Neurofibromatosis and the spine
38
Neurofibromatosis and the spine Shekar Roopan Spinal Unit King Dinuzulu Hospital Complex
-
Upload
shekar-roopan -
Category
Health & Medicine
-
view
446 -
download
1
Transcript of Neurofibromatosis and the spine

Neurofibromatosis and
the spine
Shekar Roopan
Spinal Unit
King Dinuzulu Hospital Complex

Introduction
• Multisystem disease affecting all three germ lines
(neuroectoderm, mesoderm and endoderm)
• Four varieties exist
• Neurofibromatosis 1 (NF1) the most common
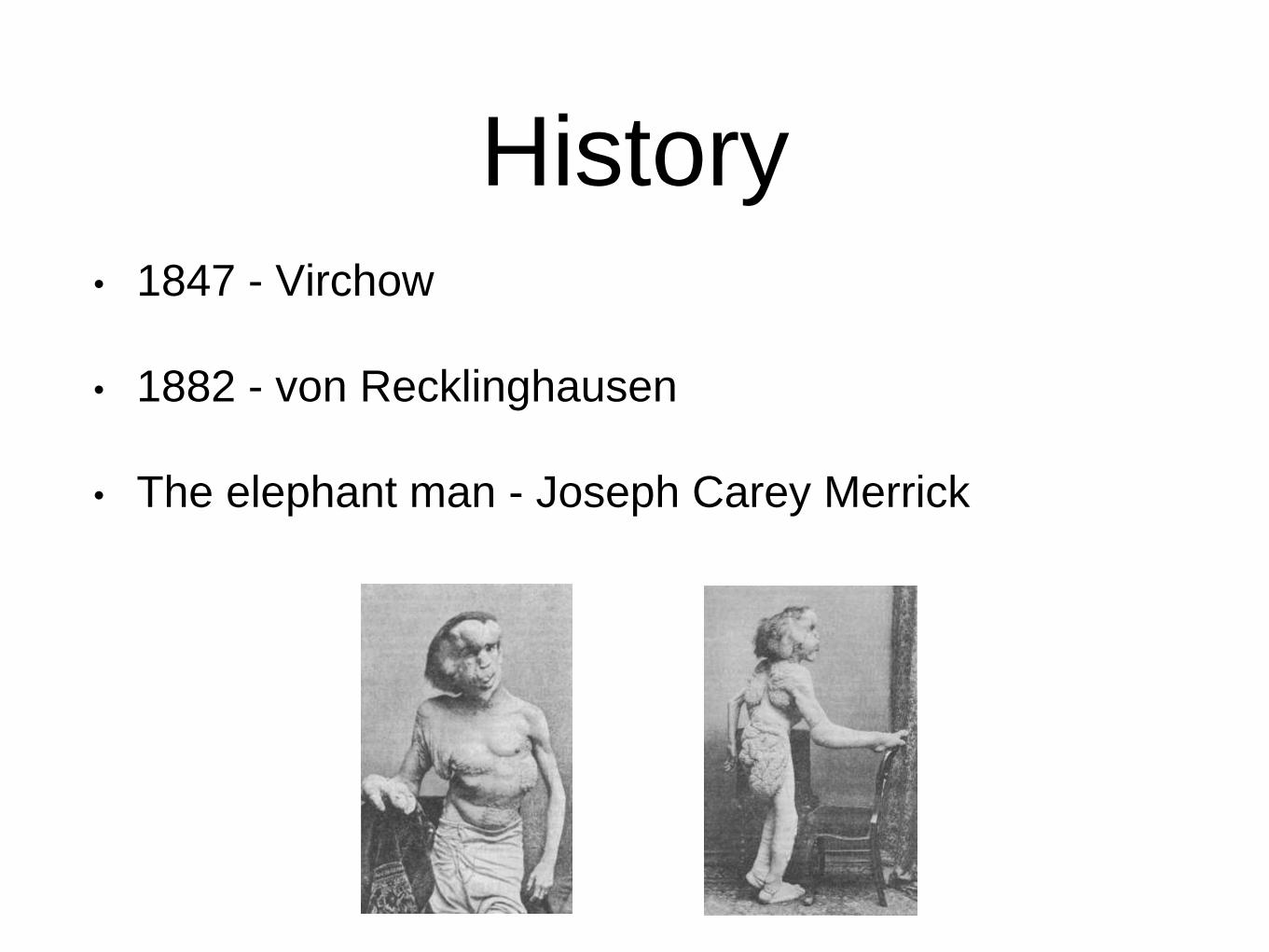
History• 1847 - Virchow
• 1882 - von Recklinghausen
• The elephant man - Joseph Carey Merrick

Classification
• Neurofibromatosis 1 - Peripheral neurofibromatosis
• Neurofibromatosis 2 - Central neurofibromatosis
• Segmental neurofibromatosis
• Schwannomatosis

Epidemiology and genetics
• Autosomal dominant
• 50% of cases spontaneous mutations
• Gene located on long arm of chromosome 17 (NF1)
• Prevalence 1:4000
• First peak - 5-10 years
• Second peak - 36-50 years (75% of clinical problems
due to malignancy)

Diagnostic Criteria
1. ≥6 cafe-au-lait spots (>5mm prepubertal, >15mm post pubertal)
2. ≥2 neurofibromas/≥1 plexiform neurofibroma
3. Axillary/inguinal freckling
4. Optic glioma
5. ≥2 Lisch nodules
6. Osseous lesion (sphenoid dysplasia/long bone cortex thinning)
7. NF1 in first degree relative
Consensus development conference of the National Institute of Health; 1987

Cafe-au-lait spots
• 90% of patients
• Melanotic in origin
• Found in skin areas not
exposed to the sun
• Under 5 years, 2 cafe au lait
spots are common and
normal
Whitehouse D; Diagnostic value of cafe-au-lait spot in children; Arch Dis Child;1966
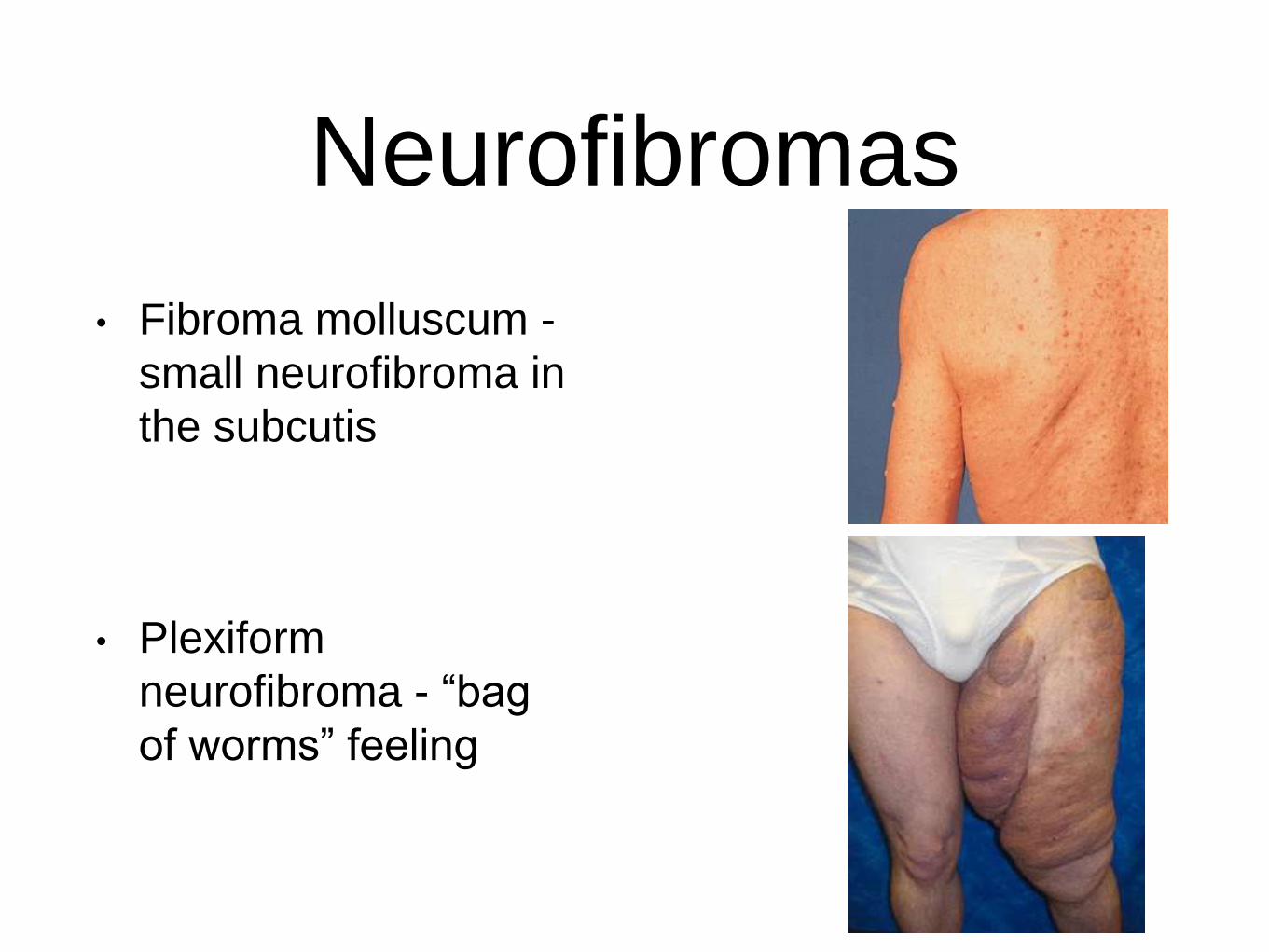
Neurofibromas
• Fibroma molluscum -
small neurofibroma in
the subcutis
• Plexiform
neurofibroma - “bag
of worms” feeling

Axillary and inguinal freckling
• diffuse, small hyper pigmented
spots (2-3mm diameter)
• 40% patients - axillary freckling

Optic Glioma
• Account for 2-5% of all brain tumours in childhood
• 70% of cases are in NF1

Lisch Nodules
• slightly raised, well
circumscribed hamartomas
on the iris
• Present in 90% of patients
>6 years
• Specific to NF1

Skeletal associations
• Generalised - osteoporosis, osteomalacia, short
stature, macrocephaly
• Focal - spinal deformities, long bone and sphenoid
wing dysplasias, chest wall and dental
abnormalities, cystic osseous lesions

Other associations
• Cardiovascular - pulmonary stenosis, hypertension
• Renal
• renal artery stenosis - 2% NF1 patients
• phaeochromocytoma - 2% NF1 patients

Spinal deformities
• Cause remains unknown
• Aetiological theories:
• infiltration of bone by localised neurofibromas,
metabolic bone deficiency, osteomalacia,
endocrine disturbance and mesodermal dysplasia
- inconclusive

Cervical spine
• Rarely reported in literature
• Presentation: asymptomatic, pain, deformity, neck
mass, neurological deficit, atlanto-axial dislocations
• Kyphosis is the most common abnormality
• All NF1 patients require x-ray c-spine before a
general anaesthetic/skull traction
Neurofibromatosis of the cervical spine; JB Craig, S Govender; JBJS Br; 1992

Thoracolumbar spine
• Scoliosis:
• Dystrophic
• Non dystrophic
• Kyphoscoliosis
• Lordoscoliosis
• Spondylolisthesis

Scoliosis
• Commonest spinal deformity in NF1 (10-20%)
• Cause of deformity unknown - ?secondary to
osteomalacia, localised neurofibromatous tumour
eroding bone, endocrine disturbances and/or
mesodermal dysplasia
• Dystrophic/non dystrophic

Non dystrophic scoliosis
• Commonest spinal deformity
• Involves 8-10 spinal segments
• Usually convex to the right
• Similar to idiopathic scoliosis

Dystrophic scoliosis
• Less common
• Usually short segment, sharply
angulated curve
• 3 or more dystrophic features on
x-ray
• The more severe the dystrophic
changes the greater the chance
the curve will deteriorate

Dystrophic features• rib pencilling

Dystrophic features• posterior vertebral scalloping

Dystrophic features
• vertebral rotation
• widening of intervertebral foramina
• lateral vertebral scalloping
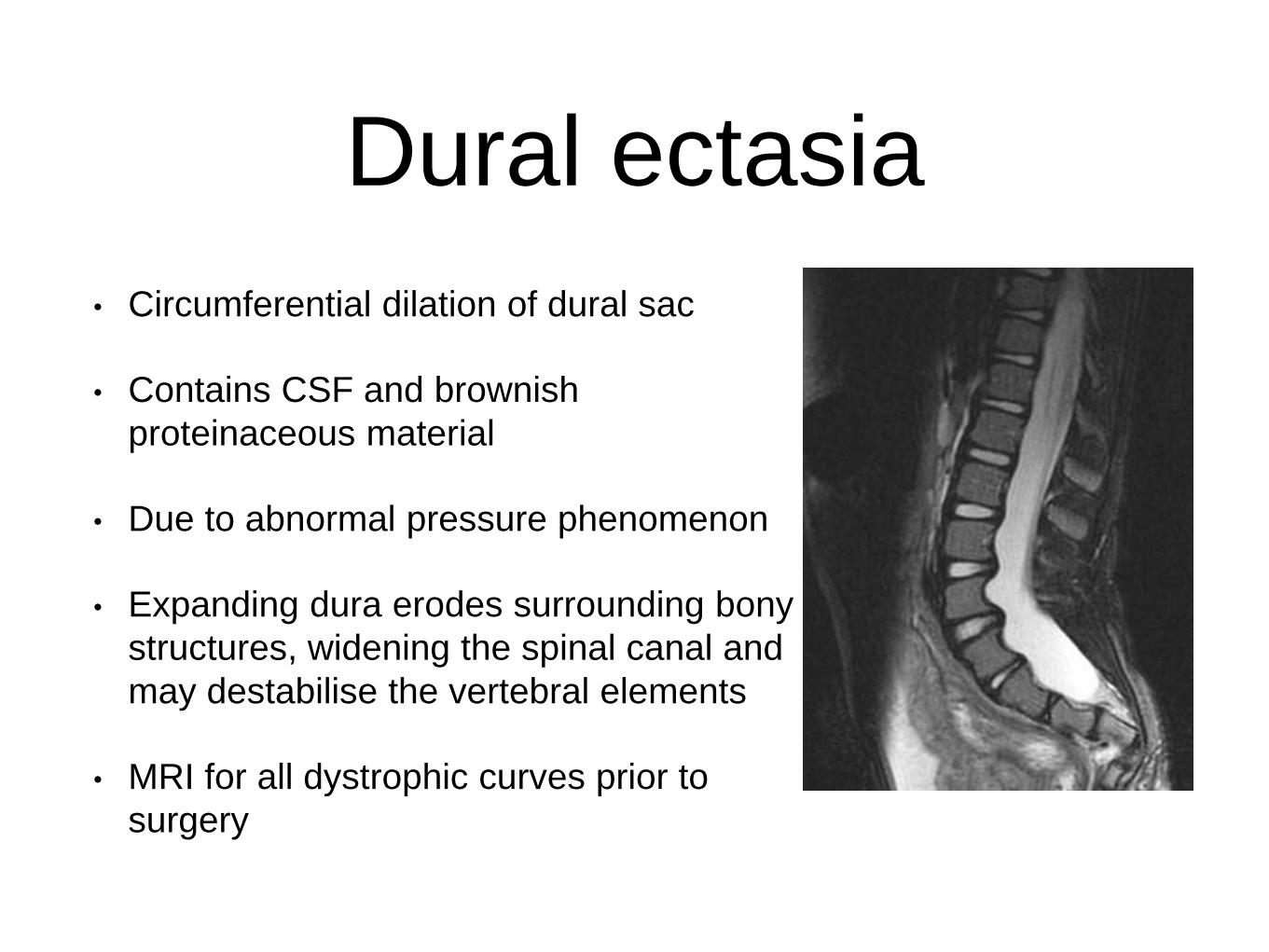
Dural ectasia
• Circumferential dilation of dural sac
• Contains CSF and brownish
proteinaceous material
• Due to abnormal pressure phenomenon
• Expanding dura erodes surrounding bony
structures, widening the spinal canal and
may destabilise the vertebral elements
• MRI for all dystrophic curves prior to
surgery

Modulation• Transformation of non dystrophic curve to dystrophic
or addition of further dystrophic features to a
dystrophic curve
• MRI studies have questioned the theory of
modulation
• Characterisation of curve as dystrophic or not
should be based on x-ray and MRI
Tsirikos et al; Assessment of vertebral scalloping in NF1 with plain
radiography and MRI
AH Crawford et al; Spine deformity preview issue; Sept 2012

Kyphoscoliosis
• Curve of 50 degrees or more in sagittal plane with
any degree of coronal deformity
• Can present with paraplegia (spinal cord elongation,
rib protrusion into canal and intraspinal tumours)
• Flexibility of curve needs to be assessed

Lordoscoliosis
• Not common
• Causes respiratory compromise and mitral valve
prolapse

Spondylolisthesis
• Rare
• Usually associated with pathologic elongation of
pedicles and pars interarticularis by lumbosacral
foramina neurofibromas or dural ectasia with
meningoceles
• Combined anterior and posterior fusion
• Postoperative immobilisation until fusion is solid

Approach• History - establish diagnosis of NF1
• Examination - define deformity, ascertain level and assess
flexibility; neurological deficit; exclude cardiovascular and
renal involvement; exclude pulmonary compromise
• Investigations
• Bloods - FBC, U&E, urinary catecholamines, PFT,
Crossmatch
• X-rays, CT, MRI - Dystrophic/Non dystrophic, curve
magnitude, intraspinal lesions/changes; c-spine

ScoliosisNon-Dystrophic
Curve
<25
Observe
25-40
Brace
40-60
PSF
>60
ASF+PSF
AH Crawford; Neurofibromatosis: etiology, commonly encountered spinal deformities,
common complications; Spine deformity preview issue; 2012
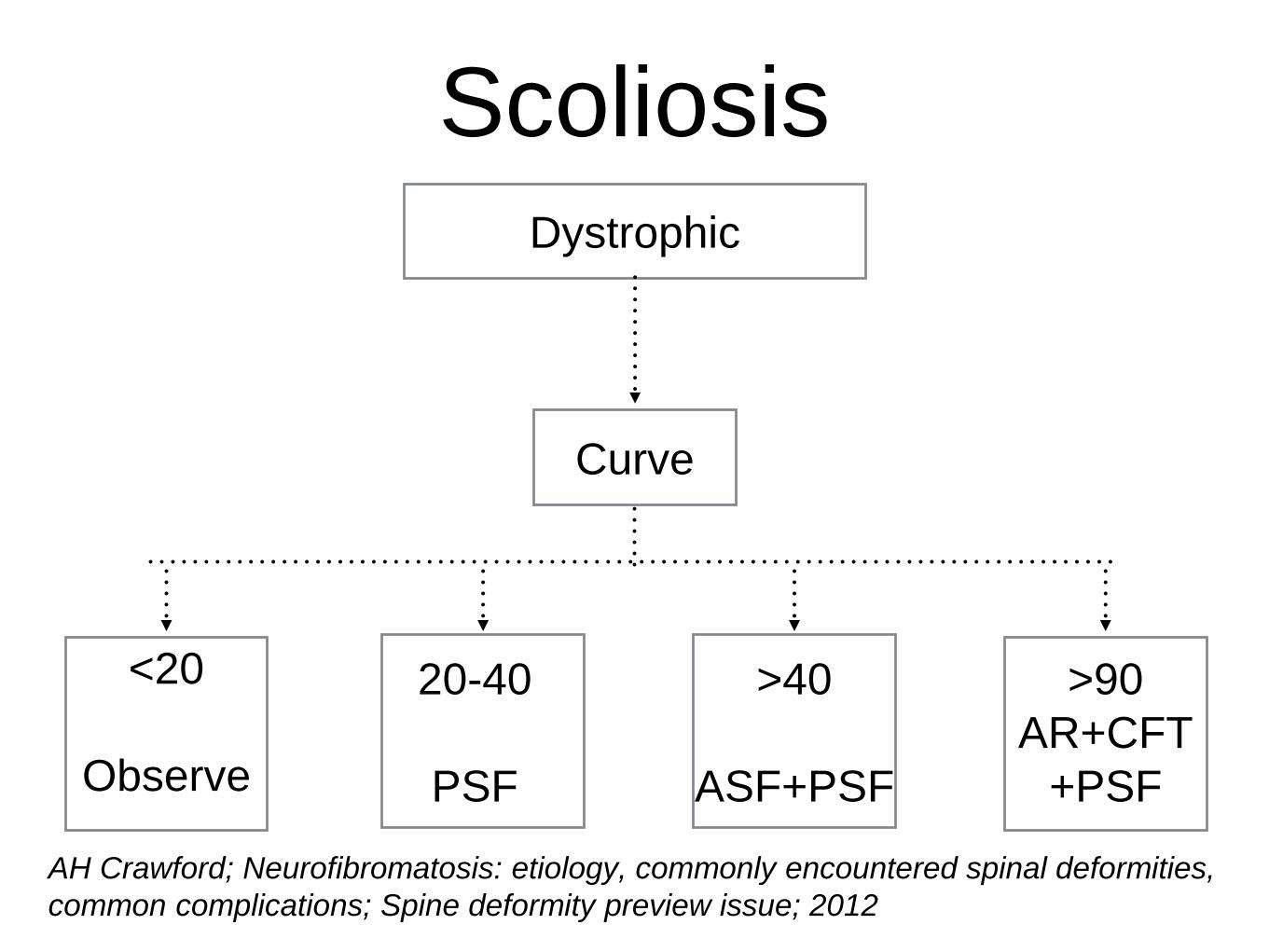
ScoliosisDystrophic
Curve
<20
Observe
20-40
PSF
>40
ASF+PSF
>90
AR+CFT
+PSF
AH Crawford; Neurofibromatosis: etiology, commonly encountered spinal deformities,
common complications; Spine deformity preview issue; 2012

KyphosisNeurology
Curve
50-70
ASF+PSF
Pre-op
CFT
>70
AR+CFT
+PSF
No Yes
Flexible
NoYes
ASF+PSF
AR+CFT
+PSF
AH Crawford; Neurofibromatosis: etiology, commonly encountered spinal deformities, common complications;
Spine deformity preview issue; 2012
Postoperative
• Immobilsation postoperatively
• Fusion mass assessed at 6 months by CT scan

Complications
• Pseudoarthrosis
• Crawford - 15% incidence
• Sirois and Drennan - 38% incidence
• Prevention - decortication, abundant autogenous
bone grafting, segmental instrumentation,
meticulous resection of pathologic soft tissue,
orthotic immobilisation until fusion mass seen on
CT, ?rhBMP-2

Complications
• Paraplegia:
• cord compression secondary to spinal deformity,
rib penetration, intraspinal tumours
• Younger patients - usually spinal deformity
• Older patients - usually tumours

Complications
• Rib protrusion
• Usually occurs on convex of curve
• Important surgical consideration for correction
• Ostectomy of 2.5-5cm of protruding rib indicated
at posterior fusion

Complications
• Bleeding
• Dural leaks

Conclusion
• Scoliosis most common spinal deformity in NF1
• Multidisciplinary treatment strategy is needed
• Management depends on recognition of non-
dystrophic or dystrophic curves
• Post operative immobilisation is always
recommended
Thank You
• Orthopaedic complications of von Recklinghausen's
disease in children. A.H Crawford. Current Orthopaedics
01/1996
• Neurofibromatosis: Etiology, Commonly Encountered
Spinal Deformities, Common Complications and Pitfalls of
Surgical Treatment; A.H. Crawford et al. / Spine Deformity
Preview Issue (September 2012)
• Spinal deformity in neurofibromatosis type-1: diagnosis
and treatment; Athanasios I. Tsirikos; Eur Spine J. Jun
2005
References