Narumanas Korwanich Department of Family and Community...
99
Narumanas Korwanich Department of Family and Community Dentistry Chiangmai University
Transcript of Narumanas Korwanich Department of Family and Community...

Narumanas KorwanichDepartment of Family and Community Dentistry
Chiangmai University

Elderly Oral Health Linkage with General Health The Mouth as a Mirror of Health The Mouth as a Portal Entry of Infection Association of Oral Infection, Diabetes, Heart
Disease/Stroke, and Adverse Pregnancy Outcome
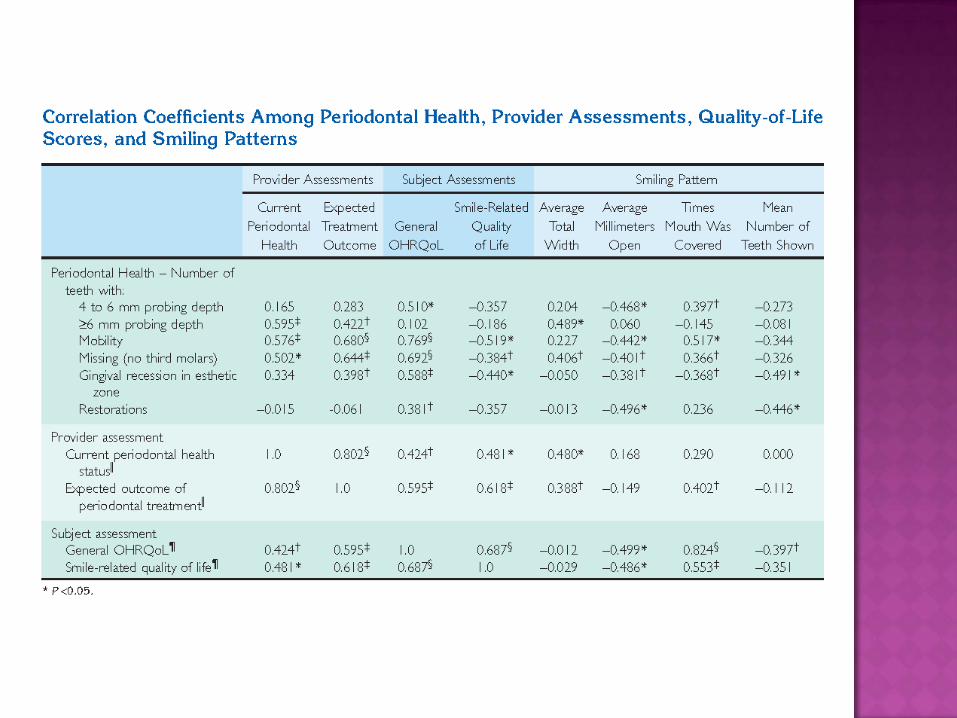
Effect on Well Being and Quality of Life Thailand Study









• The mouth and face as a mirror of health• The Mouth as a Portal Entry for Infection• Association of Oral Infection and DM, Heart
Disease, and Adverse Pregnancy Outcome
A physical examination of the mouth and face: signs of disease, drug use, domestic physical abuse, harmful habits or addictions such as smoking, and general health status
Imaging of the oral and craniofacial structures: skeletal changes e.g. osteoporosis, salivary, congenital, neoplastic, and developmental disorders
Oral cells and fluids, especially saliva: assess health and disease




Category Analyte
Drugs of abuse
AlcoholAmphetamineBarbiturateCocaineLSDMarijuanaNicotineOpiate
Antibody HIVHPVHHV
Toxin CadmiumLeadMercury
Category Analyte
Hormones CortisolProgesteroneTestosteroneSubstance PMet-enlephalin
Therapeutics AntipyrineCarbamazepineCyprofloxacinIrinoticanLithiumMethotrexatePhenytoinePhenobarbitalTheophylline

For the clinician the mouth and face provide ready access to physical signs and symptoms of local and generalized disease and risk factor exposure
Oral biomarkers and surrogate measures are also being explored as means of early diagnosis

Oral microorganisms and cytotoxic by-products associated with local infections can enter the bloodstream or lymphatic system and cause damage or potentiate an inappropriate immune response elsewhere in the body

Endocarditis is caused by bacteria that adhere to damaged endocardium(Weinstein and Schlesinger 1974)
Bacteremias from oral infections that occur frequently during normal daily activities, coincidental even with chewing food, toothbrushing, and flossing, contribute more substantially to the risk of infective endocarditis (Bayliss et al. 1983, Dajani et al. 1997, Strom et al. 1998).

Chronic obstructive pulmonary disease, characterized by obstruction of airflow due to chronic bronchitis or emphysema and by recurrent episodes of respiratory infection, has been associated with poor oral health status (Hayes et al. 1998, Scannapieco et al. 1998)
A positive relationship between periodontal disease and bacterial pneumonia has been shown (Scannapieco and Mylotte 1996)
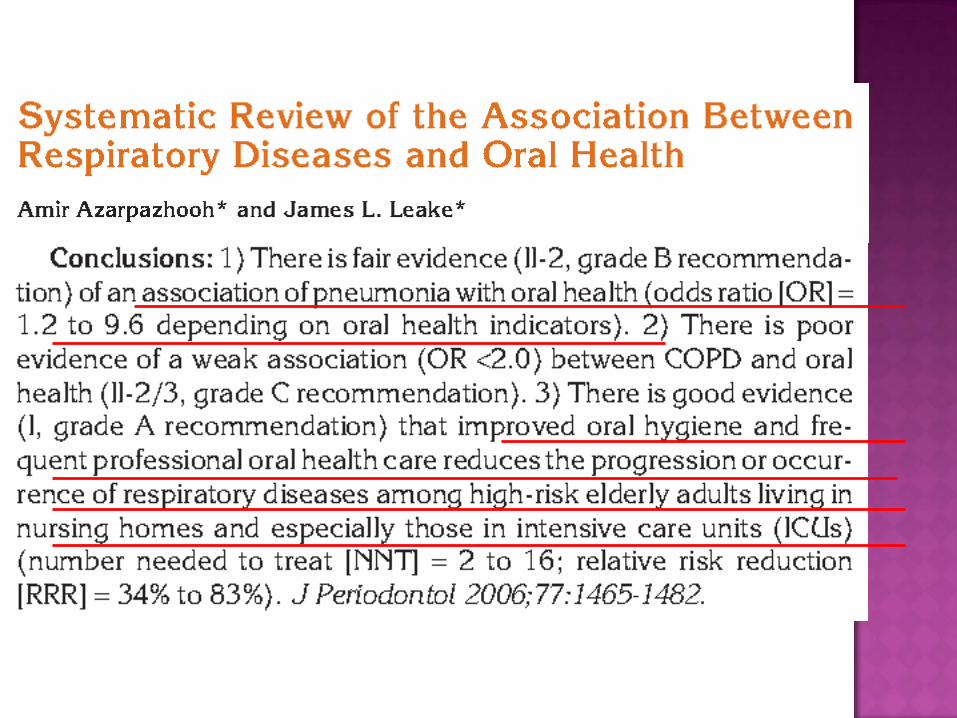
Several studies provide evidence that when the oral environment is compromised, the mouth can be a potential site of transmission of infectious microbes
Oral transmission represented 7.8 percent of primary HIV infections (Dillon et al. 2000)
Conclusion
Although oral tissues and fluids normally provide significant protection against microbial infections, but under certain circumstances, can disseminate to cause infections in other parts of the body.
The control of existing oral infections is clearly of intrinsic importance and a necessary precaution to prevent systemic complications.


Chemotherapy alters the integrity of the mucosa and contributes to acute and chronic changes in oral tissue and physiologic processes (Carl 1995)
Bacterial, fungal, and viral causes of mucositis have been identified (Feld 1997)
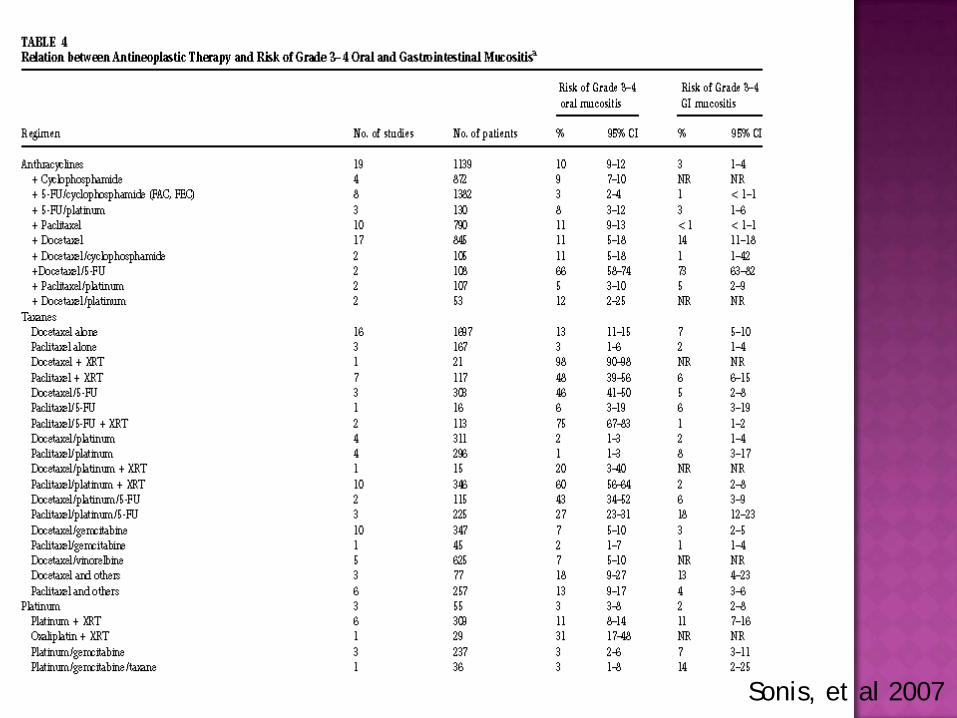
Sonis, et al 2007

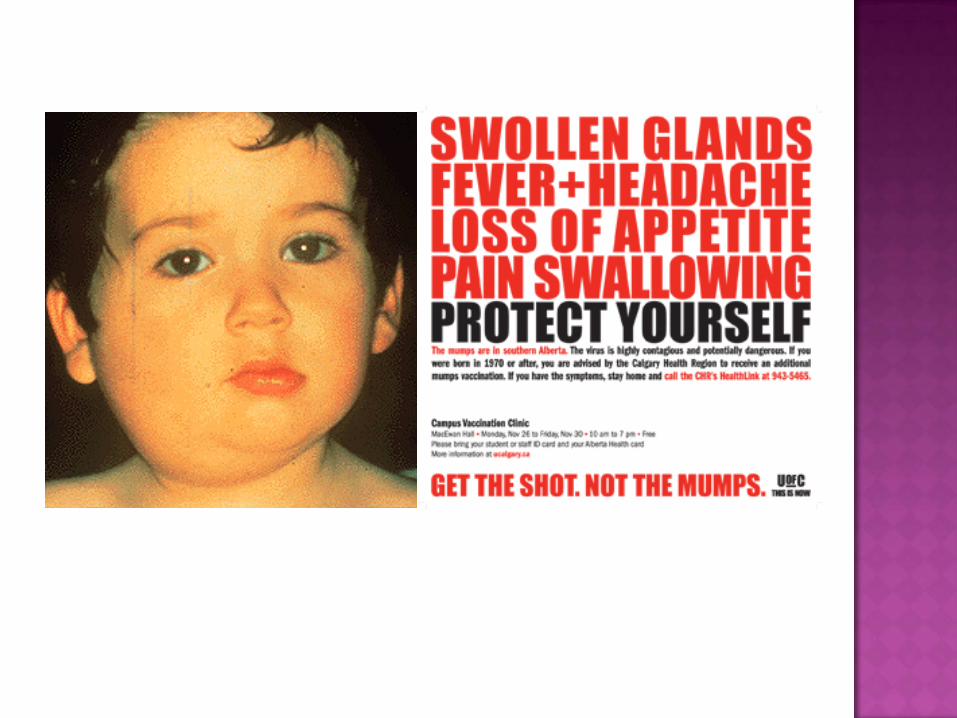
Some blood disorders, gastrointestinal disorders such as GERD (Gastro Esophageal Reflux Disease), respiratory diseases and conditions can affect oral health.
Medicine taken for other conditions may cause dry mouth, which can increase risk of dental decay, oral yeast infections and other oral infections.
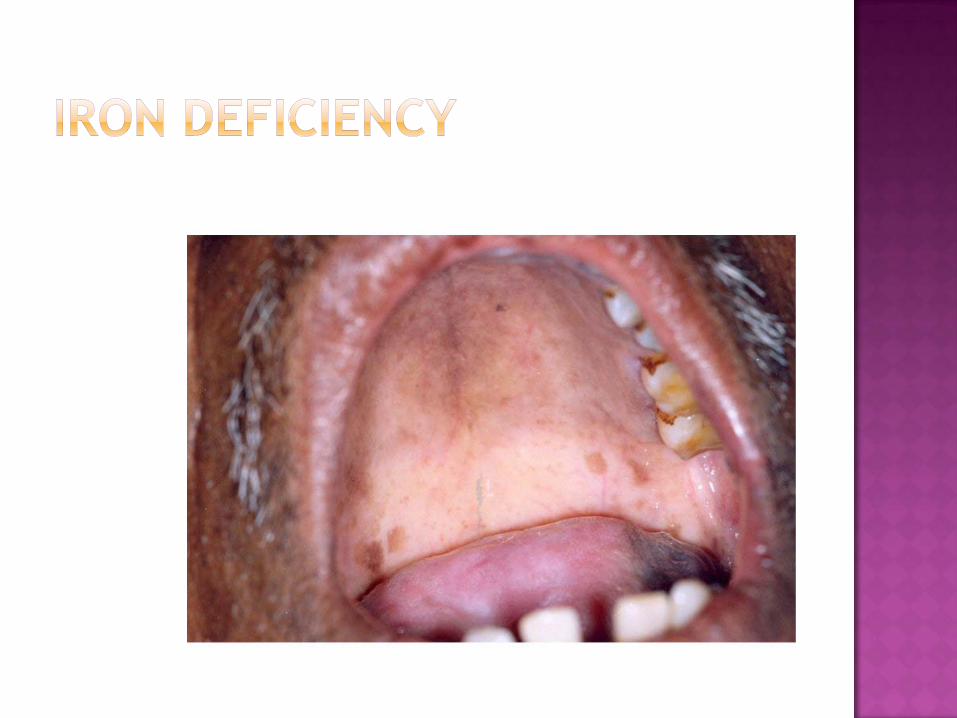
Vitamin deficiencies can have serious effects on your mouth and teeth.
Tobacco use and poor dietary practices can affect mouth and face.


There is growing acceptance that diabetes is associated with increased occurrence and progression of periodontitis
Diabetics have increased levels of systemic pro-inflammatory mediators
Diabetics have an altered response to wound healing and an abnormal immune response





Diabetic patients had a worse oral hygiene and higher severity of gingival and periodontal diseases, but they have the same extent of the periodontal diseases as compared to non-diabetics
Khader et al. 2006


The interaction of periodontal bacterial byproducts with mononuclear phagocytic cells and fibroblasts is known to induce the chronic release of cytokines (IL-1, IL-6, TNF-), PGE2 and CRP
Several recent studies have suggested that periodontal disease is a crucial aggravating factor in the health of patients with diabetes, mainly because it maintains a chronic systemic inflammatory process

Darre’s study (2008)
Aim - To investigate that periodontal disease may favour the incidence or aggravation of diabetes and its complications
Material and Methods – Literature search from 7 databases were as input of meta-analysis


These findings suggest that periodontal treatment could lead to a significant 0.79% (95% CI: 0.19, 1.40) reduction in HbA1c level
These results suggest that specific treatment of periodontal disease in diabetic subjects may improve their glycemic control
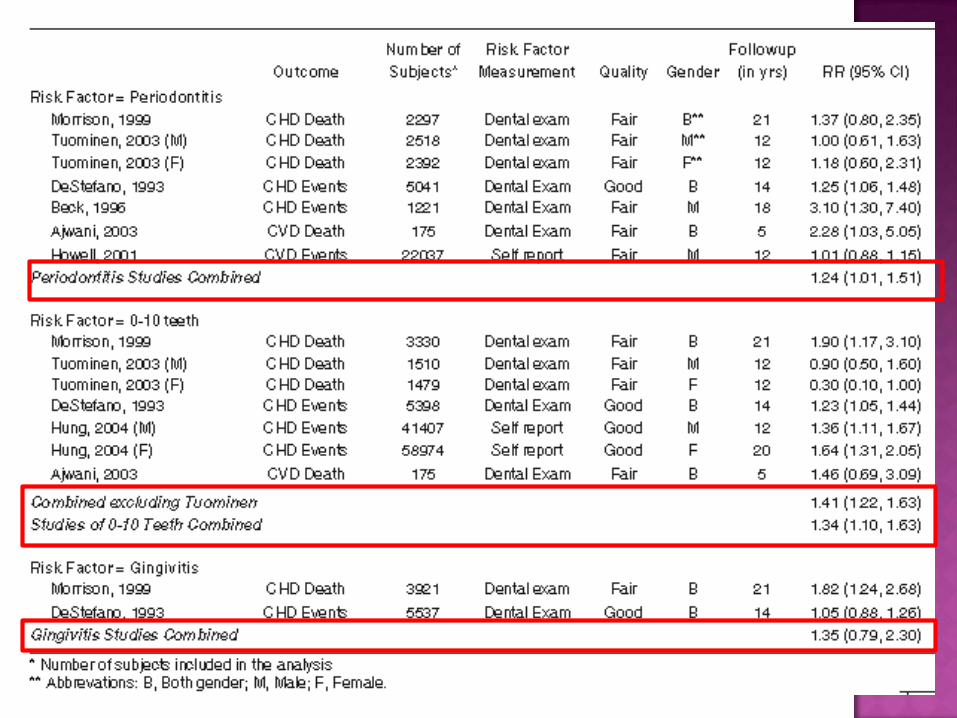
Some studies have presented evidence of the presence of bacteria and viruses in atheromatous plaques (Chiu et al. 1997, Johnston et al. 2001)
Majority of the clinical studies are seroepidemiological, reporting on associations between CHD and presence of serum antibody against the infectious agents (Mendall et al. 1994, Pasceri et al. 1998, Patel et al. 1995, Ridker et al. 1998, Saikku et al. 1992, Zhu et al. 2000).










Remote site infections, such as periodontitis, may cause PTB through hematogenous transportation of specific pathogens, organisms, or inflammatory cytokines in the amniotic fluid or chorioamniotic membranes.
Periodontal disease during pregnancy has been postulated to be 1 of the causes of PTB and LBW infants
Several case-control studies suggested that periodontitis is an increased risk factor independent of other factors






5 extracted molar versus 5 non-extracted molar rats were compared to each other in learning ability and acetylcholine release in parietal lobe brain
To examine the effects of tooth loss on the central nervous system
Kato et al., 1997
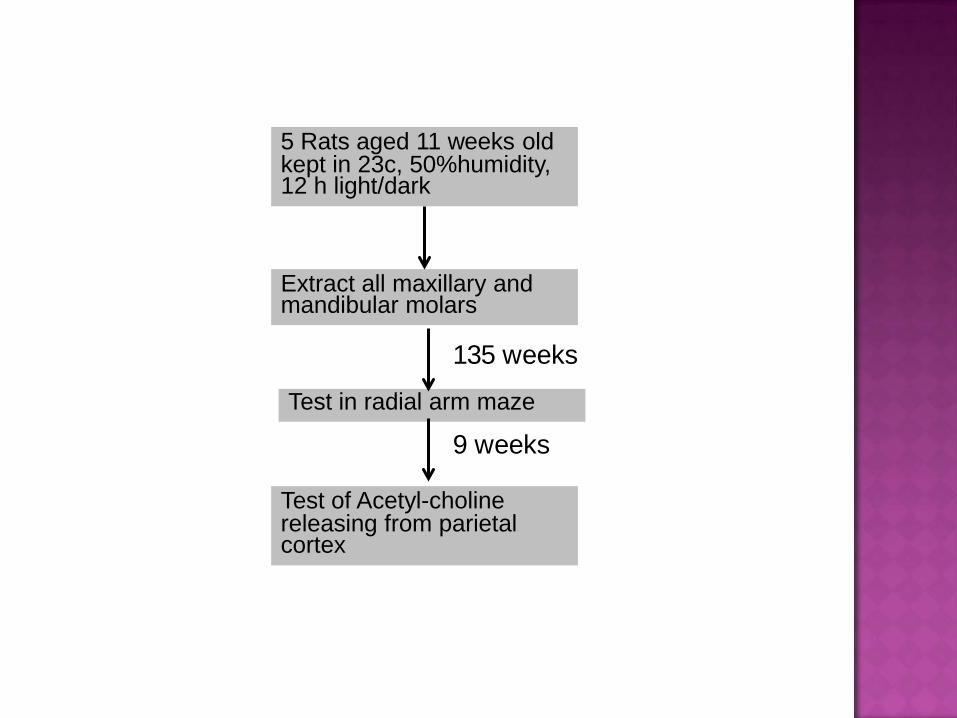
5 Rats aged 11 weeks old kept in 23c, 50%humidity, 12 h light/dark
Extract all maxillary and mandibular molars
Test in radial arm maze
Test of Acetyl-choline releasing from parietal cortex
135 weeks
9 weeks


It has been demonstrated that the neuronal activity in the brain and the cerebral blood flow were increased by mastication
Thus, one possible explanation may be that the dysfunction of cholinergic neuronal system in the teethless aged rats is caused by the long term decrease of neuron activity of the brain and/or the cerebral blood flow by the loss of teeth



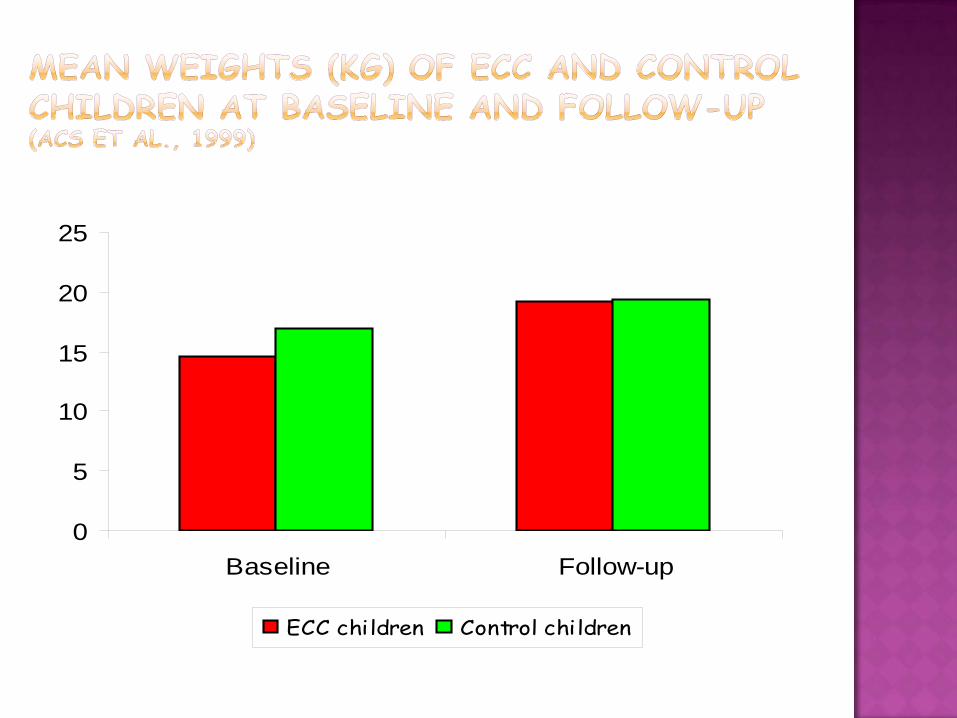
0
5
10
15
20
25
Baseline Follow-up
ECC children Control children

In the USA, it is estimated that 3.1 schooldays per 100 schoolchildren are lost due to dental illness
(US Dep’t Health and Human Services, 2000)


Medical Concept
Bio – Psycho – Social Concept

Disease ImpairmentFunctional
LimitationDisability Handicap
Death
Discomfort
Disease Impairment Functional Limitation Disability Handicap
Death
Discomfort

Authors Name of MeasureCushing et al. 1986 Social Impacts of Dental Disease
Atchinson and Dolan, 1990 Geriatric Oral Health Assessment Index
Strauss and Hunt, 1993 Dental Impact Profile
Slade and Spencer, 1994 Oral Health Impact Profile
Locker and Miller, 1994 Subjective Oral Health Status Indicators
Leao andSheiham, 1996 Dental Impact on Daily Living
Adulyanon and Sheiham, 1997 Oral Impact on Daily Performances
McGrath and Bedi, 2000 OH-QoL UK



เพือ่เปรยีบเทียบสภาวะสขุภาพรางกายในประเดน็ตางๆ ระหวางผูสงูอายท่ีุมีและไมมีฟนในชองปาก โดยประเดน็ท่ีจะทําการศกึษาไดแก ดัชนีมวลกาย (Body Mass Index; BMI) คุณภาพชีวิตอันเน่ืองมาจากสุขภาพชองปาก (Oral
Health Related Quality of Life; ORH-QOL)
ความสามารถในการเคี้ยวอาหาร (Chewing Ability Index; CAI)
สภาวะโภชนาการ (Mini-Nutritional Assessment)

ผูสงูอายุจํานวน 600 คน อายุตัง้แต 60 ปขึ้นไป 4 กลุมไดแก ผูท่ีไมมีฟนเหลืออยูเลย และไมเคยใสฟน (edentulous
group) ผูท่ีใสฟนท้ังปาก (complete denture group) ผูท่ีใสฟนบางสวน (partial denture group) ผูท่ีมีฟนธรรมชาติ (natural teeth group)
การตรวจในชองปาก Tooth status ตามแบบตรวจชองปากของ WHO หรือ
การสํารวจของจังหวัด Occluding pairs
MNAAnthropometry OIDP
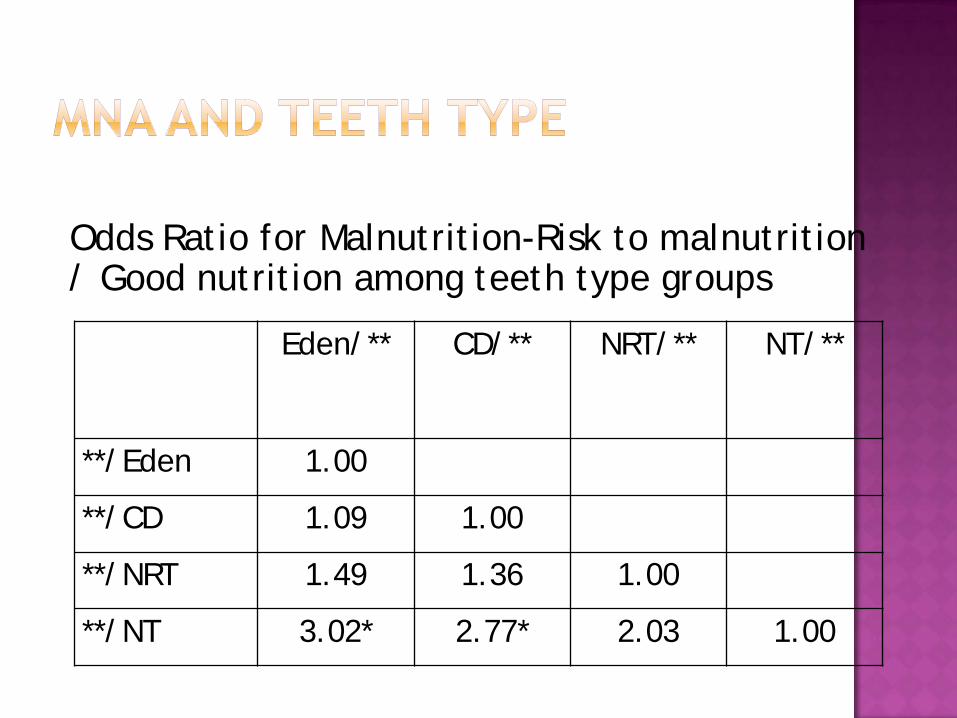
Eden/** CD/** NRT/** NT/**
**/Eden 1.00
**/CD 1.09 1.00
**/NRT 1.49 1.36 1.00
**/NT 3.02* 2.77* 2.03 1.00
Odds Ratio for Malnutrition-Risk to malnutrition / Good nutrition among teeth type groups

Eden/**Biting Chewing Swallowing
**/Eden 1.00 1.00 1.00**/CD 5.17* 5.90* 5.63***/NRT 4.69* 4.20* 4.38***/NT 7.84* 5.19* 3.86*
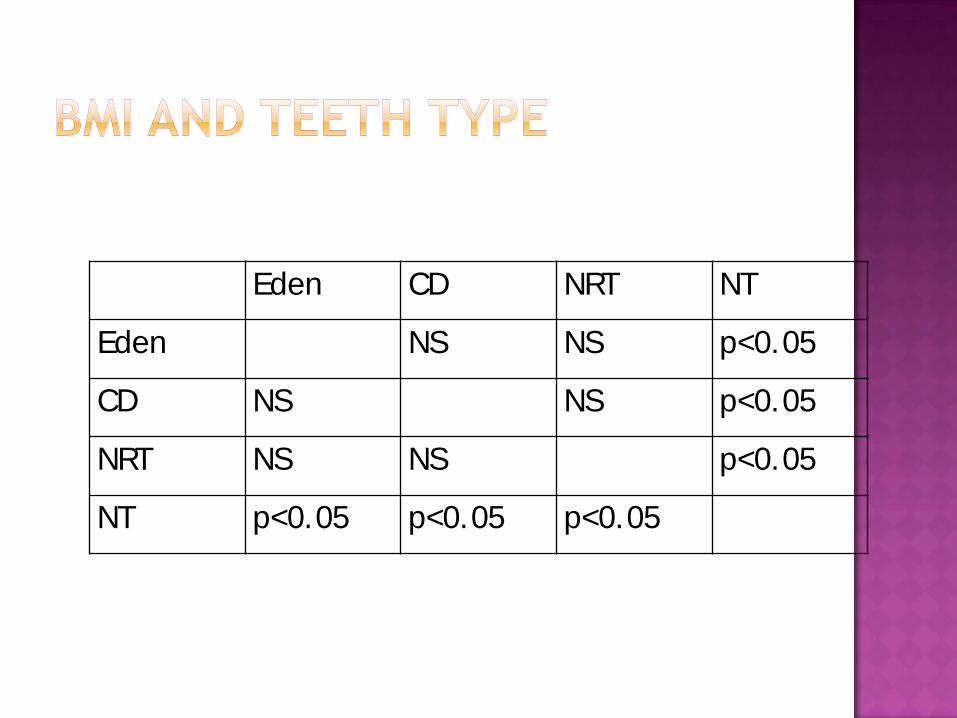
Eden CD NRT NT
Eden NS NS p<0.05
CD NS NS p<0.05
NRT NS NS p<0.05
NT p<0.05 p<0.05 p<0.05

Because oral and other chronic diseases have determinants in common, more emphasis should be on the common risk factor approach.



Don’t smoke. If you can’t, cut down
Follow a balanced diet with plenty of fruit and vegetables
Keep physically active Manage stress by, for
example, talking things through and making time to relax
If you drink alcohol, do so in moderation
Cover up in the sun, and protect children from sunburn
Practice safer sex Take up cancer
screening opportunities Be safe on the roads:
follow the highway code Learn the first aids ABC:
airway, breathing, circulation

Don’t be poor. If you can’t, try not to be poor for long
Don’t have poor parents Own a car Don’t work in a
stressful, low paid, manual job
Don’t live on damp, low quality housing
Be able to go on foreign holiday and sunbathe
Practice not loosing your job and don’t become unemployed
Take up all benefits you are entitle to, if you are unemployed, retired, sick, or disabled
Don’t live next to busy road or near a polluting factory
Learn to fill in the complex housing application form

Solely focusing on changing lifestyle of individuals is both ineffective and costly
It is incorrect to assume that lifestyles are freely chosen and can be easily changed by everyone
Health knowledge and awareness are of little value when resources and opportunities to change do not exist
Individual’ s behaviors are therefore largely determined by the conditions in which they live.
Hocusing solely on changing lifestyle is ineffective and also widen health inequalities


By integrating oral health into strategies for promoting general health and by assessing oral needs in sociodental ways, health planners can greatly enhance both general and oral health
Sheiham 2005