Neonatal ECMO Study of Temperature (NEST): A...
12
Neonatal ECMO Study of Temperature (NEST): A Randomized Controlled Trial WHAT’S KNOWN ON THIS SUBJECT: Although providing improved survival for infants with very severe cardiorespiratory problems, the use of neonatal extracorporeal membrane oxygenation has high rates of disability in survivors. Mild hypothermia has been shown to limit brain injury in a range of patient groups, including newborns. WHAT THIS STUDY ADDS: Infants who received extracorporeal membrane oxygenation and mild hypothermia did not show an improved neurodevelopmental outcome, and nonsignificant trends in the data suggested a small adverse effect. Use of hypothermia in other potential patient groups should be thoroughly tested. abstract BACKGROUND: Despite evidence to support the use of extracorporeal membrane oxygenation (ECMO) in defined groups of newborn infants, rates of impairment among survivors remain high. Therapeutic hypo- thermia has been shown to provide neuroprotection in mature infants exposed to perinatal asphyxia. We hypothesized that therapeutic hy- pothermia during ECMO would reduce the proportion of infants with brain injury, and thus later impairment. METHODS: We conducted a randomized trial in the United Kingdom to compare ECMO with cooling (34°C for the first 48 to 72 hours) with standard ECMO (37°C). The primary outcome was the cognitive com- posite score of the Bayley Scales of Infant and Toddler Development, 3rd edition, at 2 years. Prespecified secondary outcomes included death, neonatal morbidity, and other neurodevelopmental and behav- ioral outcomes at 2 years. RESULTS: A total of 111 infants were entered into the study, 14 died before 2 years of age (16% who received ECMO with cooling vs 9% who received ECMO alone). Two infants were lost to follow-up, and 8 were unable to complete the full range of tests. For 45 evaluated infants who received ECMO with cooling, mean cognitive scores at 2 years were 88.0 (SD: 16.2) compared with 90.6 (SD: 13.1) for 48 infants receiving ECMO only (difference in means: 22.6; 95% confidence interval: 28.7 to 3.4). The various secondary outcomes were not significantly different between the groups, but most favored ECMO without cooling. CONCLUSIONS: In newborn infants treated by ECMO, the use of mild hypothermia for the first 48 to 72 hours did not result in improved outcomes up to 2 years of age. Pediatrics 2013;132:e1247–e1256 AUTHORS: David Field, DM, on behalf of the NEST Study Collaborative Group Department of Health Sciences, University of Leicester, Leicester, United Kingdom KEY WORDS neonatal, ECMO, hypothermia ABBREVIATIONS aEEG—amplitude-integrated electroencephalography Bayley-III—Bayley Scales of Infant and Toddler Development, Third Edition CI—confidence interval ECMO—extracorporeal membrane oxygenation RR—relative risk Dr Field conceptualized and designed the study, secured funding, co-supervised the running of the trial, drafted the initial manuscript, and approved the final manuscript as submitted. This trial has been registered with Current Controlled Trials (identifier ISRCTN72635512). www.pediatrics.org/cgi/doi/10.1542/peds.2013-1754 doi:10.1542/peds.2013-1754 Accepted for publication Aug 23, 2013 This work was presented in part at Hot Topics in Neonatology; December 3, 2012; Washington, DC. Address correspondence to David Field, DM, Department of Health Sciences, University of Leicester, 22-28 Princess Rd West, Leicester, UK. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The author has indicated he has no financial relationships relevant to this article to disclose. FUNDING: Supported by the British Heart Foundation in the form of a research grant. The funders had no direct role in developing the protocol or undertaking the study. POTENTIAL CONFLICT OF INTEREST: The author has indicated he has no potential conflicts of interest to disclose. PEDIATRICS Volume 132, Number 5, November 2013 e1247 ARTICLE by guest on June 22, 2018 www.aappublications.org/news Downloaded from
Transcript of Neonatal ECMO Study of Temperature (NEST): A...

Neonatal ECMO Study of Temperature (NEST):A Randomized Controlled Trial
WHAT’S KNOWN ON THIS SUBJECT: Although providing improvedsurvival for infants with very severe cardiorespiratory problems,the use of neonatal extracorporeal membrane oxygenation hashigh rates of disability in survivors. Mild hypothermia has beenshown to limit brain injury in a range of patient groups, includingnewborns.
WHAT THIS STUDY ADDS: Infants who received extracorporealmembrane oxygenation and mild hypothermia did not show animproved neurodevelopmental outcome, and nonsignificanttrends in the data suggested a small adverse effect. Use ofhypothermia in other potential patient groups should bethoroughly tested.
abstractBACKGROUND: Despite evidence to support the use of extracorporealmembrane oxygenation (ECMO) in defined groups of newborn infants,rates of impairment among survivors remain high. Therapeutic hypo-thermia has been shown to provide neuroprotection in mature infantsexposed to perinatal asphyxia. We hypothesized that therapeutic hy-pothermia during ECMO would reduce the proportion of infants withbrain injury, and thus later impairment.
METHODS: We conducted a randomized trial in the United Kingdom tocompare ECMO with cooling (34°C for the first 48 to 72 hours) withstandard ECMO (37°C). The primary outcome was the cognitive com-posite score of the Bayley Scales of Infant and Toddler Development,3rd edition, at 2 years. Prespecified secondary outcomes includeddeath, neonatal morbidity, and other neurodevelopmental and behav-ioral outcomes at 2 years.
RESULTS: A total of 111 infants were entered into the study, 14 diedbefore 2 years of age (16% who received ECMO with cooling vs 9%who received ECMO alone). Two infants were lost to follow-up, and8 were unable to complete the full range of tests. For 45 evaluatedinfants who received ECMO with cooling, mean cognitive scores at 2years were 88.0 (SD: 16.2) compared with 90.6 (SD: 13.1) for 48infants receiving ECMO only (difference in means: 22.6; 95%confidence interval: 28.7 to 3.4). The various secondary outcomeswere not significantly different between the groups, but mostfavored ECMO without cooling.
CONCLUSIONS: In newborn infants treated by ECMO, the use of mildhypothermia for the first 48 to 72 hours did not result in improvedoutcomes up to 2 years of age. Pediatrics 2013;132:e1247–e1256
AUTHORS: David Field, DM, on behalf of the NEST StudyCollaborative Group
Department of Health Sciences, University of Leicester, Leicester,United Kingdom
KEY WORDSneonatal, ECMO, hypothermia
ABBREVIATIONSaEEG—amplitude-integrated electroencephalographyBayley-III—Bayley Scales of Infant and Toddler Development,Third EditionCI—confidence intervalECMO—extracorporeal membrane oxygenationRR—relative risk
Dr Field conceptualized and designed the study, securedfunding, co-supervised the running of the trial, drafted the initialmanuscript, and approved the final manuscript as submitted.
This trial has been registered with Current Controlled Trials(identifier ISRCTN72635512).
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1754
doi:10.1542/peds.2013-1754
Accepted for publication Aug 23, 2013
This work was presented in part at Hot Topics in Neonatology;December 3, 2012; Washington, DC.
Address correspondence to David Field, DM, Department ofHealth Sciences, University of Leicester, 22-28 Princess Rd West,Leicester, UK. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The author has indicated he has nofinancial relationships relevant to this article to disclose.
FUNDING: Supported by the British Heart Foundation in the formof a research grant. The funders had no direct role indeveloping the protocol or undertaking the study.
POTENTIAL CONFLICT OF INTEREST: The author has indicated hehas no potential conflicts of interest to disclose.
PEDIATRICS Volume 132, Number 5, November 2013 e1247
ARTICLE
by guest on June 22, 2018www.aappublications.org/newsDownloaded from

Extracorporeal membrane oxygenation(ECMO) is an invasive method of lifesupport used for newborn infants withacute respiratory failure and has beenshown to lead to improved outcomes.1
Despite the availability of new thera-pies, such as inhaled nitric oxide andhigh-frequency oscillation, the majorityof infants who develop the severestforms of cardiorespiratory failure stillare treated with ECMO, and the numberof referrals reported to the Extracor-poreal Life Support Organization hasremained steady since the end of the1990s.
The Cochrane review of neonatal ECMOconcludes that, compared with otherforms of intervention, ECMO is the mosteffective form of life support for infantsthat fulfills the eligibility criteria, bothin terms of improved survival and mor-bidity.2 However, childhood outcomedata from the UK collaborative ECMOtrial, the main trial included in theCochrane review, indicated that de-spite improved outcome comparedwith more conventional life support,rates of impairment and disabilityremained high.3,4 Only 32% of theoriginal cohort of infants allocated toECMO in that study survived withoutdisability at 4 years of age comparedwith 14% in the conventional treatmentarm. The origin of these impairmentsmay stem both from the underlyingcondition and from changes in cerebralperfusion that accompany the processof ECMO.3,4
There is increasing evidence of aneuroprotective effect from mild ther-apeutic hypothermia in different pa-tient groups, after a variety of cerebralinsults, but particularly in infants afteracute hypoxia-ischemia.5,6 We thereforeset out to test the potential for hypo-thermia to improve the outcome ofinfants who received neonatal ECMO.After a series of safety and feasibilitystudies relating to the use of mild hy-pothermia during neonatal ECMO,7–9
the 4 hospitals comprising the UK na-tional ECMOservice agreed to participatein a pragmatic multicenter randomizedcontrolled trial, the Neonatal ECMO Studyof Temperature (NEST). The aim of thistrial was to evaluate whether, in infantsrequiring ECMO, cooling to 34°C for thefirst 48 to 72 hours of their ECMO courseled to improved health status at age2 years.
METHODS
Trial Design and Participants
Thiswasa2-armrandomizedcontrolledtrial comparing outcomes for infantsallocated to receive ECMO and coolingwith infants allocated to receive stan-dard (normothermic) ECMO; methodsare reported in full in the publishedprotocol.10 All participants were caredfor in 1 of the 4 UK ECMO centers andincluded infants transferred fromother hospitals across the country forcare. Each infant met existing standardcriteria for ECMO eligibility based onthe clinical decision of the local ECMOteam. Infants were excluded if they
� were referred for ECMO because ofa diagnosis of congenital diaphrag-matic hernia (because of an in-creased inherent risk of poorneurodevelopmental outcome andpotentially severe underlying pul-monary hypoplasia incompatiblewith long-term survival);
� received ECMO post–cardiac sur-gery (because these infants werenot part of the original underpin-ning study and their prognosiswas likely to be heavily influencedby their primary diagnosis); or
� had received any therapeutic cool-ing before randomization.
Because of the life-threatening condi-tion of the infants involved and the needto carry out long-distance transfers ina high proportion of cases, consentprocedures involved a 2-stage process.Written (wherever possible) orwitnessed
verbal consent was taken in the firstinstance, and this consent was reaf-firmed within the subsequent 24 to 48hours with documentation in theinfant’s medical record.
Intervention and ClinicalManagement
For participants randomly assigned toreceive mild hypothermia, the processof cooling commenced immediatelyupon initiation of the ECMO circuit byadjustment of the heat exchanger in thecircuit to achieve a core temperature of34°C. Temperature was measured bynasopharyngeal, rectal, or urinary ele-ctronic temperature probes; and thewater heater was adjusted to maintainthis core temperature. All infants in thisarm received a minimum of 48 hours ofcooling (to allow for any infant thatrapidly improved while receiving ECMO)to a maximum of 72 hours before beingrewarmed over a 12-hour period, inkeeping with the published neuro-protection trials.5,6 Those infants ran-domly assigned to the control arm ofthe study received conventional ECMOthroughout, with a targeted body tem-perature of 37°C.
Apart from the temperature during thefirst 48 to 72 hours, all other aspects ofmanagement were identical withineach ECMO center. For those success-fully weaned from ECMO, referral backto their local hospital occurred whenconsidered safe by the clinical team inthe ECMO center.
As well as the routine intensive moni-toring associated with ECMO, cerebralamplitude-integrated electroencepha-lography (aEEG) recording was at-tempted in all infants during the first 72hours of ECMO. Cerebral ultrasoundassessments were also performedduring the infant’s stay in the ECMOcenter on the basis of clinical need.Most infants had left the ECMO centerbefore they were well enough to un-dergoMRI scanning of their brain; local
e1248 FIELD by guest on June 22, 2018www.aappublications.org/newsDownloaded from

units receiving the infants back afterECMOwere encouraged to performMRIscans, but this decision was left to theirdiscretion.
Outcomes
The primary outcome was the cognitivescore from the Bayley Scales of Infantand Toddler Development, Third Edition(Bayley-III), at 2 years of age correctedfor prematurity where relevant (24–27months).11 All infants were assessed bythe same pediatrician, who was blin-ded to the original allocation, in anappropriate clinical setting close totheir home or at home in a few cases.Death was not included in a compositeprimary outcome, because our in-terpretation of the literature at thetime the protocol was developed wasthat mild hypothermia was unlikely toinfluence mortality and hence wechose to focus on the outcome forwhich there was significant biologicalplausibility that a benefit might result.However, death was included as a sec-ondary outcome. A number of addi-tional psychomotor tests as well asa physical examination by the pedia-trician were also carried out. Pre-specified secondary outcomeswere asfollows:
� Death
� Neurologic optimality score12,13
� Gross and fine motor score fromthe Bayley-III11
� Cerebral palsy
� Gross motor function classificationscore14
� Seizures requiring regular anticon-vulsant treatment
� Visual difficulties not corrected byeyeglasses
� Hearing difficulties requiring aids
� Language-expressive and -recep-tive scores from the Bayley-III11
� Parent Report of Children’s Abili-ties-revised15–17
� Infant Characteristics Question-naire18
� The Brief Infant-Toddler Social andEmotional Assessment19
� Measures of growth: height, weight,and head circumference20
� Rates of “no impairment” (Bayley-III cognition, language, and motorscores $85; normal neurologic ex-amination; normal vision [includ-ing glasses]; and normal hearingwithout aids)
Sample Size
The sample size estimate was based onwhat was considered to be a clinicallyimportant difference in the Bayley-IIIcognitive score at 2 years’ correctedage, based on existing knowledge ofECMO survivors. Given that the primaryoutcome could be assessed only insurvivors, the sample size estimatewas inflated to allow for mortalityamong those who died before the ageof 2 years. Assuming a mean cognitivescore of 95 (SD: 15) in the controlgroup, recruitment of 118 infants withan estimatedmortality of 20% provideda realistic recruitment target (ie, 94surviving infants) while also giving 90%power to detect a 10-point differencebetween the 2 arms with a 2-sided 5%level of significance.
Randomization
Assignment to a treatment group wasperformed by using a secure Web-based system (hosted by the NationalPerinatal Epidemiology Unit, ClinicalTrials Unit, Oxford, UK). As soon as pa-rental consent was obtained, therecruiting ECMO specialist logged ontoa Web site and obtained the treatmentallocation of ECMO only or ECMO withcooling. A deterministic minimizationalgorithmwasused to ensureabalancedtreatment allocationwithin centerandbymethod of cannulation (veno-venous orveno-arterial).
Blinding
The parents, who completed self-reportquestionnaires at 2 years, were awareof the allocation their infant had re-ceived. It was not possible to blind thestaff involved in clinical care of the in-fant during the time on ECMO; however,the pediatrician who performed the 2-year assessments was masked to al-location and parents were asked not toreveal this information.
Statistical Methods
Infants were analyzed in their allocatedgroup, regardless of allocation receivedor deviations from the protocol. For theprimary outcome analysis, the meandifferencein theBayley-III cognitivescorebetween groups and 95% confidenceinterval (CI) were calculated and ana-lyzed by using the independent 2-samplet test. An adjusted analysis was alsoperformed, adjusting for the minimi-zation criteria (center and method ofcannulation).
Secondary outcomes were summarizedwith counts (percentages) for categori-cal variables, means (SD) for normallydistributed continuous variables, ormedians (interquartile or entire range,whichever was appropriate) for skewedcontinuous variables. The magnitudeand direction of the treatment effectswereassessedbycalculatingtherelativerisk (RR; 99% CI) for categorical out-comes, the mean difference (99% CI) fornormally distributed continuous out-comes, and the median difference (99%CI) for skewed continuous variables. SDscores were calculated for growth databy using the British 1990 growth refer-ence (revised September 1996).21
Prespecified subgroup analyses wereperformed by using a statistical test ofinteraction on the following outcomes;Bayley-III cognitive score, vision, hearing,and neurologic optimality score. Ana-lyses were performed by 2 members ofthe NEST research team: Louise Linsell,MSc and Ed Juszczak, MSc.
ARTICLE
PEDIATRICS Volume 132, Number 5, November 2013 e1249 by guest on June 22, 2018www.aappublications.org/newsDownloaded from

The subgroups examined were as fol-lows: initial method of cannulation(veno-arterial versus veno-venous),infant’s worst oxygenation index inthe 4 hours before random assignment(,60 vs $60), initial aEEG patternshown on the cerebral function moni-tor (normal versus abnormal), andprincipal clinical diagnosis leading toECMO referral (severe cardiorespira-tory failure versus other).
Oversight
The NEST protocol was approved by theTrent Multicentre Research Ethics Co-mmittee and the local research ethicscommittee of each participating hospi-tal. The conduct of the study was over-seen by an independent trial steeringcommittee with advice from an in-dependent data monitoring and ethicscommittee. The independent data mon-itoring committee met on 5 occasionsand did not recommend early stopping.
RESULTS
Recruitment and AnalysisPopulation
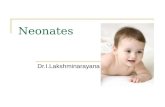
Between June 1, 2006, and March 31,2010, 111 infants were recruited to thetrial, of whom 55 were allocated toECMO only and 56 were allocated toECMO with cooling (Fig 1). We identifiedan additional 46 infants who werescreened and not recruited for a vari-ety of reason including parents de-clined, insufficient to time to seekconsent (generally because of clinicaldeterioration), and nonavailability ofstaff with approval to carry out con-sent. We recognize that a small numberof additional infants would potentiallyhave been eligible for this trial but who,for clinical reasons, were not trans-ferred for ECMO.
Follow-up occurred at 2 years of age andwithin a window of 63 months. Allassessments and neurologic examina-tions were performed by a single pedi-
atric assessor. Fourteen infants diedbefore follow-up at 2 years (12 beforehospital discharge): 5 in the ECMO-onlygroup and 9 in the ECMO-with-coolinggroup. This difference was not signifi-cant, and by chance, 3 deaths relating tounderlying metabolic/congenital anom-alies were all in the cooling arm. Pedi-atric assessments were performed for95 of 97 (98%) survivors (sample sizewas based on 94 survivors). Two survi-vors in the ECMO-only group emigrated,and no data were collected after dis-charge, although 1 infant was known tobe alive at 2 years. The baseline char-acteristics of all infants who were ran-domly assigned (n = 111) and thoseassessed by a pediatrician at age 2 (n =95) were broadly similar (Table 1). Eightassessments were partially completeddue to behavioral problems; however,only 2 of these infants (ECMO with cool-ing) were excluded from the primaryanalysis because in the other 6 infants
the cognitive score component of theassessment was completed. Eighty-eightparent questionnaires were received:there was a response rate of 43 of 48(90%) in the ECMO-only group and 45 of47 (96%) in the ECMO-with-cooling group.
All 111 infants were included in theanalysis wherever data were available.The numbers of infants included in theanalysis of the Bayley-III cognitive com-posite score (primary outcome)were 48of 55 (87%) in the ECMO-only group and45 of 56 (80%) in the ECMO-with-coolinggroup.
Compliance and Clinical OutcomesBefore Discharge
Two infants (ECMO-only group) recov-ered after trial entry and ECMO wasnot required, and 2 infants (ECMO-with-coolinggroup)diedonday2of theECMOrun. An additional 5 infants (4 in theECMO-only group, 1 in the ECMO-with-cooling group) did not require ECMO
FIGURE 1Flow of study participants.
e1250 FIELD by guest on June 22, 2018www.aappublications.org/newsDownloaded from

after 48 hours; hence, these infantsreceived cooling only up until that point(Table 2). It was observed that infantsallocated to ECMO with cooling re-ceived fewer inotropes on days 2 and 3and less heparin throughout the 72-hour period than infants in the ECMO-only group. Clinical characteristicsbefore discharge were similar in both
groups, although the number of eventsfor some conditions was low.
Health and NeurodevelopmentalOutcomes at 2 Years
The mean Bayley-III scores for cognition(primary outcome), language, and mo-tor skills at 2 years’ corrected age wereslightly lower in the ECMO-with-cooling
group; the variances were slightlygreater, but the differences were notstatistically significant (Table 3). Themean cognitive score in the ECMO-onlygroup was 90.6 (SD: 13.1) comparedwith 88.0 (SD: 16.2) in the ECMO-with-cooling group (difference in means:22.6 points; 95% CI: 28.7 to 3.4). Afteradjusting for the minimization factors,
TABLE 1 Characteristics of Infants at Trial Entry
All Randomly Assigned Infants (N = 111) Surviving Infants Assessed at 2 Years(n = 95)
ECMO Only(n = 55)
ECMO WithCooling (n = 56)
ECMO Only(n = 48)
ECMO WithCooling (n = 47)
Center, n (%)Leicester 30 (55) 29 (52) 27 (56) 26 (55)Great Ormond Street 9 (16) 12 (21) 7 (15) 8 (17)Glasgow 10 (18) 11 (20) 8 (17) 10 (21)Newcastle 6 (11) 4 (7) 6 (13) 3 (6)
Birth weight, mean 6 SD, g 3480 6 574 3415 6 601 3488 6 571 3492 6 587Male gender, n (%) 26 (47) 32 (57) 23 (48) 26 (55)Gestation at delivery, mean 6 SD, wk 40.3 6 1.5 39.6 6 1.7 40.3 6 1.5 39.8 6 1.6Intended type of cannulation, n (%)Veno-arterial 13 (24) 14 (25) 9 (19) 10 (21)Veno-venous 42 (76) 42 (75) 39 (81) 37 (78)
Apgar score,4 at 1 minute, n (%) 15 (30) 14 (26) 12 (25) 14 (30)Median score (IQR) 6 (3–9) 6 (3–9) 6 (3–9) 5 (2–7.5)Unknown, n 5 3 4 3
Apgar score,4 at 5 minutes, n (%) 4 (8) 3 (6) 4 (8) 3 (6)Median score (IQR) 8 (5–9) 7 (5–9) 8 (6–9) 7 (5–9)Unknown, n 4 3 3 3
Resuscitation at birth (any), n (%) 31 (56) 36 (64) 26 (54) 34 (72)Resuscitation method (.1 possible), n (%)Face mask oxygen 6 (11) 12 (21) 5 (10) 12 (26)Mask ventilation 19 (35) 28 (50) 17 (35) 27 (57)ET tube ventilation 13 (24) 13 (23) 11 (23) 11 (23)Cardiac massage 3 (5) 2 (4) 3 (6) 2 (4)Resuscitation drugs given 0 (0) 0 (0) 0 (0) 0 (0)
Principal clinical diagnosis leading to ECMO referrala, n (%)Meconium aspiration 12 (22) 14 (25) 11 (23) 14 (30)Persistent pulmonary hypertension 3 (5) 2 (4) 2 (4) 1 (2)Severe cardiorespiratory failure 40 (73) 38 (68) 35 (73) 31 (66)Other 0 (0) 4 (4) 0 (0) 1 (2)
Treatments used before ECMO referral (.1 possible), n (%)Nitric oxide 45 (82) 45 (80) 39 (81) 37 (78)Other pulmonary vasodilators 15 (27) 9 (16) 12 (25) 6 (13)High-frequency oscillation ventilation 39 (71) 35 (63) 35 (73) 28 (60)Surfactant 46 (84) 43 (77) 39 (81) 38 (81)Paralysis 50 (91) 52 (93) 43 (90) 43 (91)Inotropes 48 (87) 48 (86) 41 (85) 39 (83)
Head ultrasound performed before referral, n (%) 51 (93) 46 (82) 44 (92) 40 (85)Evidence of hemorrhage 1 (2) 1 (2) 0 (2) 1 (2)Evidence of parenchymal damage 2 (4) 2 (4) 1 (2) 2 (4)
Clinically recognizable seizures before referral andanticonvulsants given
7 (13) 2 (4) 5 (10) 2 (4)
Worst oxygenation index in the 4 hours before randomizationMedian score (IQR) 41 (28–63) 49 (35–69) 38 (28–61) 49 (34–66)Unknown, n 1 1 1 0
ET, endotracheal; IQR, interquartile range.a Diagnostic category chosen by the referring clinician at the point of randomization.
ARTICLE
PEDIATRICS Volume 132, Number 5, November 2013 e1251 by guest on June 22, 2018www.aappublications.org/newsDownloaded from

center, and intended cannulation, thedifference in means was 22.6 points95% CI:28.7 to 3.5).
Twelve deaths occurred before hospitaldischarge (4 ECMOonlyand8ECMOwithcooling), and 2 additional deaths werereported (1 in each arm) after dis-charge, so the proportion of deaths at 2years was 5 of 55 (9%) in the ECMO-onlygroup versus 9 of 56 (16%) in the ECMO-with-cooling group (RR: 1.77; 99% CI:0.46–6.83). Cerebral palsy was di-agnosed in 3 of 48 infants (6%) in theECMO-only group versus 7 of 47 infants(15%) in the ECMO-with-cooling group(RR [99% CI]: 2.38 [0.47–13.0] and 1.79[0.39–8.22]. respectively).
The proportion of infants with no im-pairmentwas similar in bothgroups: 28of 44 infants (64%) in the ECMO-onlygroup versus 27 of 43 infants (63%) inthe ECMO-with-cooling group (RR: 0.99;99% CI: 0.65–1.50). The proportion ofinfants who survived without impair-ment was also similar in both groups:
28 of 49 infants (57%) in the ECMO-onlygroup versus 27 of 52 infants (52%) inthe ECMO-with-cooling group (RR: 0.91;99% CI: 0.57–1.45).
Overall, this pattern of small differ-ences favoring the ECMO-only groupwas consistent throughout the healthand neurologic findings at 2 years,apart from growth outcomes, whichfavored the ECMO-with-cooling group(Table 3). The use of aEEG did not ap-pear to be helpful in predicting out-come.
Parent Report of Abilities andBehavior at 2 Years
Parent-reported outcomes showeda different pattern, which tended tofavor ECMO with cooling, but the dif-ferences were small and none of thedifferences were significant (Table 4).
Subgroup Analyses
There was no evidence that the effect ofcooling was inconsistent across spe-
cific subgroups of infants; however, CIswere very wide due to the small num-bers in each subgroup.
Safety
Serious adverse event reports were notdifferent between the 2 groups: 11 werereported in the ECMO-only group (1 infantexperienced2events)and13 in theECMO-with-cooling group (1 infant experienced3 events) (Supplemental Table 5).
DISCUSSION
This trial indicates that therapeuticcooling during neonatal ECMO does notimprove neurodevelopmental outcomeat age 2 years. The trial was relativelysmall because it was based on realisticbut nonetheless somewhat speculativeestimates of the size of improvementthat might result from the use of cool-ing. However, there is no suggestion inthese results of a trend toward im-proved outcome that the trial was toosmall to demonstrate; if anything, theopposite is true.
Wasthe interventionadequate?Whereasweplanned in theprotocol that infants inthe coolingarmcouldreceivecooling foraminimumof48hours, the vastmajorityof those recruited completed72hoursofcooling. Seventy-two hours of coolinghas been shown to be effective in pro-viding neuroprotection in infants ex-posed to significant perinatal asphyxia.Froma technical perspective, cooling onECMOproved tobeeasy toachievebyuseof the circuit and was not associatedwith an increase in complications. Itcould be argued that longer cooling orcooling to a lower temperature mighthavebeenmoreeffective,but the trend inthe results presented here of a worseoutcomewith coolingmust at least raisea strong note of caution before consid-ering the use of such approaches.10
Was this thewrongstudypopulation?Byexcluding infants with diaphragmatichernia and those receiving ECMO forpostoperative cardiac support we
TABLE 2 Clinical Outcomes of Infants Before Discharge
All Randomly AssignedInfants (N = 111)
ECMO Only(n = 55)
ECMO WithCooling (n = 56)
Infants on ECMOa, n (%)Day 1 53 (96) 56 (100)Day 2 53 (96) 54 (96)Day 3 49 (89) 53 (95)
Reported sepsis, n (%)Before admission to ECMO unit 12 (22) 11 (20)During stay in ECMO unit 6 (11) 8 (14)After stay in ECMO unit 11 (20) 7 (13)
Cardiac arrhythmia requiring intervention, n (%) 3 (5) 3 (5)Pneumonia, n (%) 6 (11) 2 (4)Pulmonary air leak, n (%) 11 (20) 10 (18)Pulmonary hemorrhage, n (%) 2 (4) 2 (4)Necrotizing enterocolitis, n (%) 0 (0) 0 (0)Renal support while receiving ECMO, n (%) 8 (15) 8 (14)Jaundice requiring intervention, n (%) 4 (7) 3 (5)Head ultrasound performed, n (%) 54 (98) 56 (100)MRI performed, n (%) 17 (31) 19 (34)Duration of hospital stay before death or discharge,
median (IQR), d21 (16–33) 22.5 (17–30.5)
Duration of respiratory support, median (IQR), d 9 (7–15) 10 (7–14)Died before after hospital discharge, n (%) 4 (7) 8 (14)
IQR, interquartile range.a Two infants (ECMO only) recovered after trial entry and ECMO was not required. The duration of the intervention (cooling)was for a minimum of 48 hours to a maximum of 72 hours, depending on the duration of ECMO required. Two infants (ECMOwith cooling) died on day 2 of the ECMO run.
e1252 FIELD by guest on June 22, 2018www.aappublications.org/newsDownloaded from

TABLE 3 Health and Neurologic Outcomes of Infants at 2 Years
ECMO Only(n = 48)
ECMO WithCooling (n = 47)
RR (99% CI) Unless OtherwiseSpecified (Mean Difference)
Surviving infants assessed at 2 years (n = 95)Bayley-III Scales of Infant and Toddler DevelopmentCognitive composite scoreMean 6 SD (primary outcome) 90.6 6 13.1 88.0 6 16.2 22.6 (28.7 to 3.4)a
Unknown, n 0 2Language composite scoreMean 6 SD 96.3 6 17.2 95.5 6 22.3 20.8 (212.0 to 10.4)Unknown, n 4 4
Motor composite scoreMean 6 SD 96.2 6 14.4 89.9 6 16.0 26.3 (214.7 to 2.0)Unknown, n 2 1
Death before 2 years (whole sample), n (%) 5/55 (9) 9/56 (16) 1.77 (0.46 to 6.83)Neurologic optimality score (maximum of 78)Median score (IQR) 77 (75–77) 77 (75–78)Optimal ($74), n (%) 40 (83) 38 (81) 1 (referent)Suboptimal (,74), n (%) 8 (17) 9 (19) 1.15 (0.37 to 3.57)
Cerebral palsy, n (%) 3 (68) 7 (15) 2.38 (0.44 to 13.0)Spastic bilateral 0 3Hemiplegia 1 3Dyskinetic 1 0Nonclassifiable 1 1
Gross Motor Function Classification Scale, n (%)No cerebral palsy 45 (94) 40 (85) 1 (referent)Level 1–2 2 (4) 5 (8) 2.38 (0.44 to 13.0)Level 3–5 1 (2) 2 (4)
Seizures requiring anticonvulsant treatment, n (%) 0 (0) 5 (11)Usual vision (with glasses if worn), n (%)Normal or near normal 48 (100) 44 (94) 1 (referent)Impaired but useful 0 (0) 2 (4)Sees light/gross movement only 0 (0) 1 (2)No useful vision (blind) 0 (0) 0 (0)
Usual hearing (with aids if worn), n (%)Normal or near normal 48 (100) 43 (91) 1 (referent)Hearing loss corrected by aids 0 (0) 3 (6)Some hearing loss not corrected 0 (0) 1 (2)No useful hearing even with aids 0 (0) 0 (0)
Functioning within the normal range: Bayley cognitive,language, and motor scores $85; Gross Motor FunctionClassification Scale = 0; and normal vision (includingglasses) and normal hearing (without aids), n (%)
28 (64) 27 (63) 0.99 (0.65 to 1.50)
Unknown, n 4 4All surviving infants not lost to follow-up (n = 95)Growth SDSb
Weight SDS, mean 6 SD 20.12 6 1.39 0.33 6 1.19 0.45 (20.08 to 0.98)Unknown, n 1 0
Height SDS, mean 6 SD 20.42 6 1.29 0.07 6 1.21 0.48 (20.03 to 0.99)Unknown, n 1 0
Head circumference SDS, mean 6 SD 21.23 6 1.34 21.11 6 1.92 0.11 (20.57 to 0.78)Unknown, n 0 0
Feeding difficulties, n (%) 4 (8) 4 (9) 1.02 (0.18 to 5.84)Head function, n (%)Normal head control 48 (100) 46 (98) 1 (referent)Abnormal head control 0 (0) 0 (0)Poor head control 0 (0) 1 (2)No head control 0 (0) 0 (0)
Trunk function, n (%)No apparent problem 46 (96) 43 (91) 1 (referent)Sits unsupported, less secure 2 (4) 2 (4) 2.04 (0.23 to 17.8)Cannot sit unless supported 0 (0) 2 (4)Difficult to place in sitting position 0 (0) 0 (0)
Lower limb function, n (%)
ARTICLE
PEDIATRICS Volume 132, Number 5, November 2013 e1253 by guest on June 22, 2018www.aappublications.org/newsDownloaded from

recruited infants to the trial who formthe core group of most ECMO programsaround the world. In addition, infants ofthis typewere shownpreviously to be atrisk of poor neurodevelopmental out-come, and indeed those previous find-ings have been mirrored in this study,with the mean cognitive score for bothgroups being #90.
In developing this study we felt thatthere was strong empirical evidencethat cooling infants who received ECMOmight result in improved outcomes. Thefact that such improvements did notresult suggests thatat least someofourjudgments in this regard were mis-placed. There was no suggestion in thedata that an increase in complicationsrelated to cooling masked an un-derlying positive effect, such as thatseen in trials of cooling in infants whohad suffered intrapartum asphyxia. Itwas, of course, in animal models ofintrapartum asphyxia that the un-derpinning research regarding theneuroprotective effects of cooling innewborns were first assessed andestablished10. It may be that the natureof the insult in infants who receive
ECMO (ie, it takes place over a relativelyprolonged period) is such that damagecannot be prevented by the the use ofcooling for a period during the insult,albeit at what is likely to be the time ofmaximum physiologic disruption.10
Existing data certainly suggest that it isthe underlying condition and or theassociated physiologic changes ratherthan the use of ECMO that results inan increased risk of long-term neuro-developmental impairment.
In terms of the wider implication of thisstudy, it seems clear that the use ofcooling for neuroprotection duringECMO (it is sometimes used to reduceoxygen consumption) is to be avoided.However, the results of this study alsohighlight the potential dangers of ex-trapolating existing research findingsfrom 1 group to another without ap-propriate testing. For example, thecurrent trend to use mild cooling totreat intrapartum asphyxia in infantswhodonotmeet the entry criteria of theoriginal trials may well be unwise be-cause the same response cannot beassumed, aswe found here. Conversely,a potential role for mild cooling for
a period after neonatal cardiac surgeryas a means of improving long-termoutcomes in these infants remains un-tested, and theresultsof thisstudyareofno direct relevance.
ACKNOWLEDGMENTSThe NEST research team acknowl-edges the support of the National In-stitute for Health Research, throughthe Medicines for Children ResearchNetwork.
The NEST study group collaborators/investigators: Dr David Field, DenisAzzopardi, Dr Peter Brocklehurst, DrFrances Cowan, Dr David Edwards,and Mr Richard Firmin. Data Moni-toring Committee members: DianaElbourne (Chair), Dr Richard Cooke,Dr Linda Franck, Dr Henry Halliday, DrDuncan Macrae, and Dr Neil Marlow.Trial Steering Committee members:Dr Andrew Wilkinson (Chair), Ms Pau-line Fellows, Dr Mary Montgomery, MsFarrah Pradhan, Dr Claire Snowdon,and Dr Marianne Thoresen. NationalPerinatal Epidemiology Unit Coordinat-ing Centre: Ms Denise Jennings, Mr EdJuszczak, Ms Ursula Bowler, Ms Sarah
TABLE 3 Continued
ECMO Only(n = 48)
ECMO WithCooling (n = 47)
RR (99% CI) Unless OtherwiseSpecified (Mean Difference)
Walks fluently 45 (94) 41 (87) 1 (referent)Gait functional but nonfluent 1 (2) 1 (2) 2.04 (0.36 to 11.7)Reduced mobility restricts lifestyle 0 (0) 1 (2)No independent walking 2 (4) 4 (9)
Upper limb function, n (%)No apparent problem 45 (94) 42 (89) 1 (referent)Some difficulty but feeds self 2 (4) 3 (6) 1.70 (0.28 to 10.4)Unable to feed self 1 (2) 2 (4)
Contractures present 1 (2) 4 (9) 4.09 (0.24 to 69.3)Usual communication, n (%)Uses speech 39 (81) 36 (77) 1 (referent)Speech plus other formal method 4 (8) 2 (4) 1.25 (0.45 to 3.50)Formal systematized method only 2 (4) 3 (6)No communication 3 (6) 6 (13)
Overall disability from any cause, n (%)No disability 38 (79) 32 (68) 1 (referent)Impairment without disability 7 (15) 10 (21) 1.53 (0.62 to 3.80)Mild disability 0 (0) 1 (2)Moderate disability 2 (4) 1 (2)Severe disability 1 (2) 3 (6)
SDS, SD score.a 95% CI for primary outcome.b Calculated by using the British 1990 growth reference (revised September 1996)21.
e1254 FIELD by guest on June 22, 2018www.aappublications.org/newsDownloaded from

Ayers, Mr Andy King, Dr MaggieRedshaw, and Ms Louise Linsell.Recruiting centers (n5 number re-cruited per centre): Glenfield Hospital(59) (Mr Giles Peek, Ms Anne-Marie Hill,Ms Gail Faulkner, Dr Hitesh Pandya, DrMarie Horan, Dr Chris Harvey); GreatOrmond Street Hospital (21) (DrAparna Hoskote, Dr Allan Goldman,Ms Liz Smith, Ms Maura O’Callaghan,Ms Helen Boardman); Freeman Hospi-
tal (10) (Dr Jane Cassidy, Dr Jon Smith,Ms Caroline McPherson, Dr AlanFenton, Dr Janet Berrington); and theRoyal Hospital for Sick Children Glas-gow (21) (Dr Judith Simpson, Mr CarlDavis, Ms Morag Liddell, Ms GillianWylie). Follow-up was carried out byDr Andrew T.M. Chew and supervisedby Dr Frances Cowan. The cranial ultra-sound and MRI interpreter was DrFrances Cowan. The Cerebral Function
Monitoring interpreter was Dr DenisAzzopardi. The writing committee con-
sisted of Dr David Field, Mr Ed Juszczak,
Ms Louise Linsell, Dr Denis Azzopardi,
Dr Frances Cowan, Dr Neil Marlow, and
Dr David Edwards.
We especially thank the parents whoagreed to let their children take part
in the NEST study and to the funders
who made it possible.
REFERENCES
1. UK Collaborative ECMO Trial Group. UK col-laborative randomised trial of neonatal ex-tracorporeal membrane oxygenation. Lancet.1996;348(9020):75–82
2. Mugford M, Elbourne D, Field D. Extracorpo-real membrane oxygenation for severe re-spiratory failure in newborn infants. CochraneDatabase Syst Rev. 2008;16(3):CD001340
3. Bennett CC, Johnson A, Field DJ, ElbourneD; UK Collaborative ECMO Trial Group. UKcollaborative randomised trial of neona-tal extracorporeal membrane oxygenation:
TABLE 4 Parent Report of Abilities and Behavior of Infant at 2 Years
Surviving Infants Assessed at 2 Years (n = 95)
ECMO Only (n = 48) ECMO With Cooling (n = 47) Mean Difference (99% CI)
PARCA-Ra
Parent-report composite scoreMean 6 SD score 84.3 6 35.8 87.4 6 44.1 3.1 (214.3 to 20.4)Unknown, n 5 5
Nonverbal Cognition ScaleMean 6 SD score 25.4 6 4.6 24.2 6 7.7 21.2 (23.9 to 1.5)Unknown, n 5 3
Linguistic Skills ScaleMean 6 SD score 58.9 6 32.7 62.2 6 39.7 3.3 (212.3 to 18.9)Unknown, n 5 4
ICQb
Fussy/difficult/demandingMean 6 SD score 53.7 6 11.7 51.7 6 13.5 21.9 (27.4 to 3.5)Unknown, n 6 3
UnadaptableMean 6 SD score 14.2 6 4.9 15.2 6 4.9 0.9 (21.2 to 3.1)Unknown, n 7 4
PersistentMean 6 SD score 26.0 6 4.8 25.7 6 5.2 20.4 (22.5 to 1.8)Unknown, n 5 4
UnsociableMean 6 SD score 11.3 6 3.6 11.3 6 3.9 20.05 (21.7 to 1.6)Unknown, n 5 4
BITSEAc
Problem subtotalMean 6 SD score 10.6 6 7.1 11.9 6 8.6 1.3 (22.0 to 4.6)Possible problem (.25th percentile), n (%) 13 (30) 11 (24)Unknown, n 5 2
Competence subtotalMean 6 SD score 16.8 6 3.0 161 6 3.9Possible delay (,15th percentile), n (%) 10 (23) 16 (36) 20.7 (22.1 to 0.8)Unknown, n 5 2
BITSEA, Brief Infant-Toddler Social and Emotional Assessment; ICQ, Infant Characteristics Questionnaire; PARCA-R, Parent Report of Children’s Abilities for Very Premature Infants.a The PARCA-R composite score (range: 0–158) is the sum of the Nonverbal Cognition Scale (range: 0–34) and the Linguistic Skills Scale (range: 0–124). A higher score indicates betterperformance.b The 4 domains of the ICQ have the following range of values: fussy/difficult/demanding (range: 16–112), unadaptable (range: 5–35); persistent (range: 6–42), and unsociable (range: 5–35). Ahigher score indicates less desirable characteristics.c A higher score for the BITSEA Problem subtotal (range: 0–62) indicates more problems. A higher score for the BITSEA Competence subtotal (range: 0–24) indicates greater competence.
ARTICLE
PEDIATRICS Volume 132, Number 5, November 2013 e1255 by guest on June 22, 2018www.aappublications.org/newsDownloaded from

follow-up to age 4 years. Lancet. 2001;357(9262):1094–1096
4. McNally H, Bennett CC, Elbourne D, Field DJ;UK Collaborative ECMO Trial Group. UnitedKingdom collaborative randomized trial ofneonatal extracorporeal membrane oxygen-ation: follow-up to age 7 years. Pediatrics.2006;117(5). Available at: www.pediatrics.org/cgi/content/full/117/5/e845
5. Gluckman PD, Wyatt JS, Azzopardi D, et al.Selective head cooling with mild systemichypothermia after neonatal encephalopa-thy: multicentre randomised trial. Lancet.2005;365(9460):663–670
6. Shankaran S, Laptook AR, Ehrenkranz RA,et al; National Institute of Child Health andHuman Development Neonatal ResearchNetwork. Whole-body hypothermia forneonates with hypoxic-ischemic encepha-lopathy. N Engl J Med. 2005;353(15):1574–1584
7. Ichiba S, Killer HM, Firmin RK, Kotecha S,Edwards AD, Field D. Pilot investigation ofhypothermia in neonates receiving extra-corporeal membrane oxygenation. Arch DisChild Fetal Neonatal Ed. 2003;88(2):F128–F133
8. Horan M, Ichiba S, Firmin RK, et al. A pilotinvestigation of mild hypothermia in neo-nates receiving extracorporeal membraneoxygenation (ECMO). J Pediatr. 2004;144(3):301–308
9. Allmark P, Snowdon C, Elbourne D, MasonS. Challenges for parents and cliniciansdiscussing neuroprotective treatments. In:Edwards AD, Azzopardi DV, Gunn AJ, eds.Neonatal Neural Rescue: A Clinical Guide.Cambridge, United Kingdom: CambridgeUniversity Press. 2013;(Chapter 6):65–72
10. Field DJ, Firmin RK, Azzopardi DV, Cowan F,Juszczak E, Brocklehurst P; NEST StudyGroup. Neonatal ECMO Study of Temper-ature (NEST)—a randomised controlledtrial. BMC Pediatr. 2010;10(24):24
11. Bayley N. Manual for the Bayley Scales ofInfant and Toddler Development. 3rd ed.San Antonio, TX: Harcourt Assessment; 2006
12. Haataja L, Mercuri E, Regev R, et al. Opti-mality score for the neurologic examina-tion of the infant at 12 and 18 months ofage. J Pediatr. 1999;135(2 pt 1):153–161
13. Haataja L, Mercuri E, Guzzetta A, et al.Neurologic examination in infants withhypoxic-ischemic encephalopathy at age 9to 14 months: use of optimality scores andcorrelation with magnetic resonance im-aging findings. J Pediatr. 2001;138(3):332–337
14. Palisano RJ, Cameron D, Rosenbaum PL,Walter SD, Russell D. Stability of the grossmotor function classification system. DevMed Child Neurol. 2006;48(6):424–428
15. Saudino K, Dale P, Oliver B, et al. The validityof a parent-based assessment of the cog-
nitive abilities of 2-year olds. Br J DevPsychol. 1998;16:349–362. http://onlinelibrary.wiley.com/doi/10.1111/j.2044-835X.1998.tb00757.x/abstract.
16. Johnson S, Marlow N, Wolke D, et al. Vali-dation of a parent report measure of cog-nitive development in very preterm infants.Dev Med Child Neurol. 2004;46(6):389–397
17. Johnson S, Wolke D, Marlow N; PretermInfant Parenting Study Group. Develop-mental assessment of preterm infants at2 years: validity of parent reports. Dev MedChild Neurol. 2008;50(1):58–62
18. Lee CL, Bates JE. Mother-child interaction atage two years and perceived difficult tem-perament. Child Dev. 1985;56(5):1314–1325
19. Briggs-Gowan MJ, Carter AS, Irwin JR,Wachtel K, Cicchetti DV. The Brief Infant-Toddler Social and Emotional Assessment:screening for social-emotional problemsand delays in competence. J Pediatr Psychol.2004;29(2):143–155
20. Mercuri E, Ricci D, Cowan FM, et al. Headgrowth in infants with hypoxic-ischemicencephalopathy: correlation with neonatalmagnetic resonance imaging. Pediatrics.2000;106(2 pt 1):235–243
21. Cole TJ, Freeman JV, Preece MA. British1990 growth reference centiles for weight,height, body mass index and head cir-cumference fitted by maximum penalizedlikelihood. Stat Med. 1998;17(4):407–429
e1256 FIELD by guest on June 22, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1754 originally published online October 21, 2013; 2013;132;e1247Pediatrics
David FieldTrial
Neonatal ECMO Study of Temperature (NEST): A Randomized Controlled
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/132/5/e1247including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/132/5/e1247#BIBLThis article cites 19 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neurology_subNeurologyhttp://www.aappublications.org/cgi/collection/neonatology_subNeonatologysubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 22, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1754 originally published online October 21, 2013; 2013;132;e1247Pediatrics
David FieldTrial
Neonatal ECMO Study of Temperature (NEST): A Randomized Controlled
http://pediatrics.aappublications.org/content/132/5/e1247located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2013/10/16/peds.2013-1754.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 22, 2018www.aappublications.org/newsDownloaded from