Multi Sensory Room
13
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
vimal-paul -
Category
Documents
-
view
247 -
download
5
Transcript of Multi Sensory Room
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Multi-sensory rooms: Comparing effects of the Snoezelen and theStimulus Preference environment on the behavior of adults withprofound mental retardation
Leonardo Fava a,b,*, Kristin Strauss c
a Department of Psychology, University of Rome ‘‘La Sapienza’’, Via dei Marsi 78, 00174 Rome, Italyb Fondazione Handicap: Dopodinoi-Onlus, Rome, Italyc University of Hamburg, Germany
A multi-sensory environment (MSE) is an environment designed to stimulate the senses through light, sound, touch andsmell. Essentially, it aims to create a feeling of safety, and to provide novel sensations, with stimulation under the user’scontrol. The MSE is both a physical space and a process. The physical space may assume a variety of different figure-groundrelationship forms or prototypes, each designed for a different set of purposes. Stimuli can be presented in isolation or incombination, intensified or reduced and shaped for passive or active interaction. Stimulation can therefore be planned to fitthe unstable sense ability requirements of an individual with debilitating perceptual difficulties and/or profound disabilities,whether these are progressive, fluctuating, stable or regressive (Pagliano, 1999). The MSE as a process becomes anindividualized behavior scaffold, specifically designed to match the user’s current motivation, interest, leisure, relaxation,therapeutic and/or educational needs (Pagliano, 2007). Although many multi-sensory gardens and pools exist (Kinross &Thomas, 2006; Lavie, Shapiro, & Julius, 2005), the most used MSE is the room, mostly located in centre or institutes for peoplewith intellectual disability.
Research in Developmental Disabilities 31 (2010) 160–171
A R T I C L E I N F O
Article history:
Received 10 August 2009
Accepted 24 August 2009
Keywords:
Snoezelen
Multi-sensory environment
Disruptive behaviors
Social behaviors
Profound mental retardation
Autism
A B S T R A C T
The present study examined whether Snoezelen and Stimulus Preference environments
have differential effects on disruptive and pro-social behaviors in adults with profound
mental retardation and autism. In N = 27 adults these target behaviors were recorded for a
total of 20 sessions using both multi-sensory rooms. Three comparison groups were
created by diagnosis and motor respective linguistic abilities. Each client was exposed to
only one multi-sensory room. Results showed that Snoezelen intervention decreased
disruptive behaviors only in individuals with autism, while Stimulus Preference increased
pro-social behaviors only in participants with profound mental retardation with co-
occurring poor motor and linguistic abilities.
Furthermore, several trend analyses of the improved behaviors were conducted
throughout all sessions toward short and mid term effects of the multi-sensory room
applications.
These findings support both the prudence of using the Snoezelen room in individuals
with developmental disabilities and the importance of using a Stimulus Preference
assessment in multi-sensory environments in clients with profound mental retardation.
� 2009 Elsevier Ltd. All rights reserved.
* Corresponding author. Tel.: +39 06 44335867; fax: +39 06 44325465.
E-mail addresses: [email protected], [email protected] (L. Fava).
Contents lists available at ScienceDirect
Research in Developmental Disabilities
0891-4222/$ – see front matter � 2009 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ridd.2009.08.006
Author's personal copy
Since the 1970s two therapists, Hulsegge and Verheul (1987), applied an approach called Snoezelen in the multi-sensoryrooms. Snoezelen is a combination of two Dutch words ‘‘snuffelen’’, meaning to seek out or explore, and ‘‘doezelen’’, whichmeans to relax.
The philosophy of Snoezelen is based on non-directive and non-threatening approaches; every implementation in theSnoezelen room should be based on relaxation; here is just, care, and free choice has to be encouraged. However, theappropriate decision regarding differential application of MSE affects the choice of contents, methods as well as forms oforganization which leads to ongoing discussions in this field (Hogg & Cavet, 1995).
Recently, the Snoezelen have been applied to people with developmental disabilities (Ashby, Broxholme, Pitcaithly, &Lindsay, 1995; Cuvo, May, & Post, 2001; Shapiro, Parush, Green, & Roth, 1997), to individuals with autism (Kaplan, Clopton,Kaplan, Messbauer, & McPherson, 2006; Mckee, Harris, Rice, & Silk, 2007), to children with brain injuries (Hotz et al., 2006) aswell as to people with chronic pain (Schofield, 2000).
Most of the aforementioned literature demonstrates a wide range of positive outcomes when Snoezelen versus non-Snoezelen environments are compared, though there is little evidence that these positive effects were carried over outsidethe Snoezelen environment, even following immediate post-Snoezelen evaluations (Ashby et al., 1995; Shapiro et al., 1997).
Moreover, other studies do yield entirely negative outcomes (Mckee et al., 2007). Mckee et al. used a strong experimentalABAB reversal design in which they evaluated ecologically targeted behaviors using inter-observer agreement amongdifferent raters. The results showed no decrease in disruptive behaviors and no increase of pro-social behaviors while thesubjects were in the Snoezelen compared to the baseline. These findings suggest that many methodological aspects shouldbe considered before claiming of any supposed significant effect of the multi-sensory rooms.
Indeed, many studies showed positive results of the Snoezelen intervention based only on qualitative data reported bycaregivers after the sessions, without previous definition of target behaviors (DeBunsen, 1994; Hagger & Hutchinson, 1991;Hope, 1998). Certainly, this research approach enhances the interdependence of these measures by subjective judgments.
Furthermore, in accordance with Lancioni, Cuvo, and O’Reilly (2002) an important aspect which has not been adequatelyconsidered concerns the fact that the relationship between caregivers and clients was not controlled both during the controlcondition and the Snoezelen session. The difference in terms of time spent together and the quality of this relation mightaffect the effectiveness of this multi-sensory treatment on people with profound mental retardation (Baker, Dowling,Wareing, Dawson, & Assey, 1997; van Lankveld, 1992). Another important aspect to be considered is the low number ofsubjects observed and the frequency of the Snoezelen sessions that were not sufficient to demonstrate any significant effectsof the Snoezelen treatment (Fagny, 1998; Holtkamp, Kerkstra, Ooms, van Campen, & Ribbe, 2001; Long & Haig, 1992).
Moreover, in various studies an individual preference assessment for the sensory stimuli in the Snoezelen sessions wasnot examined. This is a fundamental point to consider in order to allow the caregivers to expose the subjects towards thestimuli which create pleasure and are more coherent with their clinical condition. This approach could prevent or decreasesome challenging behaviors that occur while individuals are in the Snoezelen room (Ashby et al., 1995).
Recently, the necessity of performing a functional assessment of the challenging behaviors before any intervention wasdemonstrated (Ager & O’May, 2001).
Functional assessment refers to a variety of approaches used to gather information about the cause of problematicbehaviors to enable the design of effective treatments. It is vital to use stimuli that are highly preferred and functions asreinforcements if these interventions have to be effective. A systematic approach typically involves a Stimulus Preferenceassessment and a reinforcement assessment. A Stimulus Preference assessment attempts to set preference and predict thereinforcing effects of the stimuli while a reinforcement assessment tests the reinforcing effects of the same stimuli bymeasuring induced changes in the behavior’s rate (Fisher, Piazza, Hagopian, Bowman, & Toole, 1996).
Since it is well known that individuals with profound developmental disabilities rarely live within a single setting,therefore, interventions should be provided across settings and the stimuli assessed should be maintained and usedwithin multiple settings (Cannella, O’Really, & Lancioni, 2005; Matson, Bamburg, & Smalls, 2004). Stimuli identified inpreference assessments could be applied to a variety of different behaviors both in natural and in MSE in order to observethe extent of their reinforcing effects and to verify whether these effects change as response effort and complexityincrease.
With regard to the aforementioned points, in the current study we performed an analysis both in a naturalistic setting(living room) where the participants used to spend most of their time and in two different multi-sensory rooms. The firstroom, was inspired by the Snoezelen approach following the concept of non-directive and non-threatening approach. Thesecond one, called Stimulus Preference, a set of sensory stimuli, previously assessed as preferred by each individual, was usedas the main source of interaction between clients and caregivers.
Our experiment was aimed to investigate whether the Snoezelen environment and the Stimulus Preference environmenthave differential effects on disruptive behavior and pro-social behaviors of adults with profound mental retardation.Additionally, we examined whether any positive effects due to multi-sensory room exposures would continue in anecological environment (such as in the Institute’s living room) either after each session and/or at the end of the treatment.Any behavioral improvement in this naturalistic environment was the main purpose of our study.
Lastly, since Menditto (2002) demonstrated that person-centered planning treatment based on items and activitiespreferred by individuals with profound disabilities could increase social skills, starting from learning specific skills up totheir generalization into a more naturalistic environment. It was hypothesized that the Stimulus Preference room, allowingan increase of social and interactive behaviors, could be more effective than the Snoezelen room.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 161
Author's personal copy
1. Method
1.1. Settings
The study took place in three different settings at the participants’ residential Institute: the living room, the Snoezelenroom and the Stimulus Preference room.
The living room (5 m� 6 m), contained chairs, tables, a stereo, a television and two cabinets with leisure materials andmanipulative objects (e.g., puzzles, games, markers, and balls). Some of the objects in this environment were present also inboth multi-sensory rooms. Each participant had the possibility to interact freely with other patients and caregivers. Thisenvironment was considered by us as a place where the clients could improve their social behaviors either towards stimuli ortowards other patients and caregivers; this experience could result in reduction of the negative behaviors such as aggressiveand stereotyped behaviors.
The Snoezelen room (9 m� 7.50 m) had white walls, a carpeted floor, as well as commercially purchased visual, tactile,auditory, olfactory, and vestibular sensory equipment. It included a rocking chair, vibrating pillow, kaleidoscope-like colorwheel, rotating electric colored lights ball, magna light (lava lamp), color carousel ball with flashing lights, bubble column,bean bags, tactile panel with different texture tile, tactile books with textures, rotating projector (abstract shapes, planet,clouds, stars), rain stick, a fiber-optic, auditory melody disks, and aroma therapy oils. Most of the stimuli had interactive andfunctional features meaning that, for instance, some visual stimuli could start only after they had been touched by the client.Furthermore, the stimuli were distributed in the room without any specific rules and the client, supported by the caregiver,could interact in a free way and own timing with each of different stimuli. In this multi-sensory room, the concept ofavailability of sensory stimulation was encouraged in order to create a relaxing and safe atmosphere. The caregiversprovided the patients with various stimuli in different sensory modalities allowing the preference at the moment withoutany rules and structured steps to be followed in order to both create a sort of empathy with the patient and taking intoconsideration her/his needs at that precise moment.
The Stimulus Preference room is similar in size and general structure to the Snoezelen room but with some differences. Thedifferences reside in what the patients can do inside and in the relationship between them and their caregivers. The mainimportant difference was that the stimuli had already been selected by the patient in the preliminary preference assessmentusing a scientific preference assessment method which will be described in Section 1.5. In this room, the concept of sensoryreinforcement is emphasized and the patients can interact during this multi-sensory treatment exclusively with theirpreferred items. Moreover, the caregiver follows a more structured approach, using verbal and physical prompts with regardto the behaviors learned by each client toward both their preferred stimuli and toward themselves using the same stimuli asreinforcement. Consequently, in this multi-sensory room the environment was slightly different for each patient. Unlike theSnoezelen room, the stimuli were distributed regarding specific sensory modality. Each corner of the room was coupled onlywith stimuli performing to one sensory modality in order to allow a more specific interaction between caregiver and patient.
In addition, for each sensory modality, the client had a fixed timing to interact, roughly 5 min, which could have beenextended for another 2 min in case of an appropriate and active behavior with the stimuli. However, all four sensorymodalities (visual, tactile, olfactory and hearing) had to be covered during each session in this multi-sensory setting in orderto respect the purpose of re-sensitizing these individuals to different sensory functions
1.2. Participants
The participants were 27 adults in a Institute for individuals with intellectual disability. Their age ranged from 30 to 48years (MEAN 37.8 years). Everyone evinced profound mental retardation. Nine subjects had a diagnosis of autism. 18 out ofthe 27 subjects had good motor abilities, while nine had poor motor abilities. Nine clients had basic language abilities andtwelve had very poor language abilities. Thus, taking into account these variables, we divided the sample in three groups asfollows:
� Nine individuals with autism (AUT) with good motor abilities (Mw) and poor linguistic abilities (Lwo).� Nine individuals with profound mental retardation (PMRw) with good motor abilities (Mw) and good linguistic abilities
(Lw).� Nine individuals with profound and severe mental retardation (PMRwo) with poor motor abilities (Mwo) and poor
linguistic abilities (Lwo).
1.3. Target behaviors
In accordance with previous studies (Cuvo et al., 2001; Mckee et al., 2007), both disruptive and pro-social behaviors weretaken into account. Operational definitions of these behaviors were considered as dependent measures and are shown inTable 1. The caregivers were instructed to interact kindly with the individuals in order to facilitate the onset of any client’spro-social behaviors and to contain aggressive and stereotyped behaviors.
All target behaviors were scored using the records of the sessions, by three ‘‘blind’’ observers who did not know thepurpose of the experiment and were not familiar with the participants. The raters were two certified occupational therapists
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171162

Author's personal copy
and one behavioral psychologist. All target behaviors were scored indicating the frequency following the operationaldefinition shown in Table 1.
Inter-observer agreement by intra-class correlation coefficient was calculated in order to ensure that their level ofagreement remained above 80% for all of these measurements. For all target behaviors and all subjects a good reliability weredemonstrated as follows: for individuals with autism (AUT) was K = 0.86, for individuals with profound mental retardationand good motor and linguistic abilities (PMRw) was K = 0.87, and for individuals with profound mental retardation and poormotor and linguistic abilities (PMRwo) was K = 0.81.
1.4. Design
As shown in Table 2, the sample was divided into three groups (AUT; PMRwo; PMRw) and three conditions (living room;Snoezelen; Stimulus Preference). Each subject attended only one of the three experimental conditions, three times a week forseven weeks (20 sessions in total). Each session had the same length (25 min). In accordance with different activity levels andsensitiveness to the environment showed by most of the individuals with profound mental retardation during the day, wedistributed the sessions in three different times, as follows: sessions in the morning (9 a.m.), sessions at lunch time (12 a.m.),and sessions in the afternoon (4 p.m.).
Lastly, we controlled the relation between subjects and caregivers who were accompanying them in all sessions.Consequently, a permanent shift of operators was maintained in order to keep this variable constant, allowing a reduction ofother influences on the client’s behaviors besides the multi-sensory session effect.
1.5. Procedure
Target behaviors of individuals who attended either the Snoezelen or Stimulus Preference condition were recorded at fivedifferent times, while subjects belonging to the control group were measured only three times as follows:
Table 1
Target behavior definitions.
Target behavior Definition
Disruptive behaviors
Aggressive behaviors
Hitting Any attempted or completed striking of another person with any part of a client’s body.
Overturning furniture Any attempted or completed pushing over of chairs or tables.
Banging head Forceful contact of the head with a stationary object or forceful contact of the hand with the head or face.
Spitting Purposeful ejection of saliva from the mouth towards another person.
Threatening Verbal threat of aggression or a gesture of pointing and frowning at another person.
Stereotyped behaviors
Body rocking Moving the torso forwards then back to an upright position.
Body swaying Moving the torso right or left, then back to the midline position.
Picking Grasping an object between thumb and index finger, or dragging finger on surface until the finger was lifted.
Mouthing of hand or object A lick or placement of lips on hand or object (e.g., game pieces, clothing, strings, buttons, walls, chairs), or
placement of an object in mouth.
Vocal behaviors Repetitive yell operated without any specific require.
Pro-social behavior
Active behaviors toward sensorial stimuli
Glances Looking and making eye contact with any kind of stimuli for more than 3 s.
Smiles Looking and smiling at any kind of stimuli for more than 3 s.
Body and arm movements Any movements with meaningful approach towards sensory stimulation for more than 3 s.
Social behaviors toward caregiver
Approaching behaviors Any behavior considered as an interactive behavior with the caregiver such as movements of body and/or
vocal requirement in order to make a contact with the caregiver.
Request of social contact Any behavior who explicitly shows the need to be approached by the caregivers, such as shaking head
or doing anything to keep the attention of the caregiver.
Table 2
Experimental design.
Groups
AUT (Mw;Lwo) PMR (Mw;Lw) PMR (Mwo;Lwo)
Condition
Snoezelen 3 3 3
Stimulus Preference 3 3 3
Control (living room) 3 3 3
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 163
Author's personal copy
Baseline: measurement of all target behaviors for all subjects, obtained by medium value of three recorded sessions in theliving room before both multi-sensory room intervention began.Pre-session: measurement made just before both Snoezelen and Stimulus Preference sessions only for subjects whoattended one of these sessions (recorded in the living room).Dur-session: measurement made during the Snoezelen and Stimulus Preference sessions.Post-session: measurement made just after Snoezelen and Stimulus Preference sessions only for subjects who attendedone of these sessions (recorded in the living room).Baseline: measurement of all target behaviors for all subjects, obtained by medium value of three records in the livingroom after the end of both multi-sensory interventions.
All experimental conditions were recorded by two cameras. One was fixed and located in the corner of each roomcapturing the general view of the ambient. The other camera was mobile and moved by an experienced operator focusing onindividual features of the client’s behaviors while remaining outside from the visual field of the client.
Purposely, observations in the living room were conducted during regularly scheduled activity times under typicalconditions. The activities included watching television, listening to the stereo, looking at magazines, playing games, puttingtogether puzzles and interacting with various objects. The participants were allowed to engage freely in whatever activitythey chose during this time. Caregivers only occasionally attempted to engage individuals in activities. During the livingroom sessions roughly five clients and three caregivers were present and recorded.
Conversely, in the Snoezelen environment, participants attended each session individually. There was just one caregiverwho followed and kept non-directed contact with the client. The caregiver led the participants moving around theSnoezelen room in a counterclockwise manner during each session, while naming each stimulus and guiding theparticipant to activate or to use appropriately the equipment (e.g., manipulate the music instruments, turn on electricallyoperated stimuli). If the participant refused the manual guidance, the caregiver turned on the electrical equipment orplaced the sensory stimuli in a preferred place like on the table or on the mat. Regarding the non-directive approach, theparticipants were allowed to manipulate or look at whatever item for all the time they wanted. After all stimuli wereintroduced, the participants were free to move around the room and interact with the sensory equipment at their own pace.No interaction occurred between caregiver and participant unless requested by the participants or if they attempted to usethe equipment inappropriately. In the case that the participants did not engage with any of the Snoezelen equipment formore than 4 min, the caregiver was supposed to interact with the clients and offer them either to play with or to look at anysensory stimuli in the room.
Similar to the Snoezelen room, in the Stimulus Preferences several sensory stimuli were present and the participantsattended each session individually. However, as mentioned before, differing from the Snoezelen room, the StimulusPreference room was always adapted to individual choice in terms of the client’s most favorite stimuli. The preferred stimuliwere firstly listed by the caregiver for each participant, and then to these pre-selected items, a scientific preferenceassessment methodology was applied as follows.
We referred to a multiple stimulus assessment with replacement (MSW; Windsor, Piche, & Locke, 1994) where anassortment of items are presented at the same time, allowing the individual to choose one item from the array and involvingthe ability to replace an item after it had been chosen so that all items are present for each trial.
Additionally, we considered also the second version of this method introduced by DeLeon and Iwata (1996), calledmultiple stimulus assessment without replacement (MSWO) where an array of items is presented simultaneously as in theMSW assessment.
Conversely, after an item is chosen it is removed from the group and the individual chooses another item. This continuesuntil all items are selected or the individual no longer selects an item. Thus, this method without replacement requires theindividual to discriminate between stimuli, which may yield more differential responding and may give a more sensitivemeasure of preference than one with replacement.
These features are comparable with the Paired Stimulus presentation (Ivancic, 2000), where stimuli are presented in pairsand the individual has to choose one. This method seems to be the most accurate one for assessing preferred stimuli andpredicting reinforcement effectiveness. However, Carr, Nicolson, and Higbee (2000) suggested to use the Multiple Stimulusassessments in people with profound mental retardation, since it is efficient while consuming less time than the PairedStimulus assessment and is very accurate to identify preferred stimuli, at the same time.
Therefore, we decided to use a combination of MSW and MSWO, applying the preference assessment only to participantswho attended the Stimulus Preference Condition; each participant was placed in front of some objects of different sensorymodalities. This record was repeated few times and a selection percentage was calculated by dividing the number of times anitem was chosen by the number of trials it was available. These percentages were then used to rank-order the items bypreference and each preferred stimulus was put in a ‘‘Sensory Category’’, which were subsequently used by the caregivers inthe Stimulus Preference room, for motivating the subject’s to interact with stimuli in different sensory modalities.
For assessing the preference assessment each client was submitted to four experimental sessions, two with Replacement(MSW) and two without Replacement (MSWO). Nonetheless, in accordance with Zhou, Iwata, Goff, and Shore (2001), whoargued that it is necessary to repeat a preference assessment during long experiments with people with mental retardationsince the individual preferences can vary across time and situation, we repeated these four experimental sessions after tensessions, when half of the experimental trials were already performed.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171164
Author's personal copy
Furthermore, the caregiver led the participant going around the Stimulus Preference room focusing his/her attention tointeract with his/her preferred stimuli. The caregiver promoted during all sessions in this environment, the similar kind ofinteraction with their preferred stimuli, correcting only if they used the equipment inappropriately. In the case thatparticipants did not engage with any of the stimuli preferred for more than 2 min, the caregiver asked if they wanted either toplay with or look at something else in the room. Those changes were recorded by the caregiver in order to take note of apossibility that the patient could have changed their preference. For three patients some preferred stimuli were changedover the treatment.
2. Results
Firstly, we computed medium frequencies value for all target behaviors for each experimental group in the living room,creating either Baseline pre- and post-treatment, in order to compare the groups who attended multi-sensory conditionswith the control group.
Variance analysis were conducted for each group using pairwise comparisons and univariate tests focused on conditionand pathology as parameters both for disruptive and pro-social behaviors.
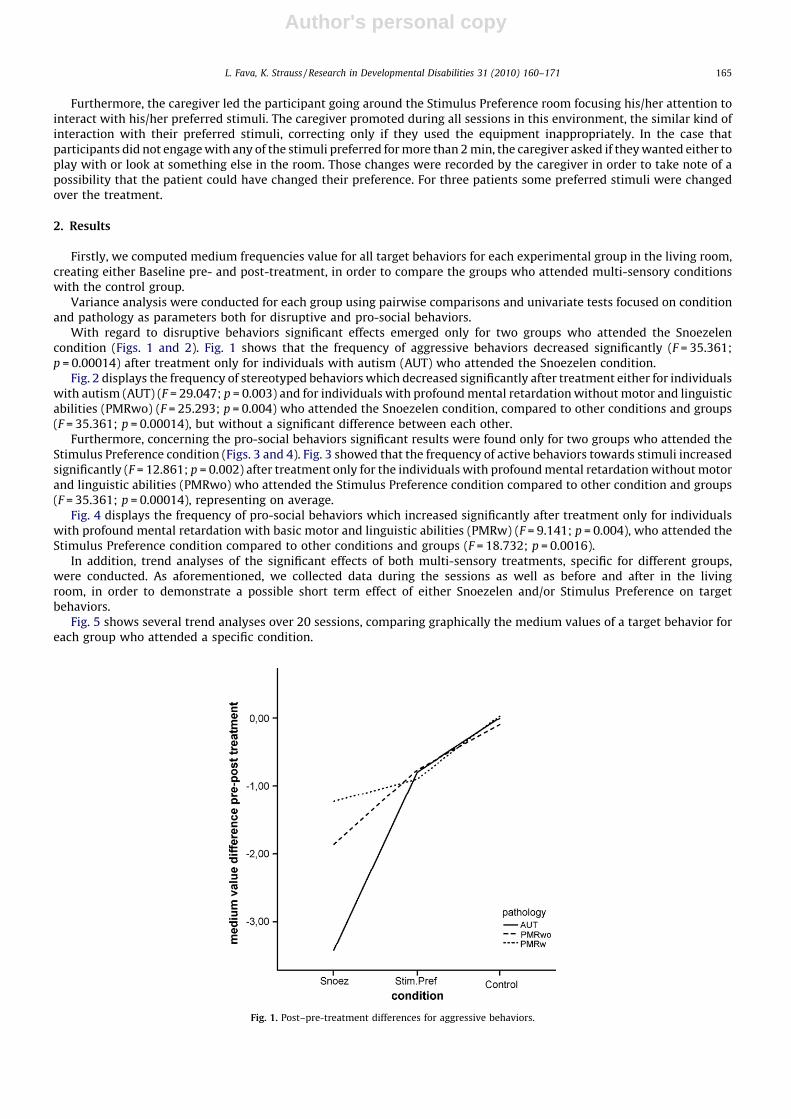
With regard to disruptive behaviors significant effects emerged only for two groups who attended the Snoezelencondition (Figs. 1 and 2). Fig. 1 shows that the frequency of aggressive behaviors decreased significantly (F = 35.361;p = 0.00014) after treatment only for individuals with autism (AUT) who attended the Snoezelen condition.
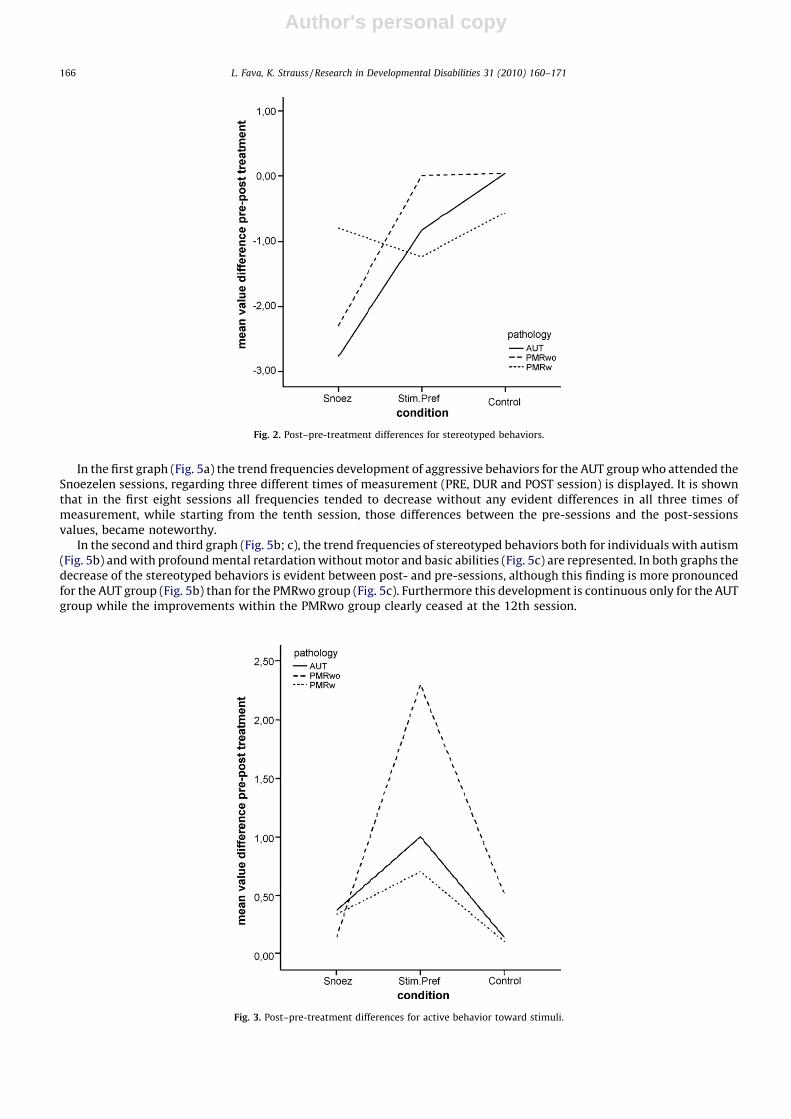
Fig. 2 displays the frequency of stereotyped behaviors which decreased significantly after treatment either for individualswith autism (AUT) (F = 29.047; p = 0.003) and for individuals with profound mental retardation without motor and linguisticabilities (PMRwo) (F = 25.293; p = 0.004) who attended the Snoezelen condition, compared to other conditions and groups(F = 35.361; p = 0.00014), but without a significant difference between each other.
Furthermore, concerning the pro-social behaviors significant results were found only for two groups who attended theStimulus Preference condition (Figs. 3 and 4). Fig. 3 showed that the frequency of active behaviors towards stimuli increasedsignificantly (F = 12.861; p = 0.002) after treatment only for the individuals with profound mental retardation without motorand linguistic abilities (PMRwo) who attended the Stimulus Preference condition compared to other condition and groups(F = 35.361; p = 0.00014), representing on average.
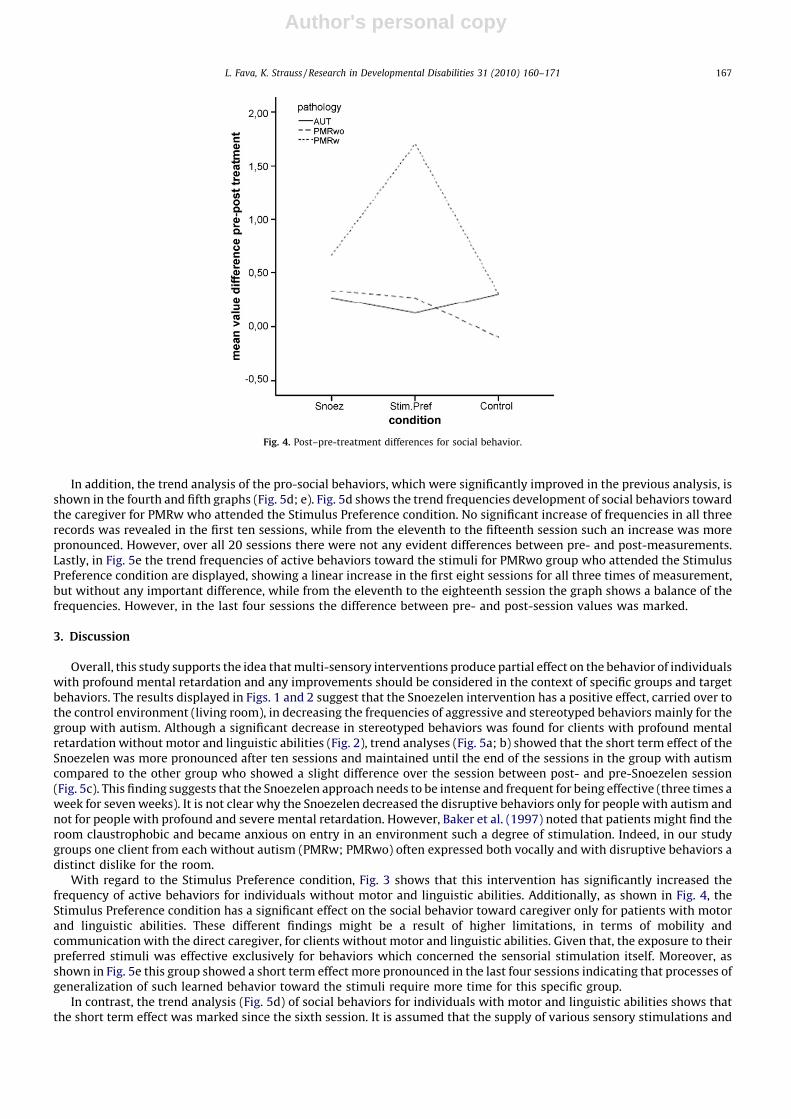
Fig. 4 displays the frequency of pro-social behaviors which increased significantly after treatment only for individualswith profound mental retardation with basic motor and linguistic abilities (PMRw) (F = 9.141; p = 0.004), who attended theStimulus Preference condition compared to other conditions and groups (F = 18.732; p = 0.0016).
In addition, trend analyses of the significant effects of both multi-sensory treatments, specific for different groups,were conducted. As aforementioned, we collected data during the sessions as well as before and after in the livingroom, in order to demonstrate a possible short term effect of either Snoezelen and/or Stimulus Preference on targetbehaviors.
Fig. 5 shows several trend analyses over 20 sessions, comparing graphically the medium values of a target behavior foreach group who attended a specific condition.
Fig. 1. Post–pre-treatment differences for aggressive behaviors.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 165
Author's personal copy
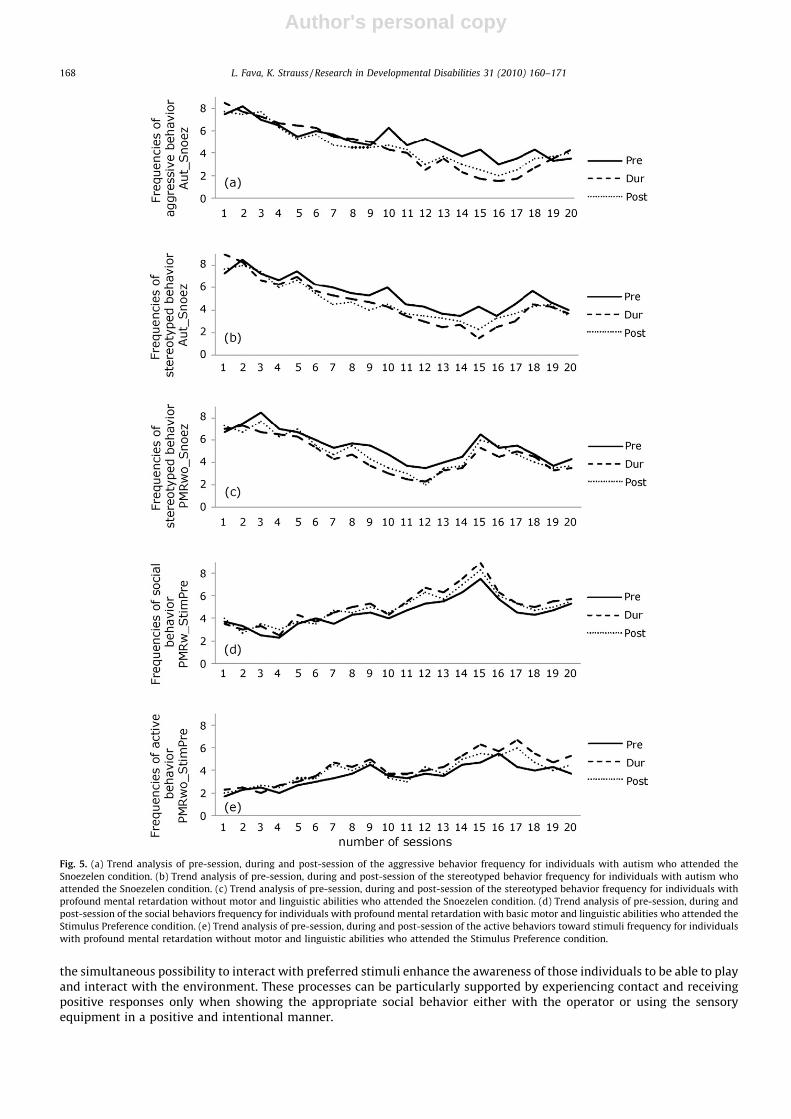
In the first graph (Fig. 5a) the trend frequencies development of aggressive behaviors for the AUT group who attended theSnoezelen sessions, regarding three different times of measurement (PRE, DUR and POST session) is displayed. It is shownthat in the first eight sessions all frequencies tended to decrease without any evident differences in all three times ofmeasurement, while starting from the tenth session, those differences between the pre-sessions and the post-sessionsvalues, became noteworthy.
In the second and third graph (Fig. 5b; c), the trend frequencies of stereotyped behaviors both for individuals with autism(Fig. 5b) and with profound mental retardation without motor and basic abilities (Fig. 5c) are represented. In both graphs thedecrease of the stereotyped behaviors is evident between post- and pre-sessions, although this finding is more pronouncedfor the AUT group (Fig. 5b) than for the PMRwo group (Fig. 5c). Furthermore this development is continuous only for the AUTgroup while the improvements within the PMRwo group clearly ceased at the 12th session.
Fig. 2. Post–pre-treatment differences for stereotyped behaviors.
Fig. 3. Post–pre-treatment differences for active behavior toward stimuli.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171166
Author's personal copy
In addition, the trend analysis of the pro-social behaviors, which were significantly improved in the previous analysis, isshown in the fourth and fifth graphs (Fig. 5d; e). Fig. 5d shows the trend frequencies development of social behaviors towardthe caregiver for PMRw who attended the Stimulus Preference condition. No significant increase of frequencies in all threerecords was revealed in the first ten sessions, while from the eleventh to the fifteenth session such an increase was morepronounced. However, over all 20 sessions there were not any evident differences between pre- and post-measurements.Lastly, in Fig. 5e the trend frequencies of active behaviors toward the stimuli for PMRwo group who attended the StimulusPreference condition are displayed, showing a linear increase in the first eight sessions for all three times of measurement,but without any important difference, while from the eleventh to the eighteenth session the graph shows a balance of thefrequencies. However, in the last four sessions the difference between pre- and post-session values was marked.
3. Discussion
Overall, this study supports the idea that multi-sensory interventions produce partial effect on the behavior of individualswith profound mental retardation and any improvements should be considered in the context of specific groups and targetbehaviors. The results displayed in Figs. 1 and 2 suggest that the Snoezelen intervention has a positive effect, carried over tothe control environment (living room), in decreasing the frequencies of aggressive and stereotyped behaviors mainly for thegroup with autism. Although a significant decrease in stereotyped behaviors was found for clients with profound mentalretardation without motor and linguistic abilities (Fig. 2), trend analyses (Fig. 5a; b) showed that the short term effect of theSnoezelen was more pronounced after ten sessions and maintained until the end of the sessions in the group with autismcompared to the other group who showed a slight difference over the session between post- and pre-Snoezelen session(Fig. 5c). This finding suggests that the Snoezelen approach needs to be intense and frequent for being effective (three times aweek for seven weeks). It is not clear why the Snoezelen decreased the disruptive behaviors only for people with autism andnot for people with profound and severe mental retardation. However, Baker et al. (1997) noted that patients might find theroom claustrophobic and became anxious on entry in an environment such a degree of stimulation. Indeed, in our studygroups one client from each without autism (PMRw; PMRwo) often expressed both vocally and with disruptive behaviors adistinct dislike for the room.
With regard to the Stimulus Preference condition, Fig. 3 shows that this intervention has significantly increased thefrequency of active behaviors for individuals without motor and linguistic abilities. Additionally, as shown in Fig. 4, theStimulus Preference condition has a significant effect on the social behavior toward caregiver only for patients with motorand linguistic abilities. These different findings might be a result of higher limitations, in terms of mobility andcommunication with the direct caregiver, for clients without motor and linguistic abilities. Given that, the exposure to theirpreferred stimuli was effective exclusively for behaviors which concerned the sensorial stimulation itself. Moreover, asshown in Fig. 5e this group showed a short term effect more pronounced in the last four sessions indicating that processes ofgeneralization of such learned behavior toward the stimuli require more time for this specific group.
In contrast, the trend analysis (Fig. 5d) of social behaviors for individuals with motor and linguistic abilities shows thatthe short term effect was marked since the sixth session. It is assumed that the supply of various sensory stimulations and
Fig. 4. Post–pre-treatment differences for social behavior.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 167
Author's personal copy
the simultaneous possibility to interact with preferred stimuli enhance the awareness of those individuals to be able to playand interact with the environment. These processes can be particularly supported by experiencing contact and receivingpositive responses only when showing the appropriate social behavior either with the operator or using the sensoryequipment in a positive and intentional manner.
Fig. 5. (a) Trend analysis of pre-session, during and post-session of the aggressive behavior frequency for individuals with autism who attended the
Snoezelen condition. (b) Trend analysis of pre-session, during and post-session of the stereotyped behavior frequency for individuals with autism who
attended the Snoezelen condition. (c) Trend analysis of pre-session, during and post-session of the stereotyped behavior frequency for individuals with
profound mental retardation without motor and linguistic abilities who attended the Snoezelen condition. (d) Trend analysis of pre-session, during and
post-session of the social behaviors frequency for individuals with profound mental retardation with basic motor and linguistic abilities who attended the
Stimulus Preference condition. (e) Trend analysis of pre-session, during and post-session of the active behaviors toward stimuli frequency for individuals
with profound mental retardation without motor and linguistic abilities who attended the Stimulus Preference condition.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171168

Author's personal copy
A possible explanation for lacking improvements of individuals with autism in social behaviors might be that this groupwas frustrated in being exposed only to stimuli carried by the caregiver through the room, following a specific sequence witha fixed order of interaction. It was evident that this frustration was the result of being not completely free to choose at whichmoment and with which frequency to interact with specific stimuli.
To sum up, the Snoezelen approach was effective on disruptive behaviors of individual with profound mental retardationand autism, while the Stimulus Preference approach was specifically effective only for clients with profound mentalretardation without autism. Since significant effects emerged only on single positive behavior such as glances towardsstimuli and approaching behaviors, we may conclude that the exclusive use of preferred stimuli in the MSE allowsimprovements of such pro-social behaviors only for a specific group. In other words, the preferred stimulus assessment wasapplied in MSE based on the assumption that knowing one’s preferences is important for developing social skills, withoutprecluding to provide opportunities for choice (Cannella et al., 2005).
4. Limitations
Although we addressed in this current study several methodological shortcomings from previous studies, there arelimitations left to be considered. First, our work has to be seen as observational study where variables interfere and are notthorough controlled. For instance, individuals with profound mental retardation occasionally show problem behaviors whenentering the multi-sensory room. In accordance with Mckee et al. (2007), the sessions were following the time schedules ofthe Institute. This could have had the unexpected effect of reinforcing patients’ negative behaviors. Furthermore, the fact thatthe room was available only at certain times could have caused frustration to the clients, decreasing the potential effect offollowing multi-sensory interventions.
Another critical point in our study is the lacking examination of quality and amount of language expressed by the clientsduring the multi-sensory room sessions. Although, we addressed this point by dividing the group regarding their languageskills, we did not collect data on this ability. As verified in certain experiments (Baker et al., 1997; van Weert, van Dulmen,Spreeuwenberg, Ribbe, & Bensing, 2005) this ability should be considered when applying the multi-sensory interventions.Indeed has emerged that some patients’ normal speech content and simple sentence structure were highly repetitive andcontinuous, and that communication was solely inducted by the insistence of the caregiver. Instead within the Snoezelensession, patients started to initiate a two-way interaction conversation about the various attributes of the room, meaningthat these multi-sensory environments evoked enough interest to divert clients from usual speech patterns.
Lastly, medications may have affected individuals in the study by reducing disruptive behaviors and increasing activebehaviors confounding the effectiveness of both multi-sensory interventions.
5. Conclusion
The current study emphasized the need to use an experimental evaluation in order to avoid false positives in reporting theeffect of multi-sensory interventions. It was demonstrated that the effect of the Snoezelen is significant only for individualsin certain target behaviors. Moreover, the importance of applying a Stimulus Preference assessment in the multi-sensoryroom was verified. Individuals with profound mental retardation are often exposed to a various amount of stimulations thatthey are not able to select and consequently interact with due to limited cognitive skill. For this reason, we believe that apossible strategy to introduce our clients into the real world would be to start from simple interactions with stimuli andother individuals and to stimulate their-self to be interactive with the environment around. These effects provided by theStimulus Preference condition might be linked specifically to the role of an individual’s preference stimuli included in thisMSE.
In addition, referring to our finding in the living room, social validity studies may also be conducted to determine howpreference assessments can be modified to make their use more likely in applied settings. This social application isrepresented in our research by the fact that we measured these target behaviors in the multi-sensory rooms but essentiallyconcentrated more attention on the disruptive and pro-social behaviors showed during the sessions recorded in the livingroom. This room represents, for the Institute’s residents, the most important living setting to spend time during the day andto interact with other people. The multi-sensory room interventions enable caregivers to create situations, where clientscan experience with all senses that could hardly be realized otherwise. In accord to Chan, Fung, Tong, and Thompson (2005)we believe that the multi-sensory environment prompts sensorial and emotional exploration by the persons through theconstructed intervention. The atmosphere and the equipment of a multi-sensory intervention can have an activating effectwhich invites the participants to spontaneously explore the space around and seek for such stimulation. Martin, Gaffan, andWilliams (1998) further suggested that the critical components of a ‘therapeutic’ multi-sensory intervention may berelated to the nature of the interactions within the therapy. If the ward environment could contain key therapeuticvariables in the multi-sensory therapy such as constant environment, increased physical contact, increased tolerance tophysical contact as well as overall compliance relaxation and freedom from demands might help to reduce clients’ problembehavior.
In addition, according with Singh et al. (2004) the maladaptive behaviors showed by individuals with severe andprofound mental retardation such as aggression, self-injury and stereotypy, can constitute avoidance behaviors because theyreduce escaping demands. Given this, maladaptive behavior might be expected to occur at lower levels during the Snoezelen
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 169

Author's personal copy
condition than in the skills training conditions; such as the Stimulus Preference condition of our study, where learningdemands are essential.
It could be useful to understand the functional timing to administer these multi-sensory interventions. It would beinteresting for the same purpose, to analyze and verify the same target behaviors after longer periods; for instance 2 monthslater, in order to establish the time when this intervention should be repeated in order to maintain the improvementsacquired by the patients. Certainly, it will be important to maintain a low level of frequencies and intensity of disruptivebehaviors and a relatively high level of positive behaviors in order to increase the quality of life for our clients and for theircaregivers.
Still, in accordance with Cannella et al. (2005) it will be important to determine treatment fidelity over an extendedperiod of time as well as administrators’ perceptions of the costs and benefits of assessments and interventions which isconsidered an issue for this multi-sensory application due to relative high cost of implementation both in terms of humanresources and in equipment.
Future studies should take into consideration to compare Snoezelen and Stimulus Preferences interventions to otherempirically validated treatments, such as Differential Reinforcement of Other (DRO) or with Non-Contingent Reinforcement(NCR; Britton, Carr, Kellum, Dozier, & Weil, 2000). Furthermore, a careful analysis of the function that behaviors have for theclient leads naturally to a highly specific individualized treatment plan, and a functional analysis is considered part of bestpractice for developing effective interventions for problematic behaviors (McCord & Neef, 2005).
Lastly, it would be useful to combine these multi-sensory therapies with a pharmacological therapy, especially withpeople with psychiatric disorders, evaluating the single and the combined effect of both therapies in order to figure out anypossible therapeutic strategy for improving the behaviors of these target populations.
Although with some limitations, this study has provided an original evaluation in examining and in verifying the effect ofslightly different multi-sensory environments on the behaviors of people with profound mental retardation; taking intoaccount the essential concept of stimulating autonomy, active sensory seeking and social interaction for individuals who aresupported in this way, to make their own choice and to find their own answers.
Acknowledgements
The authors would like to thank Prof. Marta Olivetti Belardinelli, Prof. Giulio Lancioni and Dr. Joe Hettinger for theircomments on earlier versions. Dr. Fabrizio Giorgeschi is also acknowledged for his help in collecting data.
References
Ager, A., & O’May, F. (2001). Issues in the definition and implementation of ‘‘best practice’’ for staff delivery of interventions for challenging behaviour. Journal ofIntellectual & Developmental Disability, 26, 243–256.
Ashby, M., Broxholme, S., Pitcaithly, D., & Lindsay, W. R. (1995). Snoezelen: Its effects on concentration and responsiveness in people with profound multiplehandicaps. British Journal of Occupational Therapy, 58, 303–307.
Baker, R., Dowling, Z., Wareing, L. A., Dawson, J., & Assey, J. (1997). Snoezelen: Its long-term and short-term effects on older people with dementia. British Journal ofOccupational Therapy, 60, 213–218.
Britton, L. N., Carr, J. E., Kellum, K. K., Dozier, C. L., & Weil, T. M. (2000). A variation of noncontingent reinforcement in the treatment of aberrant behavior. Researchin Developmental Disabilities, 21, 425–435.
Cannella, H. I., O’Really, M. F., & Lancioni, G. E. (2005). Choice and preference assessment research with people with severe to profound developmental disabilities:A review of the literature. Research in Developmental Disabilities, 26, 1–15.
Carr, J. E., Nicolson, A. C., & Higbee, T. S. (2000). Evaluation of a brief multiple-stimulus preference assessment in a naturalistic context. Journal of Applied BehaviorAnalysis, 33, 353–357.
Chan, S., Fung, M. Y., Tong, C. W., & Thompson, D. (2005). The clinical effectiveness of a multi-sensory therapy on clients with developmental disability. Research inDevelopmental Disabilities, 26, 131–142.
Cuvo, A. J., May, M. E., & Post, T. M. (2001). Effects of living room, Snoezelen room, and outdoor activities on stereotypic behavior and engagement by adults withprofound mental retardation. Research in Developmental Disabilities, 22, 183–204.
DeBunsen, A. (1994). A study in the implication of the Snoezelen resources at Limington House School, Sensations & Disability: Sensory environments for leisure,Snoezelen, Education & Therapy. Chesterfield: ROMPA. (pp. 138–162).
DeLeon, I. G., & Iwata, B. A. (1996). Evaluation of a multiple-stimulus presentation format for assessing reinforcer preferences. Journal of Applied Behavior Analysis,29, 519–533.
Fagny, M. (1998). Etude de l’influence de la technique du ‘‘snoezelen’’ sur les comportements d’adultes autiste profond en institution. Brussels: Universite Libre deBruxelles.
Fisher, W. W., Piazza, C. C., Hagopian, L. P., Bowman, L. G., & Toole, L. (1996). Using a choice assessment to predict reinforcer effectiveness. Journal of AppliedBehavior Analysis, 29, 1–9.
Hagger, L. E., & Hutchinson, R. B. (1991). Snoezelen: An approach to the provision of a leisure resource for people with profound and multiple handicaps. MentalHandicap, 19, 51–55.
Hogg, J., & Cavet, J. (1995). Making leisure provision for people with profound and multiple learning disabilities. London: Chapman & Hall.Holtkamp, C. C. M., Kerkstra, A., Ooms, M. E., van Campen, C., & Ribbe, M. W. (2001). Effects of the implementation of the Resident Assessment Instrument on gaps
between perceived needs and nursing care supply for nursing home residents in the Netherlands. International Journal of Nursing Studies, 38, 619–628.Hope, K. W. (1998). The effect of multi-sensory environments on older people with dementia. Journal of Psychiatric and Mental Health Nursing, 5, 377–385.Hotz, G. A., Castelblanco, A., Lara, I. M., Weiss, I. D., Duncan, R., & Kuluz, J. W. (2006). Snoezelen: A controlled multisensory stimulation therapy for children
recovering from severe brain injury. Brain Injury, 20, 879–888.Hulsegge, J., & Verheul, A. (1987). Snoezelen, another world. Chesterfield: Rompa.Ivancic, M. T. (2000). Stimulus preference and reinforcer assessment application. In J. Austin & J. E. Carr (Eds.), Handbook of Applied Behavior Analysis (pp. 19–38).
Reno, NV: Context Press.Kaplan, H., Clopton, M., Kaplan, M. L., Messbauer, L., & McPherson, K. (2006). Snoezelen multi-sensory environments: Task engagement and generalization.
Research in Developmental Disability, 27, 443–455.Kinross, L., & Thomas, L. (2006). Bloorview kids rehab takes multi-sensory stimulation to a whole new level. Exceptional Family, 2, 11–14.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171170

Author's personal copy
Lancioni, G. E., Cuvo, A. J., & O’Reilly, M. F. (2002). Snoezelen: An overview of research with people with developmental disabilities and dementia. Disability andRehabilitation, 24, 175–184.
Lavie, E., Shapiro, M., & Julius, M. (2005). Hydrotherapy combined with Snoezelen multi sensory therapy. International Journal Adolescence Medical Health, 17, 83–87.
Long, A.-P., & Haig, L. (1992). How do clients benefit from Snoezelen? An exploratory study. British Journal of Occupational Therapy, 55, 103–106.Martin, N. T., Gaffan, E. A., & Williams, T. (1998). Behavioural effects of long-term multi-sensory stimulation. British Journal of Clinical Psychology, 37, 69–82.Matson, J. L., Bamburg, J. W., & Smalls, Y. (2004). An analysis of Snoezelen equipment to reinforce persons with severe of profound mental retardation. Research in
Developmental Disabilities, 25, 89–95.McCord, B. E., & Neef, N. A. (2005). Leisure items as controls in the attention condition of functional analyses. Journal of Applied Behavior Analysis, 38, 417–426.Mckee, S. A., Harris, G. T., Rice, M. E., & Silk, L. (2007). Effects of a Snoezelen room on the behaviour of three autistic clients. Research in Developmental Disabilities, 28,
304–316.Menditto, A. A. (2002). A social-learning approach to the rehabilitation of individuals with severe mental disorders who reside in forensic facilities. Psychiatric
Rehabilitation Skills, 6, 73–93.Pagliano, P. J. (1999). Multisensory environments. London: David Fulton.Pagliano, P. J. (2007). Multisensory environment and their use in education with children with profound multiple disabilities. Paper presented at the 2nd Come to
your senses. Toronto: Mukibaum.Schofield, P. (2000). The effects of Snoezelen on chronic pain. Nursing Standard, 15, 33–34.Shapiro, M., Parush, S., Green, M., & Roth, D. (1997). The efficacy of the ‘Snoezelen’ in the management of children with mental retardation who exhibit
maladaptive behaviours. British Journal of Developmental Disabilities, 43, 140–155.Singh, N. N., Lancioni, G. E., Winton, A. S. W., Molina, E. J., Sage, M., Brown, S., et al. (2004). Effects of Snoezelen room, activities of daily living skills training, and
vocational skills training on aggression and self-injury by adults with mental retardation and mental illness. Research in Developmental Disabilities, 25, 285–293.
van Lankveld, J. D. M. (1992). Gedragsveranderingen Bij Zwakzinnegen Tijdens Snoezelen. Nederlands Tijdschrift voor Zwakzinnigenzorg, 1, 34–48.van Weert, J. C., van Dulmen, A. M., Spreeuwenberg, P. M. M., Ribbe, M. W., & Bensing, J. B. (2005). Behavioral and mood effects of Snoezelen integrated into 24-h
dementia care. Journal of the American Geriatrics Society, 53, 24–33.Windsor, J., Piche, L. M., & Locke, P. A. (1994). Preference testing: A comparison of two presentation methods. Research in Developmental Disabilities, 15, 439–455.Zhou, L., Iwata, B. A., Goff, G. A., & Shore, B. A. (2001). Longitudinal analysis of leisure-item preferences. Journal of Applied Behavior Analysis, 34, 179–184.
L. Fava, K. Strauss / Research in Developmental Disabilities 31 (2010) 160–171 171











![G ARTICLE IN PRESS - Snoezelen Multi-Sensory Environments...multi-sensory therapy is beneficial for people with sensory and learning disabilities [9]. Moffat et al. revealed positive](https://static.fdocuments.us/doc/165x107/5fe8d0c61e886b29082f1769/g-article-in-press-snoezelen-multi-sensory-environments-multi-sensory-therapy.jpg)