
Mutual of Omaha Plaza, Omaha, NE 68175 · · Mail application and appropriate forms to: Mutual of...
20
Mutual of Omaha Insurance Company Mutual of Omaha Plaza, Omaha, NE 68175 CRITICAL ILLNESS Application for Critical Illness Insurance MISSOURI · Authorization to Disclose Personal Information (HIPAA)/ MIB Authorization Form · Agent Producer Statement · HIV Consent Form (if applicable) · Other State Special Forms (if applicable) required forms to be submitted required forms left with applicant(s) Application Package Contains: · Pre-Notices · HIV Consent Form (if applicable) · Summary(ies)/Outline(s) of Coverage · Other State Special Forms (if applicable) The following forms can be downloaded from Sales Professional Access (SPA) at www.mutualofomaha.com as needed to accompany the application: · Foreign Travel Questionnaire · Replacement Notice forms that may be requested, but are not included within this package MAP567_MO · Submit the fully completed application and applicable completed forms. Unanswered questions on the application or missing or incomplete forms will result in underwriting delays. · If a question does not apply to your client, answer it as “No” or “None” rather than “N/A.” · Mail application and appropriate forms to: Mutual of Omaha Insurance Company, Records/Mailing Processing Center, 9330 State Highway 133, Blair, NE 68008-6179. · Fax application to 402-997-1804 and verify the correct facsimile number is dialed to protect the privacy of the information. Please note: use the maximum resolution to ensure the readability of the application. Application Instructions: For benefits amounts of $100,000 or more, complete the Underwriting Requirements section of the Agent/Producer Statement: · Initiate the Client Interview with the Proposed Insured- Call 1-800-775-3000 · Initiate Blood Profile/Urinalysis/Physical/Oral Fluid Test with approved Paramed Facility Additional Application Instructions (if applicable):
Transcript of Mutual of Omaha Plaza, Omaha, NE 68175 · · Mail application and appropriate forms to: Mutual of...

Mutual of Omaha Insurance CompanyMutual of Omaha Plaza, Omaha, NE 68175
CRITICAL ILLNESS
Application for Critical Illness Insurance
MISSOURI
· Authorization to Disclose Personal Information (HIPAA)/ MIB Authorization Form
· Agent Producer Statement
· HIV Consent Form (if applicable)
· Other State Special Forms (if applicable)
required forms to be submitted required forms left with applicant(s)Application Package Contains:
· Pre-Notices
· HIV Consent Form (if applicable)
· Summary(ies)/Outline(s) of Coverage
· Other State Special Forms (if applicable)
The following forms can be downloaded from Sales Professional Access (SPA) at www.mutualofomaha.com as needed to accompany the application:
· Foreign Travel Questionnaire · Replacement Notice
forms that may be requested, but are not included within this package
MAP567_MO
· Submit the fully completed application and applicable completed forms. Unanswered questions on the application or missing or incomplete forms will result in underwriting delays.
· If a question does not apply to your client, answer it as “No” or “None” rather than “N/A.”
· Mail application and appropriate forms to: Mutual of Omaha Insurance Company, Records/Mailing Processing Center, 9330 State Highway 133, Blair, NE 68008-6179.
· Fax application to 402-997-1804 and verify the correct facsimile number is dialed to protect the privacy of the information. Please note: use the maximum resolution to ensure the readability of the application.
Application Instructions:
For benefits amounts of $100,000 or more, complete the Underwriting Requirements section of the Agent/Producer Statement:
· Initiate the Client Interview with the Proposed Insured- Call 1-800-775-3000
· Initiate Blood Profile/Urinalysis/Physical/Oral Fluid Test with approved Paramed Facility
Additional Application Instructions (if applicable):

AGENT/PRODUCER STATEMENT
COMMISSION INFORMATION
Producer Name ___________________________________________ Production Number ____________________________
Social Security Number ____________________________________ Commission % Share ___________________________
If second producer, please complete below:
Producer Name ___________________________________________ Production Number ____________________________
Social Security Number ____________________________________ Commission % Share ___________________________
CONTACT INFORMATION
Division Office/MGA ___________________________________________ Phone Number _________________________________
Contact (if different than above, who should we contact on this case)
Name _______________________________________________________ Phone Number _________________________________
E-mail Address _______________________________________________
Proposed Insured: __________________________________________________________________________________________
UNDERWRITING REQUIREMENTS
Please check the underwriting requirements that have been ordered if applicable:
If benefit amount is $100,000 or more, has the client profile interview(s) been completed?......................... Yes No
If “No,” the client profile interview has been scheduled for __________ and ___________ Date Time (Indicate time zone below:
Eastern Central Mountain Pacific)
Has a medical examination of the person(s) proposed for insurance been scheduled? ................................ Yes No
If “Yes,” when? ________________________________________ By ______________________________________________
Type of Requirement:
Client Interview (call 1-800-775-3000)
Blood Urine Profile Physical Data Oral Fluid Test Ordered Through:
American Para Professional Systems (APPS) 1-800-635-1677
Hooper Holmes 1-800-765-1010
Exam One 1-877-933-9261
Examination Management Services, Inc. (EMSI) 1-800-872-3674
Superior Mobile Medics 1-800-898-3926 Long Form
EKG
ADDITIONAL INFORMATION
Do you have any reason to believe the policy applied for has replaced or will replace any existing insurance? ................................................................................................................................................. Yes NoNOTE: If Yes, fulfill all state requirements.
Has the MIB, Inc. Pre-Notice (and Notice of Information Practices, where applicable) been provided to the Proposed Insured?.......................................................................................................................... Yes No
If applying with spouse, enter spouse's name _______________________________________________________________

ADDITIONAL INFORMATION (continued)
Comments or Special Instructions:
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Agent/Producer Signature ______________________________________ Date ____________________________________ Month/Day/Year
Agent/Producer Signature ______________________________________ Date ____________________________________ Month/Day/Year
Critical Illness Insurance ApplicationApplication toMutual of Omaha Insurance Company Addition to Existing Coverage Application for policy form(s)Mutual of Omaha Plaza ____________________ CIOmaha, NE 68175 (Policy Number) CI1
Section A General Questions
1 Proposed Insured’s Name _______________________________________________________________________________First Middle Last
2 Home Phone Number ( ______ ) __________________________________ State of Birth __________________Area Code
3 Legal Residence Address ________________________________________________________________________________Number Street City State ZIP Code
E-mail Address ________________________________________________________________________________________
4 Mailing Address for Premium Notices _____________________________________________________________________Number Street City State ZIP Code
5 Is each person proposed for insurance a citizen of the United States? ................................................... Yes NoIf “No,” do all non-citizens have an alien registration receipt “Permanent Visa”? .................................. Yes No
If “Yes,” Name ________________ Permanent Visa Number ____________ Date of arrival in United States ___________
If “Yes,” Name ________________ Permanent Visa Number ____________ Date of arrival in United States ___________
6 Occupation _____________________________________ Duties _______________________________________________
Your Income _________ Spouse’s Income ___________ Household Income _________ Mortgage Balance ___________Are you currently engaged in your occupation on an active full-time basis (30 or more hours per week)? Yes No
(If “No,” explain including date of last full-time work.)
______________________________________________________________________________________________________
Name of your firm or employer and address ________________________________________________________________
Work Phone Number ( ______ ) ___________________________________Area Code
Spouse’s Occupation _____________________________ Spouse’s Duties _______________________________________
Is your spouse currently engaged in his/her occupation on an active full-time basis (30 or more hours per week)? Yes No (If “No,” explain including date of last full-time work.) _____________________________________________________________________________________________________Name of spouse’s firm or employer and address ____________________________________________________________
7 Please complete for all persons proposed for insurance.
Name (First/Middle/Last) Social Security Number Relationship to Proposed Insured Birth Date Mo./Day/Yr. Age Sex Ht. Wt.
Self
Spouse
Section B Underwriting Information
1 Has any person proposed for insurance ever received medical care for or had the following conditions: (Check all that apply. Provide explanation for all checked boxes in number 9.)
Alcoholism Eye or Ear Disorder Psychological, Emotional or Nervous condition Anemia Heart Disease Paralysis or Numbness Arthritis High Blood Pressure Prostate Disorder Back Disorder Kidney Disorder Respiratory Disorder Breast Disease or Disorder Liver Disorder Stroke or TIA (Transient Ischemic Attack) Cancer Major Organ Transplant Tumor, Polyp or Growth Diabetes Multiple Sclerosis None of These Digestive Disorder
MA5842000000 -1-
Manager/Commission Code District Sales Manager/Associate Marketer Application Reviewed By (Required Field for Brokerage)
MA5842000000 -2-
Section B Underwriting Information (Continued)
2 Has any person proposed for insurance ever been diagnosed or treated by a member of the medical profession as having Acquired Immune Deficiency Syndrome (AIDS), AIDS Related Complex (ARC) or Human Immunodeficiency Virus (HIV) infection (symptomatic or asymptomatic)? ..................................... Yes No (If “Yes,” provide explanation in number 9.)
3 During the past 10 years, other than shown in B1 and B2, has any person proposed for insurance: (Check all that apply. Provide explanation for all checked boxes in number 9.)
Been diagnosed or treated by a health care provider (including a Medical Doctor, Chiropractor, Psychologist, Podiatrist or other health care professional)?
Had or been advised to seek treatment for any illness, injury or disorder? Had surgery? Been hospitalized? Had a medical examination, diagnostic or medical evaluation or received medical care? None of These
4 Have any proposed insureds’ natural parents, brothers or sisters, either living or deceased, been diagnosed prior to age 60 with any of the conditions from the following list? Diabetes, heart disease, stroke, kidney disease or cancer (other than skin cancer)? ................................. Yes No
Person Proposed For Insurance Family Member/Relationship Diagnosis Age at Time of Diagnosis
5 (a) Within the past six months, has any person proposed for insurance taken any prescription medication? . Yes No If “Yes,” please list below. (Attach a separate signed sheet if necessary.)
Person Proposed Medication Name (Copy Dosage/ Prescribing Phone For Insurance From Pharmacy Label) Frequency Date Physician Number Reason
(b) Within the past six months, has any person proposed for insurance taken any over-the-counter drugs on a regular basis? ................................................................................................................... Yes No
If “Yes,” please list below. (Attach a separate signed sheet if necessary.)
Person Proposed For Insurance Medication Name Dosage/Frequency Reason
6 During the past 12 months, has any person proposed for insurance used:(a) any form of tobacco? .......................................................................................................................... Yes No(b) any form of nicotine replacement therapy (for example – nicotine gum, patch or spray)? .................... Yes NoIf you answered “Yes” in 6 (a) or (b), please provide details below.
Person Proposed For Insurance What Form Number Per Day Stopped On
7 During the past 10 years, has any person proposed for insurance used unlawful drugs in any form (including cocaine and hallucinogens) or used prescription drugs other than as prescribed (including sedatives, tranquilizers, or narcotics) in any form? ................................................................... Yes No (If “Yes,” provide explanation in number 9.)
8 Is any person proposed for insurance pregnant? ....................................................................................... Yes No If “Yes,” history of complications? ............................................................................................................. Yes No
(If “Yes,” provide explanation in number 9.)
9 Complete this section to provide additional information on questions 1, 2, 3, 7 and 8 in Section B.(Attach a separate signed sheet if necessary.)
Person Proposed For Insurance Condition(s) Provider, City/State Phone Number
req57806
Line
req57806
Line
req57806
Line
req57806
Line
Section C Plan Information (Availability of plan and riders is subject to change.)
Complete for Proposed Insured Yes NoBase Policy Benefit Amount $_________________Accidental Death & Dismemberment Benefit Rider .... AD&D Benefit Rider Amount $_______________Disability Benefit Rider .......................................... Hospital Confinement Benefit Rider .......................
Premium Collected $ _________________ Premium Collected $ _________________
Renewal Premium $ _________________ Renewal Premium $ _________________
Billing Mode BSP Annual Semi-Annual Quarterly PRD
Section D Other Coverage Information
1 Does any person proposed for insurance currently have, or is such person applying for, Critical Illness (lump-sum diagnostic benefits) coverage with any company? .................................................................. Yes No
If “Yes,” give details including the name(s) of such person(s), name of the company, policy/plan number and termination date. ___________________________________________________________________________
_____________________________________________________________________________________________________
2 Is any person proposed for insurance purchasing this insurance to replace any existing insurance? ......... Yes No
(a) If “Yes,” give details, including the name(s) of such person(s), name of the company, policy/plan number and termination date. ________________________________________________________________________
_________________________________________________________________________________________________
(b) If “Yes,” has each person proposed for insurance received a copy of the Notice of Replacement (if required in your state)? ................................................................................................................. Yes No
3 Is any person proposed for insurance eligible for, or receiving benefits from, Medicare or Medicaid? ....... Yes No
If “Yes,” please provide name(s) of individual(s) and details. __________________________________________________
_____________________________________________________________________________________________________
4 Has each person proposed for insurance received the appropriate Outline/Summary of Coverage? ......... Yes No
5 Complete only for Association or Franchise Coverage
I/We belong to the _______________________________________________________ Date joined __________________ (Full Name of Organization) (Mo.) (Yr.)
6 Full name of your beneficiary ____________________________________________________________________________
Relationship __________________________________________________________________________________________
7 If the spouse is a proposed insured, the full name of spouse’s beneficiary ______________________________________
Relationship __________________________________________________________________________________________
MA5842000000 -3-
Complete for Spouse (if a Proposed Insured) Yes NoBase Policy Benefit Amount $_________________Accidental Death & Dismemberment Benefit Rider .... AD&D Benefit Rider Amount $_______________Disability Benefit Rider .......................................... Hospital Confinement Benefit Rider .......................
Section E Agreement & Fraud Warning
Agreements – I/We, the undersigned, and the undersigned Producer(s), agree that (a) all answers in this application are true and complete and Mutual of Omaha Insurance Company will rely upon these answers to determine insurability, and (b) incorrect or misleading answers may void this application and any policy issued from its effective date.
If the full initial premium is paid on the date of the completed application and I am eligible for the insurance policy applied for in accordance with the health and accident underwriting standards of Mutual of Omaha Insurance Company in effect on the date of the application, the effective date of the policy will be the date of the application, or, if later, the expiration of any replaced coverage. I agree no temporary or interim insurance of any kind will be in effect.
In order for Mutual of Omaha Insurance Company to issue a policy as a result of this application, (a) the person proposed for insurance must complete all required examinations and tests (medical, paramedical, laboratory), and (b) Mutual of Omaha Insurance Company must receive the reports from all required examinations and tests, and any other information (such as an Attending Physician’s Statement) that it requires, and (c) the application must be approved for issue by Mutual of Omaha’s Underwriting Department. If all of these requirements are met, the underwriting standards of Mutual of Omaha will not apply to changes in health after the application date. If I am not eligible for the insurance applied for, I agree that no policy of any kind will be in effect unless a substitute policy is issued and accepted by me upon delivery.
I have received the Notice of Information Practices and the MIB, Inc. Pre-Notice.
No Producer can: (a) waive or change any Receipt; or (b) agree to issue a policy.
Fraud Warning – Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
I/We have: (a) read the Agreement and Fraud Warning Section and the Receipt; and (b) read and approved the answers as recorded on this application.
Signed at ______________________________________________________________ Date _____________________________ (City) (State)
________________________________________________ _________________________________________________ Signature of Proposed Insured Signature of Spouse (If Proposed for Insurance)
I/We, the Producer(s), also certify that, during an in-person interview with the person(s) proposed for insurance, I/we asked each question exactly as written and recorded the answers provided by the person(s) proposed for insurance completely and accurately. Yes No
(If “No,” please explain.) ___________________________________________________________________________________
________________________________________________________________________________________________________
X _______________________________________________ X ________________________________________________ Producer’s Signature Producer’s Signature
________________________________________________ _________________________________________________ (Date) Mo./Day/Yr. (Date) Mo./Day/Yr.
________________________________________________ _________________________________________________ Office Name Office Name
________________________________________________ _________________________________________________ Office Address Office Address
MA5842000000 -4-
M28560
PAYMENT AUTHORIZATION FORM
Payor Information
Name of payor as shown on bank account: ______________________________ Social Security No. __________________ If premium is NOT paid by Proposed Insured/Insured, indicate the bank account owner's relationship to Proposed Insured/ Insured by selecting one of the following. (Additional documentation required) Employer Living Trust Business owned by Proposed Insured/Insured or Spouse Other _______________________________________
Power of Attorney or legal guardian
Complete this form only when authorizing a bank account withdrawal for premium payment.
I authorize Mutual of Omaha Insurance Company ("Mutual of Omaha") to withdraw funds from my account for the initial and/or monthly renewal premiums and understand that the amounts may differ. Premium shortages may result from a variety of causes, including underwriting adjustments. I authorize my financial institution to pay from my account to Mutual of Omaha any preauthorized bank account withdrawals. I agree that my financial institution shall be fully protected in honoring any such payment and that its rights and responsibilities regarding the payment shall be the same as if the payment were signed personally by me. I agree to notify the business in writing of any changes in my account information. This authorization will be effective until I give you at least three business days' notice to cancel. If notice is given verbally, Mutual of Omaha may require written confirmation from me within 14 days after my verbal notice.
Date _____________________________ X __________________________________________ Mo./Day/Yr. Authorized Signature as Shown on Account
Authorization
1. Account Type (check one): Checking Savings 2. Name of Financial Institution: _________________________________________________________________________
3. Complete information below or attach a voided check here. Bank Routing Number: ___________________________ Bank Account Number: ____________________________ (Do not use Debit/Credit Card numbers)
Account Information
Memo __________________ Signed By: ______________________________________
Bank Routing Number
Bank Account Number
{{
Check Number (if shown at bottom, may be shown before or after the account #)
|:123456789:| 12345678 || 1234 || {
Payment Information
1. Initial Premium Payment Automated Bank Account Withdrawal Check Amount Quoted $____________________ When choosing automatic bank account withdrawal, MONEY WILL BE WITHDRAWN FROM YOUR ACCOUNT AT POLICY ISSUE. The first withdrawal date may be different from the monthly date selected for ongoing premiums. Depending on the amount of time elapsed between the policy date and the date the policy is issued, the amount of the first ongoing withdrawal may exceed one modal premium and may occur on a date other than the policy date. The Proposed Insured/Insured will not receive premium billing notices while on this premium payment option. We CANNOT establish electronic payments from foreign banks. 2. Ongoing Premium Payments Automated Bank Account Withdrawal (Monthly)
Specify the date premiums will be withdrawn: 1st of the Month or 15th of the Month Ongoing premiums are due and will be automatically withdrawn from the account below on the date selected above. The policy date is determined at the time the policy is issued and can be found within the policy. Ongoing withdrawals will begin once the policy is issued.
Direct Bill (select one) Annual Semiannual Quarterly
Proposed Insured/Insured: ____________________________ Policy Number(s) if known: _____________________________
Mutual of Omaha Insurance CompanyMutual of Omaha Plaza, Omaha, NE 68175, 800-775-6000
AUTHORIZATION TO DISCLOSE PERSONAL INFORMATION
This authorization specifically includes the release and disclosure of my “Personal Information,” which includes my entire medical record and any other health information concerning me (excluding psychotherapy notes) and my insurance policies and claims, including, but not limited to those containing diagnoses, treatments, prescription drug information, alcohol or drug abuse treatment information or information regarding communicable or infectious conditions, such as Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS), other matters such as hazardous activities, character and general reputation, finances, occupation, information collected by a consumer reporting agency about my credit history, credit worthiness, credit standing and credit capacity, avocation(s), motor vehicle driving record(s), and personal traits.
I authorize all hospitals, medical facilities and clinics, physicians, dentists, other medical or dental practitioners, pharmacies, pharmacists, pharmacy benefit managers, insurance companies, third party administrators, health plans, health maintenance organizations, MIB Inc., state departments of motor vehicles, other entities possessing motor vehicle records and consumer reporting agencies that have records or knowledge of me and my children, if they are proposed insureds (My Children), to release Personal Information about me or My Children to Mutual of Omaha Insurance Company, its affiliated companies (Mutual) or its reinsurers.
The Personal Information will be used to determine my and My Children’s eligibility for insurance or to resolve or contest any issues of incomplete, incorrect or misrepresented information on this application that may arise during the processing of my application or in connection with a claim.
I also authorize Mutual, or its reinsurers, to disclose my and My Children’s personal Information to MIB, Inc. I understand that my and My Children’s Personal Information received by MIB, Inc. may be disclosed, upon request, to another member company with whom I apply for life or health insurance or to whom I may submit a claim for benefits.
I understand that if the person or entity to whom Personal information is disclosed is not a health care provider or health plan subject to federal privacy regulations, the Personal information may be redisclosed without the protection of the federal privacy regulations.
I understand that I may refuse to sign this authorization. I understand if I refuse to sign, the insurance for which I am applying will not be reinstated.
This authorization will expire 24 months after the date signed. I may revoke this authorization at any time by written notice to ATTN: Individual Underwriting, Mutual of Omaha Insurance Company, Mutual of Omaha Plaza, Omaha NE 68175. A revocation is limited to the extent that Mutual has taken action in reliance on the authorization or the law allows Mutual to contest the issuance of the policy or a claim under the policy.
I understand that I will receive a copy of this authorization and that a copy is as valid as the original.
Each Proposed Insured acknowledges and agrees that if there is more than one Proposed Insured on this application, all information provided may be reviewed or shared with the other Proposed Insured. A completed and signed application will become part of each insured’s policy.
Name(s) used for medical records (if different than the name) below: ______________________________________
_______________________________________________________________________________________________________
________________________________________________________________ Date: __________________________Signature of Proposed Insured Mo Day Yr
________________________________________________________________ Date: __________________________Signature of Spouse (if Proposed Insured) Mo Day Yr
________________________________________________________________ Date: __________________________Signature of Parent or Guardian (if Proposed Insured is a Minor) Mo Day Yr
________________________________________________________________ Date: __________________________Signature of Non-minor Child (if Proposed Insured is a Non-minor) Mo Day Yr
THIS AUTHORIZATION COMPLIES WITH HIPAA AND OTHER FEDERAL AND STATE LAWS
Mutual of Omaha Insurance CompanyUnited of Omaha Life Insurance Company
L8232_0913
Notice and Consent for Testing of Biological Specimens to Include HIV (Aids Virus) Testing
Mutual of Omaha Insurance CompanyUnited of Omaha Life Insurance Company
To determine your insurability, the Insurer named above (the Insurer) has requested that you provide a biological specimen for testing and analysis. All tests will be performed by a licensed laboratory.
Unless precluded by law, tests will be performed to determine the presence of HIV (the AIDS virus), its component parts, or its antibodies. These tests are extremely reliable. Other tests which may be performed include determinations of blood cholesterol and related lipids (fats), cotinine, cocaine, and screening for liver or kidney disorders, diabetes and immune disorders.
All test results will be treated confidentially. They will be reported by the laboratory to the Insurer. When necessary for business reasons in connection with insurance you have or have applied for with the Insurer, the Insurer may disclose test results to others such as its affiliates, reinsurers, employees or contractors. If a biological specimen other than blood is tested to determine the presence of HIV virus, its component parts, or its antibodies, the Insurer may at a later time request a specimen of your blood for further HIV testing. If you choose to decline that request, the results of all testing which has been performed will be provided to the physician which you have designated to receive such results. In addition, if the Insurer is a member of the Medical Information Bureau (MIB, Inc.) and you choose to decline the request that you submit a blood specimen for further HIV testing if the test results for HIV antibodies/antigens are other than normal, the Insurer will report to the MIB, Inc., a generic code which specifies only a non-specific blood test has been ordered and not received. Regardless of the number of tests requested, if the final HIV testing results (including the results of any confirmatory tests dictated by standard medical practice) are other than normal, the Insurer will report to the MIB, Inc., a generic code which signifies only a non-specific test abnormality. If your final HIV testing results are normal, no report will be made about it to the MIB, Inc. Other test results may be reported to the MIB, Inc., in a more specific manner. The organizations described in this paragraph may maintain the test results in a file or data bank. There will be no other disclosure of test results or even that the tests have been done, except as may be required or permitted by law or as authorized by you.
If your HIV test results are normal, no routine notification will be sent to you. If the HIV test results are other than normal, the Insurer will contact you. The Insurer may also contact you if there are other abnormal test results which, in the Insurer’s opinion, are significant. The Insurer may ask you for the name of a physician to whom you authorize disclosure and with whom you may wish to discuss the results. If you are a resident of Missouri and your HIV test(s) indicates confirmed infection with HIV, and you have not provided the Insurer with the name of a physician to whom you authorize disclosure of test results, the Insurer will disclose test results to the Missouri Department of Health as required by law.
Positive HIV antibody or other significant abnormalities detected by additional tests of biological specimens will adversely affect your application for insurance. This means that your application may be declined, that an increased premium may be charged or that other policy changes may be necessary.
Physician ________________________________________ Address ______________________________________________ ________________________________________ _____________________________________________ ________________________________________ _____________________________________________ ________________________________________ _____________________________________________
I have read and I understand this Notice of Consent for Test of biological specimens which includes HIV testing. I voluntarily consent to provide biological specimen(s) for testing, to the testing of such specimen(s) and the disclosure of the test results as described above. I understand that I have the right to request and receive a copy of this information. A photocopy of this form will be as valid as the original.
____________________________________ ____________________________________ Proposed Insured Date of Birth
____________________________________ ________________________ ____________________________________ Signature of Proposed Date State of Residence Insured or Parent/Guardian
PLEASE SUBMIT MLU17135_1002
Conditional ReceiptMutual of Omaha Insurance CompanyMutual of Omaha PlazaOmaha, Nebraska 68175
■ Initial Premium paid by check Money was collected - Received $____________________ from ______________________ paid with an insurance
application on ______________________________________________________________, dated ____________________ (person(s) proposed for insurance)
(ALL CHECKS FOR PREMIUMS MUST BE MADE PAYABLE TO MUTUAL OF OMAHA INSURANCE COMPANY. DO NOT MAKE CHECKS PAYABLE TO THE PRODUCER OR LEAVE THE PAYEE BLANK.)
This Conditional Receipt will provide limited insurance coverage for each person proposed for insurance, subject to all of the provisions of the policy(ies) applied for, as of the application date, but only if all of the following conditions have been completely met:
1. Written application.2. Payment of the full initial premium.3. Completion by each Proposed Insured of all examinations and tests (medical, paramedical, laboratory) required by
Mutual of Omaha Insurance Company.4. Receipt by Mutual of Omaha Insurance Company of any additional information (such as an Attending Physician’s
Statement) requested for underwriting.5. Satisfying Mutual of Omaha Insurance Company underwriting standards.
If (a) any of the above conditions are not exactly met, or (b) the above conditions are exactly met but the person proposed for insurance dies by suicide, whether sane or insane (except in Colorado and Missouri), or (c) the application is not accepted by Mutual of Omaha, no insurance coverage will be provided under this Conditional Receipt, and Mutual of Omaha’s only liability will be to notify the applicant in writing and return the premium paid.
For each person proposed for insurance, the maximum benefit payable under this Conditional Receipt will be the lesser of: (a) the total benefit payable under all pending applications with Mutual of Omaha relating to the person proposed for insurance, or (b) $50,000. This Receipt provides no coverage for policy Riders.
Regardless of any other provision of this Conditional Receipt, any coverage that becomes effective under this Conditional Receipt will terminate on the earliest of the following: (a) the effective date of a policy issued as a result of this application; (b) the date Mutual of Omaha mails notice that the coverage applied for will not be issued and refunds any premium paid; or (c) 60 days following the date of the application. Either Mutual of Omaha or the person(s) proposed for insurance may terminate this Conditional Receipt as to such person(s) by providing written notice to the other party(ies).
If a Proposed Insured is eligible, the effective date of the insurance for that Proposed Insured will be the date of the application, or the date the number of applications received from members of your group meets the minimum participation requirements, whichever date is later. If a Proposed Insured is not eligible, no insurance or temporary or interim insurance of any kind will be in effect for that Proposed Insured.
In no event will benefits be paid for the same loss under both this Conditional Receipt and any insurance policy issued from the application.
No producer is authorized to alter the terms of this Receipt, waive any representations, or pass on insurability.
I understand and agree to the terms, conditions and limitations of this Conditional Receipt and the Agreement section of the application. These have been fully explained to me by the Producer.
Date: _________________________________________ Signed at: __________________________________________________ City State
______________________________________ _________________________________________Signature of Proposed Insured Signature of Spouse (If a Proposed Insured)
______________________________________ _________________________________________Signature of Producer Signature of Producer
Company’s Copy

IMPORTANT DOCUMENTS
LEAVE THE FOLLOWING REMAINING PAGES WITH CLIENT(S)
As part of the application process, the applicant has signed multiple forms. Applicant copies of these forms and notifications on the following pages are to be left with applicant(s).
CLIE
NT
FOR
MS
Conditional ReceiptMutual of Omaha Insurance CompanyMutual of Omaha PlazaOmaha, Nebraska 68175
■ Initial Premium paid by check Money was collected - Received $____________________ from ______________________ paid with an insurance
application on ______________________________________________________________, dated ____________________ (person(s) proposed for insurance)
(ALL CHECKS FOR PREMIUMS MUST BE MADE PAYABLE TO MUTUAL OF OMAHA INSURANCE COMPANY. DO NOT MAKE CHECKS PAYABLE TO THE PRODUCER OR LEAVE THE PAYEE BLANK.)
This Conditional Receipt will provide limited insurance coverage for each person proposed for insurance, subject to all of the provisions of the policy(ies) applied for, as of the application date, but only if all of the following conditions have been completely met:
1. Written application.2. Payment of the full initial premium.3. Completion by each Proposed Insured of all examinations and tests (medical, paramedical, laboratory) required by
Mutual of Omaha Insurance Company.4. Receipt by Mutual of Omaha Insurance Company of any additional information (such as an Attending Physician’s
Statement) requested for underwriting.5. Satisfying Mutual of Omaha Insurance Company underwriting standards.
If (a) any of the above conditions are not exactly met, or (b) the above conditions are exactly met but the person proposed for insurance dies by suicide, whether sane or insane (except in Colorado and Missouri), or (c) the application is not accepted by Mutual of Omaha, no insurance coverage will be provided under this Conditional Receipt, and Mutual of Omaha’s only liability will be to notify the applicant in writing and return the premium paid.
For each person proposed for insurance, the maximum benefit payable under this Conditional Receipt will be the lesser of: (a) the total benefit payable under all pending applications with Mutual of Omaha relating to the person proposed for insurance, or (b) $50,000. This Receipt provides no coverage for policy Riders.
Regardless of any other provision of this Conditional Receipt, any coverage that becomes effective under this Conditional Receipt will terminate on the earliest of the following: (a) the effective date of a policy issued as a result of this application; (b) the date Mutual of Omaha mails notice that the coverage applied for will not be issued and refunds any premium paid; or (c) 60 days following the date of the application. Either Mutual of Omaha or the person(s) proposed for insurance may terminate this Conditional Receipt as to such person(s) by providing written notice to the other party(ies).
If a Proposed Insured is eligible, the effective date of the insurance for that Proposed Insured will be the date of the application, or the date the number of applications received from members of your group meets the minimum participation requirements, whichever date is later. If a Proposed Insured is not eligible, no insurance or temporary or interim insurance of any kind will be in effect for that Proposed Insured.
In no event will benefits be paid for the same loss under both this Conditional Receipt and any insurance policy issued from the application.
No producer is authorized to alter the terms of this Receipt, waive any representations, or pass on insurability.
I understand and agree to the terms, conditions and limitations of this Conditional Receipt and the Agreement section of the application. These have been fully explained to me by the Producer.
Date: _________________________________________ Signed at: __________________________________________________ City State
______________________________________ _________________________________________Signature of Proposed Insured Signature of Spouse (If a Proposed Insured)
______________________________________ _________________________________________Signature of Producer Signature of Producer
Applicant’s Copy
MIB, Inc. Pre-NoticeInformation regarding your insurability will be treated as confidential. Mutual of Omaha Insurance Company or its reinsurers may make a brief report to MIB, Inc., a nonprofit membership organization of insurance companies which operates an information exchange for its members. If you apply to another MIB, Inc. member company for life or health insurance coverage, or a claim for benefits is submitted to such a company, MIB, Inc. upon request, will supply the information in its file to that company.
Upon receipt of a request from you, MIB, Inc. will arrange disclosure of any information it may have in your file. Please contact MIB, Inc. at 866-692-6901. If you question the accuracy of the information in MIB, Inc.’s file, you may contact MIB, Inc. and seek a correction in accordance with the procedures set forth in the federal Fair Credit Reporting Act. The address of MIB, Inc.’s information office is: 50 Braintree Hill Park, Suite 400, Braintree, MA 02184-8734.
In compliance with applicable law, Mutual of Omaha Insurance Company, or its reinsurers, may also release information in its file, including information given in your application, to other insurance companies to which you apply for life or health insurance or to which a claim is submitted. Information for consumers about MIB, Inc. may be obtained on its website at www.mib.com.
GIVE THIS NOTICE TO THE APPLICANT
M26978_0809
This is a Brief Description of some of the features and benefits of your coverage. It is not a contract for insurance and only the actual policy provisions will control. However, the policy itself sets forth in detail the rights and obligations of both you and Mutual of Omaha Insurance Company. PLEASE READ YOUR POLICY CAREFULLY.
This is a LIMITED BENEFIT HEALTH COVERAGE policy. Policies of this category are designed to provide to persons insured, limited or supplemental coverage.
Critical Illness BenefitsThis policy will pay all or a portion of the Maximum Benefit Amount, as designated below, for a covered Critical Illness of the Insured, provided that the first Diagnosis of the covered Critical Illness is made while this policy is in force. The amount payable is as follows:
100% of the Maximum Benefit Amount is payable for:
(a) Alzheimer’s Disease;
(b) Blindness;
(c) Life Threatening Cancer;
(d) Deafness;
(e) Heart Attack (Myocardial Infarction);
(f) Major Organ Transplant;
(g) Paralysis;
(h) Renal Failure; or
(i) Stroke.
25% of the Maximum Benefit Amount is payable only once for each of the following:
(a) the First Ever Coronary Angioplasty (surgical treatment);
(b) the First Ever Coronary Artery Bypass (surgical treatment); and
(c) the first Diagnosis of First Carcinoma in Situ as required by this policy.
In the case of a First Coronary Angioplasty or First Coronary Bypass Surgery, this first Diagnosis includes the performance of the surgical treatment as required under this policy. In the case of a Major Organ Transplant, this first Diagnosis includes verification that the Insured has been registered by the United Network of Organ Sharing (UNOS).
If a portion of the Maximum Benefit Amount is paid under this policy or certain attached riders (if applicable), the Maximum Benefit Amount will be reduced by the amount paid, and the premium will be adjusted accordingly. The Owner will be notified of the new Maximum Benefit Amount and new premium. In no event will the payment(s) for any Critical Illness Insured Condition(s) exceed the Maximum Benefit Amount then in force.
Receipt of Critical Illness Benefits may affect eligibility for Medicaid or other government benefits and entitlements.
“Maximum Benefit Amount” means the maximum amount that will be payable under this policy. This amount is payable only upon the first Diagnosis of, or required surgical treatment for, a Critical Illness Insured Condition. The initial Maximum Benefit Amount is shown on the Policy Schedule. A portion of the Maximum Benefit Amount is payable for some of the Critical Illness Insured Conditions defined in this policy. The Maximum Benefit Amount will be reduced by any portion of the Maximum Benefit Amount required to be paid under this policy. The Maximum Benefit Amount may also be reduced by any benefits paid under certain attached riders, if applicable.
Hospital Confinement Benefit in IAWhen the Insured is confined as an inpatient in a hospital as a result of a covered Critical Illness condition, We will pay $50 for each day of inpatient confinement, up to a maximum of 500 days during your lifetime.
A “Hospital” does not include a hospital or institution or a part of a hospital or institution which is licensed or used principally as a clinic, continued care or extended care facility, skilled nursing facility, or convalescent home, rest home, nursing home or home for the aged.
Definitions“Critical Illness Insured Condition” means one of the medical conditions or surgical treatments (First Coronary Angioplasty or First Coronary Artery Bypass Surgery) defined below. The
Coverage Underwritten by: Mutual of Omaha Insurance Company, Mutual of Omaha Plaza, Omaha, Nebraska 68175, 402 342 7600
MC31982_0311
Critical Illnesssummary of coverage
Mutual of Omaha Insurance Company
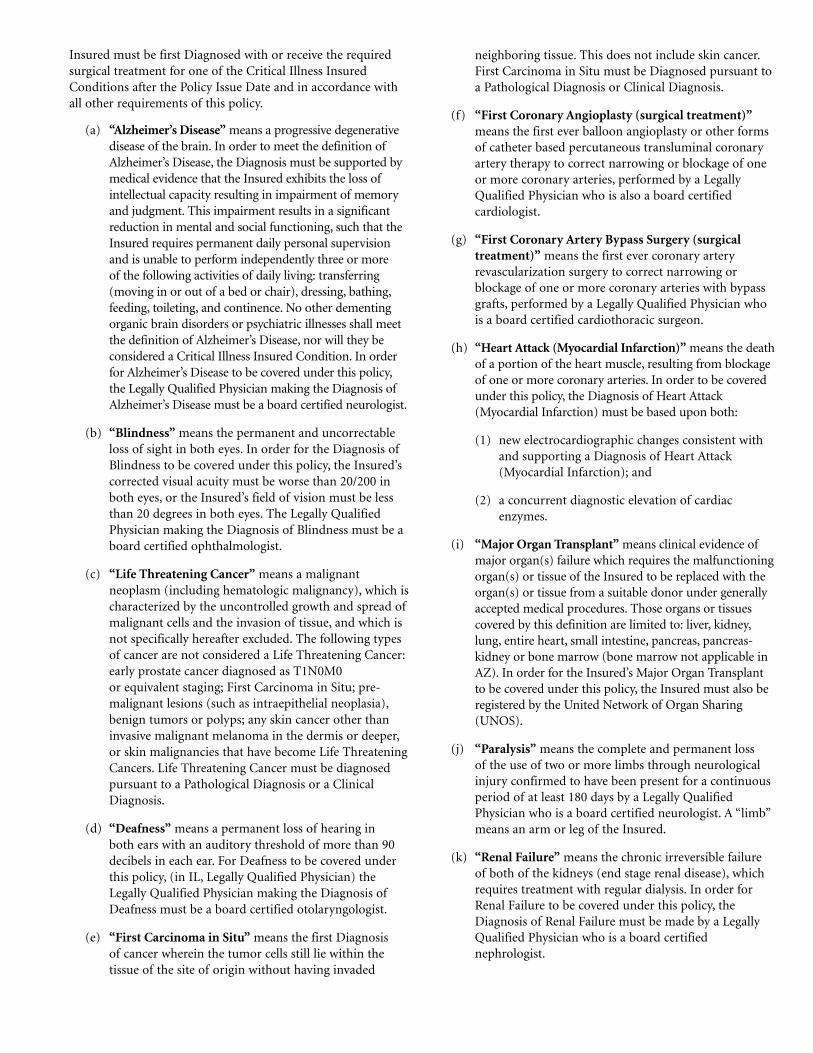
Insured must be first Diagnosed with or receive the required surgical treatment for one of the Critical Illness Insured Conditions after the Policy Issue Date and in accordance with all other requirements of this policy.
(a) “Alzheimer’s Disease” means a progressive degenerative disease of the brain. In order to meet the definition of Alzheimer’s Disease, the Diagnosis must be supported by medical evidence that the Insured exhibits the loss of intellectual capacity resulting in impairment of memory and judgment. This impairment results in a significant reduction in mental and social functioning, such that the Insured requires permanent daily personal supervision and is unable to perform independently three or more of the following activities of daily living: transferring (moving in or out of a bed or chair), dressing, bathing, feeding, toileting, and continence. No other dementing organic brain disorders or psychiatric illnesses shall meet the definition of Alzheimer’s Disease, nor will they be considered a Critical Illness Insured Condition. In order for Alzheimer’s Disease to be covered under this policy, the Legally Qualified Physician making the Diagnosis of Alzheimer’s Disease must be a board certified neurologist.
(b) “Blindness” means the permanent and uncorrectable loss of sight in both eyes. In order for the Diagnosis of Blindness to be covered under this policy, the Insured’s corrected visual acuity must be worse than 20/200 in both eyes, or the Insured’s field of vision must be less than 20 degrees in both eyes. The Legally Qualified Physician making the Diagnosis of Blindness must be a board certified ophthalmologist.
(c) “Life Threatening Cancer” means a malignant neoplasm (including hematologic malignancy), which is characterized by the uncontrolled growth and spread of malignant cells and the invasion of tissue, and which is not specifically hereafter excluded. The following types of cancer are not considered a Life Threatening Cancer: early prostate cancer diagnosed as T1N0M0 or equivalent staging; First Carcinoma in Situ; pre-malignant lesions (such as intraepithelial neoplasia), benign tumors or polyps; any skin cancer other than invasive malignant melanoma in the dermis or deeper, or skin malignancies that have become Life Threatening Cancers. Life Threatening Cancer must be diagnosed pursuant to a Pathological Diagnosis or a Clinical Diagnosis.
(d) “Deafness” means a permanent loss of hearing in both ears with an auditory threshold of more than 90 decibels in each ear. For Deafness to be covered under this policy, (in IL, Legally Qualified Physician) the Legally Qualified Physician making the Diagnosis of Deafness must be a board certified otolaryngologist.
(e) “First Carcinoma in Situ” means the first Diagnosis of cancer wherein the tumor cells still lie within the tissue of the site of origin without having invaded
neighboring tissue. This does not include skin cancer. First Carcinoma in Situ must be Diagnosed pursuant to a Pathological Diagnosis or Clinical Diagnosis.
(f) “First Coronary Angioplasty (surgical treatment)” means the first ever balloon angioplasty or other forms of catheter based percutaneous transluminal coronary artery therapy to correct narrowing or blockage of one or more coronary arteries, performed by a Legally Qualified Physician who is also a board certified cardiologist.
(g) “First Coronary Artery Bypass Surgery (surgical treatment)” means the first ever coronary artery revascularization surgery to correct narrowing or blockage of one or more coronary arteries with bypass grafts, performed by a Legally Qualified Physician who is a board certified cardiothoracic surgeon.
(h) “Heart Attack (Myocardial Infarction)” means the death of a portion of the heart muscle, resulting from blockage of one or more coronary arteries. In order to be covered under this policy, the Diagnosis of Heart Attack (Myocardial Infarction) must be based upon both:
(1) new electrocardiographic changes consistent with and supporting a Diagnosis of Heart Attack (Myocardial Infarction); and
(2) a concurrent diagnostic elevation of cardiac enzymes.
(i) “Major Organ Transplant” means clinical evidence of major organ(s) failure which requires the malfunctioning organ(s) or tissue of the Insured to be replaced with the organ(s) or tissue from a suitable donor under generally accepted medical procedures. Those organs or tissues covered by this definition are limited to: liver, kidney, lung, entire heart, small intestine, pancreas, pancreas-kidney or bone marrow (bone marrow not applicable in AZ). In order for the Insured’s Major Organ Transplant to be covered under this policy, the Insured must also be registered by the United Network of Organ Sharing (UNOS).
(j) “Paralysis” means the complete and permanent loss of the use of two or more limbs through neurological injury confirmed to have been present for a continuous period of at least 180 days by a Legally Qualified Physician who is a board certified neurologist. A “limb” means an arm or leg of the Insured.
(k) “Renal Failure” means the chronic irreversible failure of both of the kidneys (end stage renal disease), which requires treatment with regular dialysis. In order for Renal Failure to be covered under this policy, the Diagnosis of Renal Failure must be made by a Legally Qualified Physician who is a board certified nephrologist.
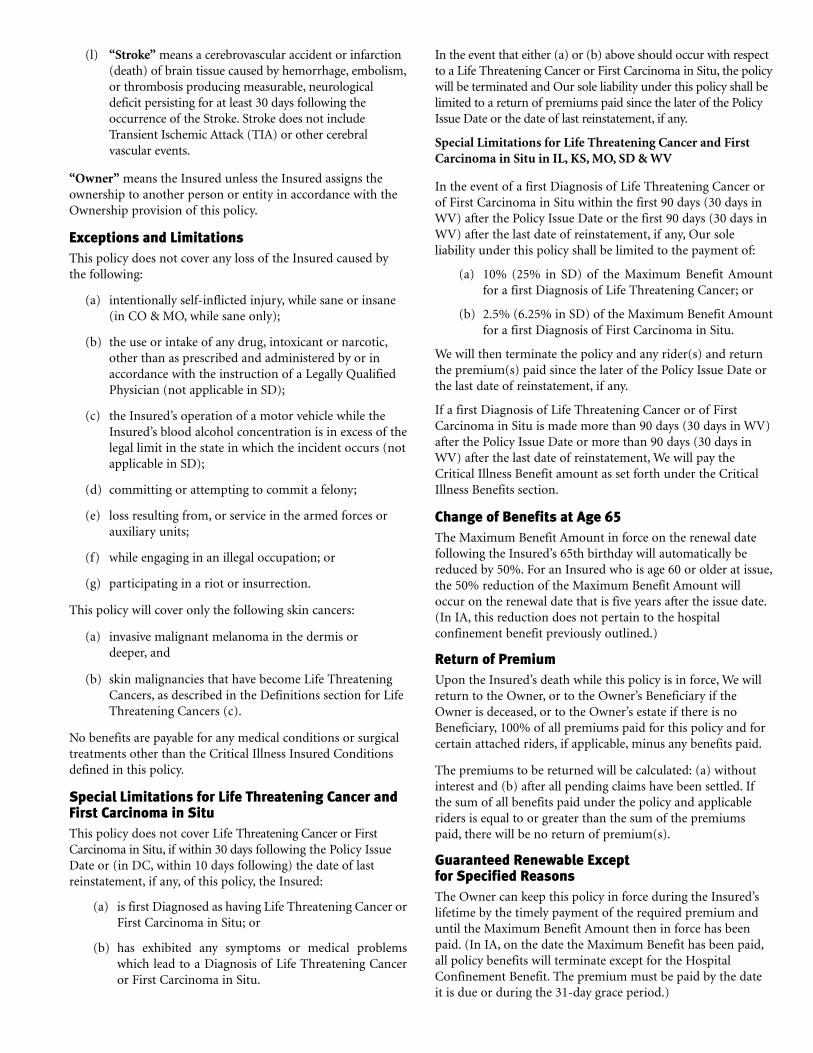
(l) “Stroke” means a cerebrovascular accident or infarction (death) of brain tissue caused by hemorrhage, embolism, or thrombosis producing measurable, neurological deficit persisting for at least 30 days following the occurrence of the Stroke. Stroke does not include Transient Ischemic Attack (TIA) or other cerebral vascular events.
“Owner” means the Insured unless the Insured assigns the ownership to another person or entity in accordance with the Ownership provision of this policy.
Exceptions and LimitationsThis policy does not cover any loss of the Insured caused by the following:
(a) intentionally self-inflicted injury, while sane or insane (in CO & MO, while sane only);
(b) the use or intake of any drug, intoxicant or narcotic, other than as prescribed and administered by or in accordance with the instruction of a Legally Qualified Physician (not applicable in SD);
(c) the Insured’s operation of a motor vehicle while the Insured’s blood alcohol concentration is in excess of the legal limit in the state in which the incident occurs (not applicable in SD);
(d) committing or attempting to commit a felony;
(e) loss resulting from, or service in the armed forces or auxiliary units;
(f) while engaging in an illegal occupation; or
(g) participating in a riot or insurrection.
This policy will cover only the following skin cancers:
(a) invasive malignant melanoma in the dermis or deeper, and
(b) skin malignancies that have become Life Threatening Cancers, as described in the Definitions section for Life Threatening Cancers (c).
No benefits are payable for any medical conditions or surgical treatments other than the Critical Illness Insured Conditions defined in this policy.
Special Limitations for Life Threatening Cancer and First Carcinoma in Situ This policy does not cover Life Threatening Cancer or First Carcinoma in Situ, if within 30 days following the Policy Issue Date or (in DC, within 10 days following) the date of last reinstatement, if any, of this policy, the Insured:
(a) is first Diagnosed as having Life Threatening Cancer or First Carcinoma in Situ; or
(b) has exhibited any symptoms or medical problems which lead to a Diagnosis of Life Threatening Cancer or First Carcinoma in Situ.
In the event that either (a) or (b) above should occur with respect to a Life Threatening Cancer or First Carcinoma in Situ, the policy will be terminated and Our sole liability under this policy shall be limited to a return of premiums paid since the later of the Policy Issue Date or the date of last reinstatement, if any.
Special Limitations for Life Threatening Cancer and First Carcinoma in Situ in IL, KS, MO, SD & WV
In the event of a first Diagnosis of Life Threatening Cancer or of First Carcinoma in Situ within the first 90 days (30 days in WV) after the Policy Issue Date or the first 90 days (30 days in WV) after the last date of reinstatement, if any, Our sole liability under this policy shall be limited to the payment of:
(a) 10% (25% in SD) of the Maximum Benefit Amount for a first Diagnosis of Life Threatening Cancer; or
(b) 2.5% (6.25% in SD) of the Maximum Benefit Amount for a first Diagnosis of First Carcinoma in Situ.
We will then terminate the policy and any rider(s) and return the premium(s) paid since the later of the Policy Issue Date or the last date of reinstatement, if any.
If a first Diagnosis of Life Threatening Cancer or of First Carcinoma in Situ is made more than 90 days (30 days in WV) after the Policy Issue Date or more than 90 days (30 days in WV) after the last date of reinstatement, We will pay the Critical Illness Benefit amount as set forth under the Critical Illness Benefits section.
Change of Benefits at Age 65The Maximum Benefit Amount in force on the renewal date following the Insured’s 65th birthday will automatically be reduced by 50%. For an Insured who is age 60 or older at issue, the 50% reduction of the Maximum Benefit Amount will occur on the renewal date that is five years after the issue date. (In IA, this reduction does not pertain to the hospital confinement benefit previously outlined.)
Return of PremiumUpon the Insured’s death while this policy is in force, We will return to the Owner, or to the Owner’s Beneficiary if the Owner is deceased, or to the Owner’s estate if there is no Beneficiary, 100% of all premiums paid for this policy and for certain attached riders, if applicable, minus any benefits paid.
The premiums to be returned will be calculated: (a) without interest and (b) after all pending claims have been settled. If the sum of all benefits paid under the policy and applicable riders is equal to or greater than the sum of the premiums paid, there will be no return of premium(s).
Guaranteed Renewable Except for Specified ReasonsThe Owner can keep this policy in force during the Insured’s lifetime by the timely payment of the required premium and until the Maximum Benefit Amount then in force has been paid. (In IA, on the date the Maximum Benefit has been paid, all policy benefits will terminate except for the Hospital Confinement Benefit. The premium must be paid by the date it is due or during the 31-day grace period.)

Premium ChangesYour premium will not be changed during the first policy year except as allowed in the Benefits section of this policy. On or after the first policy anniversary, the premium payable may change for this policy. Such changes to premium will be applied only when the same change is made on all policies of this Form, issued to persons of the same rate classification, in the Insured’s state. (In MT, the change will not be made more frequently than once a year.) We will send the Owner written notice, at the Owner’s last known address, at least 30 days (45 days in NC) prior to the date of any change in premium. (In NC, revised rates are guaranteed for 12 months.)
TerminationThis policy will end on the earliest of the following:
(a) the date that We receive the Owner’s (or Insured’s in KS) written request to end this policy;
(b) the date of the Insured’s death;
(c) the premium due date, if sufficient premium has not been paid before the end of the grace period;
(d) the date the Maximum Benefit Amount is paid (not applicable in IA); or
(e) the date the policy terminates as set forth in the Special Limitations for Life Threatening Cancer section.
In IA, on the date Maximum Benefit has been paid, all policy benefits will terminate except the hospital confinement benefits as outlined previously.
Grace PeriodThe premium must be paid on or before the date it is due or during the 31-day grace period that follows. This policy remains in force during the grace period. There is a grace period unless We write and tell the Owner it does not apply.
ReinstatementIf the premium due is not paid before the end of the grace period, this policy will end as of the premium due date. If We later accept the premium and do not require an application for reinstatement, that payment will put this policy back in force. If We require an application for reinstatement, this policy will be placed in force once the application is approved. Unless We have previously sent the Owner written notice of disapproval, the policy will be reinstated on the 45th (30th day in NM) day after the date of application.
A reinstated policy will cover only loss from a Critical Illness Insured Condition that results from a first Diagnosis after the date of reinstatement. In all other respects, the Insured, the Owner (if other than the Insured) and We have the same rights under this policy as were in effect before the lapse. After the policy has been reinstated, the time period in the Time Limit On Certain Defenses provision will be measured from the date of reinstatement as to the statements contained in the application for reinstatement, except for fraudulent
misstatements. A new 30-day (10-day in DC; 90-days in IL, KS, MO and SD) waiting period after the reinstatement date will apply for Life Threatening Cancer and First Carcinoma in Situ.
Waiting Period in KSIf this policy is in addition to or a replacement for an existing specified disease policy, you will be given credit for any waiting period you have completed under the previous specified disease policies.
Reinstatement if Suffering from Organic Brain Disease in MEWithin 90 days from the date Your policy lapsed, You or any person authorized to act on your behalf or any dependent of Yours may request reinstatement of this policy on the basis that You suffered from Organic Brain Disease on such date.
We may ask You to submit evidence, at Your expense, that You suffered from Organic Brain Disease on the date the policy lapsed. If the evidence proves, to Our satisfaction, that You suffered from Organic Brain Disease on such date, the policy will be reinstated without any evidence of insurability. The reinstated policy will cover loss as if there were no gaps in coverage.
Premiums shall be paid from the date of policy lapse at the rate which would have been in effect had the policy remained in force. Premiums must be paid within 15 calendar days following Our request.
If Your request for reinstatement is denied, We will send notice of denial to You and the person making the request, if different. The notification will advise You that You can request a hearing to appeal the denial with the Superintendent of Insurance within 30 calendar days from the date You received such notice.
“Organic Brain Disease” means a mental or nervous disorder with a demonstrable organic origin causing significant cognitive impairment, including but not limited to Pick’s Disease, Parkinson’s Disease, Huntington’s Chorea, Alzheimer’s Disease and related dementias.
Optional Benefits (Not Available In All States)
Disability Rider — Optional Rider — 0HA5M, or state equivalentIf Injuries or Sickness result in the Insured’s Total Disability, and the Insured is approved by the Social Security Administration to receive Social Security Disability Benefits, We will pay the Owner the following payments under this rider:
■ 5% of the Disability Benefit Amount will be paid every 6 months for the first 5 years of the Insured’s Total Disability. The first 6-month period will be calculated from the effective date that Social Security Disability Benefits are payable.
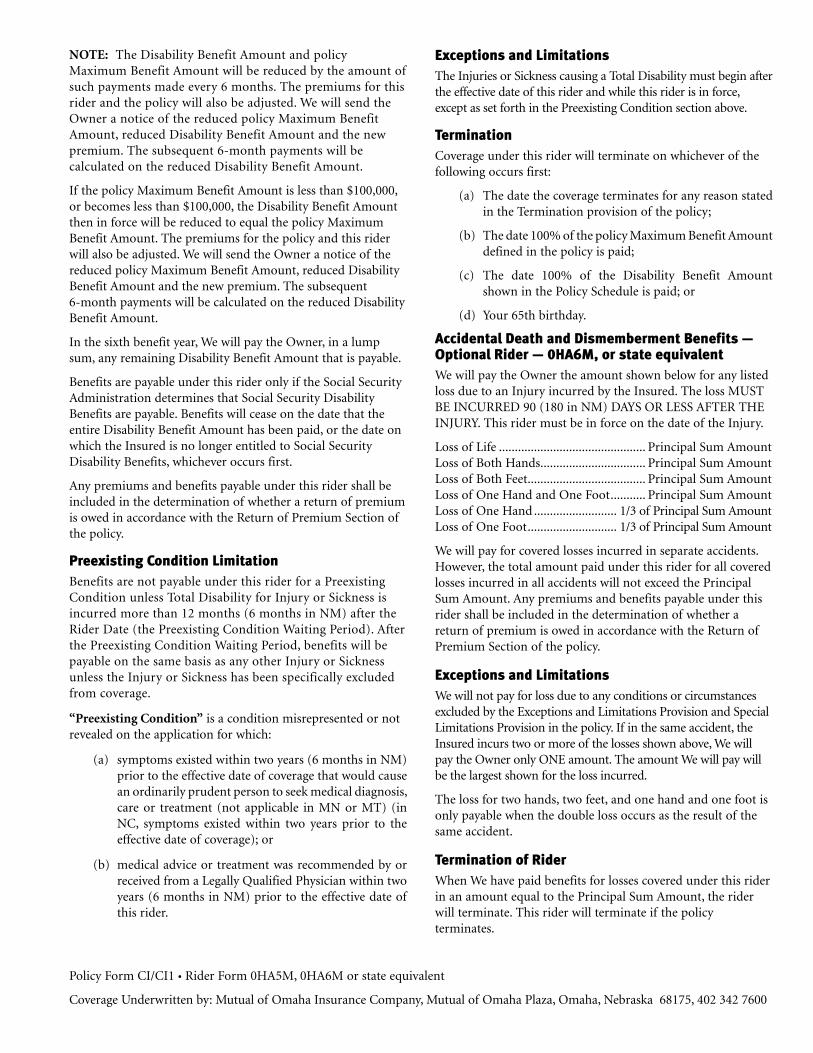
NOTE: The Disability Benefit Amount and policy Maximum Benefit Amount will be reduced by the amount of such payments made every 6 months. The premiums for this rider and the policy will also be adjusted. We will send the Owner a notice of the reduced policy Maximum Benefit Amount, reduced Disability Benefit Amount and the new premium. The subsequent 6-month payments will be calculated on the reduced Disability Benefit Amount.
If the policy Maximum Benefit Amount is less than $100,000, or becomes less than $100,000, the Disability Benefit Amount then in force will be reduced to equal the policy Maximum Benefit Amount. The premiums for the policy and this rider will also be adjusted. We will send the Owner a notice of the reduced policy Maximum Benefit Amount, reduced Disability Benefit Amount and the new premium. The subsequent 6-month payments will be calculated on the reduced Disability Benefit Amount.
In the sixth benefit year, We will pay the Owner, in a lump sum, any remaining Disability Benefit Amount that is payable.
Benefits are payable under this rider only if the Social Security Administration determines that Social Security Disability Benefits are payable. Benefits will cease on the date that the entire Disability Benefit Amount has been paid, or the date on which the Insured is no longer entitled to Social Security Disability Benefits, whichever occurs first.
Any premiums and benefits payable under this rider shall be included in the determination of whether a return of premium is owed in accordance with the Return of Premium Section of the policy.
Preexisting Condition LimitationBenefits are not payable under this rider for a Preexisting Condition unless Total Disability for Injury or Sickness is incurred more than 12 months (6 months in NM) after the Rider Date (the Preexisting Condition Waiting Period). After the Preexisting Condition Waiting Period, benefits will be payable on the same basis as any other Injury or Sickness unless the Injury or Sickness has been specifically excluded from coverage.
“Preexisting Condition” is a condition misrepresented or not revealed on the application for which:
(a) symptoms existed within two years (6 months in NM) prior to the effective date of coverage that would cause an ordinarily prudent person to seek medical diagnosis, care or treatment (not applicable in MN or MT) (in NC, symptoms existed within two years prior to the effective date of coverage); or
(b) medical advice or treatment was recommended by or received from a Legally Qualified Physician within two years (6 months in NM) prior to the effective date of this rider.
Exceptions and LimitationsThe Injuries or Sickness causing a Total Disability must begin after the effective date of this rider and while this rider is in force, except as set forth in the Preexisting Condition section above.
TerminationCoverage under this rider will terminate on whichever of the following occurs first:
(a) The date the coverage terminates for any reason stated in the Termination provision of the policy;
(b) The date 100% of the policy Maximum Benefit Amount defined in the policy is paid;
(c) The date 100% of the Disability Benefit Amount shown in the Policy Schedule is paid; or
(d) Your 65th birthday.
Accidental Death and Dismemberment Benefits — Optional Rider — 0HA6M, or state equivalentWe will pay the Owner the amount shown below for any listed loss due to an Injury incurred by the Insured. The loss MUST BE INCURRED 90 (180 in NM) DAYS OR LESS AFTER THE INJURY. This rider must be in force on the date of the Injury.
Loss of Life .............................................. Principal Sum AmountLoss of Both Hands ................................. Principal Sum AmountLoss of Both Feet ..................................... Principal Sum AmountLoss of One Hand and One Foot ........... Principal Sum AmountLoss of One Hand .......................... 1/3 of Principal Sum AmountLoss of One Foot ............................ 1/3 of Principal Sum Amount
We will pay for covered losses incurred in separate accidents. However, the total amount paid under this rider for all covered losses incurred in all accidents will not exceed the Principal Sum Amount. Any premiums and benefits payable under this rider shall be included in the determination of whether a return of premium is owed in accordance with the Return of Premium Section of the policy.
Exceptions and LimitationsWe will not pay for loss due to any conditions or circumstances excluded by the Exceptions and Limitations Provision and Special Limitations Provision in the policy. If in the same accident, the Insured incurs two or more of the losses shown above, We will pay the Owner only ONE amount. The amount We will pay will be the largest shown for the loss incurred.
The loss for two hands, two feet, and one hand and one foot is only payable when the double loss occurs as the result of the same accident.
Termination of RiderWhen We have paid benefits for losses covered under this rider in an amount equal to the Principal Sum Amount, the rider will terminate. This rider will terminate if the policy terminates.
Policy Form CI/CI1 • Rider Form 0HA5M, 0HA6M or state equivalent
Coverage Underwritten by: Mutual of Omaha Insurance Company, Mutual of Omaha Plaza, Omaha, Nebraska 68175, 402 342 7600




![Mutual of Omaha Insurance Company United of Omaha Life Insurance Company Transferring the Family [Business] [Presenter Name] Insurance products and services.](https://static.fdocuments.us/doc/165x107/5697bf851a28abf838c87860/mutual-of-omaha-insurance-company-united-of-omaha-life-insurance-company-transferring.jpg)













