Muscular System PTA 120 Pathophysiology Week 6. Discuss anatomic structures and physiologic...
53
Muscular System PTA 120 Pathophysiology Week 6
-
Upload
mariah-brown -
Category
Documents
-
view
214 -
download
0
Transcript of Muscular System PTA 120 Pathophysiology Week 6. Discuss anatomic structures and physiologic...

Muscular SystemPTA 120
Pathophysiology Week 6

Discuss anatomic structures and physiologic processes related to the muscular system
Discuss physical effects of aging on the body
Define muscular pathological conditions including signs and symptoms of each.
Objectives

Muscular atrophy Fibromyalgia Myofascial pain syndrome Complex regional pain syndrome Myopathy Muscular Dystrophy Torticollis Down Syndrome
Objectives

Discuss the modifications and precaution that may be required for the treatment of patients with muscular disorders.
Demonstrate understanding of the PTA’s role in the disease processes.
Objectives

Pathology for The Physical Therapist Assistant, Ch 1 pp 8 – 9, Ch. 6
Physical Therapy Clinical Handbook for PTAs
Textbooks


Produce movement Maintain posture Stabilize joints
Tendons – reinforce and stabilize joints Generate heat
By-product of muscle activity Vital in maintaining body temperature
Skeletal muscle – at least 40% of body mass
Function of Muscles

Follows inflammatory process
High level of blood and nerve supply
Heals with scar tissue formation which may reduce muscle function due to decreased extensibility
Healing of muscles and tendons

6 hours Fragmentation of injured muscle fibers begins
7 days Muscle tendon is reduced Scar tissue is seen in large muscles Muscle is able to produce near normal
tension 11 days
Regenerating myotubes are seen 6 weeks – 6 months
Contraction is 90% normal
Healing

5 days Wound gap is filled by phagocytes
7 days Collagen synthesis is initiated and placed
in a random disorganized way 4 weeks
Collagen is fully oriented with the tendon’s long axis
2 months Collagen is mature and realigned along
tendon’s axis
Healing time for tendons

Physiologic Change Functional Effect
Decreased muscle mass Correlates directly to decreases in activityDecreased strength and altered gait
Reduced glycogen stores Decreased endurance and increased fatigue
Degenerated elastic fibers in connective tissue
Correlates directly to decreases in activityReduced flexibility
Effects of aging on the muscular system

Muscular Disorders

Types of growth changes of cells
Atrophy Reduction in cell size
Hypertrophy Increase in cell size
Metaplasia Change of cell from one
type to another
Hyperplasia Increase in number of cells
Involution / hypoplasia Decrease in number of cells

Description Disuse atrophy Muscle wasting Decrease in muscle cell diameter Flaccidity – lacking normal tone (first
stage)
Muscular Atrophy

Etiology Prolonged inactivity Trauma Poor nutrition Motor nerve dysfunction
Signs and Symptoms Muscle appears smaller, looser, flattened Decreased strength, overall weakness
Muscular Atrophy

Treatment Physical activity Exercise Active and passive movements
Muscular Atrophy

Description Chronic, generalized syndrome Diffuse soft-tissue pain and physical
findings of multiple tender points Diagnosis made after 3 month history of
wide-spread pain and 11-18 bilateral tender points on palpation
Fibromyalgia Syndrome

Periods of exacerbation and remission 6 million people in US affected Women 20-50 years old Chronic fatigue syndrome – early form
Fibromyalgia Syndrome

Etiology Experience pain from stimuli not normally
perceived as painful Due to lowered pain thresholds Unbalanced autonomic nervous system
response to physical, chemical, and physiologic stressors
Fibromyalgia Syndrome

Imbalance of substance P (neuroreceptor and neuromodulator related to transmission of pain to the CNS) Develops after psychological trauma,
local or general infections, medications, excessive use of aspartame, physical trauma
Fibromyalgia Syndrome

Signs and Symptoms Pain
Aching, burning, gnawing Localized becoming more generalized 90% of waking hours affected
Fibromyalgia Syndrome

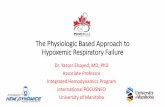
Fibromyalgia Syndrome
From Redrawn from Freundlich B, Leventhal L: The fibromyalgia syndrome. In Schumacher HR Jr, Klippel JH, Koopman, WJ, eds: Primer on the rheumatic diseases, ed 11, Atlanta, 1977, Arthritis Foundation. Copyright 1997. Reprinted with permission of the
Arthritis Foundation, 1330 W. Peachtree St., Atlanta, GA 30309.

Signs and Symptoms Muscle pain, tender points Visual disturbances Mental and physical fatigue Sleep disturbances Morning stiffness Mitral valve prolapse
z.
Fibromyalgia Syndrome

Signs and Symptoms Global anxiety Cognitive problems Irritable bowel syndrome Headaches Hypersensitivity to noise, odors, heat/cold Depression Urinary urgency or frequency TMJ dysfunction
Fibromyalgia Syndrome

Treatment Medications for depression and/or pain relief Stress reduction Pain management
Improve flexibility Graded exercise program Modalities for pain relief Aerobic exercise routines for endurance
Fibromyalgia Syndrome

Description Muscular pain disorder with the presence of
localized trigger points which produce pain Etiology
Sudden overload or overstretching of muscle Direct trauma Postural distortions Psychologic stress Chronic repetitive or sustained muscle activity
Myofascial Pain Syndrome

Myofascial Pain Syndrome

Signs and Symptoms Palpable taut band which is tender with
reproducible referred pain patterns Local twitch responses during palpation Reduced range of motion and muscle
weakness
Myofascial Pain Syndrome

Treatment Press and stretch technique Injections Acupuncture, dry needling Pain management
Physical Therapist identifies trigger points Desensitization with acupressure, modalities ,
and stretching Postural re-education Aerobic conditioning
Myofascial Pain Syndrome

Fibromyalgia vs. Myofascial Pain Syndrome
Variable Fibromyalgia MPS
Location Generalized Regional
Primary symptom
Tender points with pressure application
Trigger points and referred pain patterns with pressure application
Gender Female/Male ratio (10:1)
Equal
Systemic signs Many FewAdapted from McCance KL, Huether SE: Pathophysiology: the biologic basis for disease in adults and children, ed 5, St. Louis, 2006, Mosby.

Description Also known as Causalgia, Reflex
Sympathetic Dystrophy Chronic pain condition Continuous, intense pain out of proportion
to the severity of the injury Most often affects one arm, leg, hand, or
foot
Complex Regional Pain Syndrome

Etiology Unknown Sympathetic nervous system can play a
role Immune response triggering inflammatory
response
Complex Regional Pain Syndrome

Signs and Symptoms Pain that begins in a portion of a limb and
can spread to the entire limb Changes in color and temperature of the
skin Intense burning pain, skin sensitivity,
sweating, swelling
Complex Regional Pain Syndrome

Treatment Focused on pain relief Corticosteroids, opiates, antidepressants Sympathetic nerve block, spinal cord stimulation,
intrathecal drug pumps No drug or combination of drugs have produced
consistent long-term improvement in symptoms Early mobilization of the limb post-surgery Modalities to decrease pain and hypersensitivity Tactile desensitization activities Exercise, reduce guarding of affected limb Physical Therapy is sometimes controversial , can be
unsuccessful
Complex Regional Pain Syndrome

Description Non-specific muscle weakness secondary
to identifiable disease or condition Can be classified as inherited (Muscular
Dystrophy), or acquired (inflammatory, Rheumatoid Arthritis)
Myopathies

Signs and Symptoms Progressive proximal muscle weakness Varying degrees of pain and tenderness Acute inflammation, painful movement Symptoms of systemic illness
Fever, fatigue, morning stiffness, anorexia
Inflammatory Myopathies

Treatment Corticosteroids or immunosuppressive
medications EMG to detect changes in the muscle
Positioning and prevention of contractures Avoid overexertion to prevent damage to muscle
fibers Exercise programs, aquatic therapy Patient education with home programs, energy
conservation, any affected ADLs (activities of daily living)
Inflammatory Myopathies

Description Genetic muscle diseases characterized by
progressive weakness and atrophy of skeletal muscles
Symptoms and disease progression range from mild to severe
Many types, with Duchenne MD and Becker’s MD the most common
Muscular Dystrophy

Etiology Duchenne and Becker’s MD are x-linked,
recessive, inherited, genetic diseases Genetic defect causes lack of dystrophin in DMD,
and altered dysfunctional dystrophin in BMD Limb-girdle MD is from an autosomal dominant
or autosomal recessive genetic defect Facioscapulohumeral MD is from an autosomal
dominant genetic trait
Muscular Dystrophy

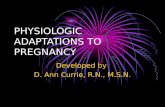
Signs and Symptoms Loss of muscular strength, lack of
coordination, progressive deformity, eventual disability
Muscles become hypertrophied with connective tissue
“Gower’s sign” Weakness spreads distally and to lungs
Muscular Dystrophy
From Jorde LB et al: Medical genetics, ed 3, St. Louis, 2006, Mosby.

Treatment No known successful cure has been
developed yet; possibility of stem-cell therapy
Orthopedic devices and surgery to address deformities
Medications if necessary to address seizures and infections as needed
Muscular Dystrophy

Duchenne muscular dystrophy Occurs only in males Age of onset: 2-6 years Muscles initially affected: hip and shoulder
girdle Symptoms/course: severe, death around
25 years of age Associated findings: mental retardation
Types of Muscular Dystrophies

Becker’s Age of onset: 5-25 years Muscles initially affected: hip and shoulder
girdle Symptoms/course: mild but progressive,
more normal life span
Types of Muscular Dystrophies

Limb/girdle Age of onset: teens to adulthood Muscles initially affected: hip and shoulder
girdle Symptoms/course: moderate weakness,
slow progression Associated findings: cardiomyopathies Life span usually normal
Types of Muscular Dystrophies

Myotonic Age of onset: usually adulthood Associated findings: cataracts, cardiac, and
endocrine disorders Life span usually normal
Maintain strength and function as long as possible, while avoiding overexertion
Equipment and adaptive device consultations, changing as disease progresses
Team approach with Occupational and Speech Therapists
Types of Muscular Dystrophies

Description Also called wryneck Spasms of the sternocleidomastoid muscle Scalenes, trapezius, splenius muscles may
be involved Unilateral causing tilt and/or rotation of
head Although a condition in children, can also
refer to acquired cases in adulthood
Torticollis

Etiology Possible injury to the sternocleidomastoid
muscle Intrauterine position, continues with
positioning after birth Result of ear or throat infection Heredity Rarely from spinal cord or brain tumor Sometimes cause unknown
Torticollis

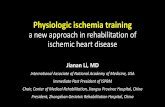
Signs and Symptoms Contraction of the SCM muscle
Head rotates toward one side and tilts toward the other
Other postural compensations Decreased range of motion, localized
tenderness
Torticollis

Torticollis

Treatment Physical therapy Extensive stretching May explore botulin toxin injections or surgery in
severe cases Parents performing home program is paramount Extensive stretching of the SCM, side tilting away from
the affected side, while rotating toward the affected side Massage Strengthening of opposing muscle groups
Torticollis

Description Also called Trisomy 21 Genetic disorder (not hereditary) Extra chromosome number 21 in each cell Arises during the formation of the a sex
cell Etiology
Inherited chromosome disorder
Down Syndrome

Down Syndrome
Signs and Symptoms Distinctive facial features Poor muscle tone,
leading to developmental delay
Cognitive delay Lowered immunity Prone to heart disease,
leukemia, Alzheimer’s disease, impaired mental function

Treatment No known cure Treat specific medical problems Folic acid supplements before and during
pregnancy Stimulate more normal muscle tone Strengthening Be aware of developmental dysplasia of the hip Family education in neurological and motor
development
Down Syndrome