NCRI Renal Cancer Clinical Studies...
10
NCRI Renal Cancer Clinical Studies Group Annual Report 2012/2013
Transcript of NCRI Renal Cancer Clinical Studies...

NCRI Renal Cancer Clinical Studies Group
Annual Report 2012/2013

Data
Section # Indicator Lowest Highest
Disease 1 Incidence of disease (UK) 8139 2,232 48,988
2 Mortality of disease UK) 3583 71 35,042
Members 3 Number of Scientific Members on CSG 14 14 264 Number of Subgroups 1 0 75 Number of Taskgroups 0 0 2
6 Number of Consumers involved in CSG, Subgroup and Taskgroup activities 3 1 4
Portfolio 7 Total number of academic/industry sponsored portfolio studies opening in year 7/2 1/2 24/138 Number of academic/industry sponsored portfolio studies open 19/6 1/1 93/299 Total number of portfolio studies(academic and industry sponsored) closing in year 3 1 21
10 Number of studies conducted internationally (outside UK) open 11 1 3911 Number of Industry Alliance Studies open in year 1 1 3
12 Participation in International Rare Cancer Initiative (IRCI) No
Portfolio Delivery 13 Total number of participants recruited (All CSG portfolio studies) 1267 269 3219714 Total number of cancer patients recruited (All CSG portfolio studies) 1025 64 1374815 Proportion of cancer patients recruited by disease 12.6 3.1 72.216 Proportion of cancer patients recruited to interventional studies (where applicable - all CSG portfolio studies) 8.6 1.1 23.517 Number of non cancer participants recruited to studies (All CSG portfolio studies) 242 0 1844918 Total number of participants recruited to industry sponsored studies (All CSG portfolio studies) 97 2 65819 Proportion of CSG industry sponsored studies closing in year and delivered to time & target 67% 0, 1 100, 320 Proportion of other CSG academic studies closing in years and delivered to time & target 17, 6 100, 1
21 Number of Local Research Networks active in delivering portfolio 37 11 40
Output 22 Number of peer review publications directly associated with CSG portfolio studies 5 0 52
23 Awareness raising/educational events Yes
Progress Review 24 Date of last Progress Review Jan-10
25 Date of next Progress Review Jun-13
NCRI Renal Cancer Clinical Studies Group
National comparison

1
NCRI Renal CSG Annual Report 2012/13
1. Executive Summary The incidence of renal cancer is increasing with 9639 cases and 4062 deaths in the UK in 2010. The development of new drugs for the treatment of renal cancer in the last 5 years and the use of new minimally invasive technologies to treat small tumours has changed the therapeutic landscape and the Renal CSG has responded to these developments. The main challenge for the Group in 2012/2013 has been poor recruitment into studies investigating cytoreductive nephrectomy in patients presenting with metastatic renal cancer (E-PREDICT, CARMENA and SURTIME).
2. Top three achievements in the year The three main achievements for the Group this year are:
Yearly trend of increasing trial recruitment since 2007 maintained with good recruitment into both industry and academic studies e.g. PANTHER
Completion of recruitment into adjuvant SORCE trial early 2013
Gerlinger et al Intratumour Heterogeneity NEJM paper from E-PREDICT trial 2nd most cited scientific paper published in 2012 (only the discovery of the Higgs Boson was more highly cited)
3. Structure of the Group Mr Michael Aitchison stepped down as Chair of the CSG in 2012; the Group would like to thank him for his leadership and vision over the last 5 years. Dr James Larkin took over Chairmanship of the group in July 2012. Professors Tim Eisen (Cambridge, Medical Oncology) and Robert Hawkins (Manchester, Medical Oncology) and Dr Emilio Porfiri (Birmingham, Medical Oncology) rotated off the group in 2012 and were replaced by Dr Hilary Glen (Glasgow, Medical Oncology) and Mr Grenville Oades (Glasgow, Urology). Currently the group has 3 Consumer Representatives, 2 Radiologists, 5 Surgeons, 6 Medical Oncologists and 1 Scientist. The CSG has a surgical subgroup Chaired by Mr Naeem Soomro.
4. Achievements and challenges of the subgroups The key achievements of the subgroups are:
Recruitment started for (CONSERVE ) trial comparing surgery with ablation for small renal masses
Recruitment ongoing for (CARMENA / SURTIME) for metastatic renal cancer
Funding approved for (SURAB) from HTA comparing ablation with active surveillance in small renal cancers
Progress being made for application for surveillance in patients with small renal cancer who are not fit for treatment.
2
The key challenges for the subgroups are:
Time spent on writing up applications and decision takes usually up to two years
Ongoing difficulties with time taken for setting up individual recruiting sites
Slow recruitment for surgical trials
Urology and imaging services may not be equally developed in certain centres which restricts the number of centres able to participate and also the recruitment rates.
5. Task groups/Working parties The CSG has no working parties or task groups.
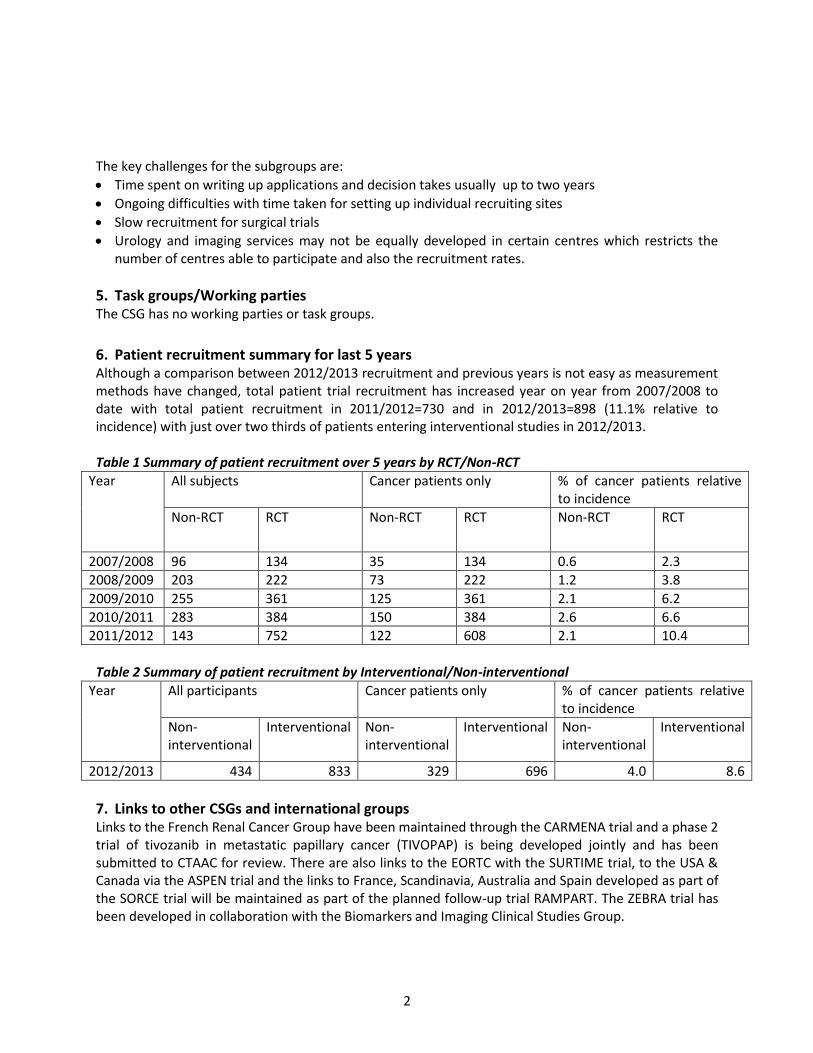
6. Patient recruitment summary for last 5 years Although a comparison between 2012/2013 recruitment and previous years is not easy as measurement methods have changed, total patient trial recruitment has increased year on year from 2007/2008 to date with total patient recruitment in 2011/2012=730 and in 2012/2013=898 (11.1% relative to incidence) with just over two thirds of patients entering interventional studies in 2012/2013.
Table 1 Summary of patient recruitment over 5 years by RCT/Non-RCT
Year All subjects Cancer patients only % of cancer patients relative to incidence
Non-RCT RCT Non-RCT RCT Non-RCT RCT
2007/2008 96 134 35 134 0.6 2.3
2008/2009 203 222 73 222 1.2 3.8
2009/2010 255 361 125 361 2.1 6.2
2010/2011 283 384 150 384 2.6 6.6
2011/2012 143 752 122 608 2.1 10.4
Table 2 Summary of patient recruitment by Interventional/Non-interventional
Year All participants Cancer patients only % of cancer patients relative to incidence
Non-interventional
Interventional Non-interventional
Interventional Non-interventional
Interventional
2012/2013 434 833 329 696 4.0 8.6
7. Links to other CSGs and international groups Links to the French Renal Cancer Group have been maintained through the CARMENA trial and a phase 2 trial of tivozanib in metastatic papillary cancer (TIVOPAP) is being developed jointly and has been submitted to CTAAC for review. There are also links to the EORTC with the SURTIME trial, to the USA & Canada via the ASPEN trial and the links to France, Scandinavia, Australia and Spain developed as part of the SORCE trial will be maintained as part of the planned follow-up trial RAMPART. The ZEBRA trial has been developed in collaboration with the Biomarkers and Imaging Clinical Studies Group.

3
8. Funding applications in last year The below table shows funding applications related to the Group made in the last year.
Table 3 Funding applications for the year
Title CI Funding body
A phase II study of anti-PD1 (nivolumab) therapy as pre-operative therapy in metastatic renal cell cancer
Dr James Larkin & Professor Charles Swanton
CTAAC
The above feasibility endorsement application was invited for resubmission.
9. Industry sponsored trials portfolio Study title Open/Closed % Target % Time Elapsed
NCRN325 - E7080 +/- Everolimus in mRCC following one prior VEGF-targeted treatment
Open 127% 87%
NCRN342 PRINCIPAL: Pazopanib Observational Study
Open 62% 51%
NCRN358: BMS-936558 vs. Everolimus in metastatic RCC after prior anti-angiogenic therapy
Open 28% 13%
NCRN211 - IMPRINT Closed 90% *see below
100%
NCRN281 GOLD - TKI258 versus sorafenib in patients with mRCC after failure of anti-angiogenic
Closed 100% 100%
NCRN302 ROVER: DC-0980 versus everolimus in mRCC progressed on/following VEGF-targeted therapy
Closed 175% 100%
*High biomarker screen failure rate. Only 2 sites did not screen a patient. Feasibility was based on an expected HLA biomarker rate of 50%. The HLA marker rate was only 24% from the screened patients in the UK so it was challenging to meet the planned target. 90% recruitment to target was considered a positive result in the circumstances. Recruited 17/18 patients at NIHR Network supported sites in England.
10. Collaborative partnership studies with industry A collaboration with Pfizer on the A-PREDICT trial which opened in 2012 has been developed. The Astra Zeneca collaboration continues with the ZEBRA trial which opened to recruitment in 2013. A collaboration with Astellas has been developed on the TIVOPAP trial. Discussions with a number of industry partners about the follow-up trial to SORCE, RAMPART, are at an advanced stage.
11. Progress towards achieving 3 year strategy The following questions have directed the Renal CSG in the development of studies; trials addressing these questions are inserted in parentheses:
4
For tumours confined to the kidney what is the most effective surgical/minimally invasive treatment? (CONSERVE)
Following nephrectomy, in patients identified at risk of developing metastases is there a role for adjuvant therapy? (SORCE/RAMPART)
Is there a role for cytoreductive nephrectomy+/-neo-adjuvant therapy in patients presenting with metastatic disease? (CARMENA/SURTIME)
Can predictive biomarkers be found to tailor individual therapy? (E-PREDICT/A-PREDICT/Biomarkers study/EUROTARGET)
Can we gain an understanding of mechanisms of resistance to systemic therapy? (E-PREDICT/A-PREDICT)
What treatments are effective in the non-clear cell type? (TIVOPAP)
Can more effective systemic treatments be developed? (ZEBRA)
Can targeted systemic therapies be scheduled differently without detriment to efficacy but with improved quality of life for patients? (STAR)
The Progress Review Report 2010 identified the need to focus more on translational research and this has been addressed with the Renal Biomarker Study, PREDICT and EUROTARGET projects. Increased consumer involvement was also identified as a potential area for expansion and the involvement of the Consumer Liaison Group members in trial design and trial steering committees has addressed this.
12. Impact of clinical trials on routine UK clinical practice The Renal CSG awaits mature trial results. The adjuvant SORCE trial which recently closed to accrual is potentially practice-changing but will not report until 2015 at the earliest. The STAR trial which opened to recruitment in 2012 is also potentially practice-changing and recruitment is currently satisfactory.
13. Consumer involvement The consumer liaison members have made major contributions to discussions at CSG meetings and to the work of the Group in terms of trial design and review and contributions to submissions to NICE. They have also provided valuable links to UK Kidney Cancer Charities (KCUK and James Whale Fund) and to national and international patient advocacy groups.
14. Open meetings / annual trials days A Urological Trial Meeting with the other 3 urological CSGs is being planned for early 2014 at the Royal College of Physicians.
15. Priorities and challenges for the forthcoming year The main priority is to manage the portfolio, particularly with respect to poorly recruiting trials. At the CSG meeting in May 2013 it was decided that continued recruitment into the EORTC SURTIME study in the UK could not be supported by the Group because of poor accrual. Recruitment into E-PREDICT and CARMEMA will be reviewed carefully in 2013/2014. Other priorities are to gain approvals and open the RAMPART trial as quickly as possible and to ensure high recruitment into STAR.
16. Concluding remarks

5
The Renal CSG has been successful in expanding the trial portfolio and increasing recruitment with a balance of academically-led and industry adopted trials with a strong translational component. The Group needs to continue to build on these strengths and manage the trial portfolio carefully to avoid poor recruitment.
17. Appendices 1. Membership of main CSG and subgroups 2. Portfolio Maps 3. Publications in previous calendar year 4. Major international presentations in previous year
Dr James Larkin (Renal CSG Chair)

Appendix 1
CSG and Subgroup membership
CSG Membership
Member Location
Mr Michael Aitchison Glasgow
Professor Roz Banks Leeds
Dr Janet Brown Leeds
Dr Hilary Glen Glasgow
Professor Vicky Goh London
Dr Pat Hanlon Birmingham
Dr Irfan Kayani London
Dr James Larkin London
Dr Paul Nathan Middlesex
Mr Tim O'Brien London
Mr Grenville Oades Glasgow
Dr Thomas Powles London
Mr Naeem Soomro Newcastle
Mr Mark Sullivan Oxford
Professor John Wagstaff Swansea
Mrs Rose Woodward Truro
Mrs Julia Wright Beaconsfield
Subgroup Membership
Surgical Subgroup
Mr Naeem Soomro (Chair)
Mr Grenville Oades
Mr Michael Aitchison
Mr Tim O’Brien
Mr Mark Sullivan

No
n-
Inte
rven
tio
nal
3rd
lin
e
Met
asta
tic
2n
d li
ne
Met
asta
tic
1st
lin
e
Met
asta
tic
Ad
juva
nt
Surg
ery
Neo
adju
van
tTu
mo
ur
Typ
e RENAL CSG PORTFOLIO MAP
Clear cell Non-clear cell
RENAL CANCERYELLOW=OPEN/RECRUITINGPURPLE=IN SET-UP/FUNDED
E-P
RED
ICT
HYP
AZ
PaZ
02
EOR
TC 3
00
73
-
SUR
TIM
E
CA
RM
ENA
S-P
RED
ICT
A-P
RED
ICT
DIR
ECTS
STA
R
ASP
EN
HYP
AZ
SOR
CE/
TRA
NSO
RC
E
SOR
CE/
TRA
NSO
RC
E
Eval
uat
ion
of
bio
mar
kers
fo
r p
rogn
osi
s o
f R
CC
Eval
uat
ion
of
bio
mar
kers
fo
r p
rogn
osi
s o
f R
CC
Ver
sio
n: F
ebru
ary
20
13
Dev
elo
ped
by
NC
RI C
SGs
& N
CR
N
EOR
TC 3
00
73
-
SUR
TIM
E
CA
RM
ENA
E-P
RED
ICT
S-P
RED
ICT
An
gio
gen
esis
&
P
rolif
erat
ion
An
gio
gen
esis
&
P
rolif
erat
ion
CO
NSE
RV
E
CO
NSE
RV
E
ZEB
RA
NC
RN
32
5
Gen
etic
s o
f p
apill
ary
kid
ney
can
cer
NC
RN
35
8
NC
RN
34
2/
PR
INC
IPA
L
NC
RN
34
2/
PR
INC
IPA
L
SCO
TRC
C
SCO
TRC
C
Adrenal
AD
IUV
O
NC
RN
39
6
NC
RN
39
6
NC
RN
48
4/
TAU
RU
S
NC
RN
48
4/
TAU
RU
S
Euro
TAR
GET
Euro
TAR
GET
NC
RN
48
8
Ph
oto
dyn
amic
th
erap
y fo
r T1
a tu
mo
ur
Ph
oto
dyn
amic
th
erap
y fo
r T1
a tu
mo
ur
NC
RN
54
4

Appendix 3 Publications arising from the Group’s portfolio
E-PREDICT Gerlinger, M, Rowan, AJ, Horswell, S, Larkin, J, Endesfelder, D, Gronroos, E, Martinez, P, Matthews, N, Stewart, A, Tarpey, P, Varela, I, Phillimore, B, Begum, S, McDonald, NQ, Butler, A, Jones, D, Raine, K, Latimer, C, Santos, CR, Nohadani, M, Eklund, AC, Spencer-Dene, B, Clark, G, Pickering, L, Stamp, G, Gore, M, Szallasi, Z, Downward, J, Futreal, PA and Swanton, C, 2012. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. New England Journal of Medicine, Mar 8;366(10):883-92. PMID: 22397650. PANTHER Powles T, Sarwar N, Jones R, Wilson P, Boleti E, Protheroe A, Crabb SJ, Shamash J, Stockdale A,
Rashid S, Nathan P, Chowdury S. An indirect comparison of the toxicity of sunitinib and pazopanib in
metastatic clear cell renal cancer. Eur J Cancer. 2012 ;48(17):3171-6. SUMR/PANTHER
Industry trials
Grünwald V, Karakiewicz PI, Bavbek SE, Miller K, Machiels JP, Lee SH, Larkin J, Bono P, Rha SY,
Castellano D, Blank CU, Knox JJ, Hawkins R, Anak O, Rosamilia M, Booth J, Pirotta N, Bodrogi I; REACT
Study Group. An international expanded-access programme of everolimus: addressing safety and
efficacy in patients with metastatic renal cell carcinoma who progress after initial vascular
endothelial growth factor receptor-tyrosine kinase inhibitor therapy. Eur J Cancer. 2012;48(3):324-32
Eisen T, Joensuu H, Nathan PD, Harper PG, Wojtukiewicz MZ, Nicholson S, Bahl A, Tomczak P,
Pyrhonen S, Fife K, Bono P, Boxall J, Wagner A, Jeffers M, Lin T, Quinn DI. Regorafenib for patients
with previously untreated metastatic or unresectable renal-cell carcinoma: a single-group phase 2
trial. Lancet Oncol. 2012 Oct;13(10):1055-62.
Mulders, P, Hawkins, R, Nathan, P, de Jong, I, Osanto, S, Porfiri, E, Protheroe, A, van Herpen, CM,
Mookerjee, B, Pike, L, Jurgensmeier, JM and Gore, ME, 2012. Cediranib monotherapy in patients
with advanced renal cell carcinoma: Results of a randomized phase II study. European Journal of
Cancer, Mar; 48 (4), 527-537.