Neonatal Jaundice
17
Click here to load reader
-
Upload
alya-afifa -
Category
Documents
-
view
151 -
download
0
Transcript of Neonatal Jaundice

Neonatal jaundice
Neonatal jaundice or Neonatal hyperbilirubinemia is a yellowing of the skin and other tissues of a newborn infant. A bilirubin level of more than 85 umol/l (5 mg/dL) manifests clinicaljaundice in neonates whereas in adults a level of 34 umol/l (2 mg/dL) would look icteric. In newborns jaundice is detected by blanching the skin with digital pressure so that it reveals underlying skin and subcutaneous tissue. Jaundice newborns have an apparent icteric sclera, and yellowing of the face, extending down onto the chest.
In neonates the dermal icterus is first noted in the face and as the bilirubin level rises proceeds caudal to the trunk and then to the extremities.[1]
This condition is common in newborns affecting over half (50 -60%) of all babies in the first week of life.[2]
Notoriously inaccurate rules of thumb have been applied to the physical exam of the jaundiced infant. Some include estimation of serum bilirubin based on appearance. One such rule of thumb includes infants whose jaundice is restricted to the face and part of the trunk above theumbilicus, have the bilirubin less than 204 umol/l (12 mg/dL) (less dangerous level). Infants whose palms and soles are yellow, have serum bilirubin level over 255 umol/l (15 mg/dL) (more serious level).
Studies have shown that trained examiners assessment of levels of jaundice show moderate agreement with icterometer bilirubin measurements.[1]
In infants jaundice can be measured using invasive or non-invasive methods. In non-invasive method Ingram icterometers and Transcutaneous bilirubinometers are used.
Classification
Physiological jaundice
Most infants develop visible jaundice due to elevation of unconjugated bilirubin concentration during their first week. This common condition is called physiological jaundice. This pattern of hyperbilirubinemia has been classified into two functionally distinct periods.
Phase one
1. Term infants - jaundice lasts for about 10 days with a rapid rise of serum bilirubin up to 204 umol/l (12 mg/dL).
2. Preterm infants - jaundice lasts for about two weeks, with a rapid rise of serum bilirubin up to 255 umol/l (15 mg/dL).
Phase two - bilirubin levels decline to about 34 umol/l (2 mg/dL) for two weeks, eventually mimicking adult values.
1. Preterm infants - phase two can last more than one month.
2. Exclusively breastfed infants - phase two can last more than one month.

Causes
Possible mechanisms involved in physiological jaundice
1. Increase bilirubin load on liver cells:
Increased red blood cell (RBC) volume
Increased labeled bilirubin
Increased circulation of bilirubin in the liver
Decreased RBC survival
2. Defective hepatic uptake of bilirubin from blood plasma:
Decreased ligadin (Y protein)
Increased binding of Y proteins by other anions
Decreased liver uptake especially in phase two
3. Defective billirubin conjugation:
Decreased UDPG activity
4. Defective bilirubin excretion
Pathological Jaundice of Neonates (Unconjugated Pathological Hyperbilirubinemia)
Any of the following features characterizes pathological jaundice:
1. Clinical jaundice appearing in the first 24 hours or greater than 48hrs of life.
2. Increases in the level of total bilirubin by more than 8.5 umol/l (0.5 mg/dL) per hour or (85 umol/l) 5 mg/dL per 24 hours.
3. Total bilirubin more than 331.5 umol/l (19.5 mg/dL) (hyperbilirubinemia).
4. Direct bilirubin more than 34 umol/l (2.0 mg/dL).
Differentiating Physiological and Pathological Jaundice
The aim of clinical assessment is to distinguish physiological from pathological jaundice. The sign which helps to differentiate pathological jaundice of neonates from physiological jaundice of neonates are presence of intrauterine growth restriction, stigma of intrauterine infections (e.g. cataracts, microcephaly, hepatosplenomegaly etc.), cephalhematoma, bruising, signs of intraventricular hemorrhage etc. History of illness is noteworthy. Family history of jaundice and anemia, family history of neonatal or early infant death due to liver disease, maternal illness suggestive of viral infection (fever, rash or lymphadenopathy), Maternal drugs (e.g. Sulphonamides, anti-malarials causing hemolysis inG-6-PD deficiency) are suggestive of pathological jaundice in neonates.
[edit]Causes of jaundice

In neonates, jaundice tends to develop because of two factors - the breakdown of fetal hemoglobin as it is replaced with adult hemoglobin and the relatively immature hepatic metabolic pathways which are unable to conjugate and so excrete bilirubin as quickly as an adult. This causes an accumulation of bilirubin in the blood (hyperbilirubinemia), leading to the symptoms of jaundice.
If the neonatal jaundice does not clear up with simple phototherapy, other causes such as biliary atresia, PFIC, bile duct paucity, Alagille's syndrome, alpha 1 and other pediatric liver diseases should be considered. The evaluation for these will include blood work and a variety of diagnostic tests. Prolonged neonatal jaundice is serious and should be followed up promptly.
Severe neonatal jaundice may indicate the presence of other conditions contributing to the elevated bilirubin levels, of which there are a large variety of possibilities (see below). These should be detected or excluded as part of the differential diagnosis to prevent the development of complications. They can be grouped into the following categories:
Neonatal jaundice
Unconjugated
bilirubin
Conjugated bilirubin
Pathologic Physiological jaundice of Neonates
Hepatic Post-
hepatic
Hemolytic Non-hemolytic
Intrinsic Extrinsic

causes causes
[edit]Non Conjugated
[edit]Hemolytic
[edit]Intrinsic causes of hemolysis
Membrane conditions
Spherocytosis
Hereditary ellipsoidosis
Systemic conditions
Sepsis
Arteriovenous malformation
Enzyme conditions
Glucose-6-phosphate dehydrogenase deficiency (also called G6PD deficiency)
Pyruvate kinase deficiency
Globin synthesis defect
sickle cell disease
Alpha-thalassemia , e.g. HbH disease
[edit]Extrinsic causes of hemolysis
Alloimmunity (The neonatal or cord blood gives a positive direct Coombs test and the maternal blood gives a positive indirect Coombs test)
Hemolytic disease of the newborn (ABO) [3]
Rh disease
Hemolytic disease of the newborn (anti-Kell)
Hemolytic disease of the newborn (anti-Rhc)
Other blood type mismatches causing hemolytic disease of the newborn
Breast milk feeding.
[edit]Non-hemolytic causes
Cephalohematoma
Polycythemia
Sepsis
Hypothyroidism
Gilbert's syndrome
Crigler-Najjar syndrome
[edit]Conjugated
[edit]Hepatic causes

Infections
Sepsis
Hepatitis B
TORCH infections
Metabolic
Galactosemia
Alpha-1-antitrypsin deficiency
Cystic fibrosis
Drugs
Total parenteral nutrition
Idiopathic
[edit]Post-hepatic
Biliary atresia or Bile duct obstruction
Alagille syndrome
[edit]Non-organic causes
[edit]Breast feeding jaundice
"Breastfeeding jaundice" or "lack of breastfeeding jaundice," is caused by insufficient breast milk intake,[4] resulting in inadequate quantities of bowel movements to remove bilirubin from the body. This can usually be ameliorated by frequent breastfeeding sessions of sufficient duration to stimulate adequate milk production. Passage of the baby through the vagina during birth helps stimulate milk production in the mother's body, so infants born by cesarean section are at higher risk for this condition[citation needed].
[edit]Breast milk jaundice
Whereas breast feeding jaundice is a mechanical problem, breast milk jaundice is more of a biochemical problem. The term applies to jaundice in a newborn baby.
First, at birth, the gut is sterile, and normal gut flora takes time to establish. The bacteria in the adult gut convert conjugated bilirubin tostercobilinogen which is then oxidized to stercobilin and excreted in the stool. In the absence of sufficient bacteria, the bilirubin is de-conjugated by brush border β-glucuronidase and reabsorbed. This process of re-absorption is called enterohepatic circulation. It has been suggested that bilirubin uptake in the gut (enterohepatic circulation) is increased in breast fed babies, possibly as the result of increased levels of epidermal growth factor (EGF) in breast milk.[5]
Second, the breast-milk of some women contains a metabolite of progesterone called 3-alpha-20-beta pregnanediol. This substance inhibits the action of the enzyme uridine diphosphoglucuronic acid (UDPGA) glucuronyl transferase responsible for conjugation and subsequent excretion of bilirubin. In the newborn liver, activity of glucuronyl transferase is

only at 0.1-1% of adult levels, so conjugation of bilirubin is already reduced. Further inhibition of bilirubin conjugation leads to increased levels of bilirubin in the blood [6][citation
needed]. However, these results have not been supported by subsequent studies.[7]
Third, an enzyme in breast milk called lipoprotein lipase produces increased concentration of nonesterified free fatty acids that inhibit hepatic glucuronyl transferase, which again leads to decreased conjugation and subsequent excretion of bilirubin [8][citation needed].
Despite the advantages of breast feeding, there is a strong association of breast feeding with neonatal hyperbilirubinemia and thus risk ofkernicterus, though this is uncommon. Serum bilirubin levels may reach as high as 30 mg/dL. Jaundice should be managed either with phototherapy or with exchange blood transfusion as is needed. Breast feeds however need not be discontinued. The child should be kept well hydrated and extra feeds given.
[edit]Non-invasive measurement of jaundice
Clinical Assessment Kramer's rule
This method is more accurate and less subjective in estimating jaundice.
Ingram icterometer: In this method a piece of transparent plastic known as Ingram icterometer is used. Ingram icterometer is painted in five transverse strips of graded yellow lines. The instrument is pressed against the nose and the yellow colour of the blanched skin is matched with the graded yellow lines and biluribin level is assigned.
Transcutaneous bilirubinometer: This is hand held, portable and rechargeable but expensive and sophisticated. When pressure is applied to the photoprobe, a xenon tube generates a strobe light, and this light passes through the subcutaneous tissue. The reflected light returns through the second fiber optic bundle to the spectrophotometric module. The intensity of the yellow color in this light, after correcting for the hemoglobin, is measured and instantly displayed in arbitrary units.
[edit]Treatment
The bilirubin levels for initiative of phototherapy varies depends on the age and health status of the newborn. However any newborn with a total serum bilirubin greater than 359 umol/l ( 21 mg/dL ) should receive phototherapy.[9]
[edit]Phototherapy
The use of phototherapy was first discovered, accidentally, at Rochford Hospital in Essex, England. The ward sister (Charge Nurse) of the premature baby unit, firmly believed that the infants under her care benefited from fresh air and sunlight in the courtyard. Although this led to the first noticing of jaundice being improved with sunlight, further studies only progressed when a vial of blood sent for bilirubin measurement sat on a windowsill in the lab for several hours. The results indicated a much lower level of bilirubin than expected based on the patient's visible

jaundice. Further investigation lead to the determination that blue light, wavelength of 420-448 nm, oxidized the bilirubin to biliverdin, a soluble product that does not contribute to kernicterus. Although some pediatricians began using phototherapy in the United Kingdom following Dr. Cremer's publishing the above facts in the Lancet in 1958, most hospitals only began to regularly use phototherapy ten years later when an American group independently made the same discovery.[10][11]
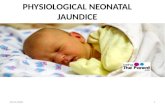
newborn infant undergoing (white light) phototherapy to treat neonatal jaundice
Infants with neonatal jaundice are treated with colored light called phototherapy. Physicians randomly assigned 66 infants 35 weeks of gestation to receive phototherapy. After 15±5 the levels of bilirubin, a yellowish bile pigment that in excessive amounts causes jaundice, were decreased down to 0.27±0.25 mg/dl/h in the blue light. This suggests that blue light therapy helps reduce high bilirubin levels that cause neonatal jaundice.[12]
Exposing infants to high levels of colored light changes trans-bilirubin to the more water soluble cis-form which is excreted in the bile. Scientists studied 616 capillary blood samples from jaundiced newborn infants. These samples were randomly divided into three groups. One group contained 133 samples and would receive phototherapy with blue light. Another group contained 202 samples would receive room light, or white light. The final group contained 215 samples, and were left in a dark room. The total bilirubin levels were checked at 0, 2, 4, 6, 24, and 48 hours. There was a significant decrease in bilirubin in the first group exposed to phototherapy after two hours, but no change occurred in the white light and dark room group. After 6 hours, there was a significant change in bilirubin level in the white light group but not the dark room group. It took 48 hours to record a change in the dark room group’s bilirubin level. Phototherapy is the most effective way of breaking down a neonate’s bilirubin.[13]
Phototherapy works through a process of isomerization that changes trans-bilirubin into the water-soluble cis-bilirubin isomer.[14][15]
In phototherapy, blue light is typically used because it is more effective at breaking down bilirubin (Amato, Inaebnit, 1991). Two matched groups of newborn infants with jaundice were exposed to intensive green or blue light phototherapy. The efficiency of the treatment was measured by the rate of decline of serum bilirubin, which in excessive amounts causes jaundice, concentration after 6, 12 and 24 hours of light exposure. A more rapid response was obtained using the blue lamps than the green lamps. However, a shorter phototherapy recovery period was noticed in babies exposed to the green lamps(1). Green light is not commonly used because exposure time must be longer to see dramatic results(1).
Ultraviolet light therapy may increase the risk of or skin moles, in childhood. While an increased number of moles is related to an increased risk of skin cancer,[16][17][18] it is not ultraviolet light that is used for treating neonatal jaundice. Rather, it is simply a specific frequency of blue light that does not carry these risks.

Increased feedings help move bilirubin through the neonate’s metabolic system.[19]
The light can be applied with overhead lamps, which means that the baby's eyes need to be covered, or with a device called a Biliblanket, which sits under the baby's clothing close to its skin.
[edit]Exchange transfusions
Much like with phototherapy the level at which exchange transfusions should occur depends on the health status and age of the newborn. It should however be used for any newborn with a total serum bilirubin of greater than 428 umol/l ( 25 mg/dL ).[9]
[edit]Complications
Prolonged hyperbilirubinemia (severe jaundice) can result into chronic bilirubin encephalopathy (kernicterus).[20][21] Quick and accurate treatment of neonatal jaundice helps to reduce the risk of neonates developing kernicterus.[22]
An effect of kernicterus is a fever. A male full term neonate had hyperbilirubinemia (kernicterus) and jaundice at the age of 4 days old. He displayed symptoms of increased lethargy, refusal to eat, and had a fever. The neonate who was diagnosed with kernicterus displayed symptoms of a fever.[23]
Another effect of kernicterus is seizures. The Neonatal Unit at Allied Hospital Faisalabad studied 200 neonates of either gender who presented seizures during their hospital stay from April 2003 to June 2004. The seizures were evaluated and one cause of the seizures was kernicterus. 4.5%, or 9 neonates, displayed seizures caused by kernicterus.[24]
High pitched crying is an effect of kernicterus. Scientists used a computer to record and measure cranial nerves 8, 9 and 12 in 50 infants who were divided into two groups equally depending upon bilirubin concentrations. Of the 50 infants, 43 had tracings of high pitched crying.[25]
Exchange transfusions performed to lower high bilirubin levels are an aggressive treatment.[26][27]
2.5. Patogenesis
Patogenesis kern ikterus bersifat multi faktorial dan melibatkan interaksi antara kadar bilirubin
yang tidak terjonjugasi, ikatan albumin dan kadar bilirubin yang tak terikat/bebas, menembusnya
ke sawar darah otak, dan kerentanan neurologik terhadap jejas. Permeabilitas sawar darah otak
dapat dipengaruhi oleh penyakit, asfiksia, dan maturasi otak.
Pada setiap bayi, nilai persis kadar bilirubin yang dapat bereaksi indirek atau kadar bilirubin
bebas dalam darah yang kalau dilebihi akan bersifat toksik, tidak dapat diramalkan, tetapi kern
ikterus jarang terjadi pada bayi cukup bulan yang sehat dan pada bayi tanpa adanya hemolisis,

yaitu bila kadar serum berada di bawah 25 mg/dL. Pada bayi yang mendapat ASI, kern ikterus
dapat terjadi bila kadar bilirubin melebihi 30 mg/dL, meskipun batasannya luas yaitu antara 21-
50 mg/dL. Onset terjadi dalam minggu pertama kehidupan, tetapi dapat terjadi terlambat hingga
minggu ke-2 bahkan minggu ke-3. Lamanya waktu pemajanan yang diperlukan untuk
menimbulkan pengaruh toksik juga belum diketahui. Bayi yang kurang matur lebih rentan
terhadap kern ikterus.
Resiko pengaruh toksik dari meningkatnya kadar bilirubin tak terkonjugasi dalam serum menjadi
bertambah dengan adanya faktor-faktor yang mengurangi retensi bilirubin dalam sirkulasi, yaitu
hipoproteinemia, perpindahan bilirubin dari tempat ikatannya pada albumin karena ikatan
kompetitif obat-obatan seperti sulfisoksazol dan moksalaktam, asidosis, kenaikan sekunder asam
lemak bebas akibat hipoglikemia, kelaparan, atau hipotermia) atau oleh faktor-faktor yang
meningkatkan permeabilitas sawar darah otak atau membran sel saraf terhadap bilirubin, atau
kerentanan sel otak terhadap toksisitasnya seperti asfiksia, prematuritas, hiperosmolalitas, dan
infeksi2.
Permukaan otak biasanya berwarna kuning pucat. Pada pemotongan, daerah-daerah tertentu
secara khas berwarna kuning akibat bilirubin tak terkonjugasi, terutama pada korpus
subtalamikus, hipokampus dan daerah olfaktorius yang berdekatan, korpus striata, talamus,
globus palidus, putamen, klivus inferior, nukleus serebelum, dan nukleus saraf kranial. Daerah
yang tak berfigmen juga dapat cedera. Hilangnya neuron, gliosis reaktif dan atrofi sistem serabut
yang terlibat ditemukan pada penyakit yang lebih lanjut. Pola jejas dihubungkan dengan
perkembangan sistem enzim oksidatif pada berbagai daerah otak dan bertumpang-tindih dengan
yang terdapat pada cedera otak hipoksik. Bukti yang mendukung hipotesis bahwa bilirubin
mengganggu penggunaan oksigen oleh jaringan otak, mungkin dengan menimbulkan jejas pada
membran sel; jejas hipoksia yang telah terjadi sebelumnya meningkatkan kerentanan sel otak
terhadap jejas. Pewarnaan bilirubin yang jelas tanpa hiperbilirubinemia atau perubahan
mikroskopik yang spesifik kern ikterus mungkin tidak merupakan kesatuan yang sama2, 9, 10.
2.6. Kriteria Diagnosis

Secara umum, ditandai dengan athetoid cerebral palsy, gangguan pendengaran hingga ketulian,
gangguan penglihatan, dan mental retardasi.
Tanda-tanda dan gejala-gejala kern ikterus biasanya muncul 2-5 hari sesudah lahir pada
bayi cukup bulan dan paling lambat hari ke-7 pada bayi prematur, tetapi hiperbilirubinemia dapat
menyebabkan sindroma setiap saat selama masa neonatus. Tanda-tanda awal bisa tidak terlihat
jelas dan tidak dapat dibedakan dengan sepsis, asfiksia, hipoglikemia, pendarahan intrakranial
dan penyakit sistemik akut lainnya pada bayi neonatus. Lesu, nafsu makan jelek dan hilangnya
refleks Moro merupakan tanda-tanda awal yang lazim. Selanjutnya, bayi dapat tampak sangat
sakit, tidak berdaya disertai refleks tendo yang menjadi negatif dan kegawatan pernapasan.
Opistotonus, dengan fontanela yang mencembung, muka dan tungkai berkedut, dan tangisan
melengking bernada tinggi dapat menyertai. Pada kasus yang lanjut terjadi konvulsi dan spasme,
kekakuan pada bayi dengan lengan yang terekstensi dan berotasi ke dalam serta tangannya
menggenggam. Rigaditas jarang terjadi pada stadium lanjut2.
Banyak bayi yang menjelek ke tanda-tanda neurologis berat ini meninggal; yang bertahan hidup
biasanya mengalami cedera berat tetapi agaknya dapat sembuh dan 2-3 bulan kemudian timbul
beberapa kelainan. Selanjutnya, pada usia 1 tahun opistotonus, rigiditas otot, gerakan yang tidak
teratur dan konvulsi cenderung kambuh. Pada tahun ke-2 opistotonus dan kejang mereda, tetapi
gerakan-gerakan yang tidak teratur dan tidak disadari, rigiditas otot atau pada beberapa bayi,
hipotonia bertambah secara teratur. Pada umur 3 tahun sering tampak sindrom neurologis yang
lengkap terdiri atas koreotetosis dengan spasme otot involunter, tanda-tanda ekstrapira-midal,
kejang defisiensi mental, wicara disartrik, kehilangan pendengaran terhadap frekuensi tinggi,
strabismus dan gerakan mata ke atas tidak sempurna. Tanda-tanda piramidal, hipotonia, atau
ataksia terjadi beberapa bayi. Pada bayi yang terkenanya ringan sindrom ini hanya dapat ditandai
melalui inkoordonasi neoromuskular ringan sampai sedang, ketilian parsial, atau “disfungsi otak
minimal” yang terjadi sendiri atau bersamaan, masalah ini mungkin tidak tampak sampai anak
masuk sekolah
Prognosis

Tanda-tanda neurologis yang jelas mempunyai prognosis yang jelek, ada 74 % atau lebih
bayi-bayi yang demikian meninggal, dan 80 % yang bertahan hidup menderita koreoatetosis
bilateral dengan spasme otot involunter. Retardasi mental, ketulian, dan kuadriplegia spastis
lazim terjadi. Bayi yang beresiko harus menjalani skrining pendengaran2.
2.11. Pencegahan
- Segera menurunkan kadar bilirubin indirek.
- Penanganan bayi ikterus; fototerapi, kemoterapi, transfusi tukar.
Bayi dengan kadar bilirubin tinggi diobati dengan menggunakan fototerapi, bahkan
dengan transfusi tukar. Kini terdapat obat baru yaitu Stanate yang dalam ujicoba terbukti dapat
memblokade produksi bilirubin sehingga dapat mencegah kern ikterus, hingga sekarang obat ini
masih terus dikembangkan4.
Tanpa memandang etiologi, tujuan terapi adalah mencegah kadar yang memungkinkan
terjadinya neurotoksikosis, dianjurkan agar fototerapi, dan jika tidak berhasil, transfusi tukar
dilakukan untuk mempertahankan kadar maksimum bilirubin total dalam serum di bawah kadar
yang ditunjukkan pada tabel 1 (untuk preterm) dan tabel 2 (untuk bayi cukup bulan). Pada setiap
bayi, resiko jejas bilirubin terhadap sistem saraf pusat harus dipertimbangkan dengan resiko yang
ditimbulkan oleh pengobatan. Belum ada persetujuan yang umum mengenai kriteria untuk
memulai fototerapi. Karena fototerapi mungkin memerlukan 6-12 jam untuk mempunyai
pengaruh yang dapat diukur, maka fototerapi ini harus dimulai saat kadar bilirubun masih berada
di bawah kadar yang diindikasi untuk transfusi darah. Bila teridentifikasi, penyebab dasar dasar
ikterus harus diobati, misalnya antibiotik untuk septikemia. Faktor-faktor fisiologis yag
menambah resiko cedera neurologis harus diobati juga (misalnya koreksi terhadap asidosis)2.
Fototerapi biasanya dimulai pada 50-70 % dari kadar maksimum bilirubin indirek. Jika
nilai sangat melebihi kadar ini, jika fototerapi tidak berhasil mengurangi kadar bilirubin
maksimum, atau jika ada tanda-tanda kern ikterus, transfusi tukar merupakan indikasi. Jadi jika
ada tanda-tanda kern ikterus selama evaluasi atau pengobatan, pada kadar bilirubin berapapun,
maka transfusi tukar darurat harus dilakukan2.

- Melakukan pemeriksaan kadar bilirubin pada semua bayi baru lahir sebelum meninggalkan
Rumah Sakit.
- Kontrol bayi baru lahir ke dokter dalam jangka waktu 24-48 jam setelah meninggalkan Rumah
Sakit.
- Meningkatkan pengetahuan orang tua tentang ikterus
Tabel 1.
Kadar bilirubin serum indirek maksimum yang disarankan pada bayi preterm.
Berat Badan Lahir
(gram)
Tidak Ada Komplikasi
(g/dL)
Ada Komplikasi*
(g/dL)
<>
1000-1250
1251-1499
1500-1999
2000-2500
12-13
12-14
14-16
16-20
20-22
10-12
10-12
12-14
15-17
18-20
*Komplikasi meliputi asfiksia perinatal, asidosis, hipoksia, hipotermia, hipoalbuminemia, meningitis, PIV,
hemolisis, hipoglikemia, atau tanda-tanda kern ikterus.