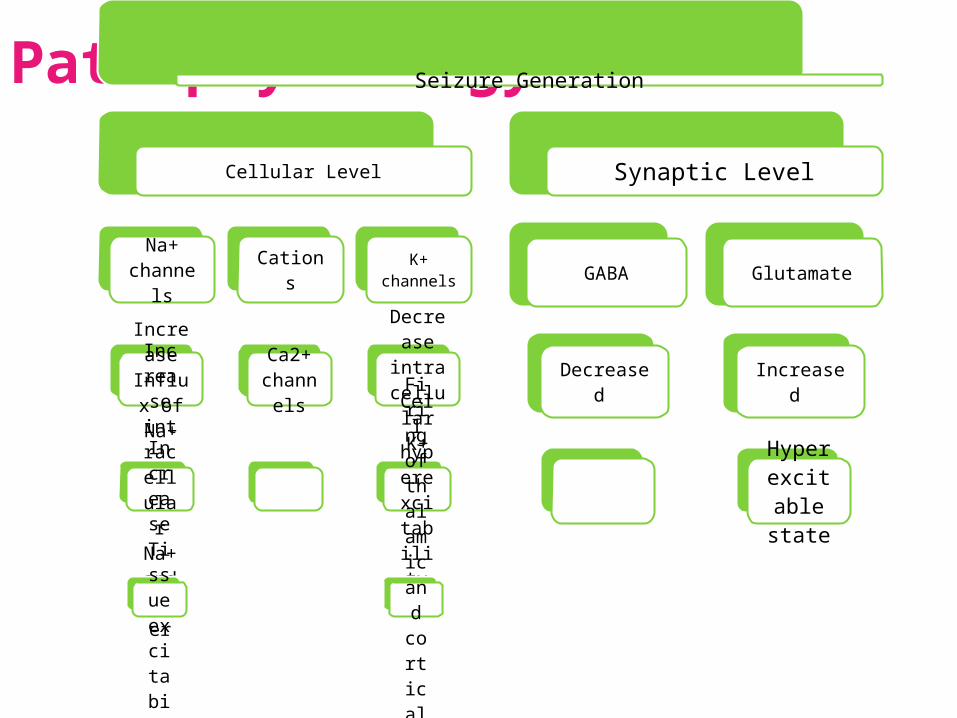
PathophysiologySeizure Generation
Cellular Level
Na+ channel
s
Increase
Influx of
Na+
Increase
intracellular Na+ and water
Increase
Tissue excitability
Cations
Ca2+ chann
els
K+ channels
Decrease
intracellular K+Cell hyperexcitabilit
y
Firing of thalamic
and
cortical neurons
Synaptic Level
GABA
Decreased
Glutamate
Increased
Hyperexcita
ble state

CASE
•II month old male infant•First onset and single episode of generalized seizure•Coughing with nasal catarrh for the last 5 days•T = 38.9C•Perinatal and postnatal histories were unremarkable.•The father admitted to be having the same episodes when he was still around 5 years old during the height of his fever.•Neurological examination was normal.
DRAVET’S SYNDROME
•Onset is in the 1st year of life.•Peaks at about 5 months of age with febrile hemiclonic or generalized status epilepticus
•Boys are twice as often affected as girls.•(+)Family History

Febrile Seizures

Febrile Seizure
Most common type of seizure that occurs during childhood that is associated with a febrile illness not caused by an infection of the central nervous system (CNS), without previous neonatal seizures or a previous unprovoked seizure, and not meeting the criteria for other acute symptomatic seizures (International League Against Epilepsy).
Rare before 9 months and after 5 years of age The peak age of onset is 14-18 months. A strong family history of febrile convulsions in siblings
and parents suggests a genetic predisposition. In a child with febrile seizure, the risk of febrile
seizure is 10% for the sibling and almost 50% for the sibling if a parent has febrile seizures as well.
References: Nelson’s Pediatrics 18th ed. and eMedicine.medscape.com

Febrile Seizure
Febrile seizures are not associated with reduction in later intellectual performance, and most children with febrile seizures have only a slightly greater risk of later epilepsy than the general population.
Usually it takes the form of a single, generalized motor seizure occurring as the temperature rises or reaches its peak.
Seldom does the seizure last longer than a few minutes.
By the time an EEG can be obtained, there is usually no abnormality.
Recovery is complete.References: Nelson’s Pediatrics 18th ed. and eMedicine.medscape.com

Risk Factors
Family history of febrile seizures High temperature Parental report of developmental delay Neonatal discharge at an age greater than
28 days (suggesting perinatal illness requiring hospitalization)
Daycare attendance Presence of 2 of these risk factors
increases the probability of a first febrile seizure to about 30%.
Maternal alcohol intake and smoking during pregnancy has a 2-fold increased risk.
References: Nelson’s Pediatrics 18th ed. and eMedicine.medscape.com
Types of Febrile Seizure
Simple Associated with a core temperature that
increases rapidly to ≥39°C. It is initially generalized and tonic-clonic in
nature. Lasts a few seconds and rarely <15 mins. Followed by a brief postictal period of drowsiness. Occurs only once in 24 hrs.
Complex Duration is >15 mins. Focal seizure activity or focal findings are present
during the postictal period. Repeated convulsions occur within 24 hrs.References: Nelson’s Pediatrics 18th ed. and
eMedicine.medscape.com

Recurrent Seizures
• Approximately 30–50% of children have recurrent seizures with later episodes of fever and a small minority has numerous recurrent febrile seizures.
• Risk factors for recurrent febrile seizures include the following:– Young age at time of first febrile seizure <12 mos.– Relatively low fever at time of first seizure– Family history of a febrile seizure in a first-degree
relative– Brief duration between fever onset and initial seizure– Multiple initial febrile seizures during same episode
• Patients with all 4 risk factors have greater than 70% chance of recurrence. Patients with no risk factors have less than a 20% chance of recurrence.
References: Nelson’s Pediatrics 18th ed. and eMedicine.medscape.com

Pathophysiology
• Febrile seizures occur in young children at a time in their development when the seizure threshold is low.
• This is a time when young children are susceptible to frequent childhood infections such as upper respiratory infection, otitis media, viral syndrome, and they respond with comparably higher temperatures.
• Animal studies suggest a possible role of endogenous pyrogens, such as interleukin 1beta, that, by increasing neuronal excitability, may link fever and seizure activity.
• Preliminary studies in children appear to support the hypothesis.
References: Nelson’s Pediatrics 18th ed. and eMedicine.medscape.com

Febrile Seizures
History• The type of seizure (generalized or focal) and its
duration should be described to help differentiate between simple and complex febrile seizures.
• Focus on the history of fever, duration of fever, and potential exposures to illness.
• A history of the cause of fever (eg, viral illnesses, gastroenteritis) should be elucidated.
• Recent antibiotic use is particularly important because partially treated meningitis must be considered.
• A history of seizures, neurologic problems, developmental delay, or other potential causes of seizure (eg, trauma, ingestion) should be sought.
Febrile Seizures
Physical Examination The underlying cause for the fever should be sought. A careful physical examination often reveals otitis
media, pharyngitis, or a viral exanthem. Serial evaluations of the patient's neurologic status are essential. Check for meningeal signs as well as for signs of trauma or toxic
ingestion.

CASE
•II month old male infant•First onset and single episode of generalized seizure•Coughing with nasal catarrh for the last 5 days•T = 38.9C•Perinatal and postnatal histories were unremarkable.•The father admitted to be having the same episodes when he was still around 5 years old during the height of his fever.•Neurological examination was normal.
FEBRILE SEIZURES
•History of infection•Ages of 3 months and 5 years•Twice more common in boys than girls•Fever and seizures

Management

Diagnostics
To determine the cause of the fever To rule out meningitis or encephalitis
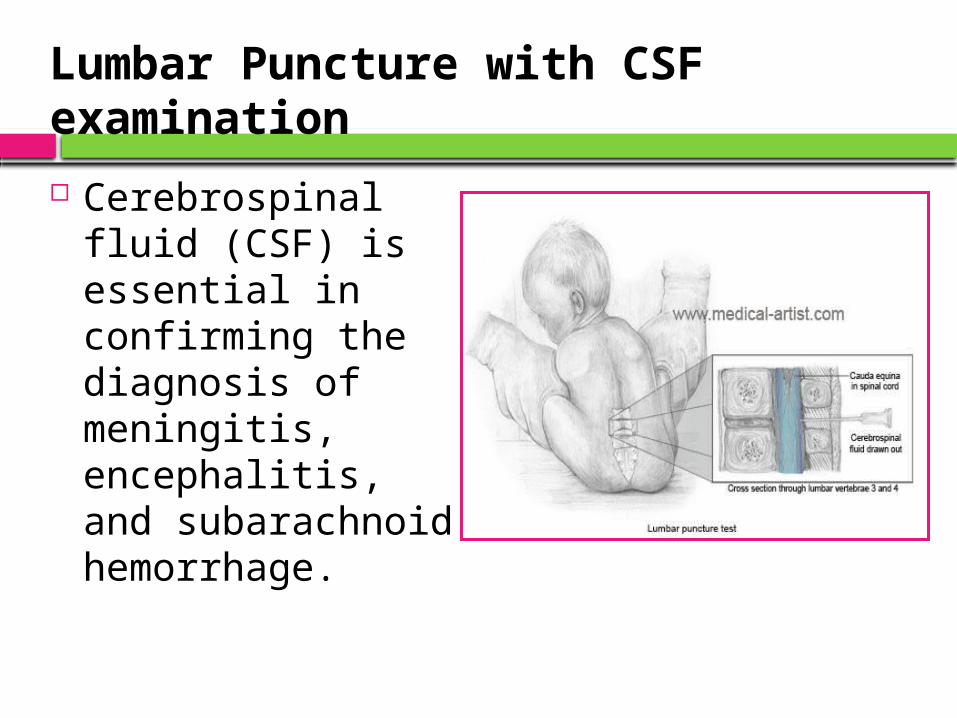
Lumbar Puncture with CSF examination Cerebrospinal fluid
(CSF) is essential in confirming the diagnosis of meningitis, encephalitis, and subarachnoid hemorrhage.

Lumbar Puncture with CSF Examination Contraindications:
Elevated ICP owing to a suspected mass lesion of the brain or spinal cord
Symptoms and signs of pending cerebral herniation in a child with probable meningitis
Critical illness Skin infection at the site of the LP Thrombocytopenia

Lumbar Puncture with CSF examination
WBC Protein Sugar Others
Normal
0-5 lymphocyte
15-45
50-75>50%
of blood sugar
Clear
Acute bacteri
al
High neutrophil→ (after 5 days)
lymphocytes
High Low Turbid
Viral N or
slight increase
Clear
TBHigh
lymphocytes
High Low <40
Xanthochromic
EEG
Not recommended after an initial simple febrile seizure in children with a normal neurologic examination.
Typically does not identify specific abnormalities or help predict recurrent seizures.
Consideration of EEG if febrile seizures are complex or recurrent.
Reference: http://www.merck.com/mmpe/sec19/ch283/ch283c.html

Treatment
Treatment for Nasal Catarrh
• Pseudoephedrine/Dextromethorphan can be given for the cough and decongesting the airways of the infant.
• It works by constricting blood vessels and reducing swelling in the nasal passages, which helps you to breathe more easily. The cough suppressant works in the brain to help decrease the cough reflex.
• However, you should not use decongestants for more than 5-7 days at a time. This is because they can only provide short-term relief for catarrh, and using them for any longer can make your symptoms worse.

Medical Treatment
Treatment of infants with seizures is different than treatment for adults. Unless a specific cause is found, most infant with first-time seizures will not be placed on medications.

Medical Treatment
• Phenobarbital - Enhances the inhibitory actions of gamma-aminobutyric acid (GABA) on neurons. - Decreases the occurrence of subsequent febrile seizures.- Oral Dosage (as recommended by the American Academy of Pediatrics): 1 to 3 mg/kg.
Medical Treatment
Benzodiazepine• Centrally acting muscle
relaxant. • Gel, rectal 2.5 mg (pediatric)• Anticonvulsant properties
may be in part or entirely due to binding to voltage-dependent sodium channels.
• It can reduce the risk of subsequent febrile seizures.
• Because it is given intermittently, this therapy probably has the fewest adverse effects. If preventing subsequent febrile seizures is essential, this would be the treatment of choice.

Medical Treatment
• Paracetamol (Acetaminophen)- Inhibits prostaglandins in CNS, but lacks anti-inflammatory effects in periphery; reduces fever through direct action on hypothalamic heat-regulating center.
-15 mg/kg; taken once every 4 hours, up to 4 times per day if needed

Prevention

Prevention
• Most seizures cannot be prevented.
• There are some exceptions, but these are very difficult to control, such as head trauma and infections during pregnancy.
• Children who are known to have febrile seizures should have their fevers well controlled when sick.

Prevention
The best way to prevent fevers is to reduce the infant's exposure to infectious diseases.
Hand-washing is the single most important prevention measure for people of all ages.
Prevention
If another seizure ensues: • The initial efforts should be
directed first at protecting the infant from additionally injuring himself.
• Lie down the infant.• Remove glasses or other
harmful objects in the area.• Do not try to put anything in
mouth. In doing so, it may injure the infant.
• Immediately check if the infant is breathing. Call a doctor or proceed to the nearest hospital.
CASE 2.4

Case 2.4
A 30 year-old female patient has been maintained on phenytoin 100 mg TID for the past 5 years with good control of her idiopathic generalized seizure. She is 3 months pregnant when she visited your clinic.
Missing Data
• (+) / (-) Frequency and Severity Associated with: • Subtherapeutic anticonvulsant levels
• Nausea and vomiting leads to missed doses.• Expanded intravascular volume lowers serum
drug levels.• Hepatic, plasma and placental enzymes
increase drug metabolism.• Increased glomerular filtration hastens drug
clearance.

Missing Data
• (+) / (-) Frequency and Severity Associated with: • Lower seizure threshold• “Exhaustion from sleep deprivation”
Missing Data
• (+) / (-) Diabetes• (+) / (-) Hypertension• (+) / (-) Intake of folic acid

Salient Features
3o year old female
1st trimester of pregnancy
Phenytoin 100mg TID for
the past 5 years

Clinical Impression:Idiopathic Generalized Seizure Disorder

Generalized Tonic Clonic Seizure• Prodromal symptoms
– Occurring hours or days before a seizure.– Mood changes, sleep disturbances,
lightheadedness, anxiety, irritability, difficulty concentrating and, rarely, an ecstatic feeling, abdominal pain, facial pallor, or headache. Most patients lose consciousness without any premonitory symptoms.
– Patients with generalized tonic-clonic seizures do not have auras. An aura represents a simple partial seizure.

Generalized Tonic Clonic Seizure• The patient may have completely nonfocal
findings on neurologic examination when not having seizures. Seizures typically are divided into tonic, clonic, and postictal phases.– Tonic phase
• The tonic phase begins with flexion of the trunk and elevation and abduction of the elbows. Subsequent extension of the back and neck is followed by extension of arms and legs. This can be accompanied by apnea, which is secondary to laryngeal spasm.

Generalized Tonic Clonic SeizureAutonomic signs are common during this phase and include increase in pulse rate and blood pressure, profuse sweating, and tracheobronchial hypersecretion.Although urinary bladder pressure rises, voiding does not occur because of sphincter muscle contraction.This stage lasts for 10-20 seconds.

Generalized Tonic Clonic Seizure
– Clonic phase• The tonic stage gives way to clonic convulsive
movements, in which the tonic muscles relax intermittently, lasting for a variable period of time.
• A generalized tremor occurs at a rate of 8 tremors per second, which may slow down to about 4 tremors per second. Each spasm is accompanied by pupillary contraction and dilation. Some patients may have tongue or cheek bites.
• The atonic periods gradually become longer until the last spasm. Voiding may occur at the end of the clonic phase as sphincter muscles relax. The atonic period lasts about 30 seconds. The patient continues to be apneic during this phase.
• The convulsion, including tonic and clonic phases, lasts for 1-2 minutes.
Generalized Tonic Clonic Seizure
– Postictal state• A variable period of unconsciousness during
which the patient becomes quiet and breathing resumes.
• The patient gradually awakens, often after a period of stupor or sleep, and often is confused, with some automatic behavior.
• Headache and muscular pain are common. The patient does not recall the seizure itself.

Generalized Tonic Clonic Seizure• Most generalized epilepsies are idiopathic,
but a definite genetic locus has been found for some of these generalized types of epilepsy.

SUBTYPE MANIFESTATIONS
Absence seizure Brief staring spells with arrest of activity, often w/ eye fluttering, which just
last a few seconds
Myoclonic seizure Very brief isolated body jerks that tend to occur in
the morning
Generalized tonic-clonic seizure
Convulsions of the whole body lasting 1-2 minutes
History
• Unusual sensations suggesting an aura
• Seizure manifestations

History
• Ask about the first and any subsequent seizures.• Duration• Frequency• Sequential evolution• Longest & shortest interval between seizures• Aura• Postictal state• Precipitating factors

History
• Risk factors• Prior head trauma or CNS infection• Drug use or withdrawal • Alcohol withdrawal• Non-adherence to anticonvulsants• Family history of seizures or neurologic disorders
• Rare triggers• Repetitive sounds• Flashing lights• Touching certain parts of the body
• Sleep deprivation• Can lower the seizure threshold

Physical Examination
A bitten tongue, incontinence (eg., urine or feces in clothing), or, in patients who have lost consciousness, prolonged confusion, suggest seizure.
Physical examination rarely indicates the cause when seizures
are idiopathic but may provide clues when seizures are
symptomatic.

Intellectual functions, neurologic exam and imaging (MRI) are normal.

Diagnostic evaluation must determine whether the event was a seizure vs. pseudoseizure or syncope.

EEG
• The only definitive test to confirm the diagnosis.
• Represents a recurrent, sudden, excessive discharge of cortical neurons.
• When abnormal, it’s very characteristic:• Interictal symmetric
bursts of 4- to 7-Hz epileptiform activity
• Interictal spike-and-wave abnormalities without any clinical seizure activity

SUBTYPE EEG CHANGES
Absence seizure Very characteristic pattern wave
complexes
Myoclonic seizure Bilateral polyspike and wave
abnormality at a rate of 4- to 6-Hz
Generalized tonic-clonic seizure
Can show either of the above patterns
or generalized spikes
EEG of the Subtypes of Generalized Seizure
Seizure and Pregnancy

Seizure and Pregnancy
• A woman with a seizure disorder can carry a pregnancy safely.
• Seizures can harm the developing fetus by reducing the blood supply to the placenta.
• For most pregnant women who have epilepsy, seizures remain the same. For a few, seizures become less frequent. For others — particularly women who have poorly controlled epilepsy — pregnancy increases the number of seizures.

Complications
• Severe morning sickness• Anemia• Vaginal bleeding during
and after pregnancy• Abruptio placenta• Pre-eclampsia• Premature baby• LBW baby

Complications
The occurrence of seizures in the first trimester poses the greatest risk of congenital malformation and developmental delay in the offspring.
For babies whose mothers take seizure medication, the risk of birth defects is 4 to 8 percent — compared with 2 to 3 percent for all babies.

An antifolate effect on blood and interference with vitamin K metabolism have been reported, for which reason pregnant women taking phenytoin should be given vitamin K before delivery and the newborn infant should receive vitamin K as well to prevent bleeding.

The obstetrician and neurologist should work together prior to conception and throughout the pregnancy to closely monitor seizures and contributing factors (eg., sleep deprivation and medication compliance).

AEDs & Pregnancy
Phenytoin
• Fetal hydantoin syndrome– craniofacial anomalies, distal digital
hypoplasia, epicanthal folds, hypertelorism, low-set ears, and developmental delay
• Mothers who received phenytoin monotherapy during pregnancy demonstrated slightly delayed locomotor development.

Phenobarbital
Fetal hydantoin syndrome and fetal alcohol syndrome

Valproic Acid
Syndrome of specific craniofacial abnormalities and long, thin digits with hyperconvex nails
Neural tube defects

Carbamazepine
Craniofacial abnormalities and hypoplastic nails
Neural tube defects and cardiac abnormalities
Trimethadione
Epicanthal folds, low-set ears, microcephaly, short stature, and irregular teeth
Rarely used in the treatment of epilepsy and should certainly be discontinued during pregnancy

Prevention and Treatment

Phenytoin: Fetal Hydantoin Syndrome
A 30 year-old female patient has been maintained on phenytoin 100 mg TID for the past 5 years with good control
of her idiopathic generalized seizure. She is 3 months pregnant when she visited your clinic.
Because exposure to multiple antiepileptic drugs (AEDs) seems to be more teratogenic than monotherapy, patients are advised to switch to a single AED prior to conception and taper to the lowest possible dose.

Supplemental folate has been shown to decrease neural tube defects in patients without epilepsy and decrease other congenital anomalies in women with epilepsy. 4 mg of folic acid should be taken daily starting two to three months
prior to pregnancy and be continued through the first
trimester.

A fetal echocardiogram should be performed at 19 to 20 weeks’ gestation with careful attention to cardiac anomalies.
Because of the increased risk neural tube defects, a maternal serum AFP and acetylcholinesterase screening test should be offered.

Preconceptual Management of Women With Epilepsy
Attempt to decrease pharmacotherapy to monotherapy.
Taper dosages of AEDs to the lowest possible dose.
In women who have not had a seizure for 2-5 years, attempt complete withdrawal of pharmacotherapy.
Establish the level of total and free AEDs necessary for achieving good clinical control.
Consider preconceptual genetic counseling.
Supplement the diet with folate at 4 mg/d.

Management of Women With Epilepsy During Pregnancy
Check total and free levels of AEDs monthly.
Consider early genetic counseling. Check maternal MSAFP levels and
perform a level II fetal survey and ultrasonography at 19-20 weeks' gestation.
Consider amniocentesis for alpha-fetoprotein and acetylcholinesterase.

Gabapentin, lamotrigine, felbamate, topiramate, and oxcarbazepine These newer anticonvulsants have not been
studied extensively in pregnancy, though the use of pregnancy registries for AEDs are providing larger sample sizes.
The benefits and risks between congenital anomalies and seizure control needs to be considered when preparing the women with epilepsy for pregnancy.
The new anticonvulsants generally have a better pharmokinetic profile and are not metabolized to known teratogens.
All of these anticonvulsants are considered US Food and Drug Administration pregnancy category C. Of note, they are still known to both cross the placenta and into breast milk.
Thank you.


![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://static.fdocuments.us/doc/165x107/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)