Mus primhe
27
Medically unexplained Medically unexplained symptoms: how can symptoms: how can doctors help, doctors help, not hinder? not hinder? Christopher Dowrick Christopher Dowrick Professor of Primary Professor of Primary Medical Care Medical Care University of Liverpool University of Liverpool
-
Upload
henkpar -
Category
Health & Medicine
-
view
346 -
download
1
description
Transcript of Mus primhe

Medically unexplained Medically unexplained symptoms: how can doctors symptoms: how can doctors
help, help, not hinder?not hinder?
Christopher DowrickChristopher DowrickProfessor of Primary Medical Professor of Primary Medical
CareCareUniversity of LiverpoolUniversity of Liverpool

FrankFrank
stomach painstomach pain‘‘Oh no, it’s starting Oh no, it’s starting
again’again’ headacheheadache mole on armmole on arm throbbing legthrobbing leg

Kroenke et al Am J Med 1989

Persistence in primary carePersistence in primary care
19% MUS >3 months19% MUS >3 months Peveler et al, Peveler et al, J Psychosom Res J Psychosom Res 19971997
21% somatoform disorders persistent21% somatoform disorders persistent Jackson & Kroenke, Jackson & Kroenke, Psychosom Med Psychosom Med 20082008

Do doctors Do doctors help, or help, or hinder?hinder?

Mismatch of help seeking and careMismatch of help seeking and care
Liverpool Primary Care StudyLiverpool Primary Care Study Psychosocial agendas voicedPsychosocial agendas voiced
61% patients referred to emotional or social 61% patients referred to emotional or social problemsproblems
70% requested explanations for symptoms70% requested explanations for symptoms But often unheardBut often unheard
In 67% consultations, GPs indicated physical In 67% consultations, GPs indicated physical disease could be presentdisease could be present
In only 16% did GPs make empathic statementsIn only 16% did GPs make empathic statements
Ring et al, Ring et al, Soc Sci Med Soc Sci Med 20052005

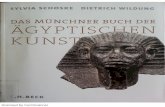
GPs more likely to propose GPs more likely to propose symptomatic management symptomatic management
0
10
20
30
40
50
60
70
Prescription Investigation Referral
DoctorsPatients
Z=12.19, P<0.001
%

Why this mismatch?Why this mismatch?
Examining the Examining the role of doctorsrole of doctors

DistancingDistancing
Somatic outcomes directly associated withSomatic outcomes directly associated with length of consultationlength of consultation
t 2.742, p 0.007t 2.742, p 0.007 patient elaborationpatient elaboration
t 1.990, p 0.047t 1.990, p 0.047 NB not associated with NB not associated with
Patients’ reference to physical diseasePatients’ reference to physical disease Patients’ proposal for somatic management Patients’ proposal for somatic management
Salmon et al, Salmon et al, Psychosom MedPsychosom Med 2007 2007

Attachment stylesAttachment styles
GP somatic interventions related toGP somatic interventions related to negative view of selfnegative view of self positive view of otherspositive view of others
i.e. more likely if GP values patient, values i.e. more likely if GP values patient, values somatic interventions, devalues own somatic interventions, devalues own psychological skills. psychological skills.
Salmon et al, Salmon et al, Gen Hosp Psych Gen Hosp Psych 20082008

How can doctors help?How can doctors help?
ReattributionReattribution Focus on Focus on
symptomssymptoms Expanding Expanding
explanationsexplanations Focus on Focus on
functionfunction

ReattributionReattribution
Three RCTsThree RCTs Effects small, limited to physical Effects small, limited to physical
symptoms symptoms Larisch et al, Larisch et al, J Psychosom ResJ Psychosom Res 2004 2004
Improved doctor-patient Improved doctor-patient communication, but not patient communication, but not patient outcomesoutcomes
Rosendal et al, Rosendal et al, Fam PractFam Pract 2005 2005 Morriss et al Morriss et al Br J PsychBr J Psych 2007 2007

ReattributionReattribution
Why limited effects?Why limited effects? Patients fear doctors will ignore their Patients fear doctors will ignore their
symptomssymptoms Peters et al, Peters et al, JGIMJGIM 2009 2009
Sympathetic GPs see many barriers to Sympathetic GPs see many barriers to implementationimplementation
Dowrick et al, Dowrick et al, BMC Fam Pract BMC Fam Pract 20082008

How can doctors help?How can doctors help?
ReattributionReattribution Focus on Focus on
symptomssymptoms Expanding Expanding
explanationsexplanations Focus on Focus on
functionfunction

Focus on symptomsFocus on symptoms
DiagnosticDiagnostic ICPC-2ICPC-2 Code by symptoms Code by symptoms
as reasons for encounter as reasons for encounter no aetiological attributionno aetiological attribution
ManagementManagement Symptom as primary focus Symptom as primary focus
Sharp M, Sharp M, Clin MedClin Med 2002 2002 Stepped care Stepped care
Kroenke K, Kroenke K, Int J Methods Psychiatry ResInt J Methods Psychiatry Res 2003 2003

Stepped Care 1 Stepped Care 1
Focused examinationFocused examination Address patient expectationsAddress patient expectations Symptom-specific treatmentsSymptom-specific treatments
analgesics, GI meds etcanalgesics, GI meds etc Watchful waitingWatchful waiting

Stepped Care 2 Stepped Care 2
Psychological screening Psychological screening Selected diagnostic testsSelected diagnostic tests Treatments:Treatments:
medicationmedication Kroenke et al, Kroenke et al, JAMAJAMA 2001 2001
psychosocialpsychosocial CBT in primary care?CBT in primary care?
Escobar et al, Escobar et al, Ann Fam Med Ann Fam Med 20072007 Arnold et al, Arnold et al, PsychosomaticsPsychosomatics 2008 2008

Stepped Care 3Stepped Care 3
Symptom care manager Symptom care manager
Referral to appropriate specialist Referral to appropriate specialist with interest in symptomswith interest in symptoms
Burton et al [in process]Burton et al [in process]

How can doctors help?How can doctors help?
ReattributionReattribution Focus on Focus on
symptomssymptoms Expanding Expanding
explanationsexplanations Focus on Focus on
functionfunction

Expanding explanationsExpanding explanations
Patients’ complex networks of meaningPatients’ complex networks of meaning Explanations valid within patients’ conceptual Explanations valid within patients’ conceptual
worldworld Dowrick et al, Dowrick et al, Br J Gen PractBr J Gen Pract 2004 2004
Need validation of bodily nature of suffering Need validation of bodily nature of suffering and and culturally basedculturally based explanations explanations
Kirmayer et al, Kirmayer et al, Can J PsychiatryCan J Psychiatry 2004 2004 Miresco et al, Miresco et al, Am J PsychiatryAm J Psychiatry 2006 2006 Dowrick, Dowrick, Beyond Depression Beyond Depression 20092009 Kovandzic et al, (submitted)Kovandzic et al, (submitted)

How can doctors help?How can doctors help?
ReattributionReattribution Focus on Focus on
symptomssymptoms Expanding Expanding
explanationsexplanations Focus on Focus on
functionfunction

Focus on functionFocus on function
[Not function of symptoms][Not function of symptoms]
Impairment or disability as a result of Impairment or disability as a result of symptomssymptoms ‘‘What does What does [x] [x] stop you doing?’stop you doing?’ ‘‘What can we do to overcome this?’ What can we do to overcome this?’
NB NB Functional Wellbeing ModelFunctional Wellbeing Model

Frank Frank
What do these What do these symptoms stop you symptoms stop you doing? doing?
‘‘taking my taking my grandson to school’grandson to school’
‘‘painting’painting’

Frank (the artist)Frank (the artist)

Final thoughtFinal thought
Just be there… Just be there…

Just be there… Just be there…
Somatic outcomes less likely if GPs’ Somatic outcomes less likely if GPs’ facilitate patients’ psychosocial talkfacilitate patients’ psychosocial talk
P=0.001P=0.001 not if GPs offer psychosocial explanationsnot if GPs offer psychosocial explanations
P=0.926P=0.926
‘‘simpler than we think, or fear’simpler than we think, or fear’
Salmon et al, Salmon et al, Psychosom MedPsychosom Med 20072007

Christopher DowrickChristopher Dowrick
Professor of Primary Medical CareProfessor of Primary Medical Care University of LiverpoolUniversity of Liverpool
[email protected]@liv.ac.uk