
MWM+PIR
22
treatment of Mobilization with Movement (MWM) and Post isometric Relaxation(PIR) with MWM alone and PIR alone for Painful Stiff Shoulder Presented By: Guided By: Devdeep Ahuja Dr.Dheeraj KV Sumanjeet Arora
description
jhbh
Transcript of MWM+PIR

Comparison of the effectiveness of a combined treatment of Mobilization with Movement (MWM) and
Post isometric Relaxation(PIR) with MWM alone and PIR alone for
Painful Stiff Shoulder
Presented By: Guided By:
Devdeep Ahuja Dr.Dheeraj KV
Sumanjeet Arora

Aim of the study
To study and compare the effects of Mobilization with Movement (MWM) and Post isometric relaxation (PIR) in patients with painful stiff shoulders.

Hypothesis
Combined treatment of MWM and PIR gives better results in cases of painful stiff shoulder than either MWM alone or PIR alone.

Design
Study is experimental in nature.
Combined effects of MWM and PIR compared with MWM alone and PIR alone. The control group received conventional exercise and stretching regime.

VariablesIndependent Variables
MWM & PIR MWM PIR
Dependent variables Visual Analog Scale (VAS) Shoulder Pain & Disability Index (SPADI) Percentage change in ROM
Control variables Active exercises Cold packs Stretching

Sampling
Sample size –total 60 (15 in each group)
Stratification done using RALLOC software by a statistician.
Allocation to four groups Group A – MWM + PIR Group B – MWM Group C –PIR Group D- Controlled

Inclusion Criteria
Pain & stiffness in the shoulder
Age 40-70yrs
No previous shoulder surgery
Symptoms for at least 3 months duration

Exclusion criteriaAny significant systemic history affecting shoulder
Myocardial infarction Osteoporosis Rheumatoid arthritis Stroke
Either shoulder documented Grade III rotator cuff tear Fractures around the shoulder
Thoracic outlet syndromeSevere skin allergies, sensitivity or other dermatological problems in the area.Trauma or any other predisposing event.

Interventions
MWM• Identification of restricted movement• Appropriate glide applied• 3 sets of ten repetition
PIR• Identification of restricted movement• 5 sec isometric hold , 2-3 sec relaxation with
exhalation • 6-10 repetitions
MWM + PIR • Both the protocols followed
• Half of the patients given MWM first, rest given PIR first to minimize the order bias
CONTROL GROUP• Cold packs
• Active exercises
• Codman’s pendular exercises
• Stretching exercises
• Strengthening exercises

Data Analysis
Two Way ANOVA was used at 5% level of Significance

ResultsOn all the parameters (percentage change in flexion, abduction, Internal Rotation, External rotation, SPADI & VAS) the experimental groups that are MWM, PIR, & the combination had significant difference in effectiveness as compared to the control.
In flexion and External rotation, the combination group gave better results than MWM alone.
In Abduction, no difference was found among the three.
In internal rotation MWM was more effective than PIR alone.
On SPADI score no significant difference was found between the three experimental groups.
On VAS, the combination was more effective when compared to MWM alone.

Percentage Change In Flexion ROM
0
10
20
30
40
50
MWM PIR MWM+PIR CONTROL
Treatment Group
Trea
tmen
t M
ean
Series1
Percentage Change In Abduction ROM
0
10
20
30
40
50
60
MWM PIR MWM+PIR CONTROL
Treatment Group
Tre
atm
ent
Mea
n
Series1

Percentage Change In Internal rotation ROM
051015202530354045
MWM PIR MWM+PIR CONTROL
Treatment Group
Trea
tmen
t M
ean
Series1
Percentage Change In External Rotation ROM
0
10
20
30
40
50
60
MWM PIR MWM+PIR CONTROL
Treatment Group
Tre
atm
ent
Mea
n
Series1
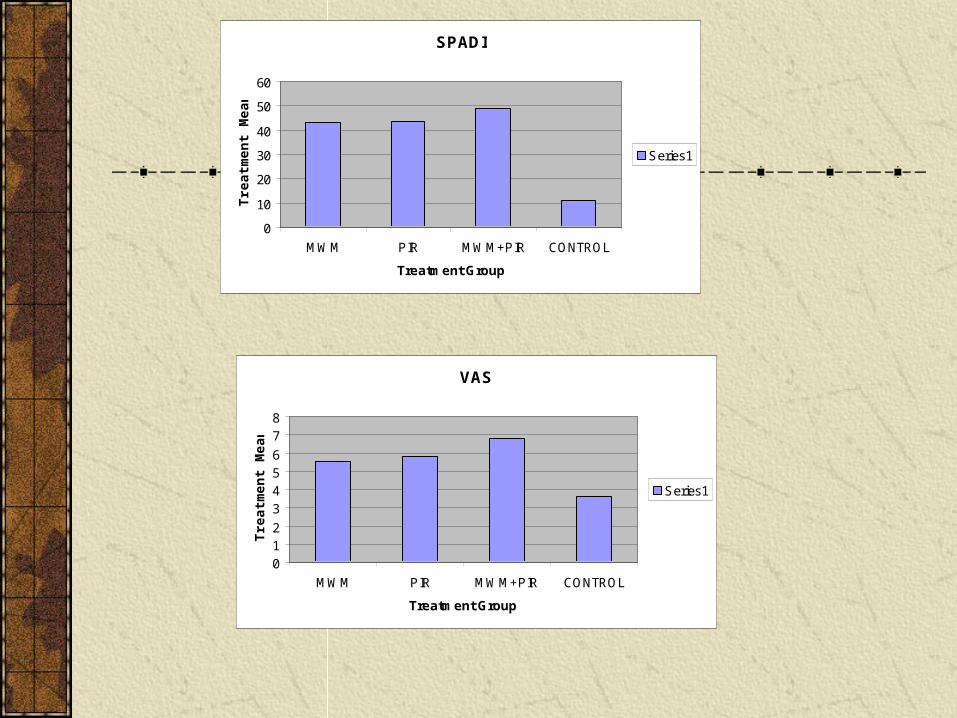
SPADI
0
10
20
30
40
50
60
MWM PIR MWM+PIR CONTROL
Treatment Group
Trea
tmen
t M
ean
Series1
VAS
012
3456
78
MWM PIR MWM+PIR CONTROL
Treatment Group
Trea
tmen
t M
ean
Series1

DiscussionIndividually used both MWM & PIR have been successful in the
management of musculoskeletal pain & joint restriction but there are no published studies
to see the effect of their combination. MWM is based on the Mulligan’s principle that a minor positional fault of the joint may occur
following an injury or strain Abbott 2001 postulated that MWM may act neurophysiologically to decrease the level of contractile
activity of shoulder rotator muscles. Wright 1995 had postulated that mechanism responsible for manual therapy treatment
effects may feasibly involve changes in the joint, muscle, pain & motor control systems Liebenson stated that PIR can relax an overactive muscle or its associated fascia, when
connective tissue or viscoelastic changes have occurred.

Our study used both MWM and PIR with the aim of addressing both the joint and soft tissue problems simultaneously and this could explain the result why combination treatment proved better than either MWM or PIR alone or the control group.
We wish to continue our study for follow up of the results at 3, 6, 9, 12 months to assess the long term effects of the results we have obtained and how far these can be retained

LimitationsSample size was very small(N=60)
No follow up was done
Doubt about the applicability and generazibility of this study to all age groups and both sexes.

Scope For Future Study 1. The study can be done with a larger sample size.
2. The study can be followed up to see the long term effect of the results obtained.
3. The study can be carried out on males and females individually to see its effects on different sexes.
4. The study can be carried out with EMG study during PIR to understand the basic mechanisms involved.
5. The study can be carried on other joints to see its overall effects
ConclusionWith our study we come to a conclusion that combination of MWM and PIR is much better than MWM alone and PIR alone for the reasons as stated in the discussion. We could thereby conclude that practicing MWM and PIR together in patients with painful stiff shoulder would enhance the recovery of the patients and thereby reduce the number of sittings required as well.

THANK
YOU


















