NephSAP Volume 16, Number 1 - Electrolytes and … de... · NephSAP Nephrology Self-Assessment...
118
NephSAP Nephrology Self-Assessment Program ® Volume 16 • Number 1 • March 2017 Electrolytes and Acid-Base Disorders Co-Editors: Asghar Rastegar, MD Manoocher Soleimani, MD Co-Directors: Gerald Hladik, MD Jerry Yee, MD
-
Upload
phungduong -
Category
Documents
-
view
288 -
download
18
Transcript of NephSAP Volume 16, Number 1 - Electrolytes and … de... · NephSAP Nephrology Self-Assessment...
-
NephSAPNephrology Self-Assessment Program
Volume 16 Number 1 March 2017
Electrolytes and Acid-Base DisordersCo-Editors:
Asghar Rastegar, MD
Manoocher Soleimani, MD
Co-Directors: Gerald Hladik, MDJerry Yee, MD
-
CO-DIRECTOR,NephSAPGerald A. Hladik, MDUniversity of North Carolina at Chapel HillChapel Hill, NC
CO-DIRECTOR,NephSAPJerry Yee, MD, FASNHenry Ford HospitalDetroit, MI
MANAGING EDITORGisela Deuter, BSN, MSAWashington, DC
ASSOCIATE EDITORSDebbie L. Cohen, MDUniversity of Pennsylvania School of MedicinePhiladelphia, PA
Richard J. Glassock, MDProfessor Emeritus, The David Geffen School ofMedicine at the University of CaliforniaLos Angeles, CA
Stanley Goldfarb, MDUniversity of Pennsylvania School of MedicinePhiladelphia, PA
Karen A. Griffin, MD, FASNLoyola University Medical CenterMaywood, IL
Jay L. Koyner, MDUniversity of ChicagoChicago, IL
Holly J. Kramer, MDLoyola University Medical CenterMaywood, IL
Ruediger W. Lehrich, MDDuke UniversityDurham, NC
Kevin J. Martin, MBBChSt. Louis University School of MedicineSt. Louis, MO
John P. Middleton, MDDuke UniversityDurham, NC
Sankar D. Navaneethan, MD, MPHBaylor College of MedicineHouston, TX
Asghar Rastegar, MDYale School of MedicineNew Haven, CT
Brad H. Rovin, MDOhio State University Medical CenterColumbus, OH
Manoocher Soleimani, MDUniversity of CincinnatiCincinnati, OH
Charuhas V. Thakar, MDUniversity of CincinnatiCincinnati, OH
John P. Vella, MDMaine Medical CenterPortland, ME
Alexander C. Wiseman, MDUniversity of Colorado at DenverDenver, CO
FOUNDING EDITORSRichard J. Glassock, MDEditor-in-Chief Emeritus
Robert G. Narins, MD
PrefaceNephSAP is one of the premiere educational activities of the American Society ofNephrology (ASN). Its primary goals are self-assessment, education, and the provision ofContinuingMedical Education (CME) credits andMaintenance of Certification (MOC) pointsfor individuals certified by the American Board of Internal Medicine. Members of the ASNreceive NephSAP electronically through the ASN website by clicking on the NephSAP linkunder Education and Meetings tab.
EDUCATION: Medical and nephrologic information continually accrues at a rapid pace.Bombarded from all sides with demands on their time, busy practitioners, academicians, andtrainees at all levels are increasingly challenged to review and understand new and evolvingevidence. Each bimonthly issue of NephSAP is dedicated to a specific theme, i.e., to a specificarea of clinical nephrology, hypertension, dialysis, and transplantation, and consists of aneditorial, a syllabus, and self-assessment questions, to serve as a self-study device. Over thecourse of 24 months, all clinically relevant and key elements of nephrology will be reviewedand updated. The authors of each issue digest, assimilate, and interpret key studies publishedsince the release of the previous issues and integrate this new material with the body ofexisting information. Occasionally a special edition is produced to cover an area not ordinarilyaddressed by core issues of NephSAP.
SELF-ASSESSMENT:Thirty, single-best-answer questionswill follow the 80 to 100 pages ofsyllabus text. The examination is available online with immediate feedback. Those answering75% correctly will receive MOC and CME credit, and receive the answers to all the questionsalong with brief discussions and an updated bibliography. Members will find a new areareviewed every 2 months, and they will be able to test their understanding with our quiz. Thisformat will help readers stay up to date in developing areas of clinical nephrology,hypertension, dialysis, and transplantation, and the review and update will support thosetaking certification and recertification examinations.
CONTINUINGMEDICALEDUCATION:Most state and local medical agencies as well ashospitals are demanding documentation of requisite CME credits for licensure and for staffappointments. A maximum of 48 credits annually can be obtained by successfully completingthe NephSAP examinations. In addition, individuals enrolled in Maintenance of Certification(MOC) through the American Board of Internal Medicine may obtain points towardMOC bysuccessfully completing the self-assessment examination of NephSAP.
This paper meets the requirements of ANSI/NISO Z39.48-1921 (Permanence of Paper),effective with July 2002, Vol. 1, No. 1.
NephSAP
2017 by The American Society of Nephrology
CONTRIBUTING AUTHORSNamrata Kirshnan, MDYale School of MedicineNew Haven, CT
Karthik Ramani, MDUniversity of Cincinnati School of MedicineCincinnati, OH
-
Editorial1 Advances in Chronic Potassium Control: Prognostic
Implications for CKDDavid B. Mount
Syllabus10 NephSAP, Volume 16, Number 1, March 2017
Electrolytes and Acid-Base DisordersAsghar Rastegar, Manoocher Soleimani, Namrata
Krishnan, Karthik Ramani
10 Learning Objectives
10 Update on Fluid Therapy in Patients with Sepsis
10 Fluid Volume
11 Fluid Type
13 Diuretic Use in Congestive Heart Failure andCardiorenal Syndrome
13 Basic Concepts
14 Loop Diuretic Braking Phenomena and Resistance
15 Furosemide versus Torsemide
15 Clinical Studies Comparing Furosemide andTorsemide in CHF
16 Using Diuretic in Cardiorenal Syndrome
18 Hyponatremia Diagnosis and Treatment: Real WorldExperience
21 Use of Tolvaptan in Treatment of Hyponatremia Dueto Syndrome of Inappropriate Antidiuretic Hormone
21 Patient Presentation
23 Cost of Treatment with Tolvaptan
23 Exercise-Associated Hyponatremia
23 Patient Presentation
25 Clinical Presentation and Treatment
26 Desmopressin-Induced Hyponatremia
26 Patient Presentation
28 Hypernatremia in Critically Ill Patients
28 Epidemiology
28 Clinical Outcome
29 Pathogenesis
30 Treatment of Hypernatremia in ICU Settings
32 Lithium and Nephrogenic Diabetes Insipidus
33 Potassium Homeostasis
33 Evolving Concepts in Renal Potassium Excretion
35 Circadian Rhythm of Potassium Excretion
37 Distal Nephron Potassium Handling
40 Epidemiologic Significance of Potassium Disorders
43 Hypokalemia, Metabolic Alkalosis, andHypertension
47 Hypokalemia, Metabolic Alkalosis, andNormotension
47 Patient Presentation
48 Bartter Syndrome
49 Gitelman Syndrome
50 Drug-Induced Bartter-like and Gitelman-likeSyndromes
51 Diagnosis of GS and BS
51 Treatment of GS/BS
52 GS and Pregnancy
52 GS and Hypertension
54 Role of Thiazides in Treatment of Post-TransplantCalcineurin InhibitorInduced Hyperkalemia
56 Treatment of Hyperkalemia
56 Patient Presentation
58 Treatment of Hyperkalemia
58 Treatment of Acute Life-Threatening Hyperkalemia
58 Potassium Binding Resins
58 Sodium Polystyrene Sulfonate
60 Patiromer
64 Sodium Zirconium Cyclosilicate
67 Serum Bicarbonate and Mortality
68 Lactic Acidosis and Sepsis
70 Metformin-Associated Lactic Acidosis
70 Patient Presentation and Discussion
71 Incidence of MALA
Volume 16, Number 1, March 2017
-
72 New Food and Drug Administration GuidelinesRegarding Metformin Use in Patients with CKD
73 Treatment and Outcome of MALA
74 Linezolid-Associated Lactic Acidosis
75 Management of Metabolic Alkalosis ComplicatingChronic Respiratory Acidosis
77 Metabolic Alkalosis
77 Factors Regulating Bicarbonate Excretion in theKidney and Their Role in the Maintenance ofMetabolic Alkalosis
78 Metabolic Alkalosis: Generation and Maintenance
78 Chloride Depletion and Metabolic Alkalosis inVolume-Depleted States
78 Potassium Depletion and the Maintenance ofMetabolic Alkalosis
79 Decreased GFR and the Impairment ofBicarbonate Elimination in MetabolicAlkalosis
79 Renin-Angiotensin-Aldosterone Activation: Rolein the Maintenance of Metabolic Alkalosis
79 Decreased HCO32 Secretion in Cortical Collecting
Duct: Role in the Maintenance of MetabolicAlkalosis
81 Metabolic Alkalosis Induced by Aminoglycosides inCystic Fibrosis
81 Metabolic Alkalosis in Patients with PendredSyndrome
82 Mechanism of Metabolic Alkalosis in Patients withPendred Syndrome
83 Nonanion Gap Metabolic Acidosis
84 Discussion
85 Overview of RTA: Roles of Acid-Base Transporters
85 Acid-Base Regulation by the Proximal Tubule
86 Acid-Base Regulation by the Collecting Duct
89 Discussion
89 Pathophysiologic Approach to HyperchloremicAcidosis
89 dRTA (Type 1)
89 Hereditary dRTA
89 A1 Mutations
90 H1-ATPase Mutations
90 CAII Mutations
90 Acquired dRTA
91 dRTA: Diagnosis and Treatment
91 Proximal RTA (Type 2)
92 Hereditary pRTA
93 Acquired pRTA
93 pRTA: Diagnosis and Treatment
93 Hyperkalemic RTA
94 RTA and Nephrolithiasis
CME Self-Assessment Questions98 NephSAP, Volume 16, Number 1, March 2017
Electrolytes and Acid-Base Disorders
Upcoming IssuesAcute Kidney Injury and Critical Care NephrologyJay L. Koyner, MD and Charuhas V. Thakar, MD
May 2017
Chronic Kidney Disease and ProgressionHolly J. Kramer, MD and Sankar D. Navaneethan, MD
September 2017
TransplantationJohn P. Vella, MD and Alexander C. Wiseman, MDNovember 2017
HypertensionDebbie L. Cohen, MD and Karen A. Griffin, MD
March 2018
Volume 16, Number 1, March 2017
-
The Editorial Board of NephSAP and KSAP extends its sincere appreciation to the following reviewers. Their efforts and insights help improvethe quality of these postgraduate education offerings.
NephSAP Review PanelMustafa Ahmad, MD, FASNKing Fahad Medical CityRiyadh, Saudi Arabia
Nasimul Ahsan, MD, FASNUniversity of Florida andOscar G. Johnson Veteran AffairsMedical CenterIron Mountain, MI
Jafar Al-Said, MD, FASNBahrain Specialist HospitalManama, Bahrain
Carmichael Angeles, MD, FASNJohn T. Mather Memorial HospitalStony Brook, NY
Kisra Anis, MBBSJacobi Medical Center/Albert Einstein College of MedicineBronx, NY
Naheed Ansari, MD, FASNJacobi Medical Center/Albert EinsteinCollege of MedicineBronx, NY
Nabeel Aslam, MD, FASNMayo Clinic FloridaJacksonville, FL
Nisha Bansal, MDUniversity of WashingtonSeattle, WA
Krishna M. Baradhi, MDUniversity of OklahomaTulsa, OK
Emmy Bell, MD, MSPHUniversity of Alabama at BirminghamBirmingham, AL
Bruce E. Berger, MDCase Western Reserve UniversityCleveland, OH
Mona B. Brake, MDRobert J. Dole Veteran AffairsMedical CenterWichita, KS
Pooja Budhiraja, MBBSUniversity of Kansas Medical CenterKansas City, KS
Ruth C. Campbell, MDMedical University of South CarolinaCharleston, SC
Chia-Ter Chao, MDNational Taiwan University HospitalTaipei, Taiwan
Chokchai Chareandee, MD, FASNUniversity of MinnesotaMinneapolis, MN
Joline L. Chen, MDLong Beach Veteran AffairsHealthcare SystemOrange, CA
Karen Ching, MDHawaii Permanente Medical GroupHonolulu. HI
W. James Chon, MDUniversity of Arkansas for Medical SciencesLittle Rock, AR
Jason Cobb, MDEmory University School of MedicineAtlanta, GA
Armando Coca, MD, PhDHospital Clnico UniversitarioValladolid, Spain
Scott D. Cohen, MD, FASNGeorge Washington UniversityWashington, DC
Beatrice Concepcion, MDVanderbilt University Medical CenterNashville, TN
Gabriel Contreras, MDUniversity of MiamiMiami, FL
Patrick Cunningham, MDUniversity of ChicagoChicago, IL
Kevin A. Curran, MDKevin A. Curran, MD, PACanton, TX
Rajiv Dhamija, MDRancho Los Amigos NationalRehabilitation CenterDowney, CA
Alejandro Diez, MDThe Ohio State UniversityColumbus, OH
John J. Doran, MDEmory School of MedicineAtlanta, GA
Randa A. El Husseini, MD, FASNHealthPartners Medical GroupSt. Paul, MN
Mahmoud El-Khatib, MDUniversity of CincinnatiCincinnati, OH
Pedram Fatehi, MDStanford MedicinePalo Alto, CA
William H. Fissell, MDVanderbilt University Medical CenterNashville, TN
D. Kevin Flood, MDMike OCallaghan Federal Medical CenterNellis AFB, NV
Lynda A. Frassetto, MD, FASNUniversity of California atSan FranciscoSan Francisco, CA
Tibor Fulop, MDUniversity of Mississippi Medical CenterJackson, MS
Maurizio Gallieni, MD, FASNUniversity of MilanoMilano, Italy
Duvuru Geetha, MD, FASNJohns Hopkins UniversityBaltimore, MD
Ilya Glezerman, MDMemorial Sloan Kettering Cancer CenterNew York, NY
Carl S. Goldstein, MD, FASNRutgers UniversityNew Brunswick, NJ
Basu Gopal, MBBS, FASNRoyal Adelaide HospitalAdelaide, Australia
Steven Gorbatkin, MD, PhDEmory University andAtlanta Veteran Affairs Medical CenterDecatur, GA
Aditi Gupta, MDUniversity of Kansas Medical CenterKansas City, KS
Susan Hedayati, MDUniversity of Texas SouthwesternDallas, TX
Marie C. Hogan, MBBCh, PhDMayo ClinicRochester, MN
Susie Hu, MDWarren Alpert Medical School of BrownUniversity,Rhode Island HospitalProvidence, RI
Volume 16, Number 1, March 2017
-
Edmund Huang, MDUniversity of California atLos Angeles School of MedicineLos Angeles, CA
Ekambaram Ilamathi, MD, FASNNorthwell Health, Southside HospitalBayshore, NY
Joshua M. Kaplan, MDRutgers New Jersey Medical SchoolNewark, NJ
Amir Kazory, MDUniversity of FloridaGainesville, FL
Quresh T. Khairullah, MDSt. Clair NephrologyRoseville, MI
Apurv Khanna, MDState University of New YorkUpstate Medical UniversitySyracuse, NY
Yong-Lim Kim, MD, PhDKyungpook National University HospitalDaegu, South Korea
Nitin V. Kolhe, MD, FASNDerby Teaching Hospital NHS TrustDerby, Derbyshire, UK
Farrukh M. Koraishy, MD, PhDSt. Louis UniversitySt. Louis, MO
Eugene C. Kovalik, MDDuke University Medical CenterDurham, NC
Steven Kraft, MDWestern NephrologyLafayette, CO
Vineeta Kumar, MDUniversity of Alabama at BirminghamBirmingham, AL
Sarat Kuppachi, MDUniversity of IowaIowa City, IA
Norbert H. Lameire, MD, PhDUniversity HospitalGent, East Flanders, Belgium
Sheron Latcha, MDMemorial Sloan Kettering Cancer CenterNew York, NY
Vincent Weng Seng Lee, MBBS, PhDWestmead HospitalSydney, NSWAustralia
Paolo Lentini, MD, PhDSt. Bortolo HospitalBassano del Grappa, Italy
Oliver Lenz, MDUniversity of Miami Health SystemMiami, FL
Tingting Li, MDWashington University in St. LouisSt. Louis, MO
Orfeas Liangos, MD, FASNKlinikum CoburgCoburg, Bayern, Germany
Michael Lioudis, MDCleveland Clinic NephrologyCleveland, OH
Ajit Mahapatra, MDThe Permanente Medical GroupSanta Clara, CA
A. Bilal Malik, MBBSUniversity of WashingtonSeattle, WA
Jolanta Malyszko, MD, PhDMedical UniversityBialystok, Poland
Ernest Mandel, MDBrigham and Womens HospitalBoston, MA
Naveed N. Masani, MDWinthrop University HospitalMineola, NY
Teri Jo Mauch, MD, PhDUniversity of Nebraska College of MedicineOmaha, NE
Hanna W. Mawad, MD, FASNUniversity of KentuckyLexington, KY
Ellen T. McCarthy, MDUniversity of Kansas Medical Center,Kidney InstituteKansas City, KS
Kirtida Mistry, MBBChChildrens National Medical CenterWashington, DC
Lawrence S. Moffatt, MDCarolinas Medical CenterCharlotte, NC
David B. Mount, MDBrigham and Womens Hospital,Harvard Medical SchoolBoston, MA
Thangamani Muthukumar, MDWeill Cornell MedicineNew York, NY
Mohanram Narayanan, MDBaylor Scott & White HealthTemple, TX
Macaulay A. Onuigbo, MDMayo ClinicRochester, MN
Rosemary Ouseph, MDSt. Louis UniversityWebster Groves, MO
Todd Pesavento, MDOhio State UniversityColumbus, OH
Phuong-Thu Pham, MDDavid Geffen School of Medicine at UCLALos Angeles, CA
Pairach Pintavorn, MD, FASNEast Georgia Kidney and HypertensionAugusta, GA
Roberto Pisoni, MDMedical University of South CarolinaCharleston, SC
James M. Pritsiolas, MD, FASNCarePoint Health - Bayonne Medical CenterBayonne, NJ
Paul H. Pronovost, MD, FASNYale University School of MedicineWaterbury, CT
Mohammad A. Quasem, MD, FASNState University of New York MedicalUniversityBinghamton, NY
Wajeh Y. Qunibi, MDUniversity of TexasHealth Science CenterSan Antonio, TX
Pawan K. Rao, MD, FASNSt. Josephs Hospital and Health CenterSyracuse, NY
Hernan Rincon-Choles, MDCleveland Clinic FoundationCleveland, OH
Dario Roccatello, MDSan Giovanni Hospital andUniversity of TorinoTorino, Italy
Helbert Rondon-Berrios, MD, FASNUniversity of PittsburghSchool of MedicinePittsburgh, PA
Mario F. Rubin, MDUniversity of Maryland School of MedicineBaltimore, MD
Ehab R. Saad, MD, FASNMedical College of WisconsinMilwaukee, WI
Mark C. Saddler, MBChBMercy Regional Medical CenterDurango, CO
Neil Sanghani, MDVanderbilt UniversityNashville, TN
Mohammad N. Saqib, MDLehigh Valley HospitalAllentown, PA
Hitesh H. Shah, MDHofstra Northwell School of MedicineGreat Neck, NY
-
Michiko Shimada, MD, PhDHirosaki UniversityHirosaki, Japan
Shayan Shirazian, MDWinthrop-University HospitalState University of New York atStony BrookMineola, NY
Arif Showkat, MD, FASNUniversity of TennesseeMemphis, TN
Stephen M. Sozio, MDJohns Hopkins University School of MedicineBaltimore, MD
Ignatius Yun-Sang Tang, MD, FASNUniversity of Illinois at ChicagoChicago, IL
Ahmad R. Tarakji, MDKing Saud University,King Khalid University HospitalRiyadh, Saudi Arabia
Hung-Bin Tsai, MDNational Taiwan UniversityHospital Taipei, Taiwan
Katherine Twombley, MDMedical University of South CarolinaCharleston, SC
Kausik Umanath, MDHenry Ford HospitalDetroit, MI
Puchimada M. Uthappa, MBBS, FASNColumbia Asia HospitalMysore, Karnataka, India
Anthony M. Valeri, MDColumbia University Medical CenterNew York, NY
Allen W. Vander, MD, FASNKidney Center of SouthLouisianaThibodaux, LA
Jon R. Von Visger, MD, PhDThe Ohio State UniversityColumbus, OH
Nand K. Wadhwa, MDStony Brook UniversityStony Brook, NY
Connie Wang, MDHennepin County Medical CenterMinneapolis, MN
Maura A. Watson, DOWalter Reed National Military Medical CenterBethesda, MD
Dawn Wolfgram, MDMedical College of WisconsinMilwaukee, WI
Sri Yarlagadda, MBBSUniversity of Kansas Medical CenterKansas City, KS
Brian Young, MDSanta Clara Valley Medical CenterSan Jose, CA
Mario Javier Zarama, MDKidney Specialists ofMinnesota, PASaint Paul, MN
-
Program Mission and ObjectivesThe Nephrology Self-Assessment Program (NephSAP) provides a learning vehicle for clinical nephrologists to renew andrefresh their clinical knowledge, diagnostic, and therapeutic skills. This enduring material provides nephrologists challenging,clinically oriented questions based on case vignettes, a detailed syllabus that reviews recent publications, and an editorial on animportant and evolving topic. This combination of materials enables clinicians to rigorously assess their strengths andweaknesses in the broad domain of nephrology.
Accreditation StatementThe American Society of Nephrology (ASN) is accredited by the Accreditation Council for Continuing Medical Education toprovide continuing medical education for physicians.
AMA Credit Designation StatementThe ASN designates this enduring material for a maximum of 10 AMA PRA Category 1 Credits. Physicians should claimonly the credit commensurate with the extent of their participation in the activity.
Original Release Date
March 2017
CME Credit Termination Date
February 28, 2019
Examination Available Online
On or before Saturday, March 15, 2017
Estimated Time for Completion
10 hours
Answers with Explanations
Provided with a passing score after the first and/or after the second attempt March 2019: posted on the ASN website when the issue is archived.
Target Audience
Nephrology certification and recertification candidates Practicing nephrologists Internists
Method of Participation
Read the syllabus that is supplemented by original articles in the reference lists. Complete the online self-assessment examination. Each participant is allowed two attempts to pass the examination (.75% correct) for CME credit. Upon completion, review your score and incorrect answers and print your certificate. Answers and explanations are provided with a passing score or after the second attempt.
Volume 16, Number 1, March 2017
-
Activity Evaluation and CME Credit Instructions
Go to www.asn-online.org/cme, and enter your ASN login on the right. Click the ASN CME Center. Locate the activity name and click the corresponding ENTER ACTIVITY button. Read all front matter information. On the left-hand side, click and complete the Demographics & General Evaluations. Complete and pass the examination for CME credit. Upon completion, click Claim Your CME Credits, check the Attestation Statement box, and enter the number of
CME credits commensurate with the extent of your participation in the activity.
If you need a certificate, Print Your Certificate on the left.
For your complete ASN transcript, click the ASN CME Center banner, and click View/Print Transcript on the left.
Instructions to obtain American Board of Internal Medicine (ABIM) Maintenance of Certification(MOC) PointsEach issue of NephSAP provides 10 MOC points. Respondents must meet the following criteria:
Be certified by ABIM in internal medicine and/or nephrology and enrolled in the ABIMMOC program Enroll for MOC via the ABIM website (www.abim.org). Enter your (ABIM) Candidate Number and Date of Birth prior to completing the examination. Take the self-assessment examination within the timeframe specified in this issue of NephSAP. Upon completion, click Claim Your MOC points, the MOC points submitted will match your CME credits claimed,
check the Attestation Statement box and submit.
ABIM will notify you when MOC points have been added to your record.
Maintenance of Certification StatementSuccessful completion of this CME activity, which includes participation in the evaluation component, enables the participantto earn up to 10 MOC points in the American Board of Internal Medicines (ABIM) Maintenance of Certification (MOC)program. Participants will earnMOC points equivalent to the amount of CME credits claimed for the activity. It is the CME activityproviders responsibility to submit participant completion information to ACCME for the purpose of granting ABIMMOC credit.
MOC points will be applied to only those ABIM candidates who have enrolled in the MOC program. It is your responsibility tocomplete the ABIM MOC enrollment process.
System RequirementsCompatible Browser and SoftwareThe ASN website (asn-online.org) has been formatted for cross-browser functionality, and should display correctly in allmodern web browsers. To view the interactive version of NephSAP, your browser must have Adobe Flash Player installed orhave HTML5 capabilities. NephSAP is also available in Portable Document Format (PDF), which requires Adobe Reader orcomparable PDF viewing software.
Monitor Settings
The ASN website was designed to be viewed in a 1024 768 or higher resolution.
Medium or Combination of Media Used
The media used include an electronic syllabus and online evaluation and examination.
Technical Support
If you have difficulty viewing any of the pages, please refer to the ASN technical support page for possible solutions. If youcontinue having problems, contact ASN at [email protected].
Volume 16, Number 1, March 2017
http://www.abim.orgmailto:[email protected]
-
Disclosure InformationThe ASN is responsible for identifying and resolving all conflicts of interest prior to presenting any educational activity to learners to ensure thatASN CME activities promote quality and safety, are effective in improving medical practice, are based on valid content, and are independent of thecontrol from commercial interests and free of bias. All faculty are instructed to provide balanced, scientifically rigorous and evidence-basedpresentations. In accordance with the disclosure policies of the Accreditation Council for Continuing Medical Education (ACCME), individuals who arein a position to control the content of an educational activity are required to disclose relationships with a commercial interest if (a) the relation is financialand occurred within the past 12 months; and (b) the individual had the opportunity to affect the content of continuing medical education with regard to thatcommercial interest. For this purpose,ASNconsider the relationships of the person involved in theCMEactivity to includefinancial relationships of a spouseor partner. Peer reviewers are asked to abstain from reviewing topics if they have a conflict of interest. Disclosure information is made available to learnersprior to the start of any ASN educational activity.
EDITORIAL BOARD:Gerald A. Hladik, MD, FASNCurrent Employer: University of North Carolina at Chapel Hill; Scientific Advisor/Membership: ASN Co-Director
for NephSAPDebbie L. Cohen, MDCurrent Employer: University of Pennsylvania School of Medicine; Scientific Advisor/Membership: Editorial Board: Journal
of Human Hypertension
Stanley Goldfarb, MD, FASNCurrent Employer: University of Pennsylvania School of Medicine; Consultancy: Genentech, Ardea Bioscience;Honoraria: Genentech, Ardea Bioscience; Scientific Advisor/Membership: Editorial Board: Clinical Nephrology, Genentech
Asghar Rastegar, MD, FASNCurrent Employer: Yale School of MedicineManoocher Soleimani, MDCurrent Employer: University of Cincinnati School of MedicineJerry Yee, MD, FASNCurrent Employer: Henry Ford Hospital; Consultancy: Optum, Merck, Vasc-Alert, Alexion, Amgen, Relypsa, Takeda,
Mallinckrodt, Global Guidepoint, ZS Pharma, CV-RX; Ownership Interest: Merck, Gilead; Honoraria: Amgen, Alexion, Global Guidepoint,American Board of InternalMedicine, Baylor Scott &White, Relypsa, ZS Pharma,Mallinckrodt, National Kidney Foundation, Takeda, Optum; Patents/Inventions: Vasc-Alert, Henry Ford Hospital; Scientific Advisor/Membership: NKF: Editor-in-Chief of Advances in CKD (journal); Am J NephrolEditorial Board: CJASN, American Journal of Nephrology, American Journal of Hypertension, ASN Co-Director, NephSAP, EBSCODynaMed
CONTRIBUTING AUTHORS:Namrata Krishnan, MDCurrent Employer: Yale School of MedicineKarthik Ramani, MD, FASNCurrent Employer: University of Cincinnati School of Medicine
EDITORIAL AUTHOR:David B. Mount, MDCurrent Employer: Brigham and Womens Hospital; Consultancy: ZS Pharma; Research Funding: Astra Zeneca;
Honoraria: UpToDate
ASN STAFF:Gisela A. Deuter, BSN, MSANothing to disclose
Commercial SupportThere is no commercial support for this issue.
Volume 16, Number 1, March 2017
-
EditorialAdvances in Chronic Potassium Control: Prognostic Implicationsfor CKD
David B. Mount, MDRenal Divisions, Brigham and Womens Hospital and VA Boston Healthcare System, HarvardMedical School, Boston, Massachusetts
Hyperkalemia is the bane of the renal patientsexistence, not to mention that of his or her nephrologist.Acute severe hyperkalemia is thus perhaps the subspe-cialtys most frequent emergency. Chronic hyperkalemia,in turn, plagues the management of patients with CKD,requiring repeated blood testing after changes in therapyand frequently necessitating a reduction or cessation inrenin-angiotensin-aldosterone system (RAAS) antago-nists. Historically, beginning in the 1950s (1), cationexchange resins were a mainstay in the chronic manage-ment of hyperkalemia. For decades, the dominant cationexchange resin available in the United States has beensodium polystyrene sulfonate (SPS), commercially avail-able as Kayexalate and Kionex. SPS exchanges Na1 forK1 in the gastrointestinal tract and has been shown toincrease the fecal excretion of K1 (2). To preventconstipation and facilitate the passage of the resin throughthe gastrointestinal tract, Flinn et al. (3) added sorbitol tothe resin. It subsequently became routine to administerSPS with sorbitol, with approximately 5 million annualdoses of the combination administered in the United Statesalone (4).
An increasing concern with SPS has been itsassociation with intestinal necrosis (48); this is fre-quently a fatal complication (4,6,7). Studies in rats hadsuggested that sorbitol is required for the intestinal injury(7); this and other observations eventually led to a re-duction in the percentage of sorbitol used and ultimately,a recommendation by the Food and Drug Administration(FDA) in 2009 to avoid the use of sorbitol with SPS.However, several lines of evidence suggest that SPSitself directly injures intestinal mucosa. A more contem-porary study in rats has shown that SPS alone cancause intestinal necrosis, suggesting that the previouslynoted toxicity of sorbitol alone may have resulted fromthe hypertonic solution in which it was suspended (9).
Clinically, SPS crystals can often be detected in humanpathologic specimens in SPS-associated necrosis, adher-ent to the injured mucosa (6,8). Several cases of colonicnecrosis after oral SPS without sorbitol have also beenreported (10,11), directly implicating SPS in the in-testinal injury.
Given the association with intestinal necrosis andthe questionable efficacy of SPS (4,12), there has beena gradual shift in recommendations for the treatment ofhyperkalemia away from the routine use of SPS (13,14).Treatment guidelines have revisited other measures forthe treatment of acute hyperkalemia, such as prolongedisotonic bicarbonate infusion (15), without a deleteriouseffect on the management of acute hyperkalemia. Thisshift away from SPS is not without controversy. One canargue, for example, that a handful of contemporarystudies have confirmed the clinical efficacy of SPS inreducing serum potassium concentrations (1618). Ad-ditionally, others have argued that the shift away fromSPS endangers lives (19) and/or that it impairs the abilityto manage hyperkalemic patients without dialysis, par-ticularly in disaster situations (20). Regardless, despitea persistent utilization of SPS for the management ofacute hyperkalemia in United States emergency rooms,its popularity for the chronic treatment of persistenthyperkalemia has waned considerably.
It is on this background that the nephrologycommunity welcomed with great interest the arrival oftwo new potassium binding agents, patiromer and sodiumzirconium cyclosilicate (ZS-9). Patiromer is FDAapproved and available in the United States, whereasapproval of ZS-9 is still under FDA review at the timeof writing.
Patiromer is a nonabsorbed polymer provided asa powder for suspension, which binds K1 in exchangefor Ca21. Preclinical studies indicated that patiromer is
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
1
-
not absorbed systemically, causing an increase in fecalpotassium excretion in hyperkalemic animals; in vitrostudies revealed higher potassium binding capacitythan SPS (21). In healthy adults, patiromer causesa decrease in urinary potassium, magnesium, andsodium excretion, suggesting the binding of the poly-mer to these cations in the intestine (22). There isa small increase in urinary calcium and a decrease inurinary phosphate in these subjects, suggesting bothmodest absorption of the released calcium and bindingof the released calcium to phosphate within the in-testine, reducing phosphate absorption and phosphateexcretion (22). The clinical efficacy of patiromer inreducing serum potassium was established in hyper-kalemic subjects enrolled in the PEARL-HF trial (heartfailure patients) (23), the AMETHST-DN trial (dia-betics with renal disease) (24), and the OPAL-HK trial(CKD patients on RAAS inhibitors) (13,14,25). A consis-tent side effect in these trials was dose-dependent hypo-magnesemia; in the AMETHYST-DN, for example, severehypomagnesemia (a serum magnesium ,1.2 mg/dl)developed in 13 (4.3%) patients (24). In a separateclinical research center study of patients with sustainedhyperkalemia, serum potassium was reduced signifi-cantly at 7 hours but was not reduced at 4 hours aftera dose of patiromer (26).
ZS-9 is an inorganic, nonabsorbable crystallinecompound that exchanges both sodium and hydrogenions for K1 and NH41 in the intestine. The binding ofK1 to ZS-9 has some similarity to the selectivity filterof K1 channels, with .25-fold selectivity for K1 overCa21 and Mg21 (27). The efficacy of ZS-9 in hyper-kalemic outpatients was evaluated in two nearly iden-tical phase 3, randomized, placebo-controlled trials: theHyperkalemia Randomized Intervention MultidoseZS-9 Maintenance Study (28) and a second largerstudy (13,14,29). Significant adverse events weresimilar with placebo and ZS-9. In these trials, thesteepest decline in serum potassium with ZS-9 oc-curred during the first 4 h of therapy. This observationmay imply an acute effect on intestinal potassiumsecretion rather than simple reduction in intestinalpotassium absorption.
The availability of these two new potassiumbinding agents generates the potential for chroniccontrol of serum potassium in patients with CKD,a goal that is arguably inappropriate with SPS. Inaddition to the obvious benefit of a reduction in thecardiac risks of hyperkalemia, the pathophysiology of
chronic hyperkalemia suggests other benefits in bothacid-base balance and aldosterone physiology. Therelevant symmetrical data are not available for patiromerand ZS-9. However, patiromer-induced reduction ofhyperkalemia in patients taking RAAS inhibitors isassociated with a reduction in circulating aldosteronelevels (30), and a reduction in hyperkalemia due toZS-9, in turn, results in an increase in serum bicarbonateconcentration (31). These additional benefits of chronicpotassium control are explored in this review; spacelimitations preclude a discussion of the potential utilityof ZS-9 and patiromer in patients with ESRD or theacute management of hyperkalemia.
Acid-Base Effect of Potassium ControlThe Role of the Kidney in Acid Excretion
Any discussion of the effect of chronic hyper-kalemia on acid-base balance necessitates a brief reviewof the relevant physiology. The kidneys have two majorfunctions in acidosis: (1) reabsorbing filtered bicarbon-ate and (2) generating new bicarbonate. In the typicaladult, the kidneys filter approximately 4200 mmol/d bi-carbonate. Renal epithelial cells reabsorb almost all ofthis bicarbonate load in a process termed bicarbonatereabsorption, accomplished by the proximal tubule andthick ascending limb (TAL). Kidneys also produce newbicarbonate in a process termed bicarbonate generation.Bicarbonate generation is equivalent to net acid excre-tion, which is the net sum of titratable urinary acidsand renal ammonium (NH41) minus urinary bicarbonateexcretion.
Titratable acids are solutes in the urine that buffersecreted protons, enabling H1 excretion without sub-stantial changes in urine pH. Titratable acid excretion isapproximately 30%40% of net acid excretion underbasal conditions. Metabolic acidosis increases titrat-able acid excretion by as much as 50% above baseline,thereby contributing to recovery from this acid-basedisorder. However, renal ammonia metabolism andtransport are the predominant mechanisms of the renalresponse to acidosis.
Ammonia exists in two molecular forms: NH3and NH41. The relative amounts of each are governedby the following buffer reaction: NH3 1 H1 4 NH41.This reaction occurs essentially instantaneously and hasa pKa under biologically relevant conditions of approx-imately 9.15. Accordingly, most ammonia is present asNH41; at pH 7.4, only approximately 1.7% of totalammonia is present as NH3. Because most biologic
2 Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
-
fluids exist at a pH substantially below the pKa of thisbuffer reaction, small changes in pH cause exponen-tial changes in NH3 concentration but almost no changein NH41 concentration.
NH3, although uncharged, has an asymmetric ar-rangement of positively charged hydrogen nuclei sur-rounding a central nitrogen atom; thus, NH3 is a polar,albeit uncharged, molecule. This molecular polaritycauses NH3 to have limited lipid permeability and finitepermeability across plasma membranes. NH41 also haslimited permeability across lipid bilayers. However, inaqueous solutions, NH41 and K1 have nearly identicalmolecular radii and biophysical characteristics, whichenable NH41 to be transported at the potassium transportsite of many proteins (32).
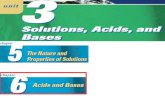
Ammonia homeostasis involves integrated func-tion of multiple portions of the kidney (Figure 1).A minimal fraction of urinary ammonia derives fromglomerular filtration. Rather, ammonia is produced bythe kidney and then selectively transported into eitherthe urine or into the renal vein. Ammonia is producedby almost all renal epithelial cells; however, theproximal tubule is the primary site. Circulating glutamineis transported into proximal tubule cells, followed byconversion to NH41 and glutamate through the actionof phosphate-dependent glutaminase. NH41 is thenexported into the tubular lumen, primarily via the apicalNa1-H1 exchanger, NHE3 (Figure 1).
Ammonium excreted by the proximal tubule issubsequently reabsorbed by the TAL (32) and concen-trated by countercurrent multiplication within the medul-lary interstitium (32,33), from whence it is transporteddown its concentration gradient via apical Rhcg NH3carriers in a-intercalated cells within the collecting duct(34); parallel H1 excretion via the apical H1-ATPaseresults in trapping of the luminal NH3 and urinaryexcretion as NH41.
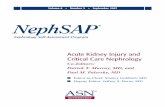
The NH41 ion is transported into TAL cells bythe apical Na1-K1-2Cl cotransporter (35) and otherK1 transporters (Figure 2); NH41 transport via apicalK1 channels and paracellular transport play lesser rolesunder physiologic conditions (32). NH41 exits the TALpredominantly via the basolateral Na1/H1 exchanger 4functioning in Na1/NH41 exchange mode (36). Thecapacity of the TAL to reabsorb NH41 and in turn,the corticomedullary gradient of NH41 are increasedduring acidosis (32,33), due in part to inductionof Na1-K1-2Cl cotransporter (35) and Na1/H1
exchanger 4 (36).
Hyperkalemia and Acid ExcretionHyperkalemia has a significant effect on the
ability to excrete an acid urine due to interferencewith the urinary excretion of NH41. Potassiumloading in humans results in modest reduction inurinary NH41 excretion and an impaired response toacid loading (37). In rats, chronic potassium loadingleads to hyperkalemia and a metabolic acidosis due toa 40% reduction in urinary NH41 excretion (38).Proximal tubular ammonia generation falls but with-out a significant effect on proximal tubular secretionof NH41 (38). As discussed above, the TAL absorbsNH41 from the tubular lumen followed by counter-current multiplication and ultimately excretion fromthe medullary interstitium (32); hyperkalemia inhibitsrenal acid excretion by competing with NH41 forreabsorption by the TAL (39). Hyperkalemia thusinduces acidosis in rats by reducing the NH41 gradientbetween the vasa recta (surrogate for interstitial fluid)and collecting duct (39) due to interference withabsorption of NH41 by the TAL.
Clinically, two case reports of patients with hyper-kalemic acidosis due to hyporeninemic hypoaldosteron-ism showed an increase in urinary NH41 excretion inresponse to normalization of plasma K1 with cationexchange resins (40,41), indicating a significant role forhyperkalemia in generation of the acidosis. However, thetranslational investigation of this phenomenon has notbeen extensive.
Intestinal Ammonium HomeostasisGiven the NH41 affinity of ZS-9, it seems
important to point out the potential effect of reducedintestinal NH41 absorption on acid-base homeostasis.Portal vein NH41/NH3 concentration is substantiallyhigher than systemic, indicating that NH41 is bothgenerated and absorbed within the intestine. The co-lonic flora ferment nonabsorbed dietary nutrients andproduce large quantities of NH3, which are thenabsorbed by the colon; 250 mmol or roughly 4 gNH41/NH3 is absorbed daily by the colon. As in thekidney, transport occurs via K1 transporters but also,by the Rh NH3 transporters, which are expressed inboth intestine (42) and liver (43) cells.
In patients with normal hepatic function, absorbedNH41/NH3 is converted to urea by the urea cycle;in patients with elevated NH3 levels (e.g., cirrhotics),there are no direct acid-base consequences. Therefore,the acid-base effects of reduced intestinal NH41
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017 3
-
absorption in hyperkalemic patients treated with ZS-9are presumably minimal. However, NH41-Cl absorp-tion can cause acidosis (44), and NH41-Cl adminis-tration is a widely used model for metabolic acidosisin human subjects (45), such that NH41 absorptionfrom the intestine may have acid-base consequences.Blockade of this NH41 absorption likely contributes tothe observed increase in bicarbonate after normalizationof hyperkalemia with ZS-9 (31), in addition to thebeneficial effects of potassium normalization on renalNH41 handling.
Clinical Relevance: Acid-Base Effects of ChronicPotassium Control
As GFR decreases in CKD from 6090 to ,20ml/min per 1.73 m2, the prevalence of metabolicacidosis increases from 2% to 39%, and the prevalenceof hyperkalemia increases from 2% to 42% (46). Thelargely nongap, inorganic acidosis seen in CKD canalso contribute to hyperkalemia. Thus, the induction ofmetabolic acidosis by the infusion of mineral acids(NH41-Cl or H1-Cl) consistently increases plasmaK1 (4751), whereas organic acidosis generally fails
to increase plasma K1 (49,5153). There are manypotential transport pathways that mediate a net K1-H1
exchange that is postulated to help maintain extracel-lular pH in response to acidosis (54). Clinically, use ofthe oral phosphate binder sevelamer hydrochloridein patients with ESRD is associated with acidosis dueto effective gastrointestinal absorption of H1-Cl.In hemodialysis patients, this acidosis has beenassociated with an increase in plasma K1, which isameliorated by an increase in dialysis bicarbonateconcentration (55).
Metabolic acidosis can lead to such clinical prob-lems as growth retardation in neonates and children;increased susceptibility to cardiac arrhythmias; decreasedcardiovascular catecholamine sensitivity; bone disor-ders, including osteoporosis and osteomalacia; recurrentnephrolithiasis; and skeletal muscle atrophy. Correctionof metabolic acidosis with alkali therapy (oral so-dium bicarbonate or citrate) in patients with serumbicarbonate concentration of ,22 mEq/L has longbeen the standard of care in the predialysis manage-ment of CKD.
More recently, there has been interest in the roleof metabolic acidosis in the progression of CKD to
Figure 1. Renal NH3/NH41 homeostasis. Ammonia produced in the proximal tubule is reabsorbed by the TAL, concentrated inthe medullary interstitium, and then, secreted by a-intercalated cells in the collecting duct. Gln, glutamine; NHE-3, Na1/H1
exchanger 3; NKCC2, Na1-K1-2Cl cotransporter; PDG, phosphate-dependent glutaminase. Reprinted with permission fromWeiner ID, Verlander JW: Role of NH3 and NH4 transporters in renal acid-base transport. Am J Physiol Renal Physiol 300:F11F23, 2011.
4 Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
-
ESRD. Individuals with CKD have a reduced numberof functioning nephrons, obligating a higher acidexcretion per nephron to cope with the acid-producingdiet of industrialized society. The renal mechanismsthat serve to augment acid excretion may also playa role in mediating progressive nephropathy; the chiefculprits include activation of the RAAS, increasedrenal endothelin, and increased renal NH41 (56). A fewsmall studies have indicated that alkali supplementationwith sodium-bicarbonate, citrate, or dietary changes(57) may be associated with reduced rate of progressionto ESRD (56,58).
In summary, the salutatory effects of ZS-9 andpotentially patiromer on acid-base parameters mayhave several clinical consequences in hyperkalemic CKDpatients.
(1) Reduced or delayed need for oral alkali therapy(2) Improvement in bone, muscle, and nutritionalhealth due to the reduced acidosis(3) Reduced rate of progression to CKD due to thereduced acidosis(4) Reduced pill burden in predialysis CKD due tothe reduction in requirement for alkali therapy(5) Expansion in the use of beneficial (57) alkalinefoods with higher K1 content, amplifying the bene-ficial effect on acidosis
Potassium Binder Therapy and AldosteroneAldosterone has a potent kaliuretic effect (59),
with important inter-relationships between circulatingK1 and aldosterone. Aldosterone release by the adrenalis thus induced by hyperkalemia and/or a high-K1 diet(60), suggesting an important feedback effect of aldo-sterone on K1 homeostasis (61). Aldosterone also hasclinically relevant effects onK1homeostasis, with a clearrelationship at all levels of serum K1 between circulatinglevels of the hormone and the ability to excrete K1.
Renin released from the kidney stimulates aldoste-rone release from the adrenal via angiotensin II (AT-II).Hyperkalemia is also an independent and synergisticstimulus for aldosterone release from the adrenal gland(60), although dietary K1 loading is less potent thandietary Na1-Cl restriction in increasing circulatingaldosterone (61). The resting membrane potential ofadrenal glomerulosa cells is hyperpolarized due to theactivity of the leak K1 channels Tandem of P domainsin a weak inwardly rectifying K1 channelrelatedAcid-Sensitive K1 channel-1 (TASK-1) and TASK-3.The resting membrane potential of adrenal glomerulosacells is hyperpolarized, due to the activity of the leakK1 channels TASK-1 and TASK-3; combined deletionof genes encoding these channels leads to baselinedepolarization of adrenal glomerulosa cells and anincrease in plasma aldosterone that is resistant todietary sodium loading (62). The KCNJ5 K1 channelalso plays a role, in that mutations of this channel thatproduce a depolarizing acquisition of KCNJ5-mediatedNa1 conductance are associated with adrenal adenomas(63). AT-II and K1 both activate Ca21 entry inglomerulosa cells via voltage-sensitive T-type Ca21
channels, primarily Cav3.2 (64). The Cav1.3 Ca21
channel, encoded by CACNA1D, is also expressedin glomeulosa cells; activating mutations in CACNA1Dare also associated with adrenal adenomas (65). Eleva-tions in extracellular K1 thus depolarize glomerulosacells and activate these Ca21 channels, which areindependently and synergistically activated by AT-II.Calcium-dependent activation of calcium-calmodulin-dependent protein kinase, in turn, activates the synthesisand release of aldosterone via induction of aldosteronesynthase. K1 and AT-II also enhance transcription of theCav3.2 Ca21 channel by abrogating repression of thisgene mediated by the neuron-restrictive silencing factor;this ultimately amplifies the induction of aldosteronesynthase (64).
Figure 2. Ammonium (NH41) transport pathways within theTAL. K1 competes with NH41 for transport by Na1-K1
-2Cl cotransporter (NKCC2; details are in the text). KCC4,K1-Cl cotransporter 4; NHE4, Na1/H1 exchanger 4;ROMK, Renal outer medullary potassium channel.
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017 5
-
The adrenal release of aldosterone due to in-creased K1 is dependent on an intact adrenal renin-angiotensin system, particularly duringNa1-Cl restriction.Angiotensin-converting enzyme (ACE) inhibitors andangiotensin receptor blockers (ARBs) completely abro-gate the effect of high K1 on salt-restricted adrenals (66).Direct G proteindependent activation of the TASK-1and/or TASK-3 K1 channels by AT1A or AT1B receptorsis thought to underlie the effect of AT-II on adrenalaldosterone release (62). Other clinically relevant activa-tors of adrenal aldosterone release include prostaglandinsand catecholamines via increases in cAMP (67). Finally,atrial natriuretic peptide exerts a potent negative effect onaldosterone release induced by K1 and other stimuli(68), at least in part by inhibiting early events inaldosterone synthesis (69). Atrial natriuretic peptideinhibits both renal renin release and adrenal aldoste-rone release, functions that may be central to the roles ofthis hormone in the pathophysiology of hyporeninemichypoaldosteronism (68).
Clinical Relevance: Aldosterone EffectPatiromer has been shown to reduce circulating
aldosterone levels in patients from the OPAL-HKTrial, all of whom were treated with RAAS inhibitors(30). The beneficial effect of potassium normalizationon aldosterone levels is relevant to the phenomenon ofaldosterone breakthrough during treatment with ACEinhibitors or ARBs, wherein aldosterone levels grad-ually increase after an initial decrease (70). This is incontradistinction to aldosterone escape, which refersto renal tubular escape from the physiologic effects ofcirculating aldosterone.
Aldosterone levels are elevated in CKD and havebeen implicated in progressive renal injury (71). It hasbeen postulated that this hyperaldosteronism is a ho-meostatic response to preserve potassium balance in thesetting of reduced nephron mass; consistent with thishypothesis, dietary potassium restriction reduces BPand circulating aldosterone in the remnant kidney ratmodel (72). There is also considerable interest in therole of mineralocorticoid antagonism in the treatmentof diabetic nephropathy and other glomerulopathies,typically in conjunction with ACE inhibitor or ARBtherapy (73,74).
Proteinuric patients treated with ACE inhibitor orARB therapy who exhibit aldosterone breakthroughexhibit greater proteinuria (75,76) and an acceleratedprogression to ESRD (77). Depending on the definition,
the incidence of aldosterone breakthrough varies from10% to 53% in generally small studies of the phenomenon(70). In the largest such study, a post hoc analysis of 567patients from the AMADEO Trial on losartan versustelmisartan, 28% developed aldosterone breakthrough de-fined as a .10% increase in aldosterone levels (78).Patients with type 2 diabetes and nephropathy whodeveloped hyperkalemia during therapy with losartanin the RENAAL trial had a graded, increased risk ofESRD and/or doubling of creatinine (79); althoughnot established, it is reasonable to speculate that thiswas due to aldosterone breakthrough in response tohyperkalemia. Therefore, hyperkalemia during treat-ment of diabetic nephropathy with ARBs is associatedwith the development of aldosterone breakthrough(78); hyperkalemia is, in turn, associated with adverserenal outcome (79), presumably due to the effect ofincreased aldosterone.
In summary, the beneficial effects of chronicpotassium control on aldosterone levels (30) may havea number of salutary effects in hyperkalemic CKDpatients.
(1) Reduction in circulating aldosterone in CKDpatients with high-dietary potassium intake and/orhyperkalemia, leading to improved renal outcomes(2) Prevention of aldosterone breakthrough in pa-tients treated with ACE inhibitor or ARB, leading toimproved renal outcomes(3) Normalization of aldosterone breakthrough inpatients treated with ACE inhibitor or ARB, leadingto improved renal outcomes
PerspectivesI anticipate that the initial utilization of both patiromer
and ZS-9 will be restricted to patients with CKD orheart failure who have persistent hyperkalemia on or offRAAS inhibitors, despite adequate dietary potassiumrestriction. The clinical outcome benefits of improvedacid-base balance and/or aldosterone homeostasis willneed to be proven before the utilization of potassiumbinders is broadened beyond these narrow indications.Regardless, the current understanding suggests profoundimplications for these new advances in the chronic controlof potassium in CKD.
Disclosures
D.B.M. acknowledges consult and advisory board paymentsfrom ZS Pharma and royalty payments from UpToDate.
6 Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
-
References1. Elkinton JR, Clark JK, Squires RD, Bluemle LW Jr., Crosley AP Jr.:
Treatment of potassium retention in anuria with cation ex-change resin; a preliminary report. Am J Med Sci 220: 547552,1950 PubMed
2. Scherr L, Ogden DA, Mead AW, Spritz N, Rubin AL: Management ofhyperkalemia with a cation-exchange resin. N Engl J Med 264: 115119, 1961 PubMed
3. Flinn RB, Merrill JP, Welzant WR: Treatment of the oliguric patientwith a new sodium-exchange resin and sorbitol; a preliminary report. NEngl J Med 264: 111115, 1961 PubMed
4. Sterns RH, Rojas M, Bernstein P, Chennupati S: Ion-exchange resinsfor the treatment of hyperkalemia: Are they safe and effective? J Am SocNephrol 21: 733735, 2010 PubMed
5. Gerstman BB, Kirkman R, Platt R: Intestinal necrosis associated withpostoperative orally administered sodium polystyrene sulfonate insorbitol. Am J Kidney Dis 20: 159161, 1992 PubMed
6. McGowan CE, Saha S, Chu G, Resnick MB, Moss SF: Intestinalnecrosis due to sodium polystyrene sulfonate (Kayexalate) in sorbitol.South Med J 102: 493497, 2009 PubMed
7. Lillemoe KD, Romolo JL, Hamilton SR, Pennington LR, Burdick JF,Williams GM: Intestinal necrosis due to sodium polystyrene (Kayex-alate) in sorbitol enemas: Clinical and experimental support for thehypothesis. Surgery 101: 267272, 1987 PubMed
8. Rashid A, Hamilton SR: Necrosis of the gastrointestinal tract in uremicpatients as a result of sodium polystyrene sulfonate (Kayexalate) insorbitol: An underrecognized condition. Am J Surg Pathol 21: 6069,1997 PubMed
9. Ayoub I, Oh MS, Gupta R, McFarlane M, Babinska A, Salifu MO:Colon necrosis due to sodium polystyrene sulfonate with and withoutsorbitol: An experimental study in rats. PLoS One 10: e0137636,2015 PubMed
10. Cheng ES, Stringer KM, Pegg SP: Colonic necrosis and perforationfollowing oral sodium polystyrene sulfonate (Resonium A/Kayexalatein a burn patient. Burns 28: 189190, 2002 PubMed
11. Goutorbe P, Montcriol A, Lacroix G, Bordes J, Meaudre E, Souraud JB:Intestinal necrosis associated with orally administered calciumpolystyrenesulfonate without sorbitol. Ann Pharmacother 45: e13,2011 PubMed
12. Malone DJ: Taking a second look at kayexalate. Hosp Pharm 50: 959960, 2015 PubMed
13. Mount DB: Treatment and Prevention of Hyperkalemia, edited byBasow DS, Waltham MA, UpToDate, 2016
14. Mount DB: Disorders of potassium balance. In: Brenner and RectorsThe Kidney, edited by Skorecki K, Chertow GM, Marsden PA, TaalMW, Yu ASL, 10th Ed., Philadelphia, W.B. Saunders Co., 2016 , pp559600
15. Blumberg A, Weidmann P, Ferrari P: Effect of prolonged bicarbonateadministration on plasma potassium in terminal renal failure. Kidney Int41: 369374, 1992 PubMed
16. Lepage L, Dufour AC, Doiron J, Handfield K, Desforges K, Bell R,Vallee M, Savoie M, Perreault S, Laurin LP, Pichette V, Lafrance JP:Randomized clinical trial of sodium polystyrene sulfonate for thetreatment of mild hyperkalemia in CKD. Clin J Am Soc Nephrol 10:21362142, 2015 PubMed
17. Mistry M, Shea A, Giguere P, Nguyen ML: Evaluation of sodiumpolystyrene sulfonate dosing strategies in the inpatient management ofhyperkalemia. Ann Pharmacother 50: 455462, 2016 PubMed
18. Hagan AE, Farrington CA, Wall GC, Belz MM: Sodium polystyrenesulfonate for the treatment of acute hyperkalemia: A retrospective study.Clin Nephrol 85: 3843, 2016 PubMed
19. Abuelo JG: Moving away from Kayexalate, sodium polystyrene sulfate.Am J Emerg Med 34: 1716, 2016 PubMed
20. Watson M, Abbott KC, Yuan CM: Damned if you do, damned if youdont: Potassium binding resins in hyperkalemia. Clin J Am SocNephrol 5: 17231726, 2010 PubMed
21. Li L, Harrison SD, Cope MJ, Park C, Lee L, Salaymeh F, Madsen D,Benton WW, Berman L, Buysse J: Mechanism of action and pharma-cology of patiromer, a nonabsorbed cross-linked polymer that lowersserum potassium concentration in patients with hyperkalemia. JCardiovasc Pharmacol Ther 21: 456465, 2016 PubMed
22. Bushinsky DA, Spiegel DM, Gross C, BentonWW, Fogli J, Hill GallantKM, Du Mond C, Block GA, Weir MR, Pitt B: Effect of patiromer onurinary ion excretion in healthy adults [published online ahead of printSeptember 27, 2016]. Clin J Am Soc Nephrol PubMed
23. Pitt B, Anker SD, Bushinsky DA, Kitzman DW, Zannad F, Huang IZ;PEARL-HF Investigators: Evaluation of the efficacy and safety ofRLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF)trial. Eur Heart J 32: 820828, 2011 PubMed
24. Bakris GL, Pitt B, Weir MR, Freeman MW, Mayo MR, Garza D, StasivY, Zawadzki R, Berman L, Bushinsky DA; AMETHYST-DN Inves-tigators: Effect of patiromer on serum potassium level in patients withhyperkalemia and diabetic kidney disease: The AMETHYST-DNRandomized Clinical Trial. JAMA 314: 151161, 2015 PubMed
25. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y,Wittes J, Christ-Schmidt H, Berman L, Pitt B; OPAL-HK Investigators:Patiromer in patients with kidney disease and hyperkalemia receivingRAAS inhibitors. N Engl J Med 372: 211221, 2015 PubMed
26. Bushinsky DA,Williams GH, Pitt B, Weir MR, FreemanMW, Garza D,Stasiv Y, Li E, Berman L, Bakris GL: Patiromer induces rapid andsustained potassium lowering in patients with chronic kidney diseaseand hyperkalemia. Kidney Int 88: 14271433, 2015 PubMed
27. Stavros F, Yang A, Leon A, Nuttall M, Rasmussen HS: Characterizationof structure and function of ZS-9, a K1 selective ion trap. PLoS One 9:e114686, 2014 PubMed
28. Kosiborod M, Peacock WF, Packham DK: Sodium zirconium cyclo-silicate for urgent therapy of severe hyperkalemia. N Engl J Med 372:15771578, 2015 PubMed
29. Packham DK, Rasmussen HS, Lavin PT, El-Shahawy MA, Roger SD,Block G, Qunibi W, Pergola P, Singh B: Sodium zirconium cyclo-silicate in hyperkalemia. N Engl J Med 372: 222231, 2015 PubMed
30. Weir MR, Bakris GL, Gross C, Mayo MR, Garza D, Stasiv Y, Yuan J,Berman L, Williams GH: Treatment with patiromer decreases aldoste-rone in patients with chronic kidney disease and hyperkalemia on renin-angiotensin system inhibitors. Kidney Int 90: 696704, 2016 PubMed
31. de Francisco A, Rasmussen H, Lavin P, Singh B, Yang A, Mann J,Jadoul M, Spinowitz B: Normalization of serum bicarbonate withsodium zirconium cyclosilicate (ZS-9) in the Phase 3 randomized,double-blind, placebo-controlled HARMONIZE study. Nephrol DialTransplant 30: iii6, 2015
32. Good DW: Ammonium transport by the thick ascending limb of Henlesloop. Annu Rev Physiol 56: 623647, 1994 PubMed
33. Packer RK, Desai SS, Hornbuckle K, Knepper MA: Role of counter-current multiplication in renal ammonium handling: Regulation ofmedullary ammonium accumulation. J Am Soc Nephrol 2: 7783,1991 PubMed
34. Biver S, Belge H, Bourgeois S, Van Vooren P, Nowik M, Scohy S,Houillier P, Szpirer J, Szpirer C, Wagner CA, Devuyst O, Marini AM:A role for Rhesus factor Rhcg in renal ammonium excretion and malefertility. Nature 456: 339343, 2008 PubMed
35. Attmane-Elakeb A, Mount DB, Sibella V, Vernimmen C, Hebert SC,Bichara M: Stimulation by in vivo and in vitro metabolic acidosis ofexpression of rBSC-1, the Na1-K1(NH41)-2Cl- cotransporter of therat medullary thick ascending limb. J Biol Chem 273: 3368133691,1998 PubMed
36. Bourgeois S, Meer LV, Wootla B, Bloch-Faure M, Chambrey R, ShullGE, Gawenis LR, Houillier P: NHE4 is critical for the renal handling ofammonia in rodents. J Clin Invest 120: 18951904, 2010 PubMed
37. Tannen RL, Wedell E, Moore R: Renal adaptation to a high potassiumintake. The role of hydrogen ion. J Clin Invest 52: 20892101,1973 PubMed
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017 7
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=14783124&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=13747532&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=13700297&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20167700&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1496969&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=19373153&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3824154&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8990142&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26413782&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11900946&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21304040&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27621500&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552710&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26576619&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27048188&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26587776&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27318747&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20798253&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26856345&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27679518&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21208974&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26172895&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=25415805&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26376130&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=25531770&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=25875277&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=25415807&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27350174&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8010753&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1912412&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=19020613&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9837954&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20484819&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=4737901&dopt=Abstract
-
38. DuBose TD Jr., Good DW: Effects of chronic hyperkalemia on renalproduction and proximal tubule transport of ammonium in rats. Am JPhysiol 260: F680F687, 1991 PubMed
39. DuBose TD Jr., Good DW: Chronic hyperkalemia impairs ammoniumtransport and accumulation in the inner medulla of the rat. J Clin Invest90: 14431449, 1992 PubMed
40. Matsuda O, Nonoguchi H, Tomita K, Shiigai T, Ida T, Shinohara S,Ideura T, Takeuchi J: Primary role of hyperkalemia in the acidosisof hyporeninemic hypoaldosteronism. Nephron 49: 203209,1988 PubMed
41. Szylman P, Better OS, Chaimowitz C, Rosler A: Role of hyperkalemiain the metabolic acidosis of isolated hypoaldosteronism. N Engl J Med294: 361365, 1976 PubMed
42. Handlogten ME, Hong SP, Zhang L, Vander AW, Steinbaum ML,Campbell-Thompson M, Weiner ID: Expression of the ammoniatransporter proteins Rh B glycoprotein and Rh C glycoprotein in theintestinal tract. Am J Physiol Gastrointest Liver Physiol 288: G1036G1047, 2005 PubMed
43. Weiner ID, Miller RT, Verlander JW: Localization of the ammoniumtransporters, Rh B glycoprotein and Rh C glycoprotein, in the mouseliver. Gastroenterology 124: 14321440, 2003 PubMed
44. Wong KM, Chak WL, Cheung CY, Chan YH, Choi KS, Chau KF, LiCS: Hypokalemic metabolic acidosis attributed to cough mixture abuse.Am J Kidney Dis 38: 390394, 2001 PubMed
45. Batlle DC, Hizon M, Cohen E, Gutterman C, Gupta R: The use of theurinary anion gap in the diagnosis of hyperchloremic metabolicacidosis. N Engl J Med 318: 594599, 1988 PubMed
46. Moranne O, Froissart M, Rossert J, Gauci C, Boffa JJ, Haymann JP,Mrad MB, Jacquot C, Houillier P, Stengel B, Fouqueray B; Nephro-Test Study Group: Timing of onset of CKD-related metabolic compli-cations. J Am Soc Nephrol 20: 164171, 2009 PubMed
47. Simmons DH, Avedon M: Acid-base alterations and plasma potassiumconcentration. Am J Physiol 197: 319326, 1959 PubMed
48. Burnell JM, Scribner BH, Uyeno BT, Villamil MF: The effect inhumans of extracellular pH change on the relationship between serumpotassium concentration and intracellular potassium. J Clin Invest 35:935939, 1956 PubMed
49. Oster JR, Perez G, Castro A, Vaamonde CA: Plasma potassiumresponse to acute metabolic acidosis induced by mineral and nonmineralacids. Miner Electrolyte Metab 4: 2836, 1980
50. Abrams WB, Lewis DW, Bellet S: The effect of acidosis and alkalosison the plasma potassium concentration and the electrocardiogram ofnormal and potassium depleted dogs. Am J Med Sci 222: 506515,1951 PubMed
51. Adrogue HJ, Madias NE: Changes in plasma potassium concentra-tion during acute acid-base disturbances. Am J Med 71: 456467,1981 PubMed
52. Fulop M: Serum potassium in lactic acidosis and ketoacidosis. N Engl JMed 300: 10871089, 1979 PubMed
53. Orringer CE, Eustace JC, Wunsch CD, Gardner LB: Natural history oflactic acidosis after grand-mal seizures. A model for the study of ananion-gap acidosis not associated with hyperkalemia. N Engl J Med297: 796799, 1977 PubMed
54. Aronson PS, Giebisch G: Effects of pH on potassium: New explanationsfor old observations. J Am Soc Nephrol 22: 19811989, 2011 PubMed
55. Sonikian M, Metaxaki P, Iliopoulos A, Marioli S, Vlassopoulos D:Long-term management of sevelamer hydrochloride-induced metabolicacidosis aggravation and hyperkalemia in hemodialysis patients. RenFail 28: 411418, 2006 PubMed
56. Goraya N, Wesson DE: Does correction of metabolic acidosis slowchronic kidney disease progression? Curr Opin Nephrol Hypertens 22:193197, 2013 PubMed
57. Goraya N, Simoni J, Jo CH, Wesson DE: A comparison of treatingmetabolic acidosis in CKD stage 4 hypertensive kidney disease withfruits and vegetables or sodium bicarbonate. Clin J Am Soc Nephrol 8:371381, 2013 PubMed
58. Kovesdy CP: Metabolic acidosis and kidney disease: Does bicarbonatetherapy slow the progression of CKD? Nephrol Dial Transplant 27:30563062, 2012 PubMed
59. August JT, Nelson DH, Thorn GW: Response of normal subjectsto large amounts of aldosterone. J Clin Invest 37: 15491555,1958 PubMed
60. Dluhy RG, Axelrod L, Underwood RH, Williams GH: Studies of thecontrol of plasma aldosterone concentration in normal man. II. Effect ofdietary potassium and acute potassium infusion. J Clin Invest 51: 19501957, 1972 PubMed
61. Palmer LG, Frindt G: Aldosterone and potassium secretion by thecortical collecting duct. Kidney Int 57: 13241328, 2000 PubMed
62. Davies LA, Hu C, Guagliardo NA, Sen N, Chen X, Talley EM, CareyRM, Bayliss DA, Barrett PQ: TASK channel deletion in mice causesprimary hyperaldosteronism. Proc Natl Acad Sci U S A 105: 22032208, 2008 PubMed
63. Choi M, Scholl UI, Yue P, Bjorklund P, Zhao B, Nelson-Williams C, JiW, Cho Y, Patel A, Men CJ, Lolis E, Wisgerhof MV, Geller DS, ManeS, Hellman P, Westin G, Akerstrom G, Wang W, Carling T, Lifton RP:K1 channel mutations in adrenal aldosterone-producing adenomas andhereditary hypertension. Science 331: 768772, 2011 PubMed
64. Somekawa S, Imagawa K, Naya N, Takemoto Y, Onoue K, Okayama S,Takeda Y, Kawata H, Horii M, Nakajima T, Uemura S, Mochizuki N,Saito Y: Regulation of aldosterone and cortisol production by thetranscriptional repressor neuron restrictive silencer factor. Endocrinol-ogy 150: 31103117, 2009 PubMed
65. Scholl UI, Goh G, Stolting G, de Oliveira RC, Choi M, Overton JD,Fonseca AL, Korah R, Starker LF, Kunstman JW, Prasad ML, HartungEA, Mauras N, Benson MR, Brady T, Shapiro JR, Loring E, Nelson-Williams C, Libutti SK, Mane S, Hellman P, Westin G, Akerstrom G,Bjorklund P, Carling T, Fahlke C, Hidalgo P, Lifton RP: Somatic andgermline CACNA1D calcium channel mutations in aldosterone-producing adenomas and primary aldosteronism. Nat Genet 45: 10501054, 2013 PubMed
66. Mazzocchi G, Malendowicz LK, Markowska A, Albertin G, NussdorferGG: Role of adrenal renin-angiotensin system in the control ofaldosterone secretion in sodium-restricted rats. Am J Physiol EndocrinolMetab 278: E1027E1030, 2000 PubMed
67. Csukas S, Hanke CJ, Rewolinski D, Campbell WB: Prostaglandin E2-induced aldosterone release is mediated by an EP2 receptor. Hyperten-sion 31: 575581, 1998 PubMed
68. Clark BA, Brown RS, Epstein FH: Effect of atrial natriuretic peptideon potassium-stimulated aldosterone secretion: Potential relevance tohypoaldosteronism in man. J Clin Endocrinol Metab 75: 399403,1992 PubMed
69. Cherradi N, Brandenburger Y, Rossier MF, Vallotton MB, Stocco DM,Capponi AM: Atrial natriuretic peptide inhibits calcium-induced ste-roidogenic acute regulatory protein gene transcription in adrenalglomerulosa cells. Mol Endocrinol 12: 962972, 1998 PubMed
70. Bomback AS, Klemmer PJ: The incidence and implications ofaldosterone breakthrough. Nat Clin Pract Nephrol 3: 486492,2007 PubMed
71. Hostetter TH, Ibrahim HN: Aldosterone in chronic kidney and cardiacdisease. J Am Soc Nephrol 14: 23952401, 2003 PubMed
72. Ibrahim HN, Hostetter TH: Role of dietary potassium in the hyper-aldosteronism and hypertension of the remnant kidney model. J Am SocNephrol 11: 625631, 2000 PubMed
73. Toto RD: Aldosterone blockade in chronic kidney disease: Can itimprove outcome? Curr Opin Nephrol Hypertens 19: 444449,2010 PubMed
74. Bertocchio JP, Warnock DG, Jaisser F: Mineralocorticoid receptoractivation and blockade: An emerging paradigm in chronic kidneydisease. Kidney Int 79: 10511060, 2011 PubMed
75. Sato A, Hayashi K, Naruse M, Saruta T: Effectiveness of aldosteroneblockade in patients with diabetic nephropathy. Hypertension 41: 6468, 2003 PubMed
8 Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2035655&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1401077&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3398981&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1674&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=15576624&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12730882&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11479167&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3344005&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=19005010&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=14446880&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=13367188&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=14885192&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7025622&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=34793&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=19702&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21980112&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=16825091&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=23380803&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=23393104&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=22851628&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=13587664&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=5054456&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10760062&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=18250325&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21311022&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=19342457&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=23913001&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10827004&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9461224&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1386372&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9658401&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17717561&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12937319&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10752521&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20625290&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21412221&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12511531&dopt=Abstract
-
76. Horita Y, Taura K, Taguchi T, Furusu A, Kohno S: Aldosteronebreakthrough during therapy with angiotensin-converting enzymeinhibitors and angiotensin II receptor blockers in proteinuric patientswith immunoglobulin A nephropathy. Nephrology (Carlton) 11: 462466, 2006 PubMed
77. Schjoedt KJ, Andersen S, Rossing P, TarnowL, Parving HH: Aldosteroneescape during blockade of the renin-angiotensin-aldosterone system indiabetic nephropathy is associated with enhanced decline in glomerularfiltration rate. Diabetologia 47: 19361939, 2004 PubMed
78. Moranne O, Bakris G, Fafin C, Favre G, Pradier C, Esnault VL:Determinants and changes associated with aldosterone breakthrough afterangiotensin II receptor blockade in patients with type 2 diabetes with overtnephropathy. Clin J Am Soc Nephrol 8: 16941701, 2013 PubMed
79. Miao Y, Dobre D, Heerspink HJ, Brenner BM, Cooper ME, ParvingHH, Shahinfar S, Grobbee D, de Zeeuw D: Increased serum potassiumaffects renal outcomes: A post hoc analysis of the Reduction ofEndpoints in NIDDM with the Angiotensin II Antagonist Losartan(RENAAL) trial. Diabetologia 54: 4450, 2011 PubMed
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017 9
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17014562&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=15551047&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=23929924&dopt=Abstracthttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20882268&dopt=Abstract
-
SyllabusNephSAP, Volume 16, Number 1, March 2017Electrolytes and Acid-BaseDisorders
Asghar Rastegar, MD,* Manoocher Soleimani, MD,yz Namrata Krishnan, MD,* andKarthik Ramani, MDy*Department of Medicine, Yale School of Medicine, New Haven, Connecticut; yDepartment ofMedicine, University of Cincinnati School of Medicine, Cincinnati, Ohio; Veterans AffairsMedical Centers, Cincinnati, Ohio; and Veterans Affairs Medical Centers, West Haven,Connecticut
Learning Objectives1. Examine recent scientific advances in our
understanding of the pathophysiology of dis-orders of fluid, electrolytes, and acid-basebalance
2. Review how the understanding of pathophys-iology can be applied to the care of patients
3. Analyze how recent studies related to fluid,electrolyte, and acid-base disorders can be ap-plied to clinical decision making
As indicated in previous Nephrology Self-AssessmentProgram (NephSAP) issues on fluid, electrolytes, and acid-base disturbances, there are very few publications on thebasis of clinical trials or well designed cohort, observational,or case-control studies in this area of nephrology. This issueof NephSAP will follow, whenever possible, a case-basedapproach. We have attempted to use actual cases from ourown experience and occasionally, the literature to betterillustrate a logical approach to patients whom you mayencounter in your practice. Herein, we examine recentadvances in the understanding of pathophysiologyof fluid, acid-base, and electrolyte disorders and theirapplicability in clinical setting. Topics that were notdiscussed in the previous two issues of NephSAP arediscussed in detail in this issue, while at the same time, wehave attempted to review all clinically important articlespublished in the past 23 years.
Update on Fluid Therapy in Patients with Sepsis
Fluid VolumeIn the previous Nephrology Self-Assessment Pro-
gram (NephSAP) issue, we reviewed the initial fluid
therapy in patients with presumed septic shock. Tosummarize, although the initial single-center study byRivers et al. (1) supported the use of protocol-based,early goaldirected therapy (EGDT), two randomized,prospective, multicenter studies in the United Statesand Australia/New Zealand did not show any differ-ence between protocol-based and usual care (2,3). Athird multicenter study carried out in the UnitedKingdom has since been published (4). The EnglishProtocolised Management in Sepsis Study, a prag-matic, open-label, multicenter, parallel-group, random-ized, controlled trial enrolled 1260 patients, with 630patients assigned to EGDT and 630 patients assigned tousual care. Although the EGDT group received moreintensive therapy as reflected by greater use of centralvenous catheters, fluids, red cell transfusions, andvasoactive drugs, the 90-day mortality rates in theEGDT group and the usual care group were similar(29.5% versus 29.2%, respectively; relative risk [RR]in the EGDT group, 1.01; 95% confidence interval[95% CI], 0.85 to 1.20; P 5 NS) (Figure 1). Severalsecondary outcomes, including the mean SequentialOrgan Failure Assessment score (on the basis ofmeasurement of major organ function) at 6 hours, thenumber of patients receiving advanced cardiovascularsupport, and the median intensive care unit (ICU)length of stay, were significantly greater in the EGDTgroup than the usual care group. The difference amongthe findings of these three large, randomized trials andthe 2001 study by Rivers et al. (1) is, in part, due toimprovement in the initial treatment of patients withpresumed septic shock. In addition, as noted in aneditorial by De Backer and Vincent (5), the patients inthese three studies were less severely ill than thosein the study by Rivers et al. (1), which was reflected
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017
10
-
in higher initial central venous oxygen saturation (ScvO2),lower rate of mechanical ventilation, lower fluid infusion,and later randomization (5). In a recent meta-analysis offive randomized, controlled trials involving 4735 patients,the mortality rates in the EGDT and control groups werevery similar at 23.2% and 22.4%, respectively. The pooledestimate of 90-day mortality that included 4063 patientsalso showed no difference between groups. The EGDTgroup had an increase in vasopressor use (odds ratio [OR],1.25; 95%CI, 1.10 to1.41; P50.001) and admission to theICU (OR, 2.19; 95% CI, 1.82 to 2.65; P50.001) (6).
The difference between the amount of fluid ad-ministered in the first 6 hours in the experimental armin the study by Rivers et al. (1) and that in the morerecent trial (5 L versus ,2 L) is striking. This has raisedthe possibility that fluid overload may have contributedto increase in admission rate and possibly, mortality inthe earlier studies. In a provocative review, Mallik andBellomo (7) argue that septic shock is not a volumeproblem but a vascular problem due to vasoplegiawith loss of arterial tone, venodilation with sequestra-tion of blood in the unstressed blood compartment andchanges in ventricular function with reduced compli-ance and reduced preload responsiveness, and there-fore, infusion of a large amount of fluid would only leadto fluid overload, which could contribute to overallmortality (7). They advocated an initial bolus of 500 ml
to assess fluid responsiveness, with maximum fluid in-fusion of 20 ml/kg in those with initial positive responseand early use of norepinephrine in those with fluid unre-sponsiveness. It is interesting to note that vasopressoragents were used in only 30% of patients in the study byRivers et al. (1), whereas in later studies, vasopressorswere used in 50%60% of patients. The relationshipbetween fluid overload and mortality is supported bystudies in pediatric patients with sepsis (8,9), adult patientswith severe malaria (10), and patients with acute respira-tory distress syndrome with or without AKI (11,12). Thestrategy advocated by these authors, although patho-physiologically logical, has not been rigorously studied.
The BP goal in the septic patient has recently beenstudied in a multicenter, open-label trial involving 776patients with septic shock undergoing resuscitation. TwoBP targets were selected: high target with a mean arterialpressure (MAP) goal of 8085 mmHg and low targetwith an MAP goal of 6570 mmHg. The primary endpoint was mortality at day 28. Serum creatinine levelsat inclusion were 1.9661.39 and 1.9361.47 mg/dl, re-spectively, and the incidence rates of AKI were 48.7%and 45.1%, respectively. The mortality rate in the high-target group was 142 of 388 patients (36.6%), and that inthe low-target group was 132 of 388 patients (34.0%;hazard ratio [HR] in the high-target group, 1.07; 95% CI,0.84 to 1.38; P5 NS). There was no difference in the 90-day mortality or serious adverse events between the twogroups (12).
To summarize, these recent studies do not sup-port protocol-based fluid resuscitation in patients withsuspected sepsis. A more individualized approach onthe basis of available clinical data that is focused onimproving major organ perfusion is advocated (13). Inaddition, fluid overload should be avoided, becausethis may increase risk of mortality in these critically illpatients. The MAP goal of 6570 mmHg is generallyadequate for initial resuscitation.
Protocol-driven EGDT of septic shock isnot superior to usual care that uses clin-ical data with the goal of increasing meanBP to >65 mmHg.
Fluid TypeIn the last issue of NephSAP, we summarized the
available studies comparing the use of chloride-liberal
Figure 1. KaplanMeier survival estimates. Shown is theprobability of survival for patients with severe sepsis re-ceiving EGDT and those receiving usual care at 90 days.Reprinted with permission from Mouncey PR, Osborn TM,Power GS, Harrison DA, Sadique MZ, Grieve RD, JahanR, Harvey SE, Bell D, Bion JF, Coats TJ, Singer M, YoungJD, Rowan KM; ProMISe Trial Investigators: Trial ofearly, goal-directed resuscitation for septic shock. N Engl JMed 372: 13011311, 2015.
Nephrology Self-Assessment Program - Vol 16, No 1, March 2017 11
-
versus balanced solutions in ICU patients. Two studieshad raised concerns about potential complications ofchloride-liberal solutions, including AKI, increase re-quirement for RRT, and hyperchloremic metabolicacidosis (14,15). During the past 2 years, another majorstudy comparing chloride-rich and balanced solutionhas been published. The 0.9% Saline versus Plasma-Lyte 148 for ICU Fluid Therapy (SPLIT) Trial isa double-blind, cluster-randomized, double-crossoverstudy in four academic ICUs in New Zealand compar-ing the incidence rates of AKI in patients receivingPlasma-Lyte 148 or 0.9% saline solution (16). Thisunique design allocated each ICU to four alternating7-week blocks, thereby permitting the use of each fluidtype twice in each ICU study; 2278 eligible patientswere enrolled. The incidence rates of AKI (defined asrisk, injury, failure, loss, and ESRD classification stage3) were 9.2% and 9.6% in patients receiving Plasma-Lyte 148 and 0.9% saline solution, respectively (P 5NS) (Figure 2). The total fluid volume administeredwas also quite low, again indicating that the populationenrolled in this study was fairly stable hemodynami-cally and in general, reasonably healthy. Although thestudy was double blind in design, two thirds of clinicianssurveyed could correctly guess the type of fluid that theirpatient was receiving.
What should the clinician derive from this study?The SPLIT Trial, although well designed, is only rel-evant to patients who were relatively healthy and re-quired small amount of fluids during their ICU stay. Itdoes not relate to patients with severe illness admittedto the ICU who often require a large amount of fluid aswell as vasopressors. For example, in a retrospectivestudy using a large database of 53,448 ICU patientswith sepsis treated with vasopressors and crystalloidsby hospital day 2, the mortality was lower in patientswho had received balanced solution (19.6% versus22.8%; RR, 0.86; 95% CI, 0.78 to 0.94) (17). Therewere no significant differences in the prevalence ofAKI (with and without dialysis) or in-hospital and ICUlengths of stay. It should, however, be noted that this isa retrospective study, and only 6.4% of patients re-ceived a balanced solution.
The debate between use of chloride-rich and useof balanced solution is not settled. However, pendinglarge, well designed, randomized or observational stud-ies, it is reasonable to conclude that, in relatively healthypatients requiring small amounts of fluid for shortperiods, there is no difference in clinical outcome
between the two types of fluids. However, in severelyill patients, such as patients with sepsis or septic shock,who require large amounts of fluid, we favor the use ofbalanced solutions over chloride-rich solution.
References1. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B,
Peterson E, Tomlanovich M, for the Early Goal-Directed TherapyCollaborative Group: Early goal-directed therapy in the treatmentof severe sepsis and septic shock. N Engl J Med 345: 13681377,2001
2. The ProCESS Investigators. A randomized trial of protocol-based carefor early septic shock. N Engl J Med 370: 16831693, 2014 PubMed
3. The ARISE Investigators and the ANZICS Clinical Trials Group: Goal-directed resuscitation for patients with early septic shock. N Engl J Med371: 14961506, 2014 PubMed
4. Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ,Grieve RD,