Neurologic*Localizaon*for*M3s - Nigel FongWhatIwill*do * •...
68
Neurologic Localiza.on for M3s Eugene Gan
Transcript of Neurologic*Localizaon*for*M3s - Nigel FongWhatIwill*do * •...

Neurologic Localiza.on for M3s
Eugene Gan



What I will not do
• Run through the details of M1 and M2 neuroanatomy
• Give a lecture about all the details of various neurological condi.ons

What I will do
• Deliver an approach to a pa.ent that integrates condi.ons related to the nervous system across all 5 pos.ngs in M3
• Outline clinically important aspects of neuroanatomy that will aid in making a diagnosis
• Show you how to build an algorithm for neurologic localiza.on
• How to wire all these into your physical examina.on steps

Reality Check
• OSCE Short Cases -‐ Examine either UL, LL or CN -‐ Examiner determines where you examine • OSCE Long Case/Real Life -‐ To examine whatever part of the neurological system succintly to arrive at a diagnosis.
-‐ History determines where you examine

Outline
• Approach to diagnosis in Neurology • Clinically Relevant Neuroanatomy • Algorithms and Physical Examina.on

History, physical examina3on Obtain signs & symptoms Syndromic diagnosis Movement (including coordina.on & fluidity)
Soma.c senses (touch, temperature, propriocep.on, nocicep.on) Special senses (vision, hearing, balance, smell, taste) Consciousness (including epilepsy) Intellect (including behaviour, language) Mood (including autonomic, endocrine)
Anatomic diagnosis ‘Where’
Pyramidal System: Brain all the way to muscle Cerebellar system Extrapyramidal: Basal ganglia and others Limbic and hypothalamic Cerebral cortex Sensory system: Receptor all the way to thalamus and sensory cortex
Ae3ologic diagnosis ‘What’
VITAMIN CD
Func3onal diagnosis Disability, Ac.vity, Par.cipa.on
Approach to diagnosis in Neurology

Diagrams of Neuroanatomical Framework




Clinically Important
NEURO ANATOMY

What is an algorithm? • It should be a dichotomy (if not 3 to 4 branches at the MOST) • Comprehensive (At every branch-‐out, check back to see if you
have covered all aspects of the heading) • High Yield – Can be dichotomized based on a clinical tool,
minimal overlap of condi.ons between categories • Logical -‐ Should follow the sequence of your thought process/
physical examina.on • Portable – Simple, pocket sized, not too difficult to remember
at the bedside
• There are always caveats

Motor System
• Pyramidal à Gross Ac.on • Extra-‐pyramidal à Fluidity • Cerebellar à Coordina.on

hbp://ebooks.sinauer.com/blumenfeld2e/text.php

Spinal Reflex Arc
hbps://figures.boundless.com/5249/full/gy-‐of-‐animals-‐a-‐reflex-‐arc.jpe
UMN from Cerebral Cortex

Cranial Reflex Arc
• Who here has seen a stroke pa.ent with a UMN CN 5/9/10/11 palsy?
• Besides Facial Nerve (lower half of motor nucleus) and Hypoglossal nerve, all other cranial nerve nuclei have bilateral innerva.on.


Examples of Reflex Arcs Spinal -‐ Anal Sphinctor Tone (S2-‐S4) -‐ Babinski, Ankle Jerk (S1) -‐ Cremasteric Reflex (L2) -‐ Hoffman’s (C8) -‐ Triceps (C7-‐8) -‐ Biceps & Brachioradialis (C5-‐6) Cranial -‐ Gag Reflex (CN IX-‐X) -‐ VOR (CV XIII – CN III/IV/VI) -‐ Corneal Reflex (CN V1 – VII) -‐ Jaw Jerk Reflex (CN V3 – VII) -‐ Pupilliary Light Reflex (CN II-‐III)

Teaching points about reflexes 1) Reflexes do not breach consciousness (Brain stem as a repository of CN nuclei)
2) An hyper-‐reflexic jerk (Nuclear) should prompt you to think upwards (Supra-‐nuclear)
3) A hypo-‐reflexic jerk should prompt you to think of -‐ Afferent -‐ Efferent

Pa.ent

Case 1 • His back pain started just last night. Both LL were weak and reflexes were down bilaterally – Where is the lesion?
• His back pain has been going on for the past 3 You no.ced his R lower limb was weak, and reflexes were down, the other leg was fine. Before you proceed on from the motor examina.on – Where could the lesion be?
• What if his back pain had been going on for 1 week reflexes were up on the R leg?
• What is the tone of the anal sphinctor in each of these clinical situa.ons?
• If I told you he was having an early morning headache and vomi.ng in the past 4 weeks and your examina.on findings were the same (BL LL Hyper-‐reflexia)

Cord Lesions
• Most onen Bilateral • Associated with a sensory level • Onen associated with bladder and bowel symptoms


Cerebral Cortex

Case 2 For some reason he was just not paying aben.on you and you only really got his aben.on when you went over to the len side of the bed. Both of his eyes were looking to the len as well. You tried to ask how he was doing, but for some reason, he had a lot of difficulty understanding you and when he replied you it completely made no sense. Where is the lesion? He says hey hello Doctor so nice of you to come and visit me. It’s terrible though, I seem to be seeing two of you and it’s so irrita.ng! He covers one eye and feels a lot more comfortable and you guys proceed to con.nue your chat. He tells you he will invite you the next Hari Raya to feast and you remind him not to eat too many fried chicken wings. Where is the lesion?

Pyramidal Tract
Corona Radiata
Internal Capsule

Cerebellar System
• What are the inputs? • Draw a broad idea of the pathway • Truncal vs. Peripheral

Brain Lesions
• Usually Unilateral signs (unless bilateral hemispheric condi.ons)
• Cor.cal vs. Subcor.cal vs. Brain Stem

Approach to UMN pabern of weakness
Unilateral
UL involved?
Below C8 C8 and above
T7 – T12
All absent?
Above T7
Bilateral
Para-‐Saggital Meningioma
Yes No Test Reflexes
in Ascending Fashion

Approach to UMN pabern of weakness
Unilateral
Cor.cal
Cor.cal Signs?
Contralateral LMN
Check CN VII
Ipsilateral UMN
Brain Stem Subcor.cal
Bilateral
No Yes
Brown Sequard (Hemi-‐Cord) Syndrome

Case 3
• 45 year old Chinese lady • No significant PMH • 1 day history of sudden onset weakness, numbness and pain in both lower limbs

Sensory System • Brain à Further localize aner motor system • Cord à Idea of sensory level. Dissocia.on of modali.es
(DCML and ST)
• Peripheral Nervous System à Most common situa.on in med sch where sensory system examina.on is clinically high yield!!

Peripheral Nervous System
• Anterior Horn Cell • Radicle/Root • Plexus • Peripheral Nerve • Neuromuscular Junc.on • Muscle

Where is the thalamus?
Where do the two sensory pathways converge?

Back to Case 3
• Which subdivision of the PNS can we rule out? • What are we len with?

Motor Exam Power 3 on R side, 0 on L side for -‐ Ankle Plantar Flexion -‐ Toe Doriflexion -‐ Ankle Dorsiflexion -‐ Ankle Inversion -‐ Ankle Eversion What nerves supply these movements? What myotomes supply these movements?

Sensory Exam

Sensory Deficit
• Specific Nerve Distribu.on • Glove and Stocking • Patchy (Dermatomal) • Con.guous

Dis.nguishing Factors
• L4/5 vs. Common Peroneal Nerve • Scia.ca in Root Lesion

Some Common Logic
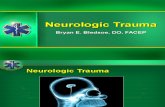
Nerves of Pelvic Viscera: Male
Anterior vagal trunk
Posterior vagal trunkandCeliac branch
lnferior phrenic arteries and
Left gastric artery and gastric
Celiac ganglia, plexus, and trunk
Left aort icorenal ganglion
Superior mesenteric ganglion
Superior mesenteric artery and
Intermesenteric (aortic) plexus
Inferior mesenteric ganglion,artery and plexus
Ureter and ureteric plexus
Superior hypogastric plexus
Superior rectal artery and plex
Hypogastr ic ner
Nerve from inferiorhypogastr ic plexusto sigmoid and descendingcolon (parasympathetic)
Sacral splanchnic nerves(sympathetic) 1_Inferior hypogastric(pelvic) plexus -
Obturator nerveand artery
Ductus deferensand plexus
Vesical plexus
Rectal plexus
Prostatic plexus
Cavernous nervesof penis
T10 spinal nerve (ventral ramus)
te and gray rami communicantes
Diaphragm
Left renal arteryand plexus
L1 spinal nerve(ventral ramus)
1st , 2nd, 3rd lumbar splanchnic nerves
Crav rami communicantes
Sympathetic trunk and ganglia
5th lumbar splanchnic nerve
L5 spinal nerve (ventral ramus)
Lumbosacral trunk
Cray rami communicantes
S1 sp ina l nerve(ventral ramus)
ic sp lanchnicnerves(parasympathetic)
al plexus
Piriformis muscle
Cluteus maximusmuscle and sacro-tuberous l igament
Coccygeus (ischiococcygeus)muscle and sacrospinousligament
Pudendal nerve
ator ani muscle
nferior anal (rectal) nerve
Perineal nerve
Dorsal nerve of penis
Plate 41O
Posterior scrotal nerves
Innervation

Now, how do I prepare and work out my own algorithms for Neurological
Cases?

What is an algorithm? • It should be a dichotomy (if not 3 to 4 branches at the MOST) • Comprehensive (At every branch-‐out, check back to see if you
have covered all aspects of the heading) • High Yield – Can be dichotomized based on a clinical tool,
minimal overlap of condi.ons between categories • Logical -‐ Should follow the sequence of your thought process/
physical examina.on • Portable – Simple, pocket sized, not too difficult to remember
at the bedside
• There are always caveats

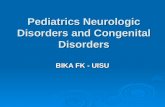
Approach to LMN Pabern of Weakness
Proximal
Sensory Loss?
Muscle (Myotonia)
Pure Motor Neuropathy
MND
Type of Sensory Loss
Distal
Sensory Loss? Yes
No
Glove & Stocking Patchy
PN (Polyneuropathy)
Myelopathy
(Lower dermatomes)
PN (Entrapment, MM)
Dermatomal (Root/Radicle)

Approach to LMN Pabern of Weakness
Proximal
Sensory Loss?
Muscle (Dystrophy, Myosi.s)
NMJ (Fa.guable, Ocular Signs)
Pure Motor Neuropathy
Peripheral Nerve (GBS – Ascending)
Plexus
Cord
Distal
Sensory Loss?
No Yes
Con.guous Patchy
Type of Sensory Deficit
Single Nerve
Dermatomal (Radicals)

Sepng out list of condi.ons
• Paeds • IM • GS • Ortho • Fam Med

Evalua.ng a pa.ent
• 4 Aspects: Medical, Func.onal, Social, Psychological
• Medical – 6 Cs • Func.onal – Body func.on, ac.vity, par.cipa.on
• Social – Pa.ent, Family, Community • Psychological

Approach to diagnosis in Neurology History, physical examina3on Obtain signs & symptoms
Syndromic diagnosis Movement (including coordina.on & fluidity) Soma.c senses (touch, temperature, propriocep.on, nocicep.on) Special senses (vision, hearing, balance, smell, taste) Consciousness (including epilepsy) Intellect (including behaviour, language) Mood (including autonomic, endocrine)
Anatomic diagnosis ‘Where’
Pyramidal System: Brain all the way to muscle Cerebellar system Extrapyramidal: Basal ganglia and others Limbic and hypothalamic Cerebral cortex Sensory system: Receptor all the way to thalamus and sensory cortex
Ae3ologic diagnosis ‘What’
VITAMIN CD
Func3onal diagnosis Disability, Ac.vity, Par.cipa.on

Case 2
Mr Ahmad 65/M/Malay Sudden onset weakness

Inspec.on
• A – Alert vs. Drowsy vs. Comatose (GCS), Toxic? • B – Breathing (Respi Distress/Laboured, Abdominal, Deep/Shallow, Kussmal, Cheyne Stokes)
• C – Colour (Pale, Cyano.c, Jaundiced, Plethoric) • D – Disability (Func.onal Aids) • E – Environment (Vitals, Suppor.ve, Related to system)

• If GCS suddenly became very poor, what would you be concerned about?
• What would you do?

Paberns of Disease in PE
• Raised ICP: Fundoscopy (Bilateral Papilloedema), False localizing 6th nerve palsy, Decreased Conscious Level (Re.cular Forma.on of the pons)
• Hernia.on: New Focal Signs, Cranial Nerve Reflexes (E.g. Fixed and Dilated Pupil)


Steps
• Tone • Reflexes • Power • Cerebellar Signs • Sensory Examina.on • Gait
Swap order for LMN pabern of weakness

Presenta.on (Finally)
• Medical

Func.onal
Hemiparesis Lost use of R hand & cannot walk steadily
Can no longer draw famous pain.ngs to earn
a living
House on 10th Floor House – Poor
occupa.onal safety No lin landing on every
floor
Male, 50 Divorced Lives alone

• Social – Family, Finances, Si.ng of care • Psychological – Depression in stroke


Some Caveats
• ALS -‐ Pseudobulbar Palsy (UMN) -‐ LMN in periphery

What are we len with?
• Cranial Nerves • Visual Fields

How about our cranial nerves?
• Motor Axis S.ll Applies! (E.g. of Ptosis) • Brain Stem • Course within the cranial cavity • Areas of convergence with other cranial nerves
• Course out of the cranial cavity

Loca3on Possible Ae3ologies
Other Cranial Nerves Involved
Other differen3a3ng
signs
Pons
CP Angle
IAM
Middle Ear
Stylomastoid Foramen
Paro.d Gland

Take Home Pointers
• Broad Categories • Distal to Proximal: Neuroaxis

Homework that will really help
• Condi.ons List across all pos.ngs • Comparison Table classified according to the Neuroaxis

Resources
• Kumar & Clarke 8th edi.on (1081 to 1089) • Black Book of Clinical Examina.on by Prof Erle Lim
• Talley O’ Connor • Blumenfield Neuroanatomy through Clinical Cases

Feedback
• hbp://goo.gl/XUJXke