Neurogenic dysphonia Neurogenic Dysphonia: Topics Neurology of the larynx Organizational Framework...
37
Neurogenic dysphonia
-
Upload
lauren-lynn-quinn -
Category
Documents
-
view
231 -
download
3
Transcript of Neurogenic dysphonia Neurogenic Dysphonia: Topics Neurology of the larynx Organizational Framework...

Neurogenic dysphonia
Neurogenic Dysphonia: Topics Neurology of the larynx Organizational Framework Selected Disorders Vocal fold paresis/paralysis Essential Tremor Spasmodic Dysphonia Selected Central Nervous System Disorders

UW-MadisonNeuro Website
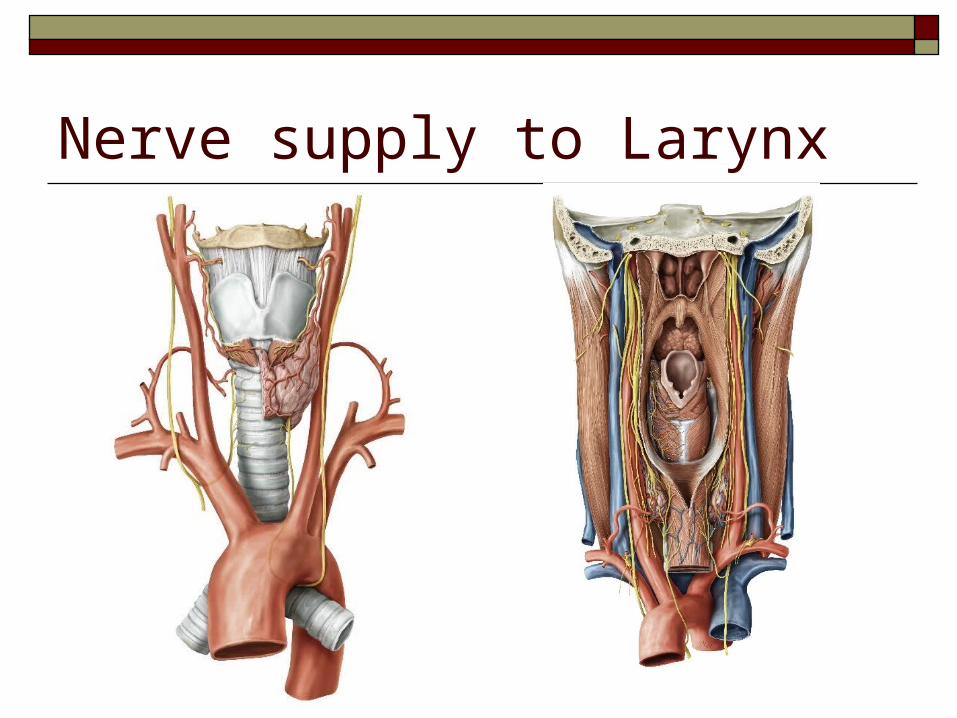
Nerve supply to Larynx

Nerve supply to Larynx
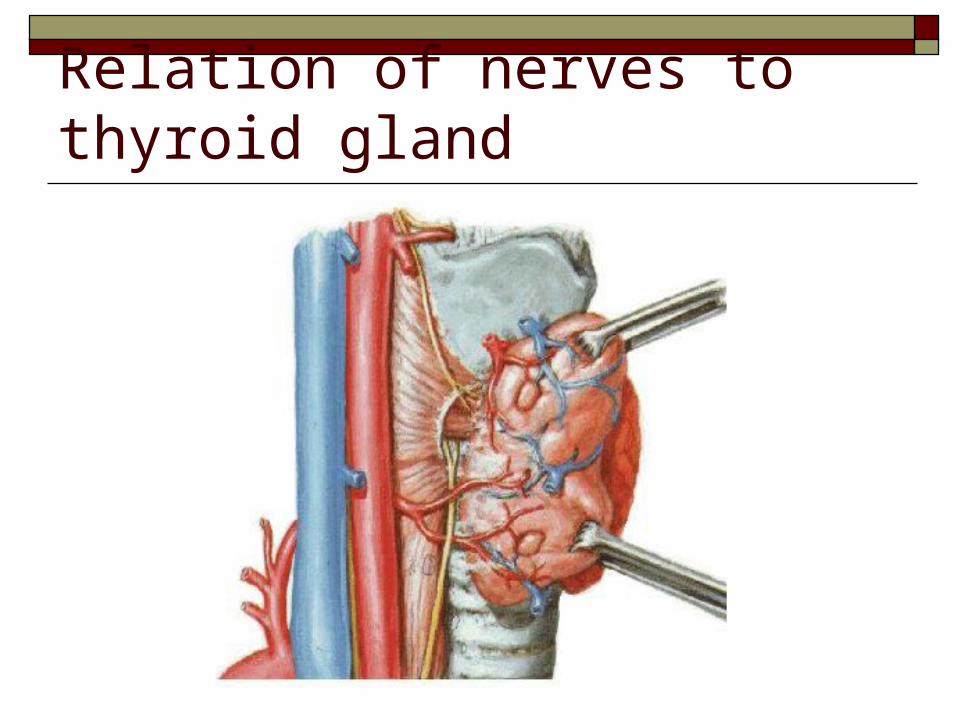
Relation of nerves to thyroid gland
Neurologic Voice Disorders: A Classification Scheme Hypoadduction Hyperadduction Phonatory Stability
Short term Long term
Phonatory Incoordination/Voiced-voiceless Mixed Miscellaneous
(Ramig & Scherer, 1992)

Vocal Fold Paresis/paralysis

Causes of vocal fold paralysis/paresisCentral Medullary lesions affecting nucleus ambiguus
Peripheral (Vagus nerve lesions) Disease (tumors of lung, esophageal, thyroid) Surgical trauma (thyroid, anterior cervical spine, lung resection, carotid
artery Sx) Nonsurgical trauma (penetrating wounds, blunt trauma) Neurological disease (Guillain-Barre, ALS) Peripheral neuropathy
Idiopathic Diagnosis of exclusion Often presumed viral

Degree of involvement
Anatomical level Pharyngeal n. Superior laryngeal n. Recurrent laryngeal n.

Degree of involvementLaterality Unilateral Bilateral
Degree of mobility Paresis
Weakness Hypomobility
Paralysis Immobility
Degree of Nerve Injury
(Rubin & Sataloff, 2007)
1°: Neurapraxia and full recovery
2°: Wallerian degeneration but full recovery
3°: Misdirected neural regeneration
4°: Scarring which may block regeneration
5°: Complete nerve transection

Breathy voice Hoarse voice Low volume Limited pitch range & pitch control problems Increased effort and frequent vocal fatigue Weak cough Aspiration of liquids during swallowing
Signs and symptoms

Vocal fold positionRecurrent laryngeal nerve Typically affects ad/abductors Paramedian position common Bilateral impairment can cause airway
problems
Superior laryngeal nerve Deceptively normal position
Superior + Recurrent laryngeal nerve Vocal fold(s) may be more abducted than in
recurrent only May affect vertical position of vocal fold
making compensation more difficult
*Reinnervation pattern will influence vocal fold position
Paramedian
Abduction
Median
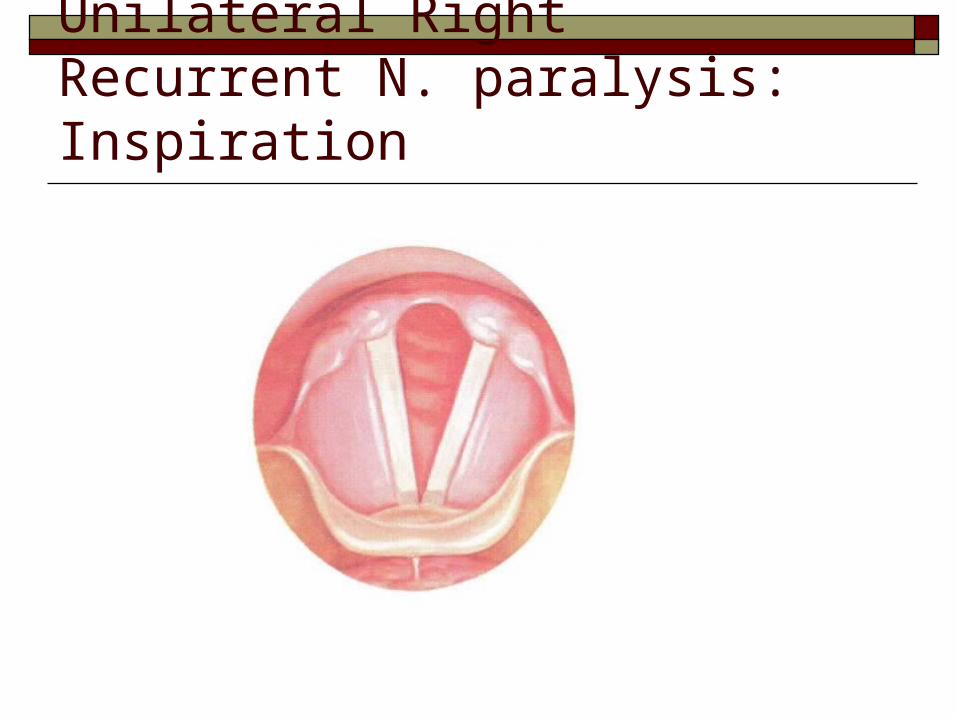
Unilateral Right Recurrent N. paralysis: Inspiration

Unilateral Right Recurrent N. paralysis: Phonation

Videoendoscopic evaluationGoals Assess vocal fold mobility Determine degree of glottic closure Relate mobility to voice production Differentiate level of involvement Identify/rule out compensatory behaviors
supraglottic compression Differentiate paresis/paralysis from CA joint
immobility*

CA joint immobility Ankylosis (fixation)/Dislocation Presumed etiology
arthritis trauma joint disease
Appearance Similar to vocal fold paralysis
Differentiating paralysis from ankylosis/dislocation Can be difficult to differentiate with indirect laryngoscopy Reduced passive mobility under direct laryngoscopy Paralysis
Mobility normal during passive movement Affected side “jostles” when contralateral arytenoid hits it
Ankylosis/dislocation Reduced mobility during passive movement Affected side does not “jostle” when contralateral arytenoid hits it

Videoendoscopic evaluationPhonatory Maneuvers Seek to isolate adductors, abductors, tensors Abduction:
sniffing/quick inhalation on/off voicing
Adduction: voicing at various levels on/off voicing Sharp cough

Videoendoscopic evaluationPhonatory Maneuvers Tensor:
glissando/pitch gliding Asymmetries often revealed during repetitive
& alternating activities

Superior laryngeal nerve damage Tricky to identify Controversial list of laryngoscopic signs
Sluggish adduction Asymmetry during glissando Laryngeal tilt toward weak side with voluntary increase in pitch Posterior commissure rotates toward weak side Obliquely shaped glottis due to rotation Lower vocal fold height on involved side Bowed, thin and shortened vocal fold Recent evidence: “movement” of petiole of epiglottis toward
affected side during phonation

Video Examples

Diagnosis: Additional tests Electromyography (EMG)

Treatment Issues Voice Quality Aspiration Airway

Treatment Behavioral Surgical
Recovery can occur up to 6-12 months post-insult
Permanent procedures need to be delayed

Behavioral Management Optimizing voice production and reduce maladaptive
behaviors Tension reduction Facilitating techniques
Treatment for “hypofunction”* Half swallow Pushing Head turn Manual compression
*need to be very careful not to create hyperfunction

Surgical Management:
Medialization procedures Reinnervation
Experimental procedures Laryngeal pacing

Surgical Management:Medialization procedures Intrafold injections Implantation (Isshiki Type I thyroplasty) Arytenoid Adduction
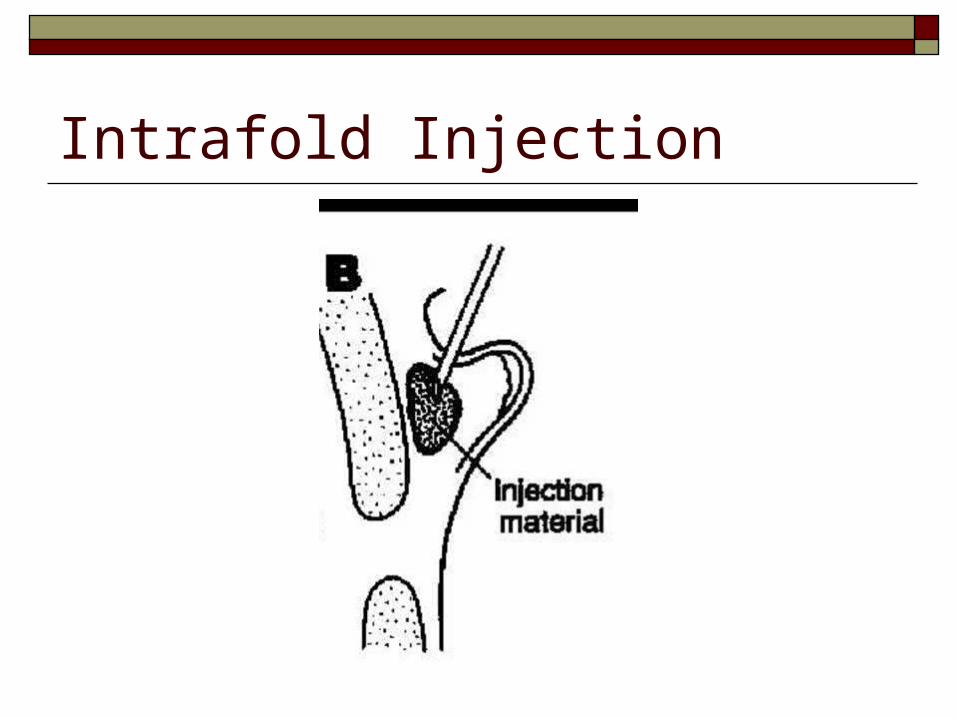
Intrafold Injection

Intrafold Injection Injection of material to increase vocal fold
bulk ~ increase glottic closure Materials include
Gelfoam (temporary) Teflon (problems with fibrosis and migration) Autologous fat (will resorb) Autologous & bovine collagen (slower to resorb) Dermis, fascia etc

Intrafold InjectionSurgical Approaches Peroral
Direct Indirect
Percutaneous (through cricothyroid space)

Implantation Placing/implanting solid material just medial
to thyroid cartilage thus pushing the vocal fold medially
Type I thyroplasty Materials include
Silicone Gore-Tex Cartilage


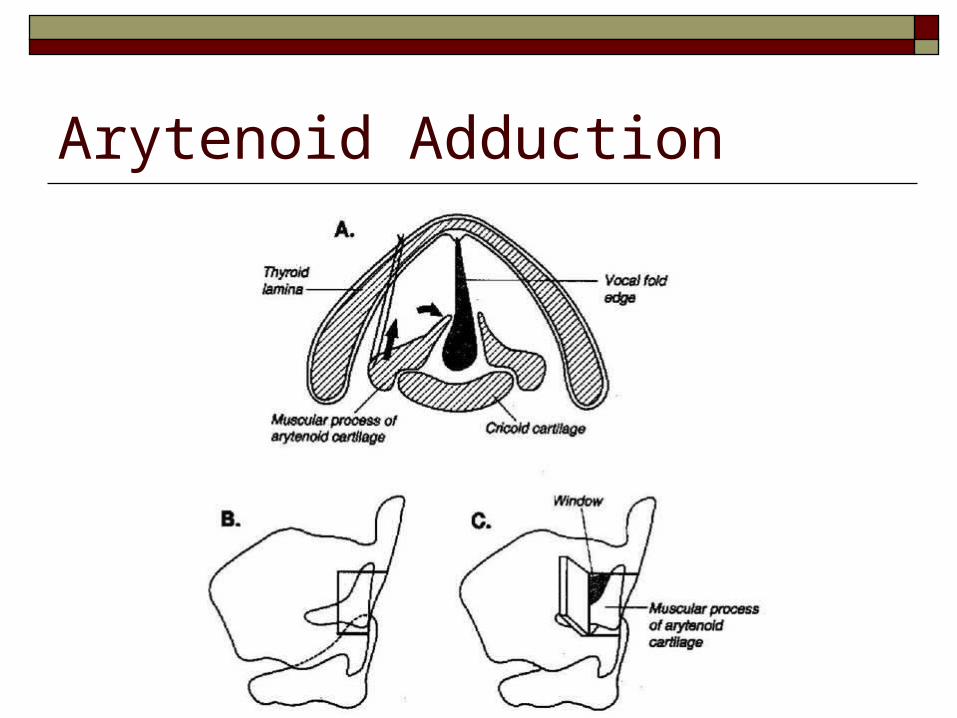
Arytenoid Adduction

Reinnervation Prevent atrophy and unfavorable
reinnervation Possibilities Ansa cervicalis phrenic n. hypoglossal n. sympathetics

Bilateral Involvement When airway problems are an issue
Options Tracheotomy Cordotomy Arytenoidectomy Thryoplasty (Lateralization) Dennervation/Reinnervation

Bilateral Involvement When airway is OK and voice is an issue
Options Medialization procedures Unilateral or bilateral