Neurologic Complications Following Obesity Surgery Review/06... · rré syndrome w were recogn gic...
13
N B.M. K No one i The id Neuro Koffman, M nvolved in th America deas and opin ologic O MD, PhD; e planning of Aut CM an Associatio 2621 S nions in this Jo Comp Obesit L.J. Green f this CME act thors/faculty ME is availabl Copy on of Neurom Superior Dr N ournal Review represent th plicat ty Sur nfield, MD, MD tivity has any have nothing le 7/15/2008 yright: 200 muscular and NW Rochest w are solely th hose of the AA t ions F rgery , PhD; I.I. y relevant fina g to disclose. - 7/15/2011 06 d Electrodiag ter, MN 559 those of the au ANEM Follow Ail, MD; N ancial relation gnostic Medi 01 uthor and do Produ wing N.A. Pirzad nships to discl icine not necessari uct: JR06 da, lose. ily
Transcript of Neurologic Complications Following Obesity Surgery Review/06... · rré syndrome w were recogn gic...

N
B.M. K
No one i
The id
Neuro
Koffman, M
involved in th
America
deas and opin
ologic O
MD, PhD;
e planning ofAut
CM
an Associatio
2621 S
nions in this Jo
CompObesit
L.J. Green
f this CME actthors/faculty
ME is availabl
Copy
on of Neurom
Superior Dr N
ournal Reviewrepresent th
plicatty Surnfield, MD,
MD
tivity has any have nothing
le 7/15/2008
yright: 200
muscular and
NW Rochest
w are solely thhose of the AA
tions Frgery, PhD; I.I.
y relevant finag to disclose.
- 7/15/2011
06
d Electrodiag
ter, MN 559
those of the auANEM
Follow
Ail, MD; N
ancial relation
gnostic Medi
01
uthor and do
Produ
wing
N.A. Pirzad
nships to discl
icine
not necessari
uct: JR06
da,
lose.
ily

CMPr CoBaprw(6anemsucocoinbydemInTheldi LeU
ReExexD AcThCoboon HoOpuvi
ME Informatioroduct: JR06 ‐
ourse Descriptariatric surgicarocedures, inc
with neurologic62%) and encend 18 (30%) hamergencies incurgical series omplications (ontrolled retronflammation orypass were evaeficiency. Rout
morbidity assocntended Audiehis course is ectrodiagnostisorders.
earning Objectpon conclusion
1. charactprogno
2. identifygastric
3. recognreduce
elease Date: 7xpiration Datexpiration date.uration/Comp
ccreditation anhe American Aouncil for Conoth sections ofnly the credit c
ow to Obtain Cnce you have urchased this pew a transcr
on Neurologic Co
tion al procedures aluding their mc symptoms afphalopathy in ad mononeurocluding Wernicreported betw(range: 0.08‐1ospective studyr an immunoloaluated in 957 tine monitoriniated with thence intended for ic medicine w
tives n of this prograterize the neuosis. y the evidencebypass. ize that routin morbidity ass
/15/2008 e: 7/15/2011. Y pletion Time: 3
nd DesignationAssociation of ntinuing Medicf this enduringcommensurate
CME reviewed the product. Answript of your
omplications Fo
are increasingmechanisms, frefter bariatric p30 (31%). Amopathies, whiccke's encephalween 1976 a6%). The onlyy identified 16ogic mechanismpatients in 8 rng of micronuse procedures
Neurologists,with the inten
am, participanurologic comp
e that suggest
ne monitoring oociated with th
Your request to
3 hours
n Statements Neuromuscul
cal Education tg material for ae with the exte
materials, youwer the questioCME by log
ollowing Obes
ly common. Inequency, and procedures. Thong the 60 pah included 17 lopathy, rhabdnd 2004, 133y prospective % of patients wm in neuropatreports. A totatrient levels a.
, Physiatrists, t to improve
ts should be abplications of b
s the role for
of micronutriehese procedur
o receive AMA
ar and Electroto provide cona combined mant of their part
u can obtain Cons and click sugging into ww
sity Surgery
n this review, wprognosis. Litehe most commatients with pe(94%) with medomyolysis, an3 of 9996 pastudy reportwith peripherahy after gastril of 236 (25%) and prompt re
and others wthe quality o
ble to: bariatric proce
inflammation
ent levels and pes.
PRA Category
odiagnostic Mntinuing medicaximum of 3 Aticipation in th
CME credit by ubmit. Once yww.aanem.org
we characterizerature reviewmon presentatieripheral neuroeralgia paresthnd Guillain‐Baratients (1.3%) ed a neuroloal neuropathy.c bypass. Micrhad vitamin Becognition of
who practice of medical car
edures, includi
or the immun
prompt recogn
1 Credits™ mu
edicine (AANEcal educationMA PRA Categhe activity.
clicking on thyour answers hg and clicking
ze the neurolow yielded 50 caions were peropathy, 40 (67hetica and 1 wrré syndrome wwere recogngic complicati. There is evideronutrient defB12 deficiency neurological c
neuromusculre to patients
ing their mec
nologic mecha
nition of neuro
ust be submitte
EM) is accredifor physiciansgory 1 creditsTM
e link in the ehave been submg View Profi
ogic complicatiase reports of ripheral neuro7%) had a polywith foot drop.were also repoized to have ion rate of 4ence to suggesficiencies followand 11 (1%) hacomplications
ar, musculosks with muscle
hanisms, freq
nism in neuro
ological compli
ed on or befor
ited by the Acs. The AANEMM. Physicians s
e‐mail receivedmitted, you wile and then
ons of such 96 patients pathy in 60 neuropathy Neurologic orted. In 18 neurologic .6%, and a st a role for wing gastric ad thiamine can reduce
keletal, and and nerve
uency, and
opathy after
ications can
re the credit
ccreditation designates hould claim
d when you ll be able to My CME.

INVITED REVIEW ABSTRACT: Bariatric surgical procedures are increasingly common. Inthis review, we characterize the neurologic complications of such proce-dures, including their mechanisms, frequency, and prognosis. Literaturereview yielded 50 case reports of 96 patients with neurologic symptoms afterbariatric procedures. The most common presentations were peripheral neu-ropathy in 60 (62%) and encephalopathy in 30 (31%). Among the 60 patientswith peripheral neuropathy, 40 (67%) had a polyneuropathy and 18 (30%)had mononeuropathies, which included 17 (94%) with meralgia parestheticaand 1 with foot drop. Neurologic emergencies including Wernicke’s enceph-alopathy, rhabdomyolysis, and Guillain–Barre syndrome were also reported.In 18 surgical series reported between 1976 and 2004, 133 of 9996 patients(1.3%) were recognized to have neurologic complications (range: 0.08–16%). The only prospective study reported a neurologic complication rate of4.6%, and a controlled retrospective study identified 16% of patients withperipheral neuropathy. There is evidence to suggest a role for inflammationor an immunologic mechanism in neuropathy after gastric bypass. Micronu-trient deficiencies following gastric bypass were evaluated in 957 patients in8 reports. A total of 236 (25%) had vitamin B12 deficiency and 11 (1%) hadthiamine deficiency. Routine monitoring of micronutrient levels and promptrecognition of neurological complications can reduce morbidity associatedwith these procedures.
Muscle Nerve 33: 166–176, 2006
NEUROLOGIC COMPLICATIONS AFTERSURGERY FOR OBESITY
BOYD M. KOFFMAN, MD, PhD, L. JOHN GREENFIELD, MD, PhD,
IMRAN I. ALI, MD, and NOOR A. PIRZADA, MD
Department of Neurology, 3120 Glendale Avenue, RHC 1450,Medical University of Ohio, Toledo, Ohio 43614, USA
Accepted 9 May 2005
Obesity affects a significant portion of the popula-tion. Alarmingly, 26% of American adults and chil-dren are obese with a body mass index (BMI) �30kg/m2. An additional 35% of the adult population isoverweight (BMI �25 kg/m2).62 Deaths attributed toobesity in the United States are estimated at280,000–325,000 annually.5 Complications of obesityinclude hypertension,88 arthralgias,135 idiopathic in-tracranial hypertension,67,135 sleep apnea,8,135 andtype 2 diabetes mellitus.88
Several series note improvement in comorbid con-ditions of obesity following bariatric surgery, includingreduced or eliminated need for insulin and antihyper-tensive medications,7,8,20,121,135 reduction in lipid dis-turbances,20,121 improvement in degenerative joint dis-ease,135 resolution of signs and symptoms of idiopathicintracranial hypertension,134,135 and elimination ofsleep apnea.8,27,107,135 Surgical treatment of severe obe-sity is increasing, driven by both medical and economicforces. Approximately 10,000 procedures were doneannually in the early 1980s,56 with predictions of 80,000bariatric procedures for 2002,82 and 100,000 for2003.119 Hospital strategists advocate bariatric surgeryprograms as a potentially lucrative market, with hospi-tal revenues in 2001 between $850 million and $1.8billion and increases for 2002 predicted at 60%–75%.6
Profit margins for hospitals may surpass 20%.119
Surgical candidates include those who are twicetheir ideal weight, demonstrate recurrent failure tolose weight through dieting, have no cardiopulmo-nary or psychiatric contraindications, and are usuallyage 50 years or younger,63 although surgery is car-
Available for Category 1 CME credit through the AANEM at www.aanem.org.
Abbreviations: APGARS, acute post–gastric reduction surgery; BMI, bodymass index; CK, creatine kinase; MUAP, motor unit action potential; NADPH,nicotinamide adenine dinucleotide phosphate; RDA, recommended dietaryallowance; SNAP, sensory nerve action potential; VLDL, very low-densitylipoproteinKey words: bariatric surgery; encephalopathy; micronutrients; myopathy;neuropathyCorrespondence to: B.M. Koffman; e-mail: [email protected]
© 2005 Wiley Periodicals, Inc.Published online 22 June 2005 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/mus.20394
166 Obesity Surgery Complications MUSCLE & NERVE February 2006

ried out in selected patients in older age groups withgood results.74
The first surgical treatments for weight reductionwere global malabsorption procedures that em-ployed either a jejunocolic shunt94 or small bowelbypass, but techniques have varied and continue toevolve9,19 (Fig. 1). Jejunocolic shunt and, subse-quently, jejunoileal bypass114 were both abandoneddue to severe metabolic derangements.4,9,42,52,122
Gastric restriction (gastric partitioning, gastroplasty,vertical banded gastroplasty, gastric stapling) sepa-rates the stomach into a restricted upper pouch(�50 ml) that empties into the rest of the stomachthrough a narrow-caliber channel (approximately 11mm).4,9,81 Weight loss following gastric restriction isnot sustained and has been deemed unsatisfactory.
Mason and Ito83 instead advocated the use ofgastric bypass, which was later modified with Roux-en-Y reconstitution and found favorable to jejuno-ileal bypass.52 Gastric bypass restricts the volume in-gested and induces a dumping syndrome if a high-carbohydrate meal is ingested, yielding sustainedweight loss.9 Roux-en-Y gastric bypass combines gas-
tric restriction and dumping physiology, is the first-line procedure for many surgeons,9 and is increas-ingly performed laparoscopically.61 For persons with“super” obesity (BMI �50 kg/m2),113 proceduresproducing selective maldigestion and malabsorptionwith partial gastric restriction have been advocated,including partial biliopancreatic bypass or modifica-tions such as distal gastric bypass,136 very, very long-limb gastric bypass,87 and biliopancreatic bypass withduodenal switch modification.79
The goals for most bariatric procedures are: (1)limited food intake; (2) satiety; and (3) normal ab-sorption and digestion,42 allowing for loss of 50–60% of excess body weight and reducing medicalcomplications of obesity.9 The first two objectives areattained by forming a small gastric pouch; the lim-ited amount of food ingested flows through a smallcaliber outflow and provides prolonged satiety.42,70
Leaving the small bowel relatively unaltered allowsnormal absorption and digestion,42 but even gastricbypass surgery may be complicated by malabsorp-tion9 or aversion for certain foods with potential lossof essential nutrients.22,70
MECHANISMS OF NEUROLOGIC INJURY
Following bariatric surgery, neurologic complica-tions may include compression mononeuropathiesas weight is lost, and dysfunction or neurologic dam-age at multiple levels of the neuraxis due to malab-sorption. The neurologic complications of malab-sorption syndromes and micronutrient (vitamin)deficiencies were reviewed in detail by Chaudhry etal.27 We will focus here on nutrient deficiencies spe-cifically associated with weight-reduction surgeries.
In 8 studies evaluating micronutrient levels follow-ing bariatric surgery in 957 patients,13,17,34,56,77,100,108,124
236 (25%; range: 2–64%) were identified with vitaminB12 deficiency, 195 (20%; range 0–35%) with serumfolate deficiency, and 11 (1%) with thiamine defi-ciency. Micronutrient analysis was neither uniform norconsistent, and patients were not characterized clini-cally. The neurologic consequences of such deficien-cies are predictable, and related to their biochemicalfunctions.
Cyanocobalamin (Vitamin B12). Gastric bypass leavesthe stomach essentially intact, yet vitamin B12 defi-ciency may occur.7,24,77,100 Gastric bypass reducedplasma vitamin B12 levels 1 year later in approxi-mately 30% of 20 patients despite a theoreticallyadequate oral intake and supplementation.100 Surgi-cal series identified low or deficient serum vitamin
FIGURE 1. Various bariatric surgical procedures. (A) Jejunoilealbypass. (B) Vertical banded gastroplasty. (C) Gastric banding.(D) Roux-en-Y gastric bypass. (E) Partial biliopancreatic bypass.(F) Very, very long-limb Roux-en-Y gastric bypass. (G) Partialbiliopancreatic bypass with duodenal switch. Reprinted from Bal-siger et al.,9 Copyright 2000, with permission from Elsevier.
Obesity Surgery Complications MUSCLE & NERVE February 2006 167

B12 levels in 24–70% of patients 1–9 years aftersurgery.7,34,56,77
Vitamin B12 deficiency following gastric bypasshas been attributed to inadequate intake,34,56 im-paired hydrolysis of vitamin B12 from dietary pro-tein,33,34,56 and a defect in either the amount ofintrinsic factor available or the interaction betweenintrinsic factor and vitamin B12.34,108 Animals areunable to synthesize vitamin B12. Vitamin B12 in an-imal products is derived primarily from bacterialsynthesis. The daily adult vitamin B12 requirement is2 �g, and the body typically stores 3000–5000�g.103,133
Intrinsic factor, produced by gastric parietal cells,binds vitamin B12 in the stomach and mediates in-testinal absorption at receptors in the ileum. It istransferred across the intestinal mucosa to transco-balamin II, a plasma transport protein that mediatesits distribution.133 Vitamin B12 also diffuses passivelyacross the intestinal mucosa at pharmacologic doses(ingestion of �30 �g).60 With enterohepatic circu-lation,133 the half-life of vitamin B12 is approximately400 days110; symptoms of deficiency may not presentuntil months to years after surgery.
Vitamin B12 participates in two enzymatic reac-tions in humans35: conversion of l-methylmalonylcoenzyme A into succinyl coenzyme A, and methyl-ation of homocysteine to methionine. Succinyl coen-zyme A enters the citric acid cycle and participates ingluconeogenesis. This pathway, linking carbohy-drate and fat metabolism, plays a role in myelinsynthesis.103 Methyl-B12 methylates animal RNA,145
which slows mRNA degradation. Impaired methyl-ation of RNA may explain the involvement of longaxons in vitamin B12 deficiency,103 since RNA turn-over in neurons is very high, and rapid degradationof mRNA might limit production of proteins essen-tial for axon maintenance.
Although deficiency is classically associated withsubacute combined degeneration,72,120 and there arereports of myelopathy associated with vitamin B12
deficiency following partial103,146 or complete gas-trectomy,10 subacute combined degeneration hasnot been reported following gastric bypass. Commonneurologic symptoms of deficiency include paresthe-sias (21%), ataxia (12%), and weakness (6%).72
Folate. Folate deficiency following gastric bypassapproaches 10%.13,57 MacLean et al. noted red-cellfolate deficiency in 3 (18%) and serum folate defi-ciency in 11 of 17 (65%) patients readmitted formalnutrition or excessive weight loss following sur-gery.77 The U.S. recommended dietary allowance(RDA) for men, nonpregnant and nonlactating
women, and adolescents is 3 �g/kg body weight;sources include liver, yeast, leafy vegetables, le-gumes, and some fruits.133
The neurologic complications of folate defi-ciency are not well characterized and are even de-batable. Older literature suggests that affective dis-orders may be associated more with folate deficiencythan with vitamin B12 deficiency.120 Case reports sug-gest that folate deficiency may be associated withperipheral neuropathy,51 myelopathy,51 or restlesslegs syndrome.12 Among 28 patients with folate de-ficiency, 6 (21%) had abnormal electrophysiologicfindings, including abnormal sural sensory nerve ac-tion potential (SNAP), and 5 also had an abnormalmedian SNAP.120 Yet, there are data to suggest thatfolate deficiency is not responsible for neurologicdeficits. Lindenbaum et al.72 found that 40 of 141(28%) patients with neuropsychiatric abnormalitiescaused by vitamin B12 deficiency did not have ane-mia, and, in a subsequent investigation,59 no corre-lation between the severity of neurologic deficit andserum folate was identified.
Pyridoxine (Vitamin B6). Three of four patients re-ceiving low-dose pyridoxine supplementation at 6months after gastric bypass, and two of two patientsreceiving low-dose pyridoxine supplementation at 12months were deficient, as measured by serum lev-els.13 Signs of deficiency include seizures, dermatitis,and anemia. Peripheral polyneuropathy and sub-acute combined degeneration attributed to pyridox-ine deficiency have been reported.92
Vitamin B6 is absorbed by the intestinal mucosa.Sources include meats, eggs, soybeans, unmilledrice, grains, and nuts. The human adult RDA is 0.016mg/g protein per day.133 Three related forms ofpyridoxine (pyridoxine, pyridoxal, and pyridoxam-ine) are converted to pyridoxal phosphate by theliver, red blood cells, and other tissues for use as acofactor in transamination reactions, decarboxyl-ation and racemization of amino acids, metabolismof lipids and nucleic acids, and as a coenzyme forglycogen phosphorylase.133
Thiamine. Thiamine is found in both plants (forti-fied grains, cereals, legumes, seeds, nuts, brewer’syeast) and animals (organ meats, pork).133 The adultRDA for thiamine is 1 mg.133 Thiamine can be de-pleted from a healthy body in 18 days.150 Thiamine islikely absorbed in the proximal small intestine by acarrier-mediated process when lumenal concentra-tions are low, and also by passive diffusion with phar-macologic doses.101,133
168 Obesity Surgery Complications MUSCLE & NERVE February 2006

Thiamine pyrophosphate is a cofactor in oxida-tive decarboxylation of carbohydrates by providingthe prosthetic group for three important enzymes.Pyruvate dehydrogenase and �-ketoglutarate dehy-drogenase catalyze the conversion of pyruvate toacetyl coenzyme A and �-ketoglutarate to succinylcoenzyme A, respectively. Transketolase transfers ac-tivated aldehydes in the hexose monophosphateshunt (pentose phosphate pathway) in the genera-tion of the reduced form of nicotinamide adeninedinucleotide phosphate (NADPH) for reductive bio-syntheses.131 Thiamine deficiency causes lactic acido-sis, reduced oxygen uptake, and depression of trans-ketolase activity predominantly in the brainstem,37
which correlates with the clinical presentation ofWernicke’s encephalopathy.
Thiamine deficiency results in both acute andchronic encephalopathies (Wernicke’s encephalop-athy and Korsakoff’s syndrome).37 The clinical triadof Wernicke’s encephalopathy (encephalopathy,nystagmus or ophthalmoplegia, and ataxia) can beprecipitated by malnutrition, administration of car-bohydrates, and intake of thiaminase present inteas142 and fish.86
Wernicke’s encephalopathy is associated with nutri-tional polyneuropathy (dry beriberi). It is unclearwhether nutritional polyneuropathy is due to isolatedthiamine deficiency or multiple vitamin deficiencies.78
Vitamin D. Sources of vitamin D include fortifiedfoods and conversion of inactive to active vitamin Dby skin exposure to ultraviolet radiation or sun-light.132 The human adult RDA of vitamin D is 5 �g(200 IU).132
Classic manifestations of vitamin D deficiencyinclude rickets in children and hypocalcemia andosteopenia in adults.132 An associated syndrome ofosteomalacic myopathy has also been described,96
with features of myopathy111,149 and diffusepain.46,97,102 Vitamin D deficiency is a common find-ing among persons with chronic nonspecific muscu-loskeletal pain.97 Myopathy attributed to vitamin Ddeficiency was identified in 3 of 106 patients follow-ing a gastrectomy procedure; nerve conductionstudies were normal in each case, and all three dem-onstrated “myopathic” motor units on electromyo-graphy.10 All improved with treatment.10
Vitamin E. Among 21 patients followed prospec-tively after gastric bypass, 6 of 20 had marginal to-copherol levels at 6 months, and 2 of 21 had mar-ginal tocopherol levels at 12 months.13 Tocopherol,a fat-soluble vitamin, is secreted into the lymph andtaken up by chylomicra, transported to the liver, and
then into the blood in very low-density lipoproteins(VLDLs). During VLDL metabolism, tocopherol istransferred to low- or high-density lipoproteins. Itfunctions as an antioxidant.132 Sources include veg-etable oils, vegetable oil products (margarine, short-ening), leafy vegetables, nuts, and wheat germ. Theadult RDA is 10 mg for males and 8 mg for fe-males.132
Human vitamin E deficiency has been associatedwith both myopathy139 and neuropathy.89 Myopathyhas been associated with reduced serum concentra-tion of vitamin E and prolongation of the QT inter-val on electrocardiogram.112 Vitamin E–deficientrats and monkeys consistently develop a reversiblenecrotizing myopathy.89
Neuropathic changes are also significant. Severevitamin E deficiency in humans can produce a pro-gressive (primarily) sensory axonopathy, especiallyinvolving large fibers in the posterior columns, sen-sory roots, and peripheral nerves.53,89,90 Vitamin Eneuropathy and myopathy are important to considersince they are potentially treatable.139
Other Micronutrients. Minerals (calcium, phos-phorus, and magnesium) and trace elements (zinc,iodine, copper, manganese, fluoride, chromium,molybdenum, selenium, and iron) have seldombeen studied in patients following gastric bypass.
Calcium is the best-characterized mineral follow-ing bariatric surgery. Calcium intake was reduced to�70% of RDA in 31 of 41 (75%) patients; serumcalcium was low in 1 patient.34 New or worseningaches or pains �1 year following gastric bypass oc-curred in 26 of 41 (65%) patients, usually within 5years after surgery.34 This pain has been called “by-pass bone disease” and is thought due to bone demi-neralization from impaired calcium absorption.34 By-rne23 recommended a calcium supplement of 1200mg daily.
Phosphorus intake was reduced to �70% of RDAin 26% of patients undergoing gastric bypass forobesity.34 Sugerman134 identified patients with mag-nesium deficiency following bariatric proceduresand recommended monitoring.
Changes in other trace elements following bari-atric surgery have not been described, but may beimportant. For example, selenium deficiency cancause a cardiomyopathy (Keshan’s disease) in hu-mans and white muscle disease in grazing cattle.71,116
CHARACTERISTICS AND PREVALENCE OFNEUROLOGIC COMPLICATIONS
Case Reports. We identified 50 case reports of neu-rologic complications of bariatric surgeries. Among
Obesity Surgery Complications MUSCLE & NERVE February 2006 169
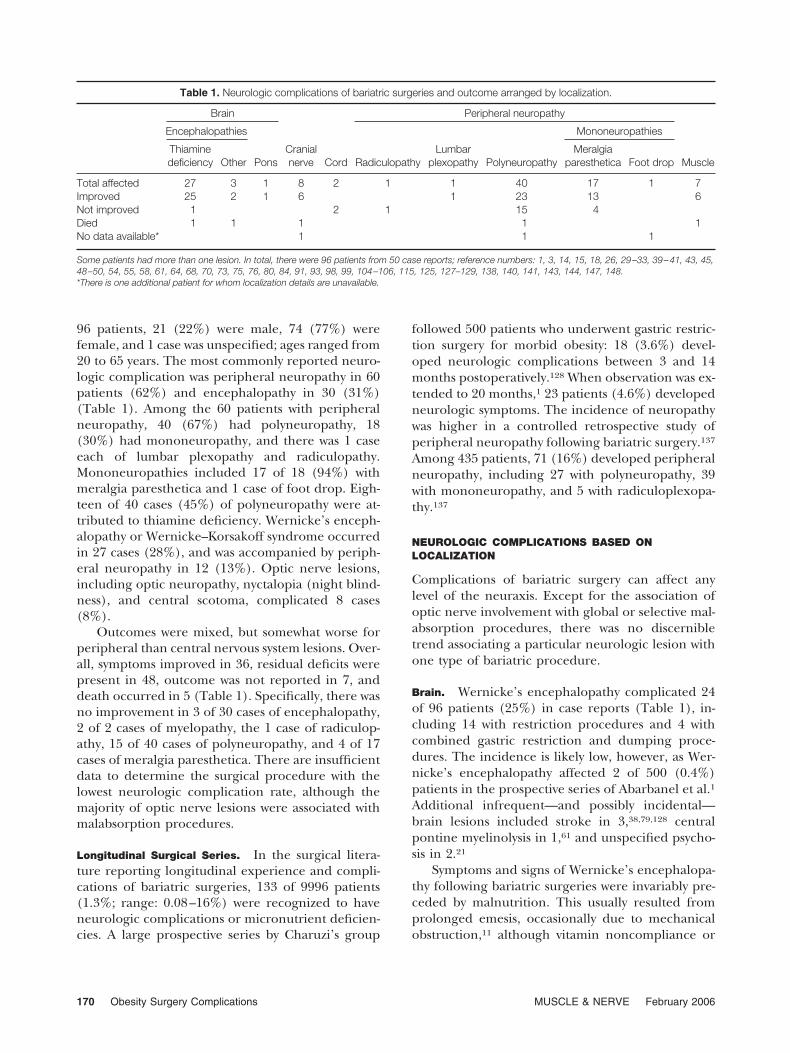
96 patients, 21 (22%) were male, 74 (77%) werefemale, and 1 case was unspecified; ages ranged from20 to 65 years. The most commonly reported neuro-logic complication was peripheral neuropathy in 60patients (62%) and encephalopathy in 30 (31%)(Table 1). Among the 60 patients with peripheralneuropathy, 40 (67%) had polyneuropathy, 18(30%) had mononeuropathy, and there was 1 caseeach of lumbar plexopathy and radiculopathy.Mononeuropathies included 17 of 18 (94%) withmeralgia paresthetica and 1 case of foot drop. Eigh-teen of 40 cases (45%) of polyneuropathy were at-tributed to thiamine deficiency. Wernicke’s enceph-alopathy or Wernicke–Korsakoff syndrome occurredin 27 cases (28%), and was accompanied by periph-eral neuropathy in 12 (13%). Optic nerve lesions,including optic neuropathy, nyctalopia (night blind-ness), and central scotoma, complicated 8 cases(8%).
Outcomes were mixed, but somewhat worse forperipheral than central nervous system lesions. Over-all, symptoms improved in 36, residual deficits werepresent in 48, outcome was not reported in 7, anddeath occurred in 5 (Table 1). Specifically, there wasno improvement in 3 of 30 cases of encephalopathy,2 of 2 cases of myelopathy, the 1 case of radiculop-athy, 15 of 40 cases of polyneuropathy, and 4 of 17cases of meralgia paresthetica. There are insufficientdata to determine the surgical procedure with thelowest neurologic complication rate, although themajority of optic nerve lesions were associated withmalabsorption procedures.
Longitudinal Surgical Series. In the surgical litera-ture reporting longitudinal experience and compli-cations of bariatric surgeries, 133 of 9996 patients(1.3%; range: 0.08–16%) were recognized to haveneurologic complications or micronutrient deficien-cies. A large prospective series by Charuzi’s group
followed 500 patients who underwent gastric restric-tion surgery for morbid obesity: 18 (3.6%) devel-oped neurologic complications between 3 and 14months postoperatively.128 When observation was ex-tended to 20 months,1 23 patients (4.6%) developedneurologic symptoms. The incidence of neuropathywas higher in a controlled retrospective study ofperipheral neuropathy following bariatric surgery.137
Among 435 patients, 71 (16%) developed peripheralneuropathy, including 27 with polyneuropathy, 39with mononeuropathy, and 5 with radiculoplexopa-thy.137
NEUROLOGIC COMPLICATIONS BASED ONLOCALIZATION
Complications of bariatric surgery can affect anylevel of the neuraxis. Except for the association ofoptic nerve involvement with global or selective mal-absorption procedures, there was no discernibletrend associating a particular neurologic lesion withone type of bariatric procedure.
Brain. Wernicke’s encephalopathy complicated 24of 96 patients (25%) in case reports (Table 1), in-cluding 14 with restriction procedures and 4 withcombined gastric restriction and dumping proce-dures. The incidence is likely low, however, as Wer-nicke’s encephalopathy affected 2 of 500 (0.4%)patients in the prospective series of Abarbanel et al.1
Additional infrequent—and possibly incidental—brain lesions included stroke in 3,38,79,128 centralpontine myelinolysis in 1,61 and unspecified psycho-sis in 2.21
Symptoms and signs of Wernicke’s encephalopa-thy following bariatric surgeries were invariably pre-ceded by malnutrition. This usually resulted fromprolonged emesis, occasionally due to mechanicalobstruction,11 although vitamin noncompliance or
Table 1. Neurologic complications of bariatric surgeries and outcome arranged by localization.
Brain
Cranialnerve Cord
Peripheral neuropathy
Muscle
Encephalopathies
Pons RadiculopathyLumbar
plexopathy Polyneuropathy
Mononeuropathies
Thiaminedeficiency Other
Meralgiaparesthetica Foot drop
Total affected 27 3 1 8 2 1 1 40 17 1 7Improved 25 2 1 6 1 23 13 6Not improved 1 2 1 15 4Died 1 1 1 1 1No data available* 1 1 1
Some patients had more than one lesion. In total, there were 96 patients from 50 case reports; reference numbers: 1, 3, 14, 15, 18, 26, 29–33, 39–41, 43, 45,48–50, 54, 55, 58, 61, 64, 68, 70, 73, 75, 76, 80, 84, 91, 93, 98, 99, 104–106, 115, 125, 127–129, 138, 140, 141, 143, 144, 147, 148.*There is one additional patient for whom localization details are unavailable.
170 Obesity Surgery Complications MUSCLE & NERVE February 2006

increased alcohol consumption were also noted.Weight loss in excess of 7 kg/month in the first fewmonths may suggest intake restriction.105 Peltier etal.95 and Printen et al.99 recognized that prolongedemesis may precipitate Wernicke’s encephalopathyand emphasized patient education regarding thesize of the gastric pouch (�50 ml) to prevent over-eating that can result in vomiting and thiamine de-ficiency.
Cranial Nerves. Optic nerve lesions complicated 8reported cases (8%).15,18,43,54,93,125,138,148 These in-cluded 6 of 9 reports of neurologic complicationsafter jejunoileal bypass, 1 of 4 reports involving bil-iopancreatic bypass, and 1 of 56 reports of compli-cations after gastroplasty, again suggesting increasedfrequency with malabsorption rather than gastricbypass procedures. Symptoms and signs includedcentral scotoma, nyctalopia, and optic neuropathy.Nutritional amblyopia and carotene deficiency fol-lowing jejunoileal bypass manifested as central sco-toma138 or nyctalopia.15,18,93,148
Spinal Cord. There are two reported cases of my-elopathy after gastric bypass (Table 1).1 The causeremained uncertain, and empiric therapy was of nobenefit. Possible etiologies include deficiencies ofserum copper, vitamin B12, pyridoxine, and folate.Copper deficiency has been implicated in the devel-opment of a myelopathy following partial gastrec-tomy69,109 or intestinal bypass.69
Peripheral Nerve. As noted earlier, peripheral neu-ropathy was found in 60 of 96 patients (62%) de-scribed in case reports (Table 1). Although mostpresented as chronic conditions, likely related tomicronutrient deficiency, Guillain–Barre syndromewas reported in 2 patients (2%), and there wereseveral additional cases among the surgical se-ries.28,126
Generalized Neuropathy. All 27 patients with ageneralized polyneuropathy were sensory-predomi-nant in one recent series.137 Most had a slow onsetwith chronic course. Some case reports of Wer-nicke’s encephalopathy were associated with poly-neuropathy (dry beriberi). It is unclear whether theneuropathy is due to isolated thiamine deficiency ormultiple vitamin deficiencies.78 Nutritional polyneu-ropathy presents insidiously with a symmetric senso-rimotor neuropathy affecting the lower extremitiesmore than the upper extremities. Symptoms includeanesthesia, tingling paresthesias, and severe pain,particularly involving the feet (“burning feet syn-drome”).78 Examination may reveal muscle tender-
ness on palpation, hyporeflexia, and sensory impair-ment involving pain and light touch in a stocking-and-glove distribution, distal vibratory and proprioceptionloss, and foot drop.78
Potentially treatable malabsorption syndromesthat may affect peripheral nerves following gastricbypass include deficiencies of vitamin B12,72 thia-mine,37 and vitamin E.89 Vitamin D deficiency mayaffect the peripheral nerves, but this has not beenconfirmed.96 Although vitamin E deficiency is asso-ciated with neuropathy,89 no specific reports wereidentified as complications of bariatric surgeries.Data from sural nerve biopsies following Roux-en-Yalso suggest the possibility of an immunologic mech-anism in polyneuropathy (see later).137
Several new terms have been proposed to identifyneuropathy complicating gastric bypass surgery, in-cluding “bariatric beriberi”47 and “acute post–gastricreduction surgery (APGARS)” neuropathy.2,25 Un-fortunately, no diagnostic criteria for this possiblesyndrome have been identified.2 Since nutritionalpolyneuropathies have been better characterizedand are thus more informative regarding mecha-nism and prognosis, there is little advantage to add-ing a new and undefined term to the lexicon, espe-cially when the acronym is easily confused withanother firmly established medical term (the Apgarscore).
Focal Mononeuropathies. Of 71 patients with pe-ripheral neuropathy in the retrospective series of435 patients by Thaisetthawatkul et al.,137 39 (55%)had mononeuropathies. Carpal tunnel syndromewas particularly common, as 31 (79% of mononeu-ropathies and 7.1% of all gastric bypass patients)presented with median mononeuropathy at thewrist. Less common syndromes included 2 patientswith ulnar neuropathy at the elbow, 1 with radialmononeuropathy, 1 with superficial radial sensoryneuropathy, and 1 with sciatic neuropathy. Althoughnot especially common with bariatric surgeries, per-oneal neuropathy and lateral femoral cutaneousneuropathy are of particular interest.
Thaisetthawatkul et al.137 reported 2 patients(0.4%) with peroneal mononeuropathy at the fibu-lar head, and Sassaris et al.106 noted onset of footdrop 9 months following bariatric surgery. Foot drophas been implicated in dieting and malnutrition inliterature prior to the era of bariatric surgery. Otherreports117,130 identified peroneal nerve palsy follow-ing weight reduction; micronutrient deficiencieswere not excluded as a contributory cause. Denny-Brown36 estimated that a transient foot drop devel-oped during captivity in approximately 10% ofWorld War II prisoners of war suffering from severe
Obesity Surgery Complications MUSCLE & NERVE February 2006 171

and prolonged malnutrition; no cause was ever de-termined.
Following gastric bypass, the incidence of lateralfemoral cutaneous neuropathy is approximately 0.5%–1.4%.1,75,137 The etiology remains elusive. Compressionby the Gomez retractor at the hip was considered alikely cause by Grace.49 However, MacGregor andThoburn75 reported 11 cases of meralgia paresthetica,most beginning shortly after surgery (Roux-en-Y gastricbypass or silicon ring vertical gastroplasty), despite us-ing an upper midline incision with an “upper hand”retractor above the level of the shoulders to avoidpressure at the hips (MacGregor, personal communi-cation). MacGregor and Thoburn75 speculated thatcertain anatomic variants of the lateral femoral cutane-ous nerve44 may predispose the nerve to compression.
Muscle. Weakness was reported in 25 of 96 patientsin case reports. Thiamine deficiency accounted forsome cases. Of the remaining case reports of weak-ness or myopathy, 7 were attributed to primary mus-cle disease (Table 1); among surgical series, therewas one report each of a myotonic syndrome1 andhypokalemic paralysis.126 Another surgical seriesnoted rhabdomyolysis in 1.4% of cases,66 and sug-gested that this may be an underestimate. Mognol etal.85 prospectively followed serum creatine kinase(CK) levels before and after operation and definedrhabdomyolysis as CK �1050 U/L; myoglobin levelswere not evaluated. By this definition, the rate ofrhabdomyolysis was as high as 22% of patients un-dergoing laparoscopic bariatric surgery,85 althoughthis is likely an overestimate since serum CK may alsobe elevated because of surgery.
In a series of 30 patients with osteomalacia,123
weakness was the presenting symptom in 30%; 97%were weak on examination, and 83% had electro-myographic findings of reduced motor unit actionpotential (MUAP) duration and amplitude withoutabnormal spontaneous activity, suggesting a myo-pathic pattern. Muscle biopsy demonstrated type 2atrophy, enlarged interfibrillar spaces, fat infiltra-tion, fibrosis, and glycogen granules.123,149 One re-port attributed myopathy following Roux-en-Y gas-tric bypass to global malnutrition.64 Myopathy mayalso be associated with vitamin D or E deficiencies.
EVALUATION AND MANAGEMENT
Electrodiagnosis. Electromyography and nerve con-duction study have been underutilized in the diag-nosis of these presentations, as only 36 (38%) of 96patients in case reports included electrodiagnosticdata, the majority in a single prospective study.1
Electrophysiologic findings from 25 patients in thecontrolled retrospective study done by Thaisettha-watkul et al.137 demonstrated moderate to severelarge-fiber neuropathy in 11, mild peripheral neu-ropathy in 8, and normal studies in 6 (who hadclinical evidence of small-fiber neuropathy). Thesedata provide insight into the sensitivity of electrodi-agnostic evaluation, as 19 of 25 patients (76%) withclinical signs of peripheral neuropathy had abnor-mal studies.137 Normal findings are more likely whensmall or unmyelinated axons are involved. Among 24of 42 partially gastrectomized patients with low se-rum vitamin B12, electrodiagnostic evidence of poly-neuropathy was seen in only 3,103 which may suggesta preferential effect on unmyelinated or small fibers,or on other parts of the nervous system. The sensi-tivity of special testing appears higher; quantitativeautonomic testing was abnormal for 2 of 7 patients,thermoregulatory sweat testing was abnormal in 4 of4, and quantitative sensory testing (all fiber classes)was abnormal in 4 of 4 patients.137 However, thereare insufficient published data characterizing neu-ropathies and myopathies after bariatric surgery foranalysis of sensitivity or specificity. Electrodiagnostictesting is critical for localization and diagnosis, andto exclude potential neurologic emergencies such asGuillain–Barre syndrome.26
Tissue or biopsy specimens were obtained fromonly 7 patients (7%) in the case reports, and severalof these were at autopsy. Sural nerve biopsy findingswere reported from 5 patients among the surgicalseries, 4 with polyneuropathy and 1 with radiculo-plexopathy; findings included prominent active ax-onal degeneration, and one biopsy had multifocalfiber degeneration. All had mononuclear inflamma-tory cell involvement of the epineurium and endo-neurium, and small or moderate perivascular inflam-matory mononuclear cells were also seen, suggestinga role for inflammation or an immunologic mecha-nism.137 Postmortem examination following gastricpartitioning suggested marked fat catabolism asmanifested by lipid droplet and lipofuscin deposi-tion in anterior horn cells, in the cytoplasm ofSchwann cells, and in macrophages of the brachialplexus.40
Tissue diagnosis, especially muscle biopsy, shouldbe considered for the same reasons as electrodiag-nostic studies. Many of these patients are at risk forneuropathy, myopathy, or both, and alternate causesof weakness (idiopathic inflammatory myopathy,critical illness myopathy) should be excluded. Giventhe low sensitivity of electrodiagnostic testing andmuscle or nerve biopsy for detecting small-fiber neu-ropathies, skin biopsy may be particularly helpful in
172 Obesity Surgery Complications MUSCLE & NERVE February 2006

patients with presumed small-fiber neuropathy orburning feet syndrome.65
Time Course of Presentation. Early or immediate po-tential complications include rhabdomyolysis andmeralgia paresthetica. Rhabdomyolysis has been as-sociated with prolonged operations and immobility;protective padding has been advocated.66 Since lat-eral femoral cutaneous neuropathy may not be re-lated to surgical technique,75 there is no clear strat-egy for prevention, and further research is necessaryto define the mechanism of injury.
Nearly half of metabolic and nutritional deficien-cies occur within the first year following Roux-en-Ygastric bypass.17 Wernicke’s encephalopathy andneuropathy associated with thiamine deficiency maypresent more acutely, beginning days to weeks afterprolonged emesis. However, nutritional polyneurop-athies or myopathies may occur months or yearslater. Due to its long half-life and enterohepaticcirculation, signs of vitamin B12 deficiency may occuryears after bariatric surgery. Neurological signs ofvitamin E deficiency from malabsorption may notappear for 5–10 years in adults.132 It may be difficultto determine whether a lesion is due to a singlevitamin deficiency or multiple deficiencies.36,78
Thus, burning feet syndrome has been attributed todeficiencies of multiple vitamins78 as well as to singlevitamins such as thiamine78 or folate.12
Micronutrient Monitoring and Supplementation. Bro-lin16 recommended monitoring complete bloodcount, serum iron, total iron-binding capacity, andserum vitamin B12 following Roux-en-Y gastric by-pass. Checking serum CK in the immediate postop-erative period is also advisable to detect rhabdomy-olysis in the clinical context of pain, weakness, andskeletal muscle swelling with myoglobin-uria.32,66,85,147 Since increased serum CK levels mayoccur as a result of surgery, elevations in the absenceof this syndrome may not be clinically relevant. Fol-lowing gastric bypass, Crowley and colleagues34 ad-vocated long-term follow-up, dietary counseling,clinical and laboratory evaluations every 6 months toinclude complete blood count, urinalysis, serumiron, total iron-binding capacity, serum vitamin B12,folic acid, and a chemistry profile that includes cal-cium, phosphorus, and alkaline phosphatase. Theyalso recommended indefinite use of the followingsupplements: a multivitamin-mineral containing vi-tamin B12, folic acid, and iron; an additional irontablet with vitamin C; an additional 50–100-�g vita-min B12 tablet; and a calcium supplement of 1000–1200 mg daily.23,34 Boylan et al.13 found that plasma
levels of vitamins B6, B12, E, and folate correlatedwith vitamin supplement intake in gastric bypass pa-tients, and also recommended use of a multivitamin-multimineral supplement providing U.S. RDA quan-tities daily. Although there is some disagreementabout whether all patients should receive oral vita-min B12 supplementation following surgery, there isconsensus about most of these recommendations.23
CONCLUSIONS
Thorough neurologic evaluation is essential for anypatient with neurologic symptoms after bariatricsurgery. We recommend obtaining levels of micro-nutrients (vitamins B6, B12, D, E, folate, calcium,magnesium, phosphorus, selenium, and copper),electrodiagnostic studies, biopsy, and empiric ther-apy (e.g., thiamine, vitamin B12, or multivitamins)after a careful search for a specific underlying cause.With the increasing popularity of bariatric surgery,clinicians will need to recognize and manage neuro-logic complications that may appear after an intervalof years to decades.
Prevention of compression injuries and rhabdo-myolysis begins in the operating room with attentionto patient positioning and the duration of immobil-ity during surgery.32,66 Routine monitoring of se-lected micronutrients and minerals (vitamins B6,B12, D, E, folate, iron, thiamine, and calcium) every6 months after surgery may detect deficiencies be-fore they become symptomatic, and vitamin/mineralsupplementation at least at the U.S. RDA level arelikely cost-effective in preventing neurologic compli-cations, although further studies of this premise areneeded.
REFERENCES
1. Abarbanel JM, Berginer VM, Osimani A, Solomon H, Cha-ruzi I. Neurologic complications after gastric restriction sur-gery for morbid obesity. Neurology 1987;37:196–200.
2. Akhtar M, Collins MP, Kissel JT. Acute postgastric reductionsurgery (APGARS) neuropathy: a polynutritional, multisys-tem disorder. Neurology 2002;58:A68.
3. Albina JE, Stone WM, Bates M, Felder ME. Catastrophicweight loss after vertical banded gastroplasty: malnutritionand neurologic alterations. J Parenter Enteral Nutr 1988;12:619–620.
4. Alden JF. Gastric and jejunoileal bypass. A comparison in thetreatment of morbid obesity. Arch Surg 1977;112:799–806.
5. Allison DB, Fontaine KR, Manson JE, Stevens J, VanItallieTB. Annual deaths attributable to obesity in the UnitedStates. JAMA 1999;282:1530–1538.
6. Alt SJ. Bariatric surgery programs growing quickly nation-wide. Health Care Strateg Manag 2001;19:17–23.
7. Amaral JF, Thompson WR, Caldwell MD, Martin HF, RandallHT. Prospective hematologic evaluation of gastric exclusionsurgery for morbid obesity. Ann Surg 1985;201:186–193.
Obesity Surgery Complications MUSCLE & NERVE February 2006 173

8. Bajardi G, Ricevuto G, Mastrandrea G, Branca M, RinaudoG, Cali F, et al. Surgical treatment of morbid obesity withbiliopancreatic diversion and gastric banding: report on an8-year experience involving 235 cases. Ann Chir 2000;125:155–162.
9. Balsiger BM, Murr MM, Poggio JL, Sarr MG. Bariatric sur-gery. Surgery for weight control in patients with morbidobesity. Med Clin N Am 2000;84:477–489.
10. Banerji NK, Hurwitz LJ. Nervous system manifestations aftergastric surgery. Acta Neurol Scand 1971;47:485–513.
11. Benotti PN. Surgery in the management of severe obesity. In:Goldstein DJ, editor. The management of eating disordersand obesity. Totowa, NJ: Humana Press; 1999. p 273–284.
12. Botez MI, Botez T, Leveile J, Bielmann P, Cadote M. Neu-ropsychological correlates of folic acid deficiency: facts andhypotheses. In: Botez MI, Reynolds EH, editors. Folic acid inneurology, psychiatry, and internal medicine. New York:Raven Press; 1979. p 435–461.
13. Boylan LM, Sugerman HJ, Driskell JA. Vitamin E, vitamin B6,vitamin B12, and folate status of gastric bypass surgery pa-tients. J Am Diet Assoc 1988;88:579–585.
14. Bozbora A, Coskun H, Ozarmagan S, Erbil Y, Ozbey N,Orham Y. A rare complication of adjustable gastric banding:Wernicke’s encephalopathy. Obes Surg 2000;10:274–275.
15. Bradley JE, Brown RO, Luther RW. Multiple nutritionaldeficiencies and metabolic complications 20 years after jeju-noileal bypass surgery. J Parenter Enteral Nutr 1987;11:494–498.
16. Brolin RE. Gastric bypass. Surg Clin N Am 2001;81:1077–1095.
17. Brolin RE, Gorman JH, Gorman RC, Petschenik AJ, BradleyLJ, Kenler HA, et al. Are vitamin B12 and folate deficiencyclinically important after Roux-en-Y gastric bypass? J Gastro-intest Surg 1998;2:436–442.
18. Brown GC, Felton SM, Benson WE. Reversible night blind-ness associated with intestinal bypass surgery. Am J Ophthal-mol 1980;89:776–779.
19. Buchwald H. Overview of bariatric surgery. J Am Coll Surg2002;194:367–375.
20. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W,Fahrbach K, et al. Bariatric surgery: a systematic review andmeta-analysis. JAMA 2004;292:1724–1737.
21. Buckwalter JA, Herbst CA Jr. Complications of gastric bypassfor morbid obesity. Am J Surg 1980;139:55–60.
22. Burge JC, Schaumburg JZ, Choban PS, DiSilvestro RA,Flancbaum L. Changes in patients’ taste acuity after Roux-en-Y gastric bypass for clinically severe obesity. J Am DietAssoc 1995;95:666–670.
23. Byrne TK. Complications of surgery for obesity. Surg Clin NAm 2001;81:1181–1193.
24. Callender ST, Witts LJ, Allison PR, Gunning A. Some meta-bolic and haematological effects of oesophagojejunostomywith by-pass of the stomach. Gut 1961;2:150–157.
25. Chang CG, Adams-Huet B, Provost DA. Acute post-gastricreduction surgery (APGARS) neuropathy. Obes Surg 2004;14:182–189.
26. Chang CG, Helling TS, Black WE, Rymer MM. Weaknessafter gastric bypass. Obes Surg 2002;12:592–597.
27. Chaudhry V, Umapathi T, Ravich WJ. Neuromuscular dis-eases and disorders of the alimentary system. Muscle Nerve2002;25:768–784.
28. Chaves LC, Faintuch J, Kahwage S, Alencar FA. A cluster ofpolyneuropathy and Wernicke–Korsakoff syndrome in abariatric unit. Obes Surg 2002;12:328–334.
29. Christodoulakis M, Maris T, Plaitakis A, Melissas J. Wer-nicke’s encephalopathy after vertical banded gastroplasty formorbid obesity. Eur J Surg 1997;163:473–474.
30. Ciongoli AK, Poser CM. Fat malabsorption neuromyopathy.Arch Neurol 1972;26:403–408.
31. Cirignotta F, Manconi M, Mondini S, Buzzi G, Ambrosetto P.Wernicke–Korsakoff encephalopathy and polyneuropathy
after gastroplasty for morbid obesity: report of a case. ArchNeurol 2000;57:1356–1359.
32. Collier B, Goreja MA, Duke BE III. Postoperative rhabdomy-olysis with bariatric surgery. Obes Surg 2003;13:941–943.
33. Crowley LV, Olson RW. Megaloblastic anemia after gastricbypass for obesity. Am J Gastroenterol 1983;78: 406–410.
34. Crowley LV, Seay J, Mullin G. Late effects of gastric bypassfor obesity. Am J Gastroenterol 1984;79:850–860.
35. Das KC, Herbert V. Vitamin B12–folate interrelations. ClinHaematol 1976;5:697–745.
36. Denny-Brown D. Neurological conditions resulting fromprolonged and severe dietary restriction. Medicine 1947;26:41–113.
37. Dreyfus PM, Victor M. Effects of thiamine deficiency on thecentral nervous system. Am J Clin Nutr 1961;9:414–425.
38. Farmer CE, Campbell JB. Treatment of 300 consecutivemorbid obesity patients with gastric bypass. J Miss State MedAssoc 1984;25:321–323.
39. Fawcett S, Young GB, Holliday RL. Wernicke’s encephalop-athy after gastric partitioning for morbid obesity. Can J Surg1984;27:169–170.
40. Feit H, Glasberg M, Ireton C, Rosenberg RN, Thal E. Pe-ripheral neuropathy and starvation after gastric partitioningfor morbid obesity. Ann Intern Med 1982;96:453–455.
41. Feit H, Glasberg MR. Neurologic complications of gastricpartitioning. Arch Neurol 1986;43:642.
42. Felder ME, Amaral JF. Gastric surgery for morbid obesity:experience with 72 consecutive patients. RI Med J 1981;64:355–359.
43. Gardner TW, Rao K, Poticha S, Wertz R. Acute visual lossafter gastroplasty. Am J Ophthalmol 1982;93:658–660.
44. Ghent WR. Further studies on meralgia paresthetica. CanMed Assoc J 1961;85:871–875.
45. Glad BW, Hodges RE, Michas CA, Moussavian SN, Righi SP.Atrophic beriberi. A complication of jejunoileal bypass sur-gery for morbid obesity. Am J Med 1978;65:69–74.
46. Gloth FM III, Lindsay JM, Zelesnick LB, Greenough WB III.Can vitamin D deficiency produce an unusual pain syn-drome? Arch Intern Med 1991;151:1662–1664.
47. Gollobin C, Marcus WY. Bariatric beriberi. Obes Surg 2002;12:309–311.
48. Gorecki PJ, Cottam D, Ger R, Angus LDG, Shaftan GW.Lower extremity compartment syndrome following a laparo-scopic Roux-en-Y gastric bypass. Obes Surg 2002;12:289–291.
49. Grace DM. Meralgia paresthetica after gastroplasty for mor-bid obesity. Can J Surg 1987;30:64–65.
50. Grace DM, Alfieri MA, Leung FY. Alcohol and poor compli-ance as factors in Wernicke’s encephalopathy diagnosed 13years after gastric bypass. Can J Surg 1998;41:389–392.
51. Grant HC, Hoffbrand AV, Wells DG. Folate deficiency andneurological disease. Lancet 1965;2:763–767.
52. Griffen WO Jr, Young VL, Stevenson CC. A prospectivecomparison of gastric and jejunoileal bypass procedures formorbid obesity. Ann Surg 1977;186:500–509.
53. Guggenheim MA, Ringel SP, Silverman A, Grabert BE, Nev-ille HE. Progressive neuromuscular disease in children withchronic cholestasis and vitamin E deficiency: clinical andmuscle biopsy findings and treatment with alpha-tocopherol.Ann NY Acad Sci 1982;393:84–95.
54. Haag JR, Smith JL, Susac JO. Optic atrophy following jeju-noileal bypass. J Clin Neuroophthalmol 1985;5:9–15.
55. Haid RW, Gutmann L, Crosby TW. Wernicke–Korsakoff en-cephalopathy after gastric plication. JAMA 1982;247:2566–2567.
56. Halverson JD. Micronutrient deficiencies after gastric bypassfor morbid obesity. Am Surg 1986;52:594–598.
57. Halverson JD, Zuckerman GR, Koehler RE, Gentry K, Mi-chael HE, DeSchryver-Kecskemeti K. Gastric bypass for mor-bid obesity: a medical–surgical assessment. Ann Surg 1981;194:152–160.
174 Obesity Surgery Complications MUSCLE & NERVE February 2006
58. Harwood SC, Chodoroff G, Ellenberg MR. Gastric partition-ing complicated by peripheral neuropathy with lumbosacralplexopathy. Arch Phys Med Rehabil 1987;68:310–312.
59. Healton EB, Savage DG, Brust JC, Garrett TJ, LindenbaumJ. Neurologic aspects of cobalamin deficiency. Medicine(Baltimore) 1991;70:229–245.
60. Herbert VD, Colman N. Folic acid and vitamin B12. In: ShilsME, Young VR, editors. Modern nutrition in health anddisease. Philadelphia: Lea & Febiger; 1988. p 388–416.
61. Higa KD, Boone KB, Ho T, Davies OG. Laparoscopic Roux-en-Y gastric bypass for morbid obesity: technique and pre-liminary results of our first 400 patients. Arch Surg 2000;135:1029–1033.
62. Hill JO, Goldberg JP, Pate RR, Peters JC. Introduction. NutrRev 2001;59(suppl):S4–S6.
63. Hornberger HR. Gastric bypass. Am J Surg 1976;131:415–418.
64. Hsia AW, Hattab EM, Katz JS. Malnutrition-induced myop-athy following Roux-en-Y gastric bypass. Muscle Nerve 2001;24:1692–1694.
65. Kennedy WR. Opportunities afforded by the study of unmy-elinated nerves in skin and other organs. Muscle Nerve2004;29:756–767.
66. Khurana RN, Baudendistel TE, Morgan EF, Rabkin RA,Elkin RB, Aalami OO. Postoperative rhabdomyolysis follow-ing laparoscopic gastric bypass in the morbidly obese. ArchSurg 2004;139:73–76.
67. Kral JG. Morbidity of severe obesity. Surg Clin N Am 2001;81:1039–1061.
68. Kramer LD, Locke GE. Wernicke’s encephalopathy. Compli-cation of gastric plication. J Clin Gastroenterol 1987;9:549–552.
69. Kumar N, McEvoy KM, Ahlskog JE. Myelopathy due to cop-per deficiency following gastrointestinal surgery. Arch Neu-rol 2003;60:1782–1785.
70. Kushner R. Managing the obese patient after bariatric sur-gery: a case report of severe malnutrition and review of theliterature. J Parenter Enteral Nutr 2000;24:126–132.
71. Levander OA. Clinical consequences of low selenium intakeand its relationship to vitamin E. Ann NY Acad Sci 1982;393:70–82.
72. Lindenbaum J, Healton EB, Savage DG, Brust JC, Garrett TJ,Podell ER, et al. Neuropsychiatric disorders caused by cobal-amin deficiency in the absence of anemia or macrocytosis.N Engl J Med 1988;318:1720–1728.
73. Loh Y, Watson WD, Verma A, Chang ST, Stocker DJ, LabuttaRJ. Acute Wernicke’s encephalopathy following bariatric sur-gery: clinical course and MRI correlation. Obes Surg 2004;14:129–132.
74. MacGregor AM, Rand CS. Gastric surgery in morbid obesity.Outcome in patients aged 55 years and older. Arch Surg1993;128:1153–1157.
75. MacGregor AM, Thoburn EK. Meralgia paresthetica follow-ing bariatric surgery. Obes Surg 1999;9:364–368.
76. MacLean JB. Wernicke’s encephalopathy after gastric plica-tion. JAMA 1982;248:1311.
77. MacLean LD, Rhode BM, Shizgal HM. Nutrition followinggastric operations for morbid obesity. Ann Surg 1983;198:347–355.
78. Mancall EL. Nutritional disorders of the nervous system. In:Aminoff MJ, editor. Neurology and general medicine. NewYork: Churchill Livingstone; 1989. p 323–339.
79. Marceau P, Hould FS, Simard S, Lebel S, Bourque RA,Potvin M, et al. Biliopancreatic diversion with duodenalswitch. World J Surg 1998;22:947–954.
80. Maryniak O. Severe peripheral neuropathy following gastricbypass surgery for morbid obesity. Can Med Assoc J 1984;131:119–120.
81. Mason EE. Vertical banded gastroplasty for obesity. ArchSurg 1982;117:701–706.
82. Mason EE. Notice. International Bariatric Surgery RegistryNewsletter 2001. IBSR Newsletter 2001;16. Available at:
http://www.surgery.uiowa.edu/ibsr/winter01.htm (last ac-cessed April 28, 2005).
83. Mason EE, Ito C. Gastric bypass. Ann Surg 1969;170:329–339.
84. Milius G, Rose S, Owen DR, Schenken JR. Probable acutethiamine deficiency secondary to gastric partition for mor-bid obesity. Nebr Med J 1982;67:147–150.
85. Mognol P, Vignes S, Chosidow D, Marmuse JP. Rhabdomy-olysis after laparoscopic bariatric surgery. Obes Surg 2004;14:91–94.
86. Murata K. Thiaminase. In: Shimazono N, Katsura E, editors.Review of Japanese literature on beriberi and thiamine.Tokyo: Igaku Shoin; 1965. p 220–254.
87. Murr MM, Balsiger BM, Kennedy FP, Mai JL, Sarr MG.Malabsorptive procedures for severe obesity: comparison ofpancreaticobiliary bypass and very very long limb Roux-en-Ygastric bypass. J Gastrointest Surg 1999;3:607–612.
88. Must A, Spadano J, Coakley EH, Field AE, Colditz G, DietzWH. The disease burden associated with overweight andobesity. JAMA 1999;282:1523–1529.
89. Nelson J. Neuropathological studies of chronic vitamin Edeficiency in mammals including humans. In: Porter R,Whelan J, editors. Biology of vitamin E. London: Pitman;1983. p 92–105.
90. Neville HE, Ringel SP, Guggenheim MA, Wehling CA,Starcevich JM. Ultrastructural and histochemical abnormal-ities of skeletal muscle in patients with chronic vitamin Edeficiency. Neurology 1983;33:483–488.
91. Oczkowski WJ, Kertesz A. Wernicke’s encephalopathy aftergastroplasty for morbid obesity. Neurology 1985;35:99–101.
92. Parry TE. Folate responsive neuropathy. Presse Med 1994;23:131–137.
93. Partamian LG, Sidrys LA, Tripathi RC. Iatrogenic nightblindness and keratoconjunctival xerosis. N Engl J Med1979;301:943–944.
94. Payne JH, DeWind LT. Surgical treatment of obesity. Am JSurg 1969;118:141–147.
95. Peltier G, Hermreck AS, Moffat RE, Hardin CA, Jewell WR.Complications following gastric bypass procedures for mor-bid obesity. Surgery 1979;86:648–654.
96. Pfeifer M, Begerow B, Minne HW. Vitamin D and musclefunction. Osteoporos Int 2002;13:187–194.
97. Plotnikoff GA, Quigley JM. Prevalence of severe hypovita-minosis D in patients with persistent, nonspecific musculo-skeletal pain. Mayo Clin Proc 2003;78:1463–1470.
98. Primavera A, Brusa G, Novello P, Schenone A, Gianetta E,Marinari G, et al. Wernicke–Korsakoff encephalopathy fol-lowing biliopancreatic diversion. Obes Surg 1993;3:175–177.
99. Printen KJ, Mason EE. Peripheral neuropathy following gas-tric bypass for the treatment of morbid obesity. Obesity/Bariatric Med 1977;6:185–187.
100. Provenzale D, Reinhold RB, Golner B, Irwin V, Dallal GE,Papathanasopoulos N, et al. Evidence for diminished B12absorption after gastric bypass: oral supplementation doesnot prevent low plasma B12 levels in bypass patients. J AmColl Nutr 1992;11:29–35.
101. Rindi G, Ventura U. Thiamine intestinal transport. PhysiolRev 1972;52:821–827.
102. Ronin DI, Wu YC, Sahgal V, MacLean IC. Intractable musclepain syndrome, osteomalacia, and axonopathy in long-termuse of phenytoin. Arch Phys Med Rehabil 1991;72:755–758.
103. Roos D. Neurological complications in patients with im-paired vitamin B12 absorption following partial gastrectomy.Acta Neurol Scand 1978;69(suppl):1–77.
104. Rothrock JF, Smith MS. Wernicke’s disease complicatingsurgical therapy for morbid obesity. J Clin Neuroophthalmol1981;1:195–199.
105. Salas-Salvado J, Garcia-Lorda P, Cuatrecasas G, Bonada A,Formiguera X, Del Castillo D, et al. Wernicke’s syndromeafter bariatric surgery. Clin Nutr 2000;19:371–373.
Obesity Surgery Complications MUSCLE & NERVE February 2006 175

106. Sassaris M, Meka R, Miletello G, Nance C, Hunter FM.Neuropsychiatric syndromes after gastric partition. Am JGastroenterol 1983;78:321–323.
107. Scheuller M, Weider D. Bariatric surgery for treatment ofsleep apnea syndrome in 15 morbidly obese patients: long-term results. Otolaryngol Head Neck Surg 2001;125:299–302.
108. Schilling RF, Gohdes PN, Hardie GH. Vitamin B12 deficiencyafter gastric bypass surgery for obesity. Ann Intern Med1984;101:501–502.
109. Schleper B, Stuerenburg HJ. Copper deficiency-associatedmyelopathy in a 46-year-old woman. J Neurol 2001;248:705–706.
110. Schlosser LL, Deshpande P, Schilling RF. Biologic turnoverrate of cyanocobalamin (vitamin B12) in human liver. ArchIntern Med 1958;101:306–309.
111. Schott GD, Wills MR. Muscle weakness in osteomalacia. Lan-cet 1976;i:626–629.
112. Scobie IN, Durward WF, MacCuish AC. Proximal myopathyafter prolonged total therapeutic starvation. Br Med J 1980;280:1212–1213.
113. Scopinaro N, Gianetta E, Adami GF, Friedman D, TraversoE, Marinari GM, et al. Biliopancreatic diversion for obesity ateighteen years. Surgery 1996;119:261–268.
114. Scott HW Jr, Sandstead HH, Brill AB, Burko H, Younger RK.Experience with a new technique of intestinal bypass in thetreatment of morbid obesity. Ann Surg 1971;174:560–572.
115. Seehra H, MacDermott N, Lascelles RG, Taylor TV. Wer-nicke’s encephalopathy after vertical banded gastroplasty formorbid obesity. Br Med J 1996;312:434.
116. Shamberger RJ. Selenium in the environment. Sci TotalEnviron 1981;17:59–74.
117. Sherman DG, Easton JD. Dieting and peroneal nerve palsy.JAMA 1977;238:230–231.
118. Shimomura T, Mori E, Hirono N, Imamura T, Yamashita H.Development of Wernicke–Korsakoff syndrome after longintervals following gastrectomy. Arch Neurol 1998;55:1242–1245.
119. Shinkman R. Battle for the bulge: bariatric surgery a steadilyincreasing revenue stream. Healthcare Leadership ManagRep 2003;11:1, 8, 10–13.
120. Shorvon SD, Carney MW, Chanarin I, Reynolds EH. Theneuropsychiatry of megaloblastic anaemia. Br Med J 1980;281:1036–1038.
121. Sjostrom CD, Lissner L, Wedel H, Sjostrom L. Reduction inincidence of diabetes, hypertension and lipid disturbancesafter intentional weight loss induced by bariatric surgery: theSOS Intervention Study. Obes Res 1999;7:477–484.
122. Sjostrom L. Surgical intervention as a strategy for treatmentof obesity. Endocrine 2000;13:213–230.
123. Skaria J, Katiyar BC, Srivastava TP, Dube B. Myopathy andneuropathy associated with osteomalacia. Acta Neurol Scand1975;51:37–58.
124. Skroubis G, Sakellaropoulos G, Pouggouras K, Mead N,Nikiforidis G, Kalfarentzos F. Comparison of nutritional de-ficiencies after Roux-en-Y gastric bypass and after biliopan-creatic diversion with Roux-en-Y gastric bypass. Obes Surg2002;12:551–558.
125. Smets RM, Waeben M. Unusual combination of night blind-ness and optic neuropathy after biliopancreatic bypass. BullSoc Belg Ophtalmol 1999;271:93–96.
126. Smith SC, Goodman GN, Edwards CB. Roux-en-Y gastricbypass: a 7-year retrospective review of 3,855 patients. ObesSurg 1995;5:314–318.
127. Sola E, Morillas C, Garzon S, Ferrer JM, Martin J, Hernan-dez-Mijares A. Rapid onset of Wernicke’s encephalopathyfollowing gastric restrictive surgery. Obes Surg 2003;13:661–662.
128. Solomon H, Abarbanel J, Berginer VM, Ronen J, Leff S,Trostler N, et al. Neurological deficits following gastric re-striction surgery for moribd obesity. Clin Nutr 1986;15:181–184.
129. Somer H, Bergstrom L, Mustajoki P, Rovamo L. Morbidobesity, gastric plication and a severe neurological deficit.Acta Med Scand 1985;217:575–576.
130. Sprofkin BE. Peroneal paralysis; a hazard of weight reduc-tion. Arch Intern Med 1958;102:82–87.
131. Stryer L. Biochemistry. San Francisco: W.H. Freeman; 1981.132. Subcommittee on the Tenth Edition of the RDAs, Food and
Nutrition Board, Commission on Life Sciences, NationalResearch Council. Fat-soluble vitamins. In: Havel RJ, editor.Recommended dietary allowances. Washington, DC: Na-tional Academy Press; 1989. p 78–114.
133. Subcommittee on the Tenth Edition of the RDAs, Food andNutrition Board, Commission on Life Sciences, NationalResearch Council. Water-soluble vitamins. In: Havel RJ, ed-itor. Recommended dietary allowances. Washington, DC:National Academy Press; 1989. p 115–173.
134. Sugerman HJ. Preface. Surg Clin N Am 2001;81:xi–xv.135. Sugerman HJ, Felton WL III, Sismanis A, Kellum JM, De-
Maria EJ, Sugerman EL. Gastric surgery for pseudotumorcerebri associated with severe obesity. Ann Surg 1999;229:634–640.
136. Sugerman HJ, Kellum JM, DeMaria EJ. Conversion of prox-imal to distal gastric bypass for failed gastric bypass forsuperobesity. J Gastrointest Surg 1997;1:517–525.
137. Thaisetthawatkul P, Collazo-Clavell ML, Sarr MG, Norell JE,Dyck PJ. A controlled study of peripheral neuropathy afterbariatric surgery. Neurology 2004;63:1462–1470.
138. Thompson RE, Felton JL. Nutritional amblyopia associatedwith jejunoileal bypass surgery. Ann Ophthalmol 1982;14:848–850.
139. Tomasi LG. Reversibility of human myopathy caused byvitamin E deficiency. Neurology 1979;29:1182–1186.
140. Toth C, Voll C. Wernicke’s encephalopathy following gastro-plasty for morbid obesity. Can J Neurol Sci 2001;28:89–92.
141. Villar HV, Ranne RD. Neurologic deficit following gastricpartitioning: possible role of thiamine. J Parenter EnteralNutr 1984;8:575–578.
142. Vimokesant SL, Nakornchai S, Dhanamitta S, Hilker DM.Effect of tea consumption on thiamine status in man. NutrRep Int 1974;9:371–374.
143. Vyas ID, Purohit MG, Bearn AR. Reversible peripheral neu-ropathy following jejuno-ileal bypass surgery for morbid obe-sity. J R Coll Surg Edinb 1979;24:278–279.
144. Wadstrom C, Backman L. Polyneuropathy following gastricbanding for obesity. Case report. Acta Chir Scand 1989;155:131–134.
145. Walerych WS, Venkataraman S, Johnson BC. The methyl-ation of transfer RNA by methyl cobamide. Biochem BiophysRes Commun 1966;23:368–374.
146. Weir DG, Gatenby PB. Subacute combined degeneration ofthe cord after partial gastrectomy. Br Med J 1963;5366:1175–1176.
147. Wiltshire JP, Custer T. Lumbar muscle rhabdomyolysis as acause of acute renal failure after Roux-en-Y gastric bypass.Obes Surg 2003;13:306–313.
148. Yarborough GW, Wilson FA, Feman S, Charles S, Chytil F,O’Leary JP. Retinopathy following jejunoileal bypass surgery:report of a case. Int J Obes 1982;6:253–258.
149. Yoshikawa S, Nakamura T, Tanabe H, Imamura T. Osteoma-lacic myopathy. Endocrinol Jpn 1979;26:65–72.
150. Ziporin ZZ, Nunes WT, Powell RC, Waring PP, SauberlichHE. Thiamine requirement in the adult human as measuredby urinary excretion of thiamine metabolites. J Nutr 1965;85:297–304.
176 Obesity Surgery Complications MUSCLE & NERVE February 2006