
National level survey relevant to health seminar (2)
45
NATIONAL LEVEL SURVEYS RELEVANT TO HEALTH Presenter: Dr. Vishal Moderator: Dr. Jugal Kishore
-
Upload
vishal-soyam -
Category
Technology
-
view
454 -
download
1
Transcript of National level survey relevant to health seminar (2)
NATIONAL LEVEL SURVEYS RELEVANT TO HEALTH
Presenter: Dr. VishalModerator: Dr. Jugal Kishore

PLAN OF PRESENTATIONSURVEY-DEFINITIONPURPOSE OF SURVEYTYPES OF SURVEYIMPORTANT NATIONAL LEVEL
SURVEYS• CENSUS• NFHS• DLHS• SRS• AHS
WHAT IS SURVEY?????? Is an epidemiological investigation undertaken to
examine certain selected features of a community, with a view to work out the frequency (either incidence or prevalence), of diseases or health related phenomena, and their distribution related to time, place and person, by obtaining information from a sample drawn from the population of interest.
PURPOSE OF SURVEY To generate information about the health status and
related aspects.
Provide general socio - demographic and basic health data for planning and organizing the health services or to make a community diagnosis.
To estimate the frequency (incidence or prevalence) of important diseases.
PURPOSE OF SURVEYTo evaluate the effectiveness of a health program, eg.
immunization program.
To assess the availability and accessibility of health care facilities.
To assess local beliefs, behaviour patterns, customs and awareness about health / risk factors as well as attitudes towards health services.

TYPES OF SURVEY
CROSS SECTIONAL SURVEY
LONGITUDINAL SURVEY
HYBRID SURVEY
HOW TO CONDUCT SURVEY????? Clearly define the survey objective “What you want to learn” ???
Determine your sample “Whom you will interview” ???
Choose interviewing methodology “How you will interview” ???
Create your questionnaire “What you will ask” ???
HOW TO CONDUCT SURVEY?????
Pre-test the questionnaire Test the questions Data collection Ask the questions Analyze the data – Produce the reports
Important National Level Survey
CENSUS NFHS DLHS SRS AHS
CENSUS
Census : An official count of a population carried
out at set intervals.
Population census: is the total process of collecting,
compiling, evaluating, analysing and publishing or
otherwise disseminating demographic, economic and
social data pertaining, at a specified time.
Census is : about you, by you and for you
Our Census ,Our future
WHY CENSUS IS IMPORTANT??? The Indian Census is the most credible source of information
on Demography, Economic Activity, Literacy and Education, Housing & Household Amenities, Urbanisation, Fertility and Mortality, Scheduled Castes and Scheduled Tribes, Language, Religion, Migration, Disability and many other socio-cultural data.
This is the only source of primary data in the village, town and ward level.
WHY CENSUS IS IMPORTANT??? Census is the basis for reviewing the country's
progress in the past decade, monitoring the on going Schemes of the Government and most importantly, plan for the future.
Provides a basic frame for conduct of other surveys.
Key Features
The recently concluded Census 2011 was the 15th
National Census of the Country in the unbroken
series since 1872 and the seventh after Independence.
The responsibility of conducting the decennial
Census rests with the Office of the Registrar General
and Census Commissioner, India (ORGI).
Census is a joint effort by the Union and State
Governments in India. Under the Census Act, 1948
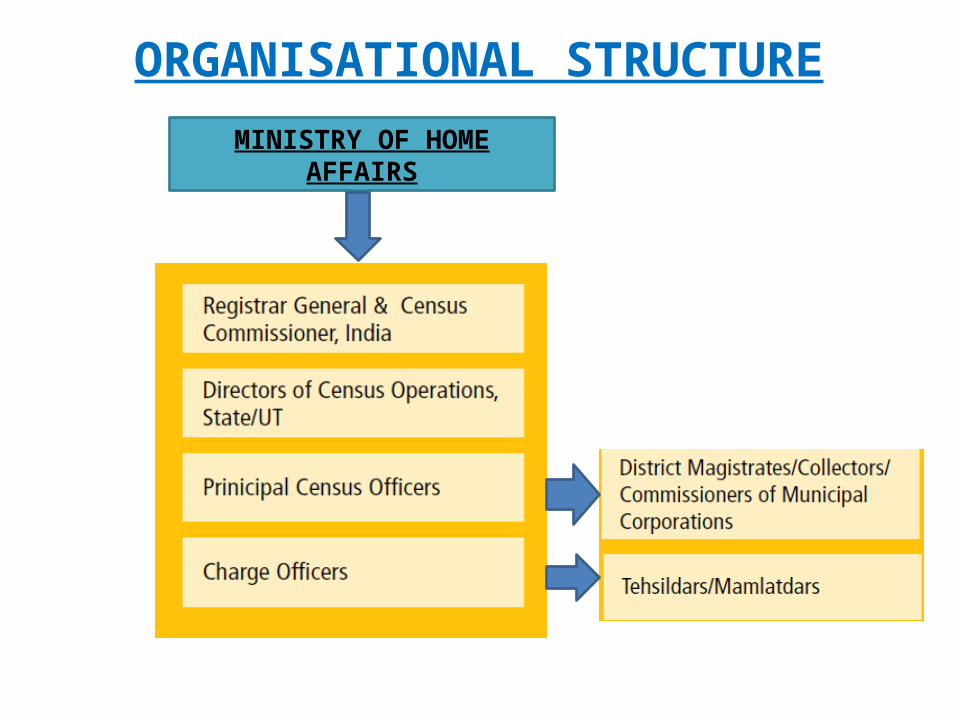
ORGANISATIONAL STRUCTUREMINISTRY OF HOME
AFFAIRS
METHODOLOGY
• Conducted once in a decade,• An extended de facto canvasser method TWO PHASES:
First phase:
Each building, house and other structures were systematically listed and numbered. Useful data on the amenities available to the households as well as the assets owned
were collected.
Second phase: The Population Enumeration exercise was held throughout the country for period of
3 weeks. Enumerators visit the households for collecting information on every person living
in the house. On the night of 3rd week the Houseless population is enumerated.
Revision Round
Strengths Covering not only the settled population but also homeless
persons and nomadic groups.
Allow analysis in terms of statistics on persons and households and for a wide variety of geographical units, ranging from the country as a whole to individual small localities or city blocks.
Many new initiatives introduced eg. Video conferencing, social networking site
The average cost of Census taking in the world is estimated as $ 4.6 per person. In India, the cost was less than $ 0.5 per person in Census 2011.
WHY NATIONAL LEVEL SAMPLE SURVEY???
Need of demographic and health related data for annual and five year planning.
The period between two census is quite large.
For periodic evaluation of various policies and national health programme.
Comparison
NFHSNFHS surveys are conducted under the
stewardship of MoHFW
IIPS is the nodal agency for the National Family
Health Surveys
NFHS covered around 99 % population of
country

GOALS To provide essential data on health and family
welfare needed by the MOHFW & other agencies for policy and program purposes.
To provide information on important emerging health and family welfare issues.
OBJECTIVE • To provide National and state estimates of fertility, Family planning, infant and child mortality, Reproductive and child health Nutrition of women and children Quality of health and family welfare services
socioeconomic conditions

Year Region & Population included
Health Issues covered
NFHS 1 1992-1993 89,777 ever married women age 13-49In 24 states and Delhi
1. Indicator on family welfare2. Maternal and child Health3. Nutrition
NFHS 2 1998-1999 91,000 ever married women age 15-49In 26 states and Delhi
1. NFHS 1 Issue2. Reproductive Health problem3. The status of women & domestic
violence4. Anthropometric measurement
extended to ever married women5. Hb estimation, lead content, iodine
content
NFHS 3 2005-2006 1,24,385 ever married women age 15-49.74,369 Men age 15-54In 29 states and Delhi - Never married women age 15-49
1. NFHS 1 + NFHS 2 issue2. Perinatal mortality3. Male involvement 4. Adolescent reproductive health5. High risk sexual behaviour, safe inj.6. Family life education7. Knowledge about TB8. Blood testing for HIV
Contd… Sample size calculation: The target sample size for NFHS
in each state was estimated in terms of the number of ever-married women in the reproductive age group to be interviewed.
• 4000 completed interview = more than 30 million• 3,000 completed interviews = between 5 and 30 million• 1,500 completed interviews = less than 5 million
• In addition, sample-size adjustments was made to meet the need for HIV prevalence estimates for the high HIV prevalence states and UP and for slum and non-slum estimates in eight selected cities.
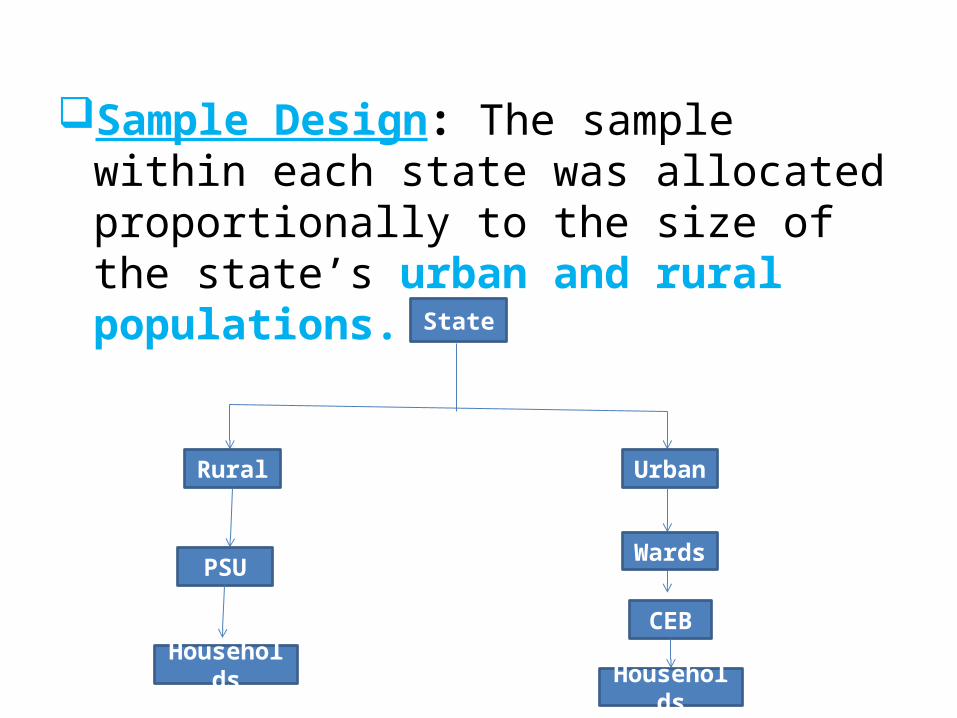
Sample Design: The sample within each state was allocated proportionally to the size of the state’s urban and rural populations.
State
Rural Urban
PSU
Households
Wards
CEB
Households
Sample selection: the Census list of villages and wards served as the sampling frame.
Stratification:• The first level of stratification was geographic.• Further stratified using selected variables from the
following list: village size, percentage of males working in the non-agricultural sector, percentage of the population belonging to scheduled castes or scheduled tribes, and female literacy.
• HIV prevalence state - ‘High’, ‘Medium’ or ‘Low’, as estimated for all the districts was used for stratification .
• Three types of questionnaires: Household Questionnaire, Woman’s Questionnaire and Village Questionnaire. • For each state and at national level three data files are
associated with these questionnaires. Also available are data files with information on children born during the three years preceding the survey along with mother's basic characteristics.
• Data files are available in user-friendly formats for SPSS, SAS, and STATA users. Data files are available in three formats: the flat format, the rectangular format and the hierarchical format.
STRENGTHS Random sampling improve the external validity.
Validated questionnaires and trained manpower with good supervision.
Wide range of health information was collected –IMR, contraception, immunization, anemia, breast feeding and HIV exposure.
WEAKNESS
Sample did not include union territories.
HIV testing include only adult population leaving
most vulnerable group.
Large number of interviewers were recruited that may
have introduced interviewer bias.
HemoCue method overestimated Hb level as
compared to the standard Cyanmethemoglobin
method.
D L H S
Objective : of the survey was to estimate the service coverage of the following:
Ante Natal Care (ANC) and Immunization services Extent of safe deliveries Contraceptive prevalence Unmet need for family planning Awareness about RTI/STI and HIV/AIDS Utilization of government health services and users’
satisfaction
WHY DLHS???
The district being the basic nucleus of planning and
implementation, and for decentralize approach GoI
has been interested in generating district level data on
utilization of the services provided by government
health facilities.
To assess people’s perceptions on quality of
services. Therefore, it was decided to undertake the
DLHS under the RCH programme in the country.
District Level House Hold Survey (DLHS) Conducted by Indian Institute of Population Science ( IIPS)
Initiated in 1997 ( I: 98-99, II : 2002-04 and, III : 2007-08)
One of the largest ever demographic and health surveys carried out in India, with a sample size of about 1000-1500 hhs. per district
To provide estimate on important indicators on1. Maternal & Child Health 2. Family Planning & other reproductive health services.3. Important interventions of NRHM ( DLHS – III)
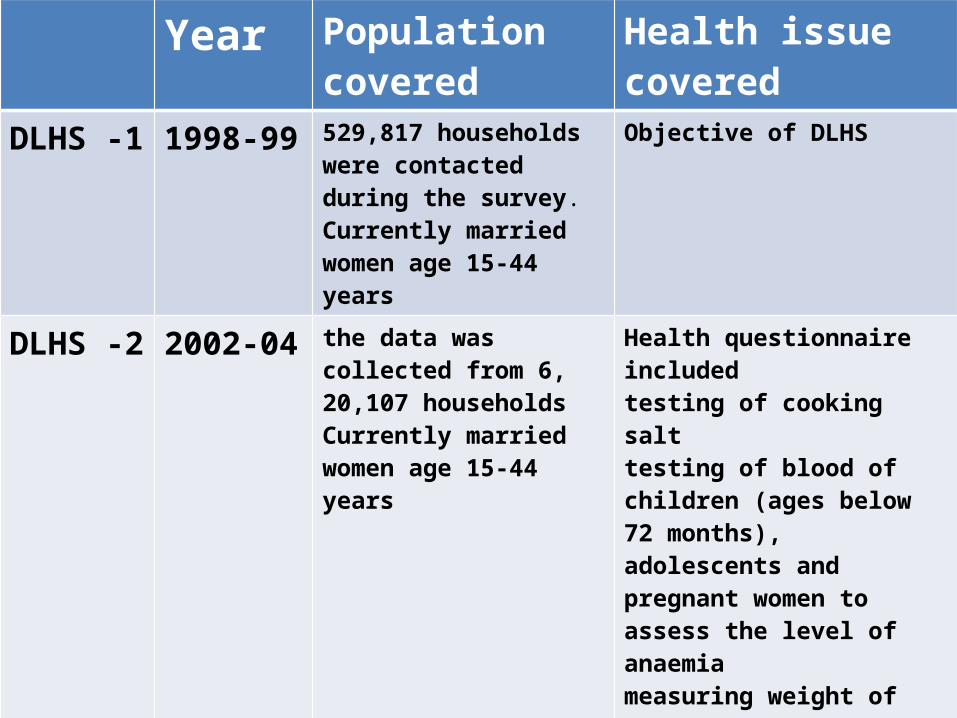
Year Population covered
Health issue covered
DLHS -1 1998-99 529,817 households were contacted during the survey.Currently married women age 15-44 years
Objective of DLHS
DLHS -2 2002-04 the data was collected from 6, 20,107 householdsCurrently married women age 15-44 years
Health questionnaire includedtesting of cooking salttesting of blood of children (ages below 72 months), adolescents and pregnant women to assess the level of anaemia measuring weight of children
DLHS -3 2007-08 7 lakh housholdsEver-married women (age 15-49).never married women (age 15-24)
-Population linked facility survey conducted-Assess the effectiveness of ASHA and JSY-Adolescent health problem
SURVEY DESIGN AND SAMPLE SIZE
• Systematic random sampling : was adopted for the selection of the districts for
PHASE1: districts within the state were arranged alphabetically, and starting at random from either first or second district, alternative districts were selected.
• Second phase : covered all the remaining districts of the country.
Survey Design and Sample Size
• In each of the selected districts, 50 Primary Sampling Units (PSUs), i.e. either villages or urban wards were selected adopting probability proportional to size (PPS) sampling. The village/ ward level population as per the previous census was used for this purpose
• The sample size for RHS-RCH was fixed at 1000 households with 20 households from each PSU. In order to take care of non-response due to various reasons, 10 percent over sampling was done.
• Further, all Sub-Centres and Primary Health Centres which were expected to serve the population of the selected Primary Sampling Units (PSUs) were also covered.
• Study tool: Household questionnaire and Woman’s questionnaire.
STRENGTHS Whole country covered under DLHS
Validated questionnaires and trained manpower with good supervision
Wide range of health information was collected –IMR, contraception, immunization, anemia, breast feeding and HIV exposure.
Along with individual data health facility services also assessed.
S R S
OBJECTIVE: Is to provide reliable estimates of birth rate,
death rate and infant mortality rate at the natural division level
for rural areas and at the State level for urban areas
Initiated on a pilot basis by the OFFICE OF THE REGISTRAR
GENERAL, INDIA in a few selected states in 1964-65, it
became fully operational during 1969-70 with about 3700
sample units
S R S• Continuous enumeration of births and deaths in selected
sample units by resident part time enumerators, generally
anganwadi workers & teachers, and an independent survey
every six months by full-time SRS supervisors.
• In rural areas : the sample unit is a village or a segment of it,
if the village population is 2000 or more.
• In urban areas: the sampling unit is a census enumeration
block with population ranging from 750 to 1000
S R S• Matching of data
• The unmatched and partially matched events are re-verified in
the field to get an unduplicated count of correct events.
• The advantage of this procedure, in addition to elimination of
errors of duplication, is that it leads to a quantitative
assessment of the sources of distortion in the two sets of
records making it a self-evaluating technique
A H S
OBJECTIVE: “ To yield benchmarks of core vital and health indicators at the district level and to map changes therein on an annual basis”
Scheme is sponsored by Ministry of Health & Family Welfare(MOHFW)
Largest Sample Survey in the World
N E E D F O R A H S9 AHS States namely, Rajasthan, Uttar Pradesh,
Uttarakhand, Bihar, Jharkhand, Orissa, Madhya Pradesh, Chhattisgarh and Assam constitute:
48 % of country’s Population 59 % of Births 70 % of Infant Deaths 75 % of Under 5 Deaths 62 % of Maternal DeathsThere is large inter-district variations in these
States.
KEY FEATURES
• Coverage- All the 284 districts of 8 EAG States and Assam
• Sample Units- 20,694 statistically selected sample units
(Census Enumeration Blocks in urban areas and Villages in
rural areas)
• Sample Population- About 18.2 million
• Sample Households- 3.6 million households
• Average Sample households per district- About 13 thousand
KEY FEATURES• Sample Size- District level sample size is based
on Infant Mortality Rate• Conduct of Field Work- Hybrid approach wherein
fieldwork has been outsourced and supervision done by the ORGI
• Third Party Audit- Third Party Audit was implemented under AHS to verify the correctness of data through an independent arrangement.
• This was over and above the regular supervision by ORGI
INDICATORS COVEREDCrude Birth Rate (CBR)
Crude Death Rate (CDR)
Infant Mortality Rate (IMR)
Neo-Natal Mortality Rate (NNMR)
Under Five Mortality Rate (U5MR)
Maternal Mortality Ratio (MMR)
Sex Ratio at Birth (SRB)
Sex Ratio (0-4 years)
Sex Ratio (All ages)
References• Comparison of HemoCue Method with Cyanmethemoglobin Method for
Estimation of Hemoglobin S.K. Kapoor* Umesh Kapil , sadanand et al.

45


















