
National Health Care Reform Overview Daniel B. McLaughlin Center for Health and Medical Affairs.
31
National Health Care Reform Overview Daniel B. McLaughlin Center for Health and Medical Affairs
Transcript of National Health Care Reform Overview Daniel B. McLaughlin Center for Health and Medical Affairs.

National Health Care Reform Overview
Daniel B. McLaughlin
Center for Health and Medical Affairs
The Best Health Care System in the World

The Best• Medical Research
• Drug and Device Development
• Innovative Care Delivery– Minute Clinic– Electronic Health Record– Health 2.0
• Health Services Research
• Passionate and skilled caregivers
• Engaged Consumers and Patients
Paradox• Geographic
Practice disparity
• Quality: over use, under use, misuse and safety
• Acute care model for Chronic disability
• Professions shortage– Primary care
– Nursing
• Emerging public health problems
• Access problems: uninsured, underinsured, bankruptcy
• Insurance: pre existing conditions, deductibles & co-pays, lifetime limits
• Welfare payment for aged and disabled
• Most costly system in the World – 17% of GDP

Federal Reform 2010
Reduce cost growth,Improve access, andImprove quality andsafety
In a way that is acceptable to the American Public
With Libertyand Justice for All
Health Care – A Systems View
Professional - Patient
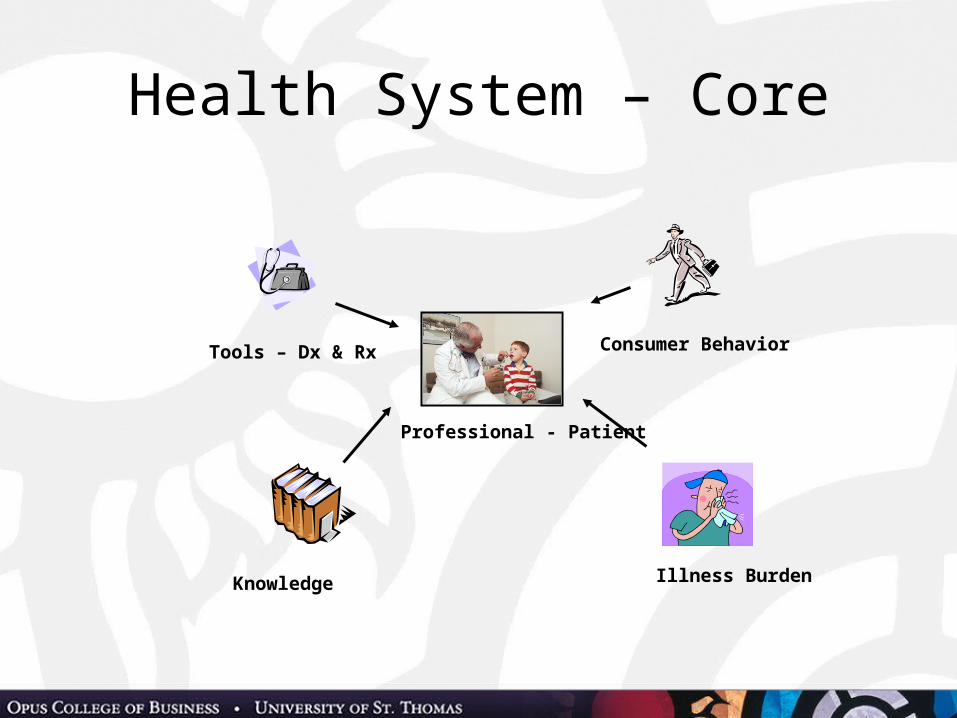
Health System – Core
Professional - Patient
Illness Burden
Consumer Behavior
Knowledge
Tools – Dx & Rx

Health System – Tools
Professional - Patient
Tools – Dx & Rx
Facilities
Medical Technology
Health Care Workers
Information Technology
Reform- $80 Billion in discounts over 10 years from drug companies + Medicaid rebates
The tradeoff – no direct negotiations with Medicare, extended patent protection
- Transparency on drug/device company relationships with providers
Reform$18 Billion for Health Information Technology (Stimulus bill)
Reform- Improved payment forprimary care services- More funding for training primary care providers
Reform: structureAccountable CareOrganizations
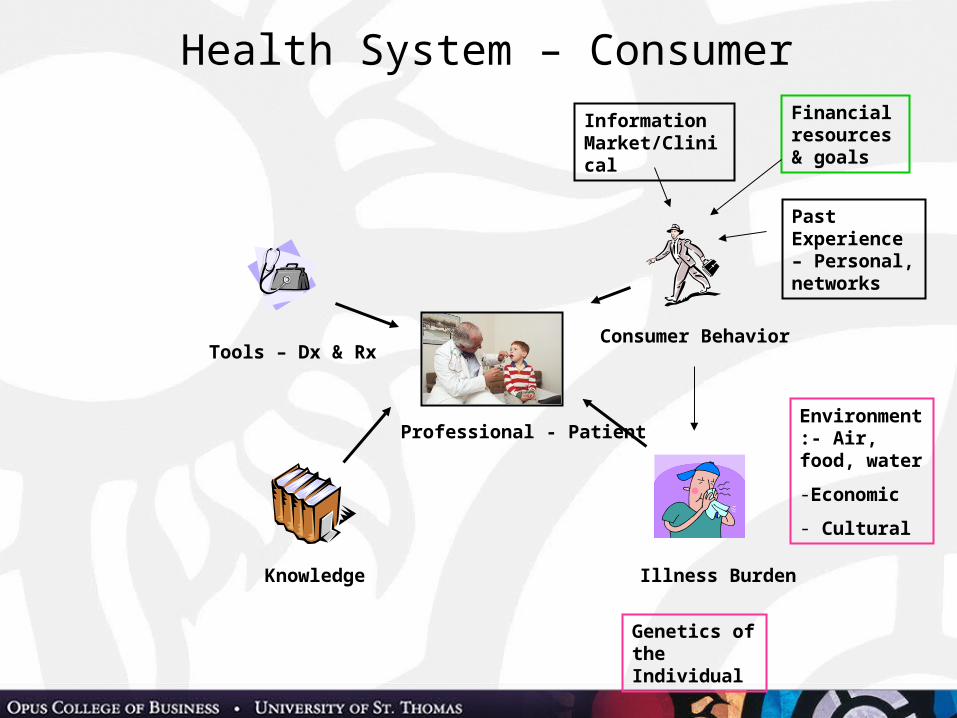
Health System – Consumer
Professional - Patient
Illness Burden
Consumer BehaviorTools – Dx & Rx
Past Experience – Personal, networks
Information Market/Clinical
Financial resources & goals
Knowledge
Environment:- Air, food, water
-Economic
- Cultural
Genetics of the Individual

Consumer Behavior and Illness
• Reform – Illness Burden – New funds and coverage for prevention – Payment for Chronic
Disease Management– Payment for Medical home– Payment for Health IT
to track chronic patients• Reform – Consumer behavior
– Increased payment for health promotion and disease prevention
– Medicare recipients get “health risk assessment”– Grants and tax incentives to employers for wellness
programs (Safeway model)– Tort reform pilots (Malpractice)
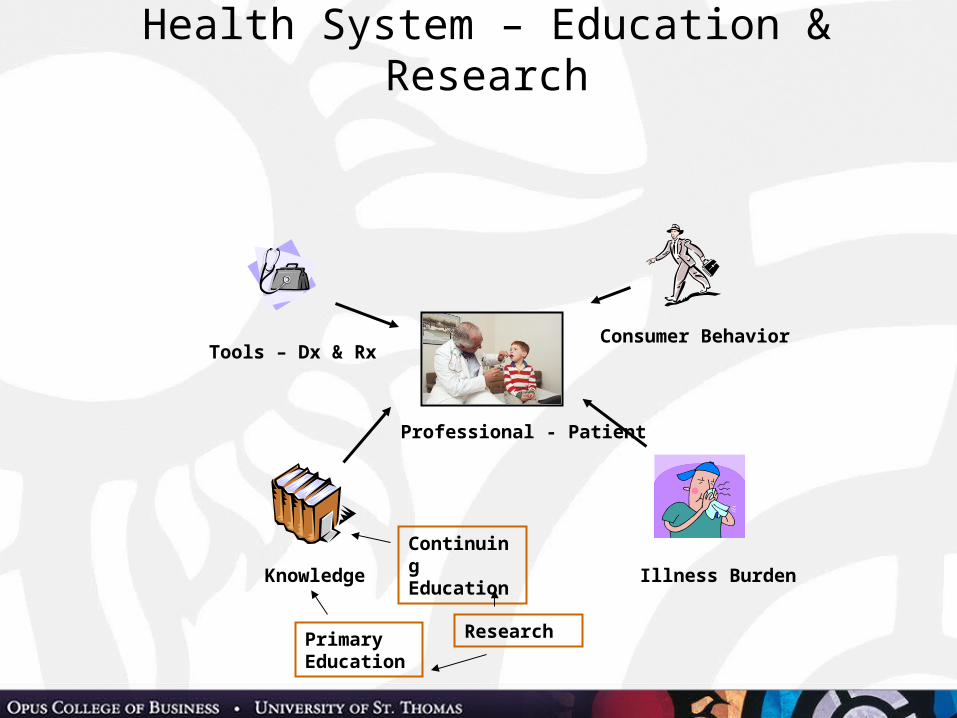
Health System – Education & Research
Professional - Patient
Illness Burden
Consumer Behavior
Knowledge
Tools – Dx & Rx
Primary Education
Continuing Education
Research
Education and Research
• Reform - Education– Revised Medicare funding for training to
emphasize primary care– Increased funding for nursing education
• Reform - Research– Funding for Comparative
Effectiveness Research (Stimulus)– Cannot be used to direct
payment policy
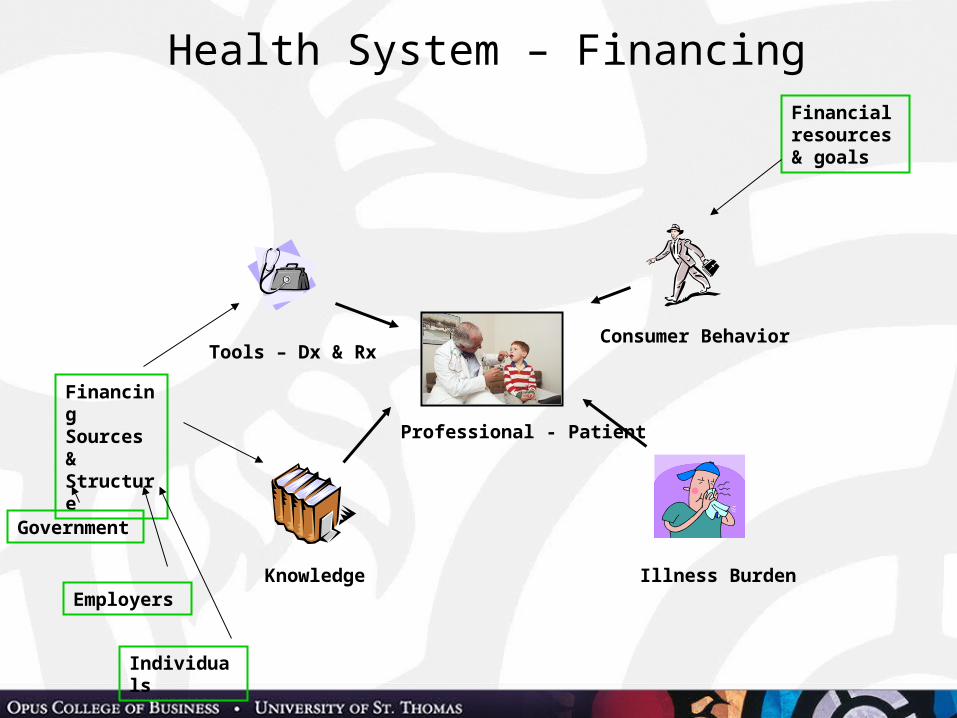
Health System – Financing
Professional - Patient
Illness Burden
Consumer Behavior
Knowledge
Tools – Dx & Rx
Financing Sources & Structure
Individuals
Employers
Government
Financial resources & goals
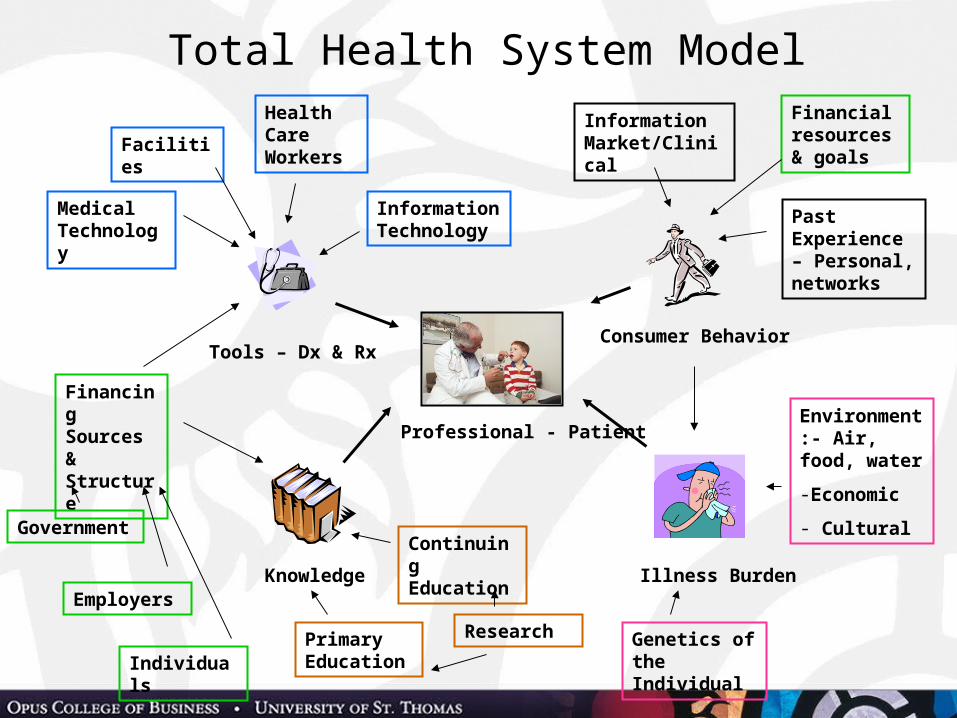
Total Health System Model
Professional - Patient
Illness Burden
Consumer Behavior
Knowledge
Tools – Dx & Rx
Facilities
Medical Technology
Health Care Workers
Financing Sources & Structure
Information Technology
Primary EducationIndividuals
Employers
GovernmentContinuing Education
Past Experience – Personal, networks
Information Market/Clinical
Genetics of the Individual
Environment:- Air, food, water
-Economic
- Cultural
Financial resources & goals
Research

Employers Remain Primary Sponsor of Coverage Distribution of 307 Million People by Primary Source of Coverage
EmployerDirect164m 53%
Uninsured49m16%
Medicare39m13%
Medicaid42m14%
Medicare41m13%
IndividualDirect14m 5%
EmployerDirect55m18%
Total Employer 164m (53%)Total Individual 14m (5%)
Source: The Lewin Group, The Path to a High Performance U.S. Health System: Technical Documentation (Washington, D.C.: The Lewin Group, 2009).
Insurance Reform• Mandates insurance: both
employers and individuals• Subsidies available for
both low income individuals and small business
• Expands Medicaid income limitsto 133% – state match held harmless
• Standardized benefit levels (Bronze – Platinum)• Eliminates pre existing condition, lifetime caps,
recissions and other insurance practices• HSAs still available• Simplified and standardized billing
The Exchange

FinancingMedicare
Advantage –Health Plans
Drug Discounts
Hospital Inflation (-1.5%), Re- admits, DSH
Personal Income Taxes> $250,000, 3.8% on unearned
income
System taxes: health plans, device
companies, tanning, Cadillac Health plans
Subsidies for individuals and small business
Medicaid eligibility buy
down
MD fees – repeal SGR
Fix Medicare donut hole
$ One Trillion
4% of total NHE1099s for
purchases > $600X
Bending the cost curveCompetition between Health Plans
Delivery system Substitution of lower priced care Inpatient, clinic, home Increased availability and use of primary care Improved chronic care (Medical home, ACO etc.) Reduced system costs (billing, overhead) Comparative effectiveness research Medicare Innovations Center
Consumers Prevention and Wellness and the Social Determinates of Health Tort Reform demonstrations Consumer Directed Health Care
Reform’s Impact on Stakeholders
Insurance Companies• Gain 30 million new customers• Cease most underwriting practices• Participate in state based insurance
exchanges• No change with large employers• Agree to standardization
– Benefits– Payment systems
• Overhead less than 20%, 15%• Become more retail and consumer
oriented
Government• Federal
– Enforce Insurance mandate– Implement new Medicare payment policies– Implement Insurance Exchange (states or feds)– Continue to fund HIT, Comparative Effectiveness
Research– Implement Medicare pilots (value purchasing, etc.)– Raise taxes– Implement fraud prevention
• States– Expand Medicaid eligibility– Operate Exchanges
Direct providers of Care
• Reduced uncompensated care• Bundled payments – value
purchasing• Incentives to form larger
groups and structures• Increased transparency and
reporting• Reduction in growth of hospital payments• Incentives to purchase HIT• Higher payment for primary care• Changes in payment due to geographic variation (?)
Consumers• Negatives
– Short term insurance rate increases– Insurance mandate– Higher taxes for some– Access issues to primary
care• Positives
– Improved access to health insurance– Lowering of health care inflation– Elimination in Medicare donut hole– Improved information about system and provider
performance– Eliminates job lock for entrepreneurs
– e

Current Issues• Individual and employer mandate
to have health insurance (State Attorney Generals)
• State’s ability to control health insurance rate increases
• Temporary high risk pools• No pre existing conditions for children• Payment to firms for early retirement coverage• Continuing health care inflation
Changes Possible
• Insurance Mandate Methods– Open enrollment– Part D penalties
• Standard Benefits• State Medicaid funding increases• Comparative Effectiveness Research• Independent Payment Advisory Board• Malpractice reform• State Waivers (e.g. public option in Vermont)
Unlikely to change• Health Insurance Exchanges• Quality• Workforce improvements
– primary care• Fraud Prevention• Prevention and Wellness• Chronic Disease Management
– ACOs, bundled Payments, Medical home• Total Repeal: due to provider/health plan resistance

“Americans always do
what is right, but only
after trying everything
else.”Winston Churchill

The Best Health Care System in the World
Additional ReadingHealth Administration Press
Further Information at: HAPMclaughlin.com