NAMI Beginnings - Winter 2008
16
The Youth Voice ★ State and Affiliate News ★ Book Review A Publication Dedicated to the Young Minds of America from the NAMI Child & Adolescent Action Center Winter 2008 ★ Issue Ten Promoting Evidence-Based Practices Ask the Doctor: Behavior Therapy for ADHD
-
Upload
nami-yakima -
Category
Documents
-
view
224 -
download
4
description
NAMI's own publication regarding the mental health and wellness of young people.
Transcript of NAMI Beginnings - Winter 2008

T h e Yo u t h Vo i c e � S t a t e a n d A f f i l i a t e N ew s � Boo k R e v i ew
A Publication Dedicated to the Young Minds of America from the NAMI Child & Adolescent Action Center
Winter 2008 � Issue Ten
PromotingEvidence-BasedPracticesAsk the Doctor:Behavior Therapyfor ADHD

2 | Nami Beginnings | Issue 10 | Winter 2008
C O N T E N T S
NAMI Beginnings is publishedquarterly by NAMI, Colonial PlaceThree, 2107 Wilson Blvd., Suite 300,Arlington, VA 22201-3042.Ph: 703.524.7600 Fax: 703.524.9094
Michael Fitzpatrick, Executive DirectorDarcy E. Gruttadaro, J.D., Editor-in-ChiefDana C. Markey, Managing and
Copy EditorJoe Barsin, Art Director
Guest Contributors:Laurie BlissMelanie Duncan, Ph.D.Kelly C. Feller, M.S.WPatrick Kanary, M.Ed.Clara LaBrierDonna PollardKeller StrotherCathy SuraceLora Thomas
Staff Contributors:Darcy Gruttadaro, Dana Markey andBianca Ruffin.
NAMI is a grassroots, family andconsumer, self-help, support, education,and advocacy organization dedicatedto improving the lives of children andadults living with severe mental illnesses.Severe mental illnesses are biologicallybased brain disorders that can profoundlydisrupt a person’s ability to think, feel,and relate to their environment and others.
NAMI web site: www.nami.orgNAMI HelpLine: 1.800.950.6264
P O L I C Y A L E R T S
NAMI Supports Federal LegislationFocused on Children
The 1st Session of the 110th
Congress is likely drawing toa close. There were a numberof bills introduced and carriedover that are designed to
improve the lives of children andadolescents living with mental illnesses.
The Keeping Families Together Act(S. 382/H.R. 687) is one of those bills.It is designed to help end the unthink-able practice of forcing families torelinquish custody of their child forthe sole purpose of accessing mentalhealth services. This practice ofcustody relinquishment is also likelyto be addressed in a bill to reauthorizethe Substance Abuse Mental HealthServices Administration (SAMHSA).
NAMI continues to supportThe Health Care Crisis Relief Act(S. 1572/H.R. 2073), legislation targetedat addressing the national workforceshortage of child mental healthproviders. This shortage is a majorbarrier to many families accessingmental health services for their child.It is not uncommon for families to betold that they must wait up to sixmonths for an initial appointment ortravel hours from their home to see achild mental health professional. Thispresents a tremendous hardship forchildren and their families.
This year the House and Senate havefocused on mental health in ournation’s schools. The Positive Behaviorfor Effective Schools Act (S. 2111/H.R.3407) was introduced. This bill wouldmake it easier for schools to use federalfunding to implement school-widepositive behavioral interventions andsupports (PBIS) that promise to createa more positive school environmentand help identify students who may be
struggling with mental health relatedconcerns. (To learn more about PBIS,visit www.pbis.org).
Also on the school front, NAMI isworking with a coalition of nationaldisability rights’ groups to call forfederal legislation to prohibit the inap-propriate use of restraint and seclusionin our nation’s schools. We are alsoclosely following draft legislation anddiscussions on the reauthorization ofthe No Child Left Behind law to helpensure that schools are held accountablefor the academic and functionalachievement of students with disabilities,including those with mental illnesses.
This year also saw the introductionof the Mental Health in Schools Act of2007 (S. 1332/H.R. 3430). This billexpands the availability of comprehen-sive school-based mental health servicesfor students in communities acrossAmerica.
You can learn more about these billsby visiting the Library of Congress“Thomas” website at thomas.loc.gov.The bill number, included above foreach piece of legislation (Senate billsare designated as “S” and House billsare designated as “H.R.”), allows you toeasily find the bill, the co-sponsors,action taken on the bill, and its currentstatus.
State House ActivityNAMI continues to work with a smallgroup of national organizations focusedon children’s mental health. Our groupwas formed largely in response toanti-psychiatry activity targeting statelegislators. NAMI chairs the workgroup, which consists of the followingnational organizations: the AmericanAcademy of Child & AdolescentPsychiatry (AACAP), American SchoolCounselor Association (ASCA),
2 POLICY ALERTSCapitol Hill and State House Watch
3 The Implementation ofEvidence-Based Practices
5 Medicaid Coverage ofMultisystemic Therapy
9 THE YOUTH VOICE
10 FAMILY VOICE
11 ASK THE DOCTOR
13 STATE NEWS
14 AFFILIATE NEWS
15 BOOK REVIEW
Capitol Hill andState House Watchby Darcy Gruttadaro, J.D., Director, NAMI Child &Adolescent Action Center

F E A T U R E
Incorporating evidence-basedpractices and best practices intosystems of care highlights theneed to merge quality outcome-based services with effective and
efficient systems. Evidence-basedpractices and effective systems of careare two parts of the whole picture andcreate a natural and synergistic rela-tionship. Both possess components thatproduce a more clinically, systemically,and fiscally responsive mental healthcare system.
Implementation ChallengesFor effective implementation ofevidence-based practices (EBPs) insystems of care to occur, there are afew key focus areas to consider. Theseimplementation challenges relate toorganizational, clinical, and practicelevel changes that must be made tomake EBPs more broadly available.These challenges also include financial,systemic, and policy issues.
Organizational/Clinical/Practice Level.Despite the growing attention to EBPs,the reality is that an extremely smallpercentage of youth and families haveaccess to evidence-based interventions.These interventions tend to be theexception and are often considered as“pilot” projects, rather than integralparts of the system of care.
There are many reasons why EBPsare not more widely available forchildren, adolescents, and theirfamilies. Here are several of the factorsthat impact the availability of EBPs:• Sufficient qualified workforce and
system capacity to deliver EBPs;• Lack of incentives or support to
change current practices;• There is a tremendous amount of
resource investment and reinvest-ment required for significantchange in moving to a system thatprimarily provides EBPs and bestpractices;
• There are significant organizationalchanges required in financing andfunding EBPs and best practices;
• There may be concerns with theeffectiveness of certain EBPs in cul-turally and racially diverse commu-nities; and
• EBPs may or may not be acceptableto families.
Financial/Funding.Asking funders to significantly shiftand reinvest dollars into EBPs requiresthat the funders be provided with thetools necessary to understand how toreinvest those dollars. Progress is ofteninhibited by communities and statesstruggling with how to design effectivefinancing strategies that match theirdesired outcomes. For example, ifstakeholders decide that their goal is tokeep youth and families together andreduce out-of-home placements, thenthey must work to create financingstrategies and procedures that providefunding for the development and avail-ability of more home and community-based services to reach their goals.
Systemic/Policy.The most significant challenge in morebroadly implementing EBPs is the needto “prepare the field” for EBP selectionand implementation. Simply droppingevidence-based practices into an exist-ing system will not work or — at the
The Implementationof Evidence-BasedPracticesby Patrick Kanary, M.Ed., Director, Center for Innovative Practices, Ohio andKelly Feller, M.S.W, Director, Utah Behavioral Health Center of Excellence
Children and Adults with AttentionDeficit/Hyperactivity Disorder(CHADD), the Child and AdolescentBipolar Foundation (CABF), theFederation of Families for Children’sMental Health (FFCMH), and MentalHealth America (MHA - formerly theNational Mental Health Association).
We received reports from advocacyleaders and members of our respectiveorganizations about anti-psychiatryinformation being shared with statelegislators. In response, our workgroup developed a state advocacytoolkit to share with grassroots lead-ers affiliated with our organizationsthat includes jointly endorsedresources and information to distrib-ute to state lawmakers. This informa-tion includes a series of fact sheets,sample letters, anti-psychiatry legisla-tion introduced in previous legislativesessions, and more.
The toolkit is near completionand will be posted on the respectiveweb sites of each of our nationalorganizations, making it easy forNAMI leaders, members, families,and friends to download. Please lookfor the toolkit on the Child &Adolescent Action Center sectionof the NAMI website at www.nami.org/CAAC.
Anti-psychiatry groups remainactive in contacting state and federallawmakers with false informationabout children’s mental health. Weneed your help in making sure thatmaterials in the toolkit get intothe hands of state legislators andpolicymakers. Together we will makea positive difference in the lives ofchildren and adolescents living withmental illnesses and their families.
Winter 2008 | Issue 10 | Nami Beginnings | 3

F E A T U R E
4 | Nami Beginnings | Issue 10 | Winter 2008
very least — will not allow for smoothsystems’ development. A thoughtfulplanning process is critical in creating asustainable environment for the accept-ance and growth of EBPs. Considerationmust be given to the culture of thesystem and how it functions, its pri-mary consumers, and the context inwhich services are provided. Thereference to “evidence-based practices”can be confusing. Consequently, clearerstatements such as “outcome- basedinterventions” and “data-drivensystems of care” may be more useful tohelp everyone understand what isbeing considered. Finally, creating anenvironment conducive to changerequires the alignment of federal, state,and local policies that support systemsof care and evidence-based practicesdevelopment.
Successful Strategies/Lessons LearnedImplementation of strong systems ofcare has taught us that the alignment ofpolicies, procedures, fiscal strategies,and clinical interventions is the key tosuccessful outcomes with systems’stakeholders, including children andfamilies, providers, funders, and policymakers. The process and the lessonsinvolved in moving systems of care toinclude more evidence-based practicesis complex. It is important to recognizethat a cookie-cutter approach will notwork; rather individualized strategicplanning for EBPs must take place toachieve effective implementation thatworks for the state and local communi-ties. Whatever steps are taken towardthe broader dissemination of EBPs,they must be framed within thestrengths, assets, risks, and opportuni-ties of that state and local community.While each state and local communitywill face unique issues, the followinggeneral strategies and lessons learnedare likely applicable:
Organizational, Clinical, andPractice Levels• Focus on EBPs that address youth
and family strengths and includediverse family voices;
• Identify specific practices, whetherevidence-based or promising, aspreferred treatment interventions
for specific behavioral healthconditions;
• Increase education, training, andprovider expectation to focus moreon outcome-based treatments;
• Devote sufficient preparation andtechnical assistance related to theEBP requirements, such as work-force skills and adequate financing,so that the opportunity for successfulimplementation will be maximized;
• Attend to the organizational, systemic,and clinical aspects of the EBPs andthe factors that must be adopted toeffectively implement the EBPs;
• Seek EBPs with structured training,coaching, and fidelity protocols;
• Ensure that providers receiveongoing coaching and consultationto maintain fidelity to the EBP andto stay true to the EBP interven-tion; and
• Track fidelity to ensure that EBPsare being implemented appropriately.
Financing/Funding• Thoroughly understand the federal,
state, and local financing strategiesthat may or may not support thespecific EBP under consideration;
• Create incentives for more integratedand consolidated resource manage-ment and family-based care, whichmay include federal Medicaidwaivers that allow for fundingbased on needs and outcomes;
• Provide financial technical assistanceto create and implement sustain-able funding strategies;
• Effectively use federal Medicaidwaivers and state funding options,including braided and blendedfunding from multiple child-serv-ing agencies (mental health, childwelfare, juvenile justice), to createfunding streams that focus onindividualized needs regardless of“systems” identification; and
• Promote collaboration, pooling ofresources, and shared risk takingacross child-serving systems toinclude child welfare, mental health,juvenile justice, and education.
Systemic/Policy• Create shared screening, assessment,
and gate keeping practices at allcritical entry points for childrenand adolescents with mental health
treatment needs to promote earlyidentification and intervention;
• Drive EBP practice selectionthrough a local planning processthat includes key stakeholders(parents/families/youth, providers,funders, representatives fromchild-serving systems, and otherappropriate public-private partners)that determines the needs of thecommunity, based on a comprehen-sive community assessment ofassets, risks, and protective factors;
• Provide both general and specificeducation on what evidence-basedpractices are and are not;
• Establish outcomes that are desirableto multiple stakeholders, includingparents/families/youth, funders,policy makers, public systems, andother key stakeholders;
• Conduct outreach, engagement,and inclusion of families as “systempartners” in all phases of systemsreform and EBP implementation;
• Identify state and local leaders whowill be EBP champions and advocates;
• Promote EBPs that will meet thegreatest need for the communityand will produce the best sharedoutcomes across child-servingsystems;
• Build early success, celebrate it, andencourage it to lead to broader sys-temic reform; and
• Create a community of culturearound the need to continue totrack and improve service outcomes.
Keys to SuccessMany of the “successful strategies”and “lessons learned” presented in thisarticle will help states and communitiesas they work to make evidence-basedpractices in children’s mental healthmore widely available. It is importantto simultaneously focus on the practice,financing, policy, and systemic levelsin order to build a sustainable plan forincorporating evidence-based practicesinto systems’ reform. Ultimately, identi-fying and harnessing all federal, state,and local resources and expanding onand adapting existing proven strategiesto specific community needs andcultures is paramount to achievingEBP implementation success.

IntroductionMedicaid funding has emerged as animportant factor in the growth ofMultisystemic Therapy (MST) programsnationally. MST is a highly toutedevidence-based practice for delinquentyouth and Medicaid funding is playinga critical role in its financial sustain-ability in approximately half of the 32states that currently have licensed MSTprograms.iWhile advocacy is recom-mended to ensure MST, as well as otherevidence-based practices, are includedin a state’s Medicaid service array,Medicaid should not be viewed as a“silver bullet” that will cover the fullcost of providing MST services foryouth. Based on the experience ofmany states and localities, additionalfunding streams are necessary to fullysupport a state’s MST program. Giventhe proven cost effectiveness of MST,state legislators and officials presentedwith the facts should be willing toappropriate funds and develop pro-grams to support this evidence-basedpractice that helps children and theirfamilies and produces cost-savings totaxpayers on the order of five dollarsfor every one dollar invested.ii
Background on MST and MedicaidMultisystemic Therapy (MST) is anintensive family and community-basedtreatment that addresses the multipledeterminants of serious antisocialbehavior in juvenile offenders acrossthe key settings, or systems, within
which youth are embedded (e.g., fami-ly, peers, school, neighborhood). MSTstrives to promote behavior change inthe youth’s natural environment, usingthe strengths of each system to facilitatechange.iii
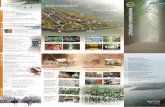
Scientific evidence shows thatjuvenile offenders treated with MST orwith one of two other evidence-basedpractices, Functional Family Therapy(FFT) and Multidimensional TreatmentFoster Care (MTFC), will be re-arrest-ed less frequently and have improvedfamily functioning and school perform-ance, and decreased substance abuse,psychiatric symptoms, and rates ofout-of-home placement.iv The benefitsof MST last into adulthood. As depict-ed below in Figure 1, a 14-year follow-up study comparing youth who
received MST with youth who receivedindividual therapy has documented a55% reduction in re-arrest rates and a57% decrease in the number of daysconfined.v
The United States Department ofJustice, the Office of Juvenile Justiceand Delinquency Prevention, theBlueprints for Violence PreventionInitiative, and the United StatesSurgeon General, are among the manyentities that have placed MST, FFT andMTFC at the top of their list of modelevidence-based programs for youthwith delinquent behavior, a high per-centage of whom have mental illness.vi
Approximately 20% to 25% of delin-quent youth have serious mental healthdisorders and up to 70% have a diag-nosable mental illness.vii
Winter 2008 | Issue 10 | Nami Beginnings | 5
F E A T U R E
Medicaid Coverage ofMultisystemic TherapyBy Cathy Surace, Managing Attorney, Maryland Disability Law Center
iA list of the states with licensed MST programs is available at http://www.mstservices.com/licensed_providers.php.ii Aos, S., Miller, M., & Drake, E., (2006 October), Cost Effectiveness of Evidence-Based Public Policy Options to Reduce Future Prison Construction, Criminal Justice Costs, and CrimeRates, Washington State Institute on Public Policy (#06-10-1201) at http://www.wsipp.wa.gov/pub.asp?docid=06-10-1201.iiiFor more information about MST, see website of MST, Inc. at www.mstservices.com and NAMI Beginnings, Fall 2003, Issue 3 athttp://www.nami.org/Template.cfm?Section=Child_and_Adolescent_Action_Center&Template=/ContentManagement/ContentDisplay.cfm&ContentID=12717.ivKey Issues, National Center for Mental Health and Juvenile Justice, Key Issue 5 at http://www.ncmhjj.com/faqs/default.asp, relying on Elliott, D. (Ed.) (1998-2002) Blueprints forViolence Prevention Series (Vols. 1-12). Boulder, CO : Center for the Study and Prevention of Violence.vSchaeffer, C. M., & Borduin, C. M. (2005). Long-Term Follow-Up to a Randomized Clinical Trial of Multisystemic Therapy With Serious and Violent Juvenile Offenders, Journal ofConsulting and Clinical Psychology, 73(3), 445-453. The researchers in this study successfully located 94% of the original participants.viTurning Knowledge Into Practice, A Manual for Behavioral Health Administrators and Practitioners About Understanding and Implementing Evidence-Based Practice, The TechnicalAssistance Collaborative, Fall 2003, at 49; Office of Juvenile Justice and Delinquency Prevention, http://ojjdp.ncjrs.org/; http://www.colorado.edu/cspv/blueprints/; Youth Violence:A Report of the Surgeon General, U. S. Department of Health and Human Services, 2001, hereinafter cited as “Youth Violence: A Report of the Surgeon General” athttp://www.surgeongeneral.gov/library/youthviolence/.
Figure1: MST and Individual Therapy Outcomes at 14-Years Post-treatment
AVERAG
EARRESTS
DAYS
14 YEARSFOLLOW UP
AVERAGE ADULTDAYS CONFINED
AVERAGE ADULTDAYS ON PROBATION
55%REDUCTION
57%REDUCTION
43%REDUCTION
1.8(M
ST)
3.9(Indvidual
Therapy)
582(M
ST)
1357
(Indvidual
Therapy)
421(M
ST)
739(Indvidual
Therapy)

Under the federal Medicaid program,states are able to recoup from 50% to83% of billable costs, depending on thestate’s average per capita income, forproviding any health care service thatis included in the State Medicaid Plan.viii
Given this strong fiscal incentive tostates, it is not surprising that Medicaidnow funds more than half of publicmental health system services and isestimated to account for two-thirds ofsuch spending by 2017.ix The Centersfor Medicare and Medicaid Services(CMS), the federal agency that admin-isters the Medicaid Program, willapprove the inclusion of a health careservice in a State Medicaid Plan if CMSdetermines that the service is coveredby the federal Medicaid Act. CMS hasalready determined MST is a coveredMedicaid service because the agencyhas approved at least one State PlanAmendment to add MST as a coveredservice in North Carolina. In 2003,CMS also created a billing code, H2033for MST under the HealthcareCommon Procedure Coding System(referred to as HCPCS).
Under the Medicaid Act’s Early andPeriodic Screening, Diagnosis, andTreatment (EPSDT) mandate, Medicaidrecipients under 21 have a legal rightto access any medically necessaryhealthcare service that could be coveredby the Medicaid Program. Since CMShas determined MST is a coveredservice, states not providing MSTservices under Medicaid are vulnerableto a legal challenge.x
It is difficult to pinpoint exactlyhow many states are billing MST toMedicaid because states are billingMST under other broader Medicaidservice and billing categories ratherthan using the MST HCPCS billingcode that would require them to addMST by name as a service in the StateMedicaid Plan.xi Officials and providersin 18 states plus the District ofColumbia have reported billingMedicaid.xii Of the 18 states, one state,Alabama, is not using licensed MSTproviders and it’s “MST-lite” or MST-like programs may not yield the samepositive outcomes for youth and theirfamilies.xiii CMS itself, along with theSubstance Abuse and Mental HealthServices Administration (SAMHSA)and the President’s New FreedomCommission on Mental Health, haveencouraged states to use Medicaid,where possible, to fund evidence-basedpractices that they have recognizedmost individuals with mental illnesscould not access.xiv
Cost and Effectiveness ComparisonsMany state juvenile justice agenciesand courts currently rely on costlysecure residential placements, such asdetention centers, that are notMedicaid reimbursable for juvenileoffenders, even though many of theseyouth could be diverted and returnedhome safely with MST or FFT, orunder other programs, at a fraction ofthe cost. For example, in Marylandwhere the cost of MST has ranged from
$5,000 to 8,000 per child or approxi-mately $40 to $44 per day for a 4 to 6month course of treatment, only a few,small MST programs exist.xv InsteadMaryland, on an average day, placed253 children in detention centers at acost of approximately $328 per day and1494 children in other residentialsettings that range in cost up to $582per day for children placed in psychi-atric residential treatment centers.xvi
The proposed spending on detentionand deep-end residential placements inMaryland accounted for almost 60% ofthe Maryland Department of JuvenileServices budget in fiscal year 2005.xvii
This huge expense is not justifiablegiven the fact that these costly place-ments, unlike MST and other evidence-based practices, do not result in posi-tive outcomes for youth. Recidivismrates in Maryland for youth releasedfrom these placements are high andreflect that 67 % will be re-arrestedwithin 2 years and 75 % will bere-arrested within 3 years.xviii In con-trast, research studies on recidivismrates of MST and FFT graduates reflectthat re-arrest rates are typically cut atleast in half despite the much lowercost for these evidence-based practices.
The Washington State Institute forPublic Policy, a non-partisan researchinstitute created by the state legislature,has done multiple reports on therelative cost effectiveness of juvenilejustice treatment programs and rankedMST highly based on documentedsavings to taxpayers and crime victims
6 | Nami Beginnings | Issue 10 | Winter 2008
F E A T U R E
viiShufelt, J. & Cocozza, J., Youth with Mental Health Disorders in the Juvenile Justice System: Results from a Multi-State Prevalence Study, National Center for Mental Health andJuvenile Justice, June 2006; Teplin, L., Abram, K., McClelland, G., Duncan, M. Mericle, A., Psychiatric Disorders in Youth in Juvenile Detention, Archives of General Psychiatry,December 2002.viiiSee http://aspe.hhs.gov/health/fmap07.htm, a notice in the Federal Register announcing the calculated “Federal Medical Assistance Percentages” and “Enhanced Federal MedicalAssistance Percentages” that were used in determining the amount of Federal matching for State medical assistance (Medicaid) and State Children's Health Insurance Programexpenditures from October 1, 2006 through September 30, 2007.ixBuck, J., Medicaid, Health Care Financing Trends, and the Future of State-based Public Mental Health Services, Psychiatric Services, 2003.xEvidence-Based Practices for Delinquent Youth with Mental Illness in Maryland: Medicaid Must Cover these Cost Effective Services, A Public Report by Maryland Disability Law Center,January 2007 at 24-25, at http://www.mdlcbalto.org/publications.htm, hereinafter cited as MDLC Public Report on Evidence-Based Practices.xiSee discussion below and MDLC Public Report on Evidence-Based Practices at 18, at http://www.mdlcbalto.org/publications.htmxiiMDLC Public Report on Evidence-Based Practices at 24-25, at http://www.mdlcbalto.org/publications.htm. These states are Alabama, Arizona, California, Colorado, Connecticut,Georgia, Hawaii, Maine, Michigan, Nebraska, New Mexico, North Carolina, Ohio, Pennsylvania, South Carolina, Tennessee, Texas, and Wyoming. MST Services, Inc. lists 12states as billing Medicaid and does not list Alabama, Colorado, Georgia, Michigan, Tennessee, Texas, and Wyoming at http://www.mstservices.com/funding_and_medicaid_standards.php.xiiiSee discussion below associated with notes 24 and 26.xivMedicaid Support of Evidence-Based Practices in Mental Health Programs, a technical assistance paper prepared jointly by SAMSHA and CMS, at http://www.medicine.uiowa.edu/icmh/evidence/documents/Medicaidsupportforebps.pdf; and Subcommittee on Evidence-Based Practices of the President’s New Freedom Commission on Mental Health,Background Paper, April 2005, at 23, at http://www.mentalhealthcommission.gov/reports/EBP_Final_040605.pdf.xvMDLC Public Report on Evidence-Based Practices at 11, 13-15, at http://www.mdlcbalto.org/publications.htm.xviId. at 10 and notes 63 – 66. The estimate of $328 per day for the cost of a detention bed has been increased from the $243 cited in this report based on testimony providedduring the 2007 budget hearing of the Maryland Department of Juvenile Services.xviiAnalysis of the FY 2005 Executive Budget, Maryland Department of Juvenile Services at 32, 2004, at http://mlis.state.md.us/.xviiiAnalysis of the FY 2007 Executive Budget, Maryland Department of Juvenile Services at 15, ex. 8, 2006, at http://mlis.state.md.us/.

Winter 2008 | Issue 10 | Nami Beginnings | 7
F E A T U R E
and a computation of benefits minuscosts, as depicted in Figure 2.xix
Medicaid reimbursement providesanother compelling cost consideration.States could be billing a significantportion of the cost of MST services forMedicaid eligible youth to CMS and bereimbursed from 50% to 83% of theirbills. In contrast, federal law prohibitsstates from accessing Medicaid reim-bursement for the cost of locked orsecure juvenile facilities as well as anyhealth care services youth in suchfacilities need.xx Thus, states now payfor the expensive secure placement plusthe potentially sizable cost of behav-ioral and somatic health care servicesfor this population with only statedollars.xxi
Even in states that do not useMedicaid funding to provide MST, suchas Florida, MST programs with signifi-cant cost savings have been ongoing asthe result of legislation appropriatingfunds or other state initiatives.
According to a February 2007 reportby the Florida legislature, theRedirection Program provided MST andFFT to 405 youth and avoided statecosts of $5.8 million just in its first twoyears of operation.xxii Not surprisingly,Florida’s legislature expanded theprogram to thirteen judicial circuits.The Florida legislation provides astarting point for drafting legislation inother states and the legislative reportdocumenting cost savings from theprogram should be helpful in securingpassage of such laws or promoting stateinitiatives elsewhere.xxiii
Medicaid Billing Is Not a PanaceaIn many of the states billing Medicaidfor MST, this funding alone has notbeen sufficient to support a MSTprogram operating with the requiredfidelity monitoring to ensure strictadherence to the model — known as“model fidelity” — and MST’s positiveoutcomes.xxiv According to estimates
from some states and the District ofColumbia, 40 to 60 percent of a model-adherent MST team’s operating budgetwill be covered by Medicaid fundingalone.xxv One obvious obstacle to fullreimbursement is that not all childrenin families in need of MST will meetthe eligibility criteria for Medicaid.Another obstacle is the inability to billsome of the standardized componentsof MST, such as training, supervision,and evaluation. This can lead statesto implement MST in a manner tomaximize Medicaid billing and reduceadherence to model fidelity. Modelfidelity is critical because one of theprimary reasons MST program replica-tions are effective is that each newprogram adheres to the same, well-specified treatment implementationand quality assurance model. Evensubtle changes in implementation canhave a negative impact on a program’soutcomes.xxvi
For example, some state Medicaidsystems only reimburse for face-to-facecontacts, and at times, only contactswith family members when the youthis present. This type of fundingstructure can easily lead to non-modeladherent practices that overemphasizeyouth treatment sessions in clinicalimplementation. In MST, therapistswork frequently and intensively withthe youth’s caregivers, extended family,and teachers to ensure they can inter-vene to effectively manage the youth’sbehavior problems, and the youth mayor may not be included in a particularsession.
From the provider perspective, thecurrent HCPCS code for MST is basedon a 15-minute billing increment that
Figure 2: MST Costs & Benefits per Participant
$20,000
$15,000
$10,000
$5,000
$0
BENEFITS TOCRIME VICTIMS
BENEFITS TOTAXPAYERS
COST OF MST
xixThe data in figure 2 is from Aos, S., Miller, M., & Drake, E., (2006 October), Cost Effectiveness of Evidence-Based Public Policy Options to Reduce Future Prison Construction,Criminal Justice Costs, and Crime Rates, Washington State Institute on Public Policy (#06-10-1201), at http://www.wsipp.wa.gov/pub.asp?docid=06-10-1201. Taxpayer savingswere estimated by considering how police and court costs are reduced when arrests go down and how jail and prison costs are reduced when sentences decrease. Benefits to crimevictims were estimated by placing a monetary value on the costs that crime victims incur that can be avoided if arrests decline. Although the cost of providing MST has increasedsince the date of this research, it is assumed that the police and court costs as well as costs to crime victims have increased as well.xxThe federal Medicaid Act and regulations prohibit federal financial participation “with respect to care or services for any individual who is an inmate of a public institution.”See 42 U.S.C. § 1396d(a)(27)(A); 42 C.F.R. §§ 441.33(a)(1), 435.1008 and 435.1009.xxiHowever, given the high incidence of delinquent children with mental illness and the lack of federal Medicaid reimbursement for these youth when confined, states do notalways provide the necessary mental health treatment for delinquent youth in detention and other secure residential settings. MDLC Public Report on Evidence-Based Practicesat 11, at http://www.mdlcbalto.org/publications.htm.xxiihttp://www.oppaga.state.fl.us/reports/crime/r07-10s.html.xxiiiId. and additional information about the Florida legislation and program is available upon request to Dan Edwards or Bob Rhen at Evidence Based Associates atwww.evidencebasedassociates.com.xxivSchoenwald, S.K., Sheidow, A.S., Letourneau, E.J. (2004). Toward effective quality assurance in evidence-based practice: Links between expert consultation, therapist fidelity, and childoutcomes. Journal of Child and Adolescent Clinical Psychology, 33, 94-104.xxvhttp://www.mstservices.com/licensed_teams_by_location.php.xxviYouth Violence: A Report of the Surgeon General, Chapter 6 at http://www.surgeongeneral.gov/library/youthviolence/toc.html; Schoenwald, S.K., Sheidow, A.S., Letourneau, E.J.,Toward Effective Quality Assurance in Evidence-based Practice: Links between Expert Consultation, Therapist Fidelity, and Child Outcomes, Journal of Child and AdolescentClinical Psychology, 33, 94-104, 2004.
TOTAL BENEFITS(minus costs)
$12,855
$9,622
$4,264
$18,213

8 | Nami Beginnings | Issue 10 | Winter 2008
F E A T U R E
is burdensome on providers who prefera daily, weekly, or monthly billing ratethat CMS will not currently approve.
Despite these obstacles, at least onestate, California, is currently fundingits MST and FFT programs forMedicaid eligible children entirelyunder Medicaid using the RehabilitationOption.xxvii Providers bill through coun-ty mental health plans based on theactual minutes spent providing directservices but at a rate that is computedbased on each provider’s actual costs forproviding model-adherent MST subjectto a maximum hourly rate imposed bythe State Department of Mental Health.Los Angeles County is starting a newinitiative to provide MST to children inthe child welfare system referred to thejuvenile justice system that will also befunded entirely with Medicaid funds.
Other positive reports on billingMST under Medicaid come surprisinglyfrom providers in states that have man-aged behavioral health care where ser-vice access is usually considered moredifficult compared to fee-for-serviceMedicaid systems. MST providers inNew Mexico and Pennsylvania reportthat it has been easier to provide MSTunder managed care. Managed careorganizations (MCOs) prefer MSTbecause of the cost savings in avoidingMedicaid covered residential place-ments, the clear eligibility criteria, andthe short-term treatment approach thatstops dependence on service providersand gives caregivers the ability to man-age youth behavior. Medicaid waiversalso give MCOs the flexibility to struc-ture the funding for MST in the formof a per diem, weekly, or monthlybilling rate that is easier for providers.
A more typical description of MSTMedicaid billing comes from theDistrict of Columbia where the privateMST provider receives a portion of theestablished per diem MST rate from theDepartment of Mental Health and isexpected to bill Medicaid under aservice called Community BasedIntervention for the remaining portion.Though technically there is no capon how much the provider can billMedicaid, the per diem rate functions
as a ceiling on the provider’s reim-bursement. Although this financingmethod fully supports model-adherentMST, the provider noted the uncertaintyeach year about whether the Departmentof Mental Health budget will containthe matching funds for the program.xxviii
ConclusionMental health advocates and profes-sionals should educate state officialsand legislators both about the costeffectiveness of MST and the coverageof MST as a behavioral health careservice under Medicaid in many states.Although Medicaid dollars alone willnot likely provide a sufficient source offunding for model-adherent MST, stateshave used Medicaid as one financingstrategy, combined with state and localdollars, to sustain and expand theavailability of MST for delinquentyouth, who have a high incidence ofmental health disorders. Advocatesshould recommend that their state
implement or expand MST programsbased on a multi-faceted fundingstream that blends or “braids” multiplesources of funding at a budgetarylevel and incorporates the availableMedicaid reimbursement with othersources of funding in such a way thatmodel adherence and client outcomesare always the primary focus forevery MST clinician and programadministrator.
When presented with clear facts onthe benefits for children and familiesplus the cost-savings generated fromproviding MST services, state officialsand legislators should be willing tobudget or appropriate state dollars thatcan be combined with Medicaid reim-bursement to finance and expand MSTprograms.
Melanie Duncan, Ph.D., ProgramDevelopment Coordinator, MST Services,and Keller Strother, President, MSTServices, contributed to this article.
xxviiInformation provided by Todd Sosna with the California Institute of Mental Health, created by the California county directors of mental health to provide technical assistance,research, policy development, and training in California’s mental health system, at www.cimh.org.xxviiiInformation provided by a representative of Youth Villages, a provider of MST Services in D.C. and several states with further information at http://www.youthvillages.org/.
NAMI’S Child & Adolescent ActionCenter Releases Family Guide onEvidence-Based Practices
N AMI’s Child & AdolescentAction Center is pleased toannounce the release of a
new publication titled: A FamilyGuide ~ Choosing the Right Treatment:What Families Need to Know AboutEvidence-based Practices. The guideis designed to educate and informfamilies about evidence-basedpractices (EBPs) in children’s mentalhealth and to share informationon an array of treatment andsupport options.
NAMI received input on theguide from families and mentalhealth advocacy organizationsto ensure the development of afamily-friendly guide.
We hope that NAMI leadersand family advocates find this guidehelpful in their efforts to bring more
effective services andsupports to childrenwith mental illnessesand their families.Educated andinformed familiesare in the best posi-tion to advocate forthe most effective
treatment and supports for their child.The guide is available as a PDF
document to download on the NAMIChild & Adolescent Action Centerwebsite (www.nami.org/caac).Sections of the guide are also avail-able in Spanish online. If you wouldlike a hard copy of the Family Guide,please contact Bianca Ruffin,Program Assistant for the CAAC,at [email protected].

Winter 2008 | Issue 10 | Nami Beginnings | 9
T H E Y O U T H V O I C E
The ABC’s ofBipolarby Clara LaBrier, High School Junior Living in Colorado
All my life I wondered whatBipolar means to meCausing you to cut?Does it make you see differently?Ever since I was diagnosed with bipolarFreeing my individuality was roughGreatly I now appreciate my disorderHighly holding my head when I’ve had enoughI still don’t understand andJust in case you don’t knowKeep your “Foot prints in the sand”Losing yourself will not help you growMy mom is here for me just like yours will be tooNot a second will you deal with this aloneOverwhelmed sometimes you may want to let goPlease believe me when I say your best help is at homeQuietly or with words left unsaidRelax, but don’t give inSitting, crying on your bedThinking your disorder is a sinUneasiness will come aroundVaguely making you think wrongWildly not making a soundX-amining where you belongYou belong here with us as one big disorderZenith are the people with bipolar
Bipolar Disorderby Clara LaBrier, High School Junior Living in Colorado
Betrayed and feeling alone in your lifeI know it’s difficult to forget the pastPerhaps if you felt like you had a friendOvercoming life’s obstacles wouldn’t be so hard andLosing the you in yourself not so easy to doAfter you find yourself lost in this painReally then will you realize you aren’t insane
Dying on the inside and crying on the outI also know it’s a tough habit to live withoutSo when you are feeling alone remember who I amOr if you need a friend remember these words, “I can”Rather than the words, “I can’t”Death is the easy way outEven if you think you have it the roughestRemember you're not alone because everyone has
something to deal with
Clara LaBrier
Mental Health Curriculum for Middle Schools
T he National Institute of Mental Health(NIMH) has introduced a mental healthcurriculum supplement, The Science of
Mental Illness, to assist educators in teachingmiddle school students about mental illnesses.
Students are taught that mental illnesses arebiologically-based and no different than otherphysical illnesses and diseases. The curriculumincludes lessons about the brain, mental illnesses, factorsthat can affect the development of a mental illness, livedexperiences, and effective treatments.
An overarching aim of the program is to helpstudents understand the importance of scientificinquiry by stressing the value of scientific evidencein making important choices about their personalhealth. Students develop skills such as observation,problem solving, and critical thinking as part ofthis goal.
The web version of the curriculum anddownloadable materials can be accessed online atwww.nimh.nih.gov (click on “Health & Outreach,”then “Publications”).

10 | Nami Beginnings | Issue 10 | Winter 2008
F A M I L Y V O I C E
My family consists ofmyself, my husbandScott, our daughtersKandyce and Keniesha,and our son Kendall.
We live in Canby, a small town insouthwest Minnesota.
Our son started to struggle in schoolin first grade. He had trouble adjustingto two teachers. He became frustratedand started acting out. We, as parents,did everything possible to help him,but nothing seemed to work. Theschool told us to have him evaluatedby a mental health agency. We calledone but they would not evaluate himwithout a referral from a social worker.This would involve Family Servicesand this scared me to death for fearthey would try and remove him fromour home. I opted not to call them atthat time.
By the summer after first grade,Kendall’s behavior got much worse.He was only eight years old and want-ed to kill himself! Then, at work onenight, a customer overheard me tellinga co-worker about my concerns withmy son. He happened to be the schoolsocial worker for Canby Schools andhe offered to help. We made anappointment for an evaluation andKendall was diagnosed with attention-deficit/hyperactivity disorder (ADHD).We put him on medication (actuallyseveral) but none of them worked. Theschool social worker helped me contactFamily Services to see if there might becommunity programs available. Wewere assigned an extremely caring andunderstanding social worker.
We worked with this social workerfor about seven years and duringthat time we accessed several evidence-based interventions, including in-homebehavior therapy, family education andsupport therapy, respite care, and amentoring program. They all helpedKendall, especially the mentoringprogram.
Kendall’s diagnosis was re-evaluatedand changed from ADHD to depressionand oppositional defiant disorder (ODD).
In-Home Behavior TherapyKendall received in-home behaviortherapy designed to help him developanger coping skills. He struggled forthe first few years with the anger cop-ing therapy, but ultimately respondedquite well to this intervention.
The behavioral therapists focused onhelping Kendall develop coping skillsfor challenging behaviors. He learnedhow to cope when he was angry bytaking action like counting to tenbefore responding to someone who wasteasing him. When counting to ten didnot help, he had a series of questionsto ask himself before acting out, suchas how would your parents feel if yougot into trouble or would you like theconsequences of your actions? Helearned how to better control his frus-tration in the classroom by leaving theclassroom to get a drink and to calmdown. The behavior therapy alsotaught him how best to handle teasingfrom other students.
One of the biggest obstacles withthe in-home behavior therapy was staffturnover. Kendall struggled every timethey switched to a new in-hometherapist, which seemed to happenall too often.
Kendall continues to use the skills
he learned in the behavior therapy andhe wishes that more people could learnthe everyday coping skills that he did.
Family Education and Support TherapyThe family education and support ther-apy benefited everyone in our family.We all learned consistent strategies andsupports to help Kendall. We alsolearned to spot the early signs ofKendall’s frustration so we could helphim before he reached a completemeltdown and became uncontrollable.Some parents fear that this type oftherapy will focus on mistakes theyare making or their “bad parenting.”However, in our experience, we learnedskills that we continue to use todayand that helped us to better supportKendall.
Respite CareThe respite care program proved tobe extremely important for our family.It allowed my husband and me to taketime away from our family to care forourselves and our relationship, whilea responsible adult caretaker tookresponsibility for our children,especially our son Kendall.
It allowed us to recharge our batter-ies and return ready to address thechallenging needs of Kendall and theneeds of our other children.
The Mentoring ProgramGod Bless the mentoring program!I would have to say that the biggestinfluence for Kendall was the mentorthat Family Services and PACT 4 foundfor him. PACT 4 is a Family Servicesand Children’s Mental HealthCollaborative. The mentor assigned tomy son was awesome. He went aboveand beyond his assigned role. Kendallliked him immediately.
The mentor worked with the in-homebehavior therapists and the familysupport therapists to help ensure thatthey were all focusing on the samelessons for Kendall at the same time.What amazed us was that even whenthe mentoring program was cut
The Road to Recoveryby Laurie Bliss, Parent
Kendall Bliss

Behavior treatment involvesboth social and psychologicaltherapies. It is a very impor-tant part of treatment forattention-deficit/hyperactivity
disorder (AD/HD) in children and teens.Behavior modification or behavior
therapy is also called psychosocialtreatment. It works by changing thebehavior of a child or adolescent.Research shows that behavioral treat-ments work well for the symptoms ofAD/HD, especially when they are usedwith stimulant medication.
Treating AD/HD in children often
involves medical, educational, andbehavioral treatments used together.Treatment should be planned andcarried out only after learning whatindividual needs each child andfamily have.
Why use behavioral treatments?Behavioral treatment for AD/HD isimportant because it helps with issuessuch as:
• problems doing well in school• behavior problems at school• problems with friendships with
others their age• problems getting along with parents
and with brothers and sisters
Behavioral treatments work byteaching new skills to parents, teachersand the children for handling problems.
What is behavior modification?With behavior modification (or behav-ior therapy), parents, teachers and thechild with AD/HD learn new skills forinteracting with others. Adults teachthe child or adolescent new ways ofbehaving by changing the ways they
Winter 2008 | Issue 10 | Nami Beginnings | 11
A S K T H E D O C T O R
Behavioral Treatment for Childrenand Teenagers with AD/HDEditor’s Note: This article was reprinted with permission from CHADD (Children and Adults with Attention-Deficit/Hyperactivity Disorder) and is from the CHADD National Resource Center on AD/HD.
because of lack of funding, the mentorcontinued to work with Kendall on hisown time. He would pick Kendall up atleast one or two times a week and theywould spend time together, often onwood-working projects. They wouldalso conduct science experiments andgo fishing. The mentor taught KendallCPR, first aid, and got him interestedin politics. They still keep in touchtoday. I truly believe this person wasthe reason my son thought life wasworth living. It's hard to find a specialperson like that these days and wewere blessed to have had him workingwith Kendall.
The Importance of EvaluationsWe completed evaluations showingimproved outcomes and positiveprogress for each of the evidence-basedinterventions we accessed for Kendall.The service evaluations our familycompleted were sent to an evaluation
committee to determine the servicesthat worked best for Kendall.
The evaluations gave us the chanceto communicate with the evaluationcommittee about what was workingand making a positive difference inKendall’s life.
Policy makers and officials makingfunding decisions about services andsupports must hear from families andconsumers about the services that aremost effective and valued. The focusshould remain on those services thatproduce the best outcomes and helppeople to develop the skills andsupport they need to ultimately leadindependent and productive lives.
Recovery and Looking BackBy the time my son was in tenth gradehe was no longer taking medication.His behavior had improved dramatically.When he got extremely frustrated, heused the skills he was taught in behav-
ior therapy and in the family supportand education program. He also usedthe skills he learned from his mentorto handle extreme frustration.
In his junior year of high school,he was invited to be a page during theMinnesota legislative session. Hisinvolvement in this program greatlyincreased his self esteem. He alsojoined the Army National Guard in thesummer of his junior year. He is now21 years old and attending college inMoorhead for pre-law and politicalscience.
He has grown into a fine young manwho we are all very proud of. I thankthe school social worker, my FamilyServices worker, PACT 4, and hismentor for not giving up on him andfor working so well with our family.We are convinced that the availabilityof effective services and caring profes-sionals helped Kendall put his life onthe road to recovery.
F A M I L Y V O I C E

12 | Nami Beginnings | Issue 10 | Winter 2008
themselves respond to the child's orteen's behaviors.
Parents and teachers should bothuse the new skills at the same time toget the best results. They should all dothe following:
• Start with goals that the child cansucceed at, in small steps.
• Be consistent -- even at differenttimes of the day, in different placesand with different people around.
• Use the new skills over the longhaul -- not just for a few months.
• Remember that teaching and learningnew skills take time, and the child'simprovement will be little by little.
How does a behavior modificationprogram begin?The health professional begins bytaking a complete history of the child'sproblems at home and school andduring social activities. Most of thisinformation comes from parents andteachers. The therapist also meets withthe child to get a sense of what thechild is like.
This evaluation should end with alist of target behaviors for treatment.Target behaviors are ones that need tobe changed so the child gets better.They can be either behaviors that needto stop or new skills that need to belearned.
The areas targeted for treatment maynot be the symptoms of AD/HD (suchas being much too active, not payingattention, and doing rash or suddenthings without thinking). Instead, theymay address the problems that thosesymptoms cause in daily life, such asplaying well with brothers and sisters,or obeying parent's requests.
Similar behavioral treatments areused both at home and at school.Parents and teachers carefully watchthe child's response to the treatment.The treatment changes as the childchanges.
Parent TrainingParents need careful teaching andsupport to learn the new parentingskills and how to use them all the time.The topics covered in parent-trainingsessions may include the following:
• Setting house rules and a routine• Learning to praise wanted behaviors
and to ignore mild unwantedbehaviors (choosing your battles)
• Using appropriate ways to let thechild know what you want from himor her
• Using "when-then" directions(when there is unwanted behavior,then adults take away rewards orprivileges)
• Planning ahead and working withchildren in public places
• Using "time outs" during or afterunwanted behavior
• Using daily charts and point systemsfor both rewards and consequences
• Using a school-home note system toreward school behavior and to trackhomework
Parent training can be done ingroups with or without the child.Parent training can also happen duringindividual family sessions that includethe child. When the child is a teenager,parent training is a bit different.Parents learn skills that are right forteens. The parents and teenager maymeet with the therapist to come upwith solutions they can agree on forbehavioral problems. Parents try togain improvements in the teenager'starget behaviors (such as better gradesin school) in exchange for rewards thatthey can control (such as allowing theteenager to go out with friends).
Therapy at SchoolMany children with AD/HD haveteachers who may not know muchabout AD/HD or behavior modification.Parents of children with AD/HD shouldwork closely with teachers to helpthem learn needed skills to managebehavior in classrooms.
Managing teenagers with AD/HDin school is different from managingchildren with AD/HD. Parents willoften work with guidance counselorsor other school staff rather than theindividual teachers who will carry outthe classroom behavior modificationprograms.
Therapy with the ChildVery often children with AD/HD have
serious problems getting along withother children. Children who overcomethese problems do better in the longrun than those who don't.
Here are five good ways to helpchildren who don't get along well withother children:
1. Teach social skills (how to get alongwith other people)2. Help to solve social problems3. Teach other skills that children findimportant, such as sports skills andboard-game rules4. Decrease unwanted behaviors suchas bossiness or not sharing5. Help to form a close friendshipbetween the child with AD/HD andanother child
To best help the child, the skillsfor changing unwanted behaviorshould be the same for the parent,school, and healthcare professional.The same behaviors should be watched,discouraged or encouraged, andrewarded in all three settings.
Social skills training groups are acommon type of treatment. Social skillsgroups with children with AD/HD onlywork well when they are matched withwhat the parents and school are doingto reduce disruptive and negativebehaviors.
What about combining behaviorapproaches with medication?Both medication and behavioral treat-ment work well to improve AD/HDsymptoms. Medication alone is moreeffective in treating AD/HD symptomsthan behavioral treatment alone. Insome cases, combining the twoapproaches works best. No one treat-ment plan is right for everyone.
This What We Know fact sheet wassupported by Cooperative AgreementR04/CCR321831 from the Centers forDisease Control and Prevention (CDC).Its contents are solely the responsibilityof the authors and do not necessarilyrepresent the official views of CDC.
To access additional informationfrom the CHADD National ResourceCenter on AD/HD, please visit www.help4adhd.org.
A S K T H E D O C T O R

NAMI Illinois was extremelypleased when the NAMIChild & Adolescent ActionCenter notified us thatIllinois was one of three
target states in a project designed tobuild a family network to promote thebroader dissemination and availabilityof evidence-based practices (EBPs) inchildren’s mental health. The project isfunded by the MacArthur Foundation.We recognized the importance of EBPsand the need to bring more effectiveservices to children and adolescentsliving with mental illnesses and theirfamilies. We appreciated the opportuni-ty to play a key role in helping toeducate and inform families abouteffective treatment choices and toprovide advocacy tools to help creategreater demand for EBPs in our stateand local communities.
Launching the EBP Project at the2006 NAMI IL MeetingThe education process began at theNAMI IL Education Conference inOctober 2006 with a presentation byRon Honberg, NAMI National PolicyDirector. The presentation outlined theevidence-based practices project andhow families in Illinois could becomemore involved in advocating for thebroader availability of EBPs. It alsocovered the growing national focus oneffective interventions and the impor-tance of EBPs to children and theirfamilies.
The presentation raised the interestof NAMI Illinois members and affiliateleaders in the project and in learninghow to effectively promote the broaderdissemination of EBPs.
Planning for Onsite TA Visits withNAMI NationalIn early 2007, we worked with NAMInational to plan a series of onsite meet-ings on EBPs in children’s mentalhealth with key stakeholders in Illinois.
We recognized the critical need toinclude just the right mix of stakehold-ers for the late spring onsite meetings.Our job was made easier by theexistence of the Illinois Children’sMental Health Partnership (ICMHP),which consists of representatives fromthe key state child-serving agencies andfamily advocacy groups. The ICMHPhas been an extremely influentialstate-wide group working to reformchildren’s mental health in Illinois.
In planning for meetings related tothe EBP project, we also collaboratedwith the Division of Mental Healthand learned that they had formed acommittee on evidence-informed prac-tices, essentially looking at bringingmore effective interventions intoIllinois. We wanted to be sure that ourNAMI onsite meetings would includekey members of the state committeefocused on EBPs. We were alsoextremely fortunate to have BarbaraBurns, Ph.D., a leading national experton evidence-based practices inchildren’s mental health, involved withNAMI national on this project.
In working with NAMI national,we ultimately decided to hold threeseparate meetings as part of the onsitetechnical assistance on EBPs. The firstmeeting was held with representativesfrom the FACE (Family Advocacy,Communication and Education)committee of the ICMHP and withrepresentatives from the Evidence-Informed Practice Committee of theDivision of Mental Health. The secondmeeting was held with representativesfrom the ICMHP and the Division ofMental Health and the third meetingwas held with families and advocacygroups from around the state.
The three onsite meetings were heldover two days in April. Dr. Burns andNAMI national participated in all threemeetings. Dr. Burns provided excellentpresentations and shared her expertiseon EBPs in children’s mental health.
Participants got to engage in a dialoguewith Dr. Burns and other key stake-holders during all the meetings.
At the first meeting, Amy Starin, theAdministrator for Child & AdolescentServices in the Illinois Division ofMental Health, provided an overviewof the work being done by the state tofocus on evidence-based interventions.The state completed a survey ofproviders on EBPs. The responsesshowed that 92% of providers wereinterested or very interested in learningmore about EBPs. The state is engagingin a five-pronged approach to address-ing evidence-based practices in thechildren’s mental health service system,which includes the following activities:
1. Providing ten mental healthagencies around the state with grantsto train and supervise providers in theskills involved in two evidence-basedinterventions — cognitive behavioraltherapy (CBT) and behavior parenttraining;
2. Educating child and adolescentmental health providers on evidence-based interventions. The state foundthat many child mental healthproviders do not understand EBPs andthat myths surrounding EBPs thatcould prevent families from accessingeffective treatment options needed tobe dispelled;
3. Supporting the development ofan EBP certification process in threegraduate schools to ensure that mentalhealth providers are adequately trainedin EBPs and can provide these servicescoming out of school. The graduateschools are interested in expanding theproject to provide ongoing training forproviders practicing in the field;
4. Looking at state level policies tosee how they might support or hinderthe use of evidence-based interven-tions. The state’s committee on EBPswill develop resources on the steps thatmust be taken to ensure a culturethat promotes the implementation of
Promoting Evidence-Based Practicesin Illinoisby Lora Thomas, Executive Director, NAMI Illinois
Winter 2008 | Issue 10 | Nami Beginnings | 13
S T A T E N E W S

In 1995, NAMI Orange Countyrecognized the need to teachstudents in schools about seriousmental illnesses. Many of ouraffiliate members were current
or former teachers so this seemed alogical target for our work.
We started the process by lookingat what other NAMI groups were doingaround the country. We recognized thatteachers are being asked to do moreand more these days, so rather thantry to convince teachers to shareinformation about serious mentalillness with students; we offered to doit for them. We volunteered to cometo the classroom and teach a lessonabout mental illnesses.
Our beginnings were humble.A group of interested volunteers met,made some decisions about what the
lesson would look like, and beganoffering our services to schools. Ourgoals were:• To help teachers and students
identify and understand the symp-toms of and treatments for mentalillness;
• To reduce the myths and stigma ofmental illness, to open minds, andto reduce discrimination;
• To encourage those experiencingsymptoms of a mental illness toseek treatment when needed;
• To raise awareness among youthabout NAMI Orange County sothey could take advantage of ouravailable resources; and
• To ensure that students wouldbecome adults that better under-stood mental illnesses and theimpact they have on society.We wanted to make sure that
students understood that mentalillnesses are physical illnesses of thebrain and that most individuals livingwith them are not dangerous. Oureffort has grown into a team of about40 volunteers, who meet quarterlyand reach from 3,000 to 6,000 studentsa year.
Some changes have occurred inour outreach efforts over the years.We developed additional materials andhired a part-time program coordinatorafter securing a few grants. We addedposters, overheads, and visuals to thelessons, thanks to volunteer graphicartists. A skilled NAMI member createda video titled, The Many Faces of MentalIllness, using a local psychiatrist andsome talented volunteer actors. One ofour volunteers taped a presentation forstudents so we could show it to newvolunteers. Our program also uses an
14 | Nami Beginnings | Issue 10 | Winter 2008
A F F I L I A T E N E W S
Reaching and Teaching Studentsabout Mental Illnessesby Donna Pollard, Program Director & Parents and Teachers as Allies Trainer,NAMI Orange County, California
evidence-based practices; and5. Educating families and consumers
on EBPs to create demand by encour-aging community providers to becomebetter trained and informed on EBPs.
NAMI national’s initiative to bring in aleading national expert on EBPs andeducate families and consumers aboutEBPs complimented the work alreadyunderway in Illinois. The FACE com-mittee and the Division of MentalHealth proved to be extremely valuablepartners, both in planning for the onsitemeetings and during the meetings.
The second meeting of the onsitevisit included the state Division ofMental Health and representatives fromthe Illinois Children’s Mental HealthPartnership. We were extremelypleased to have Barbara Shaw, the chairof the Illinois Children’s Mental Health
partnership, participating in thismeeting. Barbara Shaw has proven tobe a tremendous leader in workingto transform children’s mental healthin Illinois.
The third meeting focused onfamilies and included family advocacyleaders from across the state. There wereNAMI members and leaders, and repre-sentatives from the Illinois Federationof Families for Children’s Mental Health,Voices for Illinois Children, and otherkey groups. Dr. Burns provided anoverview of EBPs and discussed thecritical need for families to become moreinvolved in advocating for the broaderdissemination of EBPs. NAMI sharedinformation about the developmentof family resources designed to helpeducate and inform families about EBPs.
We were extremely pleased to haveDr. Burns leading the three onsite
meetings. Her national prominenceand expertise on EBPs in children’smental health helped to secure a strongturnout for these meetings. The formatof holding three meetings allowedus to meet with key stakeholders tostrategize on collaborating to ensurethe broader availability of EBPs forchildren with mental illnesses andfamilies.
We continue to work in Illinois toeducate and inform families aboutEBPs. Our ultimate goal is to improvethe treatment and service outcomes forchildren and adolescents living withmental illnesses.
To learn more about NAMI Illinois’work on this EBP project, pleasecontact Lora Thomas, NAMI IllinoisExecutive Director, at 217.522.1403 [email protected].
S T A T E N E W S

evaluation tool to help us track theeffectiveness of our program and toreport to organizations that haveprovided funding for it.
We receive many positive com-ments about our program — here aretwo of the comments:• “Your presentation was informative
and educational. I believe it isessential to educate people (espe-cially teenagers) about mentaldisorders and you do an excellentjob. Your presentation was verytouching”— from a Student.
• “I want to thank you and NAMIOrange County for speaking to myhealth classes — students bondwith real life stories because theinformation comes alive. Mysincerest thanks and appreciationto you for sharing your time andknowledge” — from a Teacher.
A school outreach volunteer maybe a family member, a professional, aperson who has had an illness, or anycombination of the above. While wehave many education professionalsinvolved in our program, we also havelawyers, business professionals, doc-tors, and others. Volunteers interestedin delivering the program must firstattend an orientation meeting, observeanother volunteer delivering theprogram, and do a presentation with amentor. Volunteers create their ownlesson plans using suggestions includ-ed in our volunteer notebooks and bymeeting our program goals. Eachvolunteer brings something unique andspecial to the classroom.
At a recent quarterly volunteermeeting, volunteers were asked toshare how they had benefited fromvolunteering for the program. Hereare just a few of the comments:• It’s life affirming.• I benefit more than others.• I am able to make a difference.• I am becoming more empowered.• We’re here to serve, a big honor.• I’ve stretched!• Sharing has lessened my denial.
I’m healthier.
These comments and othersshow an unexpected benefit from ourprogram — that not just students gain,but volunteers do as well.
It is impossible to know the trueimpact of our program and whether itimproves help-seeking behaviors, butthere are a number of instances whenstudents have self-disclosed mentalhealth concerns to our volunteers. Ourvolunteers assist students in findinghelp if it seems appropriate. Studentsalso always receive a brochure withreferral information at the end of ourpresentations. We know of a few stu-dents living with mental illnesses whohave received treatment as a result ofour program. We believe that if wereach just one student, then our workis well worth the effort.
Most of our presentations are donein high schools, but we have presentedto elementary (even kindergarten!) andmiddle schools with some college level
classes thrown in. While we have onlyscratched the surface of the program’spotential, we believe that we havemade a difference and we will continueour outreach efforts with younger andmore students. We have some teacherswho ask us to come back every semes-ter. We have also been extremely activewith NAMI’s Parents and Teachers asAllies in-service education program forschool professionals.
Another school year is upon us andwe hope that this year will be biggerthan ever for our outreach work in theschools.
To learn more about NAMIOrange County’s outreach programfor students, please contact DonnaPollard at (714) 544-8488 or [email protected].
List Price: $16.95Soft Cover: 260 Pages (2004)Publisher: Guilford Press
What a fitting title fora book that providesfamilies with theessential tools to copewith the challenges
of raising a child with depression orbipolar disorder. Dr. Mary Fristad andDr. Jill Goldberg Arnold understandthe extreme day-to-day difficultiesexperienced by families when a childis living with bipolar disorder ordepression.
This book provides families withnumerous practical approaches onhow to effectively address the needsof their child, along with the needs ofother family members impacted by theexistence of these serious illnesses.
Early in the book, the authors helpfamilies understand what is happeningwith their child and the steps neces-sary to get good treatment and a
proper evaluation.The book coverseffective treatmentoptions for depres-sion and bipolardisorder, includingmedication, psy-chotherapy, andcombined interven-tions. The real
benefit of this book is the practicaltips for parents, family exercises, andcoping skills for the child. Familieswill also greatly benefit from thechapter on strategies for helpingstudents with depression and bipolardisorder succeed in school.
Dr. Mary Fristad and Dr. JillGoldberg Arnold understand andappreciate the vital role that familiesplay when children are diagnosedwith depression and bipolar disorder.This book is chock-full of guidanceand practical advice that promises tomake life easier for families raisingchildren with these conditions.
Raising a Moody Child: How to Cope withDepression and Bipolar Disorderby Mary Fristad, Ph.D. and Jill S. Goldberg Arnold, Ph.D.
A F F I L I A T E N E W S
Winter 2008 | Issue 10 | Nami Beginnings | 15
B O O K R E V I E W

This publication is funded by an unrestricted educational grant from McNeil Pediatrics Division of McNeil-PPC, Inc.According to NAMI policy, acceptance of funds does not imply endorsement of any business practice or product.
Colonial Place Three2107 Wilson Blvd., Suite 300Arlington, VA 22201-3042703.524.7600 • www.nami.org
Non-Profit Org.U.S. Postage
PAIDPPCO24506
National Children’s Mental HealthAwareness Day
N AMI, a founding partner in acoalition of national mentalhealth, counseling and educa-
tion organizations, jointly hosted thesecond annual Capitol Hill briefingin honor of National Children’sMental Health Awareness Day. Theprogram emphasized the criticalimportance of effective school andcommunity-based mental healthservices for children, youth, andtheir families.
The briefing, Children’s MentalHealth: Key to Achieving Success inSchools and the Community, was heldon May 8th and focused on raisingawareness about effective programsfor children’s mental health needs,demonstrating how children’s mentalhealth initiatives promote positiveyouth development, recovery andresilience, and showing how childrenand youth with mental health needscan thrive in their communities.
Guest speakers included:• Moderator: Carl C. Bell, M.D.• Honorary Consumer
Spokesperson: Howie Mandel• Honorary Family Spokespersons:
Deborah Marriott Harrison andher son Scott
• Honorary Youth Spokesperson:Marvin Alexander
• Honorary Education Spokesperson:Mark Weist, Ph.D.
• Substance Abuse and MentalHealth Services AdministrationSpokesperson: Gary M. Blau, Ph.D.The briefing was an enormous
success! Mark your calendars fornext year’s National Children’sMental Health Awareness Day onMay 8th, 2008! Stay tuned formore details.
Anti-Bullying WebsiteTargets Youth
T he U.S. Department of Healthand Human Services, HealthResources and Services
Administration (HRSA) developed aninteractive website for youth thatteaches them about bullying and howto prevent it. The website is part ofHRSA’s anti-bullying campaign, TakeA Stand. Lend A Hand. Stop BullyingNow!, which aims to educate moreAmericans about how to preventbullying and youth violence.
The website includes animatedstories, games, quizzes, fact sheets, andan “ask the expert” section to help youth
identify what bullying isand what they can doabout it, whether theyare witnessing it, being
bullied, or are the bullies themselves.A team of youth experts, ages 9 to 13,provided input on the campaign’swebsite to ensure it reflected real lifeand would appeal to youth.
Parents can also visit the websiteto learn how to become a part ofthe anti-bullying campaign and bringactivities and resources that helpaddress the issue of bullying to theirlocal school and community.
To access the anti-bullying websitevisit www.stopbullyingnow.hrsa.gov.
NAMI’s Executive Director, MikeFitzpatrick (far left), poses with HowieMandel (middle and also featured on thecover), the host of NBC’s hit show “Dealor No Deal,” along with (from left to right) Robert Bernstein, Executive Director
of the Bazelon Center for Mental Health Law, Sandra Spencer, ExecutiveDirector of the Federation of Families for Children’s Mental Health and David
Shern, President and CEO of Mental Health America.