Neurologic examination
76
HI! I AM BAYMAX. YOUR PERSONAL HEALTH CARE PROVIDER
-
Upload
kristine-faith-tablizo -
Category
Health & Medicine
-
view
100 -
download
2
Transcript of Neurologic examination
HI! I AM BAYMAX. YOUR PERSONAL HEALTH CARE PROVIDER
NEUROLOGIC EXAMINATION
(INCLUDING MSE, LOC’S)KRISTINE FAITH P. TABLIZO, RN
PRC LICENSE 0576117
IN DOING PE:Prepare equipment/materials ahead.Universal precaution.Establish rapport.Explain the procedure.Ensure privacy and comfort.Comprehensive, ergonomic PE.Explain result/findings.
THE HEALTH HISTORYCommon or Concerning Symptoms Headache Dizziness or vertigo Generalized, proximal, or distal weakness Numbness, abnormal or loss of sensations Loss of consciousness, syncope, or near-syncope Seizures Tremors or involuntary movements
STROKE ATTACK WARNING SIGNS, AHA/ASASudden numbness or weakness of the face, arm, or leg
Sudden confusion, trouble speaking or understanding
Sudden trouble seeing in one or both eyesSudden trouble walking, dizziness, or loss of balance or coordination
Sudden severe headache
Facial drooping: A section of the face, usually only on one side, that is drooping and hard to move
Arm weakness: The inability to raise one's arm fullySpeech difficulties: An inability or difficulty to understand or produce speech
Time: Time is of the essence when having a stroke, and an immediate call to emergency services or trip to the hospital is recommended.[
GUIDELINES FOR NEUROLOGIC EXAMINATION (AAN)
Ms. CM, Sexing-sexy, Rawr.
Mental Status—level of alertness, appropriateness of responses, orientation to date and place
Cranial NervesMotor System-strength, coordination (cerebellar*)
Sensory SystemReflexes-hypo, hyper *with gradings
MENTAL STATUS
EXAMINATION
MSE Appearance and behavior
LOC Posture and Motor behavior Dress, grooming, hygiene Facial Expression Manner, affect
Speech and language Quantity, Rate, Volume, Articulation, Fluency
Mood
Thoughts and perceptions
Cognition, including memory, attention,
information and vocabulary, calculations, abstract thinking, and constructional ability -higher cortical fx
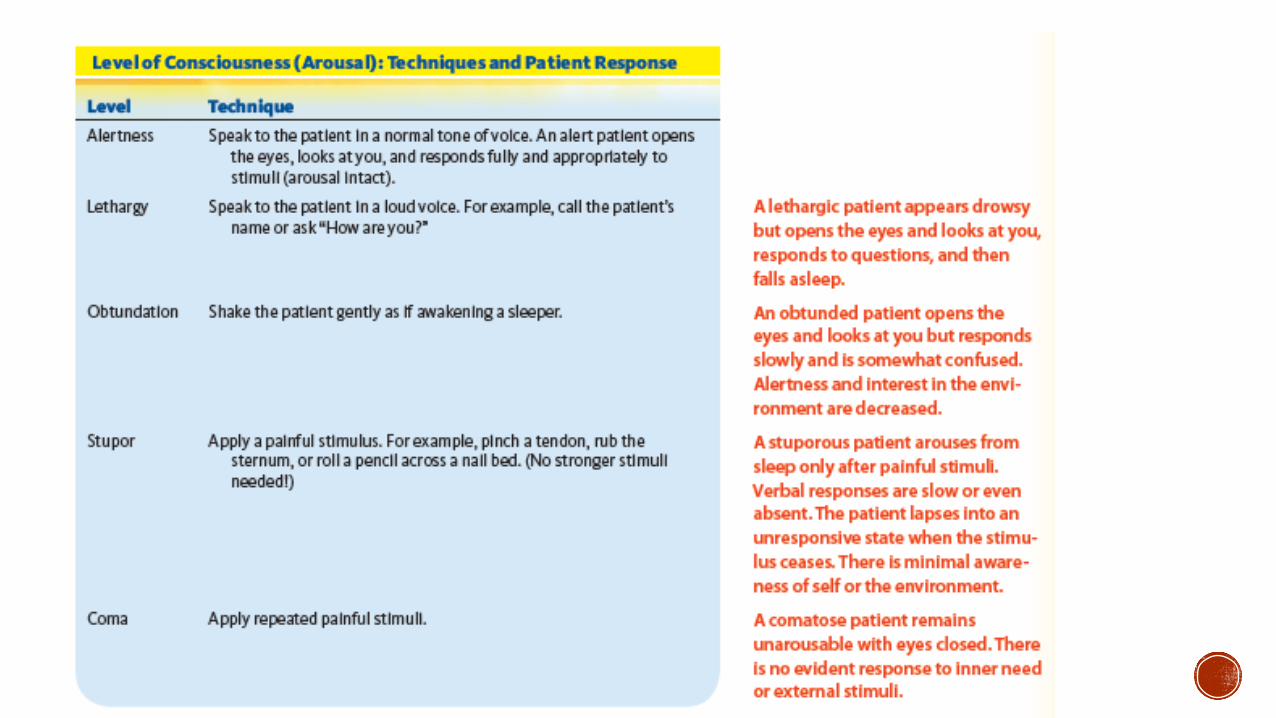
LOCpatient’s capacity for arousal, or wakefulness. determined by the level of activity that the patient can be aroused to perform in response to escalating stimuli from the examiner.
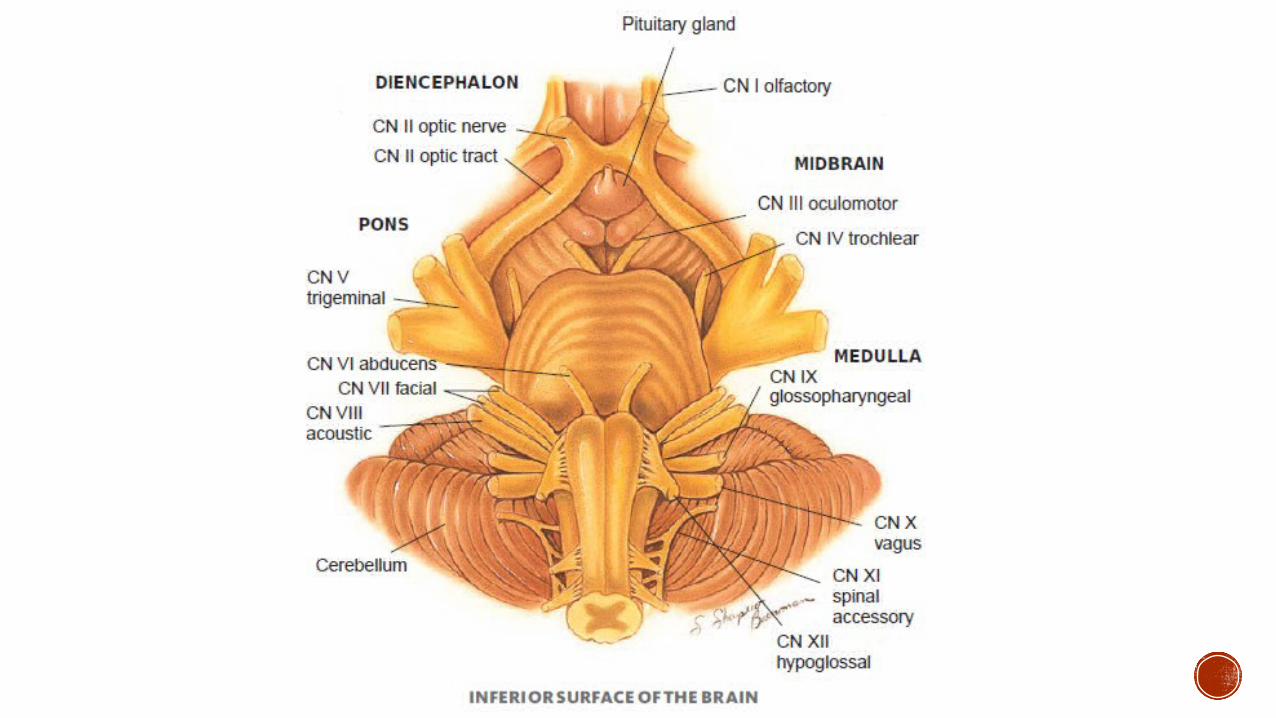
CRANIAL NERVES
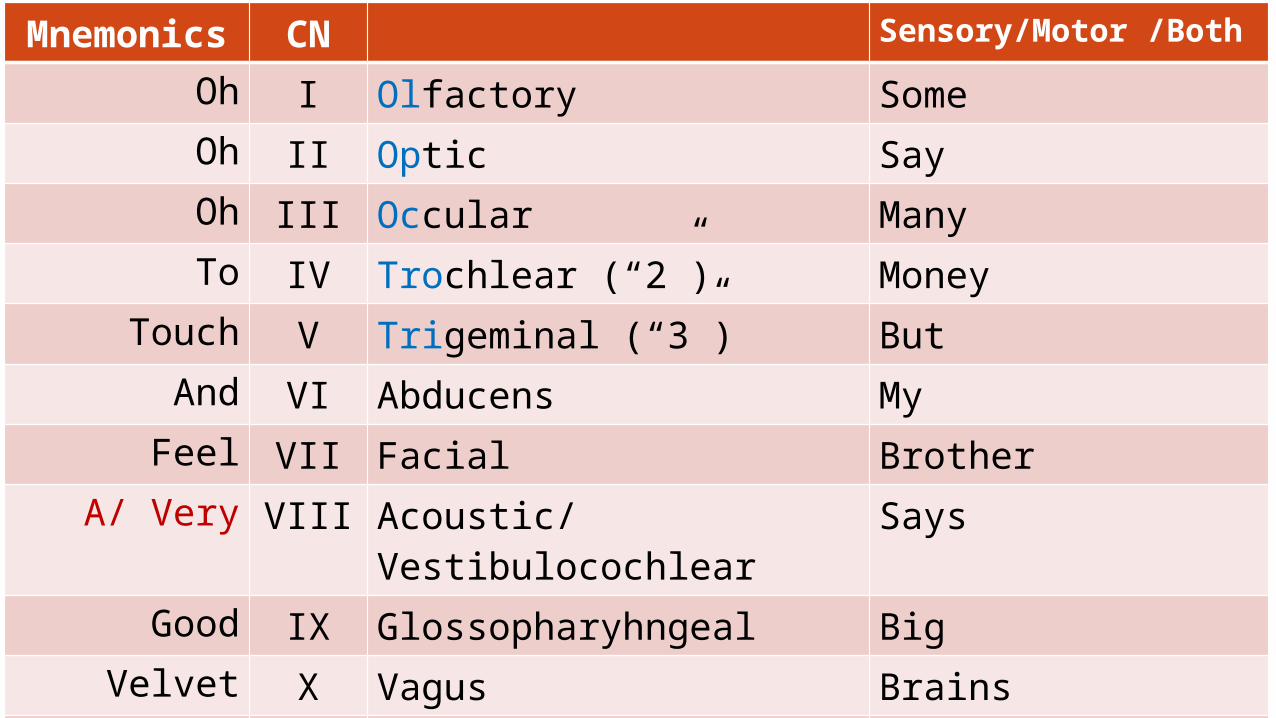
Mnemonics
CN Sensory/Motor /Both
Oh I Olfactory Some Oh II Optic Say Oh III Occular ManyTo IV Trochlear (“2”) Money
Touch V Trigeminal (“3”) ButAnd VI Abducens MyFeel VII Facial Brother
A/ Very VIII Acoustic/Vestibulocochlear
Says
Good IX Glossopharyhngeal BigVelvet X Vagus Brains
So XI Spinal Accessory MatterHeavenly XII Hypoglossal Most
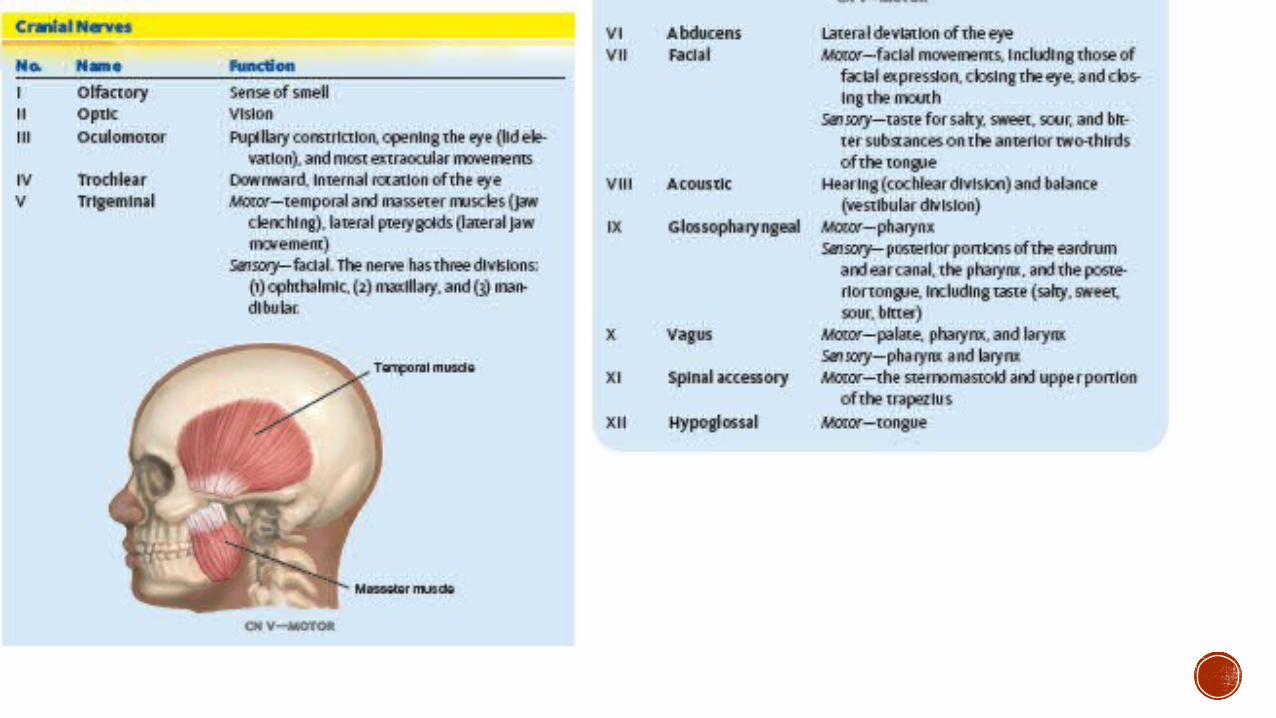
CN I- OLFACTORYSense of smell
** Loss of smell occurs in sinus conditions ,head trauma, smoking, aging, and the use of cocaine and in Parkinson disease.
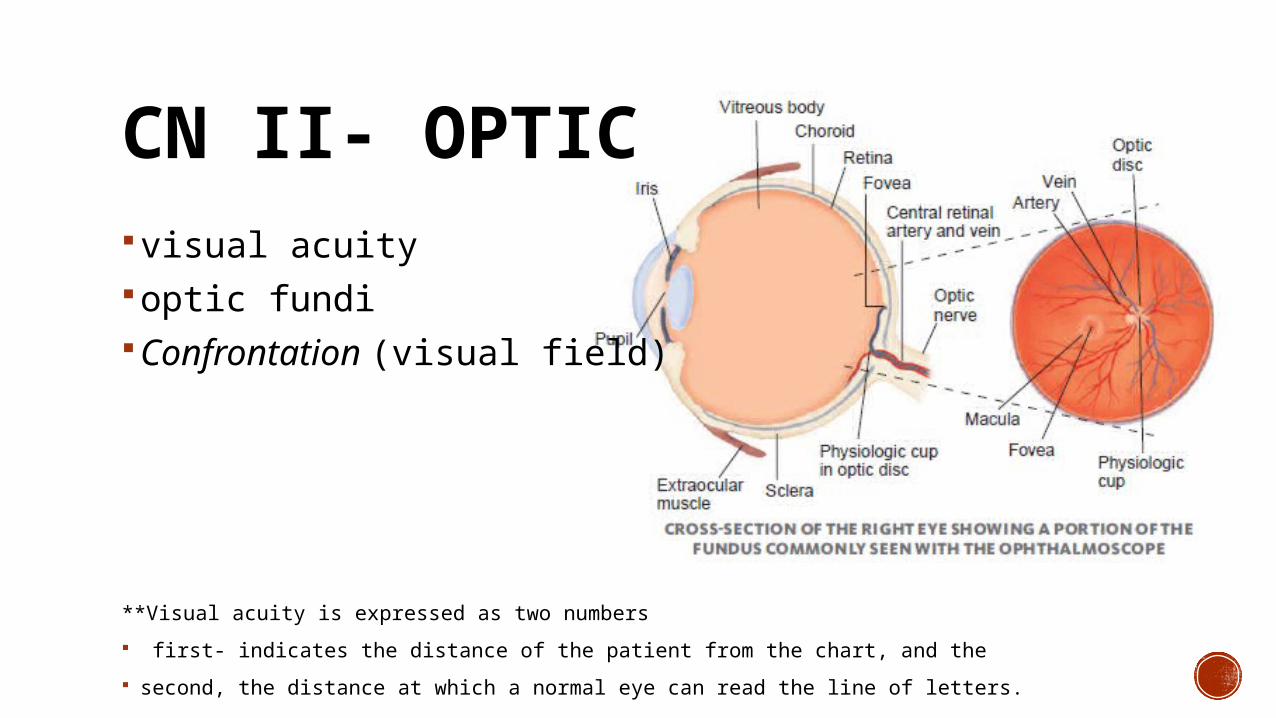
CN II- OPTICvisual acuityoptic fundiConfrontation (visual field)
**Visual acuity is expressed as two numbers
first- indicates the distance of the patient from the chart, and the
second, the distance at which a normal eye can read the line of letters.

CN II AND III
PERRLA
Near responseConvergence
Eyelid elevation
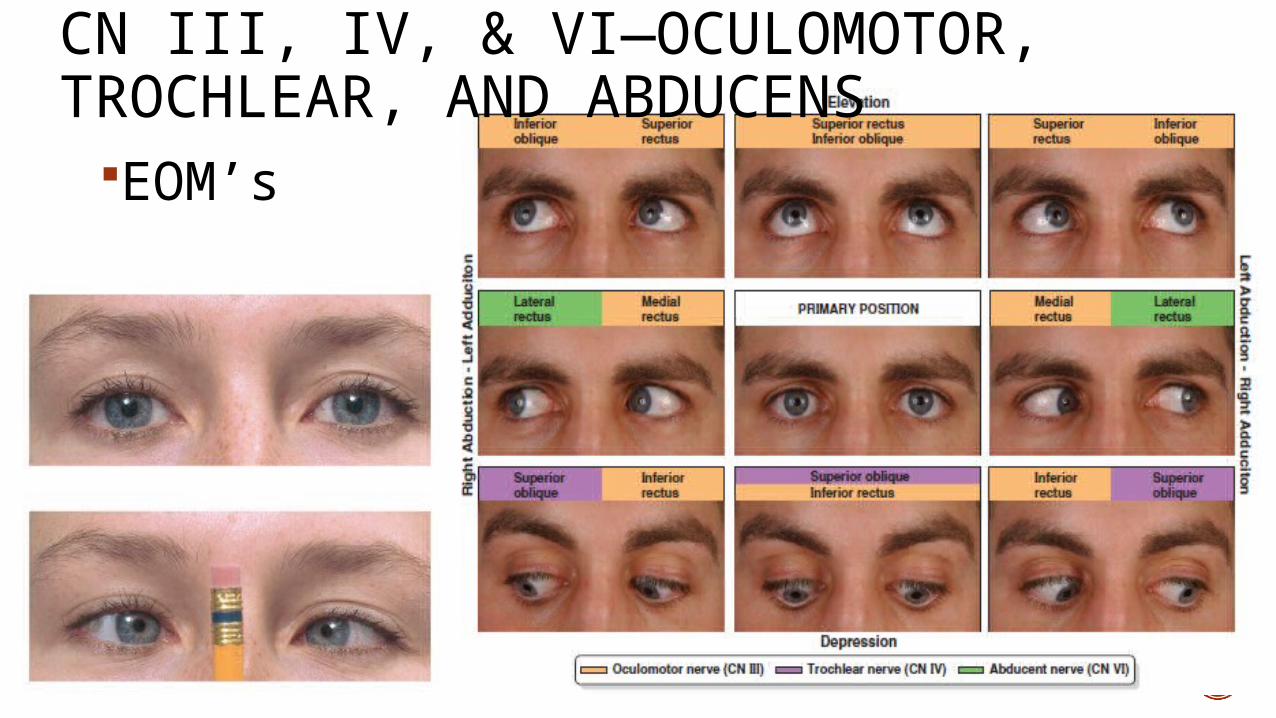
CN III, IV, & VI—OCULOMOTOR, TROCHLEAR, AND ABDUCENS
EOM’s
CN III Oculomotor Pupillary constriction, opening the eye (lid elevation), and most extraocular movements
CN IV Trochlear Downward, internal rotation of the eye
CN VI Abducens Lateral deviation of the eye
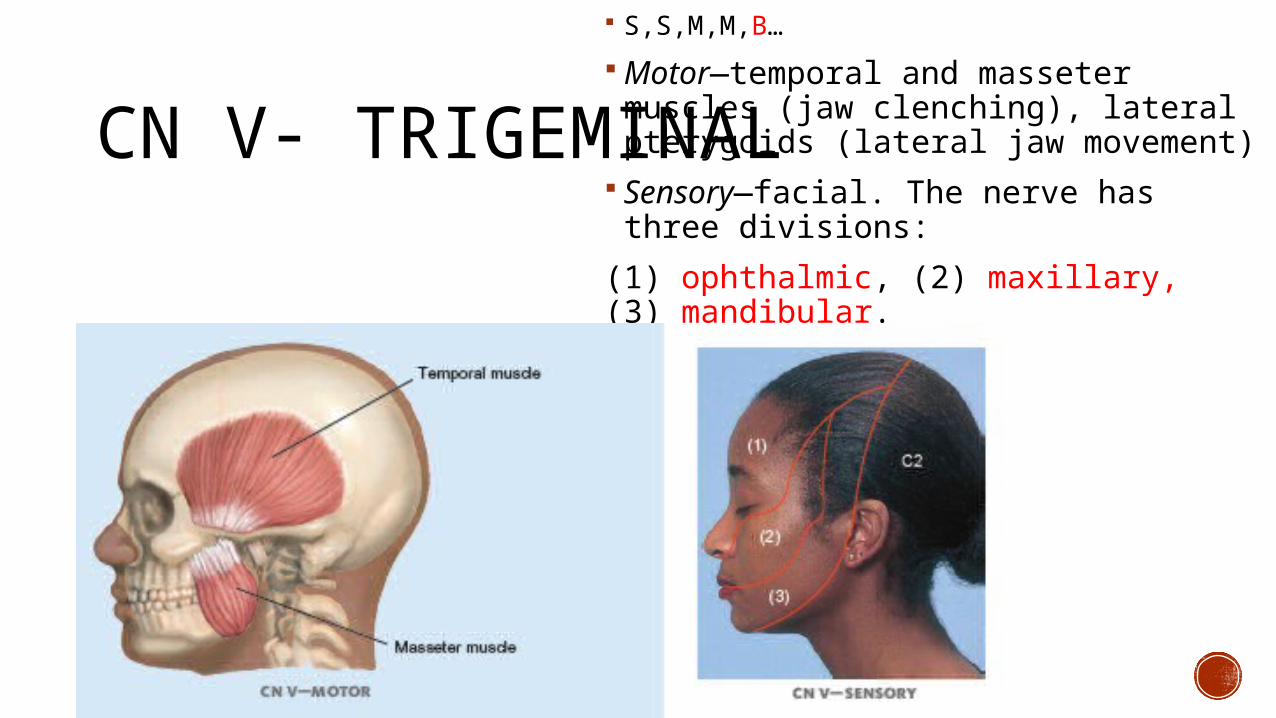
CN V- TRIGEMINAL
S,S,M,M,B…
Motor—temporal and masseter muscles (jaw clenching), lateral pterygoids (lateral jaw movement)
Sensory—facial. The nerve has three divisions:
(1) ophthalmic, (2) maxillary, (3) mandibular.
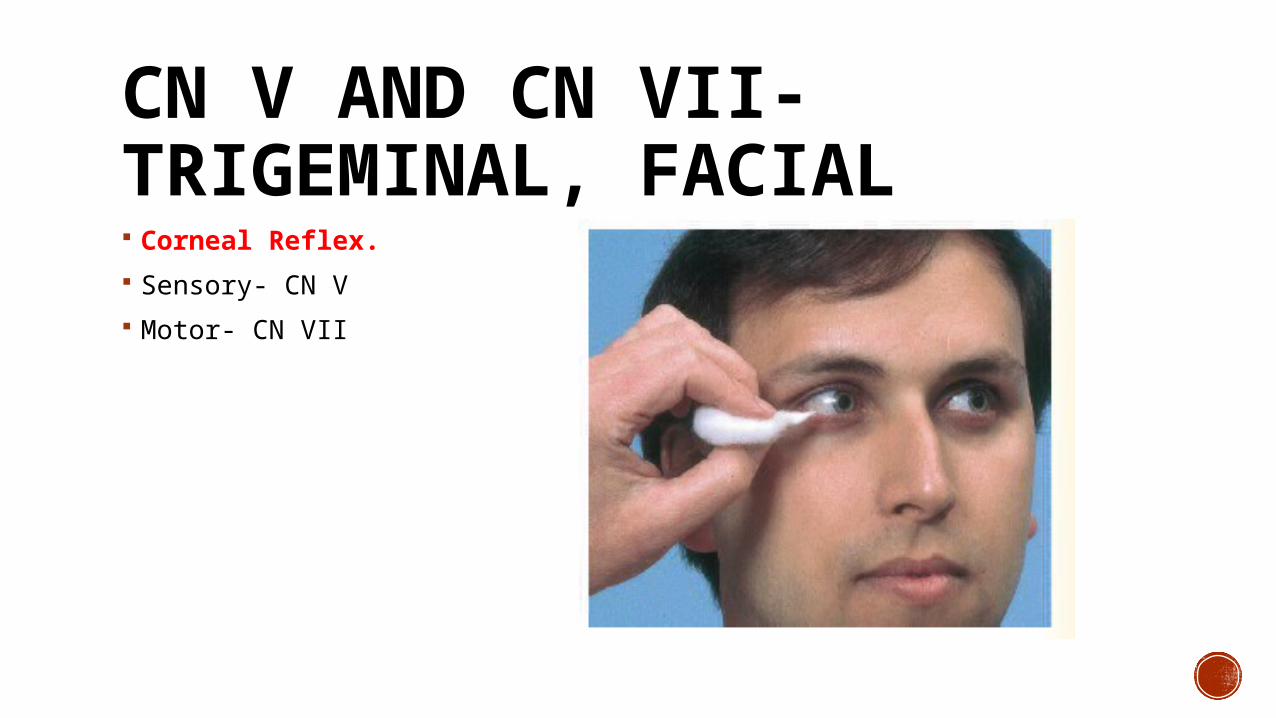
CN V AND CN VII- TRIGEMINAL, FACIAL Corneal Reflex.
Sensory- CN V
Motor- CN VII
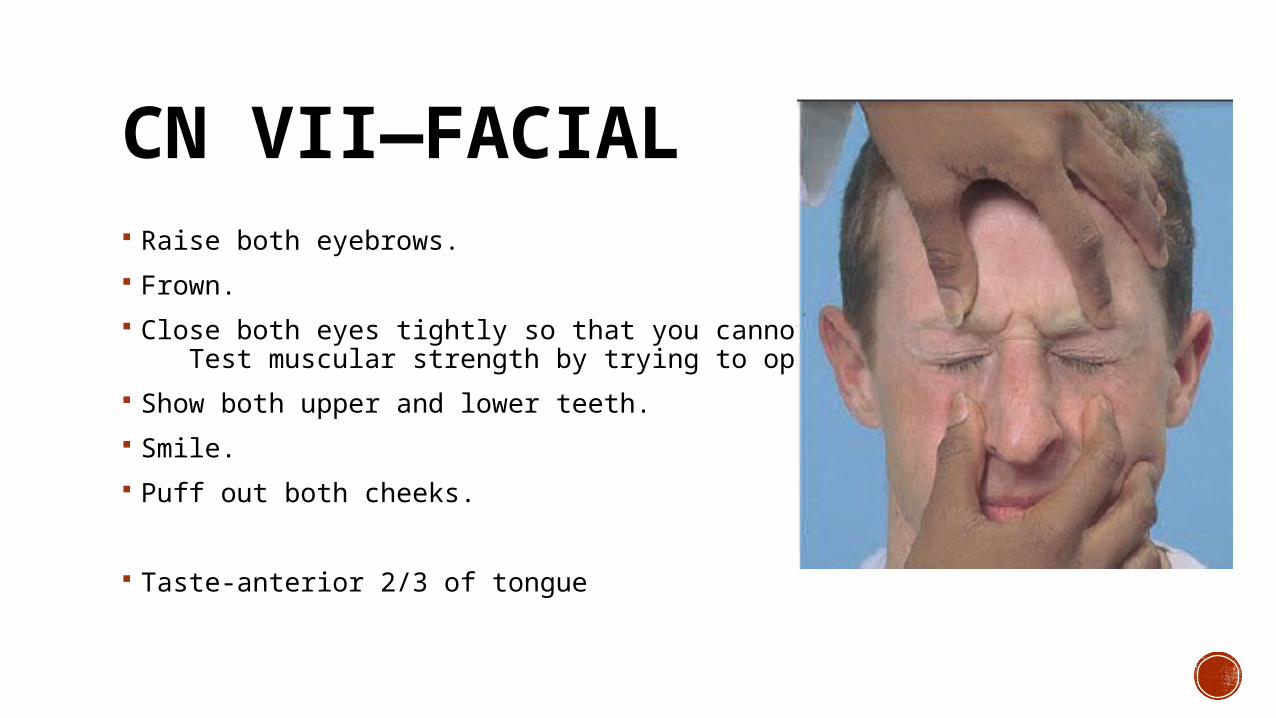
CN VII—FACIAL Raise both eyebrows.
Frown.
Close both eyes tightly so that you cannot open them. Test muscular strength by trying to open them.
Show both upper and lower teeth.
Smile.
Puff out both cheeks.
Taste-anterior 2/3 of tongue
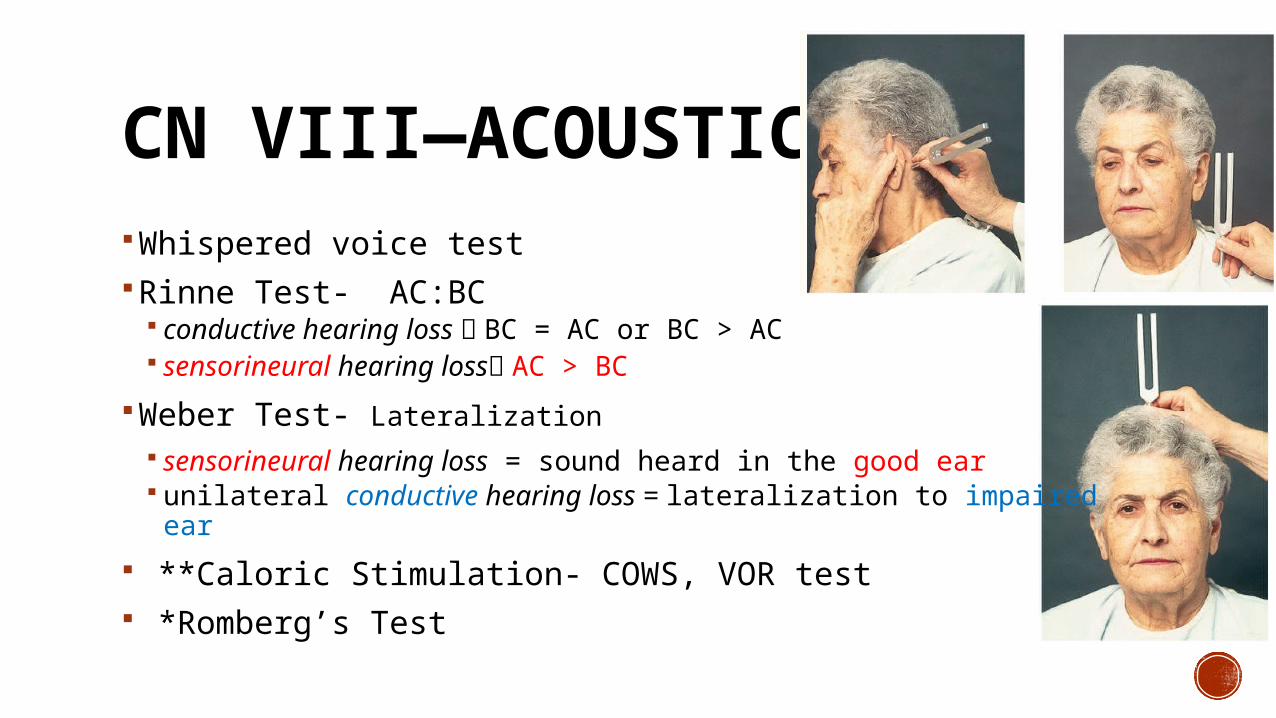
CN VIII—ACOUSTIC/VCWhispered voice testRinne Test- AC:BC
conductive hearing loss BC = AC or BC > AC sensorineural hearing loss AC > BC
Weber Test- Lateralization sensorineural hearing loss = sound heard in the good ear unilateral conductive hearing loss = lateralization to impaired ear
**Caloric Stimulation- COWS, VOR test *Romberg’s Test
CN IX- GLOSSOPHARYNGEAL
Gag reflexTaste- posterior 1/3
CN IX AND X—GL. AND VAGUS Voice? Dysphagia? Say “aaaahhh” Gag reflex
*The palate fails to rise with a bilateral lesion of CN X. In unilateral paralysis, one side of the palate fails to rise and, together with the uvula, is pulled toward the normal side.
CN XI—SPINAL ACCESSORY Observe Trapezius muscle
* Trapezius muscle paralysis, the shoulder droops, and the scapula is displaced downward and laterally.
Sternocleidomastoid
Trapezius weakness with atrophy and fasciculations- peripheral nerve disorder.
A supine patient with bilateral weakness of the sternomastoids has difficulty raising the head off the pillow.
CN XII- HYPOGLOSSAL articulation of words- CN V, VII, and X, as well as XII Tongue- atrophy or fasciculations (relaxed)
asymmetry, atrophy, or deviation from the midline (protruded) move from side to side- note the symmetry of the movement push against the inside of each cheek in turn as you palpate for strength
**Tongue atrophy and fasciculations-ALS; polio **unilateral cortical lesion-protruded tongue deviates transiently away from the side of the cortical lesion, toward the side of weakness.
MOTOR SYSTEM
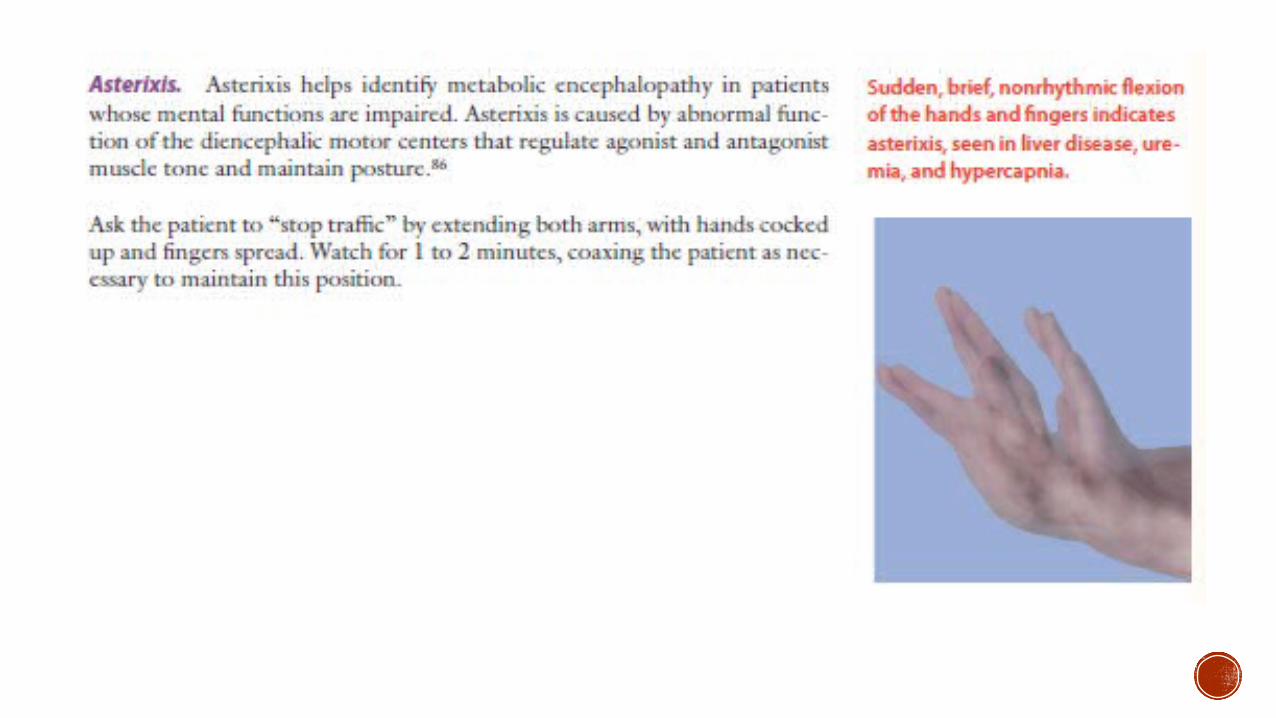
MOTOR SYSTEM FOCUS: body position -during movement and at rest. involuntary movements- tremors, tics, or fasciculations.
Note location, quality, rate, rhythm, and amplitude and relation to posture, activity, fatigue, emotion, and other factors.
characteristics of the muscles (bulk, tone, and strength) coordination
If you see an abnormality, identify the muscle(s) involved.
Determine whether the abnormality is central or peripheral in origin, and begin to learn which nerves innervate the affected muscles.
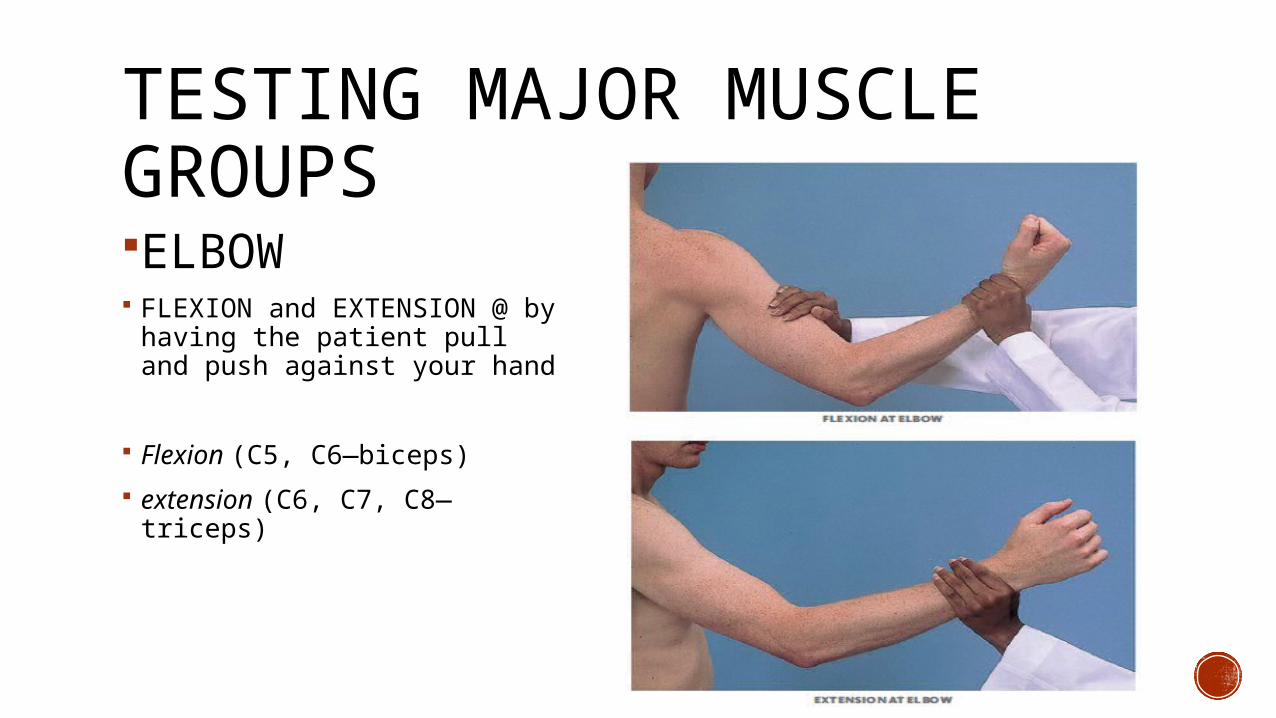
TESTING MAJOR MUSCLE GROUPSELBOW FLEXION and EXTENSION @ by
having the patient pull and push against your hand
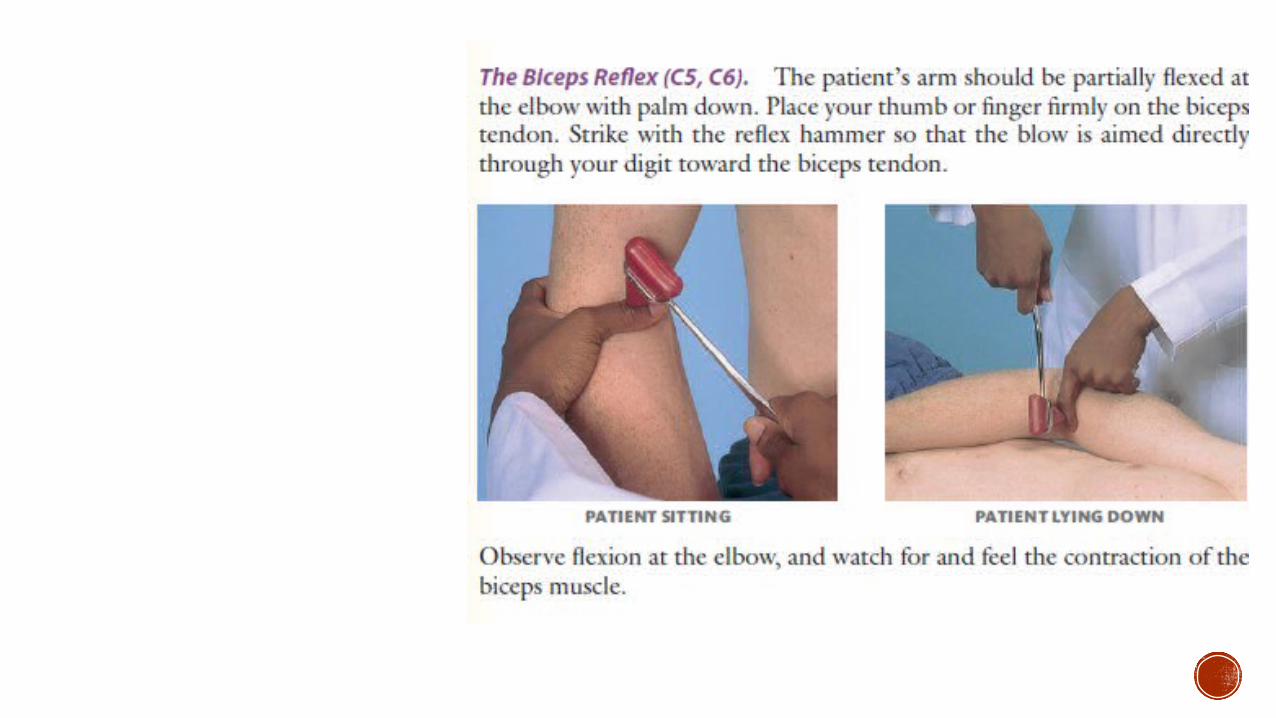
Flexion (C5, C6—biceps)
extension (C6, C7, C8—triceps)
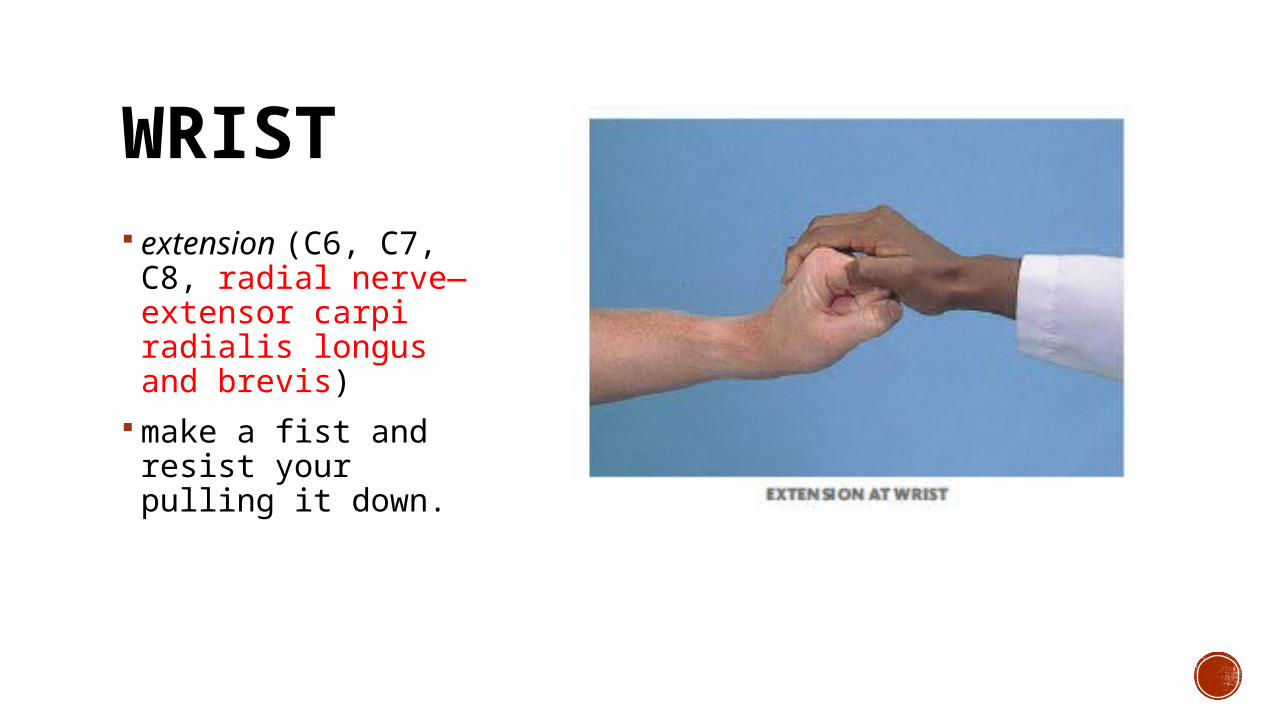
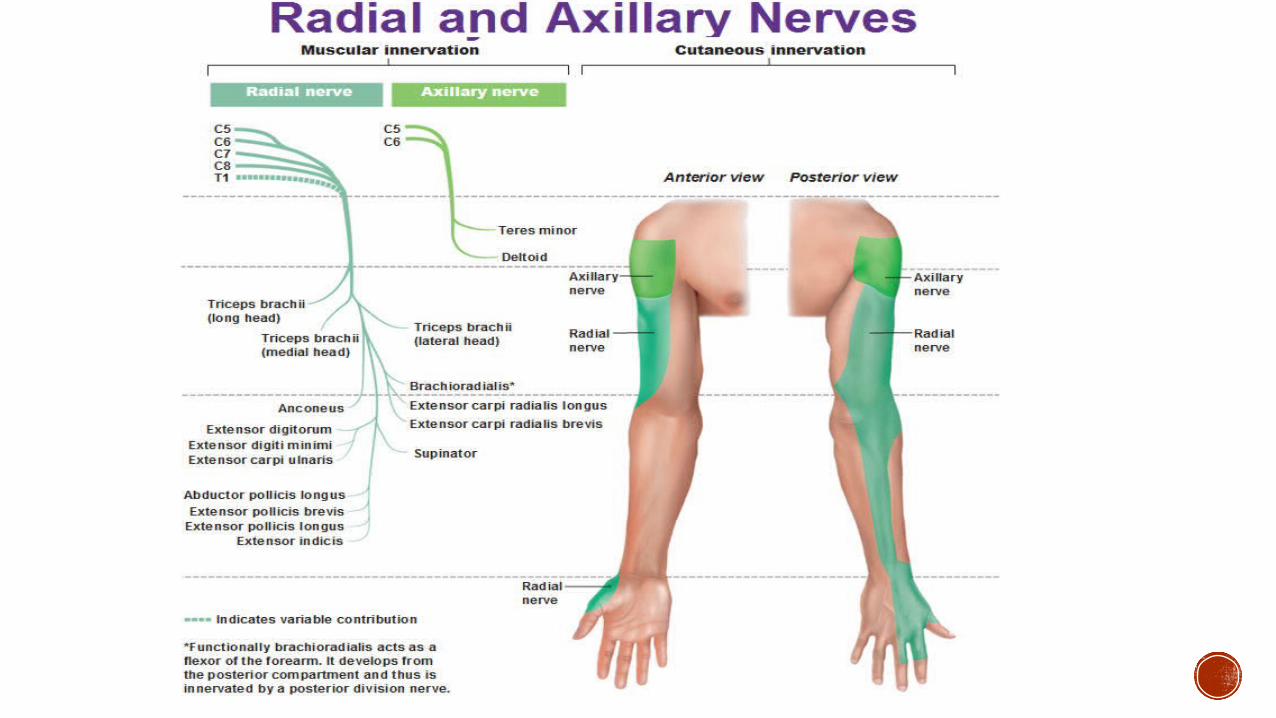
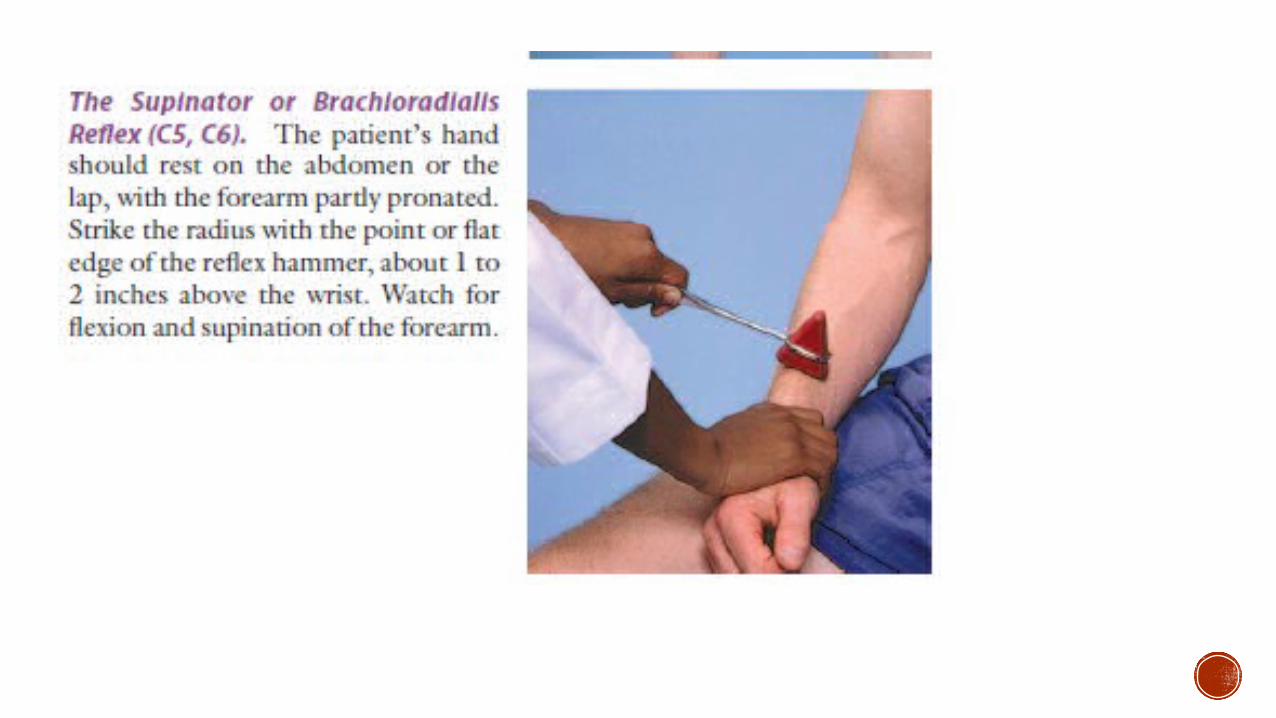
WRIST extension (C6, C7, C8, radial nerve—extensor carpi radialis longus and brevis)
make a fist and resist your pulling it down.
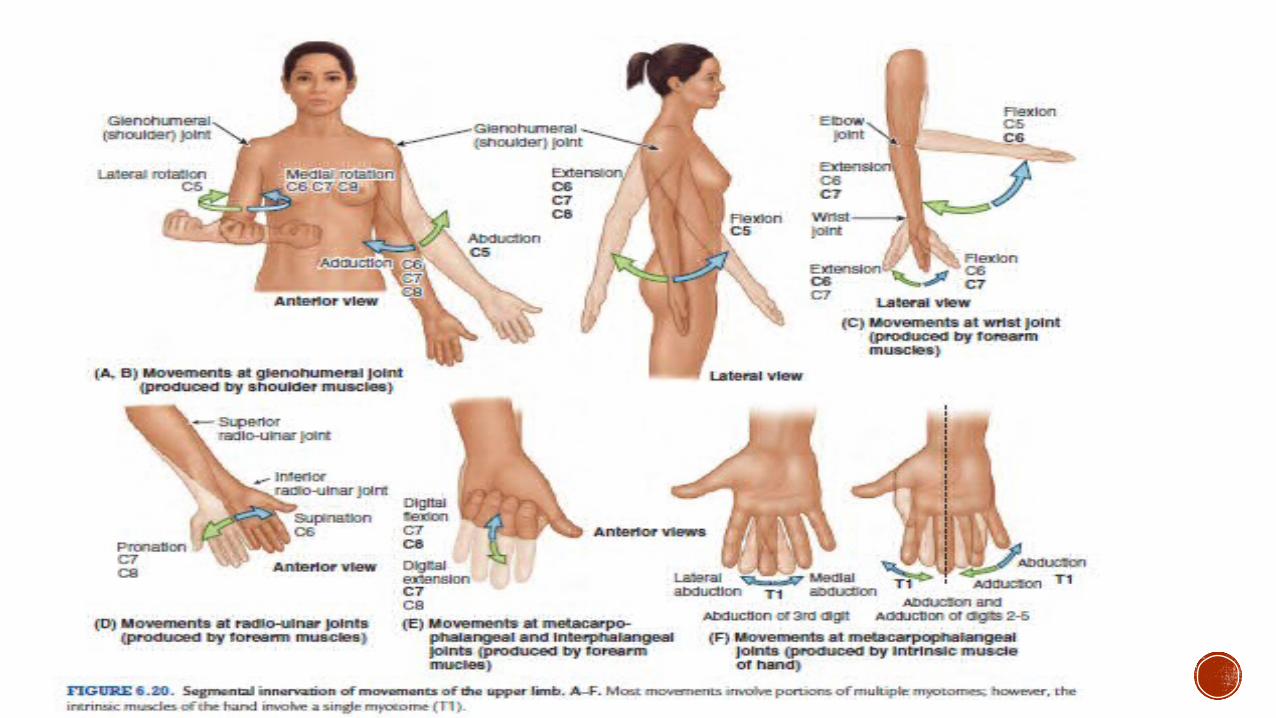
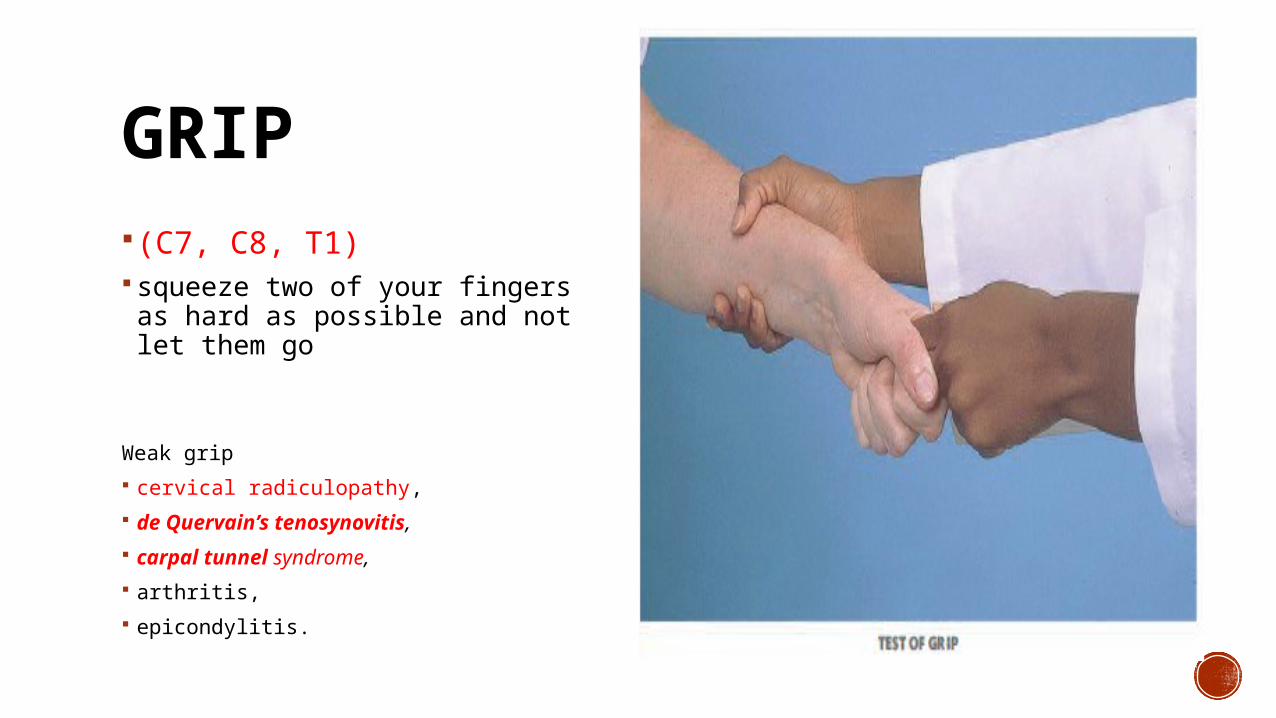
GRIP (C7, C8, T1) squeeze two of your fingers as
hard as possible and not let them go
Weak grip
cervical radiculopathy,
de Quervain’s tenosynovitis,
carpal tunnel syndrome,
arthritis,
epicondylitis.
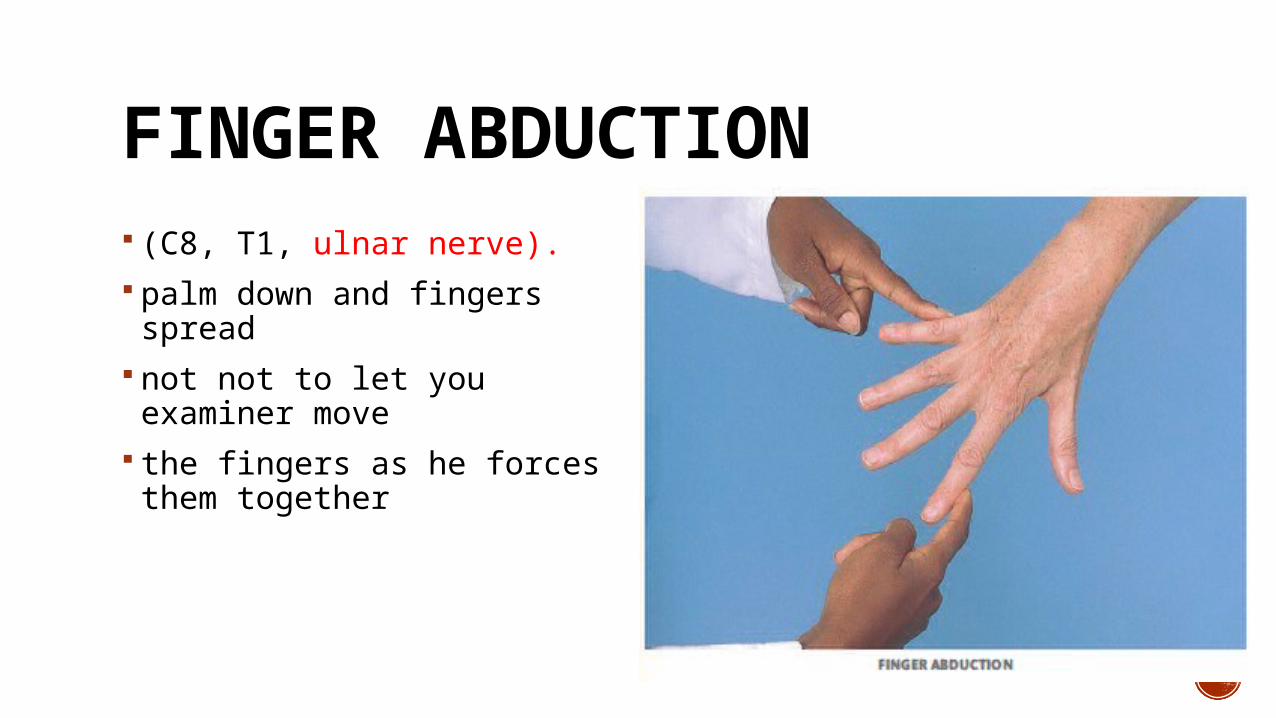
FINGER ABDUCTION (C8, T1, ulnar nerve). palm down and fingers spread
not not to let you examiner move
the fingers as he forces them together
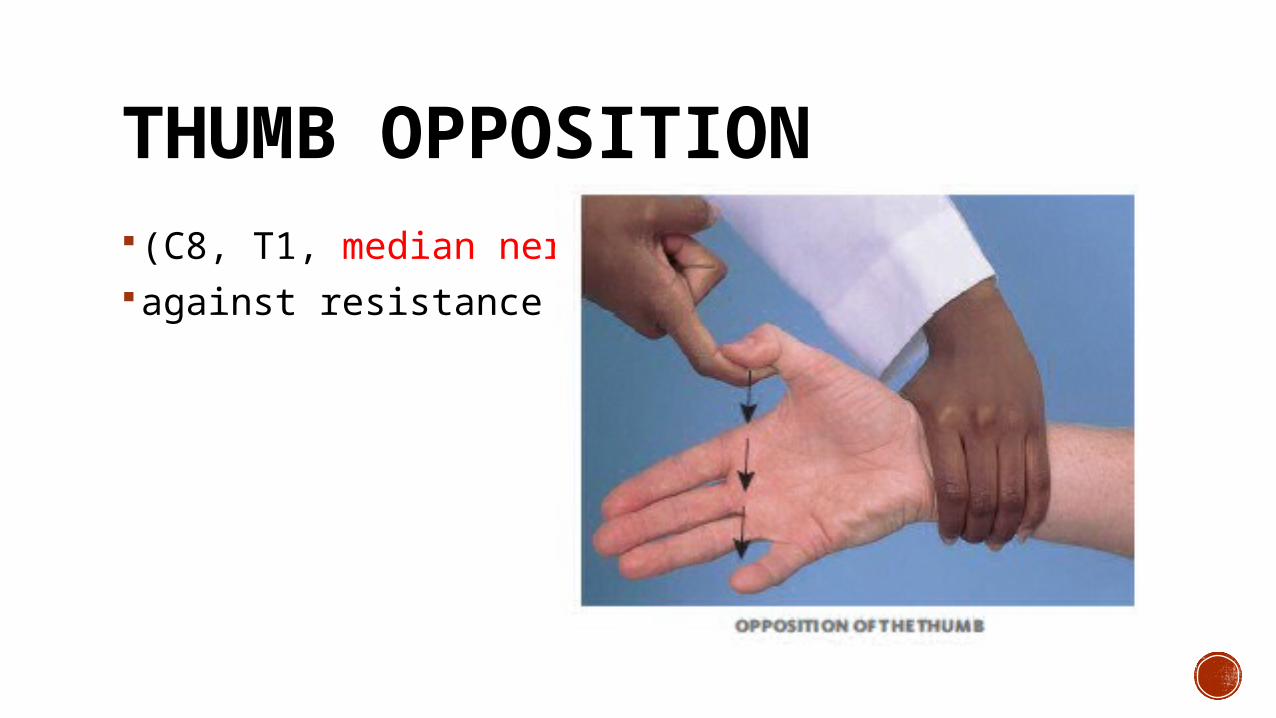
THUMB OPPOSITION (C8, T1, median nerve)against resistance
TRUNK Strength, tremors, movement
Flexion, extension, and lateral bending of the spine, and
Thoracic expansion and diaphragmatic excursion during respiration.
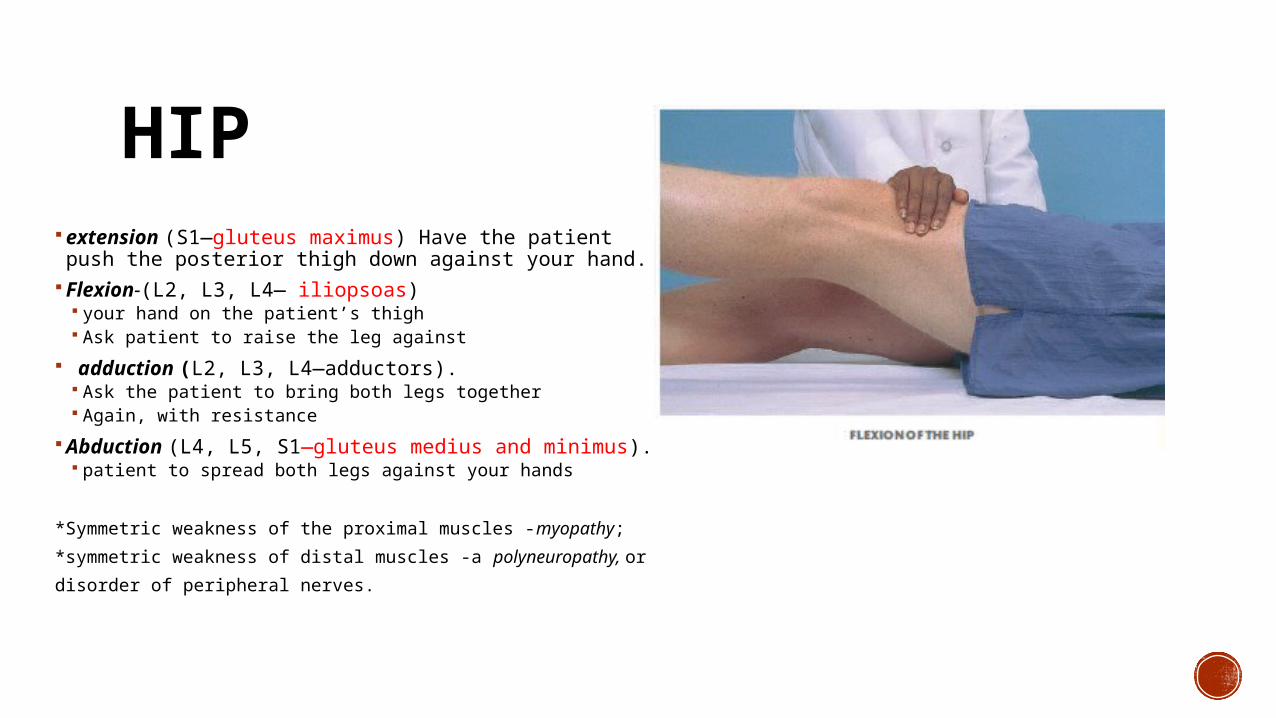
HIP extension (S1—gluteus maximus) Have the patient
push the posterior thigh down against your hand. Flexion-(L2, L3, L4— iliopsoas)
your hand on the patient’s thigh Ask patient to raise the leg against
adduction (L2, L3, L4—adductors). Ask the patient to bring both legs together Again, with resistance
Abduction (L4, L5, S1—gluteus medius and minimus). patient to spread both legs against your hands
*Symmetric weakness of the proximal muscles -myopathy;
*symmetric weakness of distal muscles -a polyneuropathy, or
disorder of peripheral nerves.
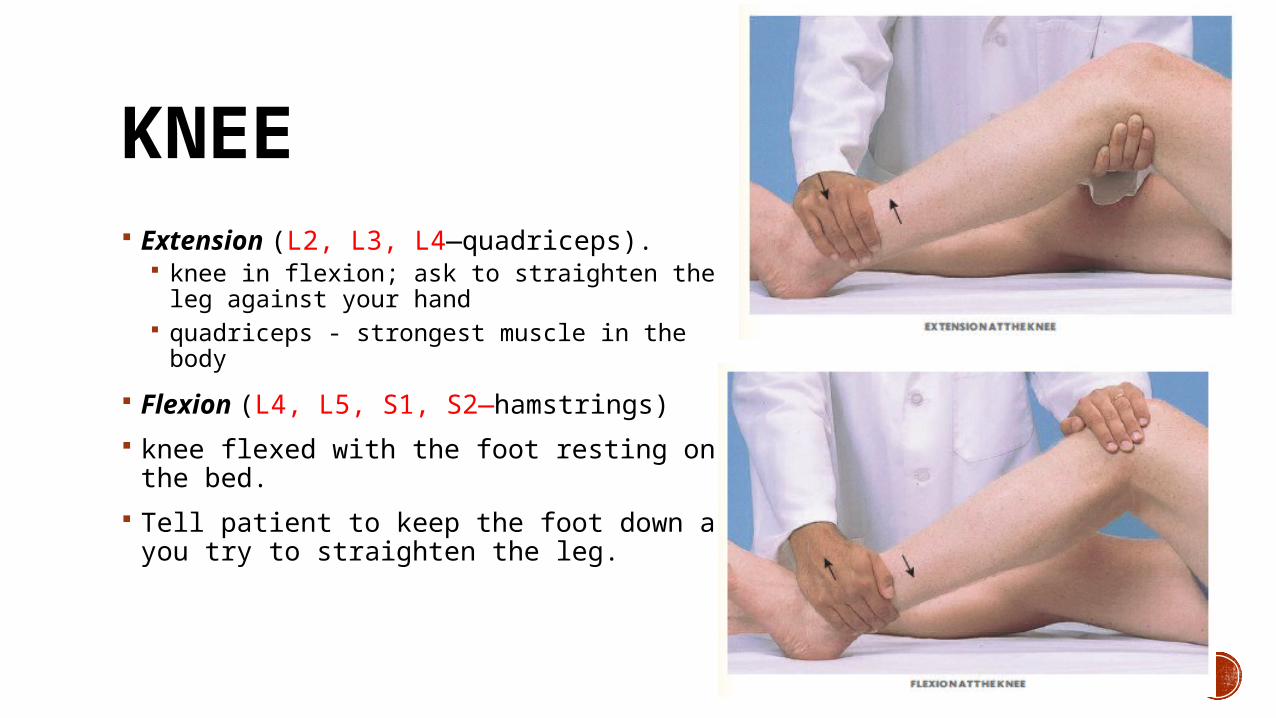
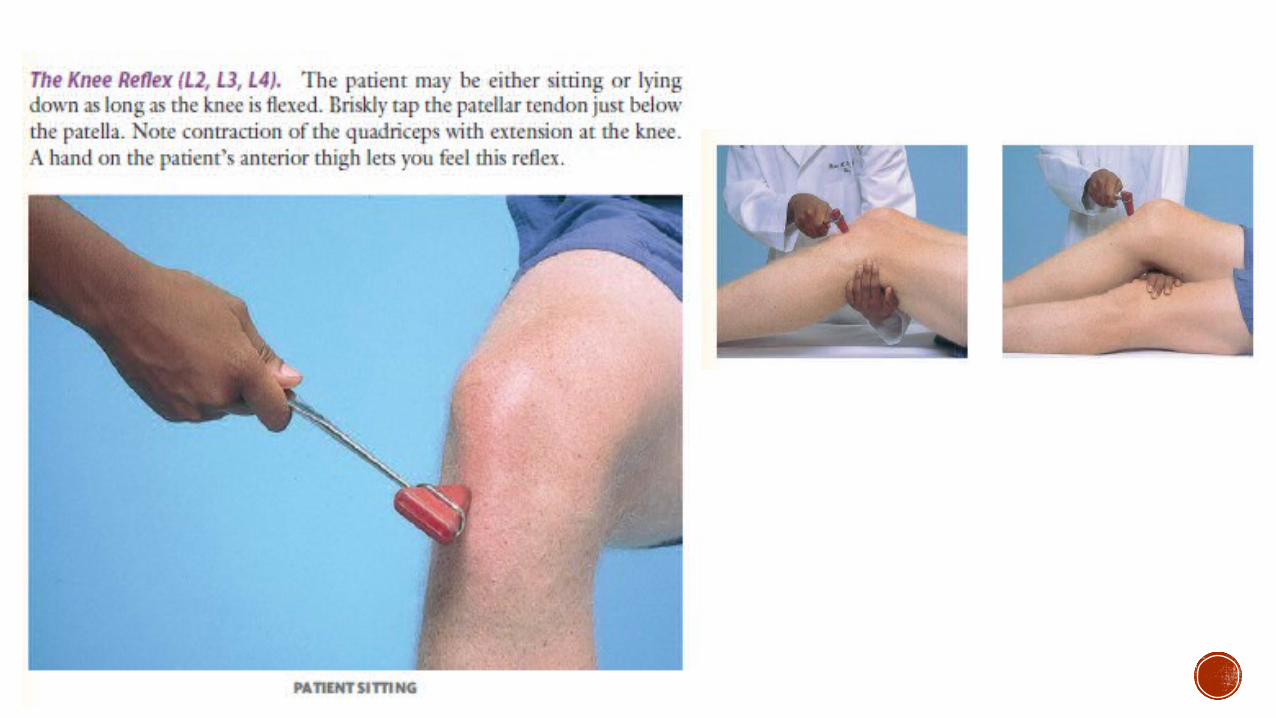
KNEE Extension (L2, L3, L4—quadriceps).
knee in flexion; ask to straighten the leg against your hand
quadriceps - strongest muscle in the body
Flexion (L4, L5, S1, S2—hamstrings)
knee flexed with the foot resting on the bed.
Tell patient to keep the foot down as you try to straighten the leg.
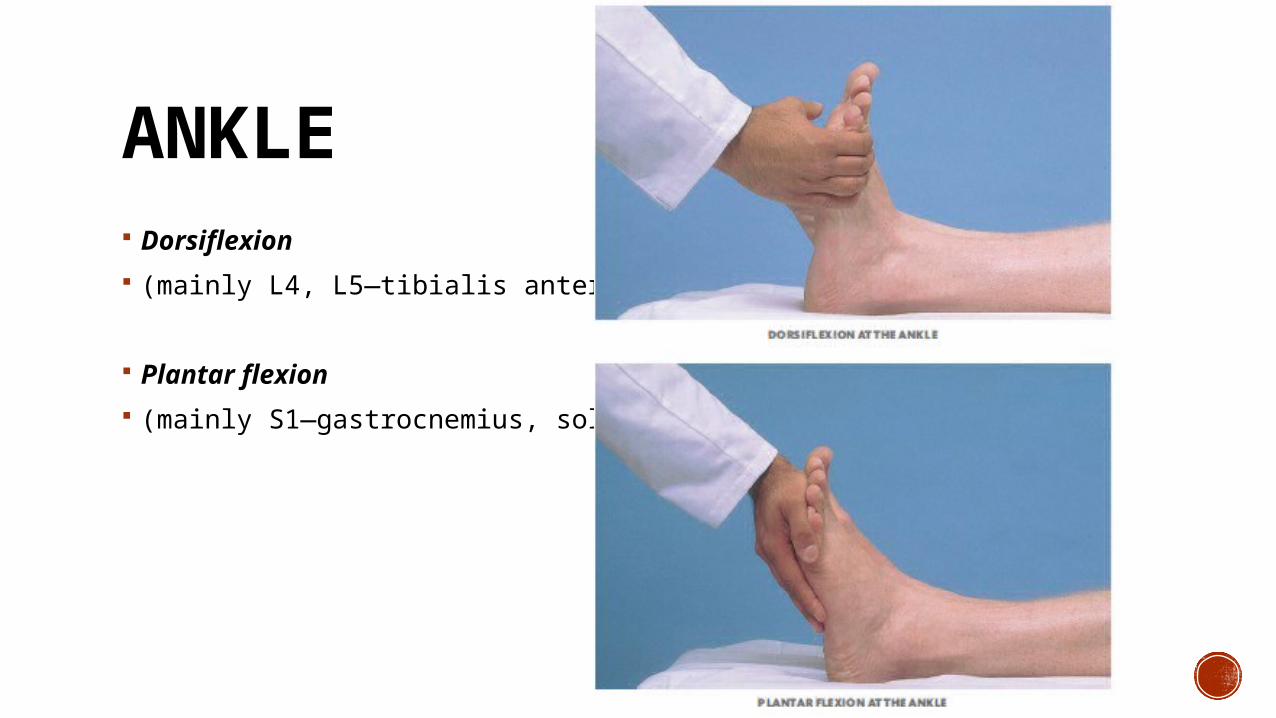
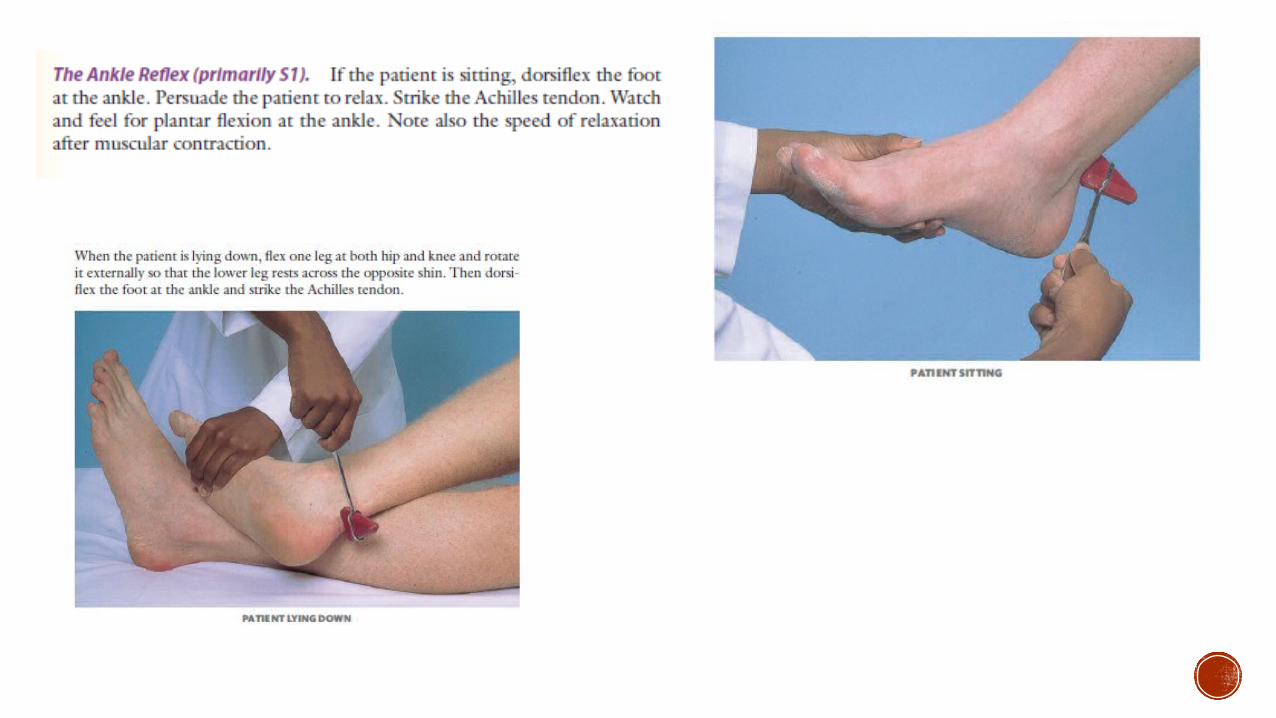
ANKLE Dorsiflexion
(mainly L4, L5—tibialis anterior)
Plantar flexion
(mainly S1—gastrocnemius, soleus)
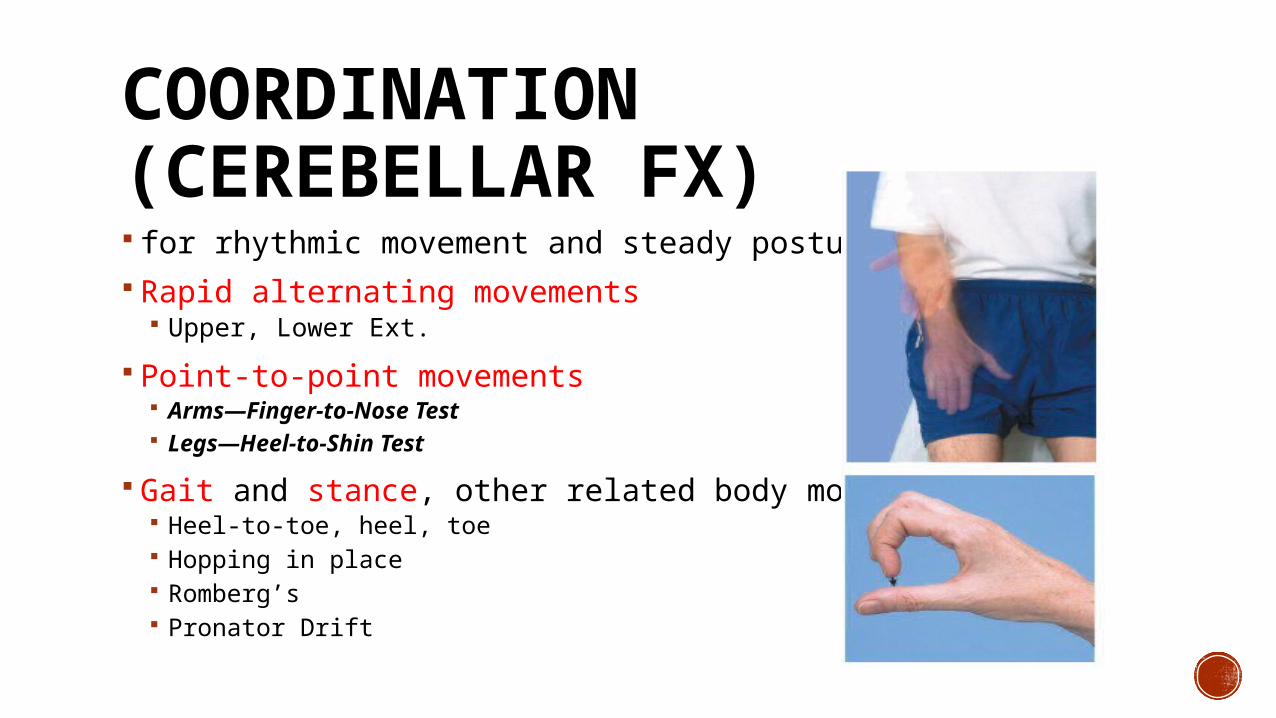
COORDINATION (CEREBELLAR FX) for rhythmic movement and steady posture Rapid alternating movements
Upper, Lower Ext.
Point-to-point movements Arms—Finger-to-Nose Test Legs—Heel-to-Shin Test
Gait and stance, other related body movements Heel-to-toe, heel, toe Hopping in place Romberg’s Pronator Drift

DYSDIACHOKINESIS In cerebellar disease one movement cannot be followed quickly by its opposite and movements are slow, irregular, and clumsy.
ATAXIA Gait that lacks coordination, with reeling and instability –ATAXIC
May be due to cerebellar disease, loss of position sense, or intoxication.
**Inability to heel-walk is a sensitive test for corticospinal tract damage.
ROMBERG SIGNDorsal column disease ataxia, vision compensates for the sensory loss.
(+) if loses balance when eyes are closed, a positive Cerebellar ataxia- difficulty standing with feet together – with yes open or closed.
PRONATOR DRIFTPronation of one forearm. Sensitive and specific for a corticospinal tract lesion originating in the contralateral hemisphere.
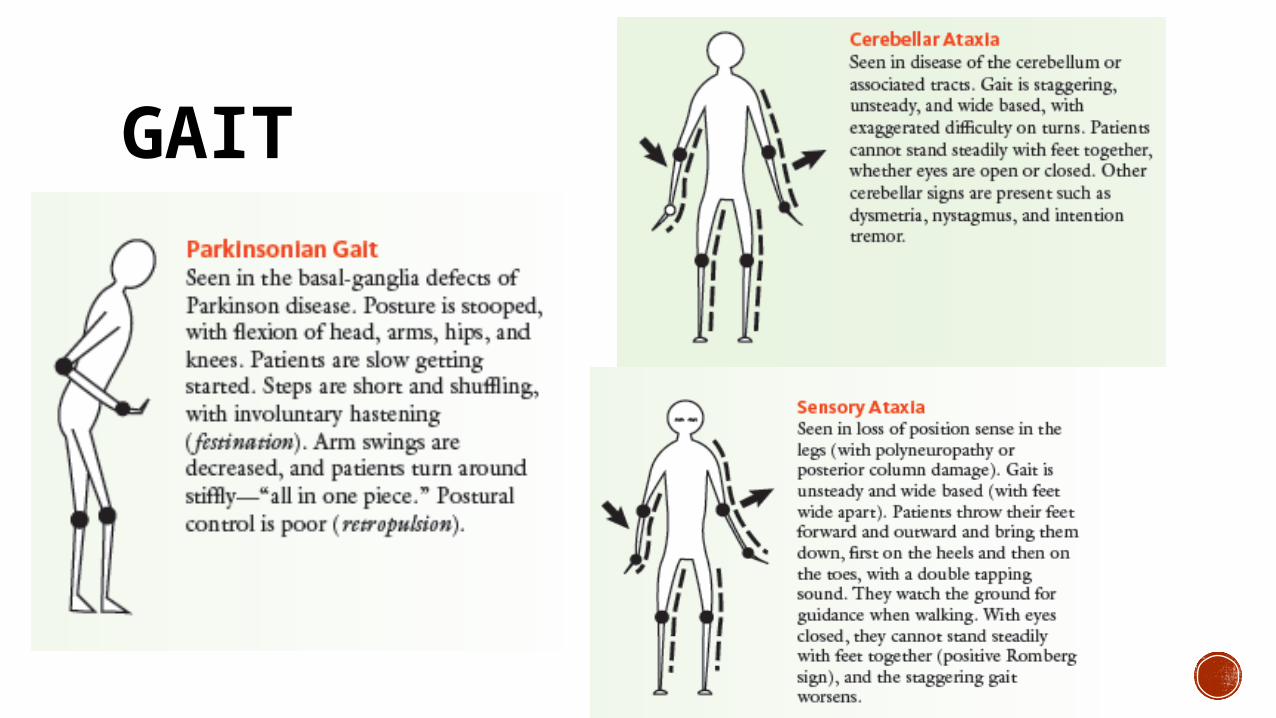
GAIT
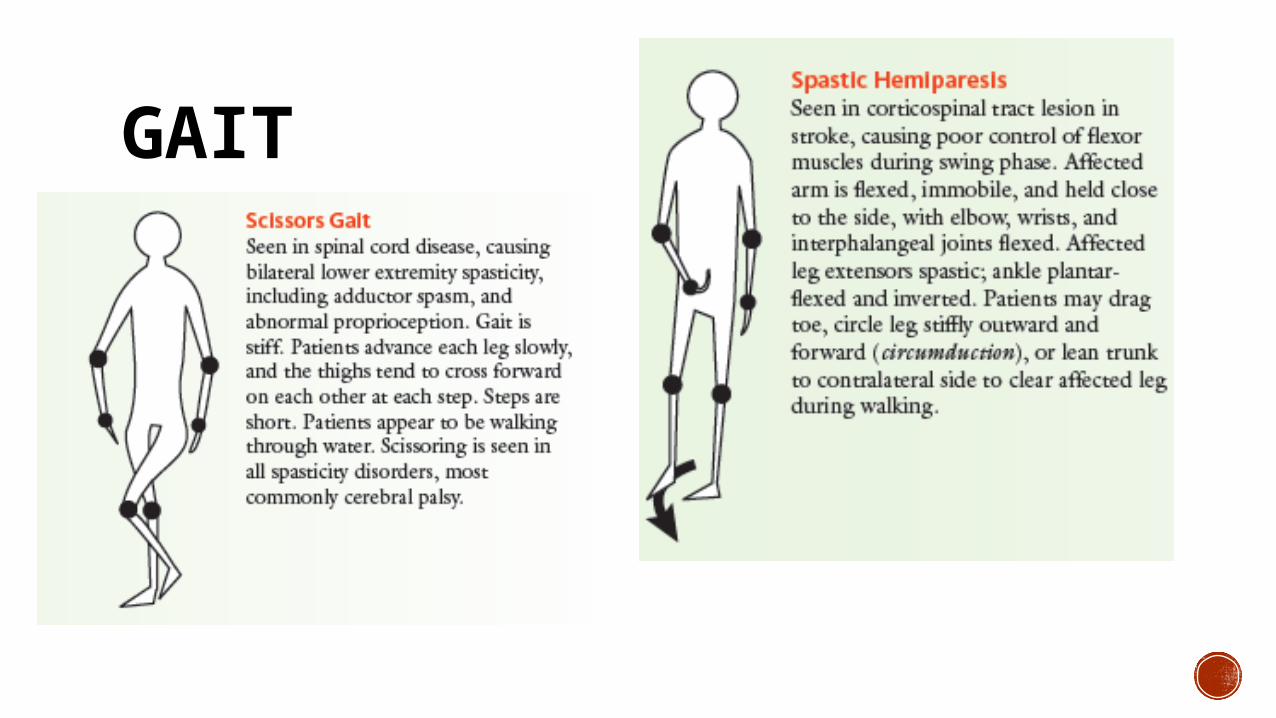
GAIT
SENSORY SYSTEM
SENSORY Pain and temperature (spinothalamic tracts)
Position and vibration (posterior columns)
Light touch (both of these pathways)
Discriminative sensations, which depend on some of the above sensations but also involve the cortex Stereognosis Graphestesia 2-point-discrimination Point localization
PATTERNS OF SENSORY TESTING Compare symmetric areas on the two sides of the body.
When testing pain, temperature, and touch sensation, also compare the distal with the proximal areas.
Scatter the stimuli to sample most of the dermatomes and major peripheral nerves both shoulders (C4) inner and outer aspects of the forearms (C6 and T1) thumbs and little fingers (C6 and C8), fronts of both thighs (L2), medial and lateral aspects of both calves (L4 and L5) little toes (S1) medial aspect of each buttock (S3).
When testing vibration and position sensation, first test the fingers and toes. If these are normal, you may safely assume that more proximal areas will also be normal.
●● Vary the pace of your testing. This is important so that the patient does not merely respond to your repetitive rhythm.
●● When you detect an area of sensory loss or hypersensitivity, map out its boundaries in detail. Stimulate first at a point of reduced sensation, and move by progressive steps until the patient detects the change.

REFLEXES
‘MJOLNIR’ SKILLS pointed end- small areas (i.e finger ), broad-end- larger areas
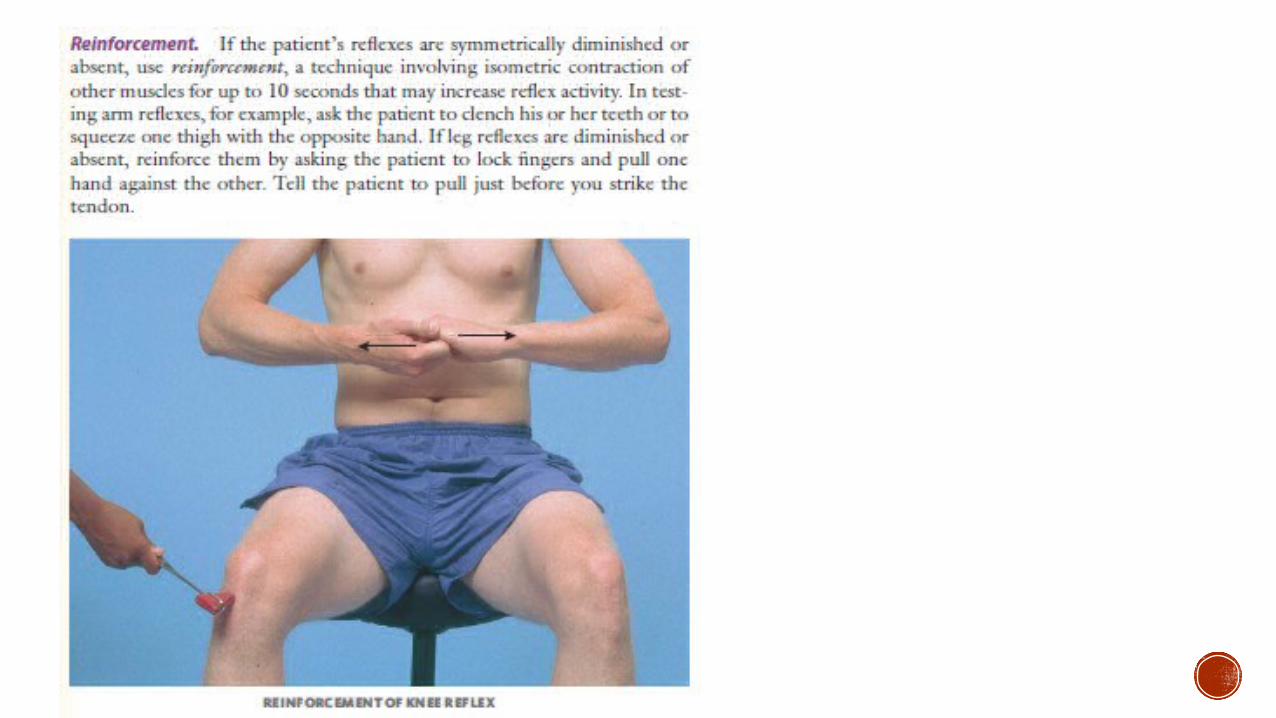
Encourage the patient to relax; position the limbs properly and symmetrically.
Hold reflex hammer loosely between your thumb and index finger so that it swings freely in an arc within the limits set by your palm and other fingers.
With wrist relaxed, strike tendon briskly using a rapid wrist movement.
Strike should be quick and direct, not glancing.
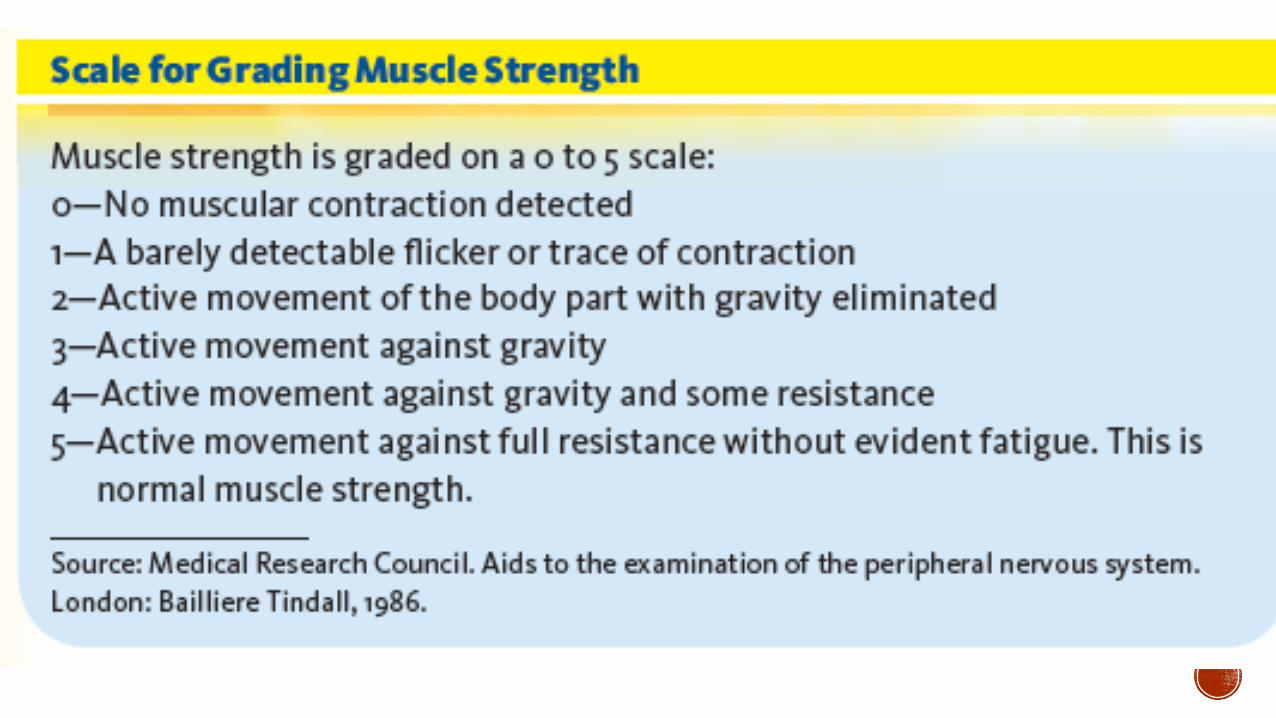
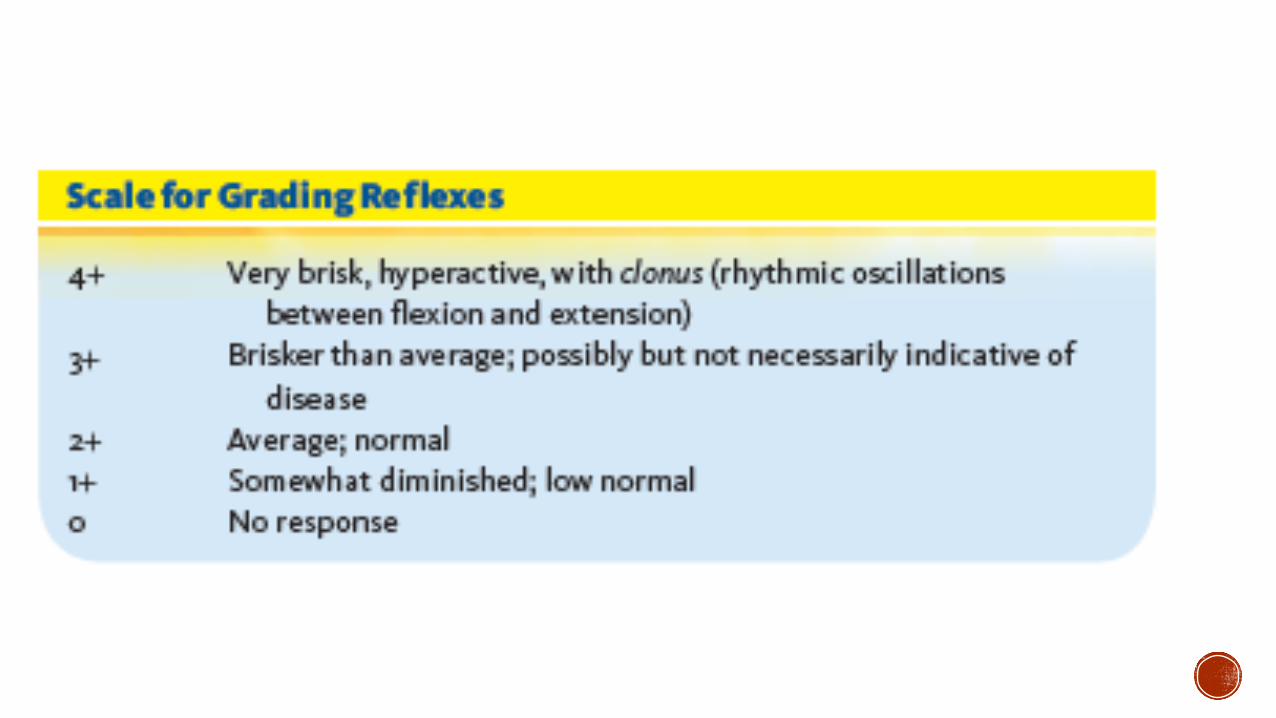
Note the speed, force, and amplitude of the reflex response and grade the response using the scale below.
Always compare the response of one side with the other. Reflexes are usually graded on a 0 to 4+ scale.
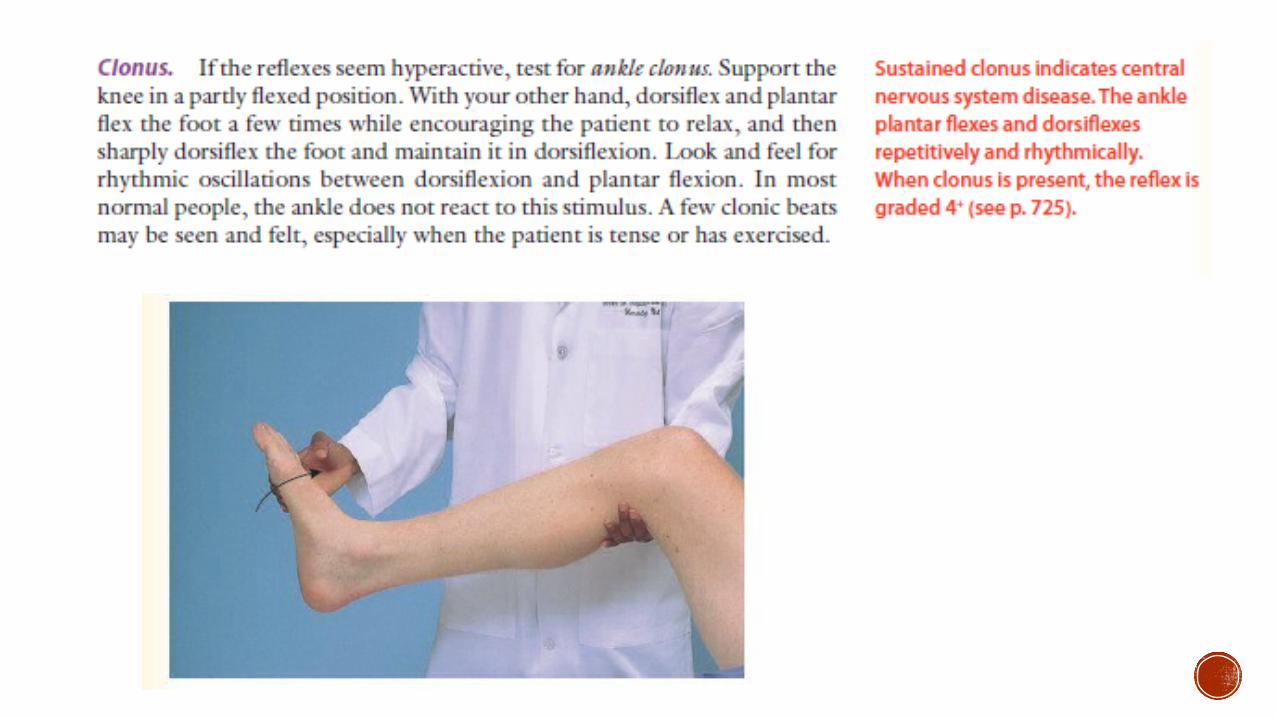
Hyperactive reflexes (hyperreflexia) - seen in CNS lesions along the descending corticospinal tract.
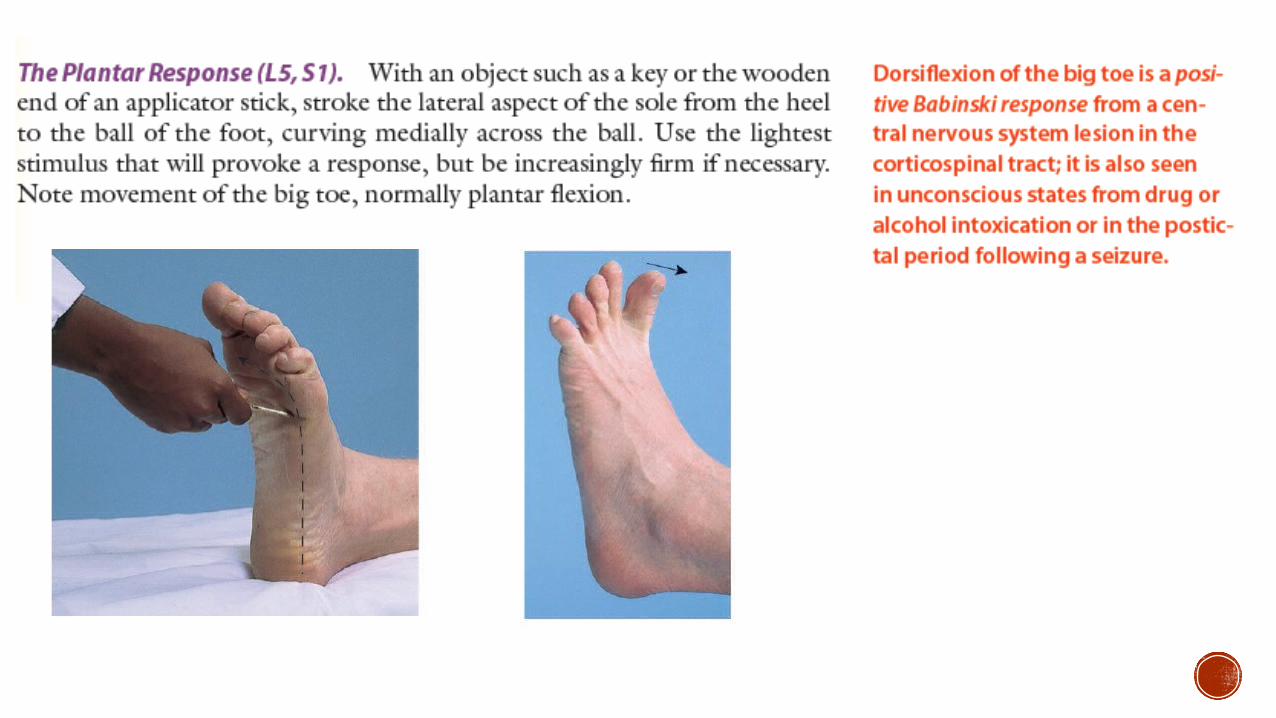
Look for associated upper motor neuron findings of weakness, spasticity, or a positive Babinski sign.
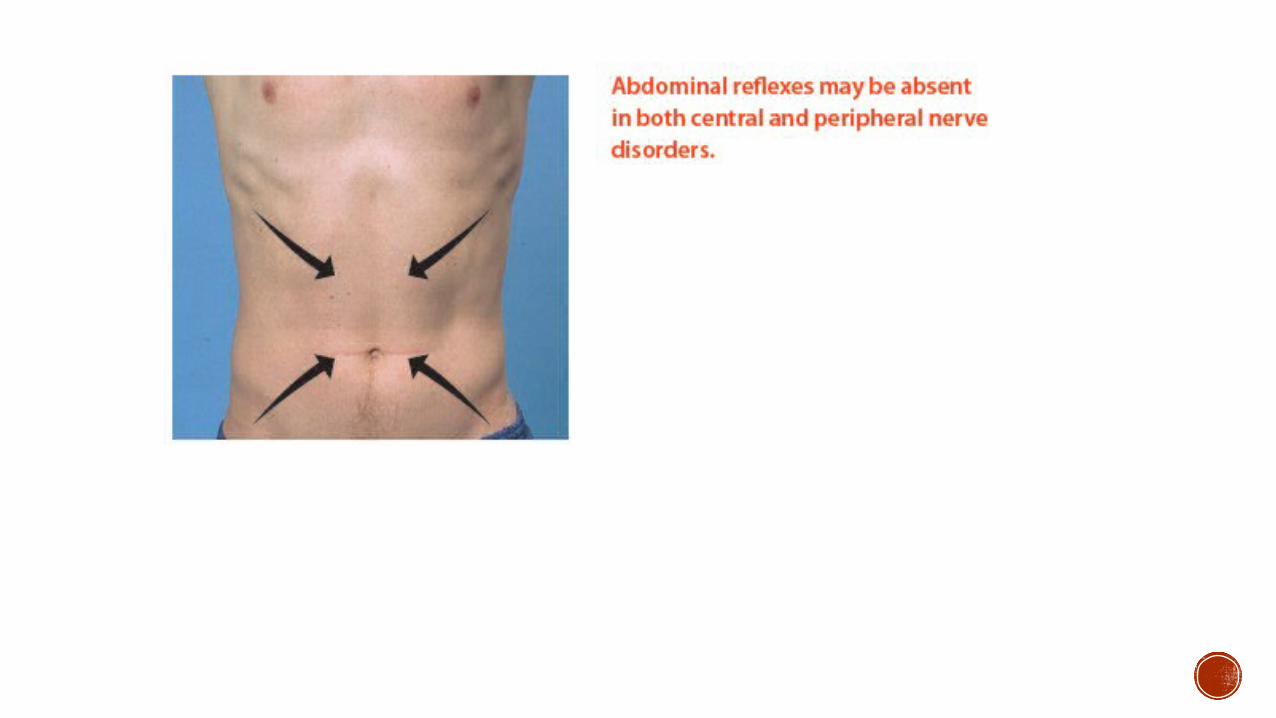
Hypoactive or absent reflexes (hyporeflexia)- seen in diseases of spinal nerve roots, spinal nerves, plexuses, or peripheral nerves.
-Look for associated findings of lower motor unit disease, namely weakness, atrophy, and fasciculations.
**MgSO4- decreases DTR

V
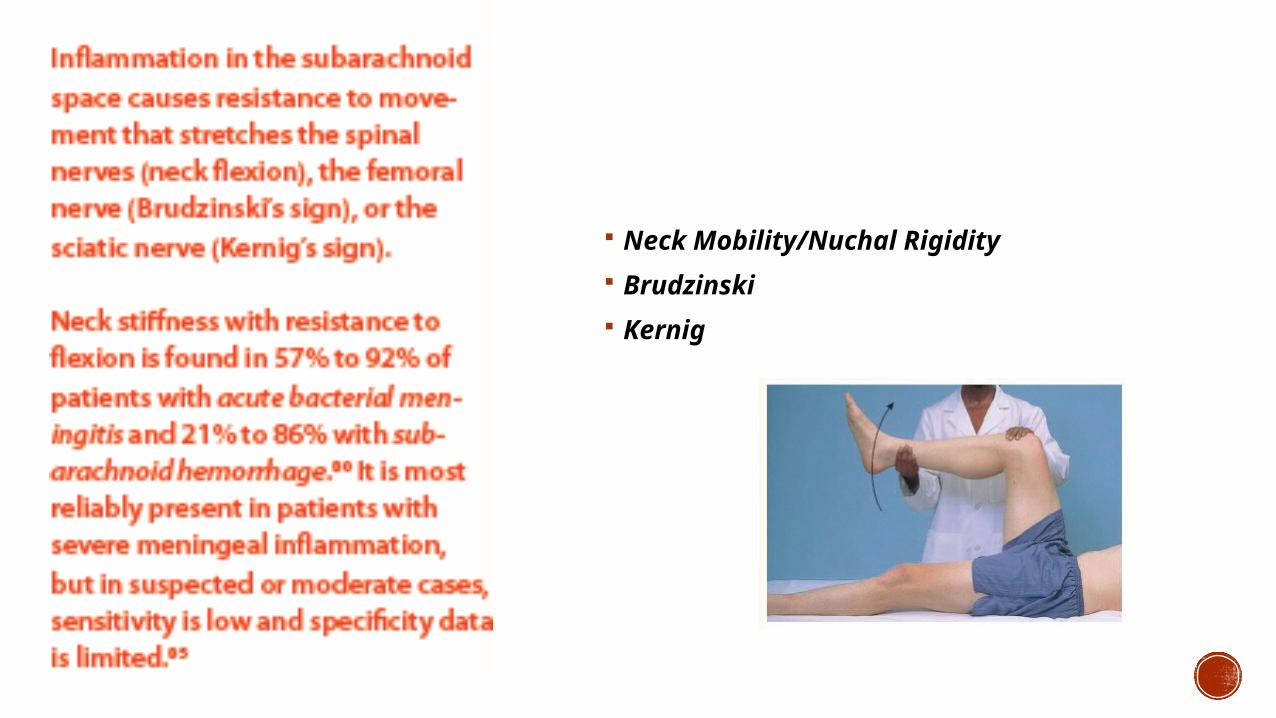
Neck Mobility/Nuchal Rigidity
Brudzinski
Kernig
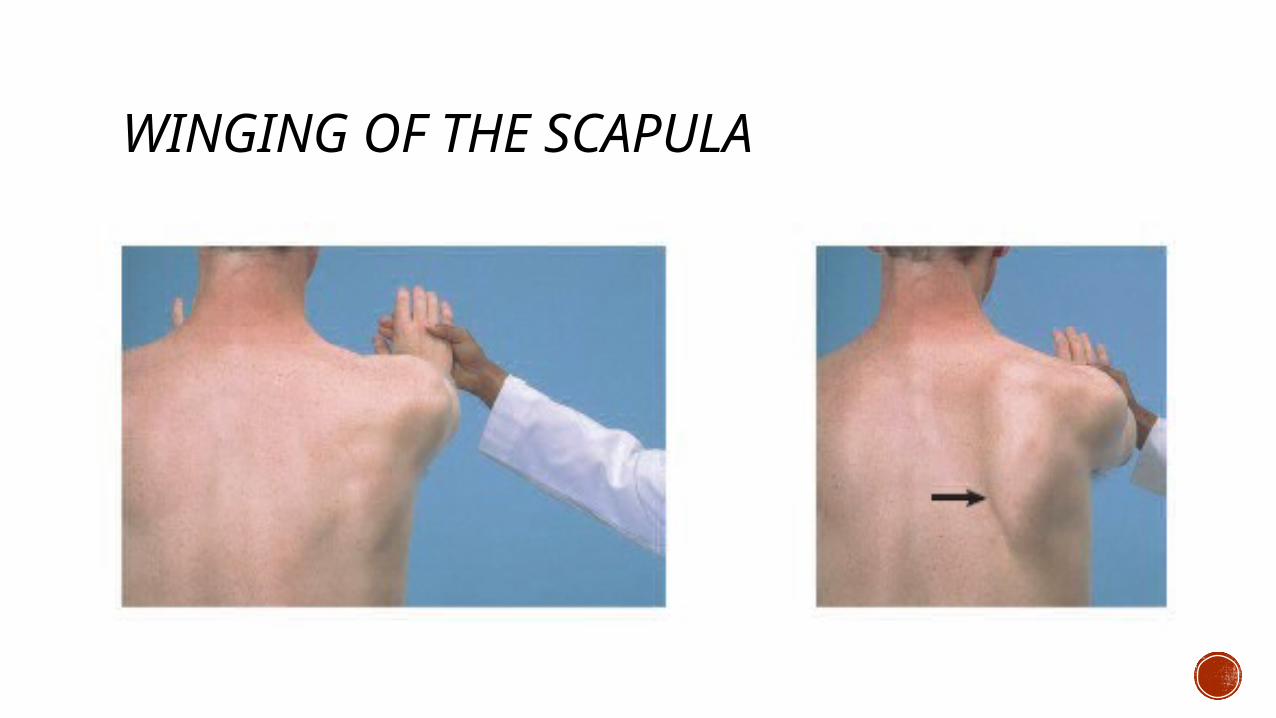
WINGING OF THE SCAPULA
Doll’s eye
I CAN NOT DEACTIVATE UNTIL YOU ARE NOT SATISFIED WITH MY CARE…
THANK YOU!