
Neuro-ICU: Day 1 - Critical Care Canada · ICP A Stepwise Approach Stephan A. Mayer, MD Professor,...
63
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
Transcript of Neuro-ICU: Day 1 - Critical Care Canada · ICP A Stepwise Approach Stephan A. Mayer, MD Professor,...

ICPA Stepwise Approach
Stephan A. Mayer, MDProfessor, Neurology & Neurosurgery
Director, Neurocritical Care,
Mount Sinai Health System


ICP: Basic Concepts
• Monroe-Kellie doctrine:
skull = fixed volume
• 3 components of
intracranial volume
• Normal ICP
–≤20 cm H20
–≤15 mm Hg
CSF150 ml
Blood 150 ml
Parenchyma
1200 ml
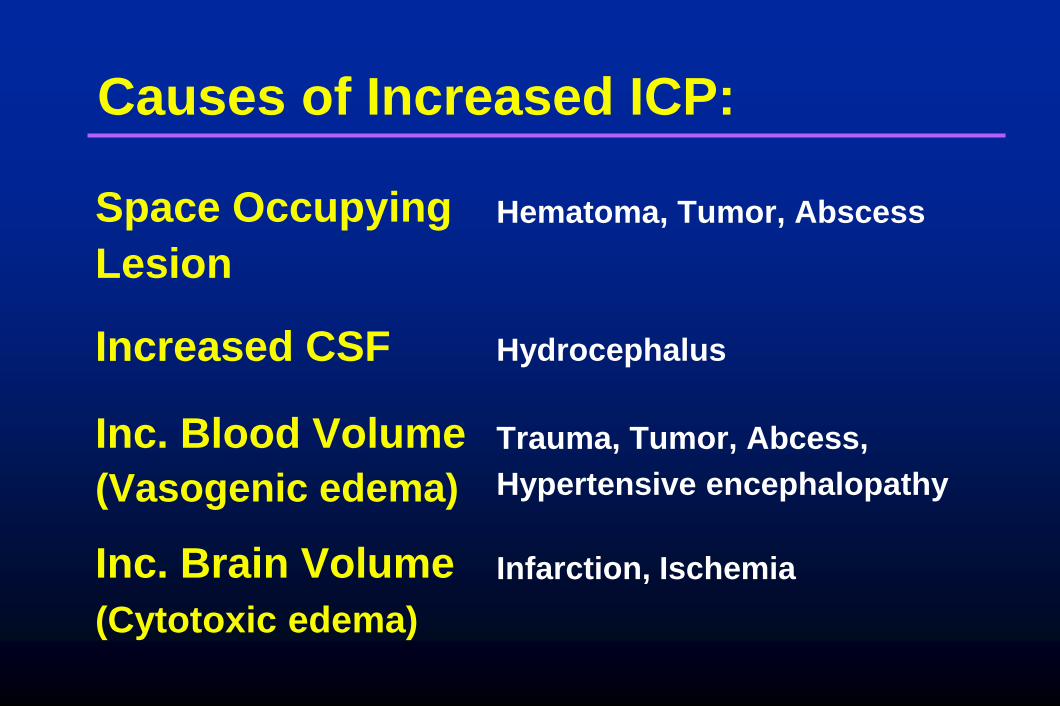
Causes of Increased ICP:
Space Occupying
Lesion
Increased CSF
Inc. Blood Volume
(Vasogenic edema)
Inc. Brain Volume
(Cytotoxic edema)
Hematoma, Tumor, Abscess
Hydrocephalus
Trauma, Tumor, Abcess,
Hypertensive encephalopathy
Infarction, Ischemia

Methods to Reduce Elevated ICP
• Remove Mass Lesion Surgical Evacuation
• Reduce CSF Volume Ventricular Drainage
• Reduce Cerebral Hyperventiation, Barbiturates,
Blood Volume Hypothermia
• Reduce Parenchymal Osmotic Diuretics
Volume (Mannitol, Hypertonic Saline)


CPP can influence ICP when you run out of room
0
25
50
75
Cerebral Perfusion Pressure (mm Hg))
Cere
bra
l B
loo
d F
low
(ml/100 g
/min
)
Zone of Normal
Autoregulation
Maximum
Constriction
Maximum
DilatationPassiveCollapse
0
25
50
ICP
(m
m H
g)
Stephan A. Mayer, MD
1501251007550250GOAL

CPP can influence ICP when you run out of room
0
25
50
75
Cerebral Perfusion Pressure (mm Hg))
Cere
bra
l B
loo
d F
low
(ml/100 g
/min
)
Zone of Normal
Autoregulation
Maximum
Constriction
Maximum
DilatationPassiveCollapse
0
25
50
ICP
(m
m H
g)
Vasodilatory Cascade Zone
Autoregulation Breakthrough Zone
Stephan A. Mayer, MD
1501251007550250GOAL

Outcome after Acute Ischemic Stroke by
Admission Blood Pressure
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0 –n = 18
< 120
n = 29
121 -140
n = 39
141 -160
n = 78
161 -180
n = 49
181 -200
n = 87
> 200
Post neuro
logic
al outc
om
e %
Systolic BP on admission (mm Hg)
C
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0 –n = 18
< 120
n = 29
121 -140
n = 39
141 -160
n = 78
161 -180
n = 49
181 -200
n = 87
> 200
Early
neuro
logic
al dete
riora
tion %
Systolic BP on admission (mm Hg)
A
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0 –Post neuro
logic
al outc
om
e %
Diastolic BP on admission (mm Hg)
D
n = 38
< 70
n = 39
71 -80
n = 48
81 -90
n = 43
91 -100
n = 30
101 -110
n = 102
> 110
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0 –n = 38
< 70
n = 39
71 -80
n = 48
81 -90
n = 43
91 -100
n = 30
101 -110
n = 102
> 110
Early
neuro
logic
al dete
riora
tion %
Diastolic BP on admission (mm Hg)
B Castillo J, et al. Stroke. 2004;35:520-526.

Lund protocol
• Reduce CMRO2 with sedation— Miazolam, thiopental, fentanyl
• Reduce BP and capillary hydrostatic
pressure (CPP 50-60 mm Hg)— IV Metoprolol (.2 mg/kg/hr) and clonidine (.5 mcg/kg prn)
• Dihydroergotamine .1-.8 mcg/kg/hr
• Maintain normal hematocritt, CVP, and albumin
levels

MAP GOAL
MMM: “Imaging” Vasodilatory
Cascade Physiology
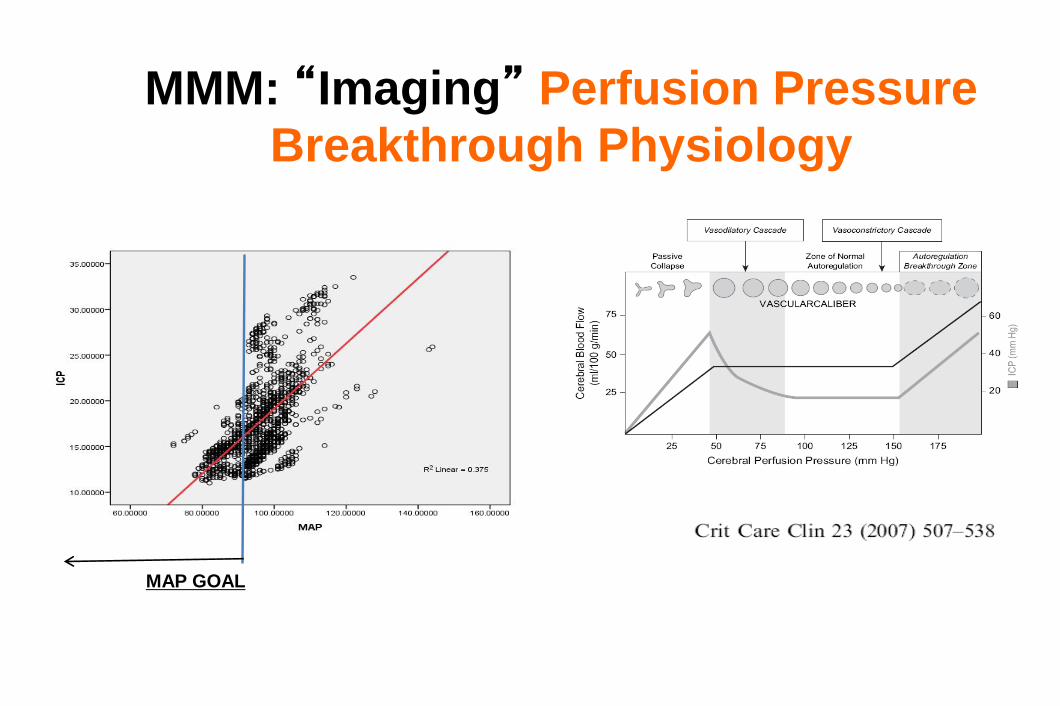
MMM: “Imaging” Perfusion Pressure
Breakthrough Physiology
MAP GOAL

Indications for ICP Monitoring
• Coma (Glasgow Coma Scale score ≤8)
• CT evidence of intracranial mass effect– Extra-axial mass lesion
– Midline shift
– Effacement of basal cisterns
– Exception: severe TBI with motor posturing
• Prognosis is such that aggressive ICU care is warranted

Clinical Signs
• Increased ICP
–Depressed level of consciousness
–Pressor response
–Projectile vomiting
–CN 6 palsies
• Brainstem herniation
–CN 3 palsey
–Motor posturing
–Lower extremity rigidity
–Loss of lateral EOMs
–Hyperventilation

Parenchymal
Micosensor
Richmond Bolt
Epidural Monitor
Ventricular catheter

ICP/CPP Treatment Thresholds
Guideline
• ICP treatment should be initiated at an upper threshold of 20 mm Hg.
Option
• Cerebral Perfusion Pressure should bemaintained at a minimum of 60 mm Hg.

Emergency Treatment of Increased ICP
• Un-monitored patient with clinical signs of herniation
–Elevate head of bed 30°
–Normal saline 100 ml/hr
–Intubate and hyperventilate (pCO2 30 mm Hg)
–Mannitol 20% 1.0 to 1.5 g/kg rapid IV infusion
–Foley catheter
–CT scan and neurosurgical evaluation

Critical Pathway for Treatment of Intracranial Hypertension in the Severe Head Injury Patient
(Treatment Option)
May Repeat Mannitolif Serum Osmolarity
< 320 mOsm/L &Pt euvolemic
High Dose
Barbiturate therapy
• Hyperventilation to PaCO2 < 30 mmHg
• Monitoring SjO2, AVDO2, and/orCBF
Recommended
Other Second
Tier Therapies
NO
YES NO
YES NO
YES NO
CarefullyWithdraw
ICP Treatment
ConsiderRepeatingCT Scan
YES
Second Tier Therapy
Intracranial Hypertension?
Hyperventilation to PaCO2 30 - 35 mmHg
Intracranial Hypertension?
Mannitol (0.25 - 1.0 g/kg IV)
Intracranial Hypertension?
Ventricular Drainage (if available)
Intracranial Hypertension?*
Maintain CPP 70 mmHg
Insert ICP Monitor

ICP
PROTOCOL

SURGICAL DECOMPRESSION
SEDATION
CPP OPTIMIZATION
OSMOTHERAPY
HYPERVENTILATION
PENTOBARBITAL
HYPOTHERMIA7
6
5
4
3
2
1
Columbia
Stepwise ICP
Protocol
2002

SURGICAL DECOMPRESSION
SEDATION
CPP OPTIMIZATION
OSMOTHERAPY
HYPERVENTILATION
HYPOTHERMIA
PENTOBARBITAL7
6
5
4
3
2
1
Revised
Columbia
Stepwise ICP
Protocol
2010

Ventricular Drainage
3-way stopcock turned off to drainage system
drainage
bag
100cc syringe of sterile
water
transpac positioned at ear
level
1LEVEL

ICU Intravenous sedation
• Goal is reversibility to allow repeated neurologic assessment
• Alternatives (in intubated pts):
–Fentanyl or Remifentanyl
–Midazolam
–Propofol » Ultrashort acting
» Allows “wake-up” in 5-15 mins
» Reduces ICP, CMRO2
» Drawbacks: hypotension, infection
2

PENTOBARBITAL ISHYPOTHERMIA IS
Complications of pentobarbital
•Hypotension
•Immunosuppression
• An extra 4 weeks in coma
• ICU neuromyopathy

CPP
OPTIMIZATION:
Dopamine
infusion
resulting in
increased MAP
and CPP, and
decreased ICP
3

Osmotherapy
• Mannitol– 0.25 to 1.5 g/kg IV wide open
– Dose up to Q1H on an as-needed basis
– Mechanisms:
» Acute dehydrating effect (osmotic gradient across BBB)
» Secondary hyperosmolality (diuretic effect)
» Reflex vasoconstriction (viscosity effect)
• Hypertonic Saline– Varying concentrations: 3%, 7.5%, 10%, and 23.4%
– Optimal dosing not known
4

30 ml 23.4% Bullets

Effect of Hypertonic Saline in CBF in SAH patients
TSENG M-Y, Stroke 2003;34:1389.)
• 10 poor grade
SAH patients
• 2 mL/kg of
23.5% saline
• ICP fell 74%
• CPP rose 27%
• CBF rose 23%
• Peak effect @
20-60 minutes
MAP
CPP
ICP
TCD
CVR

Hyperventilation
HYPERVENTILATION IS THE MOST RAPID WAY TO REDUCE ICP
EXCESSIVE HYPERVENTILATION CAN WORSEN CEREBRAL ISCHEMIA
MECHANISM OF ACTION:
HYPOCARBIA INDUCES SERUM AND CSF ALKALOSIS
ALKALOSIS INDUCES CEREBRAL VASOCONSTRICTION
VASOCONSTRICTION REDUCES CEREBRAL BLOOD VOLUME
TIME COURSE:
ICP IS REDUCED ALMOST IMMEDIATELY
PEAK REDUCTION IN 5-10 MINUTES
Hyperventilation Can Have Sustained Effects In Patients With Vasodilatory Vasogenic Cerebral Edema
5

Hypothermia
MECHANISM OF ACTION:
PROFOUNDLY REDUCES REDUCES CEREBRAL METABOLISM, AND HENCE CEREBRAL BLOOD VOLUME
TARGET
32-33° C
INDICATION
PENTOBARBITAL-REFRACTORY ICP
COMPLICATIONS:
ARRYTHMIA AND CARDIOVASCULAR DEPRESSION
IMMUNOSUPPRESSION
COAGULOPATHY
METABOLIC: SHIVERING AND REWARMING
6

HYPOTHERMIA FOR ICP CONTROL:TRAUMATIC BRAIN INJURY
• Shiozaki (J Neurosurg 1993)
– Randomized controlled study of hypothermia (34°C) for ICP refractory to pentobarbital (N=33).
– Hypothermia resulted in:
»Lower ICP (36.9 to 26.5 mm Hg)
»Increased CPP
»Reduced CBF and CMRO2
»Reduced arteriojugular venous oxygen differences
– Survival was 50% in hypothermia patients compared to 18% in the control group (P<.05).


1
6
5
4
3
2
SECOND TIERStep Up
THIRD TIERAdvance as Needed
HEMICRANIECTOMY or SALVAGE CRANIOTOMY
HYPOTHERMIATO TARGET 35 °C
HYPERVENTILATION (HV)TO pCO2 30-35 mm Hg
BOLUS OSMOTHERAPYTO SERUM OSMS <320
SEDATION to RASS -4 to -5(Quiet, Motionless State)
TARGET CPP 50-70 mm Hg
CSF DRAINAGE and/orRESCUE CRANIOTOMY
HYPOTHERMIATO TARGET 33 °C
MMM-GUIDED HV<30 mm Hg and/or THAM
BOLUS OSMOTHERAPYTO SERUM OSMS >320
PARALYSIS and/orBARBITURATES
MMM-GUIDEDCPP OPTIMIZATION

5HYPERVENTILATION (HV)
TO pCO2 30-35 mm Hg
1
SECOND TIER
6 HYPOTHERMIATO TARGET 35 °C
4 BOLUS OSMOTHERAPYTO SERUM OSMS <320
3 SEDATION to RASS -4 to -5(Quiet, Motionless State)
2 TARGET CPP 50-70 mm Hg
CSF DRAINAGE and/orRESCUE CRANIOTOMY
Advance
first-tier ICP
interventions
in stepwise
fashion to
avoid missing
essential steps

THIRD TIER
HEMICRANIECTOMY or SALVAGE CRANIOTOMY
HYPOTHERMIATO TARGET 33 °C
MMM-GUIDED HV<30 mm Hg or THAM
BOLUS OSMOTHERAPYTO SERUM OSMS >320
PARALYSIS and/orBARBITURATES
MMM-GUIDEDCPP OPTIMIZATION
Advance
second-tier ICP
interventions
as needed
to fit
available
resources and
the clinical
situation

THIRD TIER
HEMICRANIECTOMY or SALVAGE CRANIOTOMY
HYPOTHERMIATO TARGET 33 °C
MMM-GUIDED HV<30 mm Hg or THAM
BOLUS OSMOTHERAPYTO SERUM OSMS >320
PARALYSIS and/orBARBITURATES
MMM-GUIDEDCPP OPTIMIZATION
Three very bad
options for a
very bad
situation:
medically
refractory ICP!

What About the Latest Trials?

BEST-TRIP TRIAL

BEST-TRIP TRIAL
• 324 patients 13 years of age or older with severe TBI in Bolivia or Ecuador
– Protocol treating ICP based on ICP monitoring
– Protocol for treating ICP based on standing therapy, imaging and clinical examination
• Six-month mortality was 39% in the pressure-monitoring group and 41% in the imaging–clinical examination group (P = 0.60).
• Median length of stay in the ICU was similar in the two groups

BEST-TRIP TRIAL
• Number of days of brain-specific treatments (e.g., administration of hyperosmolar fluids and the use of hyperventilation) in the ICU was higher in the imaging–clinical examination group than in the pressure-monitoring group (4.8 vs. 3.4, P = 0.002).
• Serious adverse events was similar in the two groups.
BEST-TRIP
• Conclusion
For patients with severe traumatic brain injury, care focused on maintaining monitored intracranial pressure at 20 mm Hg or less was not shown to be superior to care based on imaging and clinical examination.

Survival at 14 days MUCH
better with ICP
monitoring!

Survival at 14 days better with ICP monitoring



Aneurysmal SAH with associated suddural hematoma
and bilateral motor posturing
DECRA
• 155 TBI patients
– Early bifrontal craniectomy vfersus standard care
• Surgical group had
– Lower ICPs
– Fewer ICP interventions
– Fewer ICU days
– WORSE outcomes despite similar mortality


DEAD FULL
RECOVERY

Communicating
hydrocephalus is
an almost
universal finding
in patients after
hemicraniectomy


EUROTHERM 3235
• 387 severe TBI patients
– Randomization trigger: firstepisode of ICP >20 mm Hg
• Hypothermia group
– Died more
– Less likely to survive with good outcome
• 26% vs 37%
– Cause of this worse outcome is unclear



RESCUEicp Trial
Conclusion
• When the going gets tough, when ICP is medically refractory, easy options are hard to find
• All three THIRD TIER options likely cause harm when performed early without a trial of ICU care
– Prophylactic barbiturate coma
– Straight to the OR for hemicraniectomy
– Cool to 32-35 C° at the first sign of ICP elevation
• My preference for definitive salvage intervention when ICU care is failing go to the OR

RESCUEicp Trial• 408 severe TBI patients
– Age 18-65
– Randomization trigger: Medically refractory ICP >25 mm Hg for 1-12 hours
– Time to randomization >72 hours after injury in 45%
• Hemicraniectomy group
– Absolute 22% reduction in mortality
– Better ICP control: 5 vs 17 hours with ICP >25 mm Hg
– More complications (mostly surgical related): 16% vs 9%

RESCUEicp Trial:
Craniectomy vs Barbiturates

Rescue Hemicraniectomy
Creates a 22% chance of converting death to survival in
a vegetative state or with severe disability

1
6
5
4
3
2
SECOND TIER
HYPOTHERMIATO TARGET 35 °C
HYPERVENTILATION (HV)TO pCO2 30-35 mm Hg
BOLUS OSMOTHERAPYTO SERUM OSMS <320
SEDATION to RASS -4 to -5(Quiet, Motionless State)
TARGET CPP 50-70 mm Hg
CSF DRAINAGE and/orRESCUE CRANIOTOMY
Advance
first-tier ICP
interventions
in stepwise
fashion to
avoid missing
essential steps

1
6
5
4
3
2
SECOND TIER
HYPOTHERMIA to 35 °COption: TARGET 33° C
HYPERVENTILATION (HV)Option: MMM-Guided HV <30
BOLUS OSMOTHERAPYOption: PUSH OSMS >320
SEDATION to RASS -4 to -5Option: ADD PARALYTICS
TARGET CPP to 50-70 mm HgOption: MMM-TARGETED CPP
CSF DRAINAGE and/orRESCUE CRANIOTOMY
Ultimately,
once you
realize that
you are losing
the battle,
there is really
only one
effective third
tier therapy
for ICP: pop
the lid!
HEMICRANIECTOMY or SALVAGE CRANIOTOMY
THIRD TIER

Neurocritical Care Societywww.neurocriticalcare.org


















