Multi-drug resistant Acinetobacter
46
Multi-drug resistant Acinetobacter (MDRA) Surveillance and Control Alison Holmes
Transcript of Multi-drug resistant Acinetobacter
Multi-drug resistant Acinetobacter (MDRA) Surveillance and Control
Alison Holmes
• The organism and it’s
epidemiology
• Surveillance
• Control
What is it?
What is it?
What is it?
What is it?
Acinetobacter : The organism
• Aerobic, Gram-negative bacterium, non motile, non fermenting,
coccobacillus in stationary phase, rod shaped in rapid growth, forms
biofilms and survives environmental dessication for weeks.
• Began to be recognised in 1970s as an opportunistic hospital
pathogen, causing outbreaks
• A. baumanii >80% infections
• Infections in ICUs, ventilated patients, burns units
•Pneumonia
•Bacteraemia
•Osteomyelitis (trauma/deep wound infection)
• Can cause fatal infections in debilitated patients
•Historically, a pathogen of humid climates.
• Since the 1970s, an increasingly common nosocomial problem in
temperate climates- where seasonal variation seen
•Years before a concern in ICUs in the US, it was cited as the cause of 17
% of cases of VAP in a Guatemalan ICU
•Most common cause of Nosocomial pneumonia in tertiary care hospitals
in Thailand (Werarak P et al Feb 2012)
•Ability to accumulate diverse mechanisms of resistance and emergence
of highly resistant strains
•Dramatic clonal outbreaks of MDRA have
occurred across the world, some involving
multiple hospitals
Multiple mechanisms of antibiotic resistance
• Constitutive or acquired via plasmids, integrons, and transposons.
• Methods include:
1.enzymatic inactivation of antibiotic
2.modification of antibiotic target sites,
3.expression of efflux pumps or down regulation porin
channel expression.
• Resistance to β-lactams primarily caused by β-lactamase production, including
extended spectrum β-lactamases, metallo- β-lactamases and most commonly,
oxacillinases (OXA)…which have carbapenemase activity
• Antibiotic target site alterations confer resistance to fluoroquinolones (gyrA,
parC) and aminoglycosides (arm, rmt), and to a much lesser extent, β-lactams.
• Efflux pumps contribute to resistance against β-lactams, tetracyclines,
fluoroquinolones, and aminoglycosides.
• Porin channel deletion contribute to β-lactam resistance and may contribute to
rarely seen polymyxin resistance.
• In UK - prior to 2000, virtually all A. baumannii isolates were
susceptible to carbapenems and very few genotypes
appeared to occur in multiple hospitals. These patterns
changed with the multicentric isolation of the SE clone, with its
variable resistance to imipenem and meropenem.
• The spread of two OXA-23-producing clones represent a
further ratcheting of the problem, being more consistently
resistant to carbapenems
• Emergence of A. baumanii related in part to survival ability
and rapid development of resistance to all major antibiotic
classes
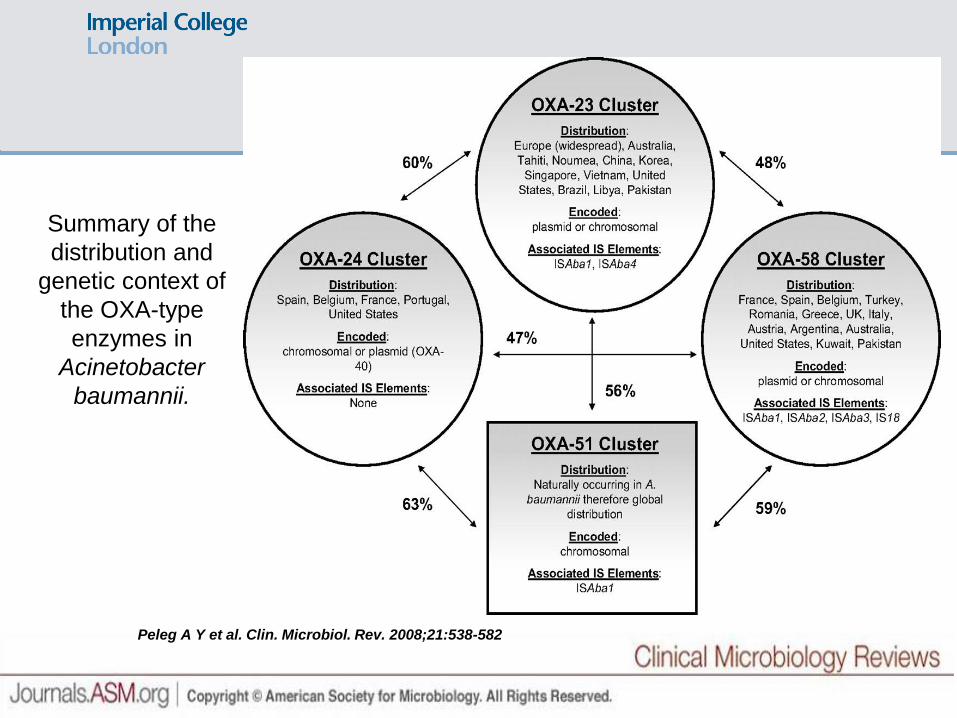
Summary of the
distribution and
genetic context of
the OXA-type
enzymes in
Acinetobacter
baumannii.
Peleg A Y et al. Clin. Microbiol. Rev. 2008;21:538-582
Common misconceptions…
• ‘ubiquitous in nature’
• ‘recovered easily from soil,
water, animals’
• ‘frequent skin* and oro-
pharyngeal coloniser’*
This may apply to other members of the genus Acinetobacter ..
But not A. baumanii (and its close relatives of clinical importance)
*But the in tropics situation e.g. HK 53 % medical students hands carried A.
baumanni in summer. Chu Y W et al ‘99 J Clin Micro 37,
Factors facilitating Spread
Towner KJ JHI 2009
Factors facilitating Spread
Towner KJ JHI 2009
‘Iraqibacter’
MDRA and Military
• Wounds and burns, bacteraemias
• High throughput, influx of trauma
• High levels broad spectrum antibiotics
for trauma injuries
• Little de-escalation or microbiology support
• Antibiotic prescribing intense and without policy
• Much equipment, much contaminated
• Multiple transfers through different units in medical evacuation
• Many procedures along the routes
• MDRA isolated in every hospital on the aeromedical evacuation routes from
Iraq and Afghanistan. Spread in units where repatriated
• High pressure lavage…aerosol generating
• Not pre-injury colonisation or inoculation at time of trauma
• Hospital unit is the habitat
• Periodic closures of units/tents for deep clean
• MDRA led to major focus of military on infection control, microbiology
support, antibiotic programme …… and MDRA control
Multi-drug resistant Acinetobacter (MDRA)
• Over the past few decades, isolates of Acinetobacter spp. have
successfully accumulated resistance to penicillins, cephalosporins,
quinolones and aminoglycosides
•Between 2003 and 2006, two carbapenemase-resistant strains (SE
clone and OXA-23) became prevalent in over 40 UK hospitals
• OXA-23 clone susceptible only to colistin
• SE clone susceptibility to carbapenems is variable
• predominantly in the London area
• isolates originated mainly from sputum and wound cultures
• majority from patients in intensive care units
Coelho JM, et al. J Clin Microbiol. 2006; 44:3623-3627
Turton JF, et al. J Hosp Infect., 2004; 58: 170-179
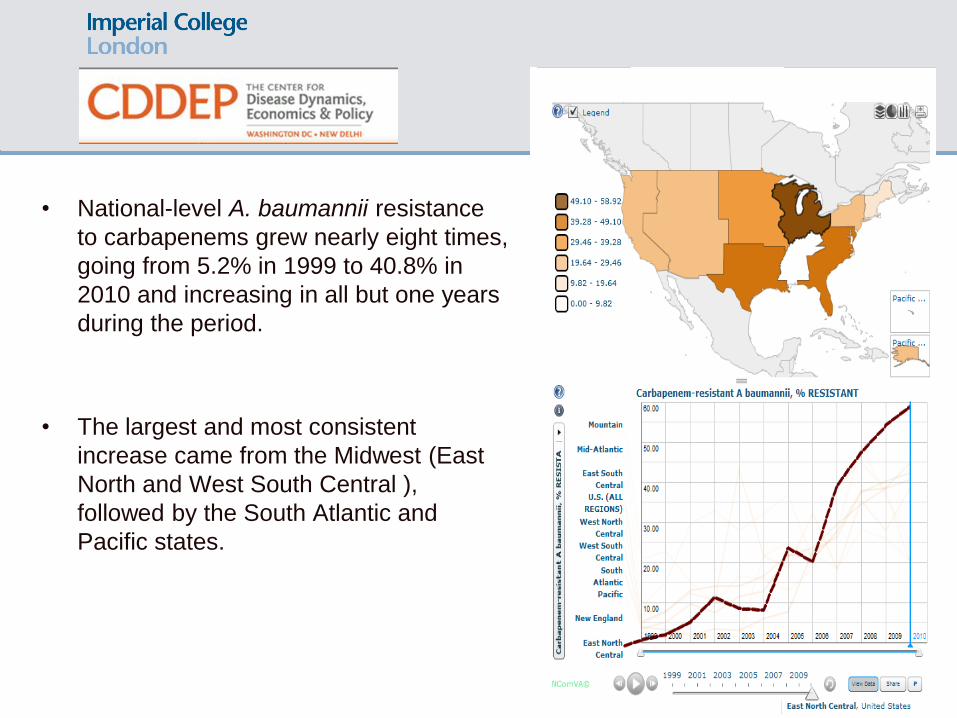
• National-level A. baumannii resistance
to carbapenems grew nearly eight times,
going from 5.2% in 1999 to 40.8% in
2010 and increasing in all but one years
during the period.
• The largest and most consistent
increase came from the Midwest (East
North and West South Central ),
followed by the South Atlantic and
Pacific states.
• Because of Acinetobacter’s low virulence,
few colonized patients develop a disease.
However, when an infection does occur, it
often results in hospital-wide outbreaks and
relatively high rates of mortality. In the
outpatient setting, the pathogen has been
associated with wound infections among
soldiers, earning it the name “Iraqibacter.”
• The striking decline in carbapenem
effectiveness points to two major
conclusions: one is the urgent need to
develop new drugs active against Gram-
negative bacteria; second is the medical
community’s need to evaluate the benefits of
large-scale vaccination of populations most
affected by A. baumannii, such as military
personnel and those in contact with them.
Surveillance
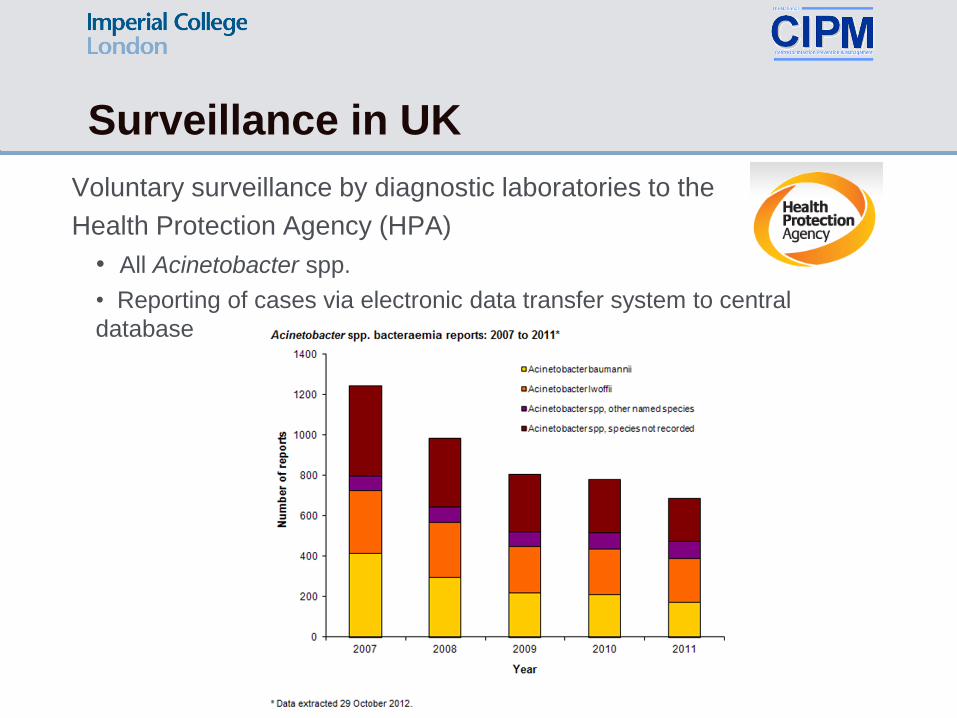
Surveillance in UK
Voluntary surveillance by diagnostic laboratories to the
Health Protection Agency (HPA)
• All Acinetobacter spp.
• Reporting of cases via electronic data transfer system to central
database
HPA Voluntary Surveillance: Data Analysis
• For A. baumannii, there has been a significant rise
in imipenem resistance from 21% in 2006 to 27% in
2010 (p<0.05)
• Only a small proportion of all isolates were tested.
• Between 2007 and 2011 there were no significant
changes.
http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317131514188
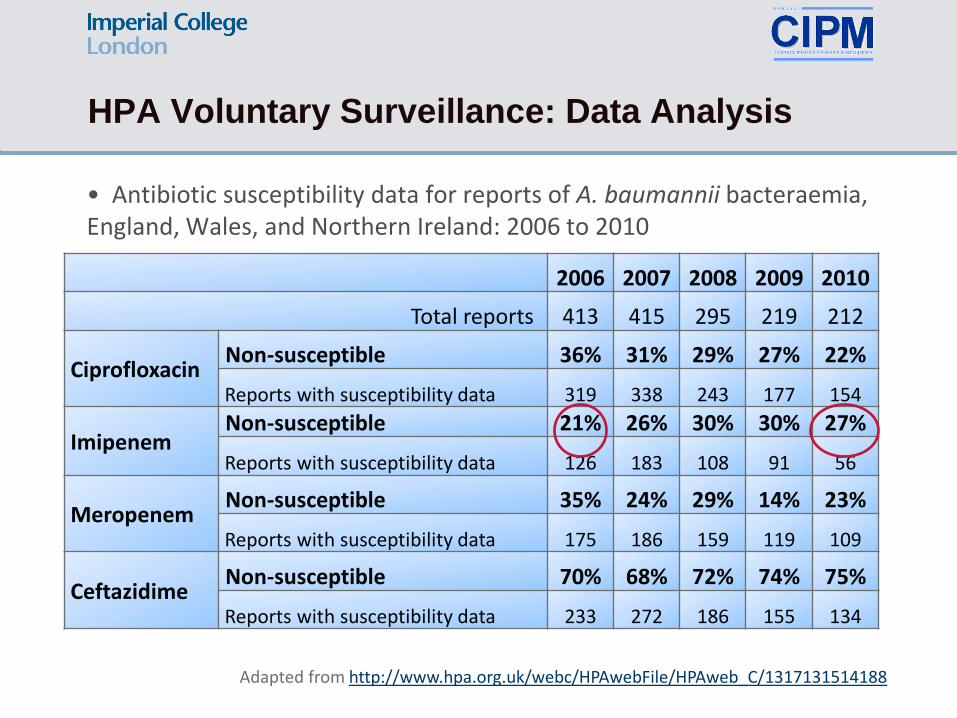
HPA Voluntary Surveillance: Data Analysis
• Antibiotic susceptibility data for reports of A. baumannii bacteraemia, England, Wales, and Northern Ireland: 2006 to 2010
2006 2007 2008 2009 2010
Total reports 413 415 295 219 212
Ciprofloxacin Non-susceptible 36% 31% 29% 27% 22%
Reports with susceptibility data 319 338 243 177 154
Imipenem Non-susceptible 21% 26% 30% 30% 27%
Reports with susceptibility data 126 183 108 91 56
Meropenem Non-susceptible 35% 24% 29% 14% 23%
Reports with susceptibility data 175 186 159 119 109
Ceftazidime Non-susceptible 70% 68% 72% 74% 75%
Reports with susceptibility data 233 272 186 155 134
Adapted from http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317131514188
Surveillance cont…
British Society for Antimicrobial Chemotherapy (BSAC)
• Respiratory Resistance Surveillance Programme
• Sentinel surveillance
• All Acinetobacter spp., identified to species level
• Hospital-acquired infections
• Lower respiratory tract specimens, from patients with clinical infection
• Susceptibility testing against variety of antimicrobials
Antimicrobial Resistance and Healthcare Associated Infections
Reference Unit (HPA)
• reference unit available for confirmation of “unusual” resistance
patterns
• Acinetobacter spp. isolates can be sent if they exhibit resistance to
carbapenems or colistin
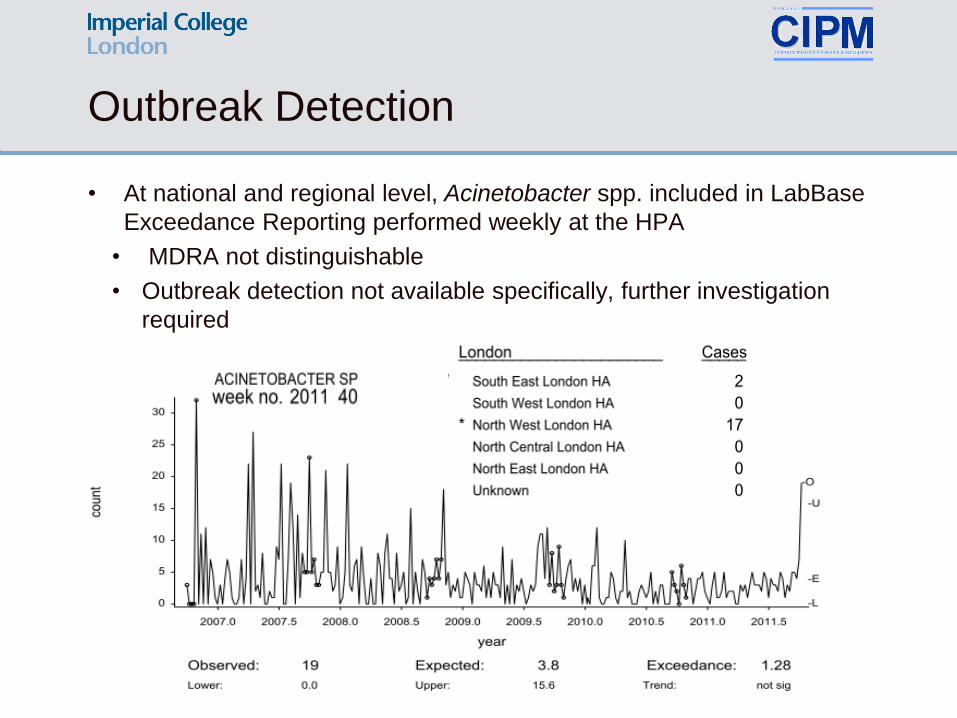
Outbreak Detection
• At national and regional level, Acinetobacter spp. included in LabBase
Exceedance Reporting performed weekly at the HPA
• MDRA not distinguishable
• Outbreak detection not available specifically, further investigation
required
Need
standardised
definitions for
surveillance
and outbreak
detection
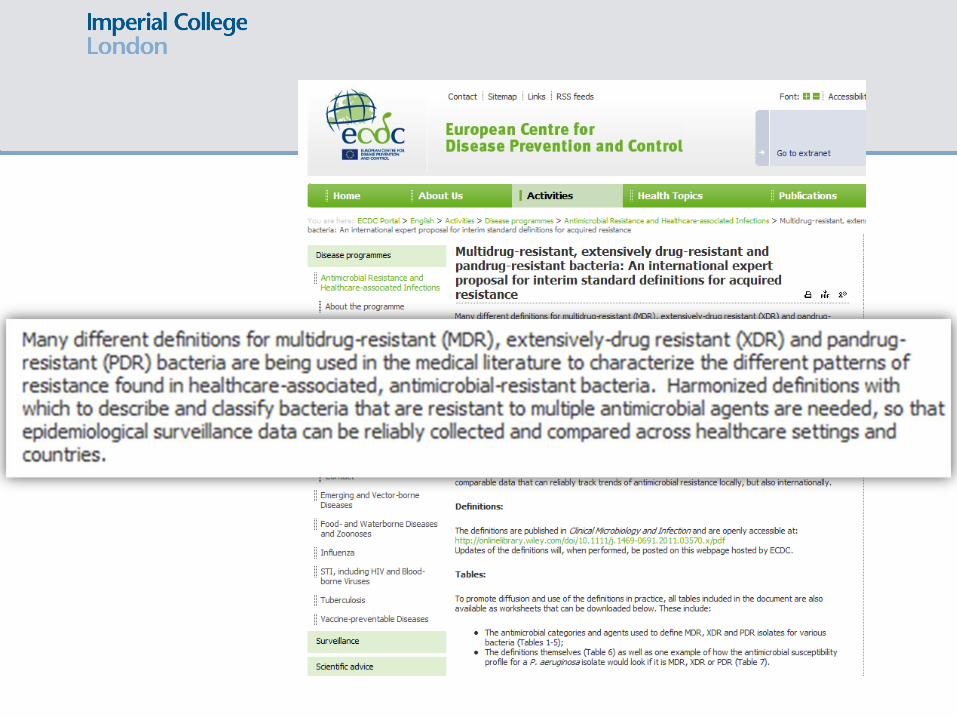
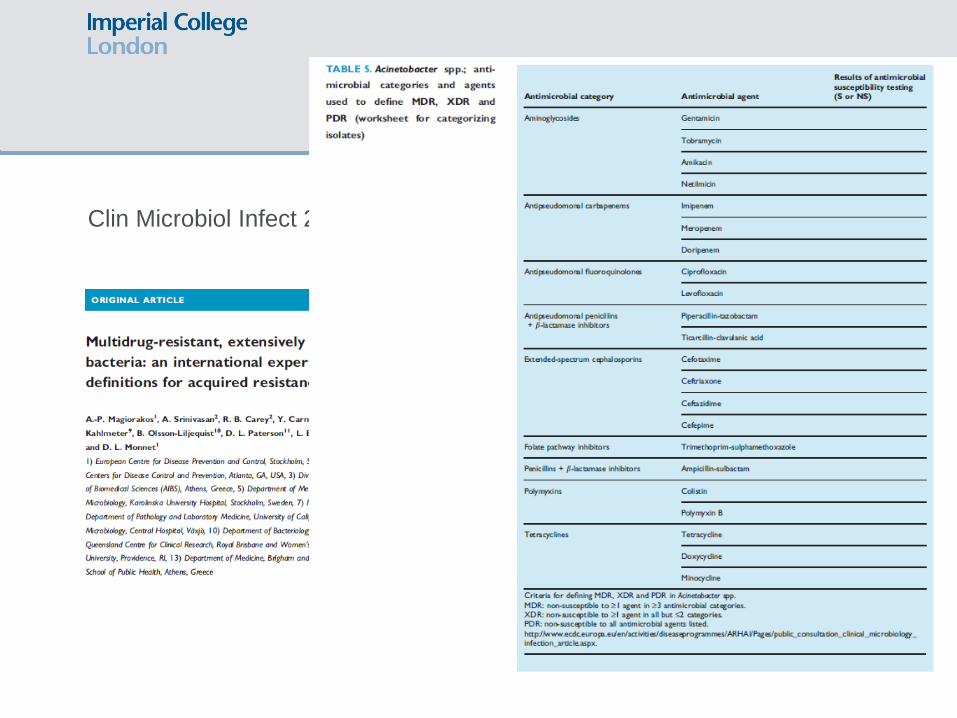
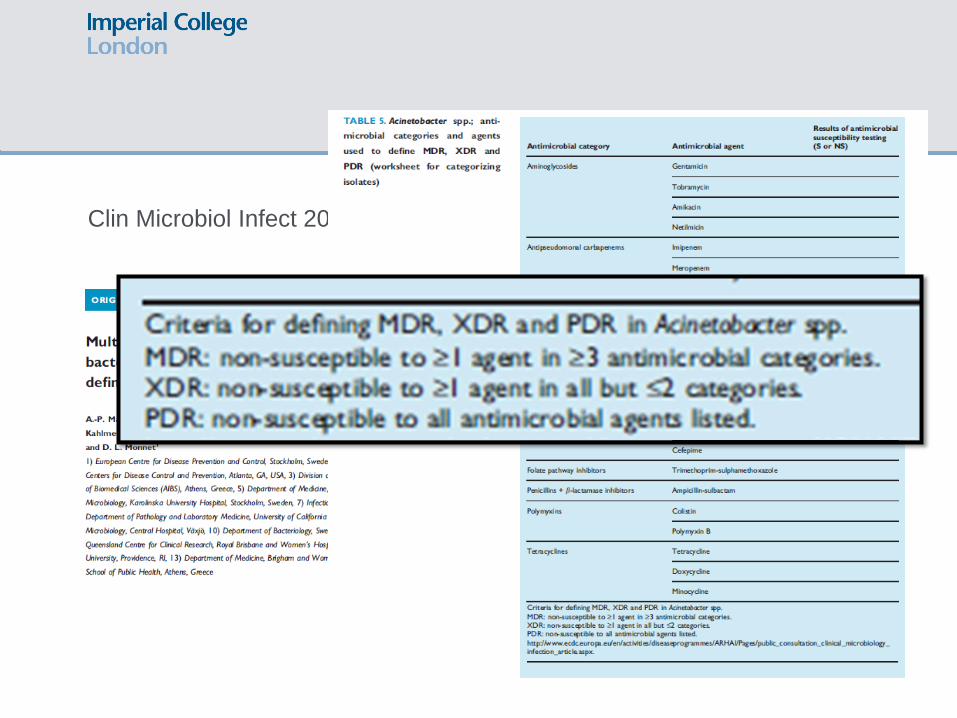
Need for Standard Definitions
Clin Microbiol Infect 2012; 18: 268–281
Clin Microbiol Infect 2012; 18: 268–281
Clin Microbiol Infect 2012; 18: 268–281
However……outside the lab…..
• Need pragmatic definitions for surveillance and for
clinicians…
• Carbapenem resistance ?
• What about ‘CRAB’ ?
• See CDDEP ( )
• Drug/Bug surveillance
• Useful as a definition....?
• Can be CRAB without being MDRA...
• Addresses importance of OXA type carbapenemase
• And clinical significance ‘resistance to critically important
drug class’
The Control
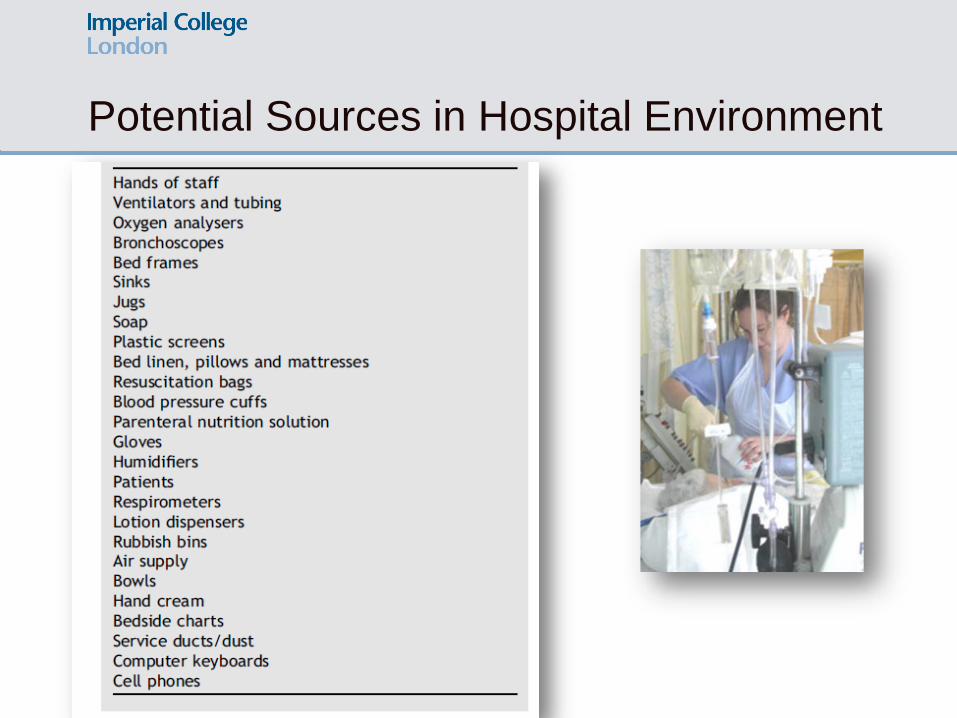
Potential Sources in Hospital Environment
Infection Control
Key measures include:
• Patient contact-isolated in side-room
• Careful review of practice
• More than one case, outbreak
management
• Typing
• Cohorting patients, nursing staff.
• Antimicrobial prescribing reviewed
• Strict hand hygiene practices
• Implementation of “deep clean”
strategies;
• Close attention to environment and all
equipment
Infection Control
• Ward closures often required
• Followed by terminal clean before re-open
• Most significant source in an outbreak situation are patients already
infected/colonised with MDRA
• The importance of adequate staffing needs to be addressed
• Once endemic in a healthcare setting, MDRA is difficult to eradicate
Detailed guidelines on how to deal with MDRA outbreaks prepared by a Working
Party of the HPA http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1194947325341
• Avoid homogeneity of
prescribing
• Minimise
carbapenem use

Novel Strategies needed
• A. baumannii poses a particular challenge due to the
intrinsic drug resistance imparted by its impermeable
outer membrane and its rapid acquisition of resistance
to new antibiotics
• Given these characteristics, small molecule antibiotics
will unlikely prove to be a lasting solution to A.
baumannii infections.
• Novel strategies for the treatment and prevention of
these infections are therefore desperately needed.
Whole Genome Sequencing
• Genomic
epidemiology
• Disruptive
technology
• Several
technologies on the
market
• Determine chains of
transmission
• Target intervention
• Pallen ‘’JHI was a
scoping study’’

The Importance of closure
Needs adequate
risk assessment
and cost
effectiveness
analysis.
What are the
health economic
implications?
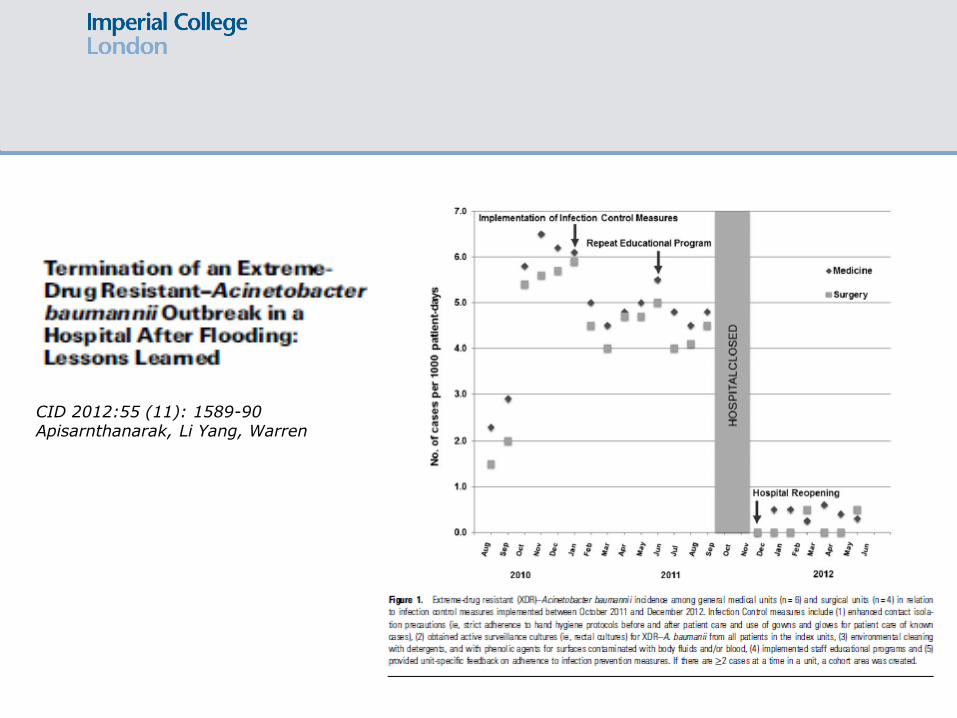
CID 2012:55 (11): 1589-90 Apisarnthanarak, Li Yang, Warren