Neurologic System - Nursing Ed · PDF fileReflex arc. a. A reflex arc is ... Pupillary...
36
Neurologic System 401 CHAPTER TWENTY PHYSIOLOGY OF THE NERVOUS SYSTEM A. Central nervous system (CNS) (Figure 20-1). B. Peripheral nervous system. 1. Twelve pairs of cranial nerves. 2. Thirty-one pairs of spinal nerves. 3. Autonomic nervous system (ANS). a. Sympathetic system: “fight or flight.” b. Parasympathetic system. Cells of the Nervous System A. Neuron: the functional cell of the nervous system. B. Function/classification. C. Supporting cells provide support, nourishment, and pro- tection to the neuron. D. Myelin sheath. 1. Dense membrane or insulator around the axon. 2. Facilitates function of the neuron. 3. Contributes to the blood-brain barrier to protect the CNS from harmful molecules. E. Nerve regeneration: entire neuron is unable to undergo complete regeneration. 1. Neuron regeneration in the CNS is very limited, pos- sibly because of the lack of neurilemma (membrane surrounding the neuron). 2. Scar tissue is a major deterrent to successful cellular regeneration. F. Impulse conduction. 1. Reflex arc. a. A reflex arc is the functional unit that provides pathways over which nerve impulses travel. b. The passage of impulses over a reflex arc is called a reflex act or a reflex and is an involuntary response to a stimulus. c. Reflex arc: the afferent neuron carries the stimulus to the spine, integrates it into and through the spine (CNS) to the efferent neuron, and crosses the synapse with the message from the CNS to the organ or muscle, which responds to the stimu- lus. This is the sequence of events evaluated when the deep tendon reflexes are tested. 2. Synaptic transmission. a. A chemical synapse maintains a one-way com- munication link between neurons. b. Chemical neurotransmitters (neuromediators) facilitate the transmission of an impulse across the synapse. (1) Acetylcholine. (2) Norepinephrine. (3) Dopamine. (4) Histamine. c. Impulses pass in only one direction. Central Nervous System The brain and the spinal cord within the vertebral column make up the CNS (see Figure 20-1). A. The brain and the spinal column are protected by the rigid bony structure of the skull and the vertebral column. B. Meninges: protective membranes that cover the brain and are continuous with those of the spinal cord. 1. Pia mater: a delicate vascular connective tissue layer that covers the surfaces of the brain and the spinal column; part of the blood-brain barrier. 2. Arachnoid: a delicate nonvascular, waterproof mem- brane that encases the entire CNS; the subarachnoid space contains the cerebrospinal fluid (CSF). 3. Dura mater: a tough white fibrous connective tissue, the outer layer of protection to the brain and spinal cord. C. Cerebrospinal fluid (CSF). 1. Serves to cushion and protect the brain and spinal cord; brain literally floats in CSF. 2. CSF is clear, colorless, watery fluid; approximately 100 to 200 mL in total volume, with a normal fluid pressure of 60 to 100 mm H 2 O. 3. Formation and circulation of CSF (Figure 20-2). a. Fluid is secreted by the choroid plexus located in the ventricles of the brain. b. CSF flows through the lateral ventricles into the third ventricle, then flows through the aqueduct of Sylvius into the fourth ventricle, where the central canal of the spinal column opens. c. From the fourth ventricle, CSF flows around the spinal cord and brain. d. Because CSF is formed continuously, it is reab- sorbed at a comparable rate by the arachnoid villi.
Transcript of Neurologic System - Nursing Ed · PDF fileReflex arc. a. A reflex arc is ... Pupillary...
L
Neurologic System
401
CHAPTER TWENTY
PHYSIOLOGY OF THE NERVOUS SYSTEM
A. Centralnervoussystem(CNS)(Figure20-1).B. Peripheralnervoussystem.
1. Twelvepairsofcranialnerves.2. Thirty-onepairsofspinalnerves.3. Autonomicnervoussystem(ANS).
a. Sympatheticsystem:“fightorflight.”b. Parasympatheticsystem.
Cells of the Nervous SystemA. Neuron:thefunctionalcellofthenervoussystem.B. Function/classification.C. Supportingcellsprovidesupport,nourishment,andpro-
tectiontotheneuron.D. Myelinsheath.
1. Densemembraneorinsulatoraroundtheaxon.2. Facilitatesfunctionoftheneuron.3. Contributestotheblood-brainbarriertoprotectthe
CNSfromharmfulmolecules.E. Nerveregeneration:entireneuronisunabletoundergo
completeregeneration.1. NeuronregenerationintheCNSisverylimited,pos-
siblybecauseof the lackofneurilemma(membranesurroundingtheneuron).
2. Scartissueisamajordeterrenttosuccessfulcellularregeneration.
F. Impulseconduction.1. Reflexarc.
a. A reflex arc is the functional unit that providespathwaysoverwhichnerveimpulsestravel.
b. Thepassageofimpulsesoverareflexarciscalledareflexactorareflexandisaninvoluntaryresponsetoastimulus.
c. Reflexarc:theafferentneuroncarriesthestimulusto the spine, integrates it into and through thespine (CNS) to the efferent neuron, and crossesthe synapse with the message from the CNS totheorganormuscle,whichrespondstothestimu-lus.Thisisthesequenceofeventsevaluatedwhenthedeeptendonreflexesaretested.
2. Synaptictransmission.a. A chemical synapse maintains a one-way com-
municationlinkbetweenneurons.
b. Chemical neurotransmitters (neuromediators)facilitatethetransmissionofanimpulseacrossthesynapse.(1) Acetylcholine.(2) Norepinephrine.(3) Dopamine.(4) Histamine.
c. Impulsespassinonlyonedirection.
Central Nervous SystemThebrainandthespinalcordwithinthevertebralcolumnmakeuptheCNS(seeFigure20-1).A. The brain and the spinal column are protected by
the rigid bony structure of the skull and the vertebralcolumn.
B. Meninges: protective membranes that cover the brainandarecontinuouswiththoseofthespinalcord.1. Piamater:adelicatevascularconnectivetissue layer
that covers the surfaces of the brain and the spinalcolumn;partoftheblood-brainbarrier.
2. Arachnoid:adelicatenonvascular,waterproofmem-branethatencasestheentireCNS;thesubarachnoidspacecontainsthecerebrospinalfluid(CSF).
3. Duramater:atoughwhitefibrousconnectivetissue,theouter layerofprotectiontothebrainandspinalcord.
C. Cerebrospinalfluid(CSF).1. Serves to cushion and protect the brain and spinal
cord;brainliterallyfloatsinCSF.2. CSF is clear, colorless, watery fluid; approximately
100to200mLintotalvolume,withanormalfluidpressureof60to100mmH2O.
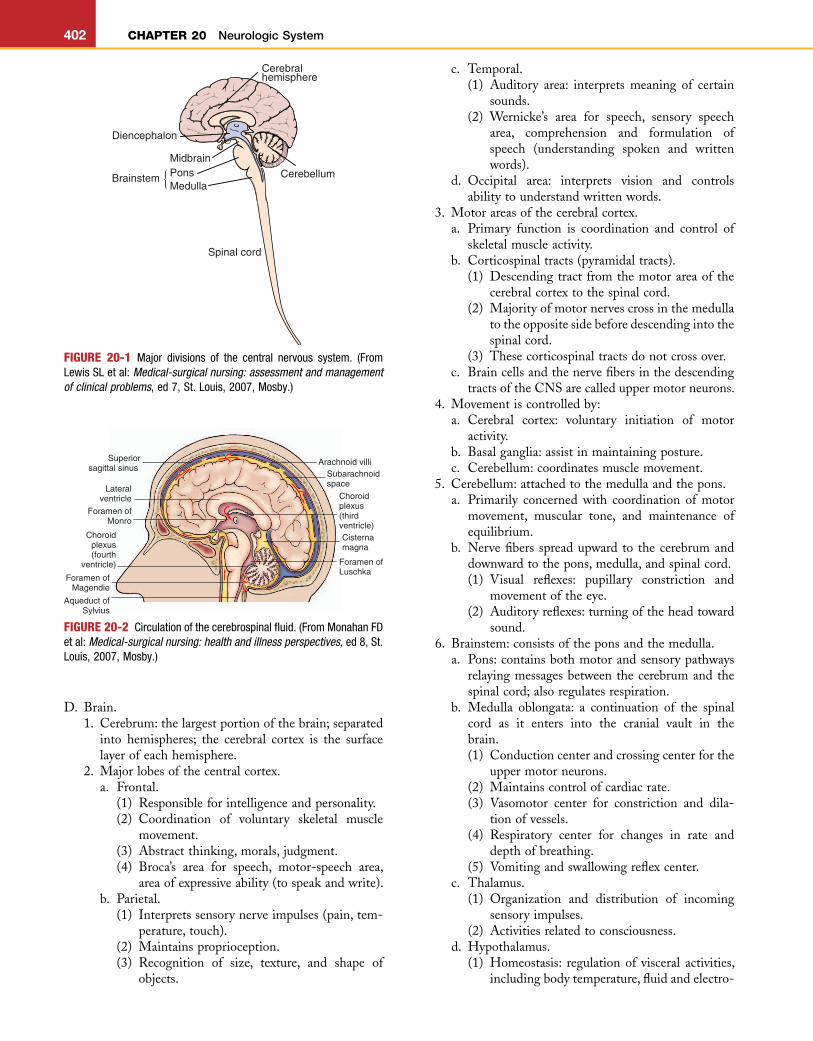
3. FormationandcirculationofCSF(Figure20-2).a. Fluidissecretedbythechoroidplexuslocatedin
theventriclesofthebrain.b. CSFflowsthroughthelateralventricles intothe
third ventricle, then flows through the aqueductof Sylvius into the fourth ventricle, where thecentralcanalofthespinalcolumnopens.
c. Fromthefourthventricle,CSFflowsaroundthespinalcordandbrain.
d. Because CSF is formed continuously, it is reab-sorbedatacomparableratebythearachnoidvilli.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
402 CHAPTER 20 Neurologic System
c. Temporal.(1) Auditory area: interprets meaning of certain
sounds.(2) Wernicke’s area for speech, sensory speech
area, comprehension and formulation ofspeech (understanding spoken and writtenwords).
d. Occipital area: interprets vision and controlsabilitytounderstandwrittenwords.
3. Motorareasofthecerebralcortex.a. Primary function is coordination and control of
skeletalmuscleactivity.b. Corticospinaltracts(pyramidaltracts).
(1) Descendingtractfromthemotorareaofthecerebralcortextothespinalcord.
(2) Majorityofmotornervescrossinthemedullatotheoppositesidebeforedescendingintothespinalcord.
(3) Thesecorticospinaltractsdonotcrossover.c. Braincellsandthenervefibersinthedescending
tractsoftheCNSarecalleduppermotorneurons.4. Movementiscontrolledby:
a. Cerebral cortex: voluntary initiation of motoractivity.
b. Basalganglia:assistinmaintainingposture.c. Cerebellum:coordinatesmusclemovement.
5. Cerebellum:attachedtothemedullaandthepons.a. Primarily concerned with coordination of motor
movement, muscular tone, and maintenance ofequilibrium.
b. Nervefibers spreadupward to thecerebrumanddownwardtothepons,medulla,andspinalcord.(1) Visual reflexes: pupillary constriction and
movementoftheeye.(2) Auditoryreflexes:turningoftheheadtoward
sound.6. Brainstem:consistsoftheponsandthemedulla.
a. Pons:containsbothmotorandsensorypathwaysrelayingmessagesbetweenthecerebrumandthespinalcord;alsoregulatesrespiration.
b. Medulla oblongata: a continuation of the spinalcord as it enters into the cranial vault in thebrain.(1) Conductioncenterandcrossingcenterforthe
uppermotorneurons.(2) Maintainscontrolofcardiacrate.(3) Vasomotor center for constriction and dila-
tionofvessels.(4) Respiratory center for changes in rate and
depthofbreathing.(5) Vomitingandswallowingreflexcenter.
c. Thalamus.(1) Organization and distribution of incoming
sensoryimpulses.(2) Activitiesrelatedtoconsciousness.
d. Hypothalamus.(1) Homeostasis: regulationof visceral activities,
includingbodytemperature,fluidandelectro-
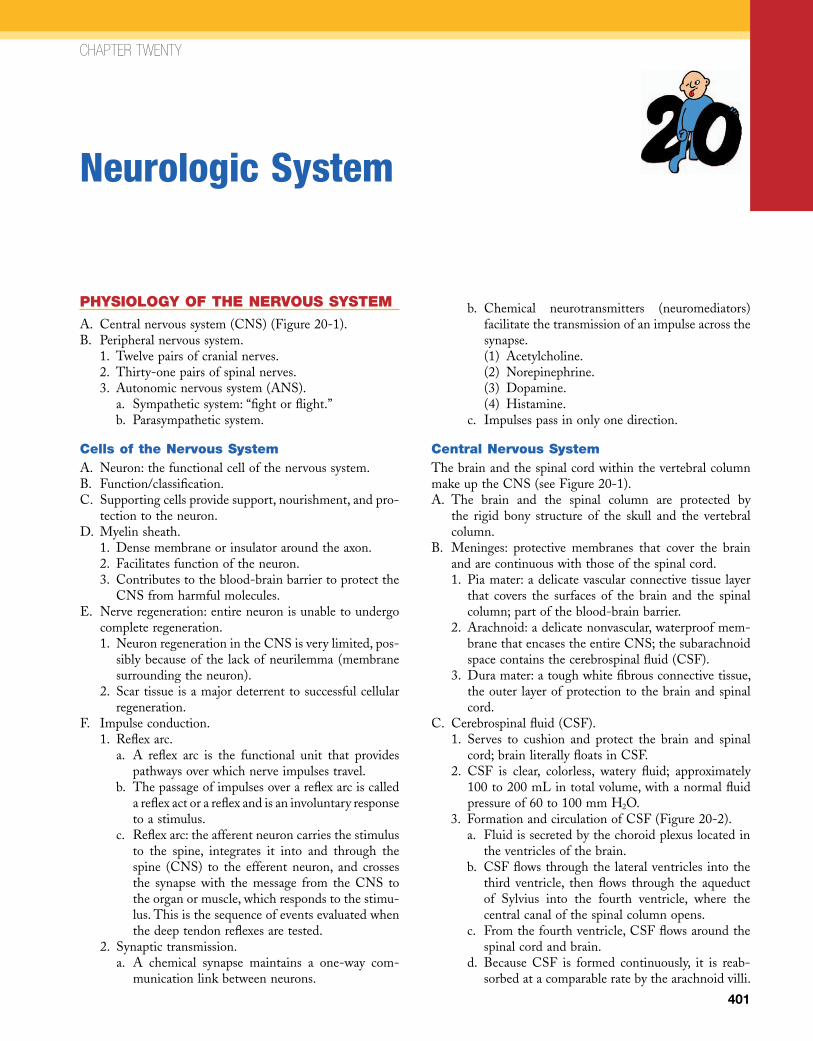
FIGURE 20-1 Major divisions of the central nervous system. (From Lewis SL et al: Medical-surgical nursing: assessment and management of clinical problems, ed 7, St. Louis, 2007, Mosby.)
Cerebralhemisphere
Diencephalon
MidbrainPonsMedulla
Brainstem Cerebellum
Spinal cord
{
FIGURE 20-2 Circulation of the cerebrospinal fluid. (From Monahan FD et al: Medical-surgical nursing: health and illness perspectives, ed 8, St. Louis, 2007, Mosby.)
Arachnoid villi
Choroidplexus(thirdventricle)
Choroidplexus(fourth
ventricle)
Foramen ofMagendie
Foramen ofLuschka
Aqueduct ofSylvius
Lateralventricle
Subarachnoidspace
Superiorsagittal sinus
Foramen ofMonro
Cisternamagna
D. Brain.1. Cerebrum:thelargestportionofthebrain;separated
into hemispheres; the cerebral cortex is the surfacelayerofeachhemisphere.
2. Majorlobesofthecentralcortex.a. Frontal.
(1) Responsibleforintelligenceandpersonality.(2) Coordination of voluntary skeletal muscle
movement.(3) Abstractthinking,morals,judgment.(4) Broca’s area for speech, motor-speech area,
areaofexpressiveability(tospeakandwrite).b. Parietal.
(1) Interpretssensorynerveimpulses(pain,tem-perature,touch).
(2) Maintainsproprioception.(3) Recognition of size, texture, and shape of
objects.
L
CHAPTER 20 Neurologic System 403
lyteregulation,motilityandsecretionsofthegastrointestinaltract,arterialbloodpressure.
(2) Nerveconnectionswiththethalamusandthecerebralcortexmakeitpossibleforemotionsto influence visceral activity (e.g., spasticcolon).
(3) Regulationof endocrineglandsvia influenceonthepituitarygland.
(4) Neurosecretion of antidiuretic hormone,whichisstoredinthepituitarygland.
7. Cerebralcirculation.a. Theinternalcarotidarteriesenterthecranialvault
atthetemporalarea.b. The circleofWillis is an arterial anastomosis at
thebaseofthebrain.Thecircleensurescontinuedcirculationifoneofthemainvesselsisdisrupted.
E. Spinalcord.1. Thespinalcordiscontinuouswiththemedullaand
extendsdownthevertebralcolumntothelevelofthefirstorsecondlumbarvertebrae.
2. Each column is divided into functional groups ofnervefibers.a. Ascending tracts: transmit impulses to the brain
(sensorypathway).b. Descending tracts: transmit impulses from the
braintothevariouslevelsofthespinalcord(motorpathways).
3. Structure.a. Intervertebral disks lie between the vertebrae to
provideflexibilitytothespinalcolumn.
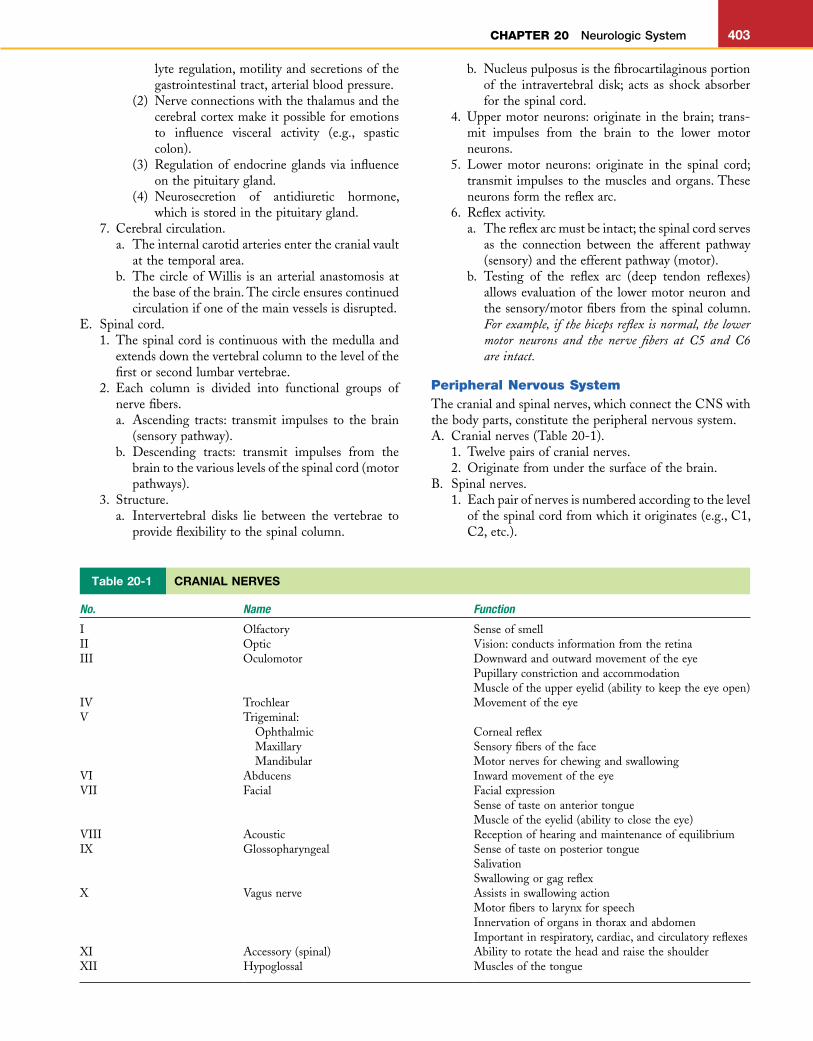
Table 20-1 CRANIAL NERVES
No. Name Function
I Olfactory SenseofsmellII Optic Vision:conductsinformationfromtheretinaIII Oculomotor Downwardandoutwardmovementoftheeye
PupillaryconstrictionandaccommodationMuscleoftheuppereyelid(abilitytokeeptheeyeopen)
IV Trochlear MovementoftheeyeV Trigeminal:
Ophthalmic Cornealreflex Maxillary Sensoryfibersoftheface Mandibular Motornervesforchewingandswallowing
VI Abducens InwardmovementoftheeyeVII Facial Facialexpression
SenseoftasteonanteriortongueMuscleoftheeyelid(abilitytoclosetheeye)
VIII Acoustic ReceptionofhearingandmaintenanceofequilibriumIX Glossopharyngeal Senseoftasteonposteriortongue
SalivationSwallowingorgagreflex
X Vagusnerve AssistsinswallowingactionMotorfiberstolarynxforspeechInnervationoforgansinthoraxandabdomenImportantinrespiratory,cardiac,andcirculatoryreflexes
XI Accessory(spinal) AbilitytorotatetheheadandraisetheshoulderXII Hypoglossal Musclesofthetongue
b. Nucleuspulposusisthefibrocartilaginousportionof the intravertebral disk; acts as shock absorberforthespinalcord.
4. Uppermotorneurons:originate in thebrain; trans-mit impulses from the brain to the lower motorneurons.
5. Lower motor neurons: originate in the spinal cord;transmit impulses to themusclesandorgans.Theseneuronsformthereflexarc.
6. Reflexactivity.a. Thereflexarcmustbeintact;thespinalcordserves
as the connection between the afferent pathway(sensory)andtheefferentpathway(motor).
b. Testing of the reflex arc (deep tendon reflexes)allowsevaluationofthe lowermotorneuronandthesensory/motorfibersfromthespinalcolumn.For example, if the biceps reflex is normal, the lower motor neurons and the nerve fibers at C5 and C6 are intact.
Peripheral Nervous SystemThecranialandspinalnerves,whichconnecttheCNSwiththebodyparts,constitutetheperipheralnervoussystem.A. Cranialnerves(Table20-1).
1. Twelvepairsofcranialnerves.2. Originatefromunderthesurfaceofthebrain.
B. Spinalnerves.1. Eachpairofnervesisnumberedaccordingtothelevel
ofthespinalcordfromwhichitoriginates(e.g.,C1,C2,etc.).
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
404 CHAPTER 20 Neurologic System
2. Each spinal nerve is connected to the cord by tworoots.a. Dorsal (posterior root): a sensory nerve carrying
messagestotheCNS.b. Ventral (anterior root): a motor nerve carrying
neuron messages to glands and the peripheralareas.
C. Somatic nervous system: consists of peripheral nervefiberssendingsensorystimulitoCNSandmotornervefibersthatstimulateskeletalmuscle.
D. Autonomicnervoussystem(ANS):regulatesinvoluntaryactivity (cardiovascular, respiratory, metabolic, bodytemperature,etc.).1. Consists of two divisions that have antagonistic
activity.2. Parasympathetic division: maintains normal body
functions.3. Sympathetic division: prepares the body to meet a
challengeoranemergency(preparationfor“fightorflight”)(Table20-2).
4. Mostof theorgansof thebody receive innervationfromboththeparasympatheticandthesympatheticdivisions. The divisions are usually antagonistic ineffectonindividualorgans:onestimulates;theotherrelaxes.
5. Chemical mediators: facilitate transmission ofimpulsesintheANS.a. Acetylcholineisreleasedbythefibersinbothdivi-
sionsoftheANS.b. Norepinephrineisreleasedprimarilybythesym-
patheticdivision.
c. Mentalstatusmustbeassessedbeforethehistorydatafromtheclientcanbeassumedtobeaccurate.
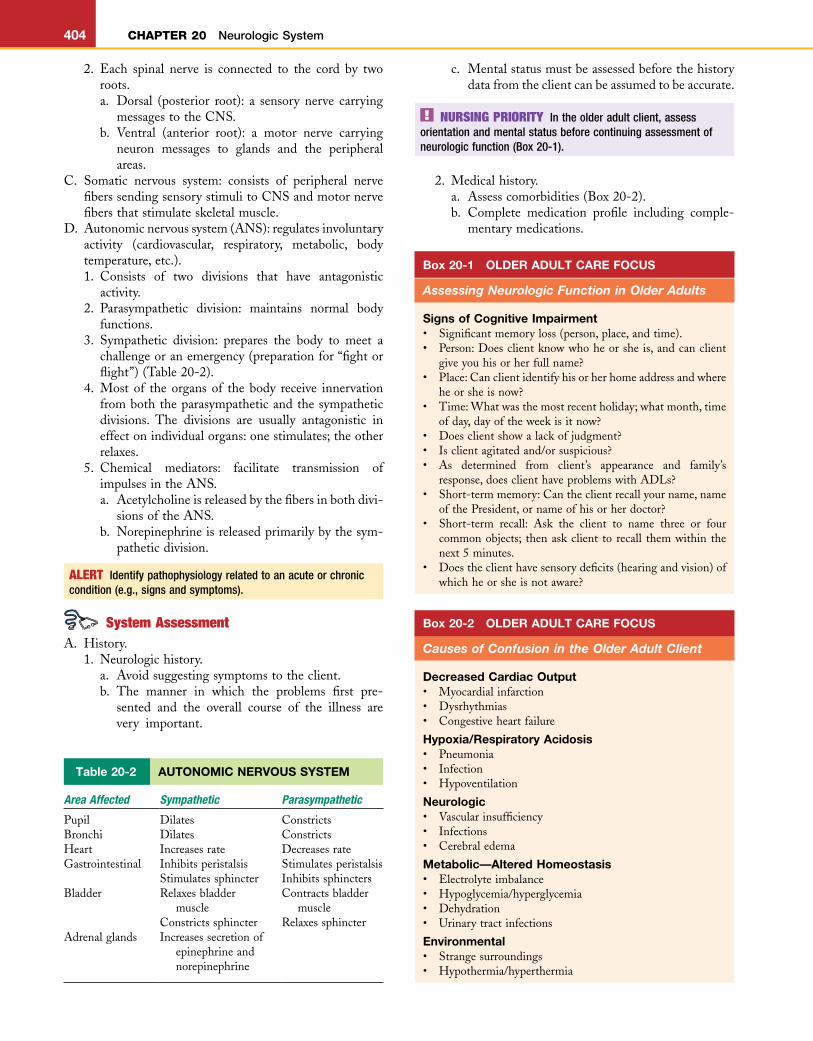
Table 20-2 AUTONOMIC NERVOUS SYSTEM
Area Affected Sympathetic Parasympathetic
Pupil Dilates ConstrictsBronchi Dilates ConstrictsHeart Increasesrate DecreasesrateGastrointestinal Inhibitsperistalsis Stimulatesperistalsis
Stimulatessphincter InhibitssphinctersBladder Relaxesbladder
muscleContractsbladder
muscleConstrictssphincter Relaxessphincter
Adrenalglands Increasessecretionofepinephrineandnorepinephrine
ALERT Identify pathophysiology related to an acute or chronic condition (e.g., signs and symptoms).
System AssessmentA. History.
1. Neurologichistory.a. Avoidsuggestingsymptomstotheclient.b. The manner in which the problems first pre-
sented and the overall course of the illness arevery important.
NURSING PRIORITY In the older adult client, assess orientation and mental status before continuing assessment of neurologic function (Box 20-1).
Box 20-1 OLDER ADULT CARE FOCUS
Assessing Neurologic Function in Older Adults
Signs of Cognitive Impairment• Significantmemoryloss(person,place,andtime).• Person:Doesclientknowwhoheorsheis,andcanclient
giveyouhisorherfullname?• Place:Canclientidentifyhisorherhomeaddressandwhere
heorsheisnow?• Time:Whatwasthemostrecentholiday;whatmonth,time
ofday,dayoftheweekisitnow?• Doesclientshowalackofjudgment?• Isclientagitatedand/orsuspicious?• As determined from client’s appearance and family’s
response,doesclienthaveproblemswithADLs?• Short-termmemory:Cantheclientrecallyourname,name
ofthePresident,ornameofhisorherdoctor?• Short-term recall: Ask the client to name three or four
commonobjects; thenaskclient to recall themwithin thenext5minutes.
• Doestheclienthavesensorydeficits(hearingandvision)ofwhichheorsheisnotaware?
2. Medicalhistory.a. Assesscomorbidities(Box20-2).b. Complete medication profile including comple-
mentarymedications.
Box 20-2 OLDER ADULT CARE FOCUS
Causes of Confusion in the Older Adult Client
Decreased Cardiac Output• Myocardialinfarction• Dysrhythmias• Congestiveheartfailure
Hypoxia/Respiratory Acidosis• Pneumonia• Infection• Hypoventilation
Neurologic• Vascularinsufficiency• Infections• Cerebraledema
Metabolic—Altered Homeostasis• Electrolyteimbalance• Hypoglycemia/hyperglycemia• Dehydration• Urinarytractinfections
Environmental• Strangesurroundings• Hypothermia/hyperthermia
L
CHAPTER 20 Neurologic System 405
c. Birth (or delivery) history. Was client a difficultdelivery?
d. Sequenceofgrowthanddevelopment.3. Familyhistory:presenceofhereditaryor congenital
problems.4. Personalhistory:activitiesofdailyliving(ADLs),any
changeinroutine.5. Historyandsymptomsofcurrentproblem.
a. Paralysisorparesthesia,syncope.b. Headache,dizziness,speechproblems.c. Visualproblems,changesinpersonality.d. Memoryloss,nausea,vomiting.
B. Physicalassessment.1. Generalobservationofclient.
a. Posture,gait,coordination;performRombergtest.b. Positionofrestfortheinfantoryoungchild.c. Personalhygiene,grooming.d. Evaluatespeechandabilitytocommunicate.
(1) Paceofspeech:rapid,slow,halting.(2) Clarity:slurredordistinct.(3) Tone:high-pitched,rough.(4) Vocabulary:appropriatechoiceofwords.
e. Facialfeaturesmaysuggestspecificsyndromesinchildren.
2. Mentalstatus(musttake intoconsiderationthecli-ent’scultureandeducationalbackground).
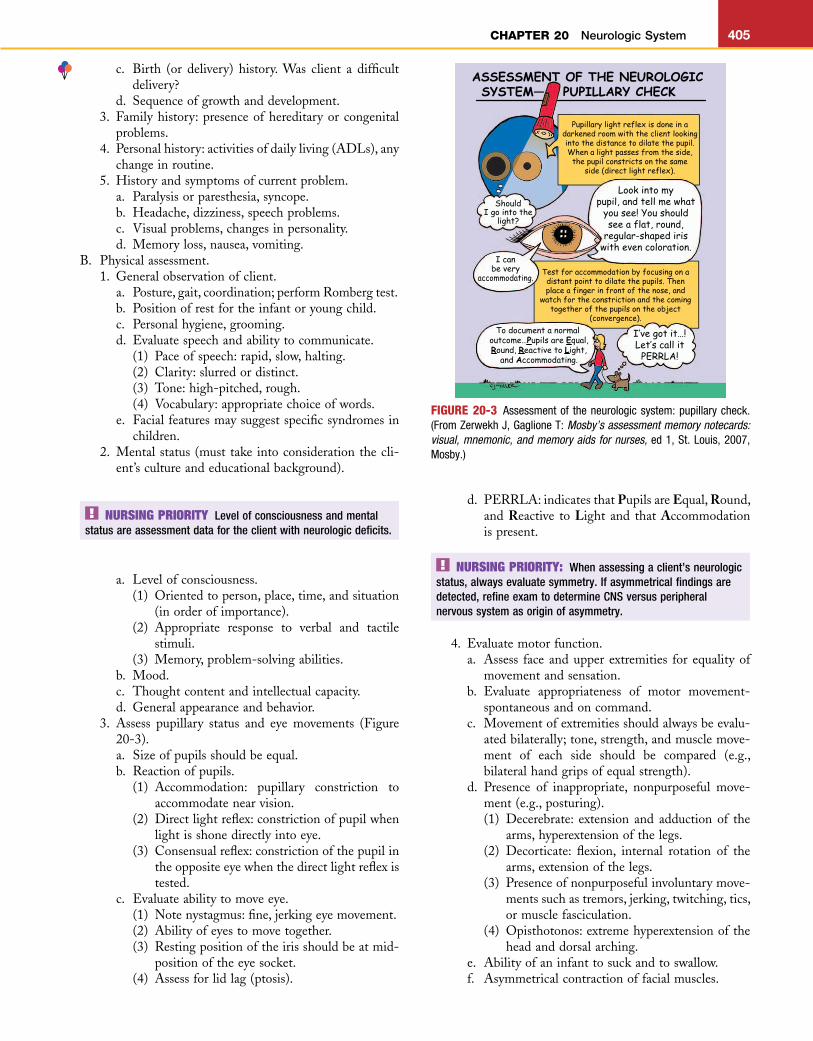
d. PERRLA:indicatesthatPupilsareEqual,Round,and Reactive to Light and that Accommodationispresent.
NURSING PRIORITY Level of consciousness and mental status are assessment data for the client with neurologic deficits.
a. Levelofconsciousness.(1) Orientedtoperson,place,time,andsituation
(inorderofimportance).(2) Appropriate response to verbal and tactile
stimuli.(3) Memory,problem-solvingabilities.
b. Mood.c. Thoughtcontentandintellectualcapacity.d. Generalappearanceandbehavior.
3. Assess pupillary status and eye movements (Figure20-3).a. Sizeofpupilsshouldbeequal.b. Reactionofpupils.
(1) Accommodation: pupillary constriction toaccommodatenearvision.
(2) Directlightreflex:constrictionofpupilwhenlightisshonedirectlyintoeye.
(3) Consensualreflex:constrictionofthepupilintheoppositeeyewhenthedirectlightreflexistested.
c. Evaluateabilitytomoveeye.(1) Notenystagmus:fine,jerkingeyemovement.(2) Abilityofeyestomovetogether.(3) Restingpositionoftheirisshouldbeatmid-
positionoftheeyesocket.(4) Assessforlidlag(ptosis).
NURSING PRIORITY: When assessing a client’s neurologic status, always evaluate symmetry. If asymmetrical findings are detected, refine exam to determine CNS versus peripheral nervous system as origin of asymmetry.
4. Evaluatemotorfunction.a. Assess face andupper extremities for equalityof
movementandsensation.b. Evaluate appropriateness of motor movement-
spontaneousandoncommand.c. Movementofextremitiesshouldalwaysbeevalu-
atedbilaterally;tone,strength,andmusclemove-ment of each side should be compared (e.g.,bilateralhandgripsofequalstrength).
d. Presence of inappropriate, nonpurposeful move-ment(e.g.,posturing).(1) Decerebrate: extension and adduction of the
arms,hyperextensionofthelegs.(2) Decorticate: flexion, internal rotation of the
arms,extensionofthelegs.(3) Presenceofnonpurposefulinvoluntarymove-
mentssuchastremors,jerking,twitching,tics,ormusclefasciculation.
(4) Opisthotonos:extremehyperextensionoftheheadanddorsalarching.
e. Abilityofaninfanttosuckandtoswallow.f. Asymmetricalcontractionoffacialmuscles.
FIGURE 20-3 Assessment of the neurologic system: pupillary check. (From Zerwekh J, Gaglione T: Mosby’s assessment memory notecards: visual, mnemonic, and memory aids for nurses, ed 1, St. Louis, 2007, Mosby.)
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
406 CHAPTER 20 Neurologic System
5. Evaluatereflexes.a. Gagorcoughreflex.b. Swallowreflex.c. Cornealreflex.d. Babinski reflex: normal is negative in adults and
childrenolderthan1year;positivesignisdorsalflexionof the footand large toewith fanningoftheothertoes.
e. Deeptendonreflexes(simplestretchreflex).6. Assess vital signs and correlate with other data;
changes often occur slowly, and the overall trendneedstobeevaluated.a. Blood pressure and pulse: intracranial problems
precipitate changes; systolic blood pressure mayincrease,andpulseratemaydecrease.
b. Respirations:rate,depth,andrhythmaresensitiveindicatorsofintracranialproblems.(1) Cheyne-Stokes respiration: periodic breath-
inginwhichhyperpneaalternateswithapnea.(2) Neurogenic hyperventilation: regular, rapid,
deephyperpnea.(3) Ataxic: completely irregular pattern with
randomdeepandshallowrespirations.c. Temperature: evaluate changes in temperatureas
relatedtoneurologiccontrolversusinfection.
DISORDERS OF THE NEUROLOGIC SYSTEM
Increased Intracranial PressureAn increase in intracranial pressure (ICP) occurs any time there is an increase in the size or amount of intracranial contents.A. Thecranialvaultisrigid,andthereisminimalroomfor
expansionoftheintracranialcomponents.B. Anincrease inanyoneof thecomponentsnecessitates
a reciprocal change in other cranial contents; this fre-quently results in ischemiaofbrain tissue.An increaseinICPresultsfromoneofthefollowing:1. Increasedintracranialbloodvolume(vasodilation).2. IncreasedCSF.3. Increaseinthebulkofthebraintissue(edema).
C. Cerebraledema.1. Edemaoccurswhenthereisanincreaseinthevolume
ofbraintissuecausedbyanincreaseinthepermeabil-ity of the walls of the cerebral vessels. Protein-richfluidleaksintotheextracellularspace.Edemaismostoften the cause of increased ICP in adults, whichreachesmaximumpressurein48to72hours.
2. Cytotoxic (cellular) edema occurs as a result ofhypoxia. This results in abnormal accumulation offluidwithinthecells(intracellular)andadecreaseinextracellularfluid.
D. Poorventilationwillprecipitate respiratoryacidosis,oranincreaseinthePaco2.1. Carbondioxidehasavasodilatingeffectonthecere-
bral arteries, which increases cerebrovascular bloodflowandincreasesICP.
2. Clients shouldbeventilated toanormocapnic statetopreventcyclicvasodilation,whichincreasesintra-cranialpressure.
E. Regardless of the cause, increased ICP will result inprogressive neurologic deterioration; the specific defi-ciencies seenaredeterminedby theareaandextentofcompressionofbraintissue.
F. If the infant’s cranial suture lines are open, increasedICP will cause separation of the suture lines and anincreaseinthecircumferenceofthehead.
NURSING PRIORITY There is no single set of symptoms for all clients with increased ICP; symptoms depend on the cause and on how rapidly increased ICP develops.
AssessmentA. Riskfactors/etiology.
1. Cerebral edema caused by some untoward event ortrauma,includingtoxicexposure,blunttrauma,fluidandelectrolyteimbalance.
2. Braintumors.3. Intracranialhemorrhagecausedbyepiduralorsubdu-
ralbleeding (closedhead injuriesor rupturedbloodvessels).
4. Subarachnoidhemorrhage,hydrocephalus.5. Cerebralembolism, resulting innecrosisandedema
ofareassuppliedbytheinvolvedvessel.6. Cerebralthrombosis,resultinginischemiaofthearea
andleadingtoedemaandcongestionofaffectedarea.7. Encephalitis/meningitis.
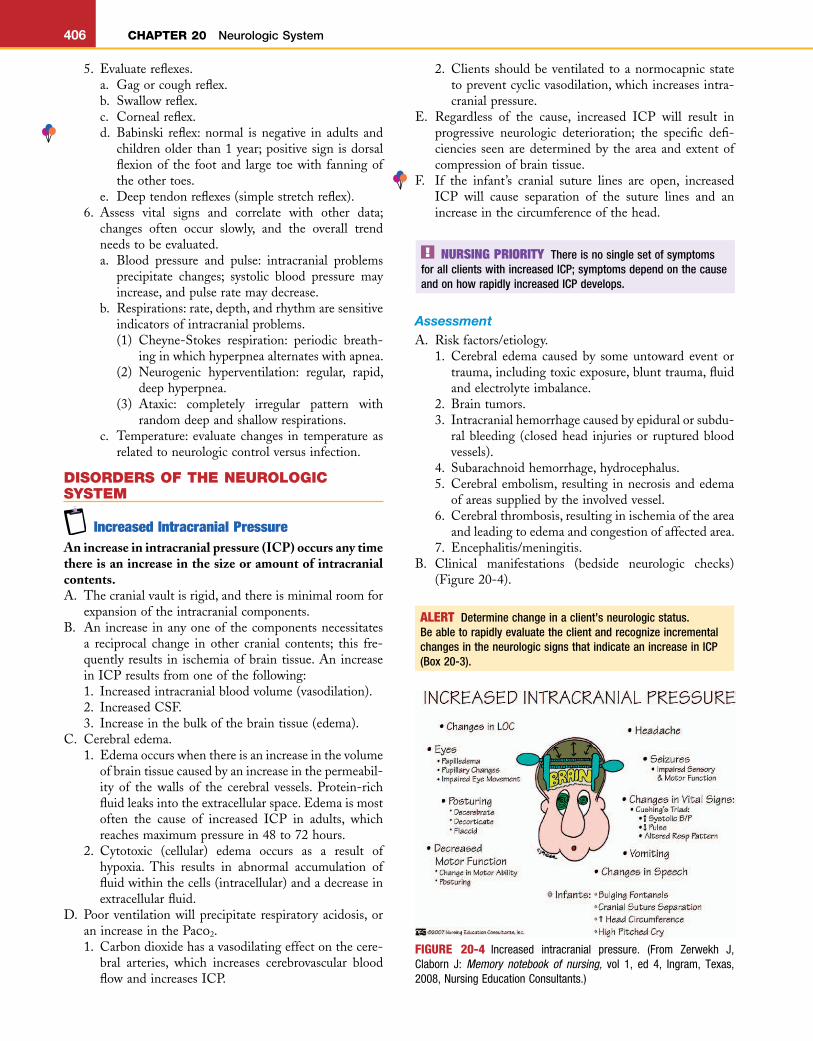
B. Clinical manifestations (bedside neurologic checks)(Figure20-4).
ALERT Determine change in a client’s neurologic status. Be able to rapidly evaluate the client and recognize incremental changes in the neurologic signs that indicate an increase in ICP (Box 20-3).
FIGURE 20-4 Increased intracranial pressure. (From Zerwekh J, Claborn J: Memory notebook of nursing, vol 1, ed 4, Ingram, Texas, 2008, Nursing Education Consultants.)
L
CHAPTER 20 Neurologic System 407
c. Unilateraldilationofpupils.d. Sluggishornopupillaryresponsetolightandpoor
orabsentaccommodation.4. Motorandsensory function:normal is indicatedby
theabilitytomoveallextremitieswithequalstrength.Abnormalfindingsinclude:a. Unilateralorbilateralweaknessorparalysis.b. Failuretowithdrawfrompainfulstimuli.c. Posturing: decerebrate, decorticate, flaccid, or
opisthotonos.d. Seizureactivity,ataxia.
5. Headache.a. Constantwithincreasingintensity.b. Exacerbatedbymovement.c. Photophobia.
6. Vomiting:projectilevomitingwithoutpriornausea.7. Infants.
a. Tense,bulgingfontanel(s).b. Separatedcranialsutures.c. Increasingfrontal-occipitalcircumference.d. High-pitchedcry.
C. Diagnostics(seeAppendix20-1).1. DirectICPmonitoring.2. Romberg test:measuresbalance.Client standswith
feet together andarmsat side,firstwitheyesopen,thenwitheyesclosedfor20to30seconds.
3. Calorictesting:testisperformedatbedsidebyintro-ducingcoldwaterintotheexternalauditorycanal.Ifthe eighth cranial nerve is stimulated, nystagmusrotates toward the irrigated ear. If no nystagmusoccurs,apathologicconditionispresent.
4. Doll’seyereflex(oculocephalicreflex).a. Doll’s eye reflex is normal when the client’s
head is moved from side to side and the eyesmove in the direction opposite that of theturning.
b. Doll’s eye reflex is abnormal when the client’seyes remain in a fixed, midline position whenthe head is turned from side to side (possiblebrainsteminvolvement).
c. Contraindicateduntilriskforspinalcordinjuryisruledout.
5. Papilledema: edema of the optic nerve; observedbyexaminingretinaareawithanophthalmoscope.
6. Nuchal rigidity:herniationofbrainstemmayoccur;anemergentcrisis.
7. Lumbarpunctureisgenerallynotperformed;decreasein CSF pressure could precipitate herniation of thebrainstem.
TreatmentA. Treatment of the underlying cause of increasing
pressure.B. Neurologiccheckseveryhourorasordered.
1. Mayinvolvecorrelationofseveralvariablesincludinglevel of consciousness, vital signs, speech, facialsymmetry, grasp strength, leg strength, and pupilresponses.
1. Assessforchanges inlevelofconsciousness,becausechangeisthecardinalindicatorofincreasedintracra-nialpressure.a. Anyalterationinlevelofconsciousness(earlysign
for both adults and children)— irritability, rest-lessness, confusion, lethargy, and difficulty inarousing—maybesignificant.
NURSING PRIORITY The first sign of a change in the level of ICP is a change in level of consciousness; this may progress to a decrease in level of consciousness.
Box 20-3 INCREASING INTRACRANIAL PRESSURE
AdultEarly:Restless,irritable,lethargicIntermediate:Unequalpupilresponse,projectilevomiting,vital
signschangesLate: Decreased level of consciousness, decreased reflexes,
hypoventilation,dilatedpupils,posturing
Infant/ChildEarly:Poorfeeding,tensefontanel,headache,nauseaandvom-
iting,increasedpitchofcry,unsteadygaitIntermediate (younger than 18 months): Increased head cir-
cumference, altered consciousness, bulging fontanel; shrillcry,severeheadache,blurredvision,stiffneck
Late:Sameasadult
b. Inappropriateverbalandmotorresponse;delayedorsluggishresponses.
c. As the client loses consciousness, hearing is thelastsensetobelost.
2. Changesinvitalsigns.a. Increaseinsystolicbloodpressurewithincreasein
pulsepressure.b. Decreaseinpulserate.c. Alteration inrespiratorypattern(Cheyne-Stokes
respiration,hyperventilation).d. Assess temperature with regard to overall prob-
lems;temperatureusuallyincreases.
NURSING PRIORITY Cushing’s triad: increasing systolic pressure, with increased pulse pressure, decreased pulse rate, and Cheyne-Stokes respirations. Increased ICP is well established when this occurs.
3. Pupillary response: normal pupils should be round,midline,equalinsize,andequallybrisklyreactivetolightandshouldaccommodatetodistance.Abnormalfindingsinclude:a. Ipsilateral: pupillary changes occurring on the
samesideasacerebrallesion.b. Contralateral:pupillarychangesoccurringonthe
sideoppositeacerebrallesion.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
408 CHAPTER 20 Neurologic System
2. Carefulcomparisontopreviousassessmentiscriticaltodetectincrementalchanges.
C. Intravenous(IV)andoralfluidstomaintainnormalfluidvolumestatusifmeanarterialpressure(MAP)islowtonormal.Often,normalsalinesolutionisfluidofchoice;5%dextroseinwaterpotentiatescerebraledema.
D. Medications.1. Osmoticdiureticcorticosteroids.2. Anticonvulsants,antihypertensives.
E. MaintainadequateventilationbymeansofmechanicalventilationtolowerPaco2(25to35mmHg)topreventvasodilationofcerebralvessels.
F. Placementofventriculoperitonealshuntduringdecom-pressionsurgery.
ComplicationsA. CSFleaks,especiallyinclientwithbasilarskullfracture,
maycausemeningitis.B. Herniation: shifting of the intracranial contents from
one compartment to another; involves herniationthroughthetentoriumcerebelli;affectsareaforcontrolofvitalfunctions.
C. Permanentbraindamage.
Nursing InterventionsGoal: ToidentifyanddecreaseproblemofincreasedICP.A. Neurologicchecks,asindicatedbyclient’sstatus(Tables
20-3and20-4).B. Maintainheadofbedinsemi-Fowler’sposition(15-30
degrees) to promote venous drainage and respiratoryfunction.
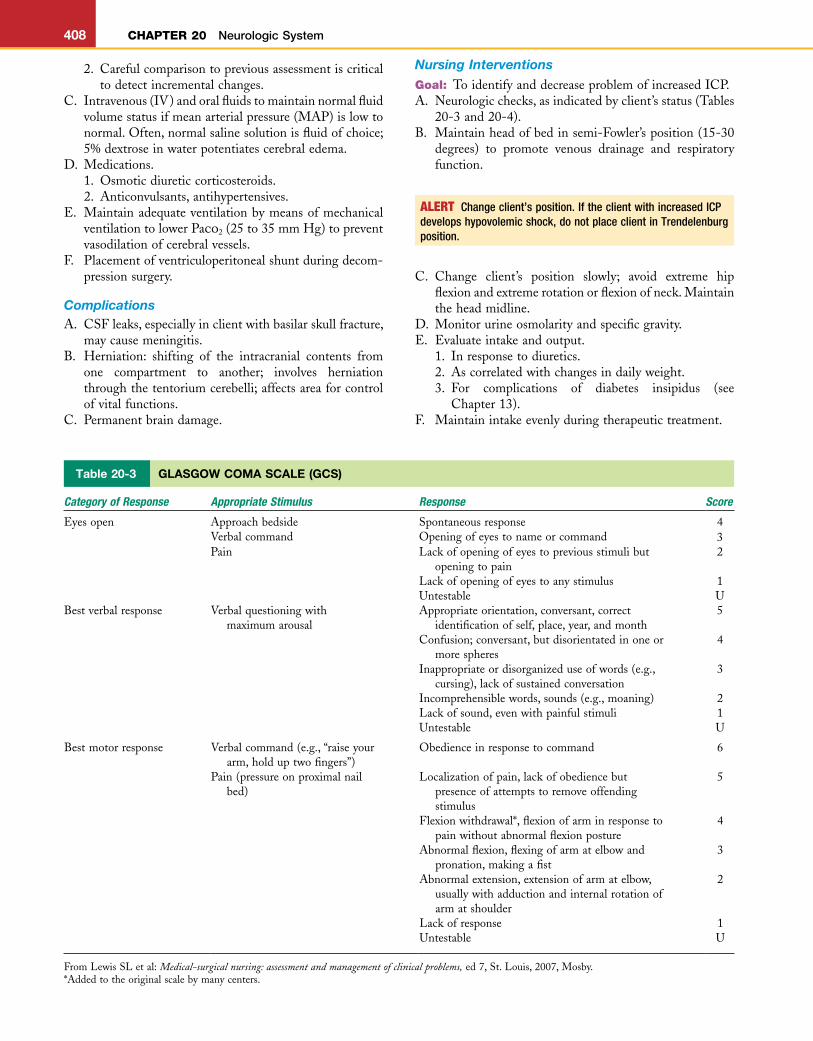
Table 20-3 GLASGOW COMA SCALE (GCS)
Category of Response Appropriate Stimulus Response Score
Eyesopen Approachbedside Spontaneousresponse 4Verbalcommand Openingofeyestonameorcommand 3Pain Lackofopeningofeyestopreviousstimulibut
openingtopain2
Lackofopeningofeyestoanystimulus 1Untestable U
Bestverbalresponse Verbalquestioningwithmaximumarousal
Appropriateorientation,conversant,correctidentificationofself,place,year,andmonth
5
Confusion;conversant,butdisorientatedinoneormorespheres
4
Inappropriateordisorganizeduseofwords(e.g.,cursing),lackofsustainedconversation
3
Incomprehensiblewords,sounds(e.g.,moaning) 2Lackofsound,evenwithpainfulstimuli 1Untestable U
Bestmotorresponse Verbalcommand(e.g.,“raiseyourarm,holduptwofingers”)
Obedienceinresponsetocommand 6
Pain(pressureonproximalnailbed)
Localizationofpain,lackofobediencebutpresenceofattemptstoremoveoffendingstimulus
5
Flexionwithdrawal*,flexionofarminresponsetopainwithoutabnormalflexionposture
4
Abnormalflexion,flexingofarmatelbowandpronation,makingafist
3
Abnormalextension,extensionofarmatelbow,usuallywithadductionandinternalrotationofarmatshoulder
2
Lackofresponse 1Untestable U
FromLewisSLetal:Medical-surgical nursing: assessment and management of clinical problems,ed7,St.Louis,2007,Mosby.*Addedtotheoriginalscalebymanycenters.
ALERT Change client’s position. If the client with increased ICP develops hypovolemic shock, do not place client in Trendelenburg position.
C. Change client’s position slowly; avoid extreme hipflexionandextremerotationorflexionofneck.Maintaintheheadmidline.
D. Monitorurineosmolarityandspecificgravity.E. Evaluateintakeandoutput.
1. Inresponsetodiuretics.2. Ascorrelatedwithchangesindailyweight.3. For complications of diabetes insipidus (see
Chapter13).F. Maintainintakeevenlyduringtherapeutictreatment.
L
CHAPTER 20 Neurologic System 409
G. Minimizerespiratorysuctioningandensurehyperoxy-genationbeforesuctioning.
H. Sedativesandnarcoticscandepressrespiration;usewithcautionbecausetheymasksymptomsofincreasingICP.
I. Client should avoid strenuous coughing, Valsalvamaneuver,andisometricmuscleexercises.
J. Avoid straining with stools (increases intrathoracicpressuresporadically).
K. In infants, measure frontal-occipital circumference toevaluateincreaseinsizeofthehead.
L. Controlhyperthermia.M. Maintainheadandspinalcolumninmidlineposition.Goal: Tomaintainrespiratoryfunction.
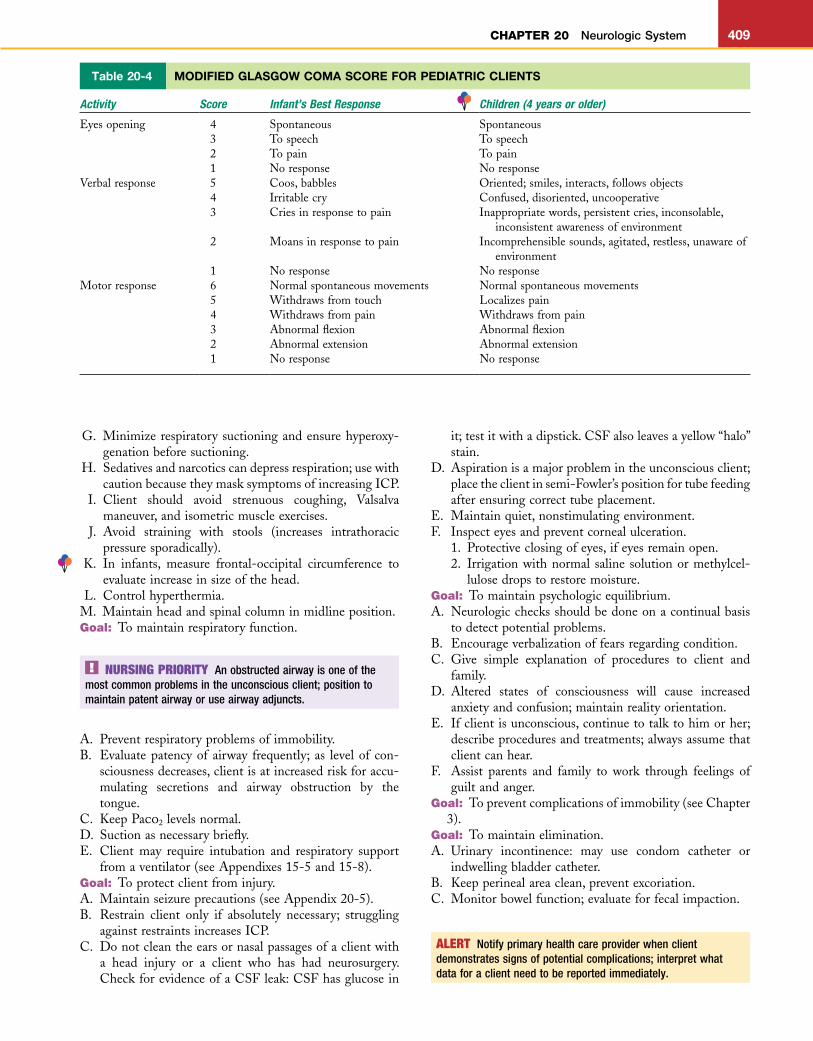
Table 20-4 MODIFIED GLASGOW COMA SCORE FOR PEDIATRIC CLIENTS
Activity Score Infant’s Best Response Children (4 years or older)
Eyesopening 4 Spontaneous Spontaneous3 Tospeech Tospeech2 Topain Topain1 Noresponse Noresponse
Verbalresponse 5 Coos,babbles Oriented;smiles,interacts,followsobjects4 Irritablecry Confused,disoriented,uncooperative3 Criesinresponsetopain Inappropriatewords,persistentcries,inconsolable,
inconsistentawarenessofenvironment2 Moansinresponsetopain Incomprehensiblesounds,agitated,restless,unawareof
environment1 Noresponse Noresponse
Motorresponse 6 Normalspontaneousmovements Normalspontaneousmovements5 Withdrawsfromtouch Localizespain4 Withdrawsfrompain Withdrawsfrompain3 Abnormalflexion Abnormalflexion2 Abnormalextension Abnormalextension1 Noresponse Noresponse
NURSING PRIORITY An obstructed airway is one of the most common problems in the unconscious client; position to maintain patent airway or use airway adjuncts.
A. Preventrespiratoryproblemsofimmobility.B. Evaluatepatencyof airway frequently; as levelof con-
sciousnessdecreases,clientisatincreasedriskforaccu-mulating secretions and airway obstruction by thetongue.
C. KeepPaco2levelsnormal.D. Suctionasnecessarybriefly.E. Client may require intubation and respiratory support
fromaventilator(seeAppendixes15-5and15-8).Goal: Toprotectclientfrominjury.A. Maintainseizureprecautions(seeAppendix20-5).B. Restrain client only if absolutely necessary; struggling
againstrestraintsincreasesICP.C. Donotcleantheearsornasalpassagesofaclientwith
a head injury or a client who has had neurosurgery.CheckforevidenceofaCSFleak:CSFhasglucosein
it;testitwithadipstick.CSFalsoleavesayellow“halo”stain.
D. Aspirationisamajorproblemintheunconsciousclient;placetheclientinsemi-Fowler’spositionfortubefeedingafterensuringcorrecttubeplacement.
E. Maintainquiet,nonstimulatingenvironment.F. Inspecteyesandpreventcornealulceration.
1. Protectiveclosingofeyes,ifeyesremainopen.2. Irrigationwithnormal saline solutionormethylcel-
lulosedropstorestoremoisture.Goal: Tomaintainpsychologicequilibrium.A. Neurologicchecksshouldbedoneonacontinualbasis
todetectpotentialproblems.B. Encourageverbalizationoffearsregardingcondition.C. Give simple explanation of procedures to client and
family.D. Altered states of consciousness will cause increased
anxietyandconfusion;maintainrealityorientation.E. Ifclientisunconscious,continuetotalktohimorher;
describeproceduresandtreatments;alwaysassumethatclientcanhear.
F. Assist parents and family to work through feelings ofguiltandanger.
Goal: Topreventcomplicationsofimmobility(seeChapter3).
Goal: Tomaintainelimination.A. Urinary incontinence: may use condom catheter or
indwellingbladdercatheter.B. Keepperinealareaclean,preventexcoriation.C. Monitorbowelfunction;evaluateforfecalimpaction.
ALERT Notify primary health care provider when client demonstrates signs of potential complications; interpret what data for a client need to be reported immediately.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
410 CHAPTER 20 Neurologic System
Home CareA. TeachclientandfamilysignsofincreasedICP.B. Callthedoctorifanyofthefollowingareobserved:
1. Changesinvision.2. Increaseddrainagefromincisionareaorcleardrain-
ageintheears.3. Abruptchangesinsleepingpatternsorirritability.4. Headachethatdoesnotrespondtomedication.5. Changesincoordination,disorientation.6. Slurredspeech,unusualbehavior.7. Seizureactivity,vomiting.
C. Reviewcareofsurgicalincision,wounds,ordrains.
Brain TumorsA. Brain tumorsmaybebenign,malignant,ormetastatic;
malignant brain tumors rarely metastasize outside theCNS.
B. Supratentorial: tumors occurring within the anteriortwo-thirdsofthebrain,primarilythecerebrum.
C. Infratentorial:tumorsoccurringintheposteriorthirdofthe brain (or below the tentorium), primarily in thecerebellumorthebrainstem.
D. Regardlessoftheorigin,site,orpresenceofmalignancy,problemsofincreasedICPoccurbecauseofthelimitedarea in the brain to accommodate an increase in theintracranialcontents.
AssessmentA. Riskfactors/etiology.
1. Age:highestincidenceinpeopleolderthan70years;commoninchildrenyoungerthan8years.
2. Presenceofmetastaticcancerofthelungorbreast.3. Familyhistory:gliomastendtooccurinotherfamily
members.4. Occupation: people who work with high levels of
radiation,formaldehyde(pathologists),vinylchloride(plastics manufacturers), and other chemicals are atincreasedriskforbraintumors.
B. Clinical manifestations: symptoms correlate with theareaofthebraininitiallyinvolved.1. Headache.
a. Recurrent. May vomit on arising and then feelbetter.
b. Moresevereinthemorning.c. Affectedbyposition.d. Headacheininfantmaybeidentifiedbypersis-
tent,irritatedcryingandheadrolling.2. Vomiting:initiallywithorwithoutnausea;progres-
sivelybecomesprojectile.3. Papilledema(edemaoftheopticdisc).4. Seizures(focalorgeneralized).5. Dizzinessandvertigo.6. Mental status changes: lethargy and drowsiness,
confusion,disorientation,andpersonalitychanges.7. Localizedmanifestations:
a. Focalweakness:hemiparesis.
8. Sensorydisturbances.a. Languagedisturbances.b. Coordinationdisturbances.c. Visualdisturbances.
9. Headtilt:childmaytilttheheadbecauseofdamagetoextraocularmuscles;maybefirst indicationofadecreaseinvisualacuity.
10. ChangesinvitalsignsindicativeofincreasingICP(Cushing’striad).
11. Cranialenlargementintheinfantyoungerthan18months.
C. Diagnostics(seeAppendix20-1).
TreatmentA. Medical.
1. Dexamethasone(seeAppendix6-7).2. Chemotherapy.3. Anticonvulsants(seeAppendix20-2).4. Complementaryandalternativemedicine.
B. Radiation: x-rays, gamma knife, stereotactic radiosur-gery.
C. Surgical intervention: craniotomy/craniectomy, biopsy,shuntplacement,reservoirplacement,laserremoval.
ComplicationsComplications include meningitis, brainstem herniation,diabetes insipidus, and syndrome of inappropriate antidi-uretichormonesecretion(seeChapter13).Residualeffectsincludeawidearrayofcomplicationssuchasseizures,dys-arthria, dysphasia, disequilibrium, and permanent braindamage.
Nursing InterventionsGoal: To provide appropriate preoperative nursing
interventions.A. Generalpreoperativecarewithexceptions,asnoted(see
Chapter3).B. Carefullyassessanddiscusswithsurgeontheappropri-
atenessofapreoperativeenema.C. Prepare client and family for appearance of the client
aftersurgery,includingpartialorcompletehairloss.D. Encourage verbalization regarding concerns about
surgery.E. Skinpreparationisusuallydoneintheoperatingroom.Goal: To monitor changes in ICP after craniotomy (see
Box20-3).A. Obtain vital signs and perform neurologic checks and
cranialnerveassessmentsasnecessary.B. Maintainpulmonaryfunctionandhygiene.C. Anticipateuseofanticonvulsantsandantiemetics.D. Discouragecoughing.E. Carefullyevaluatelevelofconsciousness;increasingleth-
argyorirritabilitymaybeindicativeofincreasingICP.F. Evaluatedressing.
1. Locationandamountofdrainage.2. Clarifywithsurgeonwhetherthenurseorthesurgeon
willchangedressing.3. EvaluateforCSFleakthroughtheincision.
L
CHAPTER 20 Neurologic System 411
G. Maintainsemi-Fowler’spositionifthereisaCSFleakfromearsornose.
H. Postoperative positioning for client who has hadinfratentorialsurgeryisasfollows:1. Bedshouldbeflat.2. Positionclientoneitherside;avoidsupineposition.3. Maintainheadandneckinmidline.4. Keep NPO for 24 hours to reduce edema around
medullaandreducevomiting. I. Postoperativepositionforclientwhohashadsupraten-
torialsurgery:semi-tolow-Fowler’sposition. J. Trendelenburg position is contraindicated for clients
who have had either infratentorial or supratentorialsurgery.
K. Maintainfluidregulation.1. Afterclientisawakeandtheswallowandgagreflexes
havereturned,beginofferingclearliquidsbymouth.2. Closelymonitorintakeandoutput.
L. Evaluateneurologicstatus inresponsetofluidbalanceanddiuretics.
M. Evaluatechangesintemperature:maybeduetorespira-torycomplicationsortoalterationinthefunctionofthehypothalamus.
N. Provideappropriatepostoperativepainrelief.1. Avoidnarcoticanalgesics.2. Acetaminophenisfrequentlyused.3. Maintainquiet,dimatmosphere.4. Avoidsuddenmovements.
O. Preventcomplicationsofimmobility(seeChapter3). P. Maintainseizureprecautions(seeAppendix20-5).
Home CareSeehomecareforclientwithincreasingICP.
Head InjuryA. Classification.
1. Penetratinghead injury:dura ispierced, as in stab-bingorshooting.
2. Closedorbluntheadinjury:headiseitherdrasticallyaccelerated(whiplash)ordecelerated(collision);mostcommonheadinjuryincivilianlife.
B. Children and infants are more capable of absorbingdirectimpactbecauseofthepliabilityoftheskull.
C. Coup-contrecoup injury: damage to the site of impact(coup) and damage on the side opposite the site of
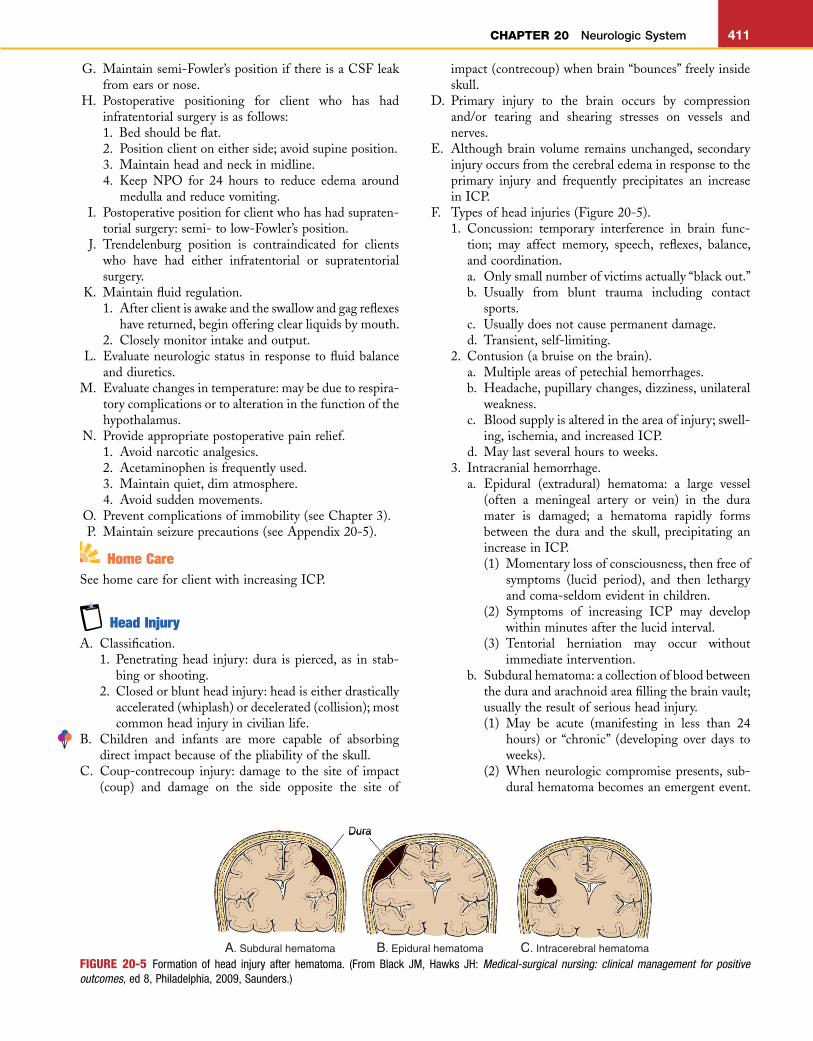
FIGURE 20-5 Formation of head injury after hematoma. (From Black JM, Hawks JH: Medical-surgical nursing: clinical management for positive outcomes, ed 8, Philadelphia, 2009, Saunders.)
Dura
A. Subdural hematoma B. Epidural hematoma C. Intracerebral hematoma
impact(contrecoup)whenbrain“bounces”freelyinsideskull.
D. Primary injury to the brain occurs by compressionand/or tearing and shearing stresses on vessels andnerves.
E. Althoughbrain volume remainsunchanged, secondaryinjuryoccursfromthecerebraledemainresponsetotheprimary injury and frequently precipitates an increaseinICP.
F. Typesofheadinjuries(Figure20-5).1. Concussion: temporary interference in brain func-
tion; may affect memory, speech, reflexes, balance,andcoordination.a. Onlysmallnumberofvictimsactually“blackout.”b. Usually from blunt trauma including contact
sports.c. Usuallydoesnotcausepermanentdamage.d. Transient,self-limiting.
2. Contusion(abruiseonthebrain).a. Multipleareasofpetechialhemorrhages.b. Headache,pupillarychanges,dizziness,unilateral
weakness.c. Bloodsupplyisalteredintheareaofinjury;swell-
ing,ischemia,andincreasedICP.d. Maylastseveralhourstoweeks.
3. Intracranialhemorrhage.a. Epidural (extradural) hematoma: a large vessel
(often a meningeal artery or vein) in the duramater is damaged; a hematoma rapidly formsbetween the dura and the skull, precipitating anincreaseinICP.(1) Momentarylossofconsciousness,thenfreeof
symptoms (lucid period), and then lethargyandcoma-seldomevidentinchildren.
(2) Symptoms of increasing ICP may developwithinminutesafterthelucidinterval.
(3) Tentorial herniation may occur withoutimmediateintervention.
b. Subduralhematoma:acollectionofbloodbetweentheduraandarachnoidareafillingthebrainvault;usuallytheresultofseriousheadinjury.(1) May be acute (manifesting in less than 24
hours) or “chronic” (developing over days toweeks).
(2) Whenneurologiccompromisepresents, sub-duralhematomabecomesanemergentevent.

L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
412 CHAPTER 20 Neurologic System
Emergencyneurosurgerymaybe required torelievepressureandpreventbrainherniation.
(3) Treatment may also include diuretics andanticonvulsants.
(4) Persistent neurologic complications—includ-ing dysarthria, unilateral weakness, memoryloss,andseizures—maycontinue.
4. With presence of retinal hemorrhage, evaluate for“shakenbabysyndrome.”
AssessmentA. Riskfactors/etiology.
1. Historyoftrauma.2. Epidural hematomas are rare in children younger
than4years.3. Subduralhematomasarecommonininfantsandmay
resultfrombirthtrauma.B. Clinicalmanifestations.
1. Epidural hematoma: decreased GCS, pupillarychanges,unilateralweakness.
2. Subdural hematoma: headache, change in LOC,numbness, headache, slurred speech, or inability tospeak.
C. Diagnostics(seeAppendix20-1).
ComplicationsComplications include increased ICP, meningitis, diabetesinsipidus,seizures,andpermanentneurologiccompromise.
Treatment
3. Bleedingorwaterydrainagefromtheearsornose.4. Lossoffeelingorsensationinanyextremity.5. Blurredvision,slurredspeech,vomiting.
NURSING PRIORITY The primary treatment objectives for the client with a head injury are to maintain a patent airway, to prevent hypoxia and hypercapnia resulting in acidosis, and to identify the occurrence of increased ICP.
A. Themajorityof clientswhoexperience concussionaretreatedathome.
B. Aperiodof unconsciousness or presenceof seizures isconsideredaseriousindicationofinjury.
C. Surgicalintervention.1. Burrholestoevacuatethehematoma.2. Craniotomy/craniectomy.
Nursing InterventionsGoal: To provide instruction for care of the client in the
homeenvironment(Box20-4).A. Problemsfrequentlydonotoccuruntil24hoursormore
aftertheinitialinjury.B. Observetheclientforincreasedperiodsofsleep;ifclient
isasleep,awakenevery2to3hourstodeterminewhetherclientcanbearousednormally.
C. Maintaincontactwithphysicianforreevaluationifcom-plicationsoccur.
D. Healthcareprovidershouldbenotifiedwhenanyofthefollowingareobserved:1. Any change in level of consciousness (increased
drowsiness,confusion).2. Inabilitytoarouseclient,seizures.
ALERT Determine family’s understanding of the consequences of the client’s illness. Written and oral instructions should be given to the client and to the family. Increased anxiety may affect comprehension of oral directions (see Box 20-4).
Box 20-4 DISCHARGE INSTRUCTIONS FOR CLIENTS WITH HEAD INJURY
Arousetheclientevery3to4hoursforthefirst24hours.Anticipatecomplaintsofdizziness,headaches.Donotallowclienttoblowhisnose;trytopreventsneezing.Noalcoholorsedativesforsleep.Acetaminophenforheadaches.Noexercisingovernext2to3days.Call the doctor if any of the following is noted:• Changeinvision:Blurredordiplopia• Poorcoordination:Walking,grasping• Drainage(serousorbloody)fromthenoseorears• Forcefulvomiting• Increasingsleepiness,moredifficulttoarouse• Slurredspeech• Headachethatdoesnotrespondtomedicationandcontin-
uestogetworse• Occurrenceofaseizure
Goal: Tomaintainhomeostasisandtomonitorandiden-tifyearlysymptomsofincreasedICP.
A. Bedrestandclearliquidsinitially.B. FrequentneurologicchecksforincreasedICP.
1. Changeordecrease in levelof consciousness is fre-quentlythefirstindication.
2. Instructclientswithheadinjurynottocough,sneeze,orblownose.
C. Evaluatedrainagefromnose,ears,andmouth.1. Donotcleanouttheears:place loosecottoninthe
auditorycanalandchangewhensoiled.2. Checkcontinuouscleardrainagefromthenosewith
Dextrostix; ifglucose ispresent, it is indicativeofaCSF leak; spinalfluid alsodrieswith a yellowhaloaroundedgesofdrainage.
3. IfaCSFleakoccurs,keeptheheadofthebedele-vated and monitor for development of an infection(meningitis).
D. Seizureprecautions(seeAppendix20-5).E. Maintain adequate fluid intake by IV infusion or oral
intake;donotoverhydrate.F. Assessforotherundetectedinjuries;stabilizespineafter
headinjuryuntilspinalcordinjuryisruledout.Goal: Toprovideappropriatenursinginterventionsforthe
clientexperiencinganincreaseinICP(seenursinggoalsforincreasedICP).
Goal: To provide adequate nutritional and caloric intakefortheclientwithaheadinjury.
A. Provideenteralfeedingsifclientisunabletoeat.B. Assistclienttotakeoralfeedingsonceswallowreflexis
normal;clientisatincreasedriskforaspiration.
L
CHAPTER 20 Neurologic System 413
Hydrocephalus Hydrocephalus is a condition caused by an imbalance in the pro-duction and absorption of CSF in the ventricles of the brain.
Classification: PrimaryA. Noncommunicating(obstructive):circulationofCSFis
blockedwithintheventricularsystemofthebrain.B. Communicating:CSFflowsfreelywithintheventricular
systembutisnotadequatelyabsorbed.
Classification: SecondaryA. Congenital.B. Acquired—possiblyfromtrauma,infection,ortumor.
AssessmentA. Riskfactors/etiology.
1. Neonate:usuallytheresultofacongenitalmalforma-tion.
2. Olderchild,adult.a. Space-occupyinglesion.b. Preexistingdevelopmentaldefects.
B. Clinicalmanifestations:infant.1. Headenlargement:increasingcircumferenceinexcess
ofnormal2cmpermonthforfirst3months.2. Separationofcranialsuturelines.3. Fontanelbecomestenseandbulging.4. Dilatedscalpveins.5. Frontalenlargement,bulging“sunseteyes.”6. SymptomsofincreasingICP.
C. Clinicalmanifestations:olderchild,adult.1. SymptomsofincreasingICP.2. Specificmanifestationsrelatedtositeofthelesion.
D. Diagnostics(seeAppendix20-1).1. Increasingheadcircumferenceisdiagnosticininfants.
TreatmentA. Noncommunicating and communicating: ventriculo-
peritonealshunt;CSFisshuntedintotheperitoneum.B. Obstructive: removal of the obstruction (cyst, hema-
toma,tumor).
Nursing InterventionsGoal: TomonitorforthedevelopmentofincreasingICP.A. Daily measurement of the frontal-occipital circumfer-
enceoftheheadininfants.B. AssessforsymptomsofincreasingICP(seeBox20-3).C. Infantisoftendifficulttofeed;administersmallfeedings
atfrequentintervalsbecausevomitingmaybeaproblem.Goal: TomaintainpatencyoftheshuntandmonitorICP
aftershuntprocedure.A. Position supine, with head turned opposite side up to
preventpressureontheshuntvalveandtopreventtoo-rapiddepletionofCSF.
B. Positionisnotaproblemwithchildrenwhoarehavingashuntrevision;theyhavenothadanincreaseinven-tricularpressure.
C. MonitorforincreasingICPandcomparewithpreviousdata.
D. Monitorforinfection,especiallymeningitisorenceph-alitis.
Home CareA. TeachparentssymptomsofincreasingICP.B. Have parents participate in care of the shunt before
client’sdischarge.C. Encourage parents and family to ventilate feelings
regardingclient’scondition.D. Referclienttoappropriatecommunityagencies.
Reye’s SyndromeReye’s syndrome is a rare acute illness that occurs after a viral illness (frequently, after aspirin has been consumed) and results in fatty infiltration of the liver and subsequent liver degeneration and increased intracranial pressure.A. Damaged liver cells no longer adequately convert
ammoniatoureaforexcretionfromthebody.B. Circulatingammoniacrossestheblood-brainbarrierto
produceacuteneurologiceffects.
AssessmentA. Riskfactors/etiology.
1. Mostoftenprecededbyanacuteviralinfection.2. Primarilyaffectschildrenfromtheageof6months
toadolescence.3. Frequently, the affected childhas received salicylate
(aspirin) for control of fever during the precedingviralinfection.
4. With warning labels now on aspirin, problem hassignificantlydecreased.
B. Clinicalmanifestations.1. Stage1.
a. Initialsymptommaybeseverepersistentvomiting.b. Lethargy,listlessness.
2. Stage2.a. Irritability,disorientation.b. ProgressestostateofincreasedICPwithdeepen-
ingcomaandposturing.C. Diagnostics(seeAppendix19-1).
1. Definitivediagnosisisaliverbiopsy.2. Prolongedprothrombintime.3. Elevatedbloodammonialevels.4. Elevated serum aspartate aminotransferase and ala-
nineaminotransferaselevels.
TreatmentA. Primarily supportive, based on stage of the disease;
mechanicalventilation,fluidandelectrolytebalance.B. MeasurestodecreaseICP.C. Earlyinterventioncriticaltosuccessfultreatment.
Nursing InterventionsGoal: To monitor progress of disease state and maintain
homeostasis.A. IVfluids.B. Monitorserumelectrolytesandliverfunctionstudies.C. Maintainrespiratorystatus;preventhypoxia.D. Assessforproblemsofimpairedcoagulation.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
414 CHAPTER 20 Neurologic System
E. Decreasestress,anxiety:childmaynotremembereventsbeforethecriticalphase.
Goal: To monitor for and implement nursing actionsappropriateforincreasingICP.
Stroke (Brain Attack)Stroke, or brain attack, is the disruption of the blood supply to an area of the brain, resulting in tissue necrosis and sudden loss of brain function. It is the leading cause of adult disability in the United States.A. Atherosclerosis (see Chapter 16), resulting in cerebro-
vasculardisease,frequentlyprecedesthedevelopmentofastroke.
B. Typesofstroke.1. Ischemicstroke.
a. Thrombotic stroke: formation of a clot thatresults in the narrowing of a vessel lumen andeventual occlusion; accounts for about 80% ofstrokes.(1) Associated with hypertension and diabetes
(i.e.,conditionsthatacceleratetheatheroscle-roticprocess).
(2) Producesischemiaofthecerebraltissuedistalto occlusion and edema to the surroundingareas.
b. Embolic stroke:occlusionof a cerebral arterybyanembolus.(1) Commonsiteoforiginistheendocardium.(2) May affect any age group; associated with
atrialfibrillation,endocarditis,andprostheticcardiacvalves.
2. Hemorrhagicstroke.a. Ruptureofacerebralarterycausedbyhyperten-
sion,trauma,oraneurysm.b. Bloodcompressesthebrain.
C. The area of edema resulting from tissue damage mayprecipitatemoredamagethanthevasculardamageitself.
D. TIAandRIND.1. Transientischemicattack(TIA,silentstroke).
a. Brief episode, less than 24 hours, of neurologicdysfunction; usually resolves within 30 to 60minutes.
b. Shouldbeconsideredawarningsignofanimpend-ingstroke.
c. Neurologicdysfunction ispresent forminutes tohours, but no permanent neurologic deficitremains.
2. Reversibleischemicneurologicdeficit(RIND).a. SymptomssimilartoTIA.b. Neurologic symptoms last longer than 24 hours
butlessthanaweek.3. Stroke:clienthasneurologicdeficitsrelatedtomobil-
ity,sensation,andcognition.E. Neuromusculardeficits resulting froma stroke aredue
todamageofmotorneuronsofthepyramidaltract.1. Damage to the left side of the brain will result in
paralysisoftherightsideofthebody(Figure20-6).
2. Bothupperandlowerextremitiesoftheinvolvedsideareaffected.
AssessmentA. Riskfactors/etiology(Box20-5).B. Clinicalmanifestations.
1. Transientischemicattack(TIA)andreversibleisch-emicneurologicdeficit(RIND).a. Visualdefects:blurredvision,diplopia,blindness
ofoneeye,tunnelvision.b. Transienthemiparesis,gaitproblems.c. Slurredspeech,confusion.d. Transientnumbnessofanextremity.
2. Completestroke(occurssuddenlywithanembolism,more gradually with hemorrhage or thrombosis);manifestations vary according to which cerebralvesselsareinvolved.a. Hemiplegia:lossofvoluntarymovement;damage
to the right sideof thebrainwill result in left-sidedweaknessandparalysis.
b. Aphasia: defect in using and interpreting thesymbolsoflanguage;mayincludewritten,printed,orspokenwords.
c. Maybeunawareoftheaffectedside;neglectsyn-dromeensues.
d. Cranial nerve impairment: chewing, gag reflex,dysphagia,impairedtonguemovement.
e. Maybeincontinentinitially.f. Agnosia:aperceptualdefectthatcausesadistur-
banceininterpretingsensoryinformation;client
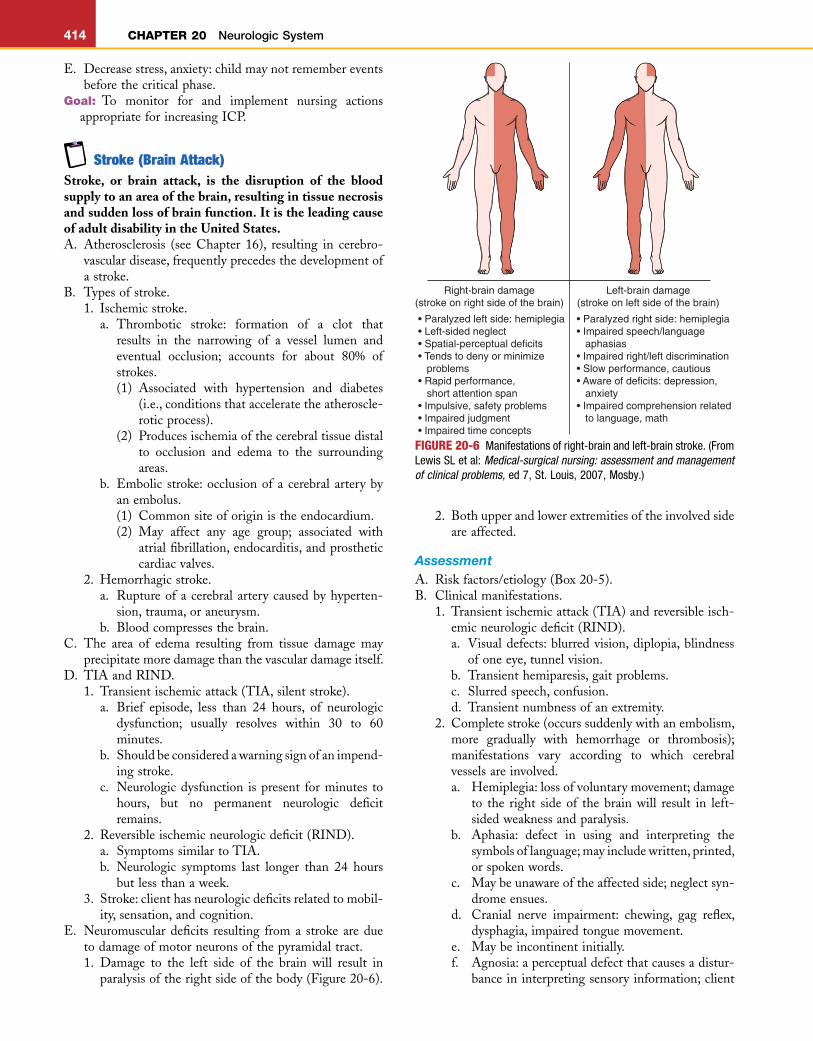
FIGURE 20-6 Manifestations of right-brain and left-brain stroke. (From Lewis SL et al: Medical-surgical nursing: assessment and management of clinical problems, ed 7, St. Louis, 2007, Mosby.)
Right-brain damage(stroke on right side of the brain)
Left-brain damage(stroke on left side of the brain)
• Paralyzed left side: hemiplegia• Left-sided neglect• Spatial-perceptual deficits• Tends to deny or minimize problems• Rapid performance, short attention span• Impulsive, safety problems• Impaired judgment• Impaired time concepts
• Paralyzed right side: hemiplegia• Impaired speech/language aphasias• Impaired right/left discrimination• Slow performance, cautious• Aware of deficits: depression, anxiety• Impaired comprehension related to language, math
L
CHAPTER 20 Neurologic System 415
maynotbeabletorecognizepreviouslyfamiliarobjects.
g. Cognitiveimpairmentofmemory,judgment,pro-prioception(awarenessofone’sbodyposition).
h. Hypotonia(flaccidity)fordaystoweeks,followedbyhypertonia(spasticity).
i. Visualdefects.(1) Homonymoushemianopia:lossofsamehalf
ofvisualfieldineacheye;clienthasonlyhalfofnormalvision.
(2) Horner’ssyndrome:ptosisoftheuppereyelid,constrictionofthepupil,andlackoftearingintheeye.
j. Apraxia:canmovetheaffectedlimbbutisunabletocarryoutlearnedmovements.
k. IncreasedICP,drowsinesstocoma. l. Painineye,nose,orface.m. Gaitdisturbances.
C. Diagnostics(seeAppendix20-1).
TreatmentA. Prophylactic.
1. Aspirin,plateletinhibitors.2. Antihypertensives,anticoagulants.
B. Immediate treatment (differs depending on whetherthromboticorhemorrhagicstroke).1. Medical.
a. Medicationstodecreasecerebraledema.(1) Osmoticdiuretics.(2) Corticosteroids(dexamethasone).
b. Anticoagulants for thrombotic stroke (neveradministeredtoaclientwithhemorrhagicstroke).
c. Anticonvulsants.
d. Thrombolytictherapyorfibrinolytictherapy(suchas recombinant tissue plasminogen activator(rtPA[Retavase])consideredfornonhemorrhagicstrokes within 3 hours of first manifestation ofstrokesigns.
e. Antihypertensivesandantidysrhythmics.2. Surgical.
a. Carotid endarterectomy, especially for transientischemicattack.
b. Craniotomyforevacuationofhematoma.c. Extracranial-intracranialbypassformildstrokes.
C. Specifictherapiestoresolvephysical,speechoroccupa-tionalcomplications,includinguseofassistivedevices.
Nursing InterventionsGoal: Topreventstrokethroughclienteducation(seeBox
20-5).A. Identificationof individualswith reversible risk factors
andmeasurestoreducethem.B. Appropriate medical attention for control of chronic
conditionsconducivetothedevelopmentofstroke.C. Teach high-risk clients early signs ofTIA and RIND
andtoseekmedicalattentionimmediatelyiftheyoccur.Goal: To maintain patent airway and adequate cerebral
oxygenation.A. Placeclientinside-lyingpositionwithheadelevated.B. Assess for symptomsofhypoxia; administeroxygenor
assistwithendotrachealintubationandmechanicalven-tilationasnecessary(seeAppendix15-8).
C. Maintain patent airway; use oropharyngeal airway topreventairwayobstructionbythetongue.
D. Client is prone to obstructed airway and pulmonaryinfection; have client cough and deep-breathe every2hours.
Goal: To assess for and implement measures to decreaseICP(seenursinggoalsforincreasedICP).
Goal: Tomaintainadequatenutritionalintake.A. Beforeoralfeedings,evaluateneedforswallowstudies.B. Administeroralfeedingswithcaution;startafterfirst24
hours;checkforpresenceofgagandswallowingreflexesbeforefeeding.
C. Place foodon theunaffected sideof themouth;beginwithclearfoods(gelatins).
D. Selectfoodsthatareeasytocontrolinthemouth(thickliquids) and easy to swallow; liquids often promotecoughing,becauseclientisunabletocontrolthem.
E. Maintainhigh-Fowler’spositionforfeeding.F. Maintainprivacyandunrushedatmosphere.G. Ifclientisunabletotolerateoralintake,enteralfeedings
maybeinitiated.
Box 20-5 RISK FACTORS ASSOCIATED WITH STROKE
Modifiable• Smoking• Obesity• Increasedsaltintake• Sedentarylifestyle• Increasedstress• Oralcontraceptives
Partially Modifiable• Hypertension• Cardiacvalvedisease• Dysrhythmias• Diabetesmellitus• Hypercholesterolemia
Nonmodifiable• Sex:Increasedincidenceinmen• Age• Race: Increased incidence in the African-American popu-
lation• Hereditarypredisposition
ALERT Identify potential for aspiration; assess client’s ability to eat.
Goal: Topreservefunctionofthemusculoskeletalsystem.A. Passiverangeofmotion(ROM)onaffectedside;begin
earlybecausetheexercisesaremoredifficult ifmusclesbegintotighten.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
416 CHAPTER 20 Neurologic System
B. ActiveROMonunaffectedside.C. Prevent foot drop: passive exercises; rigid boots; have
clientoutofbedassoonaspossible.D. Legsshouldbemaintainedinaneutralposition;prevent
externalrotationofaffectedhipbyplacingatrochanterrollorrolledpillowatthethigh.
E. Repositionevery2hours,but limit theperiodof timespentontheaffectedside.
Goal: Tomaintainhomeostasis.A. Evaluateadequacyofcardiacoutput.B. Monitorhydrationstatus:preventfluidoverload.
1. CarefullyregulateIVfluidintake.2. Evaluateresponsetodiuretics.3. Assessforthedevelopmentofperipheraledema.4. Restrictfluidintake,asindicated.5. Assess respiratory parameters indicative of fluid
overload.6. Monitordailyweight.
C. Determinepreviousbowelpatternsandpromotenormalelimination.1. Avoiduseofurinarycatheter, ifpossible; ifcatheter
isnecessary,removeassoonaspossible.2. Offerbedpanorurinalevery2hours;helpestablish
aschedule.3. Preventconstipation:provide increasedbulk indiet,
stoolsofteners,etc.4. Provide privacy and decrease emotional trauma
relatedtoincontinence.
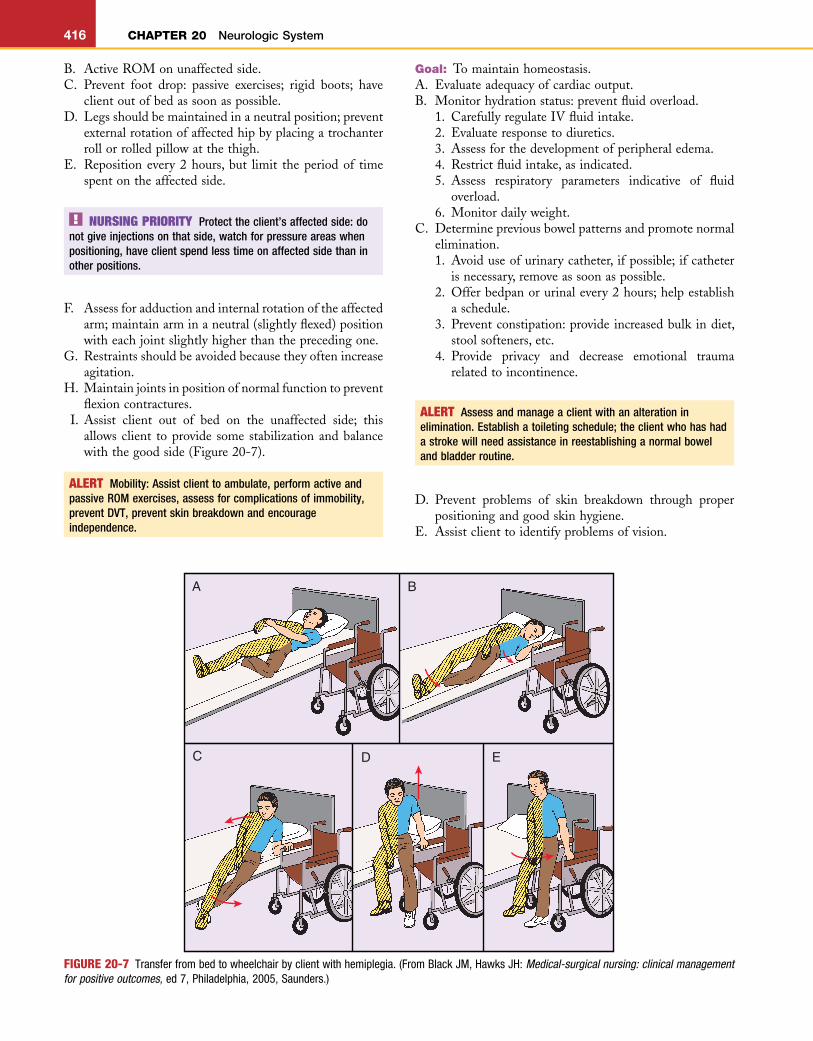
FIGURE 20-7 Transfer from bed to wheelchair by client with hemiplegia. (From Black JM, Hawks JH: Medical-surgical nursing: clinical management for positive outcomes, ed 7, Philadelphia, 2005, Saunders.)
EDC
BA
NURSING PRIORITY Protect the client’s affected side: do not give injections on that side, watch for pressure areas when positioning, have client spend less time on affected side than in other positions.
F. Assessforadductionandinternalrotationoftheaffectedarm;maintainarminaneutral(slightlyflexed)positionwitheachjointslightlyhigherthantheprecedingone.
G. Restraintsshouldbeavoidedbecausetheyoftenincreaseagitation.
H. Maintainjointsinpositionofnormalfunctiontopreventflexioncontractures.
I. Assist client out of bed on the unaffected side; thisallowsclient toprovide some stabilizationandbalancewiththegoodside(Figure20-7).
ALERT Mobility: Assist client to ambulate, perform active and passive ROM exercises, assess for complications of immobility, prevent DVT, prevent skin breakdown and encourage independence.
ALERT Assess and manage a client with an alteration in elimination. Establish a toileting schedule; the client who has had a stroke will need assistance in reestablishing a normal bowel and bladder routine.
D. Prevent problems of skin breakdown through properpositioningandgoodskinhygiene.
E. Assistclienttoidentifyproblemsofvision.
L
CHAPTER 20 Neurologic System 417
F. Maintainpsychologichomeostasis.1. Clientmaybeveryanxiousbecauseofalackofunder-
standingofwhathashappenedandbecauseofhisorherinabilitytocommunicate.
2. Speak slowly and clearly and explain what hashappened.
3. Assess client’s communication abilities and identifymethodstopromotecommunication.
Home CareA. EncourageindependenceinADLs.B. Provideclothingthatiseasytogetinandoutof.C. ActiveparticipationinROM;haveclientdohisorher
ownROMonaffectedside.D. Physical,occupational,andspeechtherapyforretraining
oflostfunction.E. Assist client tomaintain senseofbalancewhen in the
sittingposition;clientwillfrequentlyfalltotheaffectedside(unilateralneglectsyndrome).
F. Encourage participation in carrying out daily personalhygiene.
G. Teach client safe transfer from bed to wheelchair andprovideassistanceasneeded(seeFigure20-7).
H. Bowelandbladdertrainingprogram.1. Topromotebladdertone,encourageurination(with
or without assistance) every 2 hours rather thanallowingtheclienttovoidwhenheorshefeelstheurge.
2. TeachclienttoperformKegelexercisesregularly.3. Adviseclienttoavoidcaffeineintake.4. Increased bulk in diet will help avoid constipation
(seeTable18-2).5. Increasefluidsto2000mLperdayastolerated.6. AdministerstoolsoftenersPRN.7. Establishregulardailytimeforbowelmovements.
I. Encouragesocialinteraction(seeAppendix20-6).1. Speechtherapy.2. Frequentandmeaningfulverbalstimuli.3. Allowclientplentyoftimetorespond.4. Speakslowlyandclearly;donotgivetoomanydirec-
tionsatonetime.Useshortsentences.5. Donot“talkdownto”clientortreatclientasachild
(elderspeak).6. Client’smentalstatusmaybenormal;donotassume
itisimpaired.7. Nonverbalclientsdonotlosetheirhearingability.
J. Evaluate family supportandtheneed forhomehealthservices.
bral aneurysm occurring in the arterial junction of the circle of Willis. A ruptured cerebral aneurysm often results in hemorrhagic stroke.A. Asubarachnoidhemorrhageisapotentiallyfatalcondi-
tion in which blood accumulates below the arachnoidmaterinthesubarachnoidspace;mostoftenoccurssec-ondarytoananeurysm.
B. An aneurysm frequently ruptures and bleeds into thesubarachnoidspace.
C. Symptomsoccurwhenananeurysmenlarges,orwhenit ruptures. As blood collects in the subarachnoidspace, it compresses and damages the surroundingbraintissue.
D. Subarachnoidhemorrhagemayleadtoneurologiccom-promise including seizures, stroke, permanent braindamage,andevendeath.
E. Often, symptoms do not appear until rupture hasoccurred.
AssessmentA. Riskfactors/etiology.
1. Age:morecommoninadults30to60yearsofage.2. Atherosclerosis, connective tissue disease, cigarette
smoking,andhypertension—causingfragility in thevesselwall.
3. Head trauma and congenital vessel weakness mayincreasetherisk.
B. Clinicalmanifestations.1. Rupturemaybeprecededby:
a. Severeheadache.b. Intermittentnausea.
2. Rupturefrequentlyoccurswithoutwarning.a. Suddensevereheadache,seizures.b. Nuchalrigidity,hemiparesis.c. Lossofconsciousness.d. Symptoms of increasing ICP: nausea, vomiting,
photophobia.3. Severityofsymptomsdependsonthesiteandamount
ofbleeding.C. Diagnostics(seeAppendix20-1).
TreatmentA. Aminocaproicacid:inhibitsfibrinolysisinlife-threaten-
ingsituations.B. Osmoticdiuretics,anticonvulsants.C. Corticosteroids:dexamethasone(Decadron).D. Calcium channel blockers: minimize vasospasm after
hemorrhage.E. Stoolsofteners.F. Analgesicsforrecurrentheadache.G. Fluids to maintain systolic blood pressure at 100 to
150mmHg(increaseinvolumeandpressureincreasesbloodflowthroughnarrowedvessels).
H. Surgicalintervention:ligationor“clipping”oftheaneu-rysm to reduce the swellingandminimize the risk forre-bleeding.
I. Procedure to block abnormal arteries or veins andpreventbleeding.
ALERT Assist family to manage care of a client with long-term care needs; determine needs of family regarding ability to provide home care after discharge.
Cerebral Aneurysm, Subarachnoid HemorrhageA cerebral aneurysm occurs when a weakened saccular outpouching of the cerebral vasculature bulges from pres-sure on the weakened tissue. A Berry aneurysm is a cere-
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
418 CHAPTER 20 Neurologic System
Nursing InterventionsGoal: To prevent further increase in ICP and possible
rupture.A. Immediate bed rest; bathroom privileges may be
permitted.B. PreventValsalvamaneuver.C. Client should avoid straining, sneezing, pulling up in
bed,andacuteflexionoftheneck.D. Elevate head of the bed 30 degrees to 45 degrees to
promotevenousreturn.E. Quiet, dim, nonstimulating environment: disconnect
telephone;promoterelaxation.F. Constantmonitoringofconditiontoidentifyoccurrence
of bleeding, as evidenced by symptoms of increasingICP.
G. Administeranalgesicscautiously;theclientshouldcon-tinuetobeeasilyarousedsothatneurologiccheckscanbeperformed.
H. No hot or cold beverages or food, no caffeine, nosmoking.
I. Maintainseizureprecautions.
3. Chillsandhighfever.4. Severeandpersistentheadache.5. Increasing irritability, malaise, changes in level of
consciousness.6. Respiratorydistress.7. Generalizedseizures.8. Nauseaandvomiting.9. PositiveKernigsign:resistanceorpainattheknee
andthehamstringmuscleswhenclientattemptstoextendthelegafterthighflexion.
10. Positive Brudzinski sign: reflex flexion of the hipswhentheneckisflexed.
11. Photophobia.C. Clinicalmanifestations:neonateandinfant.
1. Fever.2. Apneicepisodes.3. Bulgingfontanel.4. Seizures.5. Cryingwithpositionchange.6. Opisthotonospositioning:adorsalarchedposition.7. Changesinsleeppattern,increasingirritability.8. Poorsucking;mayrefusefeedings.9. Poormuscletone,diminishedmovement.
10. Irritability.D. Diagnostics(seeAppendix20-1).
1. LumbarpuncturerevealsincreasingCSFpressure;ifICPispresent,thenaCTscanmaybedonebeforetheprocedure.
2. ElevatedWBCs.3. CSFandbloodculturespositive formeningococcus
bacteria.
TreatmentA. Respiratory isolation until positive organism is
identified.B. IVantibiotics,steroids(seeAppendixes6-9,6-7).C. Optimumhydration.D. Anticonvulsantmedications(seeAppendix20-2).E. Antivirals(seeAppendix7-1).F. Maintainventilation.
ComplicationsA. IncreasingICPresultinginpermanentbraindamage.B. Visualandhearingdeficits,paralysis.C. Subdural effusion; may be aspirated or allowed to
absorbwhenmeningitistreatmentisstartedandproteinleakstops.
Nursing InterventionsGoal: To identify the causative organism, control spread,
andinitiatetherapy.A. Maintainrespiratorydropletprecautionsuntilorganism
is identified; place client in a private room (Appendix6-9).
B. Begin administration of IV antibiotics after lumbarpunctureduringwhichCSFsamplewasobtained.
C. Identify family members and close contacts who mayrequireprophylactictreatment.
NURSING PRIORITY If the client survives the rupture of the aneurysm and re-bleeding occurs, it is most likely to occur within the next 24 to 48 hours.
Goal: To assess for and implement nursing measures todecreaseICP(seenursinggoalsforincreasedICP).
Goal: To provide appropriate preoperative nursing inter-ventions(seenursinggoalsforbraintumor).
Goal: To maintain homeostasis and monitor changes inICPaftercraniotomy(seenursinggoalsforcraniotomy).
MeningitisMeningitis is an acute viral or bacterial infection that causes inflammation of the meningeal tissue covering the brain and spinal cord.A. Infectious process increases permeability of protective
membraneandresultsinanincreasedproteinconcentra-tionintheCSF.
B. Inflammatoryprocessresultsinthedevelopmentofcere-braledema.
C. Bacterial meningitis is less common but more severethanviralmeningitis.
AssessmentA. Riskfactors/etiology.
1. Pathogenicorganismmostoftengainsentryfromaninfectionelsewhereinthebody.
2. Meningococcal meningitis is the only form that isreadilycontagious;transmittedbydirectcontactwithdropletsfromtheairwayofaninfectedperson.
3. Increasedmortalityrateamonginfants.B. Clinicalmanifestations:olderchildandadult.
1. Rash,petechiae,purpura.2. Nuchalrigidity.
L
CHAPTER 20 Neurologic System 419
Goal: To monitor course of infection and preventcomplications.
A. FrequentnursingassessmentforincreasedICP(seeBox20-3).
B. Maintain adequate hydration; cerebral edema mayrequirelimitingfluidintake.
C. MonitorinfusionsiteforcomplicationsofIVpiggybackantibiotics.
D. Assessforsideeffectsofhighdosageofantibiotics.E. Decreasestimuliinenvironment:dimlights,quietenvi-
ronment,noloudnoises.F. Avoidmovementorpositioningthat increasesdiscom-
fort;clientgenerallyassumesaside-lyingposition.G. Seizureprecautions.H. Preventcomplicationsofimmobility. I. Goodrespiratoryhygiene. J. Measurestodecreasefever.
encephalitisEncephalitis is an inflammatory process of the CNS, or “inflammation of the brain.”
AssessmentA. Riskfactors/etiology.
1. Commonly occurs as a complication after a viralinfection(measles,chickenpox,mumps).
2. Maybe transmittedbyavector suchas amosquitoortick.
3. Causative organism may be herpes simplex virus inmiddle-agedadults.
B. Clinicalmanifestations.1. Severeheadache,nuchalrigidity.2. Suddenfever.3. Seizures.4. Changesinlevelofconsciousness.5. Motor involvement: ataxia, dysphasia, tremor,
convulsions.6. Drowsiness,confusion,disorientation.7. Irritability.8. Bulgingfontanelsininfants.
C. Diagnostics.1. ExaminationoftheCSF.2. Viralstudiestoisolatethevirus.3. EEGforseizureactivity.4. BloodtestforWestNilevirus.
TreatmentA. Anticonvulsants.B. TreatmenttodecreaseICP.C. Hydration,bedrest,propernutrition.
Nursing InterventionsNursinginterventionsforencephalitisarethesameasthosefor meningitis, with the exception of antibiotic therapy.Encephalitisiscausedbyaviralagentandisnotresponsivetoantibiotic therapy;antibiotic therapymaybeorderedtopreventbacterialinfection.
Spinal Cord InjurySpinal cord injury (SCI) is damage to the spinal cord housed inside the spinal column. Most SCIs exist with the spinal cord intact yet compromised from injury or disease. SCI most often occurs as a result of direct trauma to the head or neck area.A. Riskfactors.
1. Morethan80%ofclientswithSCIsaremale.2. MorethanhalfofSCIsoccurbetweentheagesof16
and35years.3. Alsoanincreasedriskafter60yearsofage,whenfalls
becomemorecommon.4. Otherriskfactors:osteoarthritis,cancer,involvement
insports.B. Initiallyaftertheinjury,thenervefibersswell,andcir-
culationtothespinalcordisdecreased;hemorrhageandedemaoccur,causinganincreaseintheischemicprocess,which progresses to necrotic destruction of the spinalcord.
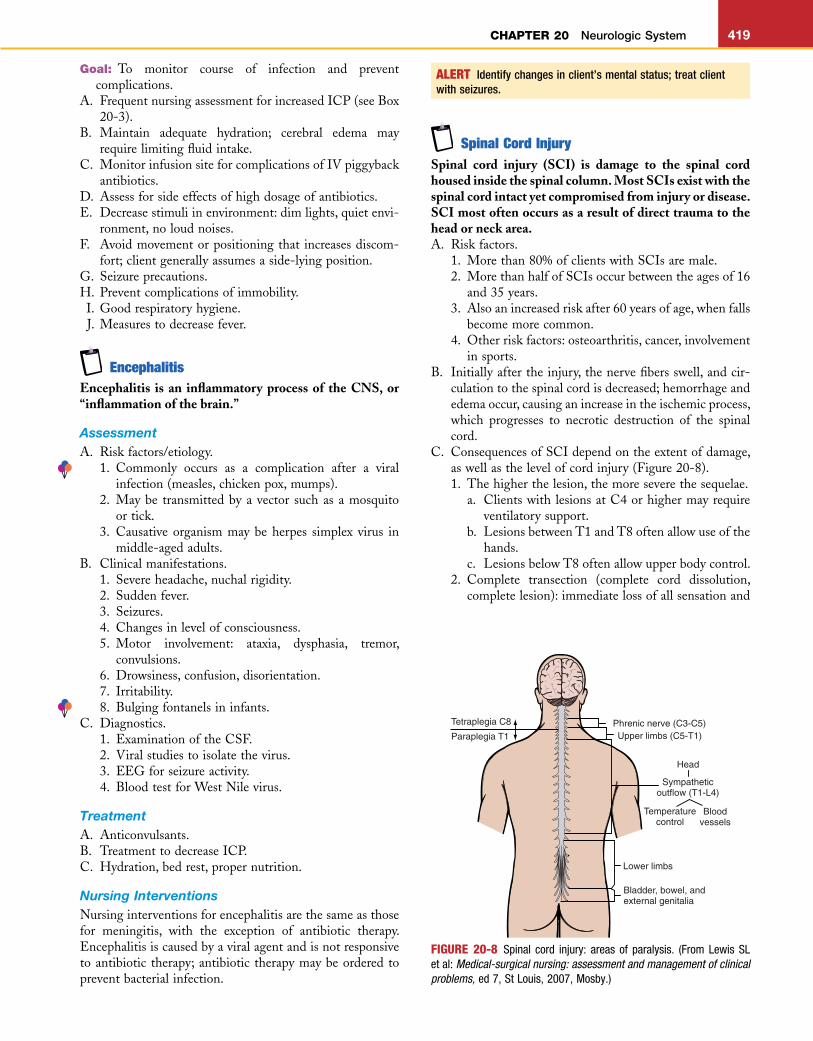
C. ConsequencesofSCIdependontheextentofdamage,aswellasthelevelofcordinjury(Figure20-8).1. Thehigherthelesion,themoreseverethesequelae.
a. ClientswithlesionsatC4orhighermayrequireventilatorysupport.
b. LesionsbetweenT1andT8oftenallowuseofthehands.
c. LesionsbelowT8oftenallowupperbodycontrol.2. Complete transection (complete cord dissolution,
completelesion):immediatelossofallsensationand
ALERT Identify changes in client’s mental status; treat client with seizures.
FIGURE 20-8 Spinal cord injury: areas of paralysis. (From Lewis SL et al: Medical-surgical nursing: assessment and management of clinical problems, ed 7, St Louis, 2007, Mosby.)
Tetraplegia C8
Paraplegia T1Phrenic nerve (C3-C5)Upper limbs (C5-T1)
Head
Lower limbs
Bladder, bowel, and external genitalia
Sympatheticoutflow (T1-L4)
Temperaturecontrol
Bloodvessels
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
420 CHAPTER 20 Neurologic System
voluntary movement below the level of injury;minimal,ifany,returnoffunction.
3. Incomplete(partial).a. Central cord syndrome: center of cord is
damaged; results primarily in impairment ofupperextremities.
b. Damagetoonesideofthecord(Brown-Séquardsyndrome): motor function and position sensemaybepresentononeside;temperatureandsen-sationmaybelostontheoppositeside.
c. Anterior cord damage: disruption of blood flowresultsinamixedlossofsensoryandmotorfunc-tionbelowthelevelofinjury.
4. Cordedemapeaksinabout2to3daysandsubsideswithinabout7daysaftertheinjury.
5. Lumbosacralinjuries.a. Variablepatternofmotorandsensoryloss.b. Frequentlyresultinneurogenicbowelandbladder.
D. Spinalcordshock(areflexia):temporarylossordysfunc-tion of spinal reflex activity; occurs predominantly incompletecord lesions; lossof communicationwith thehighercentersofcontrolresultsinflaccidityandlossoffunctionalcontrolbelowthelevelofinjury.1. SCIinterruptssympatheticnerveimpulsetransmis-
sion; parasympathetic impulses are not counter-checked, resulting in vasodilation; loss of venousreturn results in hypotension, which is neurogenicshock.
2. Hypothalamus loses control of body temperature,which assists in vasoconstriction and vasodila-tion.
3. Conditionmaypersist forseveralweeksandreversespontaneously; resolution of spinal shock will beevidentbyreturnofreflexes.
4. Hyperreflexiawilloccurasrecoveryprogresses;spasticmovementsmaybeprecipitatedbyemotionandcuta-neousstimulation.
E. AutonomicdysreflexiaoccursinclientswithaninjuryatT6orhigher.1. A noxious stimulus below the level of injury trig-
gers the sympathetic nervous system, which causesa release of catecholamines (epinephrine, norepi-nephrine).
2. Mostcommonstimulicausingtheresponseareafullbladder or bowel, UTI, pressure ulcers, and skinstimulation.
3. Severe hypertension (systolic may be greater than300), nausea, poundingheadache, bradycardia, rest-lessness,flushingpiloerection,andblurredvisionarethemostcommonbodyresponses.
F. Bladderdysfunctionwilloccurasaresultoftheinjury;normalbladdercontrolisdependentonthesensoryandmotor pathways and the lower motor neurons beingintact.1. Neurogenicbladderoccursinclientswithbothupper
andlowermotorneurondisorders.a. Upper motor neuron disorders produce a spastic
orreflexbladder.
b. Lowermotorneurondisorders produce aflaccidbladder.
2. Managementofbladderproblemsdependsonclient’spreferencesandlifestyle,aswellasclient’sfunctionalabilities.
G. Long-term rehabilitation potential depends on theamountofdamagedonetothecord,whichmaynotbeevidentuntilseveralweeksaftertheinjury.
AssessmentA. Clinical manifestations: depend on level of SCI (see
Figure20-8).1. Injury at C3 through C5 will cause respiratory
compromise.2. Dependingondegreeofinjury,thedegreeofparalysis
andamountofsensorylossbelowthelevelofinjurywillvary.
3. Spinalshock.a. Generallyoccurswithin72hoursandmaylastfor
severalweeks.b. Flaccidparalysis.c. Lossofsensationandabsenceofreflexes.d. Bowelandbladderdysfunction.e. Hypotensionandbradycardia.f. After spinal shock, reflexes and autonomic
activity return, as evidenced by development ofspasticity.
4. Autonomicdysreflexia inclientswith injuriesatT6orhigher.a. Severehypertension,bradycardia.b. Complaintsofheadache.c. Flushing and diaphoresis above level of
injury.B. Diagnostics(seeAppendix20-1).C. Complications.
1. Respiratorystasis;pulmonaryedemaandemboli.2. Cardiovascular compromise from neurogenic shock,
orautonomicdysreflexia.3. Skin breakdown resulting in localized and systemic
infections.4. Immobility issues causing renal andgastrointestinal
compromise.5. Psychologic,social,andbodyimageissues.
TreatmentA. Emergencyinterventionrequired.B. Corticosteroids within 8 hours of injury (methylpred-
nisolone).C. Immobilization of the vertebral column in cervical
fracture.1. Cervicaltongs(Crutchfield,Gardner-Wells)forcer-
vicalimmobility.2. Halovest/jackettractiontopromotemobility.3. Sterno-occipital mandibular immobilizer (SOMI)
bracewornwithcervicalfusion.D. Spinal surgery to remove bone fragments and assure
spinalalignment.E. Respiratorysupportasnecessary.
L
CHAPTER 20 Neurologic System 421
Nursing InterventionsGoal: To maintain stability of the vertebral column and
preventfurthercorddamage.A. Emergencycareandtreatment.
1. SuspectSCIifthereisanyevidenceofdirecttraumatotheheadorneckarea(contactsports,divingacci-dents,motorvehicleaccident).
2. Immobilizeclientandplaceonspinalboardwiththeheadandneckinaneutralposition;donotallowthenecktoflex.
3. Airway, status of breathing, and circulation are theprimaryconcernsinitiallyafterinjury.
4. Neurogenic shock may occur within the first 24hours;observefordecreasedB/P,severebradycardia.
Goal: To identify level of damage and changes in neuro-logicstatus.
A. Assess respiratory function: symmetrical chest expan-sion,bilateralbreath sounds,presenceof retractionsordyspnea.
B. Motorandsensoryevaluation.1. Ability tomoveextremities; strengthof extremities.2. Sensoryexamination,includingtouchandpain.3. Presenceofdeeptendonreflexes.
C. Ongoingassessmentandstatusof:1. Bladder,gastric,bowelfunction.2. Psychologicadjustmenttotheinjury.
D. Evaluatehistoryofhowinjuryoccurred;obtaininforma-tionregardinghowclientwastransported.
E. Determinestatusofpain.Goal: Tomaintainrespiratoryfunction.A. Frequentassessmentof respiratory functionduringthe
first48hours.1. Changesinbreathingpattern.2. Observe breathing pattern for use of sternocleido-
mastoidandintercostalmusclesforrespiration.3. Evaluatearterialbloodgasvaluesandpulseoximetry.4. Determinedevelopmentofhypoxia.
B. Maintainadequaterespiratoryfunction,asindicated.1. Chestphysiotherapy.2. Incentivespirometry.3. Changingpositionwithinlimitsofinjury.4. Assess for complications of atelectasis, pulmonary
emboli,andpneumonia.5. Nasopharyngealorendotrachealsuctioningbasedon
airwayandlevelofinjury.Goal: Tomaintaincardiovascularstability.A. Spinalshock.
1. Monitorvitalsignsandevaluatechanges.2. Vagal stimulation, hypothermia, and hypoxia may
precipitatespinalshock.3. Assess deep tendon reflexes and muscle strength as
resolutionofshockoccurs.B. Assess for development of autonomic dysreflexia; if it
occurs:1. Elevate the head of the bed, and check the client’s
bloodpressure.2. Assess for sources of stimuli: distended bladder
(checkurinarytubing),fecalimpaction,constipation,tightclothing.
3. Relievethestimuli,anddysreflexiawillsubside.4. Maintain cardiovascular support during period of
hypertension.5. A hypertensive crisis from dysreflexia will require
immediateintervention.C. Evaluatecardiovascularresponseswhenturningorsuc-
tioningclient.D. Apply antiembolism stockings or elastic wraps to the
legstofacilitatevenousreturn.(Lackofmuscletoneandlossofsympathetictoneintheperipheralvesselsresultin decreases in both venous tone and venous return,whichpredisposeclienttodeepveinthrombosis.)
E. Implementmeasurestopromotevenousreturn.
NURSING PRIORITY Do not hyperextend the neck in a client with a suspected cervical injury. Airway should be opened by the jaw-lift method. Improper handling of the client often results in extension of the damaged area.
5. Maintain in extended position with no twisting orturning;donotremovecervicalcollarorspinalboarduntilareaofinjuryisidentified.
6. Maintainpatentairwayduringtransportation.B. Maintainstabilityof thevertebralcolumnas indicated
bythelevelofinjury.1. Prescribeandmaintainbedrestonfirmmattresswith
supportive devices (sandbags, skin traction, etc.);maintain alignment in the supine position; logrollwithoutanyflexionortwisting.
2. Maintaincervicaltraction:tongsareinsertedintotheskullwithtractionandweightsapplied;donotremoveweights;logrolltomaintainspinalimmobility.
3. Halo vest/jacket traction: maintains cervical immo-bilitybutallowsclienttobemobile.a. If bolts or screws come loose, keep the client
immobilizedandcallthedoctor.b. Cleanpinsitesaccordingtofacilitypolicy,observe
forinfection.c. Rollclientontohisorhersideattheedgeofthe
bedandallowclienttopushupfromthemattresstoasittingposition.Neverusethehalovestframetoassisttheclienttoturnorsitup.
d. Correctsizeofwrenchshouldbekeptatbedsideto remove the anterior bolts in case ofemergency.
e. Assist client tomaintainbalancewhenstanding;thetractionisheavyforapersonwhoisweak,andtheclientisatincreasedriskforfalling.
4. Maintainextremitiesinneutral,functionalposition.
ALERT Apply, maintain, or remove orthopedic devices (e.g. traction, splints, braces, casts).
C. Performappropriatenursinginterventionwhensurgeryisindicatedtostabilizetheinjury.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
422 CHAPTER 20 Neurologic System
Goal: Tomaintainadequatefluidandnutritionalstatus.A. Duringthefirst48hours,evaluategastrointestinalfunc-
tionfrequently;decreaseinfunctionmaynecessitateuseofanasogastrictubetodecreasedistention.
B. Preventcomplicationsofnauseaandvomiting.C. Evaluatebowelsoundsandclient’sabilitytotolerateoral
fluids.D. Increase protein and calories in diet; may need to
decreasecalciumintake.E. Evaluateforpresenceofparalyticileus.F. Increaseroughageindiettopromotebowelfunction.Goal: To prevent complications of immobility (see
Chapter3).Goal: Topromotebowelandbladderfunction.A. Urineisretainedasaresultofthelossofautonomicand
reflexivecontrolofthebladder.1. Intermittent catheterization or indwelling catheter
maybeusedinitiallytopreventbladderdistention.2. Perform nursing interventions to prevent urinary
tract infection; avoid urinary catheterization, ifpossible.
B. Determinetypeofbladderdysfunctionbasedonlevelofinjury.
C. Assessclient’sawarenessofbladderfunction.D. Initiatemeasurestoinstitutebladdercontrol.
1. Establishascheduleforvoiding;haveclientattempttovoidevery2hours.
2. UsetheCredémethod(inadults)formanualexpres-sionofurine.
3. Maybenecessarytoteachclientself-catheterization.4. Recordoutputandevaluate forpresenceof residual
urine.E. Evaluatebowelfunctioning.
1. Incontinenceandparalyticileusfrequentlyoccurwithspinalshock.
2. Incontinenceandimpactionarecommonlater.F. Initiatemeasurestopromotebowelcontrol(afterspinal
shockisresolved).1. Identifyclient’sbowelhabitsbeforeinjury.2. Maintainsufficientfluidintakeandadequatebulkin
thediet.3. Establish specific time each day for bowel evacua-
tion.4. Assessclient’sawarenessofneedtodefecate.5. Teach client effective use of the Valsalva maneuver
toinducedefecation.6. Inducedefecationbydigitalstimulation,suppository,
orasalastresort,enema.
Goal: Tomaintainpsychologicequilibrium.A. Providesimpleexplanationsofallprocedures.B. Anticipate outbursts of anger and hostility as client
beginstoworkthroughthegrievingprocessandadjuststochangesinbodyimage.
C. Anticipateandacceptperiodsofdepressioninclient.D. Encourageindependencewheneverpossible;allowclient
to participate in decisions regarding care and to gaincontroloverenvironment.
ALERT Prevent complications of immobility; prevent venous stasis: identify symptoms of deep venous thrombosis, apply compression stockings, and change client’s position.
ALERT Assess and manage a client with alteration in elimination; initiate a toileting schedule; the client with SCI may need bowel and bladder retraining, depending on level of the injury.
ALERT Plan measures to deal with client’s anxiety and promote client’s adjustment to changes in body image; assist client and significant others to adjust to role changes. Note: These items are all part of the test plan, and the test could include questions about the client with SCI.
E. Encouragefamily involvement in identifyingappropri-atediversionalactivities.
F. Avoidsympathyandemphasizeclient’spotential.G. Initiate frank, open discussion regarding sexual func-
tioning.H. Assistclientandfamilytoidentifycommunityresources. I. Assistclienttosetrealisticshort-termgoals.
Myasthenia GravisMyasthenia gravis is a sporadic, progressive neuromuscu-lar disease characterized by a decrease in the acetylcholine level at the receptor sites in the neuromuscular junction. This inadequate acetylcholine level results in a distur-bance in nerve impulse transmission, causing progressive weakness in skeletal muscles. Myasthenia gravis literally means “grave muscle weakness.”
AssessmentA. Riskfactors/etiology.
1. Autoimmunedisease.2. Morecommoninwomenyoungerthan40andmen
olderthan60butmayoccuratanyage.B. Clinicalmanifestations.
1. Primaryproblemisskeletalmusclefatiguewithsus-tained muscle contraction; symptoms are predomi-nantlybilateral.a. Muscularfatigueincreaseswithactivity.b. Ptosis (drooping of the eyelids) and diplopia
(doublevision)arefrequentlythefirstsymptoms.(Ophthalmologist may be first contact regardingdysfunction.)
c. Impairmentoffacialmobilityandexpression.d. Impairmentofchewingandswallowing.e. Speechimpairment(dysarthria).f. No sensory deficit, loss of reflexes, or muscular
atrophy.g. Poorbowelandbladdercontrol.
2. Courseisvariable.a. Maybeprogressive.b. Maystabilize.c. May be characterized by short remissions and
exacerbations.
L
CHAPTER 20 Neurologic System 423
3. Myastheniccrisis:anacuteexacerbationofsymptomsthatmayrequireintubationandmechanicalventila-tion to support respiratory effort; caused by majormuscularweaknessandinabilitytomaintainrespira-toryfunction.a. Severerespiratorydistressandhypoxia.b. Increasedpulseandbloodpressure.c. Decreasedorabsentcoughorswallowreflex.
4. Cholinergiccrisis:atoxicresponsetotheanticholin-esterase medications; anticholinesterase medicationsmustbewithheld—thisresponseisrarewithproperdosingofMestinon.a. Nausea,vomiting,anddiarrhea.b. Weaknesswithdifficultyinswallowing,chewing,
andspeaking.c. Increasedsecretionsandsaliva.d. Musclefasciculation,constrictedpupils.
C. Diagnostics(seeAppendix20-1).1. Electromyography: shows a decreasing response of
musclestostimuli.2. Ice pack test: assess clients with ptosis; muscles
improvewithcoldapplication;placepackonclosedlidsfor2minutestoseewhetherptosisimproves.
3. Tensilontest.a. Usedfordiagnosingmyastheniagravis.b. Usedtodifferentiatecholinergiccrisisfrommyas-
theniccrisis.c. IV injection of neostigmine or edrophonium
causes immediate, although short-lived, relief ofmuscleweakness.
TreatmentA. Anticholinesterase (cholinergic) medications (see
Appendix20-3).1. Neostigmine(Prostigmin).2. Pyridostigmine(Mestinon).
B. Corticosteroids(seeAppendix6-7).C. Plasma electrophoresis (plasmapheresis): separation
of plasma to remove autoantibodies from the blood-stream.
D. Immunosuppressivetherapy.E. Surgicalremovalofthethymus(thymectomy).
Nursing InterventionsClientmaybehospitalizedforacutemyastheniccrisisorforrespiratorytractinfection.Goal: Tomaintainrespiratoryfunction.A. Assess for increasing problems of difficulty breathing.
Measureforcedvitalcapacityfrequentlytoassessrespi-ratorystatus.
B. Determine client’s medication schedule. When wasmedicationlasttaken?
C. Assess ability to swallow; prevent problems ofaspiration.
D. Evaluateeffectivenessofcoughreflex.E. Bepreparedtointubateorprovideventilatoryassistance.Goal: To distinguish between a myasthenic crisis and a
cholinergiccrisis.A. Maintainadequateventilatorysupportduringcrisis.B. AssistinadministrationofTensilontesttodifferentiate
crisis.1. Myastheniccrisis:client’sconditionwillimprove.2. Cholinergiccrisis:client’sconditionwilltemporarily
worsen.C. If myasthenic crisis occurs, neostigmine may be
administered.D. If cholinergic crisis occurs, atropine may be adminis-
tered,andcholinergicmedicationsmaybereevaluated.E. Avoid use of sedatives and tranquilizers, which causes
respiratorydepression.F. Providepsychologicsupportduringcrisis.
Home CareA. Teach client importance of taking medication on a
regularbasis;peakeffectofthemedicationshouldcoin-cidewithmealtimes.
B. Ifptosisbecomessevere,clientmayneedtowearaneyepatchtoprotectcornea(alternateeyepatchesifproblemisbilateral).
C. Emotionalupset,severefatigue,infections,andexposureto extreme temperatures may precipitate a myastheniccrisis.
Multiple SclerosisMultiple sclerosis (MS) is characterized by multiple areas of demyelination from inflammatory scarring of the neurons in the brain and spinal cord (CNS).A. Theprogressionofthediseaseresultsintotaldestruction
ofthemyelin,andthenervefibersbecomeinvolved.1. Lossofmyelinsheathcausesdecreasedimpulsecon-
duction,destructionofthenerveaxon,andablockageoftheimpulseconduction.
2. The demyelination occurs in irregular scatteredpatchesthroughouttheCNS.
3. Theoriesastocauseincludeautoimmunityandexpo-suretoviruses.
B. Clinicalcourse.1. Relapsing-remitting MS: most common course,
causing sporadic attacks with exacerbations andremissions lasting days to months; client has a sig-nificant“flare-up”orexacerbation,followedbypartialorcompleterecovery.
2. Primary-progressiveMS:afteranumberofyearsofthe relapsing-remitting form, client experiences aslow steady worsening of symptoms without com-plete improvement between exacerbations; plateausofseveritymayoccur,butbaselinefunctionprogres-sivelyworsens.
3. Secondary-progressive MS: progressively worsensfrom onset with acute exacerbations; baseline func-tioncontinuestoworsen.
ALERT Identify clients at high risk for aspiration; do not give the client experiencing a myasthenic crisis anything to eat or drink.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
424 CHAPTER 20 Neurologic System
4. Progressive-relapsingMS:gradualprogressivewors-eningofdiseasewithoutremissions;onsetinthirdorfourthdecadeoflifewithequalincidenceinmenandwomen.
AssessmentA. Riskfactors/etiology:causeisunknown.
1. Morecommoninwomen.2. Problemofyoungadults.3. Morecommonincoolerclimates.
B. Clinicalmanifestations.1. Signsandsymptomsvaryfrompersontoperson,as
wellaswithinthesameindividual,dependingontheareaofinvolvement.
2. Cerebellardysfunction:nystagmus,ataxia,dysarthria,dysphagia.
3. Motordysfunction:weaknessofeyemuscles,weak-nessorspasticityofmusclesinextremities.
4. Sensory: vertigo, blurred vision, decreased hearing,tinnitus.
5. Bowelandbladderdysfunction.6. Sexualdysfunction.7. Psychosocial.
a. Intellectualfunctioningremainsintact.b. Emotionallability:increasedexcitabilityandinap-
propriateeuphoria.c. Emotional effects of the chronic illness and
changesinbodyimage.C. Diagnostics:nodefinitivediagnostictest.
TreatmentA. Nocure;medical treatment isdirected toward slowing
ofthediseaseprocessandreliefofsymptoms.B. Medicationstodecreaseedemaandinflammationofthe
nervesites.1. Antiinflammatoryagents.2. Immunosuppressiveagents:interferons.3. Adrenocorticotropic hormone for acute exacerba-
tions.
Nursing InterventionsClient may be hospitalized for diagnostic workup or fortreatmentofacuteexacerbationandcomplications.Goal: Tomaintainhomeostasisandpreventcomplications
duringanacuteexacerbationofdiseasesymptoms.A. Maintainadequaterespiratoryfunction.
1. Preventrespiratorytractinfection.2. Goodpulmonaryhygiene.3. Preventaspiration;sittingpositionforeating.4. Evaluateadequacyofcoughreflex.
B. Maintainurinarytractfunction.1. Preventurinarytractinfection.2. Increasefluidintake,atleast2000mL/24hr.3. Evaluate voiding: assess for retention and inconti-
nence.C. Maintainnutrition.
1. Evaluatecoughingandswallowingreflexes.2. Providefoodthatiseasytochew.
3. Ifclientisexperiencingdifficultyswallowing,observeclientcloselyduringfluidintake.
Goal: To prevent complications of immobility (seeChapter3).
Goal: Topromotepsychologicwell-being.A. Focusonremainingcapabilities.B. Encourageindependenceandassistclienttogaincontrol
overenvironment.C. Ifimpotenceisaproblem,initiatesexualcounseling.D. Assistclienttoworkthroughthegrievingprocess.E. Identifycommunityresourcesavailable.
Home CareA. Medicalregimenandsideeffectsofthemedications.B. Physical therapy to maintain muscle function and
decreasespasticity.C. Measures to maintain voiding; may need to perform
self-catheterization.D. Safetymeasuresbecauseofdecreasedsensation.
1. Checkbathwatertemperature.2. Wearprotectiveclothinginthewinter.3. Avoidheatingpadsandclothingthatisconstrictive.
E. Client should understand that relapses are frequentlyassociatedwith an increase inphysiologic andpsycho-logicstress.
ALERT Determine client’s ability to care for self; plan with family to assist client to meet self-care needs.
Guillain-Barré SyndromeGuillain-Barré syndrome is an acute, rapidly progressing motor neuropathy involving segmental demyelination of nerve roots in the spinal cord and medulla. Demyelination causes inflammation, leading to edema, nerve root com-pression, decreased nerve conduction, and rapidly ascend-ing paralysis. Both sensory and motor impairment occur. It is also called Landry’s paralysis.
AssessmentA. Risk factors/etiology: cause is unknown; frequently,
clienthasarecenthistoryofacuteillness.B. Clinicalmanifestations.
1. Progressiveweaknessandparalysisbegininthelowerextremitiesandascendbilaterally.
2. Paralysisascendsthebodysymmetrically.a. Paralysisofrespiratorymuscles.b. Cranial nerve involvement, most often facial
nerve (CN VII), produces difficulty talking andswallowing.
3. Loss of sensation and function of bowel andbladder.
4. Manifestations may progress rapidly over hours ormayoccurover2to4weeks.
5. Muscleatrophyisminimal.6. Paralysisdecreasesastheclientbeginsrecovery;most
often,therearenoresidualeffects.
L
CHAPTER 20 Neurologic System 425
C. Diagnostics(seeAppendix20-1).1. ElevatedproteinconcentrationinCSF.
Treatment (Supportive)A. Respiratorysupport,possiblymechanicalventilation.B. Corticosteroids.C. Immunosuppressivesandimmunoglobulins.D. Plasmapheresis:plasmaexchange.
Nursing InterventionsGoal: Toevaluateprogressofparalysisandinitiateactions
topreventcomplications.A. Evaluate rate of progress of paralysis; carefully assess
changesinrespiratorypattern.B. Frequentevaluationofcoughandswallowreflexes.
1. Remainwithclientwhileclientiseating;havesuctionequipmentavailable.
2. MaintainNPO(nothingbymouth)statusifreflexesareinvolved.
C. If assent of paralysis is rapid, prepare for endotrachealintubationandrespiratoryassistance.
D. Prevent complications of immobility during period ofparalysis(seeChapter3).
E. Assess for involvement of the autonomic nervoussystem.1. Orthostatichypotension.2. Hypertension.3. Cardiacdysrhythmias.4. Urinaryretentionandparalyticileus.
Goal: To prevent complications of hypoxia if respiratorymusclesbecomeinvolved(seeChapter15).
Goal: Tomaintainpsychologichomeostasis.A. Simpleexplanationofprocedures.B. Completerecoveryisanticipated.C. Provide psychologic support during period of assisted
ventilation.D. Keepclientandfamilyawareofprogressofdisease.
Amyotrophic Lateral SclerosisAmyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a rapidly progressive, invariably fatal degeneration of nerves controlling voluntary muscles. Replacement of motor neurons with fibrous tissues causes hardening of anterior and lateral columns of the spinal cord, thus “lateral sclerosis.”
AssessmentA. Clinicalmanifestations.
1. Twitching,cramping,andmuscleweakness.2. Dysarthriaanddysphagia.3. Fatigue;asymmetricalmuscleatrophyandweakness.
4. Progressivemuscleweakness.a. Begins with upper extremities and progressively
involvesmusclesofneckandthroat.b. Trunk and lower extremities are involved late in
courseofdisease.5. Mostoftenfatalwithin2to5yearsafteronset.6. Intellectualfunctioningandallfivesensesareusually
unaffected.B. Diagnostics: electromyography and nerve conduction
studies. Muscle biopsy may be performed to rule outotherpathologies.
TreatmentA. Riluzole (Rilutek)prolongs lifeby a fewmonths;pro-
tectsmotorneuronsfromdegenerationanddeath.B. Supportivecare.
Nursing InterventionsGoal: Toprovideongoingassessmentinassistingclientto
dealwithprogressivesymptoms.A. PromoteindependenceinADLs.
1. Conserveenergy;spaceactivities.2. Avoidextremesofhotandcold.3. Useofappliancestoprolongindependenceinambu-
lationandADLs.B. Promotenutrition.
1. Smallfrequentfeedings.2. Have client sit upright with head slightly flexed
forwardwhileeating.3. Keep suction equipment easily available during
meals.C. Encouragefamilyandclienttotalkaboutlossesandthe
difficultchoicestheyface.D. Assist family and client to identify need for advanced
directivesandtocompletethem.
Muscular DystrophyMuscle dystrophy (MD) is a group of genetic diseases characterized by progressive weakness and skeletal muscle degeneration affecting a variety of muscle groups. The term pseudohypertrophy describes the characteristic muscle enlargement (caused by fatty infiltration) that occurs in muscular dystrophy.A. Duchenne’s muscular dystrophy is the most common
andmostsevereformofMD.B. Condition is characterized by gradual degeneration of
musclefibersandprogressivesymmetricalweaknessandwastingofskeletalmuscle.
AssessmentA. Riskfactors/etiology.
1. Genetic: sex-linked disorder primarily affectingmales.
2. Onset generally occurs between the ages of 3 and5years.
B. Clinicalmanifestations.1. Historyofdelay inmotordevelopment,particularly
adelayinwalking.
NURSING PRIORITY Of the neuromuscular disorders, Guillain-Barré syndrome is the most rapidly developing and progressive condition. It is potentially fatal if unrecognized.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
426 CHAPTER 20 Neurologic System
2. Abnormalwaddlinggait.a. Child falls frequentlyanddevelopscharacteristic
mannerofrising.b. Gower’s sign: from sitting or squatting position,
thechildassumesakneelingpositionandpushesthetorsoupby“walking”hisorherhandsupthethighs.
3. Progressive muscle weakness, atrophy, and contrac-tures.a. Ambulationisfrequentlyimpossiblebytheageof
9to11years.b. Ultimately destroys essential muscles of respira-
tion;deathoccursfromrespiratorytractinfectionorcardiacfailure.
C. Diagnostics.1. Electromyography,musclebiopsy.2. Serum enzymes: creatinine phosphokinase level is
increasedinneonate,thengraduallydeclines.
TreatmentA. Steroids administered to boys older than 5 years
ofage.
Nursing InterventionsChildisfrequentlycaredforathomeandhospitalizedonlywhencomplicationsoccur.Goal: To maintain optimal motor function as long as
possible.A. Regularphysicaltherapyforstretchingandstrengthen-
ingmuscles;ROMexercises.B. Maintainchild’sindependenceinADLs.C. Assistfamilytoidentifyresources,toadaptphysiologic
barriers within the home, and to promote mobility ofthechildinawheelchair.
D. Assistfamilytoidentifymethodsofpreventingrespira-torytractinfection;assessforrespiratoryproblems.
E. Provide braces, splints, and assistive devices asneeded.
Goal: Toassistparentsandchild tomaintainpsychologicequilibriumandtoadapttochronicillness.
A. Assist parents to understand importance of indepen-dence and self-help skills; frequently, parents areover-protectiveofthechild.
B. Counseling to assist parents and family members toidentify family activities that can be modified to meetchild’sneeds.
C. Mothermayfeelparticularlyguiltybecauseoftransmis-sionofdiseasetoherson.
D. Identifyavailablecommunityresources.E. Counselingtoassistfamilyandchildwithchronicillness
andchild’seventualdeath.
Cerebral PalsyCerebral palsy is a nonprogressive, lifelong neuromuscu-lar genetic disorder resulting from damaged motor centers of the brain that cause nerve impulses to be incorrectly sent and/or received. The overall result is impairment of muscle control with poor muscle coordination.
AssessmentA. Riskfactors/etiology.
1. Mayresultfromexistingprenatalbrainabnormalities(kernicterus,hemolyticdiseaseofnewborn).
2. Prematurityissinglemostimportantdeterminantofcerebralpalsy;however,inabout24%ofcases,causeisnotidentifiable.
B. Clinicalmanifestations.1. Delayedachievementofdevelopmentalmilestones.2. Increased or decreased resistance to passive move-
ment.3. Abnormalposture.4. Presenceofinfantilereflexes(tonicneckreflex,exag-
geratedMororeflex).5. Associateddisabilities.
a. Mentalretardation,seizures.b. Attention-deficitproblems.c. Visionandhearingimpairment.
6. Muscletightnessandspasms.C. Diagnostics.
1. Diagnosticteststoruleoutotherneurologicdysfunc-tion:EEG,MRI,bloodtests.
2. Frequentlydifficulttodiagnoseinearlymonths;con-ditionmaynotbeevidentuntilchildattemptstositaloneorwalk.
3. Gaitlabanalysis:evaluateswalkingability.
TreatmentA. Maintainandpromotemobilitywithorthopedicdevices
andphysicaltherapy.B. Skeletalmusclerelaxants.C. Anticonvulsants,asindicated.
Nursing InterventionsChildisfrequentlycaredforathomeandonanoutpatientbasisunlesscomplicationsoccur.Goal: To assist child to become as independent and self-
sufficientaspossible.A. Physical therapy program designed to assist individual
childtogainmaximumfunction.B. Assist child to progress according to developmental
level and functional abilities; encourage crawling,sitting, and balancing appropriate to developmentallevel.
C. Assist child to carry out ADLs as age and capacitiespermit.
D. Speechtherapy,asindicated.E. Encourageplayappropriateforage.F. Encourageappropriateeducationalactivities.G. Bowelandbladdertrainingmaybedifficultbecauseof
poorcontrol.Goal: Tomaintainphysiologichomeostasis.A. Maintainadequatenutrition.
1. Mayexperiencedifficultyeatingbecauseofspasticity;may drool excessively; use of manual jaw controlwhenfeeding.
2. Encourage independence in eating and use of self-helpdevices.
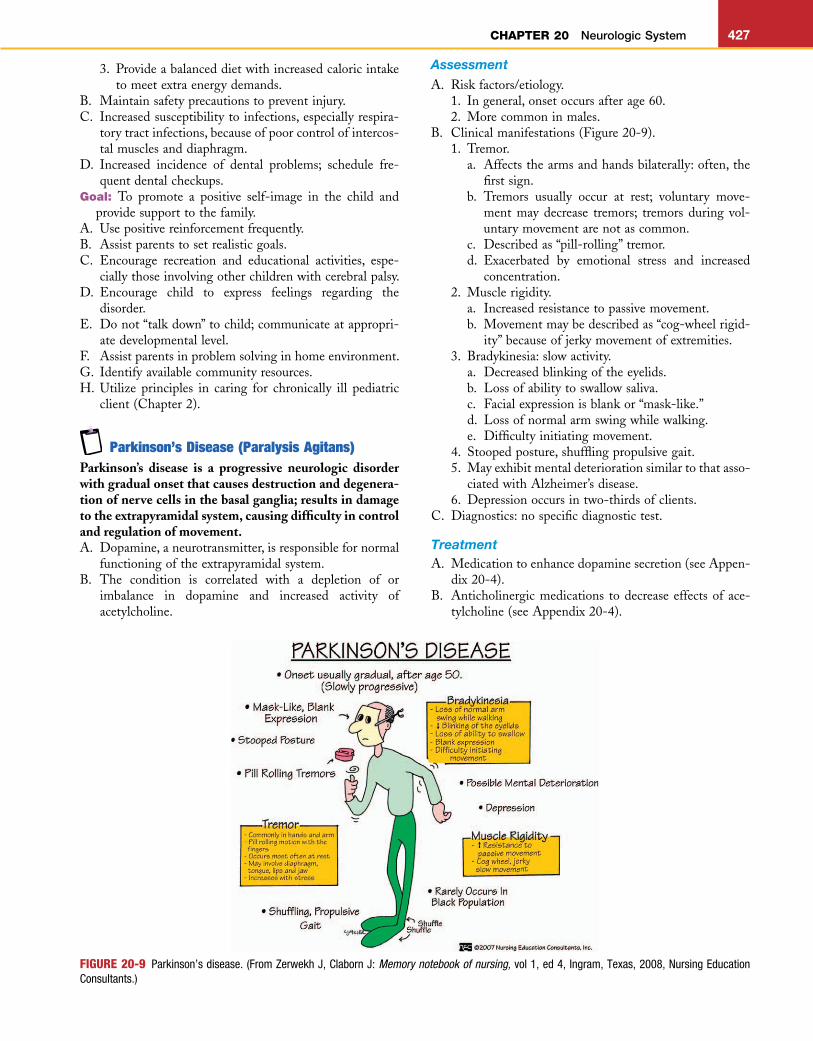
L
CHAPTER 20 Neurologic System 427
3. Provideabalanceddietwithincreasedcaloricintaketomeetextraenergydemands.
B. Maintainsafetyprecautionstopreventinjury.C. Increasedsusceptibilitytoinfections,especiallyrespira-
torytractinfections,becauseofpoorcontrolofintercos-talmusclesanddiaphragm.
D. Increased incidence of dental problems; schedule fre-quentdentalcheckups.
Goal: To promote a positive self-image in the child andprovidesupporttothefamily.
A. Usepositivereinforcementfrequently.B. Assistparentstosetrealisticgoals.C. Encourage recreation and educational activities, espe-
ciallythoseinvolvingotherchildrenwithcerebralpalsy.D. Encourage child to express feelings regarding the
disorder.E. Donot“talkdown”tochild;communicateatappropri-
atedevelopmentallevel.F. Assistparentsinproblemsolvinginhomeenvironment.G. Identifyavailablecommunityresources.H. Utilize principles in caring for chronically ill pediatric
client(Chapter2).
Parkinson’s Disease (Paralysis Agitans)Parkinson’s disease is a progressive neurologic disorder with gradual onset that causes destruction and degenera-tion of nerve cells in the basal ganglia; results in damage to the extrapyramidal system, causing difficulty in control and regulation of movement.A. Dopamine,aneurotransmitter,isresponsiblefornormal
functioningoftheextrapyramidalsystem.B. The condition is correlated with a depletion of or
imbalance in dopamine and increased activity ofacetylcholine.
FIGURE 20-9 Parkinson’s disease. (From Zerwekh J, Claborn J: Memory notebook of nursing, vol 1, ed 4, Ingram, Texas, 2008, Nursing Education Consultants.)
AssessmentA. Riskfactors/etiology.
1. Ingeneral,onsetoccursafterage60.2. Morecommoninmales.
B. Clinicalmanifestations(Figure20-9).1. Tremor.
a. Affectsthearmsandhandsbilaterally:often,thefirstsign.
b. Tremors usually occur at rest; voluntary move-ment may decrease tremors; tremors during vol-untarymovementarenotascommon.
c. Describedas“pill-rolling”tremor.d. Exacerbated by emotional stress and increased
concentration.2. Musclerigidity.
a. Increasedresistancetopassivemovement.b. Movementmaybedescribedas“cog-wheelrigid-
ity”becauseofjerkymovementofextremities.3. Bradykinesia:slowactivity.
a. Decreasedblinkingoftheeyelids.b. Lossofabilitytoswallowsaliva.c. Facialexpressionisblankor“mask-like.”d. Lossofnormalarmswingwhilewalking.e. Difficultyinitiatingmovement.
4. Stoopedposture,shufflingpropulsivegait.5. Mayexhibitmentaldeteriorationsimilartothatasso-
ciatedwithAlzheimer’sdisease.6. Depressionoccursintwo-thirdsofclients.
C. Diagnostics:nospecificdiagnostictest.
TreatmentA. Medicationtoenhancedopaminesecretion(seeAppen-
dix20-4).B. Anticholinergicmedications todecreaseeffectsof ace-
tylcholine(seeAppendix20-4).
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
428 CHAPTER 20 Neurologic System
C. Clients frequentlybecome tolerant tomedications andrequireadjustmentsintypesofmedicationsandmedica-tionschedules.
D. Surgicaltherapy:aimistodecreasesymptoms.1. Ablation(destructionoftissue).2. Deepbrainstimulation(DBS).
Nursing InterventionsGoal: Tomaintainhomeostasis.A. EncourageindependenceinADLswithuseofself-help
devices.B. Maintainnutrition.
1. Increase calories and protein; provide more easilychewedfoods.
2. Frequentsmallmeals.3. Allowampletimeforeating.4. Monitorweightloss.5. Providepleasantatmosphereatmealtime;clientfre-
quentlypreferstoeatalonebecauseofdifficultyswal-lowingandinabilitytocontrolsaliva.
6. Increasefluid intakewith increasedbulk inthediettodecreaseproblemwithconstipation.
C. Maintainmusclefunction.1. FullROMtoextremitiestopreventcontracture.2. Decreaseeffectsoftremors.3. Exerciseandstretchdaily.4. Physicaltherapy,asindicated.
D. Closelymonitor response toor changes in response tomedications.
accompanied by dizziness, tinnitus, or lacrimation;associatedwithstressandpremenstrualsyndrome.
2. Migraine:constrictionofintracranialvessels leadingtoan intense throbbingpainwhenvessels return tonormal; prodromal or aura; crescendo quality; uni-lateral pain, often beginning in eye area; nausea,vomiting, photophobia—migraines are seriouslydebilitating and may require lifestyle and occupa-tional changes.
3. Clusterheadache:rareheadachethatismorecommoninmen;occurs innumerousepisodesorclusters;noaura; unilateral pain often arising in nostril andspreadingtoforeheadandeye;oftenoccursatsametimeofday.
TreatmentA. Migraine: sumatriptan (Imitrex); dihydroergotamine
mesylate(Migranal).B. Nonsteroidalantiinflammatorydrugs.C. Relaxation,yoga,stressmanagement.D. Clusterheadachestreatedwithhighflowoxygen.
Nursing InterventionsA. Prevention: recognize triggers, decrease stress, adjust
medicationsduringmenstrualcycle.B. Watch for signsofominousheadache:new-onsetuni-
lateralheadacheinpersonolderthan35years;vomitingnotaccompaniedbynausea;painthatawakensclient.
C. Encourage client to keep a “headache diary” for bestmanagementandtreatment.
Trigeminal NeuralgiaTrigeminal neuralgia is a fleeting unilateral sensory dis-turbance of cranial nerve V, causing brief, paroxysmal pain and facial spasm; also known as tic douloureux.
AssessmentA. Riskfactors/etiology.
1. Onset generally occurs between 20 and 40 yearsofage.
2. Increasedfrequencywithaging.B. Clinicalmanifestations.
1. Abruptonsetofparoxysmalintensepaininthelowerandupperjaw,cheek,andlips.a. Tearingoftheeyesandfrequentblinking.b. Facialtwitchingandgrimacing.c. Painisusuallybrief;endsasabruptlyasitbegins.d. Pain may be described as severe, stabbing, and
shock-like.2. Recurrenceofpainisunpredictable.3. Pain is initiated by cutaneous stimulation of the
affectednervearea.a. Chewing.b. Washingtheface.c. Extremesoftemperature:eitheronthefaceorin
food.d. Brushingteeth.
ALERT Identify situations that necessitate role changes; evaluate family involvement in health care; review necessary modifications to promote home safety.
Goal: Topromoteapositiveself-image.A. Encouragediversionalactivities.B. Assistclienttosetrealisticgoals.C. Explore reasons for depression; encourage client to
discusschangesoccurringinlifestyle.D. Assist client ingainingcontrolofADLsandenviron-
ment.E. Assistclienttoidentifyandavoidactivitiesthatincrease
frustrationlevels.F. Encouragegoodpersonalhygiene.
HeadacheHeadache is a very common symptom of various underly-ing pathologic conditions in which pain-sensitive nerve fibers respond to unacceptable levels of stress and tension, muscular contraction in the upper body, pressure from a tumor, or increased ICP.
AssessmentA. Typesofheadaches.
1. Tension headache (muscle contraction headache):most commonof allheadaches; feelingof tightnesslikeabandaroundthehead;onsetisgradual;maybe
L
CHAPTER 20 Neurologic System 429
TreatmentA. Medicalmanagementofpain(seeAppendix20-2):car-
bamazepine(Tegretol)andgabapentin(Neurontin).B. Surgicalintervention.
1. Localnerveblock.2. Surgical intervention to interrupt nerve impulse
transmission.a. Percutaneous stereotactic rhizotomy—destroys
someofthenervefibers;assiststomanagepain.b. Microvascular decompression (craniotomy) to
relievepainandpreservefacialsensation.
Nursing InterventionsGoal: Tocontrolpain.A. Assessthenatureofapainfulattack.B. Identify triggering factors; adjust environment to
decreasefactors.1. Keeproomataneven,comfortabletemperature.2. Avoidtouchingclient.3. Avoidjarringthebed.4. AllowclienttocarryoutownADLsasnecessary.
C. Administeranalgesicstodecreasepain.
4. Maintainmeticulousoralhygiene.5. Havefrequentdentalcheckups.
Bell’s PalsyBell’s palsy is a transient cranial nerve disorder affecting the facial nerve (cranial nerve VII), characterized by a dis-ruption of the motor branches on one side of the face, which results in muscle weakness or flaccidity on the affected side.
AssessmentA. Clinicalmanifestations.
1. Lagorinabilitytocloseeyelidonaffectedside.2. Droopingofthemouth.3. Decreasedtastesensation.4. Upward movement of the eyeball when the eye is
beingclosed.B. Diagnostics(seeAppendix20-1).
TreatmentA. Corticosteroids:administrationshouldbestartedimme-
diatelyaftersymptomsarise.B. Antivirals.C. Moistheatmayrelievepain,ifpresent.
Nursing InterventionsGoal: Toassessnervefunctionandpreventcomplications.A. Analgesicstodecreasepain.B. Evaluateabilityofclienttoeat.C. Meticulousoralhygiene.D. Preventdryingofthecorneaontheaffectedside.
1. Instill methylcellulose drops frequently duringtheday.
2. Ophthalmic ointment and eye patches may berequiredatnight.
E. As function returns, active facial exercises may beperformed.
Goal: Toassistclienttomaintainapositiveself-image.A. Changesinphysicalappearancemaybedramatic.B. Tellclientthattheconditionisusuallyself-limitingwith
minimal,ifany,residualeffects.C. Clientmayrequirecounseling,ifchangeinfacialappear-
anceispermanent.
NURSING PRIORITY Because of the severe pain caused by the condition, clients are susceptible to severe depression and suicide.
Goal: Tomaintainnutrition.A. Frequently,clientdoesnoteatbecauseofreluctanceto
stimulatethepain.B. Providelukewarmfoodthatcanbeeasilychewed.C. Increaseproteinandcalories.
Home CareA. Identifypresenceofcornealreflex;provideprotectiveeye
careifreflexisabsent.B. Ifthereislossofsensationtothesideoftheface,client
should:1. Chewontheunaffectedside.2. Avoidtemperatureextremesinfoods.3. Check themouthafter eating to remove remaining
particlesoffood.
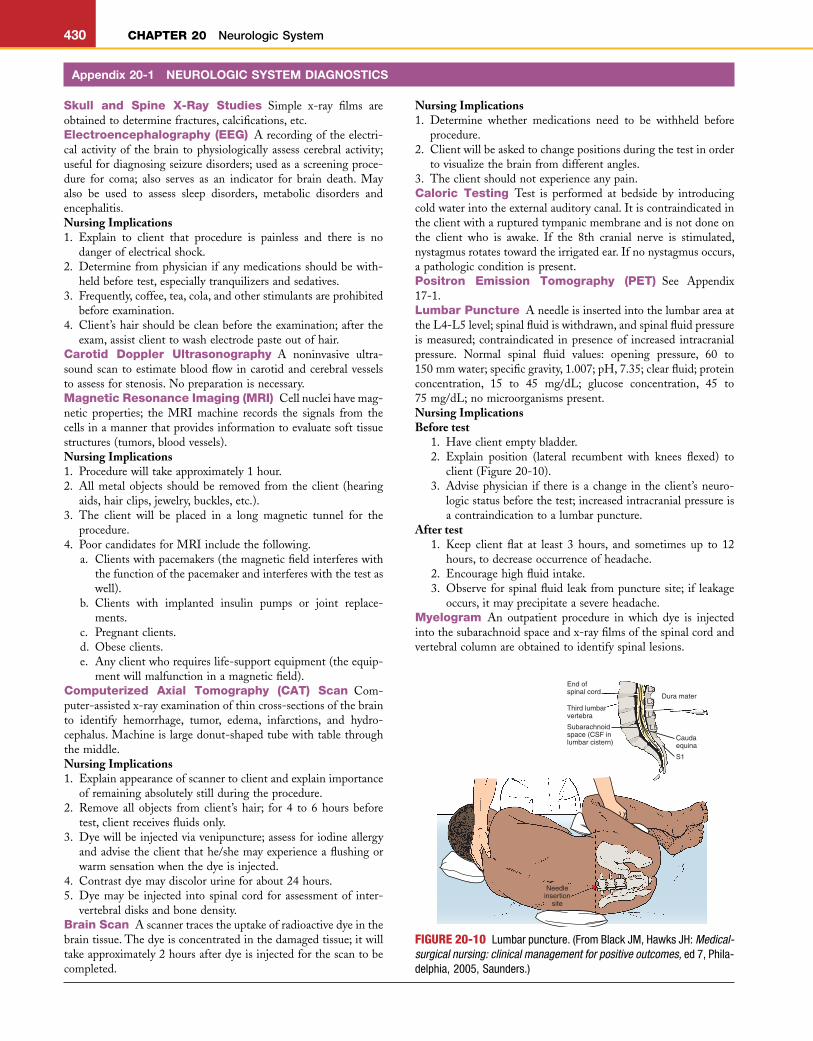
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
430 CHAPTER 20 Neurologic System
Skull and Spine X-Ray Studies Simple x-ray films areobtainedtodeterminefractures,calcifications,etc.Electroencephalography (EEG) Arecordingoftheelectri-calactivityof thebrain tophysiologicallyassesscerebralactivity;usefulfordiagnosingseizuredisorders;usedasascreeningproce-dure for coma; also serves as an indicator for brain death. Mayalso be used to assess sleep disorders, metabolic disorders andencephalitis.Nursing Implications1. Explain to client that procedure is painless and there is no
dangerofelectricalshock.2. Determinefromphysicianifanymedicationsshouldbewith-
heldbeforetest,especiallytranquilizersandsedatives.3. Frequently,coffee,tea,cola,andotherstimulantsareprohibited
beforeexamination.4. Client’shairshouldbecleanbeforetheexamination;afterthe
exam,assistclienttowashelectrodepasteoutofhair.Carotid Doppler Ultrasonography A noninvasive ultra-soundscantoestimatebloodflowincarotidandcerebralvesselstoassessforstenosis.Nopreparationisnecessary.Magnetic Resonance Imaging (MRI) Cellnucleihavemag-netic properties; the MRI machine records the signals from thecellsinamannerthatprovidesinformationtoevaluatesofttissuestructures(tumors,bloodvessels).Nursing Implications1. Procedurewilltakeapproximately1hour.2. Allmetalobjects shouldbe removed from theclient (hearing
aids,hairclips,jewelry,buckles,etc.).3. The client will be placed in a long magnetic tunnel for the
procedure.4. PoorcandidatesforMRIincludethefollowing.
a. Clientswithpacemakers(themagneticfieldinterfereswiththefunctionofthepacemakerandinterfereswiththetestaswell).
b. Clients with implanted insulin pumps or joint replace-ments.
c. Pregnantclients.d. Obeseclients.e. Anyclientwhorequireslife-supportequipment(theequip-
mentwillmalfunctioninamagneticfield).Computerized Axial Tomography (CAT) Scan Com-puter-assistedx-rayexaminationofthincross-sectionsofthebrainto identify hemorrhage, tumor, edema, infarctions, and hydro-cephalus.Machineislargedonut-shapedtubewithtablethroughthemiddle.Nursing Implications1. Explainappearanceofscannertoclientandexplainimportance
ofremainingabsolutelystillduringtheprocedure.2. Remove all objects from client’s hair; for 4 to 6 hours before
test,clientreceivesfluidsonly.3. Dyewillbeinjectedviavenipuncture;assessforiodineallergy
andadvisetheclientthathe/shemayexperienceaflushingorwarmsensationwhenthedyeisinjected.
4. Contrastdyemaydiscolorurineforabout24hours.5. Dyemaybe injected into spinal cord forassessmentof inter-
vertebraldisksandbonedensity.Brain Scan Ascannertracestheuptakeofradioactivedyeinthebraintissue.Thedyeisconcentratedinthedamagedtissue;itwilltakeapproximately2hoursafterdyeisinjectedforthescantobecompleted.
Nursing Implications1. Determine whether medications need to be withheld before
procedure.2. Clientwillbeaskedtochangepositionsduringthetestinorder
tovisualizethebrainfromdifferentangles.3. Theclientshouldnotexperienceanypain.Caloric Testing Test is performed at bedside by introducingcoldwaterintotheexternalauditorycanal.Itiscontraindicatedintheclientwitharupturedtympanicmembraneandisnotdoneonthe client who is awake. If the 8th cranial nerve is stimulated,nystagmusrotatestowardtheirrigatedear.Ifnonystagmusoccurs,apathologicconditionispresent.Positron Emission Tomography (PET) See Appendix17-1.Lumbar Puncture AneedleisinsertedintothelumbarareaattheL4-L5level;spinalfluidiswithdrawn,andspinalfluidpressureismeasured;contraindicated inpresenceof increased intracranialpressure. Normal spinal fluid values: opening pressure, 60 to150mmwater;specificgravity,1.007;pH,7.35;clearfluid;proteinconcentration, 15 to 45 mg/dL; glucose concentration, 45 to75mg/dL;nomicroorganismspresent.Nursing ImplicationsBefore test
1. Haveclientemptybladder.2. Explain position (lateral recumbent with knees flexed) to
client(Figure20-10).3. Advisephysician if there isachange in theclient’sneuro-
logicstatusbeforethetest;increasedintracranialpressureisacontraindicationtoalumbarpuncture.
After test1. Keep client flat at least 3 hours, and sometimes up to 12
hours,todecreaseoccurrenceofheadache.2. Encouragehighfluidintake.3. Observe forspinalfluid leakfrompuncturesite; if leakage
occurs,itmayprecipitateasevereheadache.Myelogram An outpatient procedure in which dye is injectedintothesubarachnoidspaceandx-rayfilmsofthespinalcordandvertebralcolumnareobtainedtoidentifyspinallesions.
Appendix 20-1 NEUROLOGIC SYSTEM DIAGNOSTICS
FIGURE 20-10 Lumbar puncture. (From Black JM, Hawks JH: Medical-surgical nursing: clinical management for positive outcomes, ed 7, Phila-delphia, 2005, Saunders.)
Dura mater
End of spinal cord
Caudaequina
Third lumbarvertebra
Subarachnoidspace (CSF inlumbar cistern)
Needleinsertion
site
L2
L3
L4
L5
S1
L
CHAPTER 20 Neurologic System 431
Nursing ImplicationsBefore test
1. Sameasforlumbarpuncture.2. Checkwhetherclienthasanyallergiestodye.
After test1. Keep the head of the bed elevated 30 to 50 degrees to
decreasedispersionofthedyeintheCSFandtothebrain.2. Headachemayoccurasa resultof irritationof thecentral
nervoussystem.3. Clientshouldnotreceiveanyofthephenothiazinesbefore
orimmediatelyaftertheexamination.Cerebral Angiogram Injection of contrast material into thecerebralcirculation;seriesofx-rayfilmsistakentostudythecere-bralbloodflow;dye isusually injected via a soft catheter that isinsertedandthreadedthroughthefemoralartery.Nursing ImplicationsBefore test
1. Clientshouldbewell-hydrated,butshouldreceivenothingbymouthfor6to8hoursbeforethetest;clientshouldvoidbeforeprocedure.
2. Determineifclienthasanyallergiestoiodineortoshellfish.3. Informclientthatheorsheshouldremainverystillduring
theprocedure.4. Afeelingofwarmthinthefaceandmouthandametallic
tasteinthemoutharecommonwhendyeisinjected.
Appendix 20-1 NEUROLOGIC SYSTEM DIAGNOSTICS—cont’d
After test1. Evaluate client’s neurologic status; complications involve
occlusionofcerebralarteries.2. Observeinjectionsiteforhematomaformation.3. Posttestcomplicationsincludecontinuousbleedingatinjec-
tionsite,rash,dizziness,andtinglinginanextremity.4. Checkcirculationdistaltoareaofpuncture.
Electromyography (EMG) Measureselectricaldischargefromamuscle.Flatelectrodesorsmallneedlesareplacedinthemuscle.Theclientmaybeaskedtomoveandperformsimpleactivities;theelectricalstimulusforthemusclewillberecorded.Usefulfordiag-nosis in spinal cord deformity, muscular dystrophy, myastheniagravisoramyotrophiclateralsclerosis.Nursing ImplicationsBefore test
1. Maydeterminepretestserummuscledeterminations.2. Explaintotheclientthatsmallneedleswillbeinsertedinto
theskin.After test
1. Client may need something for pain because of musclestimulation.
2. Assessneedle sites forareasofhematomas; apply icepacktopreventand/orrelieve.
Appendix 20-2 ANTIEPILEPTICS
MEDICATIONS SIDE EFFECTS NURSING IMPLICATIONSAntiepileptics (AED) Suppress discharge of neurons within a seizure focus to reduce seizure activity.
Phenobarbital(Sodium Luminal):IM,PO,rectal,IV
Drowsiness,ataxia,excitationinchildrenandtheelderly
1. Clientshouldavoidpotentialhazardousactivitiesrequiringmentalalertness.
Primidone(Mysoline):PO 2. Suddenwithdrawalfromchronicusemayprecipitatesymptoms.
3. Closelyobserveresponseinchildrenandelderly.
4. Usedtotreatgrandmalandfocalseizures.5. SeeAppendix15-5forcareofclientwith
seizures.
Phenytoin(Dilantin):PO,IV Gingivalhyperplasia,skinrash,hypoglycemia
Bradycardia,hypotensionVisualchanges:nystagmus,diplopia,
blurredvision
1. AdministerPOpreparationswithmealsormilktodecreasegastricirritation.
2. Frequentlyusedwithphenobarbitalforcontrolofgrandmalseizures.
3. IMinjectionisnotrecommended.4. Donotmixwithanyothermedications
whenadministeringIVsolution.5. Promotegoodoralhygiene;gumhyperplasia
isaproblemwithlong-termuse.6. SeeAppendix15-5forcareofclientwith
seizures.7. AEDsshouldbewithdrawnslowlyover6
weekstoseveralmonthswhenmedicationtherapyisdiscontinued.
Continued
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
432 CHAPTER 20 Neurologic System
MEDICATIONS SIDE EFFECTS NURSING IMPLICATIONSDivalproexsodium(Depakote):
POGIdisturbances,rash,weightgain,
hairloss,tremor,blooddyscrasias1. Shouldnotbegiventoclientswithsevere
liverdysfunction.GI,dermatologiceffects,blood
dyscrasias2. Potentiatesactionofphenobarbital,
phenytoin,diazepam.3. Uses:seizures,bipolardisorder,migraine.
Carbamazepine(Tegretol):PO,suspension
Drowsiness,dizziness,headache;visualdisturbancescommonduringfirstfewweeksoftreatment
1. Weanclientfrommedicationassoonasseizuresarecontrolled.
2. Antimanicpropertiesaswell.
Clonazepam(Klonopin):PO CNSdepression,ataxia 1. Antianxietyeffectsmayassistwithseizurecontrol.
2. Monitorresultsofliverfunctiontests.
CNS,Centralnervoussystem;GI,gastrointestinal;IM,intramuscular;IV,intravenous;PO,bymouth(orally).
Appendix 20-2 ANTIEPILEPTICS—cont’d
Appendix 20-3 CHOLINERGIC (ANTICHOLINESTERASE) MEDICATIONS
MEDICATIONS SIDE EFFECTS NURSING IMPLICATIONSCholinergic Medications Intensify transmission of impulses throughout the CNS, where acetylcholine is necessary for transmission.
Neostigminebromide(Prostigmin):PO,subQ,IM
Excessivesalivation,increasedGImotility,urinaryurgency,bradycardia,visualproblems
1. Primarygroupofmedicationsusedfortreatmentofmyastheniagravis.
2. Atropineistheantidoteforoverdose.3. Intreatmentofmyastheniagravis,medication
isfrequentlyadministered30to45minutesbeforemeals.
4. Mestinonisgivenasmaintenancetherapyfortheclientwithmyastheniagravis.
5. Tensilonisusedfordiagnosticpurposes;notrecommendedformaintenancetherapy.
6. Teachclientsymptomsofsideeffectsandadviseclienttocallthedoctoriftheyarepresent.
Pyridostigminebromide(Mestinon):PO,IM,IV
Edrophoniumchloride(Tensilon):IV,IM
CNS,Centralnervoussystem;GI,gastrointestinal;IM,intramuscular;IV,intravenous;PO,bymouth(orally);subQ,subcutaneous.
Appendix 20-4 ANTIPARKINSONISM AGENTS
MEDICATIONS SIDE EFFECTS NURSING IMPLICATIONSAnticholinergics Inhibit action of acetylcholine at sites throughout the body and CNS. Decrease synaptic transmissions in the CNS.
Benztropinemesylate(Cogentin):PO,IM,IV
Trihexyphenidylhydrochloride(Artane):PO,IM,IV
Procyclidine(Kemadrin):PO
Paralyticileus,urinaryretention,cardiacpalpitations,blurredvision,nauseaandvomiting,sedation,dizziness
Minorsideeffectssuchasdrymouth,jitteriness,andnausea
1. AdministerPOpreparationswithmealstodecreasegastricirritation.
2. Medicationshavecumulativeeffect.3. Shouldnotbeusedinclientswithglaucoma,
myastheniagravis,GUorGItractobstructionorinchildrenyoungerthan3years.
4. Monitorclientcarefullyforbowelandbladderproblems.
5. MaybeusedtotreatsideeffectsofThorazine.
L
CHAPTER 20 Neurologic System 433
Appendix 20-4 ANTIPARKINSONISM AGENTS—cont’d
MEDICATIONS SIDE EFFECTS NURSING IMPLICATIONSDopaminergics Assist to restore normal transmission of nerve impulses.
Levodopa(L-DOPA, Larodopa):PO
Early:Anorexia,nauseaandvomiting,abdominaldiscomfort,posturalhypotension
Long-term:Abnormal,involuntarymovements,especiallyinvolvingtheface,mouth,andneck;behavioraldisturbancesinvolvingconfusion,agitation,andeuphoria
1. AdministerPOpreparationswithmealstodecreaseGIdistress.
2. Almostallclientswillexperiencesomesideeffects,whicharedoserelated;dosagegraduallyincreasedaccordingtoclient’stoleranceandresponse.
3. Onsetofactionisslow;therapeuticresponsemayrequireseveralweekstomonths.
4. VitaminB6(pyridoxine)isantagonistictotheeffectsofthemedication;decreaseclient’sintakeofmultiplevitaminsandfortifiedcereals.
Carbidopa/levodopa Sameasforlevodopa 1. Sameasforlevodopa.(Sinemet):PO 2. Useofcarbidopasignificantlydecreasesthe
amountoflevodoparequiredfortherapy.3. Preventsinhibitoryeffectsoflevodopaonvitamin
B6.
Amantadinehydrochloride(Symmetrel):PO
Orthostatichypotension,dyspnea,dizziness,drowsiness,blurredvision,constipation,urinaryretention(sideeffectsaredoserelated)
1. Lesseffectivethanlevodopa;producesamorerapidclinicalresponse.
CNS,Centralnervoussystem;GI,gastrointestinal;GU,genitourinary;IM,intramuscular;IV,intravenous;PO,bymouth(orally).
A seizure disorder is the interruption of normal brain function-ing by uncontrolled paroxysmal discharge of electrical stimuli from the neurons.
Classification of SeizuresSimple Partial Seizures (remains conscious throughout seizure)Rarely last longer than 1 minute; an aura may occur before theseizure.1. Confinedtoaspecificarea(hand,arm,leg);clientmayexperi-
enceunusualsensations.2. One-sidedmovementofanextremity.3. Autonomicchanges;skinflushing,changeinheartrate,epigas-
tricdiscomfort.
Complex Partial Seizures (may have impairment of consciousness)1. Maylooseconsciousnessfor1to3minutes.2. Mayproduceautomatisms(lipsmacking,grimacing,repetitive
handmovements).3. Client may be unaware of environment and wonder what is
happeningatthebeginningoftheseizure.4. In theperiodafter theseizure,clientmayexperienceamnesia
andconfusion.5. Alsocalledtemporallobeseizuresorpsychomotor.
Appendix 20-5 SEIZURE DISORDERS
Generalized Seizures (Bilaterally Symmetric and Without Local Onset)Nowarningoraura,asclientlosesconsciousnessforafewsecondstoseveralminutes.1. Absence (petit mal): Characterized by a short period of time
whentheclientisinanalteredlevelofconsciousness.Staring,blinkingperiod(followedbyresumptionofnormalactivity)ischaracteristic.Mayoccurmorethan100timesperday;maygounnoticed;ingeneral,onsetisinchildhoodbetweentheagesof4and12years.
2. Tonic-clonic seizures: May last 2 to 5 minutes. Full recoverymay take several hours; clientmaybe confused, amnesic, andirritableduringthisrecoveryperiod.Tonic phase:Lossofconsciousnesswithstiffeningandrigidity
of muscles. Apnea and cyanosis are common during thisperiod;phasegenerallylastsforabout1minute.
Clonic phase:Hyperventilation,withrapidjerkingmovements.Tonguebiting,incontinence,andheavysalivationmayoccurduringthisperiod(Figure20-11).
Seizure EtiologyAcute Disorders• Increasedintracranialpressure,metabolicalterations• Infections, febrile episodes in children (generally between 6
monthsand3years)
Continued
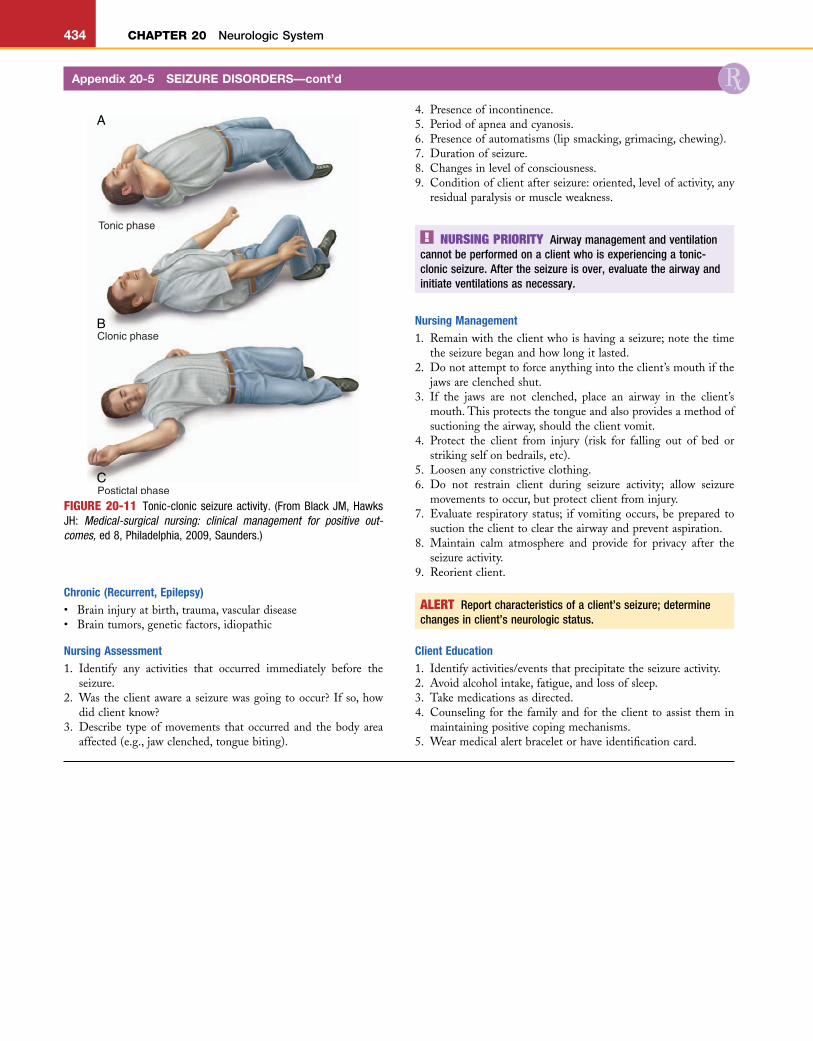
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
434 CHAPTER 20 Neurologic System
Chronic (Recurrent, Epilepsy)• Braininjuryatbirth,trauma,vasculardisease• Braintumors,geneticfactors,idiopathic
Nursing Assessment1. Identify any activities that occurred immediately before the
seizure.2. Wastheclientawareaseizurewasgoingtooccur?Ifso,how
didclientknow?3. Describe typeofmovements thatoccurred and thebody area
affected(e.g.,jawclenched,tonguebiting).
4. Presenceofincontinence.5. Periodofapneaandcyanosis.6. Presenceofautomatisms(lipsmacking,grimacing,chewing).7. Durationofseizure.8. Changesinlevelofconsciousness.9. Conditionofclientafterseizure:oriented,levelofactivity,any
residualparalysisormuscleweakness.
Appendix 20-5 SEIZURE DISORDERS—cont’d
FIGURE 20-11 Tonic-clonic seizure activity. (From Black JM, Hawks JH: Medical-surgical nursing: clinical management for positive out-comes, ed 8, Philadelphia, 2009, Saunders.)
Tonic phase
Clonic phase
Postictal phase
A
B
C
NURSING PRIORITY Airway management and ventilation cannot be performed on a client who is experiencing a tonic-clonic seizure. After the seizure is over, evaluate the airway and initiate ventilations as necessary.
Nursing Management1. Remainwiththeclientwhoishavingaseizure;notethetime
theseizurebeganandhowlongitlasted.2. Donotattempttoforceanythingintotheclient’smouthifthe
jawsareclenchedshut.3. If the jaws are not clenched, place an airway in the client’s
mouth.Thisprotectsthetongueandalsoprovidesamethodofsuctioningtheairway,shouldtheclientvomit.
4. Protect the client from injury (risk for falling out of bed orstrikingselfonbedrails,etc).
5. Loosenanyconstrictiveclothing.6. Do not restrain client during seizure activity; allow seizure
movementstooccur,butprotectclientfrominjury.7. Evaluate respiratory status; if vomitingoccurs,beprepared to
suctiontheclienttocleartheairwayandpreventaspiration.8. Maintain calm atmosphere and provide for privacy after the
seizureactivity.9. Reorientclient.
ALERT Report characteristics of a client’s seizure; determine changes in client’s neurologic status.
Client Education1. Identifyactivities/eventsthatprecipitatetheseizureactivity.2. Avoidalcoholintake,fatigue,andlossofsleep.3. Takemedicationsasdirected.4. Counseling for the familyand for theclient toassist themin
maintainingpositivecopingmechanisms.5. Wearmedicalalertbraceletorhaveidentificationcard.
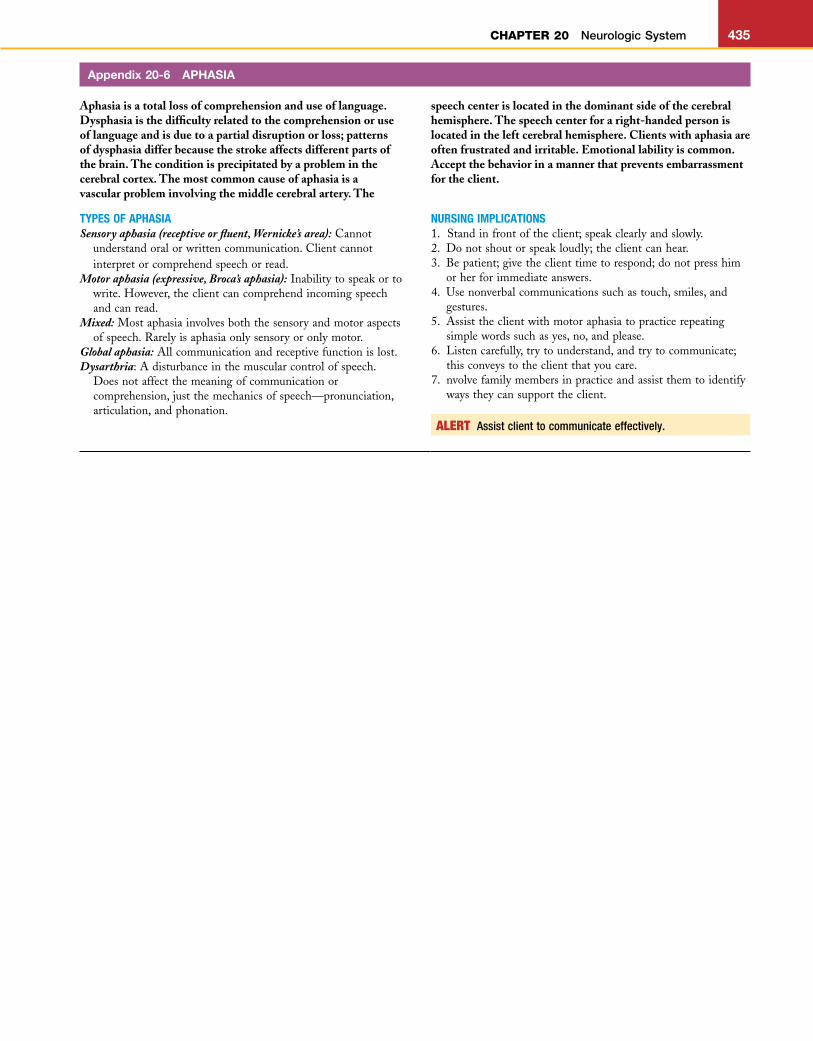
L
CHAPTER 20 Neurologic System 435
Aphasia is a total loss of comprehension and use of language. Dysphasia is the difficulty related to the comprehension or use of language and is due to a partial disruption or loss; patterns of dysphasia differ because the stroke affects different parts of the brain. The condition is precipitated by a problem in the cerebral cortex. The most common cause of aphasia is a vascular problem involving the middle cerebral artery. The
Appendix 20-6 APHASIA
speech center is located in the dominant side of the cerebral hemisphere. The speech center for a right-handed person is located in the left cerebral hemisphere. Clients with aphasia are often frustrated and irritable. Emotional lability is common. Accept the behavior in a manner that prevents embarrassment for the client.
TYPES OF APHASIA NURSING IMPLICATIONSSensory aphasia (receptive or fluent, Wernicke’s area):Cannot
understandoralorwrittencommunication.Clientcannotinterpretorcomprehendspeechorread.
Motor aphasia (expressive, Broca’s aphasia):Inabilitytospeakortowrite.However,theclientcancomprehendincomingspeechandcanread.
Mixed:Mostaphasiainvolvesboththesensoryandmotoraspectsofspeech.Rarelyisaphasiaonlysensoryoronlymotor.
Global aphasia:Allcommunicationandreceptivefunctionislost.Dysarthria:Adisturbanceinthemuscularcontrolofspeech.
Doesnotaffectthemeaningofcommunicationorcomprehension,justthemechanicsofspeech—pronunciation,articulation,andphonation.
1. Standinfrontoftheclient;speakclearlyandslowly.2. Donotshoutorspeakloudly;theclientcanhear.3. Bepatient;givetheclienttimetorespond;donotpresshim
orherforimmediateanswers.4. Usenonverbalcommunicationssuchastouch,smiles,and
gestures.5. Assisttheclientwithmotoraphasiatopracticerepeating
simplewordssuchasyes,no,andplease.6. Listencarefully,trytounderstand,andtrytocommunicate;
thisconveystotheclientthatyoucare.7. nvolvefamilymembersinpracticeandassistthemtoidentify
waystheycansupporttheclient.
ALERT Assist client to communicate effectively.
L
HHHHH5HHHHH10HHHHH15HHHHH20HHHHH25HHHHH30HHHHH35HHHHH40HHHHH45HHHHH50HHHHH55H56H57H58
436 CHAPTER 20 Neurologic System
Study Questions Neurologic System More questions on companion CD!
1. The nurse is obtaining a health history from a clientwho states he is having pain in his left arm. Whichquestionbythenursewillelicitthemostusefulresponsefromtheclient?1 “Does the pain feel like pins and needles in your
arm?”2 “Doesthepainradiatefromyournecktoyourarms?”3 “Canyoudescribethepainyouareexperiencingin
yourarm?”4 “Is the numbness in your arm intermittent or
constant?”2. Thenurseisassessingaclientwithatentativediagnosis
ofabraintumor.Whatwouldthenurseanticipatetheclient’sprimarycomplainttobe?1 Decreasedappetite2 Frequentinsomnia3 Recurrentheadaches4 Peripheraledema
3. Thenurse is caring for a clientwhohashad a right-sided stroke.Whatwouldbeappropriatenursingcareforthisclient?1 PerformingpassiveROMexercisestoaffectedside,
activeROMonunaffectedside2 Placing food on the affected side of the client’s
mouth3 Applying hot packs to the right leg to decrease
musclespasms4 Turningclientevery2hoursandmaintainingposi-
tionontherightsidefor2hours4. A client is scheduled for an electroencephalogram.
Whatwillthenurseexplaintotheclientregardingthepurposeofthistest?1 Evaluateselectricalcurrentsofskeletalmuscles2 Measuresultrasonicwavesinthebrain3 Determinessizeandlocationofbrainactivity4 Recordsbrainelectricalactivity
5. Aclientwhohashadastrokeisaphasic;ithasbeenaweek since his stroke. He is beginning to show func-tional improvement and demonstrates an ability tofollow verbal directions.What will rehabilitation nowinclude?1 Aright-legbrace2 Ambulationtraining3 Speechtraining4 Vocationalretraining
6. Thenurseiscaringforaclientwhoisdoingwellafterhiscraniotomy.Whatwillthebowelcareforthisclientinclude?1 An enema every other day to avoid the Valsalva
maneuver2 High-fiber diet and stool softeners to prevent
constipation3 Low-residue diet to decrease stool formation and
preventconstipation4 Daily checking for impaction caused by loss of
bowelinnervation
7. After a grand mal seizure, what nursing action is thehighestpriority?1 Loosenorremoveconstrictingclothingandprotect
clientfrominjuringhimselforherself.2 Maintainapatent airwayby turning the clienton
hissideandsuctioning,ifnecessary.3 Remainwiththeclientandadministeranticonvul-
santmedicationsasorderedbythephysician.4 Describeandrecordeventsbeforetheonsetofthe
seizure,duringtheseizure,andaftertheseizure.8. A client with Parkinson’s disease is experiencing
anorexia and vomiting.The client is taking levodopa.Whatwillbetheinitialnursingactivity?1 Assessclient’sfoodpreferences.2 Monitorclient’sbloodpressure.3 Holdclient’smedicationandnotifythephysician.4 Administerclient’smedicationwithfood.
9. An8-year-oldchildisadmittedafteranaccidentwherehesustainedaclosedheadinjury.Thechildisalertandorientedbutverylethargic.Thereisclearfluiddrainingfromthechild’snose.Whatisthebestnursingaction?1 Gentlysuctionthefluidfromthenasalarea.2 Turnfromsidetosideonly.3 Keepheadofbedelevated.4 Encourageparticipationingamestoplayinbed.
10. When obtaining a health history, the nurse expects aclientwitharecentdiagnosisofParkinson’sdiseasetoreportwhichsignorsymptom?1 Weightloss2 Slownessofmovement3 Continualmotortremors4 Depression
11. Whilecaring foraclientwhohas recentlybeendiag-nosedwithParkinson’sdisease,thenurseshouldunder-standthat:1 Intellectualcapabilitieswilldecrease.2 Diversionalinterestsmaydecrease.3 Moodfluctuationsmayoccur.4 Communicationskillsmayfluctuate.
12. Pneumonia is a common problem in children withspastic cerebral palsy.Thenurseunderstands that thisoccursbecause:1 Thereisanassociateddysfunctionoftherespiratory
centerinthecentralnervoussystem.2 Theimmunologicsystemisimmatureanddoesnot
produceadequateantibodiestofightinfection.3 Decreased mobility leads to stasis of secretions in
therespiratorypassages.4 There is aweaknessof the voluntarymuscles that
controlrespiration.
Answers and rationales to these questions are in the section at the end of the book titled Chapter Study Questions: Answers and Rationales.