NEUROENDOCRINE TUMORS Somatostatin Receptor Scintigraphy
51
NEUROENDOCRINE TUMORS Somatostatin Receptor Scintigraphy Dr. Augusto Llamas Olier Nuclear Medicine Department Instituto Nacional de Cancerología
Transcript of NEUROENDOCRINE TUMORS Somatostatin Receptor Scintigraphy

Logo
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Dr. Augusto Llamas Olier
Nuclear Medicine Department
Instituto Nacional de Cancerología

Logo
Neuroendocrine tumors
Heterogeneous group of neoplasias derived from NE cells of the diffuse
endocrine system.
Characterized by:
Having neurosecretory granules
Producing bioactive amines (serotonine, catecholamines, histamine) and
polypeptidic hormones (somatostatin, gastrin).
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Basis of the clinical utility of radiolabelled specific ligands

Logo
DIAGNOSIS AND THERAPEUTIC APPROACH OF NETs
• I-131/I-123 Metaiodobencylguanidine (MIBG)
Cellular structures for amine uptake and storage
Prefered indications: pheocromocytoma (specif. 80-100%) and
neuroblastoma (specif. 84%).
Sensitivity: 36% - 85%
• Somatostatin analogs (SA)
Overexpression of receptors for regulatory peptides (i.e.,
somatostatin).
Sensitivity: 78% - 100% (Indium-111 DTPA –Octreotide)
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
DIAGNOSIS AND THERAPEUTIC APPROACH OF NETs
Other radioligands
• [68Ga-DOTA]-D-Phe1-Tyr3-Octreotide (68Ga-DOTA TOC)
• [68Ga-DOTA]-Tyr3-Octreotate (68Ga-DOTA TATE)
• [90Y-DOTA]-D-Phe1-Tyr3-Octreotide (90Y-DOTA TOC)
• [177Lu-DOTA ]-Tyr3-Octreotate (177Lu-DOTA TATE)
• [18F]-L-dihydroxyphenylalanine (18F-L-DOPA)
• [11C]-5-hydroxytryptophan (11C-5-HTP)
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo

Logo
SOMATOSTATIN
Peptide regulatory
CNS and peripheral tissues
Hypothalamus
Action:
Neurotransmitter
Hormonal effects:
Inhibitory peptide
GH
Insuline
Glucagon
Gastrin
Serotonin
Calcitonin
Other effects:
Antiproliferative
in tumors
Specific regulation
of immune responses
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Logo
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
Mediated by membrane receptors
Cloned : sstr1 – sstr5
SOMATOSTATIN EFFECTS
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy



Logo


Logo
INTERNALIZATION
Endosome
(dephosphorylation)
RECYCLED
(resensitized)
Lysosome
In-111 DTPA D-Phe OC

Logo
SOMATOSTATIN RECEPTOR EXPRESSION
Normal human tissues
High incidence and density in human neoplasias
Non-endocrine
Non-neural cell tumors
Lymphoma
Breast cancer
Renal-cell cancer
Hepatocellular cancer
Prostate cancer
Sarcoma
Gastric carcinoma
Pituitary adenomas
Pancreatic islet-cell tumors
Gastroenteral NE tumors (carcinoids)
Paragangliomas
Pheochromocytomas
SCLC
Medullary thyroid cancer
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
DOMINATING EXPRESSION OF sstr 2
Simultaneous expression of multiple subtypes of sstr
Prostate: sstr 1
Non-functioning pituitary adenomas: sstr3
Inhibitory, antiproliferative and apoptotic effects
Basis for the clinical application of SA
Human hypophysis ≠ sstr 4
~100% gastrinomas express sstr
10%-50% insulinomas express sstr
¿Tumors with dominant sstr 4 expression?
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Logo
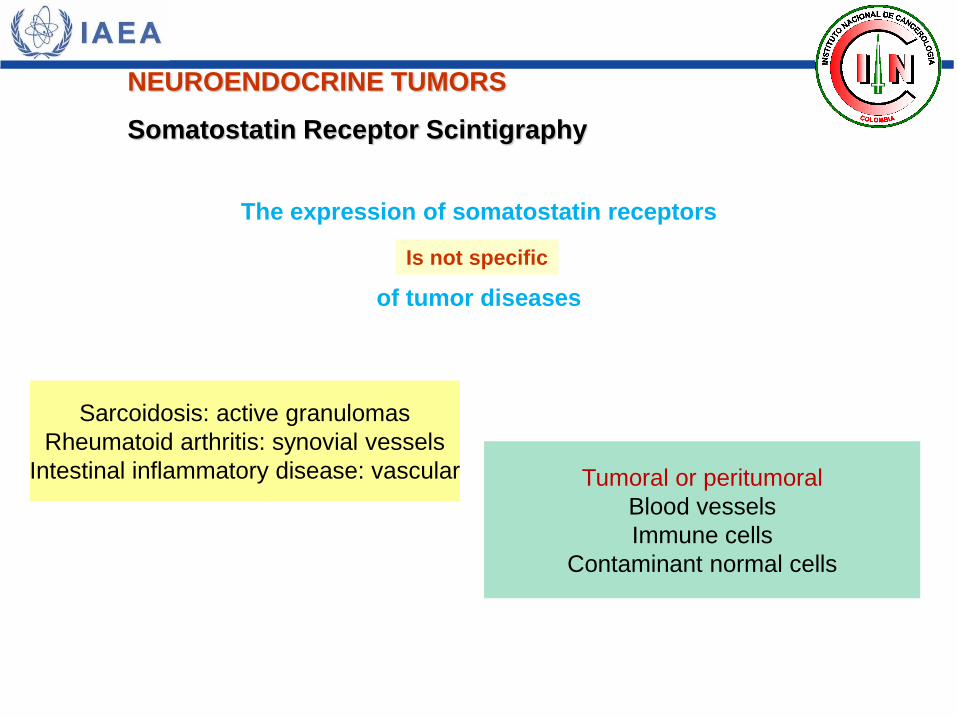
The expression of somatostatin receptors
of tumor diseases
Sarcoidosis: active granulomas
Rheumatoid arthritis: synovial vessels
Intestinal inflammatory disease: vascular
Is not specific
Tumoral or peritumoral
Blood vessels
Immune cells
Contaminant normal cells
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología
Logo
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología

Logo 23-03-06
9-10-08
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología
Phe
Trp
Lys
Tre
Ala - Phe - Asn -
Thr - Ser -
H -
Phe -
Gly - Cys - Lys -
Cys - OH -
s
s DTrp
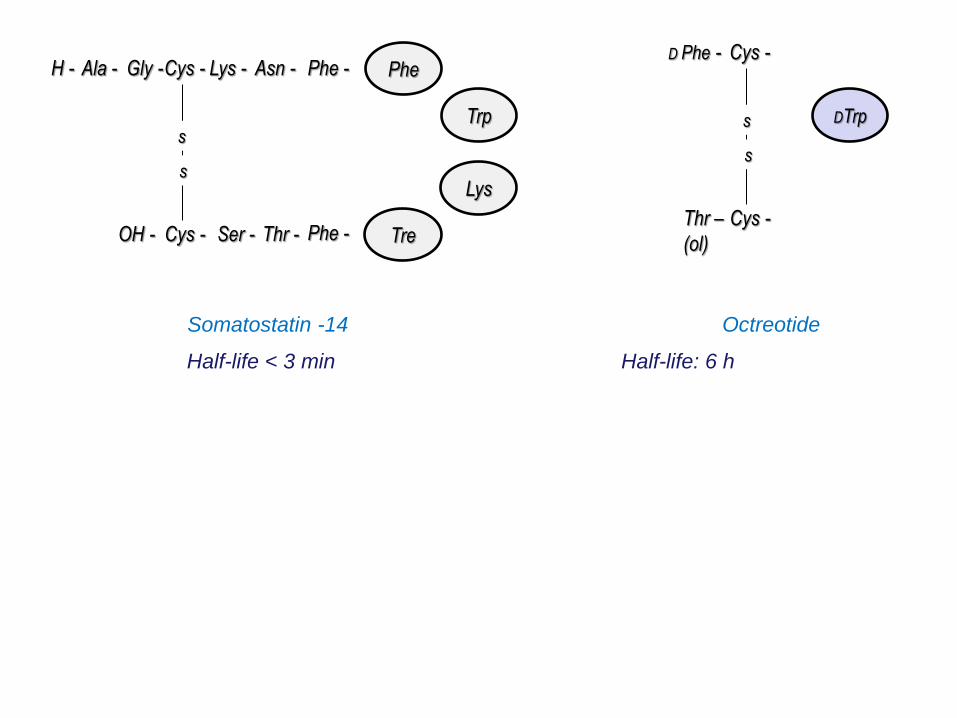
Somatostatin -14 Octreotide
Half-life < 3 min Half-life: 6 h
D Phe - Cys -
Cys - Thr –
(ol)
s
s
Phe
DTrp
Lys
Thr
D Phe - Cys -
Cys - Thr –
(ol)
s
s
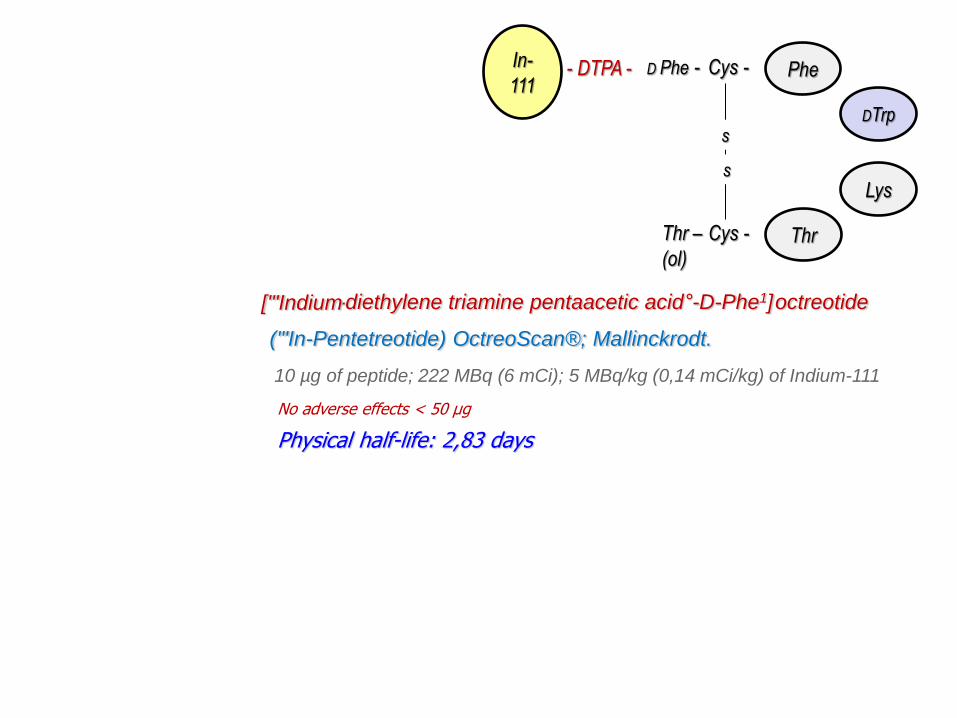
- DTPA - In-
111
('"In-Pentetreotide) OctreoScan®; Mallinckrodt.
10 µg of peptide; 222 MBq (6 mCi); 5 MBq/kg (0,14 mCi/kg) of Indium-111
-diethylene triamine pentaacetic acid°-D-Phe1] octreotide ['"Indium
No adverse effects < 50 µg
Physical half-life: 2,83 days

Tyr
DTrp
Lys
Thr
D Phe - Cys -
Cys - Thr –
(ol)
s
s
- DOTA - Ga-
68
68Ga-DOTA-Tyr3-OC
Phe
DTrp
Lys
Thr
D Phe - Cys -
Cys - Thr –
(ol)
s
s
- DTPA - In-
111
111In-DTPA-OC
Tyr
Thr -
Lys
Thr
Cis -
Cys -
s
s
DPhe -
DTrp
Octreotate
99mTc-HYNIC-TOC
Tc-
99m - HYNIC -
Affinity 9 : 1
Affinity for sstr2 (DTPA o DOTA):
14- to 17-fold >octreotide
8- to10-fold >TOC
Affinity 3 : 1
Higher affinity, higher rate of internalization, higher tumor uptake

Logo

Logo
99mTc- Hynic-Tyr3-Octreotide 111In-DTPAº-Phe1-Octreotide
Nuclear Medicine Department – Instituto Nacional de Cancerología

Logo
Characteristics of a good scintigraphic scan
• Dose: 222 MBq (6 mCi, adults), 5 MBq/Kg (0.14 mCi/Kg, children)
• Spect should have enough counts per projection
• 6-fold contrast enhancement
• Separate overimposed structures
• Enhanced diagnostic sensitivity
• High-count static images are better than wholebody scanning
• Special projections and delayed imaging to solve doubts
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
Characteristics of a good scintigraphic scan
• Dose: 222 MBq (6 mCi, adults), 5 MBq/Kg (0.14 mCi/Kg, children)
• Spect should have enough counts per projection
• 6-fold contrast enhancement
• Separate overimposed structures
• Enhanced diagnostic sensitivity
• High-count static images are better than wholebody scanning
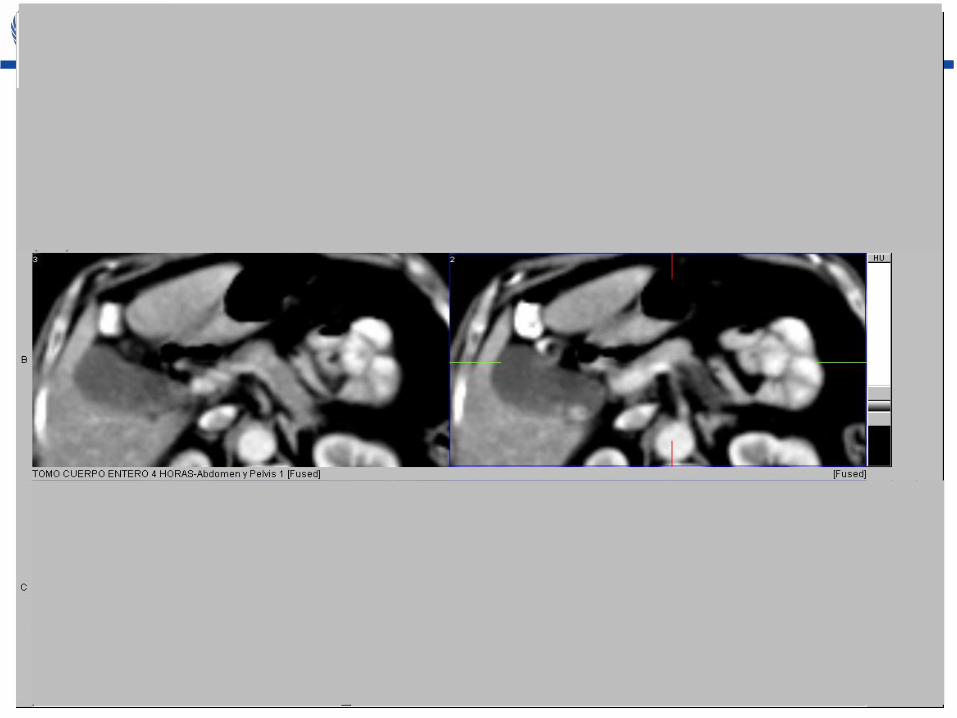
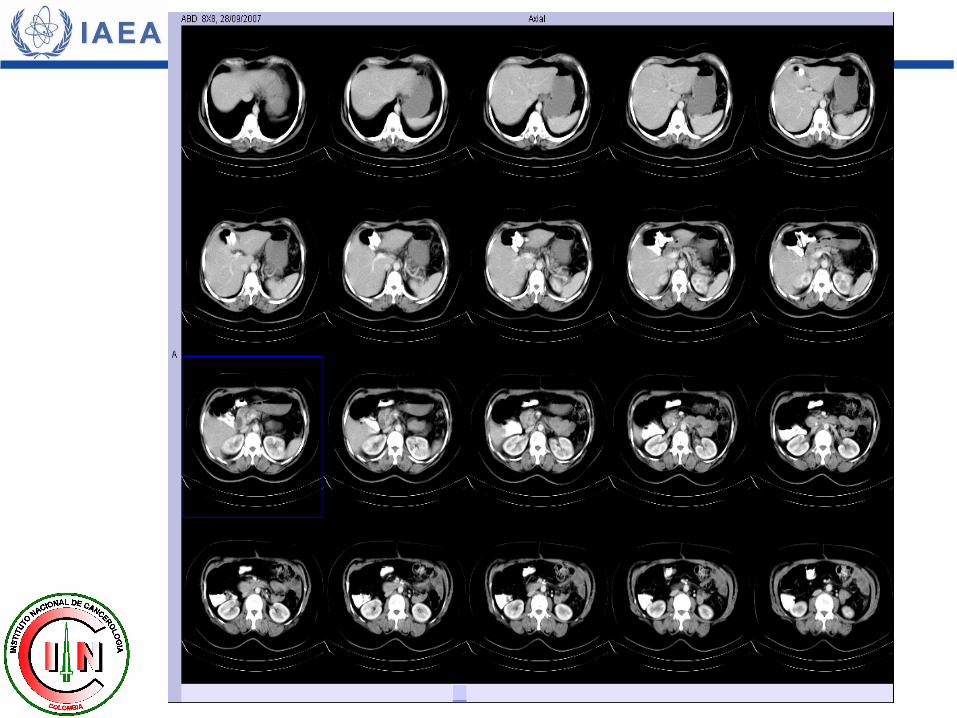
• Special projections and delayed imaging to solve doubts SPECT/ CT
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología

Logo

Logo

Logo

Logo
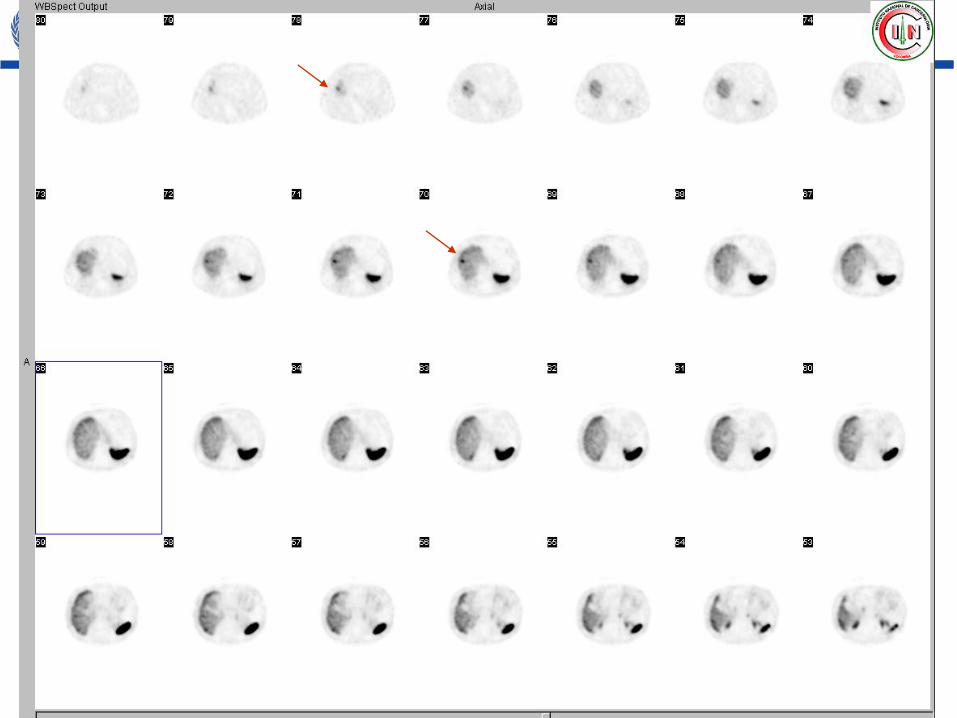
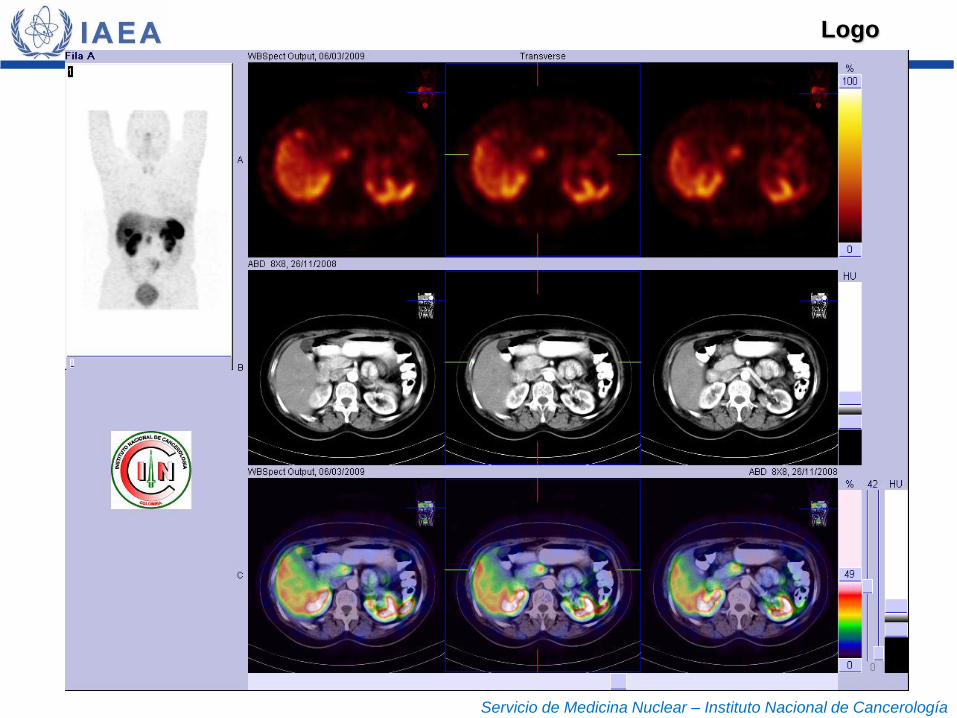
Physiologic vs pathologic
gastric uptake
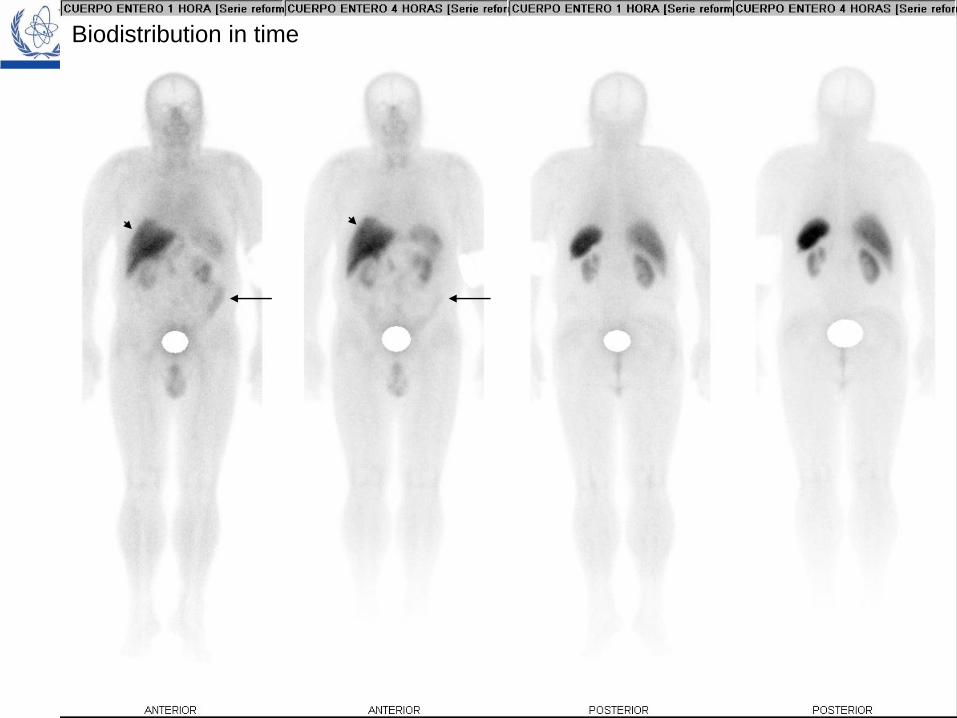
Logo Biodistribution in time
Logo
Logo
Spect corporal total:
Logo

Logo

Logo

Logo
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología
Logo
Servicio de Medicina Nuclear – Instituto Nacional de Cancerología

Logo
SPATIAL RESOLUTION vs MOLECULAR RESOLUTION
CT/ MR Structural
Molecular resolution in the range of 2 nm
Sen
sitiv
ity
Spatial Resolution
mmol
mol
pmol
nmol
1 mm 5 mm 10 mm
PET/ SPECT Metabolism
Sensitivity: capacity to detect a molecular marker Courtesy: Dr. Diana Páez
MOLECULAR IMAGING

Logo
• Post surgical follow-up
• Screen for recurrences when
tumor markers are elevated
• Differential diagnosis between
NETs are space-occupying lesions
• Radioguided surgery of small
tumors/ confirmation of complete
resection.
• Search for primary tumor
• Assess extent of disease
• Assess treatment response.
• Select patients for radionuclide
treatment
IN-111-OCTREOTIDE SCINTIGRAPHY FOR GEP-NETs
INDICATIONS
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
• Post surgical follow-up
• Screen for recurrences when
tumor markers are elevated
• Differential diagnosis between
NETs are space-occupying lesions
• Radioguided surgery of small
tumors/ confirmation of complete
resection.
IN-111-OCTREOTIDE SCINTIGRAPHY FOR GEP-NETs
INDICATIONS
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Logo

Logo

Logo

Logo

Logo
IN-111-OCTREOTIDE SCINTIGRAPHY FOR GEP-NETs
Clinical Impact
Changes in management: 17% - 28%
Identification of new lesions
Clear up imaging findings
Avoids unnecessary surgery
Detects previously
undetected metastases
Cost-benefit relationship
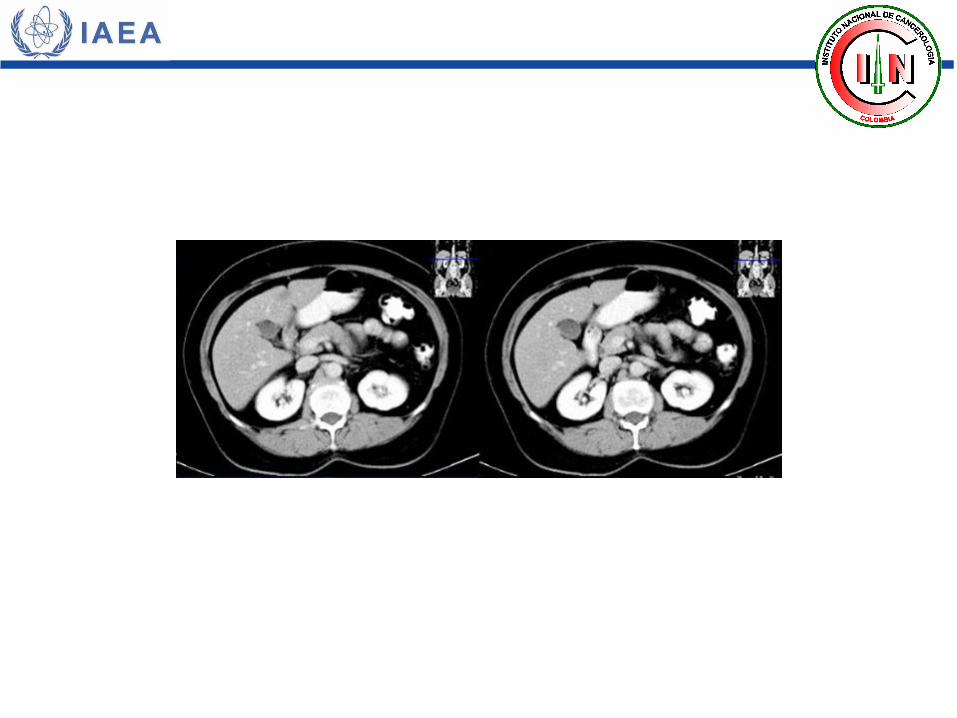
SPECT/CT
Enhances image interpretation
Precise anatomical localization (32%)
Further changes in management (14%)
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
COMING UP
Somatostatin analogs labelled with positron emitters
ADVANTAGES OVER GAMMA EMITTERS
• Better affinity for sstr2
• Bind to other sstr: useful for non sstr2-expressing tumors
• Better spatial and molecular resolution
(detectability: SPECT 1-2 cm / PET 0,5-1 cm)
• Combined anatomic and metabolic information: better sensitivity
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
COMING UP
Somatostatin analogs labelled with positron emitters
[68Ga-DOTAº,Tyr3]Octreotide o [68Ga-DOTAº,Tyr3]Octreotate
• Multiple analogs in use with little infoormation exchange from center to
center.
• Will become the new standard in sstr-imaging
o High affinity for sstr2
o 68Ga: produced in generators / easy labelling on a daily basis
o90Y- and 177Lu -labelled counterparts are used for therapy
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy

Logo
1. SRS: to assess NETs and to identify candidates for
metabolic therapies
CONCLUSIONS I
5. TOC and TATE: more affinity, higher internalization rate than octreotide
2. Tumor uptake: depends on affinity for sstr2 and rate of internalization
3. Small changes in peptide structure, chelating agents, radiometal
will enhace affinity and internalization rate.
4. [111Indio-DTPAº, Phe1] octreotide: current standard but not perfect
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy
Logo
6. Same peptide for diagnosis and therapy
CONCLUSIONS II
7. New standard: [68Ga-DOTAº,Tyr3] Octreotide or
[68Ga-DOTAº,Tyr3] Octreotate
NEUROENDOCRINE TUMORS
Somatostatin Receptor Scintigraphy