Musculoskeletal Examination - download.e-bookshelf.de · musculoskeletal system. This understanding...
30
Musculoskeletal Examination 3rd Edition Jeffrey M. Gross, MD Clinical Associate Professor of Rehabilitation Medicine New York University School of Medicine Medical Director Union Square Rehabilitation and Sports Medicine New York, New York Joseph Fetto, MD Associate Professor of Orthopedic Surgery New York University School of Medicine Associate Professor and Consultant Manhattan V.A. Medical Center New York, New York Elaine Rosen, PT, DHSc, OCS Associate Professor of Physical Therapy Hunter College City University of New York Partner Queens Physical Therapy Associates Forest Hills, New York A John Wiley & Sons, Ltd., Publication
Transcript of Musculoskeletal Examination - download.e-bookshelf.de · musculoskeletal system. This understanding...

BLBK145-Gross February 13, 2009 21:2
MusculoskeletalExamination3rd Edition
Jeffrey M. Gross, MDClinical Associate Professor of Rehabilitation MedicineNew York University School of MedicineMedical DirectorUnion Square Rehabilitation and Sports MedicineNew York, New York
Joseph Fetto, MDAssociate Professor of Orthopedic SurgeryNew York University School of MedicineAssociate Professor and ConsultantManhattan V.A. Medical CenterNew York, New York
Elaine Rosen, PT, DHSc, OCSAssociate Professor of Physical TherapyHunter CollegeCity University of New YorkPartnerQueens Physical Therapy AssociatesForest Hills, New York
A John Wiley & Sons, Ltd., Publication
i


BLBK145-Gross February 13, 2009 21:2
MusculoskeletalExamination3rd Edition
Jeffrey M. Gross, MDClinical Associate Professor of Rehabilitation MedicineNew York University School of MedicineMedical DirectorUnion Square Rehabilitation and Sports MedicineNew York, New York
Joseph Fetto, MDAssociate Professor of Orthopedic SurgeryNew York University School of MedicineAssociate Professor and ConsultantManhattan V.A. Medical CenterNew York, New York
Elaine Rosen, PT, DHSc, OCSAssociate Professor of Physical TherapyHunter CollegeCity University of New YorkPartnerQueens Physical Therapy AssociatesForest Hills, New York
A John Wiley & Sons, Ltd., Publication
i

BLBK145-Gross February 13, 2009 21:2
This edition first published 2009 C© 1996, 2002, 2009 by Jeffrey Gross, Joseph Fetto, Elaine Rosen
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishingprogram has been merged with Wiley’s global Scientific, Technical and Medical business to formWiley-Blackwell.
Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex,PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to applyfor permission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance withthe Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise,except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permissionof the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print maynot be available in electronic books.
Designations used by companies to distinguish their products are often claimed as trademarks. All brandnames and product names used in this book are trade names, service marks, trademarks or registeredtrademarks of their respective owners. The publisher is not associated with any product or vendormentioned in this book. This publication is designed to provide accurate and authoritative informationin regard to the subject matter covered. It is sold on the understanding that the publisher is not engagedin rendering professional services. If professional advice or other expert assistance is required, theservices of a competent professional should be sought.
Library of Congress Cataloging-in-Publication Data
Gross, Jeffrey M., 1957–Musculoskeletal examination / Jeffrey M. Gross, Joseph Fetto, Elaine Rosen.—3rd ed.
p. ; cm.Includes bibliographical references and index.ISBN 978-1-4051-8049-81. Musculoskeletal system—Examination. I. Fetto, Joseph. II. Rosen, Elaine. III. Title.[DNLM: 1. Musculoskeletal Diseases—diagnosis. 2. Musculoskeletal Physiology.
3. Musculoskeletal System—anatomy & histology. 4. Physical Examination—methods.WE 141 G878m 2009]
RC925.7.G76 2009616.70076–dc22
2008039510
ISBN: 978-1-4051-8049-8
A catalogue record for this book is available from the British Library.
Set in 10/12pt Sabon by Aptara R© Inc., New Delhi, IndiaPrinted & bound in Singapore
1 2009
Commissioning Editor: Ben TownsendDevelopment Editor: Laura MurphyProduction Editor: Cathryn GatesEditorial Assistant: Madeleine Hurd
ii

BLBK145-Gross February 13, 2009 21:2
Contents
How to Use This Book, iv
Acknowledgments, v
1 Introduction, 1
2 Basic Concepts of Physical Examination, 14
3 Overview of the Spine and Pelvis, 31
4 The Cervical Spine and Thoracic Spine, 34
5 The Temporomandibular Joint, 82
6 The Lumbosacral Spine, 95
7 Overview of the Upper Extremity, 139
8 The Shoulder, 141
9 The Elbow, 199
10 The Wrist and Hand, 235
11 The Hip, 293
12 The Knee, 335
13 The Ankle and Foot, 379
14 Gait, 432
Appendices, 445
Bibliography, 449
Index, 453
iii

BLBK145-Gross February 13, 2009 21:2
How to Use This Book
Musculoskeletal Examination is to be used as botha teaching text and a general reference on the tech-niques of physical examination. This volume rep-resents the joint authoring efforts of a physiatrist,an orthopedic surgeon, and a physical therapist andpresents the information in a clear and concise for-mat, free of any professional biases that reflect onespecialty’s preferences. The importance of this willbe seen as we take you through each anatomical re-gion and delineate the basic examination. Includedin each chapter are the abnormalities most frequentlyencountered noted while performing an examination.
The book is organized into regional anatomical sec-tions including the spine and pelvis, the upper extrem-ity, and the lower extremity. The book opens withtwo chapters that define the structures of the muscu-loskeletal system and discuss the basic concepts andparts of the musculoskeletal exam. A final chapterdescribes the examination of gait.
Each main chapter is organized in an identical man-ner:� overview of the anatomical region� observation of the patient� subjective examination� gentle palpation� trigger points (where applicable)� active movement testing� passive movement testing� physiological movements� mobility testing� resistive testing� neurological examination� referred pain patterns� special tests� radiological views
In Chapter 2, Basic Concepts of the Physical Ex-amination, we provide you with a framework for per-forming the examination, beginning with observationand ending with palpation. However, in each regionalanatomy chapter, palpation follows observation andsubjective examination and precedes all other sec-tions. This is deliberate. For reasons of length, wefelt it important to discuss each anatomical regionand its own special anatomical structures as soon aspossible in each chapter. This avoids repetition, givesyou the anatomy early in each chapter, and then al-lows you to visualize each structure as you read thesubsequent sections on testing. Hopefully, this willreinforce the anatomy and help you apply anatomyto function and function to the findings of yourexamination.
Each chapter includes a generous number of origi-nal line drawings, many of which are two color. Theseprovide clear snapshots of how to perform each exam-ination technique. Thirty-two x-rays and MRIs havebeen included to help you with radiological anatomy.Paradigms and tables provide additional informationthat will help you understand the how and why ofeach examination technique.
By using Musculoskeletal Examination as a guideand reference, the reader will be able to performthe complete basic examination and understand com-mon abnormalities and their pathological signifi-cance. We hope that our readers will gain an ap-preciation for the intimate relationship between thestructure and function of the components of themusculoskeletal system. This understanding shouldthen enable any reader to make a correct diag-nosis and a successful treatment plan for eachpatient.
iv

BLBK145-Gross February 13, 2009 21:2
Acknowledgments
The writing of Musculoskeletal Examination wouldnot have been possible without the overwhelmingsupport and understanding of my wife Elizabeth andmy sons, Tyler and Preston. I also want to thank myparents, Malcolm and Zelda Gross, as well as myteachers Dr. Joseph Goodgold, Dr. Bruce Grynbaum,Dr. Howard Thistle, and Dr. Matthew Lee for theirguidance and efforts on my behalf.
J.G.
Thank you to my wife and family for their under-standing, patience, support, and love.
J.F.
To my husband, Jed, for his unlimited patience, un-derstanding, and encouragement.To my business partner and friend, Sandy, for beingthere whenever I needed her.To my family for their support, and to my many pa-tients, colleagues, and friends who have helped megrow.
E.R.
v

BLBK145-Gross February 13, 2009 21:2
vi

BLBK145-Gross February 13, 2009 21:50
C H A P T E R 1
IntroductionThe intention of this book is to provide the readerwith a thorough knowledge of regional anatomy andthe techniques of physical examination. A second andequally important intention is to describe a methodfor the interpretation and logical application of theknowledge obtained from a physical examination.
What Is a Physical Examination?
The physical examination is the inspection, palpation,measurement, and auscultation of the body and itsparts. It is the step that follows the taking of a patienthistory and precedes the ordering of laboratory testsand radiological evaluation in the process of reachinga diagnosis.
What Is the Purpose of the PhysicalExamination?
The physical examination has two distinct purposes.The first is to localize a complaint, that is, to associatea complaint with a specific region and, if possible, aspecific anatomical structure. The second purpose ofa physical examination is to qualify a patient’s com-plaints. Qualifying a complaint involves describingits character (i.e., dull, sharp, etc.), quantifying itsseverity (i.e., visual analog scale; grade I, II, III), anddefining its relationship to movement and function.
How Is the Physical ExaminationUseful?
By relating a patient’s complaints to an anatomicalstructure, the physical examination brings meaningto a patient’s history and symptoms. This, however,
presupposes that the clinician possesses a thoroughknowledge of anatomy. It also requires a method-ology for the logical analysis and application of theinformation obtained from the patient’s history andphysical examination. This methodology is derivedfrom a clinical philosophy based on specific concepts.These concepts are as follows:1. If one knows the structure of a system and
understands its intended function, it is possible topredict how that system is vulnerable tobreakdown and failure (injury).
2. A biological system is no different from aninorganic system in that it is subject to the samelaws of nature (physics, mechanics, engineering,etc.). However, the biological system, unlike theinorganic system, has the potential not only torespond but also to adapt to changes in itsenvironment.Such concepts lay the foundation for understanding
the information obtained on physical examination.They also lead to a rationale for the treatment andrehabilitation of injuries. A correlation of this typeof analysis is that it becomes possible to anticipateinjuries. This in turn permits proactive planning forthe prevention of injuries.
How Does the MusculoskeletalSystem Work?
The musculoskeletal system, like any biological sys-tem, is not static. It is in a constant state of dynamicequilibrium. This equilibrium is termed homeostasis.
As such, when subjected to an external force orstress, a biological system will respond in a very spe-cific manner. Unlike the inorganic system (i.e., an air-plane wing that is doomed to fail after a predictablenumber of cycles of load), the biological system willattempt to reestablish an equilibrium state in responseto a change that has occurred in its environment. In
1

BLBK145-Gross February 13, 2009 21:50
2 Introduction Chapter 1
X
Stress
Time
X
Chronic overuse failure
Acu
te fa
ilure
Maximum tolerance limit
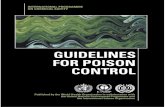
Figure 1.1 Biological systems, like inorganic systems, can fail under one of two modes: an acute single supramaximal stress orrepetitive submaximal chronic loading.
doing so, the biological system will experience one ofthree possible scenarios: adaptation (successful estab-lishment of a new equilibrium state without break-down), temporary breakdown (injury), or ultimatebreakdown (death). These scenarios can be expressedgraphically. Any system can be stressed in one of twomodes: acute single supratolerance load or chronicrepetitive submaximal tolerance load (Figure 1.1). Inthe first mode, the system that suffers acute failure isunable to resist the load applied. In the second mode,the system will function until some fatigue limit isreached, at which time failure will occur. In the bi-ological system, either failure mode will initiate aprotective-healing response, termed the inflammatoryreaction. The inflammatory reaction is composed ofcellular and humoral components, each of which ini-tiates a complex series of neurological and cellularresponses to the injury. An important consequence ofthe inflammatory reaction is the production of pain.The sole purpose of pain is to bring one’s attention tothe site of injury. Pain prevents further injury fromoccurring by causing protective guarding and lim-ited use of the injured structure. The inflammatory
response is also characterized by increased vascular-ity and swelling in the area of injury. These are thecauses of the commonly observed physical signs (i.e.,redness and warmth) associated with the site of in-jury.
However, the problem with pain is that although itbrings protection to the area of injury (the consciousor unconscious removal of stress from the injuredarea), and permits healing to take place by remov-ing dynamic stimuli from the biological system, thisremoval of stimuli (rest) promotes deterioration of asystem’s tolerance limit to a lower threshold. In thisway, when the injury has resolved, the entire system,although “healed,” may actually be more vulnerableto reinjury when “normal” stresses are applied to therecently repaired structures. This initiates the “viciouscycle of injury” (Figure 1.2).
Contrary to this scenario is one in which the biolog-ical system successfully adapts to its new environmentbefore failure occurs. This situation represents condi-tioning of a biological system. The result is hypertro-phy, enhanced function, and a consequent increase inthe system’s tolerance limit. The concept acting here is

BLBK145-Gross February 13, 2009 21:50
3Chapter 1 Introduction
Injury
Acute trauma
Repetitive overuse
Activity
Weakness, stiffness, etc.
Inflammatory response
Pain
Rest
“Vicious Cycle of Injury”
Figure 1.2 The “vicious cycle of injury” results from the reinjuryof a vulnerable, recently traumatized system. This increasedvulnerability occurs due to a diminishing of a system’s tolerancelimit as a result of adaptation to a lower level of demand duringthe period of rest necessitated by pain.
that the biological system’s tolerance limit will adaptto increased demands if the demands are applied at afrequency, intensity, and duration within the system’sability to adapt (Figure 1.3).
Therefore, during the physical examination, asym-metry must be noted and analyzed as representing ei-ther adaptation or deconditioning of a given system.Any of these fundamental principles under which themusculoskeletal system functions makes it possibleto organize the information obtained from a physi-cal examination and history into general categoriesor pathological conditions (traumatic, inflammatory,metabolic, etc.), and the subsets of these conditions(tendinitis, ligamentous injuries, arthritis, infection,etc.). From such an approach, generalizations calledparadigms can be formulated. These paradigms pro-vide a holistic view of a patient’s signs and symptoms.In this way, diagnoses are arrived at based on an anal-ysis of the entire constellation of signs and symptomswith which a given patient presents. This method,relying on a multitude of factors and their interrela-tionships rather than on a single piece of information,
such as the symptom of clicking or swelling, ensures agreater degree of accuracy in formulating a diagnosis.
What Are Paradigms?
Paradigms are snapshots of classic presentations ofvarious disease categories. They are, as nineteenth-century clinicians would say, “augenblick,” a blink-of-the-eye impression of a patient (Table 1.1). Fromsuch an impression, a comparison is made with anidealized patient, to evaluate for congruities or dis-similarities. Here is an example of a paradigm for os-teoarthritis: a male patient who is a laborer, who is atleast 50 years old, whose complaints are asymmetri-cal pain involving larger joints, and whose symptomsare in proportion to his activity. Another examplemight be that of rheumatoid arthritis. This paradigmwould describe a female patient who is 20–40 yearsold, complaining of symmetrical morning stiffness in-volving the smaller joints of the hands, with swelling,possibly fever, and stiffness reducing with activity.
Paradigms may also be created for specific tissues(i.e., joints, tendons, muscles, etc.). The paradigm fora joint condition such as osteoarthritis would be well-localized pain, swelling, stiffness on sedentary postur-ing, and pain increasing in proportion to use, whereasa paradigm for a mild tendon inflammation (tendini-tis) may be painful stiffness after sedentary posturingthat becomes alleviated with activity and gentle use.A paradigm for ligament injury would include a his-tory of a specific traumatic event, together with theresultant loss of joint stability demonstrated on activeand passive tensile loading of a joint.
The reader is encouraged to create his or her ownparadigms for various conditions—paradigms that in-clude the entire portrait of an injury or disease processwith which a given patient or tissue may be com-pared. In this process, it will become obvious that itis not sufficient to limit one’s expertise to the local-ization of complaints to an anatomical region. It isalso necessary to be able to discriminate between theinvolvement of specific structures that may lie in closeproximity within that region (i.e., bursae and tendonsoverlying a joint).
It can be concluded therefore that an accurate phys-ical examination is as critical to the process of diag-nosis as is a complete and accurate history of a pa-tient’s complaints. An accurate physical examinationdemands a thorough knowledge and familiarity withanatomy and function.

BLBK145-Gross February 13, 2009 21:50
4 Introduction Chapter 1
Time
Tolerance limit 3
Tolerance limit 2
Tolerance limit 1
Figure 1.3 Conditioning is the adaptation of a biological system to the controlled application of increasing stress at a frequency,intensity, and duration within the system’s tolerance limit, with a resultant increase in the system’s tolerance limit.
What Are the Components of theMusculoskeletal System?
The musculoskeletal system is composed of bone, car-tilage, ligaments, muscle, tendons, synovium, bursae,and fascia. This system is derived embryologicallyfrom the mesenchyme and is composed of soft andhard connective tissues. These tissues have evolved
Table 1.1 Paradigms for osteoarthritis and rheumatoidarthritis.
Paradigm for rheumatoidParadigm for osteoarthritis arthritis
Male FemaleLaborer 20–40 years old50+ years old Symmetrical small joint
involvementLarge joint involvement Associated swelling, fever,
rash, morning stiffnessAsymmetrical involvement Abating with usePain in proportion to activity
to serve two basic functions: structural integrity andstable mobility. The tissues are composite materialsmade up of cells lying within the extracellular matrixthey produce.
Collagen, a long linear protein (Figure 1.4a), is themost abundant of the extracellular materials foundin connective tissues. The foundation of collagenis a repetitive sequence of amino acids that formpolypeptide chains. Three such chains are thenbraided together to form a triple helical strand calledtropocollagen. These strands join to make microfib-rils; long linear structures specifically designed toresist tensile loading. The microfibrils are bondedtogether through chemical cross-linking to form col-lagen fibers. The degree of cross-linking determinesthe physical properties of a specific collagen fiber.The more cross-linking that exists, the stiffer the fiberwill be. The degree of collagen cross-linking is in partgenetically and in part metabolically determined. Thisexplains why some people are much more flexiblethan others. Vitamin C is critical for the formationof cross-links. As such, scurvy, a clinical expressionof vitamin deficiency, is characterized by “weak tis-sues.” Hypermobility of joints (i.e., ability to extend

BLBK145-Gross February 13, 2009 21:50
5Chapter 1 Introduction
(a)
(b)
(c) �1 chains
�2 chain
All �1 chains
Type I collagen
Type II collagen
Figure 1.4 (a) Collagen is a linear protein made of α-chains that wind into a triple helix. (b) Collagen fibrils are formed by thecross-linking of collagen monomer proteins. (c) The different types of collagen are determined by the number of α1 and α2 collagenmonomers that join to form a triple-helix collagen molecule. For example, two α1 chains and one α2 chain that join to form atriple-helix make type I collagen, which is found in bone, tendon, ligament, fascia, skin, arteries, and the uterus. Type II collagen,which is found in articular cartilage, contains three α1 chains. There are at least 12 different collagen types.
the thumbs to the forearms, ability to hyperextend atthe knees and elbows, excessive subtalar pronationwith flat, splayed feet) is a clinical manifestationof genetically determined collagen cross-linking(Figure 1.4b).
Different types of collagen exist for different cate-gories of tissues. These types are defined by the spe-cific composition of the polypeptide chains that formthe strands of the collagen molecules. Type I collagenis found in connective tissue such as bone, tendons,and ligaments. Type II is found uniquely in articularhyaline cartilage. Other collagen types exist as well(Figure 1.4c).
If collagen represents the fiber in the compositestructure of connective tissue, ground substancerepresents the “filler” between the fibers. The maincomponents of ground substance are aggregates ofpolyglycan macromolecules. An example of sucha macromolecule is the proteoglycan hyaluronicacid, found in articular cartilage. Hyaluronic acidis a molecule of more than 1 million daltons. It iscomposed of a long central core from which are pro-jected many protein side chains containing negatively
charged sulfate radicals. It can best be visualized as abristle brush from which many smaller bristle brushesare projected (Figure 1.5). These strongly negativesulfate radicals make the hyaluronic acid moleculehighly hydrophilic (water attracting). This ability toattract and hold water allows the connective tissueground substance to function as an excellent hydro-static bearing surface that resists compression load.
Immobilization reduces the diffusion and migrationof nutrients throughout the connective tissues. Thisin turn compromises cellular activity and upsets thenormal homeostatic balance of collagen and groundsubstance turnover. The result is an atrophy of col-lagen fibers and a diminution of ground substance(Cantu and Grodin, 2001), with subsequent deteri-oration of the connective-tissue macrofunction (i.e.,chondromalacia patellae).
Bone
Bone provides the structure of the body. It is the hard-est of all connective tissues. One-third of bone is com-posed of collagen fibers and two-thirds mineral salts,

BLBK145-Gross February 13, 2009 21:50
6 Introduction Chapter 1
Hyaluronic acid (HA)
Hyaluronic acidcentral “core”
Linkprotein
Keratansulfate-richregion
Chrondroitin sulfate-richregion
Keratansulfatechain
Chrondroitin sulfatechain
Protein core
Protein sidechain core
Sulfate radicals(chrondroitin and keratan sulfate)
Proteoglycan “bristle brushes”
Figure 1.5 The proteoglycan aggregate is formed on abackbone of hyaluronic acid and has the appearance of a bristlebrush.
primarily calcium hydroxyapatite. Bone is formed inresponse to stress. Although genetically determined,the size and shape of a bone are dependent on environ-mental factors for its full expression. This response ofbone to its loading history has been termed Wolff’slaw. There are two major types of bone: cortical andcancellous. All bones are covered by highly vascular-ized and innervated tissue called periosteum, exceptwhen they are within the synovial cavity of a joint(Figure 1.6).
Cortical bone is very dense, highly calcified, anduniquely constructed to resist compression loads. Itcan also resist tensile bending and torsional loads,but much more poorly. This is a direct function ofcortical bone’s ultrastructure, which is a compositeof flexible collagen fibers and rigid mineral crystals.Cortical bone is usually found within the diaphysisof long bones. It has a hollow central cavity that istermed the medullary canal or marrow cavity.
At the end of long bones and at the sites of tendonand ligament attachments, bones tend to expand andcortical bone gives way to a more porous structure,termed cancellous or trabecular bone. The trabeculaeof cancellous bones lie in the direction of transmitted
Articular cartilage
Line of epiphysealcartilage
Trabeculae ofspongy bone
Compact orcortical bone
Periosteum
Line of epiphysealcartilage
Articular cartilage
Marrow cavity
Figure 1.6 The structure of a typical long bone.
loads. They act as conduits of load from the articularsurface to the underlying diaphyseal cortical bone.Overload of the trabeculae will, on a microscopicscale, duplicate overload of an entire bone (i.e., frac-ture). This overload, because of the innervation thatexists within a bone, will give rise to pain (arthriticdiscomfort due to mechanical overload secondary tojoint deformity or erosion of articular cartilage). Theresultant healing of these microfractures leads to in-creased calcium deposition, hence subchondral scle-rosis noted around articular joints on x-ray films, andhypertrophy of stressed sites such as the midshaft ofthe tibia secondary to stress fractures occurring fromoveruse in distance running.
Cartilage
Cartilage is a connective tissue made of cells (chon-droblasts and chondrocytes) that produce an extra-cellular matrix of proteoglycans and collagen fiberswith a high water content. The tensile strength ofcartilage is due to the collagen component. Its resis-tance to compression is due to the ability of proteogly-can to attract and hold water. Cartilage types include

BLBK145-Gross February 13, 2009 21:50
7Chapter 1 Introduction
Tidemark
Subchrondral bone
Composition and Structure of CartilageArticular hyaline cartilage
HistologyZone I
Tangential
Orientation of collagen fibers
Zone IIOblique
Zone IIIVertical
Zone IVVertical
End plate
Trabecularbone
Calcified cartilage
Chondrocytesin lacunae
Matrix
Lamina splendens
Groundsubstance
H2O in and out due topressure of joint surfaces
on one another
Figure 1.7 The composition and structure of articular hyaline cartilage. Water moves in and out of the cartilage due to the pressure ofthe joint surfaces on one another and attraction of the water by the ground substance. Note the orientation of the collagen fibers.
articular or hyaline cartilage (Figure 1.7); fibrocarti-lage, which exists at the attachment sites of ligaments,tendons, and bones; fibroelastic cartilage, found inmenisci and intravertebral discs; and growth-platecartilage, located in the physis of immature bones.With age, cartilage tends to decrease in water con-tent and the number of cross-links among collagenmolecules increases. The result is that cartilage tis-sue becomes more brittle, less supple, and less ableto resist tensile, torsional, and compression loading.Hence, cartilage becomes more vulnerable to injurywith age.
Articular cartilage lines the spaces in synovialjoints. It is attached to the underlying bone by a com-plex interdigitation analogous to that of a jigsaw puz-zle. Regeneration of this cartilage is slow and incon-sistent in terms of restoration of articular integrity. Itcan be replaced by a less mechanically efficient fibro-cartilage after injuries have occurred. There are noblood vessels within articular cartilage and nutritionis solely dependent on the loading and unloading ofthe joint, which allows water-soluble nutrients andwaste products to enter and leave the cartilaginousmatrix through a porous surface layer.
The fibroelastic cartilage of the intervertebral discallows for very minimal movement between adjacentvertebrae while providing shock absorption. Becauseof the orientation of the fibers, they are more vulner-able to flexion and rotational forces. Fibroelastic car-tilage is also present in the menisci of the knee. Here,it functions not only to absorb shock but also to in-crease the functional surface area of the joint, therebyproviding additional stability. Because of its elastincontent, fibroelastic cartilage is resilient and able toreturn to its prior shape following deformation.
Ligaments
Ligaments are the static stabilizers of joints. They con-nect bones to bones (Figure 1.8). Ligaments and othercapsular structures of the joint are made of dense, or-ganized connective tissue. Ligaments contain collagenand a variable amount of elastin. The collagen pro-vides tensile strength to the ligaments and elastin pro-vides suppleness. The fibers of collagen are arrangedmore or less parallel to the forces that the ligamentis intended to resist. Most ligaments and capsular tis-sues enter the bone as a progression from collagen

BLBK145-Gross February 13, 2009 21:50
8 Introduction Chapter 1
Medial collateralligament
Lateralcollateralligament
Posteriorcruciate
ligament
Anteriorcruciateligament
Figure 1.8 The ligaments of the knee. Because of the inherentinstability of the joint, ligaments are necessary to prevent motionin all planes. They act as the primary stabilizers of the joint andare assisted by the muscles and other connective tissues.
fibers to fibrocartilage to calcified cartilage and thenfinally bone. Some ligaments (and tendons) attach tothe periosteum first, which then attaches to the bone.The site of ligament failure is a function of the load itexperiences. Ligaments resist slow loading better thanrapid loading. Therefore, rapid loading may producean intraligamental lesion, whereas a slower patternof loading will create injuries at or near the bone–ligament interface.
Elastin is a protein that permits elastic recoiling tooccur in a tissue. Some ligaments, such as the cruciateligament of the knee, contain almost no elastin. Otherligaments, such as the ligamentum flavum of the spine,contain large amounts of elastin. Figure 1.9 showsthat because it contains more collagen than elastin,the anterior cruciate ligament can resist tensile loadswith little elongation. In this way, the anterior cruci-ate ligament serves the knee well as a stabilizing struc-ture. On the other hand, the ligamentum flavum of thespine, being composed mostly of elastin and little col-lagen, can be stretched a great deal before breaking,but can only resist very weak tensile loading.
Ligaments function to limit joint motion and toguide the bones as they move. Ligaments thereforeusually have a dual internal structure, such that theymay stabilize the joint at either extreme of motion.Ligaments are most lax at midrange of joint motion.The capsule of a synovial joint is in fact a weak lig-amentous structure. Disruption of a ligament can re-sult in severe joint instability and increased frictionalstresses to the articular surfaces of that joint. Thiswill result in premature osteoarthritis. Conversely, aloss of normal capsular laxity from fibrosis follow-ing trauma will result in a severe restriction in jointmotion (i.e., posttraumatic adhesive capsulitis of theshoulder).
Ligaments have very little vascularity; hence theyheal poorly. However, they do have innervation,which may be useful to quantify the severity of a givenligamentous injury. When the structural integrity ofa ligament has been completely compromised (gradeIII sprain), relatively little pain is produced on at-tempts to passively stretch the injured ligament. Thisis because no tension load can be created across acompletely disrupted ligament. However, in a less se-vere partial tear (grade I sprain), severe and exquisitepain will be produced when tension is applied acrossthe damaged structure. This paradoxical pain pattern(less pain equals a more severe sprain) can be a sig-nificant diagnostic clue obtained during the physicalexamination of a recently injured ligament. This alsohas dramatic import in defining a patient’s prognosisand determining a treatment plan.
Muscle
Skeletal muscle is a contractile tissue made up of fibersthat contain specialized proteins (Figures 1.10 and1.11). A loose connective tissue known as endomy-sium fills the space between these fibers. This tissueattaches to a stronger connective tissue that surroundsthe muscle vesiculae, known as perimysium. Perimy-sium is in turn connected to the epimysium, whichencases the entire muscle. This in turn is anchored tothe fascial tissues of the nearby structures. Musclestherefore are composed of two elements: contractiletissues and inert, noncontractile tissues. The forcesgenerated by the muscles are extrinsically applied tothe muscle and will affect both types of tissue.
Muscles exist in many shapes and sizes. Some ofthese are shown in Figure 1.12.
Muscles contain three different fiber types: I, IIa,and IIb. They are defined by the chemical machineryused to generate adenosine triphosphate (ATP).

BLBK145-Gross February 13, 2009 21:50
9Chapter 1 Introduction
Anteriorlongitudinalligament
Ligamentum flavum
Breaking point
Breaking point
STRAIN (extension/original length)
STR
ESS
(lo
ad/c
ross
-sec
tion
are
a)
Figure 1.9 The mechanical response of stress and strain on the anterior longitudinal ligament and the ligamentum flavum. Theanterior cruciate ligament, having more collagen than elastin, can handle a larger load but will only stretch a short amount beforebreaking. The ligamentum flava, having more elastin than collagen, cannot tolerate a very large load but can stretch a lot beforebreaking.
Genetic makeup, training, and neuromuscular dis-ease can affect the composition of a given musclewith respect to fiber type. Characteristics of thesevarious fiber types are shown in Table 1.2.
Muscles act to move body parts or to stabilize ajoint. As dynamic stabilizers of joints, muscles serveto duplicate the static stabilizing action of ligaments.Muscle fibers are capable of shortening to about50% of their original length. The tension developedby a contracted muscle can be either active or pas-sive. Active tension is due to the contractile compo-nents, namely, actin and myosin. Passive tension re-sults from elastic properties of the contractile tissueswithin the muscle.
The strength of the muscle is proportional to itscross-sectional area and mass. The force of contrac-tion of a muscle is related to many factors, includ-ing the length of the fibers, the velocity of contrac-tion, and the direction in which the fiber is movingat the time of its contraction. Types of muscle con-traction include concentric or shortening, eccentricor lengthening, and isometric, in which the muscle
does not change length. Muscles are characterized bytheir function; agonists are prime movers, antagonistsresist the action of prime movers, and synergists sup-port the function of the agonists. For example, inankle dorsiflexion, the anterior tibialis is the agonist.The extensor hallucis longus and extensor digitorumlongus muscles assist the tibialis anterior muscle andtherefore are synergists. The gastrocnemius and soleusand plantar flexors of the toes are antagonists of thetibialis anterior.
Muscles are described in anatomy texts as havingorigins and insertions. It is very important to recog-nize that this is an arbitrary distinction. A muscle thatis referred to as a hip flexor because it brings the thightoward the torso can function just as well to bring thetorso over the thigh. In order for muscles to functionnormally, they must be both strong and flexible.
With respect to innervation of muscles, except forthe deepest layers of the vertebral muscles, the exactinnervation of the limb and trunk muscles is simi-lar between individuals, with some variability. Tableslisting segmental innervation differ from text to text.

BLBK145-Gross February 13, 2009 21:50
10 Introduction Chapter 1
I bandA band
A bandSarcomere(from Z line to Z line)
Muscle fiber is a bundleof myofibrils
Muscle consists ofmuscle fibers
Intact muscle
Muscle cell (fiber)
Myofibril
Two sarcomeres
Z lines
Enlarged view
Z lineZ line M line
Stripes or striations
Figure 1.10 A microscopic view of muscle shows the repeated patterns of the sarcomeres and the fibrils.
Injuries to muscles are termed strains. Analogous toligament injuries, they are classified by severity intothree grades: grade I indicates minimal damage;grade II represents an intermediate amount of dam-age to the muscle structure; and grade III, completedisruption.
Tendons
Tendons connect muscles to other structures (see Fig-ure 1.13). Like ligaments, tendons are also composedof collagen, ground substance, and cells. The collagenof tendons is aligned in a very strict linear fashion

BLBK145-Gross February 13, 2009 21:50
11Chapter 1 Introduction
Muscle fascicles
Muscle fiber
Z Z
H
A
M
Z Z
I
Myofilaments
Sarcomere
Endomysium
Epimysium
Perimysium
Myofibril
SarcolemmaSarcoplasmNuclei
Satellite cell Basement
Muscle
Figure 1.11 The organization of skeletal muscle tissue.
Parallel muscle fibers
Fan-shaped fibers
Unipennate muscle
Bipennate muscle
Fusiform muscle
Figure 1.12 Different types of muscle–fascicle arrangements.

BLBK145-Gross February 13, 2009 21:50
12 Introduction Chapter 1
Table 1.2 Characteristics of skeletal muscle fibers based on their physical and metabolic properties.
Muscle fiber type
Property Slow-twitch Intermediate Fast-twitch
Speed of contraction Slow Intermediate FastRate of fatigue Slow Intermediate FastOther names used Type I Type II B Type II A
Slow oxidative Fast oxidative/glycolytic Fast glycolyticMuscle fiber diameter Small Intermediate LargeColor Red Red WhiteMyoglobin content High High LowMitochondria Numerous Numerous FewOxidative enzymes High Intermediate LowGlycolytic enzymes Low Intermediate HighGlycogen content Low Intermediate HighMyosin ATPase activity Low High HighMajor source of ATP Oxidative phosphorylation Oxidative phosphorylation Glycolysis
ATP, adenosine triphosphate.
and is always oriented in the line of the pull of themuscle. Tendons have been designed to transmit theforce of the muscular contractile tissues to bone andother connective tissues, such as skin and ligaments,to which they are attached. Tendons are said to beable to withstand at least twice the maximum forcethat muscles can exert on them. The zone wherethe muscle blends into the tendinous tissues is calledthe musculotendinous junction. Muscle–tendon unitsrepresent tensile structures. As such, they may failin the muscle, at the muscle–tendon junction, withinthe tendon, or at the tendon–bone insertion. Mostcommonly, however, failure occurs at the pointof transition between two different materials (i.e.,the musculotendinous junction). Some tendons aresurrounded by a double-walled tubular covering,
referred to as a tendon sheath or a peritendon (i.e.,Achilles tendon or flexor tendons of the hand). Thisis lined with a synovial membrane. The sheath is usedboth to lubricate the tendon and to guide it towardthe bony attachment. Tendon sheaths provide apathway for the gliding movement of the tendonwithin the sheath. An inflamed tendon sheath cancause a locking or restricted movement, as in a triggerfinger. Inflammation of the tendon structure is termedtendinitis.
Synovium and Bursae
Synovial tissue lies in the inner aspect of synovialjoints and bursal sacs. It has two functions: to pro-duce lubricating fluids and to phagocytize (remove)
Muscle
Ligament
Tendon
Figure 1.13 A tendon.

BLBK145-Gross February 13, 2009 21:50
13Chapter 1 Introduction
Ulna
Humerus
Radius
Olecranon process
Olecranon bursa
Skin
Skin
Figure 1.14 The olecranon bursa is between the skin and theolecranon process at the elbow.
foreign debris. Synovium is highly vascularized andinnervated. As such, when traumatized or inflamed,synovial tissue will rapidly enlarge and produce sig-nificant pain.
Bursal sacs serve to reduce friction. Therefore, theyare located wherever there is need for movement be-tween structures in close proximity. For example, theolecranon bursa lies between the olecranon process ofthe ulna and the skin overlying the posterior part ofthe elbow (see Figure 1.14). The subacromial bursalies between the acromioclavicular arch above and
the rotator cuff tendons below. Inflammation of syn-ovial or bursal tissues due to trauma, inflammatoryprocesses, or foreign materials is termed synovitis orbursitis.
Fascia
There are three kinds of fascial tissues: superficial,deep, and subserous. The fascia is composed of looseto dense connective tissue. Superficial fascia is underthe skin; deep fascia is beneath the superficial and alsoenvelops the head, trunk, and limbs. Subserous fasciasurrounds organs in the thorax, abdomen, and pelvis.
Superficial fascia contains fat, blood vessels, andnerves. It is loose in consistency and very thin. It isattached to the undersurface of the skin.
Deep fascia is dense and tough and has two lay-ers. It wraps around regions of the body and splitsto envelop superficial muscles such as the sartoriusand tensor fasciae latae. Periosteum, perimysium, andperichondrium are all elements of the deepest layer ofthe deep fascia. The deep fascia serves to interconnectthe different muscle groups. By being continuous, itcan provide tension at a distant site when pulled bya contracting muscle. Some muscles take their ori-gin from the deep fascia. The fascia also separatesgroups of muscles with similar function, for exam-ple, the flexor and extensor groups of the leg. Becauseof the relative inelasticity of fascia, abnormally highpressure within a fascial compartment (i.e., due to in-jury or inflammation) can compromise the functionof the nerves and blood vessels that course throughthat compartment. This may result in serious com-promise of the tissues supplied by these nerves andvessels. Fascia may, as other tissues, experience an in-flammatory reaction, fasciitis. This condition can beaccompanied by moderate or even severe discomfortand scarring (fibrosis). Fibrosis can lead to stiffnessand restricted movement.

BLBK145-Gross February 13, 2009 20:34
C H A P T E R 2
Basic Concepts of PhysicalExaminationIntroduction
The ability to examine a joint completely and accu-rately is a critical part of the diagnostic process forthe clinician evaluating an orthopedic problem. Toaccomplish this, the clinician must possess a thoroughknowledge of anatomy, biomechanics, and kinesi-ology, as well as an understanding of the structure,purpose, and response of the various tissues. Informa-tion is obtained through observation and palpation.The clinician must be able to determine whether thepatient’s pathology is of musculoskeletal origin.
The examination process must be performed in aspecific and logical order. This order will remain thesame regardless of whether the clinician is examiningthe shoulder joint or the spine. It is important forthe examiner to develop the habit of utilizing a setsequence in order to be as organized and efficientas possible and to avoid inadvertently omittinginformation.
Observation
The examination should begin in the waiting roombefore the patient is aware of being observed.Information regarding the degree of the patient’spain, disability, level of functioning, posture, andgait can be observed. The clinician should pay carefulattention to the patient’s facial expressions withregard to the degree of discomfort the patient reportsthat he or she is experiencing. Observing the patientsitting and coming to a standing position will provideinsight into the patient’s ability to tolerate flexion andto then go from flexion to extension. Observation ofthe patient’s gait will provide information regardingthe ability to bear weight, strength of push-off,
balance in relationship to unilateral stance, andcadence. The information gathered in this shortperiod could be very useful in creating a total pictureof the patient’s condition.
Subjective Examination (History)
The patient should be escorted to a private area toenable the clinician to begin the subjective portionof the examination. The patient will be much morecomfortable and relaxed if he or she is allowed to re-main dressed during this part of the examination. Theclinician should pay close attention to the details ofthe present bout and all previous related bouts. Thepatient deserves and will appreciate the examiner’sundivided attention, even if only for a short period. Askilled clinician must be able to listen politely whiledirecting the interview. Concise and direct questionsposed in a logical order will help to provide the ap-propriate information.
The clinician should begin the interview by deter-mining the history of the present bout. Questionsshould include the following: When did the episodebegin? What was the etiology (traumatic vs. insidi-ous)? Are the symptoms the same or are they increas-ing? It is important to determine whether there wereany previous episodes, and if there were, to determinewhen they occurred, what the etiology was, how longthey lasted, and how they resolved (Box 2.1).
It is helpful to elicit whether the pain is constantor intermittent. Symptoms that are brought about bychanging position may be mechanical in nature. If thesymptoms remain unaltered regardless of position oractivity, they may be chemical in nature, secondaryto the release of noxious substances that are at asufficient level to irritate the nerve endings. Constantpain that changes in intensity or quality is considered
14

BLBK145-Gross February 13, 2009 20:34
15Chapter 2 Basic Concepts of Physical Examination
Box 2.1 Typical Questions for the SubjectiveExamination
Where is the pain located?How long have you had the pain?How did the pain start? Was it traumatic or insidious?Is the pain constant or intermittent?If it is intermittent, what makes it better or worse?How easy is it to bring on the complaint?Describe the pain (nature of pain)?What is the intensity of the pain (0–10)?Does the pain awaken you at night?What position do you sleep in?What are your work and leisure activities?What type of mattress and pillow do you use?How many pillows do you sleep on?Does the pain change as the day progresses?Have you had a previous episode of this problem?If yes, how was it treated?
Past medical history (PMH):Thorough systems reviewSpecific questions are beyond the scope of this text
Medications:Are you taking any medication?For which problem (symptom) is the medication providingrelief?
Special questions:Specific questions and concerns related to each joint arediscussed in the individual chapters.
to be intermittent (Cyriax, 1979). It is also useful todetermine what makes the symptoms better or worseand how long the symptoms remain following theironset. If a patient develops pain very quickly whileperforming an activity and the pain lasts a long time,the clinician would consider the patient’s pain to beirritable (Maitland et al., 2005). It would be beneficialto modify the physical portion of the examinationso as not to exacerbate the symptoms. The pain canalso be followed over a 24-hour period. Is the patientbetter or worse at times throughout the course ofthe day? If the patient is stiffer in the morning onarising, he or she may not be using a firm mattress,may be sleeping in an inappropriate position, or mayhave osteoarthritis, which presents with increasedstiffness following prolonged inactivity. A painscale (McGill Pain Scale; Melzack, 1975) or numeric(visual pain rating, 0–10) may be used to gain a betterunderstanding of the patient’s perception of pain.
To organize the information that is obtained, it ishelpful to use a body chart (Figure 2.1). This chart
allows information to be recorded graphically for ob-servation and comparison. The chart also enables therecording of information concerning areas other thanthe one affected. If an area is examined and foundto be asymptomatical (clear), a check mark can beplaced over that area to indicate that it has been ex-amined and found to be free of symptoms. For ex-ample, if the patient presents with pain in the righthip on the day of the initial examination but returnswith pain in the left hip 2 weeks later, the cliniciancan quickly refer back to the diagram to confirm thehistory.
Information must be gathered regarding the pri-mary area of the complaint and any related area(s).Areas of radiating pain, anesthesia, or paresthesiashould be noted. This allows the clinician to developa better total picture of the problem. It will alsohelp to assess whether there is any relationshipbetween the areas. For example, if the patient’smajor complaint is that of low back pain andpain in the right knee, there may or may not be adirect relationship. Perhaps the patient has radicularpain in an L3 dermatomal pattern, or perhaps thatpatient’s injury was secondary to a fall in which thepatient landed on the right knee at the same timethe back was injured. The quality or description ofthe pain (stabbing, nagging) in the patient’s ownwords must also be noted. If the patient complainsof burning pain, the nerve root might be implicated,whereas a deep ache may be associated with muscledysfunction.
Objective Examination
Dominant Eye
Accuracy in observation requires the use of visual dis-crimination. This can best be accomplished by usingthe dominant eye. Determination of the dominant eyeis done as follows: the clinician extends both armsand uses the thumb and the index finger to make asmall triangle. A distant object is then selected andaligned in the center of the triangle. The clinician thencloses the left eye and checks if the object remainsin the same position or if it moves. If it remains,the clinician is right-eye dominant. The procedure isrepeated for the other eye. The dominant eye shouldbe checked periodically since it may change. Thedominant eye should be placed over the center ofall structures as they are being examined to allow

BLBK145-Gross February 13, 2009 20:34
16 Basic Concepts of Physical Examination Chapter 2
X
X
Figure 2.1 Body chart.
for more accuracy in visualization (Isaacs andBookhout et al., 1992).
Structural Examination
The posture or structural examination is a staticobservation of the patient. This is an extremely
important part of the total examination process. Youcan obtain a considerable amount of informationregarding the patient on the basis of structurealone. Normal posture is maintained by balanced,strong, and flexible muscles, intact ligaments, freelymoving fascia, healthy, properly functioning joints,a balanced line of gravity and good postural habits.

BLBK145-Gross February 13, 2009 20:34
17Chapter 2 Basic Concepts of Physical Examination
Changes in postural alignment may be secondary tostructural malformation, joint degeneration, bonedeterioration, joint instability, a change in the centerof gravity, poor postural habits, or pain. Faultyalignment creates unnecessary stress and strain onthe individual, creating either excessive elongation oradaptive shortening of muscles. Muscle elongation orshortening results in decreased efficiency while per-forming even the easiest of activities. The structuralexamination will help you gain a better understandingof the patient’s predisposition to overuse or to injury.
The structural examination allows you to integratethe structure and function of all the joints. Recognizethat when a person develops elongated or shortenedmuscles, he or she may not develop symptoms imme-diately. It may take many years of stress and strainfor problems to reach clinical recognition.
To begin the examination, the patient is asked todisrobe and is provided with an appropriate garment,which allows you to expose the areas that are be-ing examined. It is important that the lighting in theroom is equally distributed so there are not any shad-ows. The patient should be instructed to stand in themiddle of the examining room with their feet approx-imately 6 in. apart so that you can observe him orher from the anterior, posterior, and lateral views.Note whether the patient is distributing the weightequally between both feet. Most examiners prefer tohave the patient remove his or her shoes to observe thefeet. If, however, the patient has a known leg lengthdiscrepancy and uses a lift or wears an orthotic de-vice, have the patient wear the shoes with the liftor orthotic device in place. Observe the patient withand without inserts or lifts. Pay particular attentionto symmetry of structure including bony landmarks,muscle tone, bulk, guarding, atrophy, and alignmentof the joints. The optimal, most efficient posture issymmetrical and balanced. Recognizing that no oneis perfectly symmetrical, minor variations are con-sidered to be functional. Significant differences maybe secondary to anatomical malposition which is ei-ther congenital or acquired; mechanical dysfunctionwhether hypomobile or hypermobile; or dysfunctionof the soft tissue whether hypertrophied, atrophied,taut, or slack.
The examination is approached in a logical fash-ion, proceeding either in a cranial or caudal direction.Here, we describe the examination from the feet firston the basis of the assumption that the weight-bearingstructures will influence the structures that rest onthem. It is helpful to compare any affected jointsto those on the “normal” opposite side. Information
from this examination can be quickly recorded on abody chart for ease of documentation and recall.
Posterior View
Normal
In a normal individual the calcaneus is in neutralalignment with the Achilles tendon vertically aligned.The feet should show 8–10 degrees of toeing out.The medial malleoli should be of equal height onboth sides. The tibias should be straight without anybowing or torsion. The popliteal fossae should be ofequal heights and the knee joints should show 13–18 degrees of valgus. The greater trochanters and thegluteal folds should be of equal heights. The pelvisshould be the same height on both sides, with theposterior superior iliac spines level on the horizontalplane. The spine should be straight without any lat-eral curves. The scapulae should be equidistant fromthe spine and flat against the thoracic cage. The levelsof the inferior angles and the spines of the scapulaeshould be equal in height. The shoulders should be ofequal height. Patients may demonstrate a hand dom-inance pattern where the dominant shoulder is lowerand the corresponding hip higher (Kendall, 1993).The head and neck should be straight without anylateral tilt or rotation (Figure 2.2).
Possible Deviations from the Norm
Start by observing the patient’s feet. Does the patientdemonstrate pes planus or cavus and to what degree?Is the patient able to put the entire foot on the groundwhile not wearing shoes, or does he or she need a shoewith a heel because of an equinus deformity? Whatis the alignment of the calcaneus? Is there an exces-sive degree of varus or valgus (Figure 2.3)? Checkthe alignment of the Achilles tendon. Note the girthand symmetry of the calves. Is any atrophy or edemanoted? Note the length of the leg. Does one tibia ap-pear to be shorter than the other? Is there any bowingof the tibia or tibial torsion?
Check the alignment of the knee joints. From theposterior aspect you can observe genu recurvatum,varum, or valgum (Figure 2.4). Any of these deformi-ties will cause a functional leg length difference unlessthey are symmetrical bilaterally. Note the height ofthe fibular heads. A difference in height may indicatean anatomical leg length difference in the tibia andfibula.

BLBK145-Gross February 13, 2009 20:34
18 Basic Concepts of Physical Examination Chapter 2
Figure 2.2 Normal posterior view.
Figure 2.3 Calcaneal valgus deformity.
(a)
(b)
Figure 2.4 Genu varum (a) and valgum (b) deformities.

BLBK145-Gross February 13, 2009 20:34
19Chapter 2 Basic Concepts of Physical Examination
Figure 2.5 Scoliosis.
Note the alignment of the hip joint. Increased flex-ion may be present secondary to a hip flexion con-tracture (see pp. 324, 327, Figure 11.66). To confirmthis, a Thomas test would have to be performed to testfor hip flexor length. Is there excessive medial or lat-eral rotation? Check the relative heights of the greatertrochanters. A difference in height may be secondaryto a structural difference in the length of the femur.
Check the pelvis. Place your hands on the iliac crestsand observe their relative heights. If one is higher thanthe other, it may be secondary to a pelvic torsion,a structural anomaly, or a structural or functionalshort leg. Place your hands on the posterior superioriliac crests and note their relative location. A changein height may be secondary to a pelvic rotation, asacroiliac dysfunction, or a leg length discrepancy.
Observe the spine. First pay attention to the soft tis-sue. Are there any areas of muscle guarding or spasm?These may be secondary to a facilitated segment orsurrounding an area of dysfunction. Note any differ-ences in the skinfolds. This will allow you to bettervisualize lateral curves and spinal rotations. Note thealignment of the spinous processes. Is the back instraight alignment or does the patient present witha scoliosis (Figure 2.5) or kyphosis (Figure 2.6)? If
scoliosis is present, note the rib cage, the degree of ro-tation, and the presence of any lateral humps. Is theresymmetrical rib expansion both anteriorly/posteriorlyand laterally? Is a lateral shift present? Is the patientable to stand in the erect position or is he or she for-ward or laterally flexed?
Observe the scapulae. Are they equidistant fromthe spine? Are they of equal height? Are they overlyabducted or adducted (Figure 2.7)? Is one side winged(Figure 2.8)? This may be secondary to weaknessof the serratus anterior muscle or long thoracicnerve palsy. Is a Sprengel’s deformity present (Figure2.9)? Note the muscle bellies of the infraspinatus,supraspinatus, and teres major and minor musclesover the scapula. Is there an area of atrophy?Disuse atrophy may occur in the supraspinatus orinfraspinatus following a rotator cuff injury. Note therelative shoulder heights and position. Pay attentionto the upper trapezius and note any hypertrophy oratrophy. Note the upper extremities. Does the patientposition both arms in the same manner? Is one armheld farther away from the trunk or in either moreinternal or external rotation? This can be secondaryto muscle shortening and imbalances or fascialrestrictions.

BLBK145-Gross February 13, 2009 20:34
20 Basic Concepts of Physical Examination Chapter 2
Figure 2.6 Rounded thoracic kyphosis.
X
X is more than two inches
Figure 2.7 Abducted scapula.
Figure 2.8 Winged scapula.
Observe the position of the head and neck. Is thehead in a forward, rotated, or laterally flexed posture?Can the patient hold the head up against gravity?
Anterior View
Normal
The feet should show 8–10 degrees of toeing out.There should be a normal medial longitudinal archthat is symmetrical bilaterally. The navicular tuberos-ity should be located on Feiss’ line (see p. 385, Fig-ures 2.19, 13.7) (from the medial malleolus to thefirst metatarsophalangeal joint). The tibias shouldbe straight without bowing or torsion. The kneesshould show 13–18 degrees of valgus (normal Q an-gle) (see Figures 12.9, 12.12). The patellae shouldpoint straight ahead. The fibular heads should be ofequal height. The pelvis should be of equal height onboth sides. The anterior superior iliac spines shouldbe level bilaterally. The spine should be straight with-out any lateral curves. Although the spine is not di-rectly visible from this view, you can surmise curvesby observing the anterior trunk and the pattern inwhich the hair grows. The rib cage should be sym-metrical without any protrusion or depression of theribs or sternum. The shoulders should be of equal

BLBK145-Gross February 13, 2009 20:34
21Chapter 2 Basic Concepts of Physical Examination
Figure 2.9 Sprengel’s deformity.
height. The slope and development of the trapezeiishould be symmetrical. The acromioclavicular joints,the clavicles, and the sternoclavicular joints should beat equal heights and symmetrical. The arms shouldhang equally from the trunk with the same degree ofrotation. The elbows should demonstrate equal val-gus (carrying angle) (see p. 201) bilaterally. The headand neck should be straight without any rotation orlateral tilt.
The normal posture of the jaw should be wherethe lips are touching but relaxed and with a smallspace between the upper and lower teeth. The tongueshould be on the hard palate behind the upper teeth(see pp. 92–93, Figure 5.16 and Figure 2.10).
Possible Deviations from the Norm
Starting from the feet, observe the patient’s mediallongitudinal arch. Does the patient have a normalarch or is a pes planus (Figure 2.11) or cavus present?Note whether the patient has hammertoes (Figure2.12), hallux valgus (Figure 2.13), or claw toes. Whatis the appearance of the toenails? Are they discolored,brittle, thickened, or absent? Note the color of the pa-tient’s feet and the pattern of hair growth. This willgive the information regarding the patient’s peripheralvascular status by noting any deviations from normal.
Figure 2.10 Normal anterior view.
Feiss’s line
Figure 2.11 Pes planus deformity.

BLBK145-Gross February 13, 2009 20:34
22 Basic Concepts of Physical Examination Chapter 2
Figure 2.12 Hammertoe deformity.
Observe the tibia. Note whether any bowing ortibial rotation is present. The patient may have tibialtorsion. Note the relative heights of the fibular heads.Pay attention to the patellae. Do they squint (Figure2.14) or are they bullfrog eyes (see pp. 340–341 and
Figure 2.13 Hallux valgus deformity.
Figure 2.14 Squinting patellae. The patellae face each other.
Figure 12.10)? Are they of equal height? Observethe anterior aspect of the thigh and note whether thepatient presents with quadriceps atrophy. Does thepatient present with genu recurvatum, valgum, orvarum (Figure 2.15)?
Observe the hip joint. Is there excessive medial orlateral rotation? There may be an excessive amountof anteversion or retroversion present. Is a hip flexioncontracture present? Is the patient’s hip postured inan abnormal position? Note the heights of the greatertrochanters. Place your hand over the iliac crest andcheck for leg length discrepancies. Place your fingersover the anterior iliac crests and note whether theyare symmetrical. Changes in relative height may besecondary to pelvic rotation, sacroiliac dysfunction,or structural or functional leg length discrepancies.
Observe the patient’s trunk. If the patient has chesthair, you will more easily be able to determine if a sco-liosis is present by observing changes in the growthpattern. Observe the patient’s chest. Note symmetryof expansion during the breathing cycle. Is there sym-metrical rib expansion both anteriorly/posteriorly andlaterally? If a scoliosis is present, note the rib cage,the degree of rotation, and the presence of any lateralhumps. Is a lateral shift present? Is the patient able to