An Analysis of Health Insurance Premiums Under the Patient ...

1
Navigating Health Care Reform Leading Age Delta Region Meeting
Presented by Erika James Oct. 9, 2013 Erika James Vice President, Employee Benefits Phone: 925-407-0416 Email: [email protected]

2
Table of Contents
▲ State of the Union: Healthcare Trends
▲ Understanding the Affordable Care Act (ACA)
▲ Timeline and Compliance Checklists
▲ Plan Design Requirements / Provisions
▲ Employer Obligations
▲ Premium Tax Credits and Cost Sharing Subsidies
▲ Health Insurance Exchanges
▲ Emerging Healthcare Models for Employers and Employees
▲ Additional Resources

____ __ ____ _____ ____ ______ _______
3
State of the Union: Healthcare Trends

4
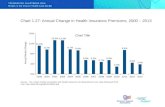
$508
$999
$2,875
$4,885
2003 2013
ER Contribution EE Contribution
$3,383
$5,884 74% Total Premium Increase
97% EE Contribution Increase
Average Annual Health Insurance Premiums and Worker Contributions
for Single Coverage

5
$2,411
$4,565
$6,657
$11,786
2003 2013
ER Contribution EE Contribution
$9,068
$16,351
80% Total Premium Increase
89% EE Contribution Increase
Average Annual Health Insurance Premiums and Worker Contributions
for Family* Coverage
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2013 * Family coverage is defined as health coverage for a family of four.

6
▲ Since 2002, premiums in California rose by 169.7%, more than five times the 31.5% increase in the state's overall inflation rate
▲ Average 2012 annual premiums for single and family coverage in California were 16% and 6% higher than national respectively
▲ Proportion of CA employers offering coverage has declined significantly over the last decade, from 71% in 2002 to 60% in 2012
— Higher offering rates are associated with larger firms, firms with higher wages, and firms with fewer part-time workers
$6,540
$16,632
$5,616
$15,744
Single Coverage Family Coverage
CA US
Source: California HealthCare Foundation/NORC California Employer Health Benefits Survey, 2012

____ __ ____ _____ ____ ______ _______
7
Understanding the Affordable Care Act (ACA)

8
Understanding ACA… Easy as 1, 2, 3!
1. Comply Implement all ACA
health coverage and associated requirements
2. Understand How is ACA/HCR
supposed to work?
How will it change coverage marketplaces (Individual, Group, Public Programs)?
Where could it fail?
What does it mean for your organization?
3. Strategize A compliance
strategy is not a HCR/health care management strategy
Don’t take your eye off the cost
Where does your organization want to be: reactive vs. proactive?

9
Understanding ACA New Industry Taxes and Fees
▲ Comparative Effectiveness Research Fee (PCORI) — $1 PMPY (due July 2013) for plans ending on or after
10/1/12
▲ Health Insurance Industry Fee — $8 billion in 2014 — +$100 billion over 10 years — Expected to increase premiums 2%-2.5% in 2014, 3%-4%
in later years
▲ Reinsurance Assessment Fee — Program to stabilize carriers in individual market from
“guarantee issue” risk — 2014―fully insured & self-insured plans — Approx. $60 PMPY
▲ Employer Excise (“Cadillac”) Tax — 2018―Employer Plan Sponsors with coverage costs
exceeding threshold are responsible for a 40% excise tax on the difference
$10,200 single/$27,500 family — Estimates are that many employer plans will exceed the
threshold based on current health care costs and industry norm trends

10
Understanding ACA Implications by Financing Options
FULLY INSURED PLANS SELF-INSURED PLANS
• Carriers in defensive position due to plethora of ACA-related requirements & changes
• Guarantee Issue & No Pre-Ex for Ind./Small Group markets
• Weak Individual Mandate
• Modified Community Rating for Ind./Small Group markets
• Required Coverage of Essential Health Benefits for Ind./Small Group Plans
• Essential Health Benefits cannot have dollar limits and are defined by State’s BM Plan
• MLR Requirements
• Insurance Industry Fee = +2%-2.5% (2014), +3%-4% (later yrs.)
• Plan sponsors are not subject to community rating rule s and other carrier requirements
• Elimination of taxes and carrier pass through fees
• Essential Health Benefits not required, but if covered cannot have dollar limits
• Plan sponsor defines EHB
• Plan sponsors are able to customize plans to meet specific needs – Value -based plan design – Custom provider networks – Direct return on successful population health
management strategies / claims impact
• Employers of various sizes embracing self-insured strategies

11
Understanding the ACA How is it supposed to work?
PROVIDE ACCESS FOR 48 MILLION UNINSURED /
IMPROVE ACCESS FOR OTHERS STRENGTHEN COVERAGE STABILIZE COVERAGE COSTS
• All individual coverage is guarantee issue/no pre-ex, no medical UW
• Establishes Health Insurance Exchanges for individuals/ small businesses
• Employer mandate & child eligibility to age 26
• Insurance Affordability Programs
Medicaid expansion, federal premium tax credits & subsidies
• “Minimum Essential Coverage” Plan Requirements
• Individual / Small Group Coverage Reforms
Essential Health Benefits requirement with no annual/ lifetime dollar limits
100% preventive care requirement
Deductible limits
Out-of-pocket limits
Actuarial value 60%
• Large Group / Employer Coverage Reforms
No annual / lifetime limits on Essential Health Benefits
100% preventive care
Out-of-pocket limits
Minimum value 60%
• Phase out of most Limited Medical Plans
• “Individual Coverage Requirement” (Individual Mandate)
• New Individual/ Small Group Market Rating Reform
“Modified Community Rating” & “Single risk pool” requirements
• Reinsurance, Risk Corridors & Risk Adjustment Programs to Stabilize Individual/Small Group Markets
• New Medical Loss Ratio Requirements for Carriers
• Some provisions allowing individual coverage costs to be tied to health/ wellness factors

12
Understanding the ACA Will it work?
PROVIDE ACCESS: STRENGTHEN COVERAGE: STABILIZE COVERAGE COSTS:
• Will guarantee issue/no pre-ex requirement cause huge carrier losses? Who will buy?
• Will health insurance exchanges be ready, much less work?
• Will employers exit?
• Will the U.S./ state fiscal situation lead to a scaling back of Insurance Affordability Programs?
• Will new coverage requirements lead to spiraling costs?
• Individual/Small Group coverage requirements are staggering for carriers
Essential Health Benefits
60% Minimum Actuarial Value
Exchange Requirements―Qualified Health Plans
• Will the Individual Mandate be sufficient enough to motivate younger uninsured individuals to buy and maintain coverage?
$95 (2014)
$695 (2016)
• Will new Individual/ Small Group Market Rating Reform work or throw insured market into turmoil?
GI / No pre-ex ― carriers must take all comers
Modified community rating ― changes the playing field
Reinsurance, Risk Corridors & Risk Adjustment Programs ― unsubstantiated

13
Understanding the ACA Implications by Financing Options?
FULLY INSURED PLANS SELF-INSURED PLANS
• Carriers in defensive position due to plethora of ACA-related requirements & changes
• Guarantee Issue & No Pre-Ex for Ind./Small Group markets
• Weak Individual Mandate
• Modified Community Rating for Ind./Small Group markets
• Required Coverage of Essential Health Benefits for Ind./Small Group Plans
• Essential Health Benefits cannot have dollar limits and are defined by State’s BM Plan
• MLR Requirements
• Insurance Industry Fee = +2%-2.5% (2014), +3%-4% (later yrs.)
• Employers of various sizes embracing self-insured strategies
• Elimination of taxes and carrier pass through fees
• Essential Health Benefits not required but if covered cannot have dollar limits
• Plan sponsor defines EHB
• Plan sponsors are able to customize plans to meet specific needs – Value -based plan design – Custom provider networks – Direct return on successful population health
management strategies / claims impact
• Stop-loss markets are responsive and competitive (down market)

____ __ ____ _____ ____ ______ _______
14
Timeline & Compliance Checklists

15
Affordable Care Act Implementation Timeline
2010 2011 2012 2013 2014 2015 2018 Small Business Tax
Credits Funding for Small Business Wellness
Programs
Summaries of Benefits and
Coverage
FSA Limits 90-Day Max Waiting Period
60-Day Max Waiting Period CA
Small Group
Employer Mandate-Play or Pay
Cadillac Tax
Adult Dependent Coverage
Medical Loss Ratio Rebates
Medicare Tax Increase
Individual Mandate Automatic Enrollment
No Lifetime Dollar Limits
No Part D Deduction Health Insurance Exchanges
New Nondiscrimination
Rules
Restrictions on Annual Dollar Limits
PCORI Fee Community Rating-Small Group &
Individual
Employer Reporting Requirements*
No Rescissions Except Fraud
Health Insurance Exchange
Notifications
Guaranteed Issue / No Pre-Ex
No Pre-existing Conditions for
Children
No Annual Dollar Limits
No OTC Reimbursement from FSA, HSA
Enhanced Wellness Incentive/ Penalty
External Review Procedures
Cost Sharing & Ded. Limits
Full Coverage of Preventive Services
*2016 requirement for 2015 plan year

16
Employer Compliance Checklist Notices and Disclosures
Notice/Disclosure Plans Impacted Effective Date GF/non-GF
Notice of Exchange* Small/ Large Employer Oct. 1, 2013 Both
Summary of Benefits and Coverage Small/ Large Employer
First OE and plan years beginning on or after
9/23/12 Both
60-Day Notice of Plan Changes Small/ Large Employer SBC plan year effective
date Both
Notice of Rescission Small/ Large Employer Plan years beginning on
or after 9/23/10 Both
Statement of Grandfathered Plan Status Small/ Large Employer Plan years beginning on
or after 9/23/10 GF
Notice of Patient Protections and Selection of Providers
Small/ Large Employer Plan years beginning on
or after 9/23/10 Non-GF
* No penalty for non-compliance

17
Employer Compliance Checklist Plan Design & Coverage Requirements ― in Effect
Requirements Effective Now Plans Impacted Effective Date plan years beginning
on or after:
GF/ non-GF
Dependent Coverage to Age 26 Small/ Large Employer 9/23/10 Both
No Lifetime Dollar Limits/Dollar Limit Restrictions on Annual Limits
Small/ Large Employer 9/23/10 Both
No Rescissions (except for fraud and material misrepresentations)
Small/ Large Employer 9/23/10 Both
No Pre-Existing Condition Exclusions for Children Small/ Large Employer 9/23/10 Both
No reimbursement for OTC Medicine and Drugs (w/o a prescription)
Small/ Large Employer 1/1/11 Both
No Cost-sharing for Preventive Care Services Small/ Large Employer 9/23/10 Non-GF
Additional Preventive Care Services for Women Small/ Large Employer 8/1/12 Non-GF
Requirements for Internal Claims and Appeals and External Review
Small/ Large Employer 9/23/10 Non-GF
Patient Protections and Selection of Providers (PCP, OB/GYN, ER)
Small/ Large Employer 9/23/10 Non-GF
$2,500 Employee Contribution Limit to Health FSAs Small/ Large Employer 1/1/13 Both

18
Employer Compliance Checklist Plan Design & Coverage Requirements ― 2014
2014 Requirements Plans Impacted Effective Date plan years beginning
on or after:
GF/ non-GF
No Pre-Existing Condition Limitation Small/ Large Employer 1/1/14 Both
No Annual Dollar Limits on Essential Health Benefits
Small/ Large Employer 1/1/14 Both
90-day Waiting Period Limit 60-Day Waiting Period Limit for CA Small Groups
Small/ Large Employer 1/1/14 Both
Deductible Limits for Health Plans Small Employer 1/1/14 Non-GF
Out-of-Pocket Max Limits for Health Plans Small/ Large Employer 1/1/14 Non-GF
Required Coverage of Clinical Trials Small/ Large Employer 1/1/14 Non-GF
Non-discrimination for Fully Insured Plans* Small/Large Employer Delayed Non-GF
Required Coverage of Essential Health Benefits Small Employer 1/1/14 Non-GF
* Regulations pending or not final

19
Employer Compliance Checklist Employer Obligations
Provision Plans Impacted Effective Date
W-2 reporting Large Employer** 2013 for 2012 pay year
Comparative Effectiveness Research Fee Small/ Large Employer 2013
Transitional Reinsurance Fees Small/ Large Employer 2014
Additional Medicare Tax N/A 2013 pay year
Employer Penalties for Not Offering Coverage- Section 4980H “Play or Pay”*
Large Employer Delayed until 1/1/15
Automatic Enrollment* Large Employer unknown
Employer Health Plan Reporting* Large Employer Delayed until 1/1/15
* Regulations pending or not final **Required if ≥ 250 EE W-2’s issued

20
Employer Compliance Checklist Miscellaneous
Provision Plans Impacted Effective Date plan years beginning
on or after:
GF/ non-GF
Non-discriminatory Health-contingent Wellness Programs
Small/Large Employer 1/1/14 Both
MLR Rebate Participant Distributions (if any)
Small/Large Employer Fully Insured
8/1/12, 8/1/13, 9/1/14 Part. Distributions w/in
90 days Both
New Notice of HIPAA Privacy Practices Self-Insured Plans 9/23/13 Both

21
“Play or Pay” Section 4980H Basics
Large employers are required to offer coverage to full-time employees (and dependents*) or pay a penalty/excise tax
Defines who is a full-time employee and when they must be offered coverage
• Eligibility Definition
• Eligibility Determination
• Waiting Period
Defines acceptable Employer Coverage as that which has “Minimum Value” and is “Affordable”
*Employers are required to offer coverage to dependent children; however, employers are not required to contribute to coverage for dependent children

22
“Play or Pay” Section 4980H Large ER Full-Time EE Determination
▲ Full-time = 30 hours/week average (130 hours/month)
— Hours of service include PTO, vacation, sick time, leave etc.
— Hours of service must be “reasonably” calculated for certain positions
▲ If EE is expected to be full-time at the time of hire, they are
full-time for the purposes of 4980H
▲ What about variable hour and seasonal EEs?
— IRS acknowledges practical challenges in determining full-time status
on a monthly basis and is providing a more flexible approach
▲ IRS Safe Harbor allows for ERs to use a look back approach
(“Measurement Period”) to determine full-time status for
subsequent predetermined “Stability Period”

23
4980H Full-Time EE Determination Ongoing Employees
▲ ERs define Standard Measurement Period (SMP) to determine if ongoing EEs were FT (30 hrs. per service week/130 hrs. per mo.)
— SMP can range from 3 to 12 months
▲ If ongoing EE was FT during the SMP, they must be considered FT for the entire Stability Period (SP)
— Formula used is total hours worked in SMP divided by months in the MP ≥ 130 hours
— If ≥ 130 hours, ER must offer EE coverage for entire SP or face penalty
— SP must be at least 6 months, but not shorter than the SMP
▲ If ongoing EE was not FT during the SMP, they would not be considered FT for the entire SP
— SP cannot be longer than SMP
▲ Administrative Period (AP) allowed (up to 90 days) to calculate FT status; however, AP cannot create a “gap if covered”
▲ Allows different MPs & SPs to be used for different EE classifications (hourly vs. salary, CBA/non-CBA, different states)

24
4980H Full-Time EE Determination New Variable Hour/Seasonal EEs
▲ ERs may use same look-back (Measurement Period)/ Stability Period approach with a few differences
▲ “Initial Measurement Period” (IMP) allowed for any new Variable Hour EE if ER cannot reasonably determine if they are expected to work more than 30 hours per week
— After Date of Hire, IMP can range from 3 to 12 months
▲ If Variable Hour EE was FT during the IMP, the EE must be considered FT for the entire Stability Period (SP)
— ISP must be at least 6 months, but not shorter than the IMP
▲ If Variable Hour EE was not FT during the IMP, they would not be considered FT for the entire SP
— SP cannot be longer than the IMP + 1 month and cannot exceed the end of the SMP + AP (90 days)
▲ Administrative Period (AP) allowed (up to 90 days) on both front end and/or back end of IMP to calculate FT status
— However, the IMP and AP together cannot extend beyond last day of the first month beginning on or after the anniversary of the EE’s start date
▲ Once Variable Hour EE has been employed for one full SMP, they must be retested as a ongoing EE

25
4980H Full-Time EE Determination Example

26
ACA Employer Penalties
▲ In general, failure to comply can result in excise tax under the Internal Revenue Code or penalties under PHSA or ERISA, depending on which of these statutes is applicable to the employer – $100/day “with respect to each individual
to whom such failure relates”
– Maximum for unintentional failure is the lesser of: • 10% of the total spent of the group health
plan for preceding year; or
• $500,000

27
DOL Plan Audits
▲ DOL Plan Audit Program is underway
▲ Because there is no history of audits, health and welfare plan compliance is often lacking
▲ Auditors looking at historic areas of non-compliance in plan documentation
▲ Review also encompasses ACA-required provisions

____ __ ____ _____ ____ ______ _______
28
Plan Design Requirements and Select Provisions

29
Cost-sharing Limitations
Deductible Limits
• $2,000/$4,000
• Non-GF Small Group Plans
Cost Sharing
Limits
• Pegged to IRS CDHP OOP Limits ($6,250/$12,500 for 2013)
• Non-GF Individual, Small Group Large Group, and Self-insured Plans

30
Essential Health Benefits (EHB) Basics
▲ Fully insured, non-GF small group and individual plans must cover all EHB w/o an annual or lifetime dollar caps on EHB
▲ Fully insured large group and self-insured plans are not required to cover EHB, but if they do so are prohibited from imposing any annual or lifetime dollar caps on EHB
▲ ACA-defined 10 EHB Categories:
1 Ambulatory patient
services
2 Emergency services
3 Hospitalization
4 Mental health and substance abuse
disorders/behavioral health treatment
5 Maternity and newborn care
6 Prescription drugs
7 Rehabilitative
services/devices
8 Laboratory services
9 Preventive and
wellness services and chronic disease
management
10 Pediatric services,
incl. oral and vision care

31
Essential Health Benefits Defining Covered Items & Services
▲ DHHS authorized states to define EHB through establishment of a benchmark plan
▲ States may choose from four existing health plan options for benchmark plan to establish the covered items/services within each EHB category : • Largest plan by enrollment in any of the three largest small group products • Any of the largest three state employee health benefit plans by enrollment • Any of the largest three federal employee health plan options by
enrollment • Largest insured commercial non-Medicaid HMO operating in the state
▲ State mandates associated with the selected benchmark plan will be included in the EHB package
▲ If State does not select a benchmark plan, default option will be largest small group product in the state

32
Essential Health Benefits Plans Effected ▲ Effective for plans beginning on or after 1/1/14
* Large group = 51+ in all states currently (will be 101+ in all states as of 1/1/16)
Plan/Funding Type
Grandfather Status
Must Cover EHBs?
Defines EHB Annual Lifetime Limits on EHB
Permitted?
Individual and Fully Insured Small Group
Non-GF Yes State No
GF No State No
Fully Insured Large Group
Non-GF No Employer No
GF No Employer No
ASO Small Group and Large Group
Non-GF No Employer No
GF No Employer No

33
Other Plan Design & Coverage Requirements ▲ Contraceptive Services Requirements
• Exemptions for Religious Employers
• Accommodations for Religious Affiliated Organizations
▲ 90-day Waiting Period Limit
▲ Required Coverage for Participants in Clinical Trials • Cannot deny a qualified individual the right to participate in an approved
clinical trial
• Cannot limit or impose additional conditions on coverage of routine patient costs for items and services furnished in connection with the approved clinical trial
• Cannot discriminate against a qualified individual based on participation in an approved clinical trial
▲ Non-discrimination Rules for Fully Insured Health Plans • Expected to closely follow IRS Section 105H Rules for self-insured plans

34
Non-discriminatory Wellness Programs Proposed Regulations
▲ Explains differences in types of incentive based wellness programs (participatory vs. health factor)
▲ Increases permissible incentive (penalty) for health factor contingent wellness programs
▲ 2014―permissible incentive increased to 30% of cost of coverage (up to 50% for tobacco cessation standards)
▲ Health factor contingent wellness programs must meet revised non-discrimination requirements
— Reasonably designed — Include annual opportunity to comply — Provide “reasonable alternative” standard for participants
• Not clear if “reasonable alternative” is medically driven
▲ Aggressive programs must comply with ADA, HIPAA & GINA
▲ Wellness programs that are not contingent on a health factor have more flexibility w/ incentives

____ __ ____ _____ ____ ______ _______
35
Employer Obligations

36
“Play or Pay” Section 4980H Basics
Large employers are required to offer coverage to full-time employees (and dependents*) or pay a penalty/excise tax
Defines who is a full-time employee and when they must be offered coverage
• Eligibility Definition
• Eligibility Determination
• Waiting Period
Defines acceptable Employer Coverage as that which has “Minimum Value” and is “Affordable”
*Employers are required to offer coverage to dependent children; however, employers are not required to contribute to coverage for dependent children

37
“Play or Pay” Section 4980H Large Employer Determination ▲ Large Employer
• Defined as employer that averaged at least 50 full-time employees during prior calendar year Transition rule 2014―employers may
use any consecutive 6 mo. period from 2013
• To calculate full-time employees: Add number of full‐time employees
(30 or more hours a week) and number of full‐time equivalent employees (FTEs)
Divide total monthly part time hours by 120
▲ Must include all full‐time employees and FTEs in “controlled group” to determine if Large Employer (but penalty applies on member‐by-member [separate tax ID] basis)

38
“Play or Pay” Section 4980H Large ER Full-Time EE Determination
▲ Full-time = 30 hours/week average (130 hours/month) • Hours of service include PTO, vacation, sick time, leave etc.
• Hours of service must be “reasonably” calculated for certain positions
▲ If employee is expected to be full-time at the time of hire then they are full-time for the purposes of 4980H
▲ What about variable hour and seasonal employees? • IRS acknowledges practical challenges in determining full-time status
on a monthly basis and is providing a more flexible approach
▲ IRS Safe Harbor allows for employers to use a look back approach (“Measurement Period”) to determine full-time status for subsequent predetermined “Stability Period”

39
“Play or Pay” 4980H Large Employer Requirements
▲ Must offer Minimum Essential Coverage to all full-time employees
– Employer subject to a penalty for failure to do so if any single full time employee receives federal premium tax credit (“assistance”) to purchase coverage through a qualified exchange
– $2,000 penalty for each full-time employee (minus first 30 EEs)
▲ Minimum Essential Coverage must provide “Minimum Value” and be “Affordable”
— Employer is subject to a penalty of the lesser of the $2,000 coverage penalty OR $3,000 for each full-time employee receiving a federal premium tax credit (assistance) to purchase coverage through a qualified exchange
▲ Employer penalties are triggered if employee(s) receive federal premium tax credit (assistance) for coverage through a qualified exchange ▲ Only apply to full time employees (defined as those working
30 hours per week or more)

40
“Play or Pay” Section 4980H Employer Requirements
Potential Annual Penalties Beginning in 2015 for Large Employers Applies to For-profit and Nonprofit Organizations
Not a large employer (Fewer than 50 full-time equivalent employees)
Large employer: 50 or more full-time equivalent employees
Does not offer coverage Does not offer coverage Offers coverage
A No full-time
employees receive credits for
exchange coverage
B 1 or more full-time employees receive
credits for exchange coverage
C No full-time
employees receive credits for
exchange coverage
D 1 or more full-time employees receive
credits for exchange coverage
No penalty No penalty Number of full-time employees minus 30 multiplied by $2,000
No penalty Lesser of: • Number of full-time
employees minus 30, multiplied by $2,000.
• Number of full-time employees who receive credits for exchange coverage, multiplied by $3,000.

41
4980H Full-Time EE Determination Ongoing Employees ▲ Employers define Standard Measurement Period (SMP)
to determine if ongoing employees were full-time status (30 hrs. per service week/130 hrs. per mo.) • SMP can range from 3 to 12 months
▲ If ongoing employee was full-time status during the SMP, then they must be considered full-time status for the entire Stability Period (SP) • Formula used is total hours worked in SMP divided by months
in the MP ≥ 130 hours • If ≥ 130 hours, employer must offer EE coverage for entire SP
or face penalty • SP must be at least 6 months but not shorter than the SMP
▲ If ongoing employee was not full-time status during the SMP, then they would not be considered full-time status for the entire SP • SP cannot be longer than SMP
▲ Administrative Period (AP) allowed (up to 90 days) to calculate FT status; however, AP cannot create a “gap if covered”
▲ Allows different MPs & SPs to be used for different employee classifications (hourly vs. salary, CBA/non-CBA, different states)

42
4980H Full-Time EE Determination New Variable Hour/Seasonal EEs
▲ Employers may use same look-back (Measurement Period)/ Stability Period approach with a few differences
▲ “Initial Measurement Period” (IMP) allowed for any new Variable Hour Employee if employer cannot reasonable determine if they are expected to work more than 30 hrs. per week • After Date of Hire, IMP can range from 3 to 12 months
▲ If Variable Hour Employee was full-time status during the IMP, then the EE must be considered full-time for the entire Stability Period (SP) • ISP must be at least 6 months but not shorter than the IMP
▲ If Variable Hour Employee was not full-time status during the IMP, then they would not be considered full-time status for the entire SP • SP cannot be longer than the IMP + 1 month and cannot
exceed the end of the SMP + AP (90 days) ▲ Administrative Period (AP) allowed (up to 90 days) on both front
end and/or back end of IMP to calculate the full-time status • However, the IMP and AP together cannot extend beyond
last day of the first month beginning on or after the anniversary of the EEs start date
▲ Once Variable Hour Employee has been employed for one full SMP they must be retested as a ongoing employee

43
Large ER Requirements 4980H Minimum Value Determination ▲ Minimum Value―Plan’s share of the total allowed costs of benefits
provided under the plan ≥ 60%
▲ Employers may select from three methodologies for determining Minimum Value of Plan • Minimum Value Calculator
• Plan Design Checklist Safe Harbor
• Certification by certified actuary
▲ Employer HSA contributions & HRA contributions newly made available count toward Plan’s Minimum Value
▲ 60% Minimum Value requirement based only on Essential Health Benefits*
* Note: Large group and self-insured employer plan sponsors are not required to cover specific EHB and it appears MV
calculation is based all covered benefits

44
Large ER Requirements 4980H Affordable ER Coverage Determination
▲ ACA and Subsequent Federal Regulations/Guidance define “affordable” employer coverage as: • Single (Self-only) coverage costing employee no more than 9.5% of
income
• IRS Safe Harbor allows employers to base affordability on employee W-2 income. For example:
FT Employee earning $20,000 year;
Employer could not charge EE more than $1,900 year ($158 mo.) for Single (Self-only) coverage
▲ Employees w/o access to affordable ER coverage may be eligible for federal Premium Tax Credits & Subsidies (Households @ 100%-400% FPL)

45
“Play or Pay” Section 4980H Miscellaneous
▲ Under the proposed regulations’ transition relief, solely for purposes of stability periods beginning in 2014, employers may adopt a transition measurement period that: • Is shorter than 12 months, but not less than 6 months long; and
• Begins no later than July 1, 2013, and ends no earlier than 90 days before the first day of the first plan year beginning on or after Jan. 1, 2014.
▲ Proposed regulations provide allowances to use standard payroll periods for the purposes of Measurement Period calculations with exception

46
“Play or Pay” Section 4980H Miscellaneous
▲ Authorized Safe Harbor / “95% Rule”: • Employer complies with 4980H if it
offers Minimum Essential Coverage to at least 95% of full-time employees (and dependents)
▲ Dependent coverage requirement: Must provide coverage to children of full-time employees under age 26 • No penalty in 2014 if employer takes
steps toward compliance
▲ Fiscal year plans: Employers will not be subject to 4980H penalties until the first day of the 2015 plan year.
▲ Common Law Employer standard used to determine employer -employee relationship

____ __ ____ _____ ____ ______ _______
47
Premium Tax Credits and Cost Sharing Subsidies

48
Premium Tax Credits & Subsidies Why They Matter to Employers
▲ Premium Tax Credits and Cost-Sharing Subsides are available to households with low to moderate incomes (100%-400% FPL) if they meet eligibility requirements
▲ Low- to middle-income employees (households) may have more affordable coverage options through a Public Exchange due to these Insurance Affordability Programs
▲ Premiums Tax Credits
– Households w/ incomes b/t 100%-400% FPL eligible for advanceable tax-credits capping premiums for a 70% “Silver Plan” at 2% to 9.5% of modified adjusted gross household income
• 133%-400% threshold in states that enact Medicaid expansion
▲ Cost Sharing Subsides
– Households w/ incomes b/t 100% to 250% FPL are eligible for additional cost sharing subsides
• Increase the actuarial value of the Silver Plans to greater than 70%

49
Premium Tax Credits/Subsidies Why They Matter to Large Employers ▲ If employee is offered affordable
coverage by employer, they are not eligible for Premium Tax Credits/ Subsidies through Public Exchange for both self/dependents
▲ If employer does not offer affordable coverage, EEs may be eligible for Premium Tax Credits/ Subsidies for self/dependents
▲ The eligibility requirements for Premium Tax Credit/Subsidy appear to create an incentive for employers to make coverage less affordable for certain lower-wage employees so they can qualify

50
Premium Tax Credit Cost Analysis EE w/ Family Example
ER EE
EE 395.69$ 336.34$ 59.35$
EE+Sp 791.39$ 474.83$ 316.55$
EE+Ch 791.39$ 474.83$ 316.55$
Fam 1,187.08$ 712.25$ 474.83$
ER EE
EE 395.69$ 218.62$ 54.84$
EE+Sp 791.39$ 308.64$ 292.50$
EE+Ch 791.39$ 308.64$ 292.50$
Fam 1,187.08$ 462.96$ 438.74$
Family Income FPL % of income Cap
35,137 150% 4%
46,850 200% 6.3%
70,275 300% 9.5%
93,700 399% 9.5%
Cost w/o affordable ESI ER EE EE Savings 192.78$
250.00$ 245.96$ ER Savings 212.96$
EE Unaffordable Threshold (9.5%)
278.17$
370.90$
556.34$
741.79$
Cost ESI (80/20 Plan)
Tax Adjusted Cost ESI
Premium Cap (Mo.)
117.12$
EE+Child
245.96$
556.34$
741.79$

51
Tax Credits/Subsidies Why They Matter to Individuals PPACA Premium and Cost-Sharing Subsidy
PREMIUM SUBSIDY COST-SHARING SUBSIDY³
INCOME (%PPL)
ANNUAL INCOME (BASED ON TRENDED
2014 FPL¹)
PREMIUM PERCENT OF INCOME CAP²
MONTHLY MAXIMUM PREMIUM
REDUCTION IN MAXIMUM OOP LIMIT
REDUCED MAXIMUM ANNUAL LIMITATION OF COST SHARING (2014)
REQUIRED ACTUARIAL VALUE OF
BENEFIT PLAN
<133% $15,455 2.00% $26 66.70% $2,250 94%
150% $17,430 4.00% $58 66.70% $2,250 87%
200% $23,240 6.30% $122 20.00% $5,200 73%
250% $29,050 8.05% $195 N/A $6,400⁴ 70%
300% $38,860 9.50% $276 N/A $6,400* 70%
400% $46,480 9.50% $386 N/A $6,400* 70%
1. Based on 2012 100% FPL of $11,170 for a single individual, trended two years at 2% annual trend (rounded). 2. Premium tax credit percentages are for 2014 and will be indexed in the future. 3. Excluding cost-sharing reductions for Indians with household income not more than 300% FPL of proposed rule for cost-sharing reductions 4. HHS estimated 2014 maximum annual limitation on cost sharing. For future years, will be based on IRS dollar limit on cost sharing for high-deductible plans..

52
Tax Credits/Subsidies Considerations ▲ Most employers offer affordable self-only coverage, would they
adjust contributions to allow certain workers eligibility for premium tax credits and subsidies?
▲ Is it appropriate for an employer to drive lower wage workers to the exchanges to qualify for these programs? • Sustainability • Public relations aspect • Will increased pay be required for those who don’t qualify for these
programs be required to offset higher employee premium contributions
▲ Many questions and uncertainties exist about these insurance affordability programs
▲ Will the premium tax credits/subsidies be scaled back in 2014 and beyond?
▲ Legal challenges to premium tax credits/subsidies through federal exchanges?

____ __ ____ _____ ____ ______ _______
53
Health Insurance Exchanges

54
Qualified Health Insurance Exchanges
Medicaid & CHIP Insurance Affordability Programs: Subsidized
Coverage - Premium Tax Credits & Cost Sharing
Subsidies
Unsubsidized Coverage SHOP/Small Group ER Coverage
< 100%/133% FPL (state option) including adults
100%/133% - 400% FPL w/out affordable ESI
> 400% FPL ERs < 50/100 (state option)
Carriers Products Plan Types Actuarial Value
Cigna Aetna Kaiser BC/BS
Etc.
HMO PPO POS
Co-Op Plans State Basic Health Plan
Platinum Gold Silver
Bronze Catastrophic Plan (≤30)
90% 80% 70% 60% N/A
Product Choices
Programs
Exchanges
Federal State Partnership (Federal + State)

55
Health Insurance Exchange State Progress & Federal Defaults

____ __ ____ _____ ____ ______ _______
56
Emerging Healthcare Models for Employers and Employees

57
Emerging Models Employer/Employee Health Coverage
POPULATION HEALTH & RISK MANAGEMENT
MARKETPLACE APPROACH
• Self-insured models
• Wellness programs that actually achieve behavior change
• Incentives and penalties (ACA increases wellness allowance to 30%)
• Value-based benefit design
• Multi-purchasing Coalitions, Value-Based Networks, Patient-Centered Medical Home Models
– Direct contracting for larger self-insured employers
• Market alternatives exist
– GI & No Pre-Ex
– Exchanges (Public & Private)
• Defined Contribution Model
• Reallocation of compensation & benefits spend based on best available options
– Leverage Premium Tax Credits & Subsides
• Stability of non-large group market in question!

58
Guess What? It’s Still About Rising Health Care Costs

59
Health Care Strategy Fundamentals
Employee Education/ Communication Campaign on Health Care Costs & Quality!
Population Health Management
Delivery System Strategies
• Total Rewards Conversation
• Value-Based Benefit Design
• Keep healthy members healthy!
• Keep those with costly health issues compliant and from getting worse!
• Incentives/ Penalties
• Carrier programs are very limited/ that’s not enough
• Population Health Management within your organization is up to you!
• Centers of Excellence
• Focus/ Narrow Networks
• Pay for Performance Initiatives
• Patient-Centered Medical Home/ ACO’s
• On-site Clinics
• Tele-Medicine

60
Defined Contribution Approach Through Public/Private Exchange DEFINED CONTRIBUTION
SUBSIDY INSURED PLAN OFFERINGS FOR PARTICIPANTS
THROUGH EXCHANGE (Public or Private)
1 2 3
Health Care Credit Standardized Plans Competing Carriers
Employer makes a defined contribution per month
Bronze -60% Silver-70% Gold-80%
Platinum-90%
Aetna Cigna
United Kaiser
▲ Many questions remain about this model ▲ Group or Individual products ▲ Employer tax deduction/employee tax
deduction status in question ▲ What does it do to impact underlying health
care costs?

61
Modeling Coverage Scenarios Impact on Employer & Employee Costs Potential Employer Scenarios Employer Costs Employee
Expenses
Status Quo • Maintain current ER plan • Continue to treat all benefit-eligible EEs the same • Employer costs are plan costs less EE contributions
Employer Plan
Cost-sharing
EE contributions
Encourage Exchanges for Certain EEs • Maintain current ER Plan for certain EEs • Steer EE’s to most cost-effective coverage source • Employer costs are combination of plan costs less EE
contributions, 4980H taxes/fees, possible increased EE compensation for higher-income EEs (+400% FPL)
Employer Plan Cost-sharing
EE contributions
PPACA Fees Subsidies
Exit Completely • Terminate current ER plan • Increase EE compensation or use “Defined Contribution”
strategy & allow EEs to purchase individual coverage through Public Exchange, Private Exchange, or off exchange
• Employer costs are combination of 4980H taxes/fees & defined contribution/increased EE compensation
Increased Compensation
Cost-sharing
PPACA Fees Subsidies

____ __ ____ _____ ____ ______ _______
62
Additional Resources

63
Additional Resources
▲ Kaiser Family Foundation www.kff.org
▲ Federal Government HCR Website www.healthcare.gov
▲ Health Insurance Tax Credit Calculator http://healthreform.kff.org/subsidycalculator.aspx
▲ California Health Insurance Exchange Website www.CoveredCa.com Contact: Erika James, Vice President, Employee Benefits Ascension Benefits & Insurance Solutions 925-407-0416 [email protected]

64
We appreciate the work you do …
Thank You!