
NCA - TBC - Session 1 Slides
69
We will begin shortly… Welcome 1
-
Upload
chc-connecticut -
Category
Healthcare
-
view
794 -
download
0
Transcript of NCA - TBC - Session 1 Slides

We will begin shortly…
Welcome
1
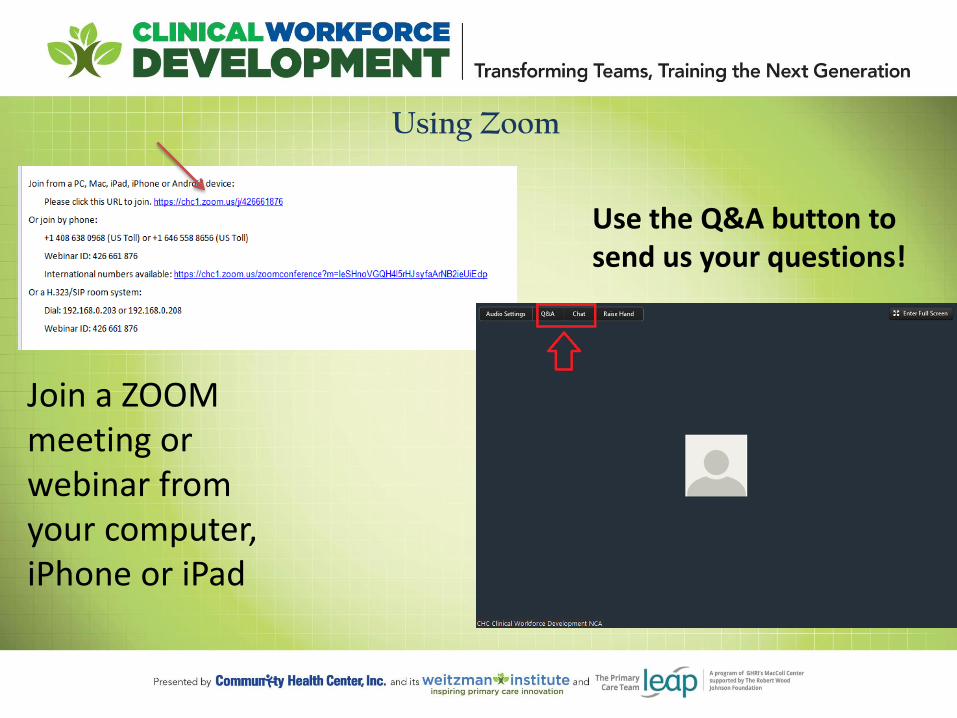
Using Zoom
Join a ZOOM meeting or webinar from your computer, iPhone or iPad
Use the Q&A button to send us your questions!
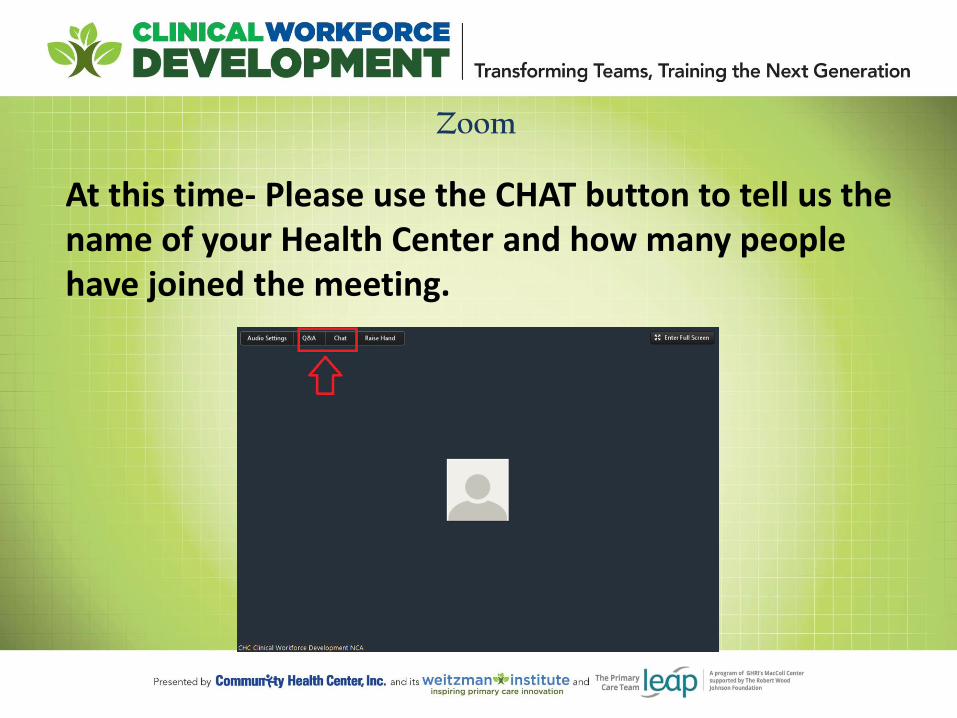
Zoom
At this time- Please use the CHAT button to tell us the name of your Health Center and how many people have joined the meeting.
4
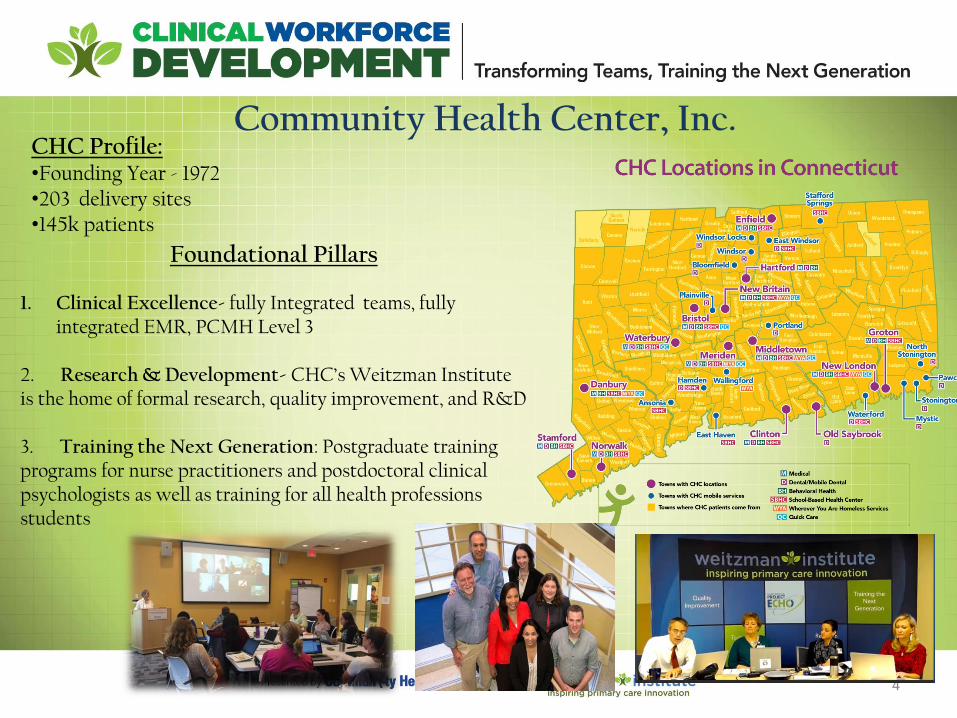
Community Health Center, Inc.
Foundational Pillars
1. Clinical Excellence- fully Integrated teams, fully integrated EMR, PCMH Level 3
2. Research & Development- CHC’s Weitzman Institute is the home of formal research, quality improvement, and R&D 3. Training the Next Generation: Postgraduate training programs for nurse practitioners and postdoctoral clinical psychologists as well as training for all health professions students
CHC Profile: •Founding Year - 1972 •203 delivery sites •145k patients
The Community Health Center, Inc. and its Weitzman Institute will provide education, information, and training to interested health centers in Transforming
Teams and Training the Next Generation
• National Webinars on advancing team based care, implementing post-graduate residency programs, and health professions students in FQHCs.
• Invited participation in Learning Collaboratives to advance team based care or implement a post-graduate residency program at your health center.
CHC’s NCA on Clinical Workforce Development The National Training and Technical Assistance Cooperative Agreements (NCAs) provide free training and technical assistance that is data driven, cutting edge and focused on quality and operational improvement to support health centers and look-alikes.

National Webinar Series -2892 viewers attended the webinar series -Most attended webinar: Enhancing the Role of the Medical Assistant -(March 3, 2016) 373 attendees - Videos: Viewed a total of 1,102 times - Slides: Viewed a total of 6,746 times - Representation from all 50 states, US Virgin Islands, Puerto Rico and
Canada.

The LC Teams
147,769
1,708 0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Tota
l Pat
ien
ts
Participating FQHCs
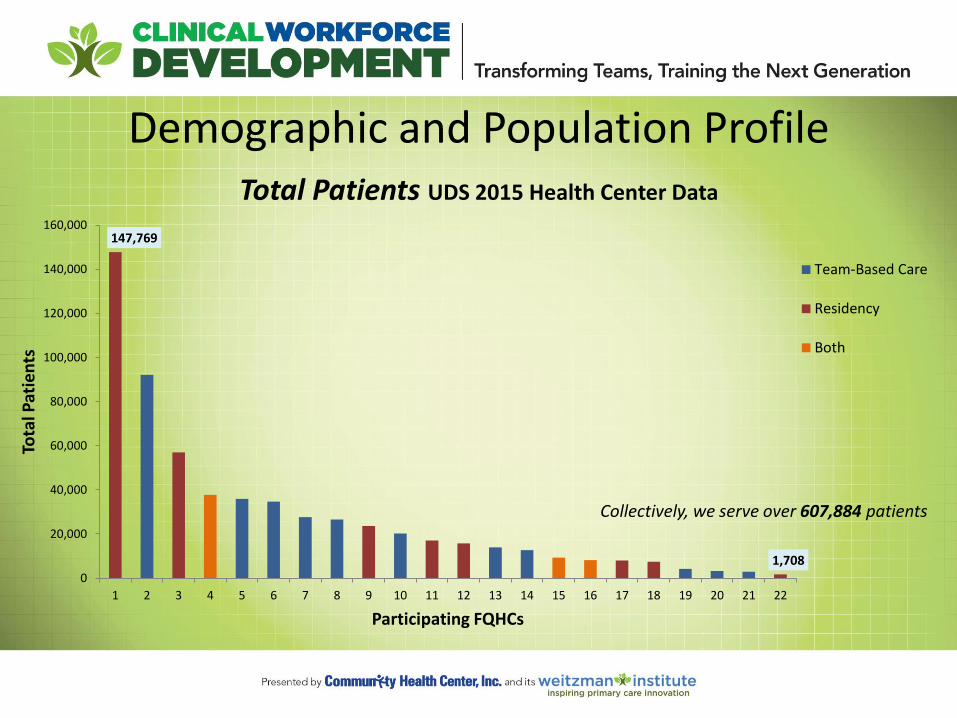
Total Patients UDS 2015 Health Center Data
Team-Based Care
Residency
Both
Demographic and Population Profile
Collectively, we serve over 607,884 patients

Demographic and Population Profile
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
% o
f To
tal P
atie
nts
Participating FQHCs
Age UDS 2015 Health Center Data
Older Adults (age 65 and over)
Adult (18 - 64)
Children (< 18 years old)

Patient Characteristics
Uninsured 18%
Medicaid/CHIP 57%
Medicare 9%
Other Third Party
16%
Payor Data UDS 2015 Health
Center Data
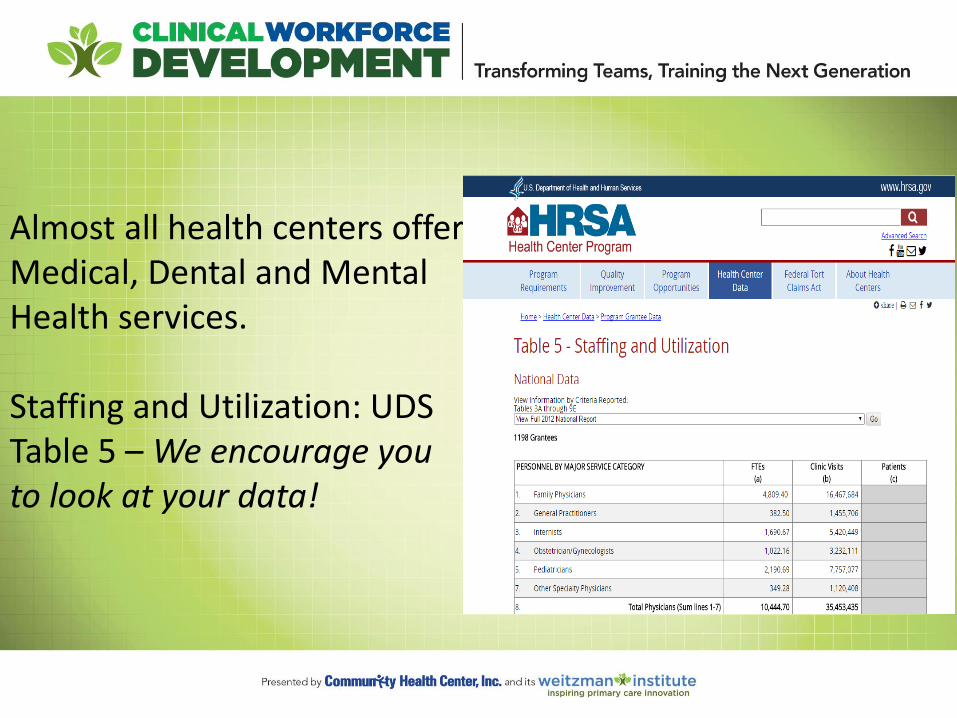
Almost all health centers offer Medical, Dental and Mental Health services.
Staffing and Utilization: UDS Table 5 – We encourage you to look at your data!

Quality Improvement Education Patti Feeney
Manager, Quality Improvement Education
Effective Meeting Skills
Providing meeting and team structure for coaches
I. AGENDA II. MEETING ROLES III. ACTION PLAN



Define the Problem Fishbone Diagram; a useful cause & effect tool

Developing a Project Specific Aim
All tools referenced in today’s session and support material can be found by following theses links:
NCA Team-Based Care Learning Collaborative
NCA Post-Graduate Residency Learning Collaborative
Tools and Resources >> Quality Improvement

We will begin shortly…
Welcome
20

Team Based Care (TBC)
Learning Collaborative
Session One
September 21, 2016
3:35 - 4:30 EST
Introductions
TBC Collaborative Design, Facilitation, Faculty
Ann Marie R Hess NP, MS
National Cooperative Agreement
Anna Rogers, Director
Reema Mistry, Project Assistant
Mentors , Coaching Faculty
Deborah Ward, RN (1:8)
Kasey Harding (1:8)
3:35
Evaluation Faculty
Kathleen Thies, PhD, RN
Improvement Science Faculty
Patti Feeney
Mark Splaine, MD

Session 1 Objectives
Teach effective meeting skills, cause and effect diagramming, and writing specific aims to support team improvement work.
Provide an overview of the learning collaborative structure and expectations.
Help teams ‘get started’ redesigning roles.
Review Action Period 1 assignments for improving team based care.
Learning Session 1 Agenda
Team Based Care Participants
3:35 10 min Introductions
3:45 10 min Collaborative Goal, Structure and Expectations, Resources
3:55 15 min Getting Started Tools : Role Activity Assessment , Cycle Time
4:10 10 min Action Period 1 Assignments
4:20 10 min Brief Team Meeting Break Out
Interviews : General Impressions
Many asked for clarification of team and coach definitions
Lots of recent growth and change in many organizations
Many reported EHR challenges re: data, documentation, duplication, and getting actionable reports
Few have depth of experience with primary care redesign models and QI methods (e.g Wagner, Bodenheimer, Nuka Alaska, PCMH, IHI)
Most are familiar with term PDSA
Most not meeting weekly to focus on QI, ‘fit into’ day of back to back visits
All have been evolving their team based model of care over time, multiple starts, looking for “refresh”
Many working on PCMH certification, recertification
Few practices have experience with coaching model
Introductions

Interviews : Goals and Expectations
Want structure, guidance, resources from the Collaborative: how-to’s vs concepts
Learn from others’ and their mistakes
Common Goals | Global Aims
• better efficiency, improved workflows
• staff working at top of license, includes standing orders and protocols
• team role clarity and standardization (care management, documentation)
• improve quality outcome measures (e.g. UDS outcomes)
• improve patient and team satisfaction
Reduce stress and “put the joy back into practice, need “relief from the chaos”
We have a cohesive, good team but we “all work in our silos to get the work done”
Introductions

Introductions
Name of FQHC Coach Team
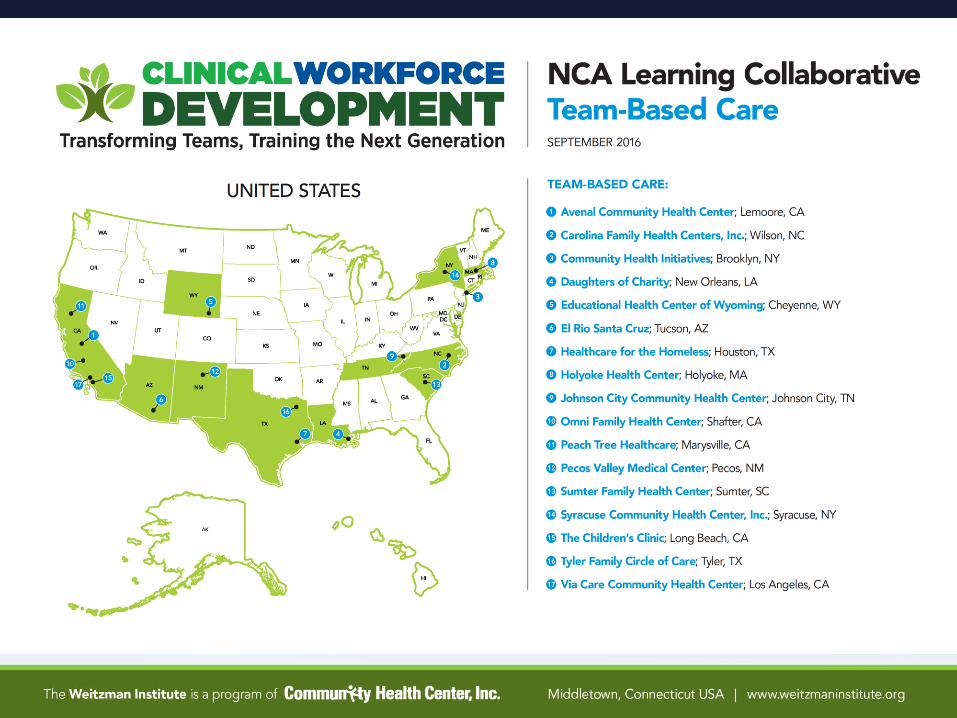
Carolina Family Health Centers , Inc.
Chasity Godwin 1 MD, 1 NP, 2 LPN, 1 Care Coordinator, 1 Front Desk, 1 Interpreter,
1 CNA
Community Health Initiatives Zlata Vainstein 1 Medical Director, 1 Physician, 2 MA, 1 Front Desk
Daughters of Charity Grace Mena 1 Area Practice Manager, 1 MD, 3 FNP, 2 Care Coordinator, 4 MA
Healthcare for the Homeless Carlie Brown Need new team
Holyoke Health Center Megan T. Wechsler (Primary) 1 Director of Quality and Compliance, 1 Physician, 3 RN, 1 MA, 1
Front Desk
Johnson City Community Health Center
Flo Weierbach 1 front Desk, 1 PNP, 1 LCSW, 1 RN, 1 Interpreter
Sumter Family Health Center Sandra Sturkie
1 Director of Patient Services, 1 Clinical Manager, 1 BH Clinical Manager, 1 BH RN, 1 Physician, 2 Case Managers, 1 MA, 1 Dental Services Coordinator, 1 Patient Financial Coordinator, 1 Clinical IT,
1 Pharmacist, 1 Call Center Rep, 1 Referrals Manager
Syracuse Community Health Center, Inc.
Cathy Brigden
1 Physician, 1 FNP, 1 LPN, 2 RN, 3 MA, 1 Office Manager
Tyler Family Circle of Care Sherri Gould 1 CMO, 1 COO, 1 LVN, 1 OA, 1 PNP, 1 Process Improvement
Manager

Name of FQHC Coach Team
Avenal Community Health Center John Kalfayan 1 BH, 1 Physician, 1 MA, 1 Medical Director, 1 Front Desk
Educational Health Center of Wyoming Brenda Burnett 1 Provider, 2 RN, 1 Radiologic Technologist, 1 EMR Manager, 1
MA, 1 Clinical Manager
El Rio Santa Cruz Josh Carzoli 1 MA, 1 RN, 1 BH, 1 Chief Clinical Officer, 1 LPN, 2 Physician, 1
Front Desk, 1 COO, 3 RN Clinic Manager, 1 IT
Peach Tree Healthcare Ruben Ruiz 1 Chief Quality Officer, 1 Quality Coordinator, 1 Dir of
Operations, 1 Site Manager, 1 Dir of HR, 1 NP, 3 MA, 1 Data Analyst, 1 Ops Specialist, 1 Clinical Support Services Manager
Pecos Valley Medical Center L. David Young 2 RN, 1 NP, 1 MA
The Children’s Clinic Karla Rodriguez 1 Provider, 1 MA, 1 Care Team Rep
Via Care Community Health Center Kimberly McFerguson 1 FNP, 1 MA, 1 Outreach & Enrollment Specialist, 1 MSW, 1
Front Office Lead MA
Introductions
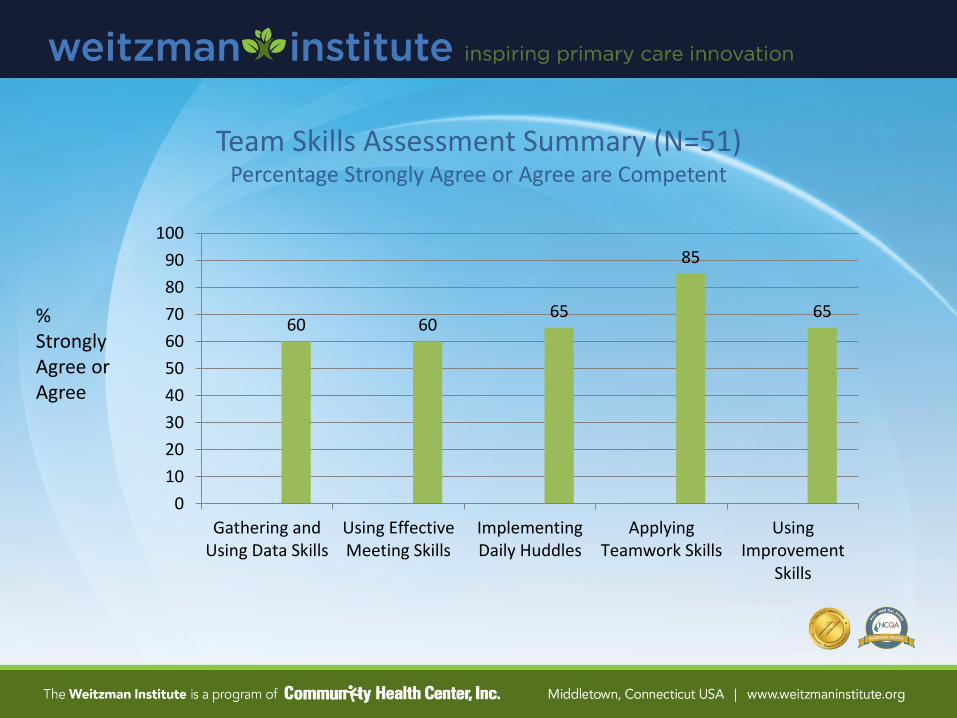
Team Skills Assessment Summary (N=51) Percentage Strongly Agree or Agree are Competent
% Strongly Agree or Agree
60 60 65
85
65
0
10
20
30
40
50
60
70
80
90
100
Gathering andUsing Data Skills
Using EffectiveMeeting Skills
ImplementingDaily Huddles
ApplyingTeamwork Skills
UsingImprovement
Skills

Coach Skills Assessment Summary (N=16)
Percentage who rated themselves Competent, Proficient, or Expert
35
65
47 47
59
0
10
20
30
40
50
60
70
80
90
100
Data andInformation
Systems
Meeting andInterpersonal Skills
Improvement Skills Technical Skills(excel, webinar)
Art of CoachingSkills
%

Level D: Just Getting Started Level C: Early Stages of Change Level B: Implemented Basic Changes Level A: Achieved Most or All of the Important Change Required
Team Based Practice Assessment (LEAP)

0
1
2
3
4
5
6
7
Level A Level B Level C Level D
Self-Management Support
Planned Care
Care Management
Medication Management
Care Activities Assessment (N=11) Number of sites reporting level of performance implementing key processes
Just getting started
Early stages of change
Implemented basic changes
Achieved most or all of the
important changes required
0
1
2
3
4
5
6
7
Level A Level B Level C Level D
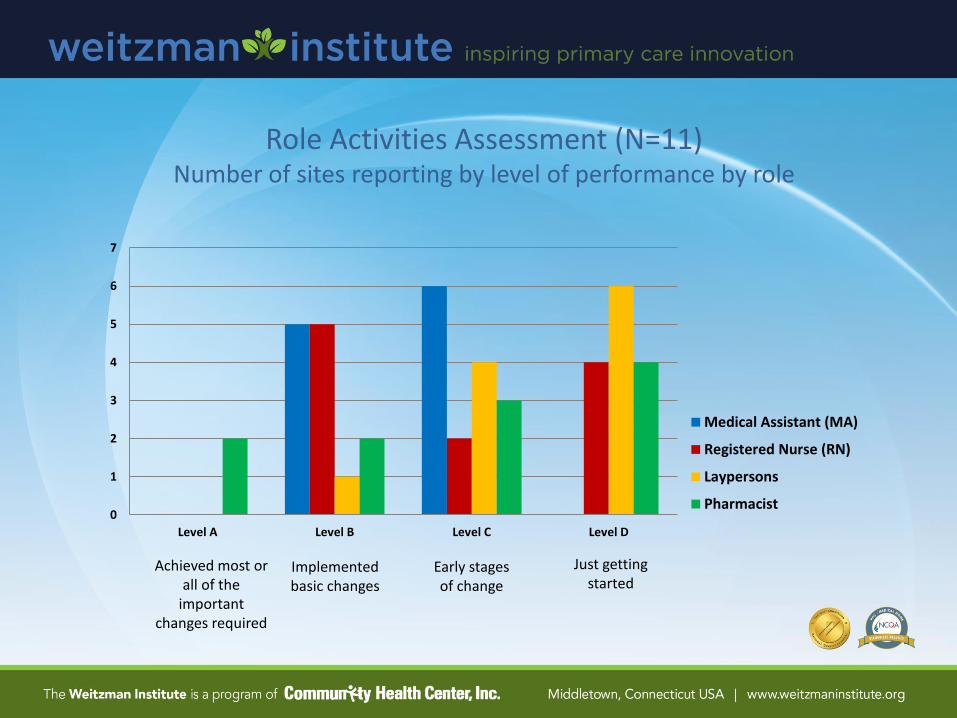
Medical Assistant (MA)
Registered Nurse (RN)
Laypersons
Pharmacist
Role Activities Assessment (N=11) Number of sites reporting by level of performance by role
Just getting started
Early stages of change
Implemented basic changes
Achieved most or all of the
important changes required

Transformational Team Based Care Improves Outcomes
Learning Session 1 Agenda
Team Based Care Participants
3:35 10 min Introductions
3:45 10 min Collaborative Goal, Structure and Expectations, Resources
3:55 15 min Getting Started Tools : Role Activity Assessment , Cycle Time
4:10 10 min Action Period 1 Assignments
4:20 10 min Brief Team Meeting (break out)

Goal
The Team-Based Care Learning Collaborative is designed to provide transformational* strategies and mentored coaching support,
to help a core team implement an advanced model of team-based care over 12 months.
*Transformation can take up to 18-24 months
3:45
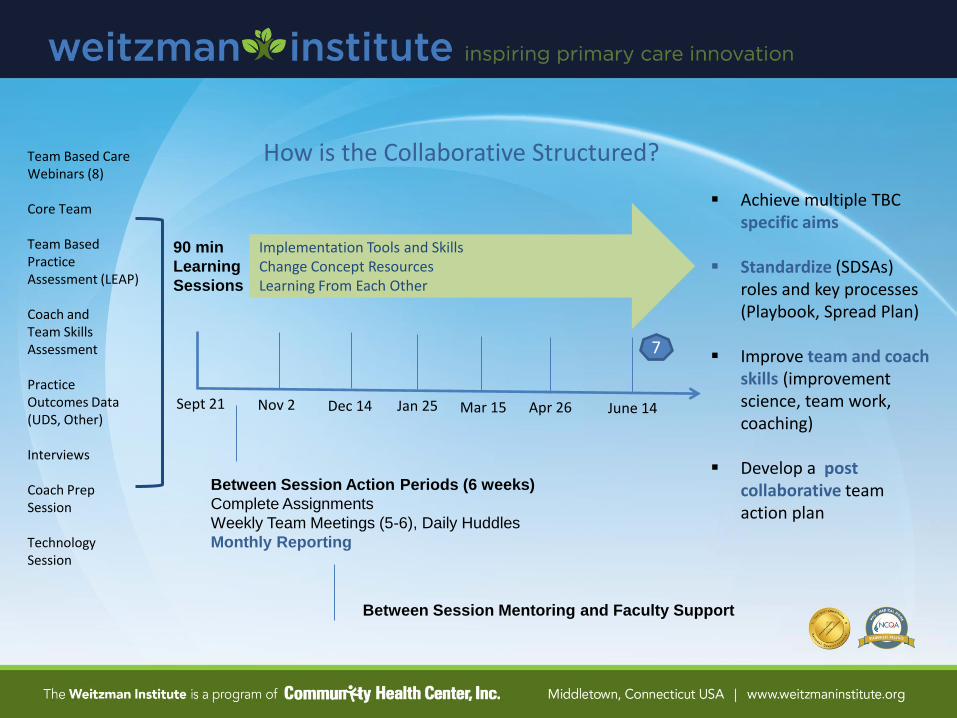
Achieve multiple TBC specific aims
Standardize (SDSAs)
roles and key processes (Playbook, Spread Plan)
Improve team and coach
skills (improvement science, team work, coaching)
Develop a post
collaborative team action plan
How is the Collaborative Structured?
90 min
Learning
Sessions
Between Session Action Periods (6 weeks)
Complete Assignments
Weekly Team Meetings (5-6), Daily Huddles
Monthly Reporting
Implementation Tools and Skills Change Concept Resources Learning From Each Other
Team Based Care Webinars (8)
Core Team Team Based Practice Assessment (LEAP) Coach and Team Skills Assessment Practice Outcomes Data (UDS, Other) Interviews Coach Prep Session Technology Session
Between Session Mentoring and Faculty Support
7
Sept 21 Nov 2 Dec 14 Jan 25 Mar 15 Apr 26 June 14

Improvement Science Theory Bursts (10 min) Developing Skills
Session 1 : Sept 21st
o Running effective team meetings using tools
o Developing and using a cause and effect diagram to inform PDSAs
o Writing a specific aim statement
Session 2 : Nov 2nd
o Developing a process map or current state workflow
o Applying PDSA methodology for improvement
Session 3 : Dec 14
o Using data for improvement (run charts, control charts)
Session 4 : Jan 25
o Standardizing (SDSAs) and Reliability Science
Session 5 : March 15
o Spreading Change
Session 6 : April 26
o Gantt Charting : 3-6 month Core Team improvement plan

Mentor and Coach Roles
Coaches (posted role descriptions)
Help and support teams in learning new skills and achieving their aims
Help teams complete action period assignments, monthly reports, evaluation
Meet weekly with Mentor and other coaches, 1:1 as needed
Participate in 7 learning sessions
Support weekly team meetings, and between meeting assignments, session prep
Mentors (posted role descriptions)
Provide support and resources for developing coaching skills
Facilitate weekly debriefs with Coaches
Provide individual support as needed

NCA Online Learning Network Find material for download, TBC webinars, and team folders for sharing your work... Improvingprimarycare.org
Discussion Board Ask questions or make requests of teams, faculty….

Any Questions?
Before “Getting Started”….
3:55

Implementing Team Based Care (Webinar #1)
Webinar 1

Defining Structure and Staff Responsibilities
Practice Managers and Leaders : must stay involved, engaged in your work

Start with Core Team, Then Expanded Team
Current State Examples: 8 Participating Teams
1 MD, 1 NP, 2 LPN, 1 Care Coordinator, 1 Front Desk, 1 Interpreter, 1 CNA
1 MD, 2 MA, 1 Front Desk
1 PNP, 1 LCSW, 1 RN, 1 Interpreter, 1 front Desk,
1 MD, 3 FNP, 2 Care Coordinator, 4 MA
1 MD, 1 FNP, 1 LPN, 2 RN, 3 MA, 1 Office Manager
1 FNP, 1 MA, 1 Outreach Specialist, 1 MSW, 1 Front Office, Lead MA
1 BH, 1 MD, 1 MA, 1 Front Desk
1 Provider, 2 RN, 1 Radiologic Tech, 1 MA

TBC Concept Resource (webinar #1 and #2) Principle
Patients want to receive their care from smaller teams (PODS) and know them personally Physical
Wall colors differentiate pods in practice , match business cards Central open area surrounded by exam rooms Co location of pod members, all carry laptops 3 exam rooms per provider – all care comes to patient 2 pods share procedure room - standardized
TBC Structure Break down large systems into PODS (care teams) 4 “Empaneled” Providers (3FTEs), 3 MAs dedicated to provider (dyad) 1 BH, 1 RN, 1 Case Coordinator (navigator, health coach), 1 front desk, Patient empaneled both to a pod and to a Dyad Flow Coordinator and Team Manager rotating roles (RN, MA) Medical Records staff – input electronic data
Roles and Responsibilities Defining and Training, Standing Orders and Protocols
Standardizing Workflows • Making ‘hundreds’ accessible to all
Teams Need to Meet • Daily Huddles : 8am and 2pm • Weekly Meetings : Improvement Work, Population Health Management
Poll Question
Would you say that you have ‘significant’ work to do defining your “core” and “extended” team structure?
Yes
No

Role Activity Assessment
Who Does What Now?
4:08

Why analyze your team’s roles?
Have the right person doing the right thing at highest level of training and licensure
Eliminate duplication or unnecessary work
Reduce interruptions
Challenge assumptions about what staff are doing
Increase capacity to take on new activities
Develop specific aims for improvement

Implementing Team Based Care (Webinar #1)
Webinar 1

Role Assessment of ‘the work’: Webinars 1-8

Role Activity Assessment (customizable)

Role Tracking Worksheet
Consider Tracking
Interruptions
Role Activity Analysis
Position:
Tic Marks (each time
activity done, may add AM,
PM)
Total Tic Marks
Estimated Time per Activity in minutes
Total Time
Access and Communication Processes Activity
1. Schedules patients with a personal clinician for continuity of care
||||| ||||| |||||
15
4 min 60 min
2. Coordinates visits with multiple clinicians and/or diagnostic tests and procedures
3. Triages how soon a patient needs to be seen including a process for after-hours care
4. Monitors access to appointment, backlog and wait time using telephone and email requests
5. Monitors and triages secure patient portal messages
6. Provides advice on clinical issues via telephone or
portal messaging
7. Identifies and arranges for language services
8. Collects patient demographic and insurance information, including preferred method of communication
9. Helps patients activate their Personal Health Record by signing up during office visit
10. Identifies and refers patients who might benefit from care management support, other practice resources, community services
Population Health Management Activity
1. Uses population registries and clinical quality reports to monitor a panel of patient’s health and risk status and close care gaps.
2. Communicates with many patients at once via bulk outreach letters and portal messaging (e.g. reminders for preventive care visits ,testing, screening gaps)
3. Provides outreach services to patients overdue for visit to follow up management of chronic
SampleData.Hess.2009
Worksheet.clinicalmicrosystem.org
IHI.org Poster
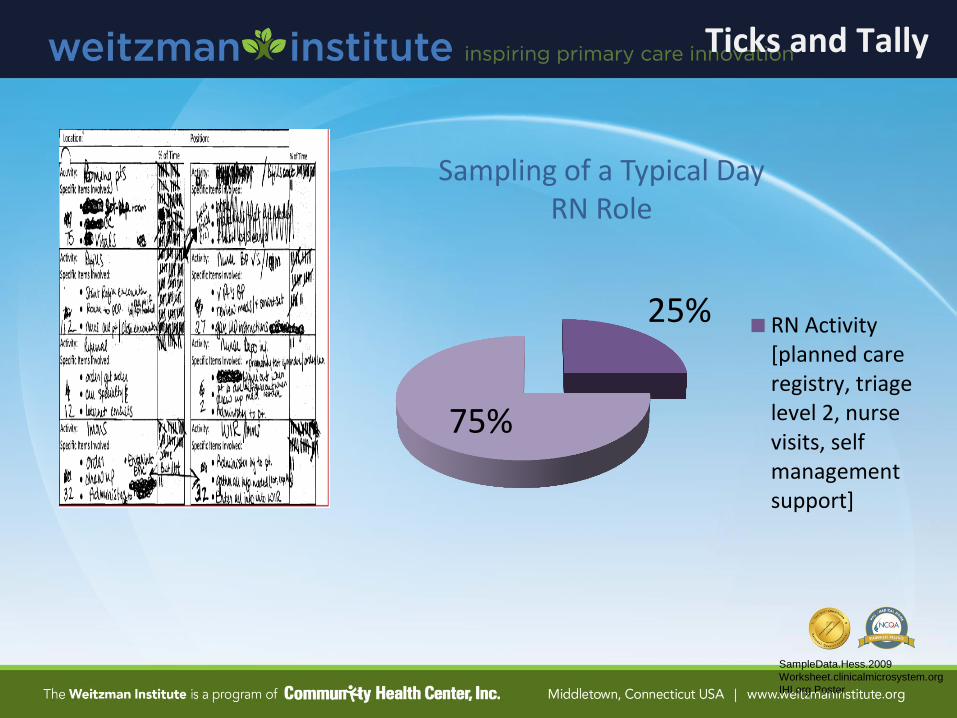
25%
75%
RN Activity[planned careregistry, triagelevel 2, nursevisits, selfmanagementsupport]
Sampling of a Typical Day RN Role
Ticks and Tally

55
33%
67%
Non-Physician Tasks Physician Tasks
Non-Physician Tasks
-immunizations
-obtaining consults
-obtaining MR
-setting up room
-filling out clerical fms
-finding interpreter
-bringing pt to room
-data entry
-finding information

Webinar #1

Receptionists
Telephone Encounters: Significant # of calls were within 3 days after a visit Printing All AVSs (thought they had to) : 50% patients did not want paper, shred.

Poll Question
Have you ever participated in any type of analysis of what you do every day (tasks and functions)?
YES
NO

Using Cycle Time to Improve Efficiency
and Office Flow
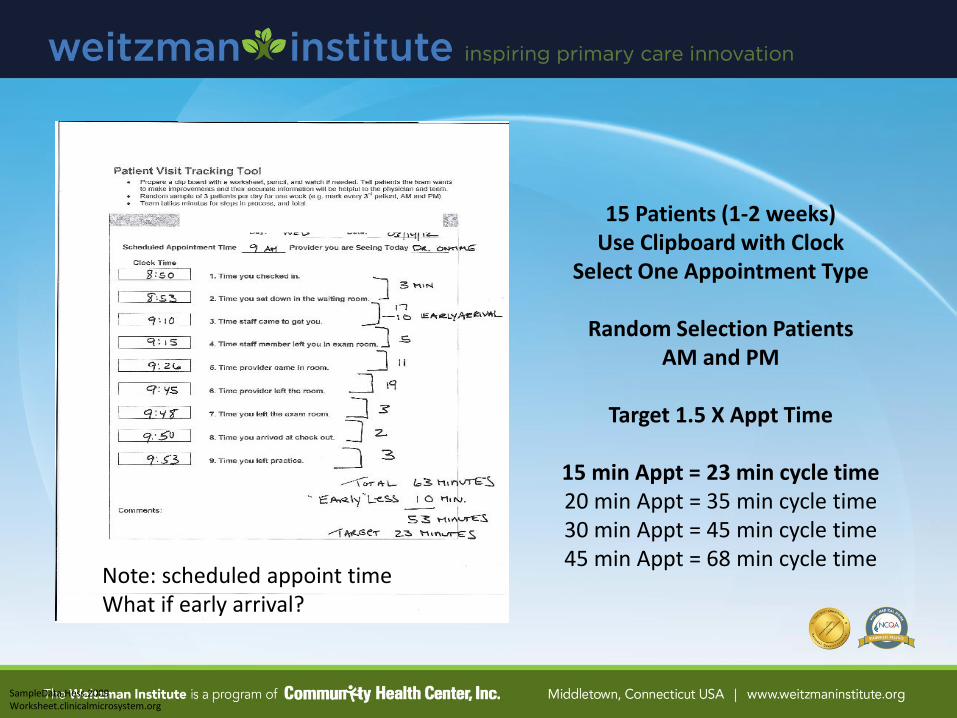
15 Patients (1-2 weeks) Use Clipboard with Clock
Select One Appointment Type
Random Selection Patients AM and PM
Target 1.5 X Appt Time
15 min Appt = 23 min cycle time 20 min Appt = 35 min cycle time 30 min Appt = 45 min cycle time 45 min Appt = 68 min cycle time
SampleData.Hess.2009 Worksheet.clinicalmicrosystem.org
Note: scheduled appoint time What if early arrival?
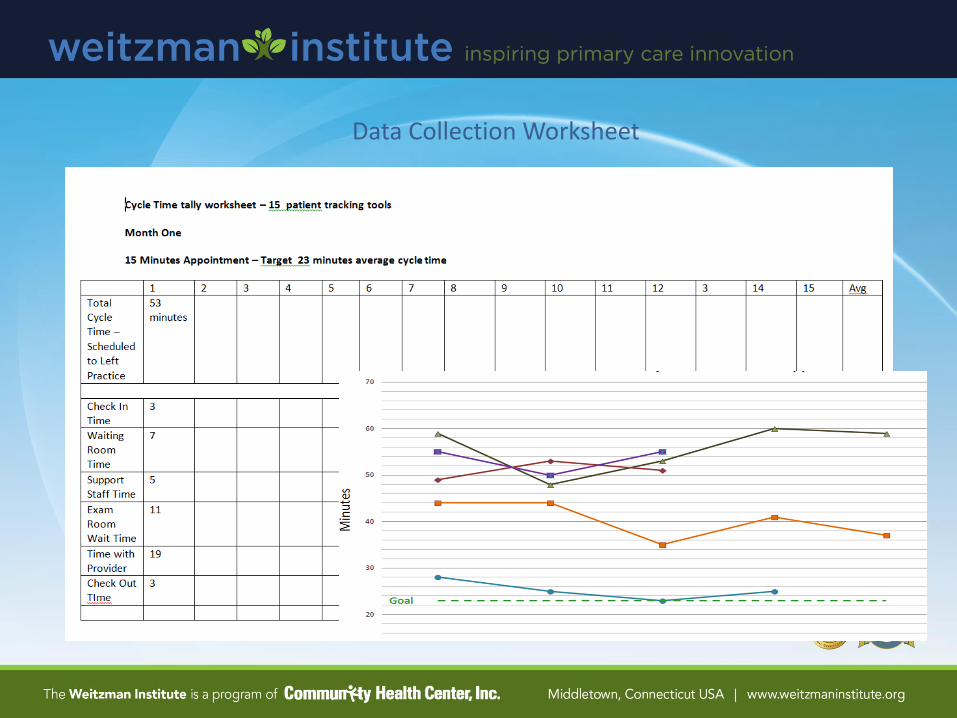
Data Collection Worksheet
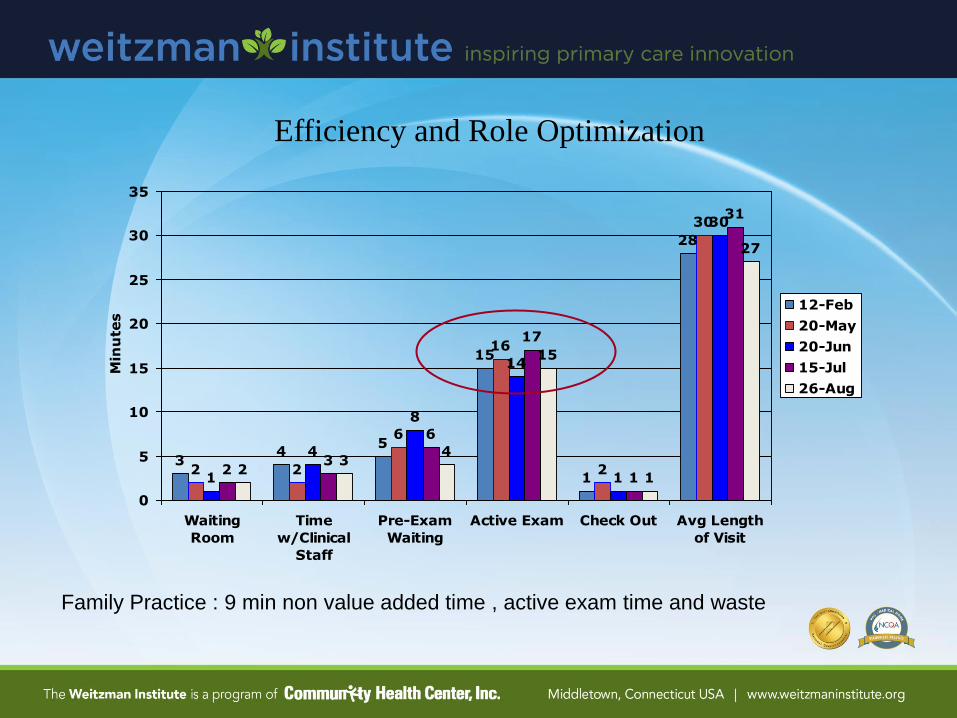
Efficiency and Role Optimization
34
5
15
1
28
2 2
6
16
2
30
1
4
8
14
1
30
23
6
17
1
31
23
4
15
1
27
0
5
10
15
20
25
30
35
Waiting
Room
Time
w/Clinical
Staff
Pre-Exam
Waiting
Active Exam Check Out Avg Length
of Visit
Min
ute
s
12-Feb
20-May
20-Jun
15-Jul
26-Aug
Family Practice : 9 min non value added time , active exam time and waste

Hess.CPM.2010
Example: Assessment data (long cycle time) is analyzed using Fishbone Diagram Problems that have high leverage for improving results, inform your PDSAs (session 2). Top of the Ramp – Specific Aim
Putting It Together for Action Period 1

Action Period 1 Assignments
1. Meet weekly (50 min) as a Core Team
Practice effective meeting skills and use tools with coaching support
2. Continue Daily Huddles (5-10 min) | Starting is Optional
3. Complete and share the following by uploading to TBC website: - Within 4 weeks
a) What is your global aim? – the broad objective you want to achieve in the longer run
b) Role Activity Assessment (who does what now)
c) Role Activity Tracking Data (1-3 days, all roles, coach inputs data)
Fishbone diagram with drivers of role problem(s)
Document any ‘quick hits’, insights
Write a specific aim for improvement using role data
d) Cycle Time Assessment (15 )
Fishbone diagram with drivers of cycle time problem
Document any ‘quick hits’, insights
Write a specific aim for improvement using cycle time data
4. Upload monthly progress report to inform Session 2 Planning.
5. Upload all missing assessments.

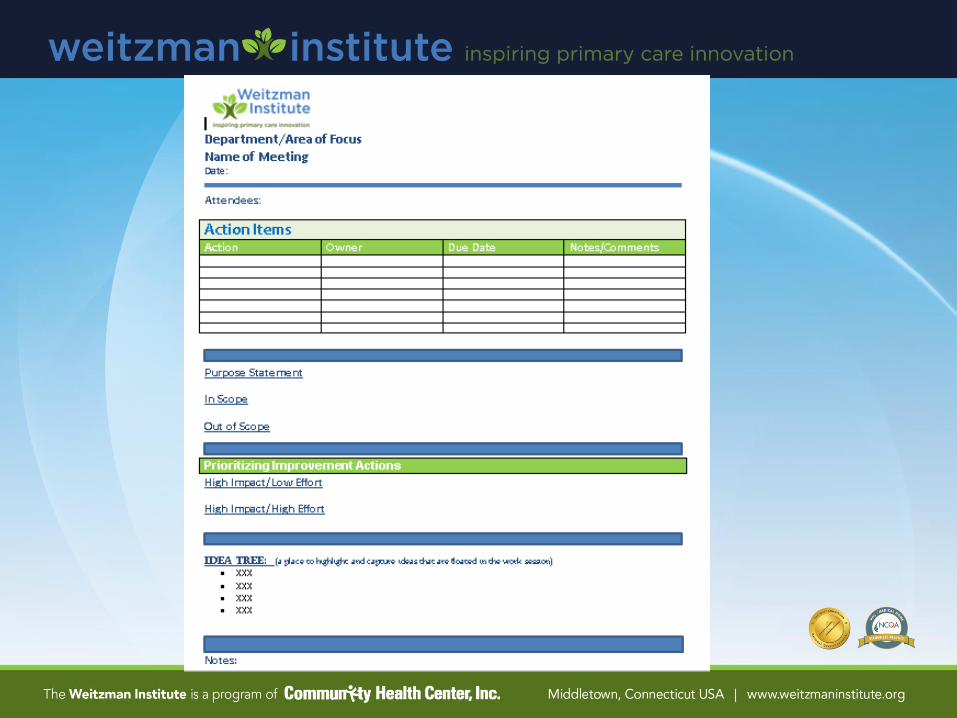
Monthly Reporting
Tool
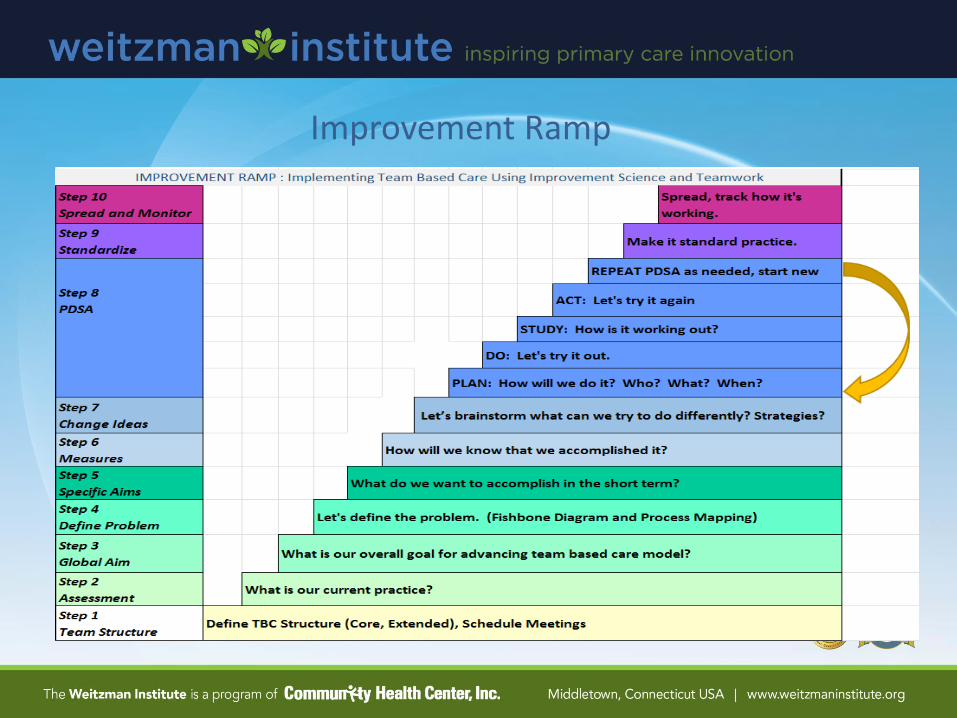
Improvement Ramp

Wrap Up and Questions
Set Up Brief Team Meeting
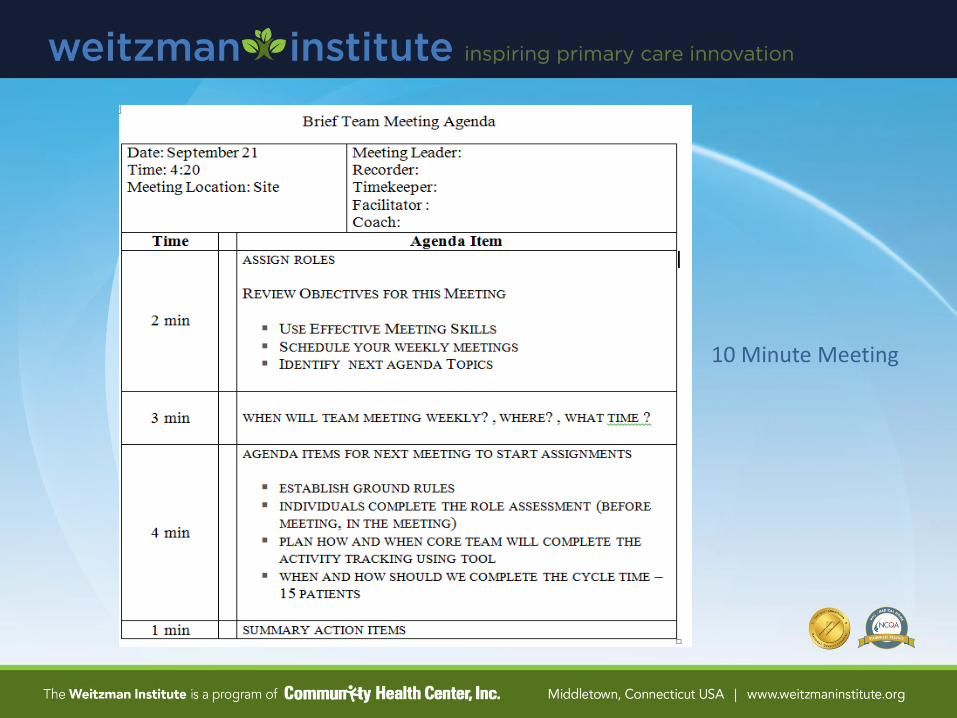
10 Minute Meeting

Thank Your Colleagues



![OUTDOOR POWER EQUIPMENT · [tbc] tbc-270pfds 20 tbc-270pfs 17 tbc-270s 17 tbc-270sfs 24 tbc-290 18 tbc-290d 20 tbc-290s 18 tbc-340 18 tbc-340d 21 tbc-340ds 21 tbc-340pf 18 tbc-340pfd](https://static.fdocuments.us/doc/165x107/5e2726727836ca4a7e750b4c/outdoor-power-equipment-tbc-tbc-270pfds-20-tbc-270pfs-17-tbc-270s-17-tbc-270sfs.jpg)














