Neu Motor Ax
6
Postgraduate Education Corner CHEST IMAGING AND PATHOLOGY FOR CLINICIANS CHEST 1174 Postgraduate Education Corner CHEST 2013; 143(4):1174–1179 A 50-year-old mixed-race Ugandan businessman in otherwise good health presented to his local hos- pital with left-sided pleuritic chest pain and dyspnea 2 days following a short domestic flight. There was no prodromal illness or prior physical injury. He was a nonsmoker whose medical history was notable for asthma and asymptomatic hepatitis B infection. Initial vital observations included a temperature of 36.2°C, BP of 110/70 mm Hg, sinus tachycardia of 110/min, respiration of 32/min, and oxygen satura- tion as measured by pulse oximetry of 99% on room air. Examination of the oral cavity, neck, and axillae was unremarkable. Symmetrical chest expansion with quieter breath sounds over the left hemithorax was noted. Laboratory results confirmed normal CBC, C-reactive protein level, erythrocyte sedimentation rate, and renal and liver biochemistry findings. Plain chest radiography showed a large left-sided pneumothorax and widely distributed pulmonary nodules (Fig 1A). After unsuccessful needle thoracen- tesis, an intercostal chest drain was placed. Despite application of high-volume/low-pressure wall suc- tion for 48 h, the pneumothorax failed to resolve. Contrast-enhanced thoracic CT scanning demon- Spontaneous Pneumothorax in a 50-Year-Old Man With Diffuse Pulmonary Nodules Natalie Stolagiewicz, MBBS; Brendan Tinwel, MBBCh; Ian S. Cormack, MBBS; Sebastian B. Lucas, BMBCh; Anand Devaraj, MBBS, MD; Tuck Kay-Loke, MD; and Felix Chua, MBBS, PhD Figure 1. A, Frontal chest radiograph showing left-sided pneu- mothorax and diffuse pulmonary nodules. B, CT image demon- strating extensively distributed small centrilobular (circle) and paralymphatic (arrow) pulmonary nodules and left-sided pneu- mothorax. strated a profusion of 3- to 4-mm solid, well-defined lung nodules that were mostly disseminated in a Manuscript received March 8, 2012; revision accepted September 7, 2012. Affiliations: From the Respiratory Medicine Department (Drs Stolagiewicz and Chua), Pathology Department (Dr Tinwell), and Radiology Department (Dr Devaraj), St. George’s Hospital NHS Trust, London; Department of Genito-Urinary Medicine (Dr Cormack), Department of Respiratory Medicine (Dr Loke), Croydon University Hospital, Croydon; and Histopathology Department (Prof Lucas), School of Medicine, King’s College London, London, England. Correspondence to: Natalie Stolagiewicz, MBBS, Respiratory Medicine Department, St. George’s Hospital NHS Trust, Blackshaw Rd, Tooting, London, SW17 0QT, England; e-mail: [email protected] © 2013 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1378/chest.12-0633 Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014
Transcript of Neu Motor Ax
Postgraduate Education CornerCHEST IMAGING AND PATHOLOGY FOR CLINICIANS
CHEST
1174 Postgraduate Education Corner
CHEST 2013; 143 ( 4 ): 1174 – 1179
A 50-year-old mixed-race Ugandan businessman in otherwise good health presented to his local hos-
pital with left-sided pleuritic chest pain and dyspnea 2 days following a short domestic fl ight. There was no prodromal illness or prior physical injury. He was a nonsmoker whose medical history was notable for asthma and asymptomatic hepatitis B infection.
Initial vital observations included a temperature of 36.2°C, BP of 110/70 mm Hg, sinus tachycardia of 110/min, respiration of 32/min, and oxygen satura-tion as measured by pulse oximetry of 99% on room air. Examination of the oral cavity, neck, and axillae was unremarkable. Symmetrical chest expansion with quieter breath sounds over the left hemithorax was noted. Laboratory results confi rmed normal CBC, C-reactive protein level, erythrocyte sedi mentation rate, and renal and liver biochemistry fi ndings.
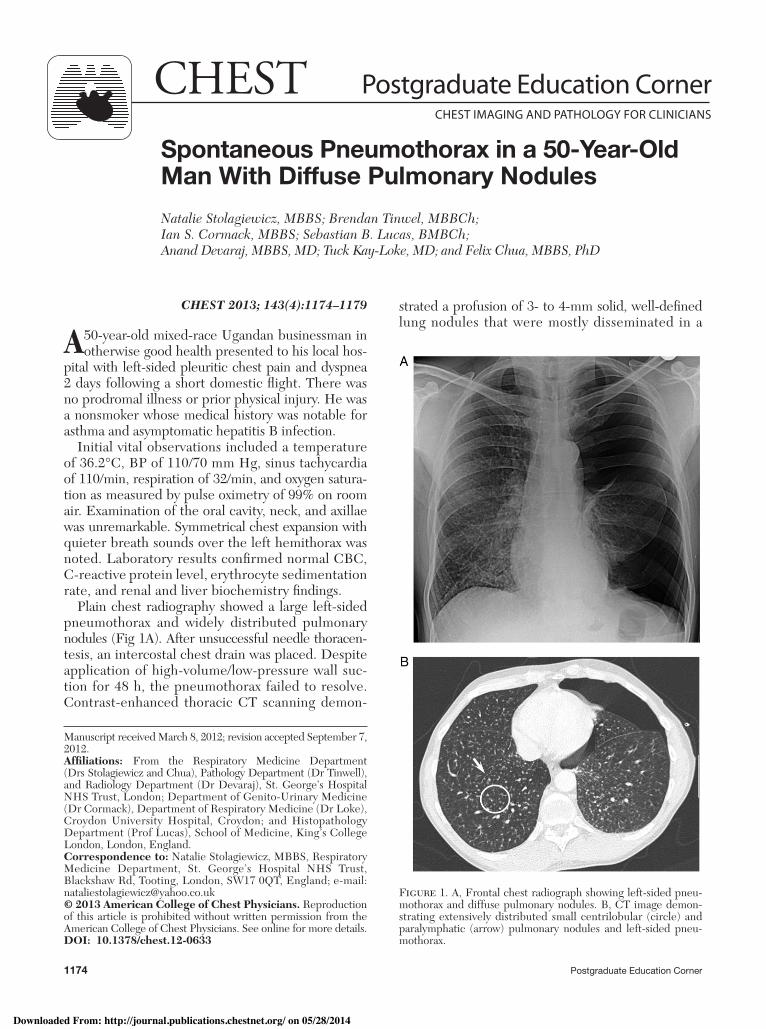
Plain chest radiography showed a large left-sided pneumothorax and widely distributed pulmonary nodules ( Fig 1A ). After unsuccessful needle thoracen-tesis, an intercostal chest drain was placed. Despite application of high-volume/low-pressure wall suc-tion for 48 h, the pneumothorax failed to resolve. Contrast-enhanced thoracic CT scanning demon-
Spontaneous Pneumothorax in a 50-Year-Old Man With Diffuse Pulmonary Nodules Natalie Stolagiewicz , MBBS ; Brendan Tinwel , MBBCh ; Ian S. Cormack , MBBS ; Sebastian B. Lucas , BMBCh ; Anand Devaraj , MBBS, MD ; Tuck Kay-Loke , MD ; and Felix Chua , MBBS, PhD
Figure 1. A, Frontal chest radiograph showing left-sided pneu-mothorax and diffuse pulmonary nodules. B, CT image demon-strating extensively distributed small centrilobular (circle) and paralymphatic (arrow) pulmonary nodules and left-sided pneu-mothorax.
strated a profusion of 3- to 4-mm solid, well-defi ned lung nodules that were mostly disseminated in a
Manuscript received March 8 , 2012 ; revision accepted September 7 , 2012 . Affi liations: From the Respiratory Medicine Department (Drs Stolagiewicz and Chua), Pathology Department (Dr Tinwell), and Radiology Department (Dr Devaraj), St. George’s Hospital NHS Trust, London; Department of Genito-Urinary Medicine (Dr Cormack), Department of Respiratory Medicine (Dr Loke), Croydon University Hospital, Croydon; and Histopathology Department (Prof Lucas), School of Medicine, King’s College London, London, England. Correspondence to: Natalie Stolagiewicz, MBBS, Respiratory Medicine Department, St. George’s Hospital NHS Trust, Blackshaw Rd, Tooting, London, SW17 0QT, England; e-mail: [email protected] © 2013 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1378/chest.12-0633
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014
CHEST / 143 / 4 / APRIL 2013 1175journal.publications.chestnet.org
random manner, although some had a centrilobular or peribronchovascular confi guration ( Figs 1B , 2 ). No signifi cant lymphadenopathy, bronchial wall thick-ening, mosaic parenchymal attenuation, or signs of interstitial fi brosis were evident.
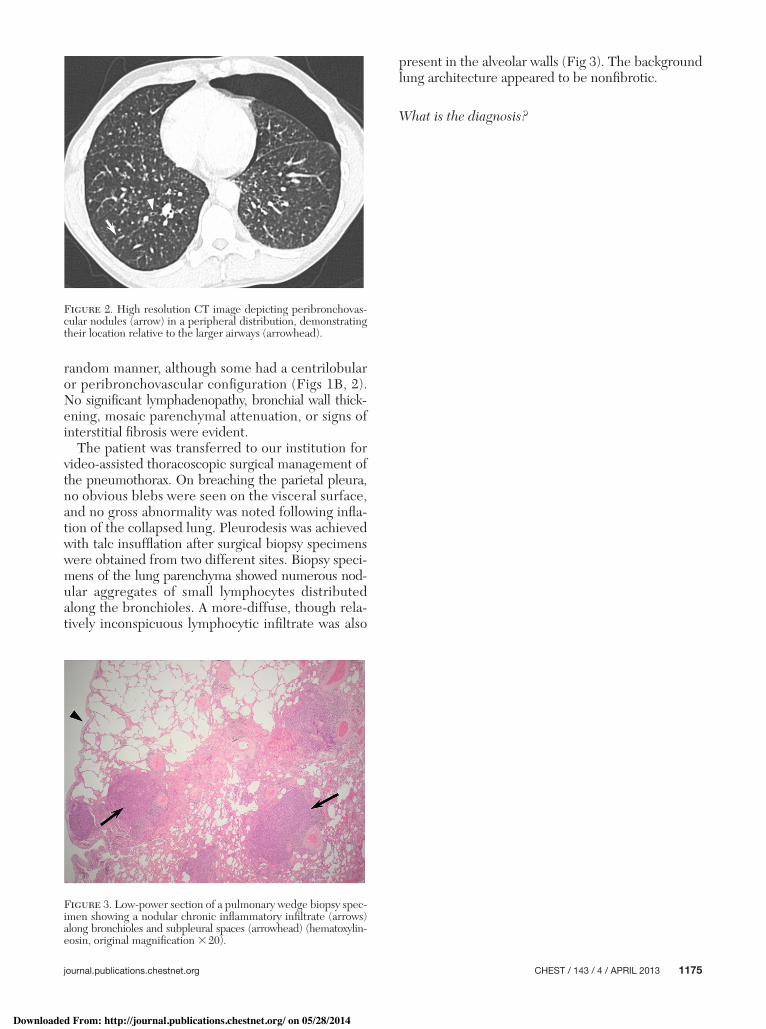
The patient was transferred to our institution for video-assisted thoracoscopic surgical management of the pneumothorax. On breaching the parietal pleura, no obvious blebs were seen on the visceral surface, and no gross abnormality was noted following infl a-tion of the collapsed lung. Pleurodesis was achieved with talc insuffl ation after surgical biopsy specimens were obtained from two different sites. Biopsy speci-mens of the lung parenchyma showed numerous nod-ular aggregates of small lymphocytes distributed along the bronchioles. A more-diffuse, though rela-tively inconspicuous lymphocytic infi ltrate was also
present in the alveolar walls ( Fig 3 ). The background lung architecture appeared to be nonfi brotic.
What is the diagnosis?
Figure 2. High resolution CT image depicting peribronchovas-cular nodules (arrow) in a peripheral distribution, demonstrating their location relative to the larger airways (arrowhead).
Figure 3. Low-power section of a pulmonary wedge biopsy spec-imen showing a nodular chronic infl ammatory infi ltrate (arrows) along bronchioles and subpleural spaces (arrowhead) (hematoxylin-eosin, original magnifi cation 3 20).
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014
1176 Postgraduate Education Corner
Diagnosis: Follicular bronchiolitis secondary to infection with HIV
Discussion Clinical Discussion
Follicular bronchiolitis (FB) is an unusual disorder characterized histologically by hyperplastic peri-bronchiolar lymphoid follicles containing reactive germinal centers. It is believed to arise from either excessive polyclonal stimulation of bronchus-associated lymphoid tissue or an aberrant systemic immune state. 1 Although an idiopathic form is recognized, FB is more commonly associated with connective tissue diseases; immunodefi cient states, including HIV dis-ease; hypersensitivity reactions; or airway infection. 2 , 3 Milder degrees of reactive follicular hyperplasia can occur in bronchiectasis, COPD, and even asthma. 4 It has been proposed that FB and lymphocytic inter-stitial pneumonia (LIP) occupy the same disease con-tinuum and share certain pathologic aspects; both represent examples of pulmonary lymphoid hyper-plasia. 4 , 5
Although FB may occur at any age, its disease course varies between children and adults. 6 , 7 Patients without clear immunologic dysfunction tend to be middle-aged or older. 6 In most patients, FB presents as progressive dyspnea over weeks or months and is associated with lassitude, weight loss, fever, or recur-rent symptoms of infection. In contrast, the clinical history in the present patient was short and evolved quickly. Pulmonary function tests in FB may be normal or show an obstructive, restrictive, or mixed ventila-tory defect, frequently with decreased lung diffus ing capacity. 2 , 8
In the present patient, screening for connective tissue disease, lymphoma, and other forms of immu-nologic disease was negative. Evidence of acquired immunodefi ciency was confi rmed by positive enzyme-linked immunosorbent assay for HIV-1 and a plasma HIV RNA load of 141,000 copies/mL. HIV genotyp-ing revealed the presence of wild-type virus with no evidence of antiretroviral-associated genetic muta-tions or drug resistance. Screening for opportunistic infections did not detect any AIDS-defi ning diag-noses; however, an initial CD4 count of 287 cells/ m L (13%) suggested an increased susceptibility to bacte-rial infections and lymphoproliferative disorders. 3 The patient had not developed overt manifestations of HIV until the acute pneumothorax that ultimately led to the diagnosis of FB. Two months after com-mencing highly active antiretroviral therapy (HAART), his CD4 count normalized, but he subsequently devel-oped pneumococcal pneumonia, which warranted a brief hospitalization. The patient remains well on
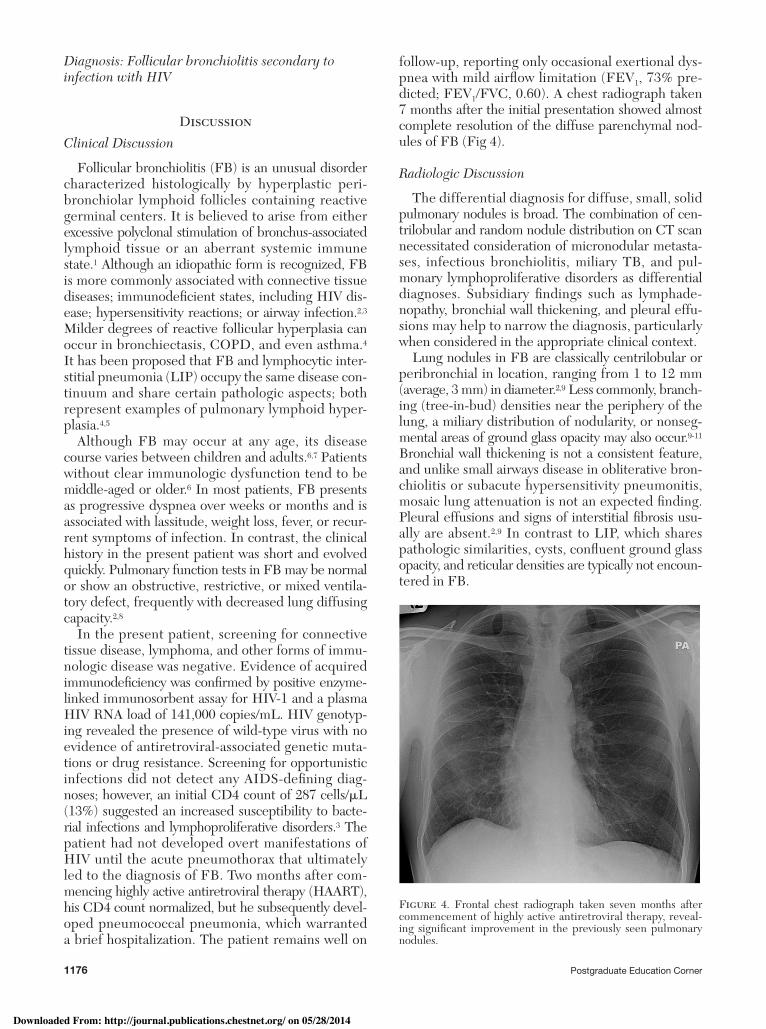
Figure 4. Frontal chest radiograph taken seven months after commencement of highly active antiretroviral therapy, reveal-ing signifi cant improvement in the previously seen pulmonary nodules.
follow-up, reporting only occasional exertional dys-pnea with mild airfl ow limitation (FEV 1 , 73% pre-dicted; FEV 1 /FVC, 0.60). A chest radiograph taken 7 months after the initial presentation showed almost complete resolution of the diffuse parenchymal nod-ules of FB ( Fig 4 ).
Radiologic Discussion
The differential diagnosis for diffuse, small, solid pulmonary nodules is broad. The combination of cen-trilobular and random nodule distribution on CT scan necessitated consideration of micronodular metasta-ses, infectious bronchiolitis, miliary TB, and pul-monary lymphoproliferative disorders as differential diagnoses. Subsidiary fi ndings such as lymphade-nopathy, bronchial wall thickening, and pleural effu-sions may help to narrow the diagnosis, particularly when considered in the appropriate clinical context.
Lung nodules in FB are classically centrilobular or peribronchial in location, ranging from 1 to 12 mm (average, 3 mm) in diameter. 2 , 9 Less commonly, branch-ing (tree-in-bud) densities near the periphery of the lung, a miliary distribution of nodularity, or nonseg-mental areas of ground glass opacity may also occur. 9 - 11 Bronchial wall thickening is not a consistent feature, and unlike small airways disease in obliterative bron-chiolitis or subacute hypersensitivity pneumonitis, mosaic lung attenuation is not an expected fi nding. Pleural effusions and signs of interstitial fi brosis usu-ally are absent. 2 , 9 In contrast to LIP, which shares pathologic similarities, cysts, confl uent ground glass opacity, and reticular densities are typically not encoun-tered in FB.
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014

CHEST / 143 / 4 / APRIL 2013 1177journal.publications.chestnet.org
Pathologic Discussion
Precise histologic characterization is necessary to distinguish FB from other bronchiolar disorders with similar radiologic appearances ( Table 1 ). In this case, surgical biopsy specimens from two different lobes demonstrated numerous peribronchovascular lymphoid follicles that contained polyclonal CD20 1 , CD79a 1 , and BCL2 2 B cells. Many bronchioles appeared com-pressed by these follicles, and a mild infi ltrate com-prising T cells (CD4 1 and CD8 1 ) and plasma cells
Table 1 —Comparison of Salient Features of FB With Other Potential Differential Diagnoses 4,12,13
Characteristic FB LIP NLH BALT Lymphoma
Clinical associations Collagen vascular disorders (eg, rheumatoid arthritis), immunodefi ciency syndromes, hypersensitivity disorders, and infl ammatory airway conditions (eg, bronchiectasis)
Collagen vascular disorders (eg, Sjögren disease), hematologic diseases, immunosuppressive states, and idiopathic entity. Polyclonal hypergammaglobulinemia found in 80% cases.
Rare form of localized reactive lymphoid proliferation; considerable diagnostic overlap with low-grade BALT lymphoma. No consistent association with collagen vascular disease reported
Rare extranodal non-Hodgkin’s lymphoma. Postulated association with microbe-induced immunogenic stimulation ( Cytomegalovirus , Pneumocystis jiroveci , Mycobacterium species, among others)
Age range Children to adults Infants to elderly, but most common between fourth and sixth decades
Adults (median age, 65 years)
Most common in fi fth to sixth decades
CT scan fi ndings Centrilobular ! peribronchiolar nodules, which commonly are , 3 mm but can be as large as 12 mm.
Solid nodules (may be centrilobular) associated with randomly distributed cysts and ground glass opacities.
Unilateral or bilateral, a discrete solitary mass-like lesion in two-thirds of cases.
Well-circumscribed single or multiple randomly distributed nodules (larger than in LIP and FB) or consolidation (which may contain air bronchograms or bubble-like lucencies).
Pathologic features Typically peribronchial or peribronchiolar lymphoid follicles with reactive germinal centers. May cause partial bronchiolar obstruction, resulting in OP-like changes, obstructive pneumonitis, and intraluminal neutrophilic exudate.
Diffuse process resulting in dense interstitial infi ltrate of lymphocytes (principally T cells). Focal lymphoid follicles (usually B cells) occur in a peribronchial and peribronchiolar distribution.
Polymorphic infi ltrate, including randomly distributed benign follicles and interfollicular plasma cells. Variable fi brosis may be present. Tumor-like growth also present, often subpleural, single, or multiple, up to 60 mm in size.
Monomorphic infi ltrate (mainly B cells), centrocyte-like, or monocytoid cells ! plasmacytic differentiation. Lymphoid follicles are focal, randomly distributed, and may show mantle zone colonization. Tumor-like growth causes destruction of alveolar architecture. Lymphangitic growth is present, and lymphoepithelial lesions are common.
Spread usually is limited to bronchovascular bundles with minor interstitial component. Tumor-like and lymphangitic growth rare.
Other recognized features include type 2 pneumocyte hyperplasia, focal lymphocytic vasculitis, focal OP-like changes, variable interstitial fi brosis, poorly formed granulomas, and amyloid deposition (rare).Tumor-like and lymphangitic growth absent.
Other recognized features are intranuclear inclusions (Dutcher bodies), hyaline sclerosis, and giant lamellar bodies in alveolar spaces. Granulomas rarely occur.
Differential diagnoses to consider
Occasional cases overlap with LIP
MALT-type MZL, cellular NSIP, and hypersensitivity pneumonitis
MALT-type MZL, infl ammatory myofi broblastic tumor
LIP
BALT 5 bronchus-associated lymphoid tissue; FB 5 follicular bronchiolitis; LIP 5 lymphocytic interstitial pneumonia; MALT 5 mucosa-associated lymphoid tissue; MZL 5 marginal zone lymphoma; NLH 5 nodular lymphoid hyperplasia; NSIP 5 nonspecifi c interstitial pneumonia; OP 5 orga-nizing pneumonia.
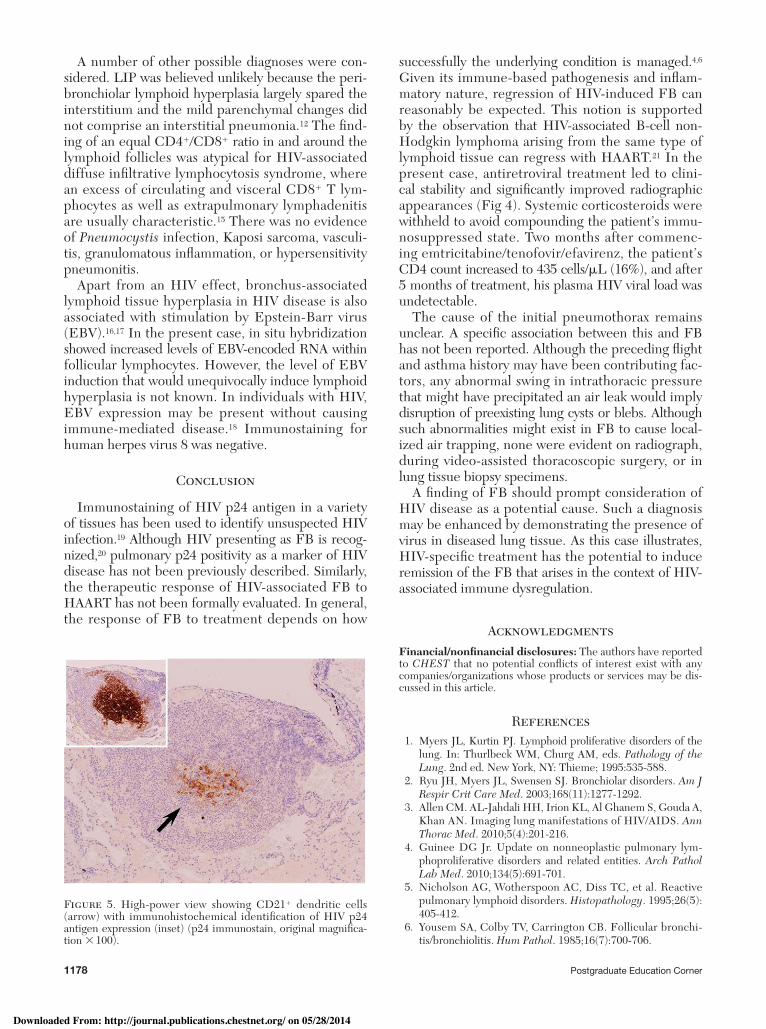
was present in adjacent alveolar septae. Crucially, some follicular germinal centers were distorted by CD21 1 dendritic cells containing visible quantities of HIV p24 capsid protein ( Fig 5 ). Detection of this anti-gen, absent in cells outside the lymphoid aggregates, indicated a causal association between HIV dis ease and the resultant bronchiolar pathology. In asymp-tomatic individuals with HIV seropositive dis ease, the presence of HIV-1 DNA in nodal germinal cen-ters has been linked to subsequent development of lymphoid hyperplasia and B-cell lymphomas. 14
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014
1178 Postgraduate Education Corner
A number of other possible diagnoses were con-sidered. LIP was believed unlikely because the peri-bronchiolar lymphoid hyperplasia largely spared the interstitium and the mild parenchymal changes did not comprise an interstitial pneumonia. 12 The fi nd-ing of an equal CD4 1 /CD8 1 ratio in and around the lymphoid follicles was atypical for HIV-associated diffuse infi ltrative lymphocytosis syndrome, where an excess of circulating and visceral CD8 1 T lym-phocytes as well as extrapulmonary lymphadenitis are usually characteristic. 15 There was no evidence of Pneumocystis infection, Kaposi sarcoma, vasculi-tis, granulomatous infl ammation, or hypersensitivity pneumonitis.
Apart from an HIV effect, bronchus-associated lymphoid tissue hyperplasia in HIV disease is also associated with stimulation by Epstein-Barr virus (EBV). 16 , 17 In the present case, in situ hybridization showed increased levels of EBV-encoded RNA within follicular lymphocytes. However, the level of EBV induction that would unequivocally induce lymphoid hyperplasia is not known. In individuals with HIV, EBV expression may be present without causing immune-mediated disease. 18 Immunostaining for human herpes virus 8 was negative.
Conclusion
Immunostaining of HIV p24 antigen in a variety of tissues has been used to identify unsuspected HIV infection. 19 Although HIV presenting as FB is recog-nized, 20 pulmonary p24 positivity as a marker of HIV disease has not been previously described. Similarly, the therapeutic response of HIV-associated FB to HAART has not been formally evaluated. In general, the response of FB to treatment depends on how
Figure 5. High-power view showing CD21 1 dendritic cells (arrow) with immunohistochemical identifi cation of HIV p24 antigen expression (inset) (p24 immunostain, original magnifi ca-tion 3 100).
successfully the underlying condition is managed. 4 , 6 Given its immune-based pathogenesis and infl am-matory nature, regression of HIV-induced FB can reasonably be expected. This notion is supported by the observation that HIV-associated B-cell non-Hodgkin lymphoma arising from the same type of lymphoid tissue can regress with HAART. 21 In the present case, antiretroviral treatment led to clini-cal stability and signifi cantly improved radiographic appearances ( Fig 4 ). Systemic corticosteroids were withheld to avoid compounding the patient’s immu-nosuppressed state. Two months after commenc-ing emtricitabine/tenofovir/efavirenz, the patient’s CD4 count increased to 435 cells/ m L (16%), and after 5 months of treatment, his plasma HIV viral load was undetectable.
The cause of the initial pneumothorax remains unclear. A specifi c association between this and FB has not been reported. Although the preceding fl ight and asthma history may have been contributing fac-tors, any abnormal swing in intrathoracic pressure that might have precipitated an air leak would imply disruption of preexisting lung cysts or blebs. Although such abnormalities might exist in FB to cause local-ized air trapping, none were evident on radiograph, during video-assisted thoracoscopic surgery, or in lung tissue biopsy specimens.
A fi nding of FB should prompt consideration of HIV disease as a potential cause. Such a diagnosis may be enhanced by demonstrating the presence of virus in diseased lung tissue. As this case illustrates, HIV-specifi c treatment has the potential to induce remission of the FB that arises in the context of HIV-associated immune dysregulation.
Acknowledgments Financial/nonfi nancial disclosures: The authors have reported to CHEST that no potential confl icts of interest exist with any companies/organizations whose products or services may be dis-cussed in this article .
References 1 . Myers JL , Kurtin PJ . Lymphoid proliferative disorders of the
lung . In: Thurlbeck WM , Churg AM , eds . Pathology of the Lung . 2nd ed . New York, NY : Thieme ; 1995 : 535 - 588 .
2 . Ryu JH , Myers JL , Swensen SJ . Bronchiolar disorders . Am J Respir Crit Care Med . 2003 ; 168 ( 11 ): 1277 - 1292 .
3 . Allen CM . AL-Jahdali HH, Irion KL, Al Ghanem S, Gouda A, Khan AN. Imaging lung manifestations of HIV/AIDS . Ann Thorac Med . 2010 ; 5 ( 4 ): 201 - 216 .
4 . Guinee DG Jr . Update on nonneoplastic pulmonary lym-phoproliferative disorders and related entities . Arch Pathol Lab Med . 2010 ; 134 ( 5 ): 691 - 701 .
5 . Nicholson AG , Wotherspoon AC , Diss TC , et al . Reactive pulmonary lymphoid disorders . Histopathology . 1995 ; 26 ( 5 ): 405 - 412 .
6 . Yousem SA , Colby TV , Carrington CB . Follicular bronchi-tis/bronchiolitis . Hum Pathol . 1985 ; 16 ( 7 ): 700 - 706 .
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014

CHEST / 143 / 4 / APRIL 2013 1179journal.publications.chestnet.org
7 . Kinane BT , Mansell AL , Zwerdling RG , Lapey A , Shannon DC . Follicular bronchitis in the pediatric population . Chest . 1993 ; 104 ( 4 ): 1183 - 1186 .
8 . Aerni MR , Vassallo R , Myers JL , Lindell RM , Ryu JH . Follic-ular bronchiolitis in surgical lung biopsies: clinical implica-tions in 12 patients . Respir Med . 2008 ; 102 ( 2 ): 307 - 312 .
9 . Howling SJ , Hansell DM , Wells AU , Nicholson AG , Flint JDA , Müller NL . Follicular bronchiolitis: thin-section CT and histologic fi ndings . Radiology . 1999 ; 212 ( 3 ): 637 - 642 .
10 . Koch JS , Whitman GJ , Chew FS . Bronchus-associated lym-phoid tissue hyperplasia of the lung . AJR Am J Roentgenol . 1997 ; 168 ( 4 ): 1044 .
11 . Pipavath SJ , Lynch DA , Cool C , Brown KK , Newell JD . Radiologic and pathologic features of bronchiolitis . AJR Am J Roentgenol . 2005 ; 185 ( 2 ): 354 - 363 .
12 . Travis WD , Galvin JR . Non-neoplastic pulmonary lymphoid lesions . Thorax . 2001 ; 56 ( 12 ): 964 - 971 .
13 . Arnaoutakis K , Oo TH . Bronchus-associated lymphoid tis-sue lymphomas . South Med J . 2009 ; 102 ( 12 ): 1229 - 1233 .
14 . Becker JL , Steigbigel RT , Nuovo GJ . In situ detection of PCR-amplifi ed HIV-1 and EBV nucleic acids in hyperplastic lymph nodes and in AIDS-related lymphoma . J Histochem Cytochem . 1996 ; 44 ( 10 ): 1085 - 1089 .
15 . Itescu S , Brancato LJ , Buxbaum J , et al . A diffuse infi ltrative CD8 lymphocytosis syndrome in human immunodefi ciency
virus (HIV) infection: a host immune response associated with HLA-DR5 . Ann Intern Med . 1990 ; 112 ( 1 ): 3 - 10 .
16 . Koss MN . Pulmonary lymphoid disorders . Semin Diagn Pathol . 1995 ; 12 ( 2 ): 158 - 171 .
17 . Greiner T , Armitage JO , Gross TG . Atypical lymphoprolifera-tive diseases . Hematology Am Soc Hematol Educ Program . 2000 ; 2000 ( 1 ): 133 - 146 .
18 . Toro AA , Altemani AM , da Silva MT , Morcillo AM , Vilela MM . Epstein-Barr virus (EBV) gene expression in interstitial pneu-monitis in Brazilian human immunodefi ciency virus-1-infected children: is EBV associated or not? Pediatr Dev Pathol . 2010 ; 13 ( 3 ): 184 - 191 .
19 . Moonim MT , Alarcon L , Freeman J , Mahadeva U , van der Walt JD , Lucas SB . Identifying HIV infection in diagnostic histopathology tissue samples—the role of HIV-1 p24 immu-nohistochemistry in identifying clinically unsuspected HIV infection: a 3-year analysis . Histopathology . 2010 ; 56 ( 4 ): 530 - 541 .
20 . Exley CM , Suvarna SK , Matthews S . Follicular bronchiolitis as a presentation of HIV . Clin Radiol . 2006 ; 61 ( 8 ): 710 - 713 .
21 . Baraboutis IG , Marinos L , Lekakis LJ , et al . Long-term com-plete regression of nodal marginal zone lymphoma trans-formed into diffuse large B-cell lymphoma with highly active antiretroviral therapy alone in human immunodefi ciency virus infection . Am J Med Sci . 2009 ; 338 ( 6 ): 517 - 521 .
Downloaded From: http://journal.publications.chestnet.org/ on 05/28/2014