NCHA Update 8:2016 - AAHAM · Key 2016 Legislative Priorities ... 12. PLE Regions (Draft as of...
25
NCHA Update Ronnie Cook Financial Services Consultant
Transcript of NCHA Update 8:2016 - AAHAM · Key 2016 Legislative Priorities ... 12. PLE Regions (Draft as of...

NCHA Update
Ronnie CookFinancial Services Consultant

Agenda
• Key 2016 Legislative Priorities• Medicaid Reform• Payor Update• Regulatory Update

Key 2016 Legislative Priorities
• Certificate of Need (CON) - Preserved• Taxes – Protected• Graduate Medical Education - Restored• Behavioral Health – Funded• Medicaid Reform - Submitted

Certificate of Need
• Certificate of Need– Determines placement of facilities and
services based on population shifts– Around since the 1970s.– Multiple efforts to repeal or carve out.– Eliminating CON would cost NC Hospitals an
estimated $533 million per year.

Taxes
• North Carolina Non Profit health systems receive a refund on sales taxes. – Effort every year to reduce the amount. – Current cap of $45 million.
• Municipalities would like an option to tax the property of non-profits

Graduate Medical Education
• 2015 required elimination of Medicaid GME– Restored in 2016 as long as funds are
available.– Essential for Medicaid transformation

Behavioral Health
• Issues:– Involuntary commitment– Payment models do not incentivize
community based care– EMTALA– No where for patients to go

Behavioral Health
• 2016 budget– Governor’s taskforce– Funded construction of community based
crisis centers– Set aside funds for rural behavioral health
beds that are either new construction or conversion from existing acute care beds.

Medicaid Reform - DHHS Timetable
9

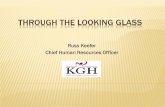
Hospital Supplemental Funding
10
BaseRateSupplementalFunds
60% 40%
Hospitalsrelyonsupplemental funding forasmuchas40%oftheirMedicaidpayments.TheStatealsoreliesonsupplemental funds fortheirbudget.

The Future of Supplemental Payments
11
• CMSmustapprovethe1115waiver,includinghowsupplementalpaymentsarehandled
• CMShasrecentlypushedsomeotherstatesseeking1115managedcarewaiverstowardsotherformsofpayments
• CMSissuedaruleinlateApril,2016thatappearstophaseoutsupplementalpaymentsovera10yearperiod,beginningin2017

Other Aspects of Reform
• Commercial managed care companies will compete with regional provider-led entities to provide services
• The vast majority of Medicaid services will be under capitation (eventually) • LMEs and Dual Eligibles are carved out initially
• Plans will be regulated by DOI and DHHS– DOI will regulate financial solvency– DHHS will regulate network adequacy and general
insurance-related issues
12

PLE Regions (Draft as of March 1, 2016)
13

Moving Parts/Challenges
• CMS negotiations with the State will define the waiver– CMS views, rules on supplemental funding are crucial– Impact on provider rates still unknown with so many
variables in play– CMS may raise issue of Medicaid expansion
• Carve-outs of services:– Dual eligibles are exempted in first round of waiver– LMEs (mental health) will continue under their own
capitated system for 4 years after capitation begins; creates challenges for hospitals and other providers in aligning whole patient care
14

Moving Parts/Challenges
• Managed Care companies may seek legislation or regulatory changes adverse to hospitals
– For example, preventing a hospital from being in both a statewide provider-led health plan and forming its own regional PLE plan
• 2016 Elections: changes in governance (federal or state) could impact waiver negotiations, rules, RFPs, contracts, etc.
15

Payor Update
• Medicare Provider Workgroup• Medicaid Technical Advisory Workgroup• VA Workgroup• Managed Care Committee• Network Adequacy Workgroup (NCDOI)

Payor Update
• CY 2017 ACA Market Update• Medicaid Payment of Inpatient
Rehabilitation Services• Reference Based Pricing Products

State Health Plan – CY 2017 Medicare Advantage Update
• For CY 2017, moving to one Medicare Advantage carrier, UnitedHealthcare (UHC) and providing three plan options for Medicare retirees
• Members enrolled in Humana Medicare Advantage Plan for 2016 will have to take action during Open Enrollment
• Plan staff recommended assigning all Humana members to the UHC Base Plan for Open Enrollment. Members who take no action will remain in the UHC Base Plan for 2017.

Regulatory Update – NOTICE Act Delayed
• Notice of Observation Treatment and Implication for Care Eligibility Act requires hospital and CAHs to provide:– Written and oral notification to beneficiaries receiving
observation for more than 24 hours– Medicare Outpatient Observation Notice (Moon) to
beneficiary• Notice is required to be provided no later than
36 hours after observation is initiated, or sooner if the individual is transferred, discharges, or admitted as inpatient

Regulatory Update – NOTICE Act Delayed
• CMS significantly revised proposed MOON– Removed physician name, date and time
observation was initiated, hospital name, QIO contact information
– Added field for specific information as to why patient was in observation vs. inpatient
– Provided required and recommended items for “Addition Information” section

Regulatory Update – NOTICE Act Delayed
• NOTICE Act requirements were originally set to take effect August 6, 2016
• MOON subject to Paperwork Reduction Act and must undergo 30-day review and comment period
• After MOON has been finalized, providers have 90 calendar days to implement – Expected effective date January 1, 2017

Regulatory Update – Site Neutral
• Certain off-campus PBDs would be permitted to bill for excepted services under OPPS– Excepted items and services are:
• All items and services furnished in a dedicated emergency department
• Items and services that were furnished and billed prior to November 2, 2015
• Item and services furnished in a hospital department within 250 yards of hospital or remote location of the hospital
• No exception for under construction

Regulatory Update – Site Neutral
• Service Expansions, Relocations, and Changes of Ownership– Additional items and services beyond those within
the clinical families of services furnished and billed prior to November 2, 2015 will not be excepted services
– An excepted off-campus PBD will lost its excepted status if it changes location
– New owners accepting the existing Medicare provider agreement from the prior owner, the PBD may maintain its excepted status

Regulatory Update – Site Neutral
• CMS proposes one-year transitional policy while it explores changes to allow PBD to bill Medicare under Part B payment system– During this period, CMS will pay physicians
furnishing services in PBD at the higher “non-facility” PFS rate
– No payment made directly to hospital by Medicare