
Mucinous adenocarcinoma of the colon - a histochemical study
8
Rom J Morphol Embryol 2011, 52(3):783–790 ORIGINAL PAPER Mucinous adenocarcinoma of the colon – a histochemical study M. IONILĂ 1) , CL. MĂRGĂRITESCU 2) , D. PIRICI 3) , S. S. MOGOANTĂ 4) 1) PhD student in Histology 2) Department of Pathology 3) Department of Histology 4) Department of Surgery University of Medicine and Pharmacy of Craiova Abstract Colorectal carcinoma is a major cause of cancer associated with a high rate of morbidity and mortality in the western world. One of the pathologic features considered to be important for prognostic is mucin production. Many authors confirmed that colon carcinomas with high mucin content tend to re-occur locally and carry a poor prognosis. For histochemical evaluation of mucin content, we investigated 149 patients who underwent surgical resection of sporadic colon adenocarcinomas, all over a 5-year period. For histological classification we used the WHO recommendation (2000) and to be more accurate we sub-classified mucinous adenocarcinomas by morphometrical analysis in three categories: pure mucinous, with extracellular mucin more than 80% of the tumoral volume; mixed type, with 50–80% extracellular mucin; and mixed type with less than 50% extracellular mucin. For histochemical investigation, we used stains such as: mucicarmine, PAS/Alcian Blue and High Iron Diamine/Alcian Blue. Our study proved the predominance of mixed mucinous adenocarcinomas with less than 50% extracellular mucin, followed by the pure mucinous type. From the biochemical composition’s point of view, the predominant cases were those with acidic mucins, especially in pure mucinous adenocarcinomas (>90%), while those with mixtures of acidic and neutral mucins were present in 62% of the cases. In addition, our study showed the prevalence of sialomucins over sulphomucins (68%), particularly in pure mucinous adenocarcinomas (77%). Clinical pure mucinous forms were detected mainly in advanced stages, but in terms of lymph node metastasis rate, they were secondary after mixed type with 50–80% extracellular mucin. Keywords: colon adenocarcinoma, mucins, histochemistry. Introduction Colorectal cancer (CRC) is the fourth most commonly diagnosed malignant disease worldwide, with over one million new cases and approximately 500 000 deaths each year [1]. Over time there have been investigated a number of morphoclinic parameters with prognostic value in colon cancer, such as: tumor resection margins, histologic size, lesional topography, obstruction and perforation, lymph node involvement, lymphatic vessel invasion, blood vessel invasion [2]. These studies have resulted in 2000, after the Consensus Conference of the Colorectal Working Group of the American Joint Committee on Cancer Prognostic Factors (AJCC) [3, 4] in determining the establishment of four categories of prognostic factors with clear implications in treatment planning and survival estimation for these patients. One of the histological features of colorectal cancers with important impact on prognosis and therapeutic management of these patients is tumor cells’ mucin production. According to WHO, digestive tract tumor classification [5], mucinous adenocarcinoma (MA) is a subtype of colorectal adenocarcinoma with more than 50% of the lesion composed of mucin. Most authors agree that patients with MA in terms of its presence at a more advanced stage of disease also have a poorer prognosis than those with other types of carcinoma [6, 7]. Also, it is considered that because of these differences in colorectal MA, the lesional topography and its presentation stage would rather be responsible for their survival, than the histological type [6]. However, it seems that MAs are heterogeneous tumors with respect to their clinicopathological and molecular features [8]. For these reasons, the purpose of our study was to clarify the clinicopathological characteristics of colon MA in the population of Dolj County, especially in what it regards the histochemical types of mucin components. Materials and Methods A series of 149 consecutive cases of mucinous colorectal carcinomas (only surgical resections), retrieved from the Pathology department’s files between 2006–2010 were studied. Only MA were included in this study and they were divided into the following groups based on mucin content, morphometric analysis on transverse sections of surgical specimens: (i) pure mucinous with extra- cellular mucin more than 80% of the tumoral area (PMA); (ii) mixed type with 50–80% extracellular R J M E Romanian Journal of Morphology & Embryology http://www.rjme.ro/
Transcript of Mucinous adenocarcinoma of the colon - a histochemical study

Rom J Morphol Embryol 2011, 52(3):783–790
OORRIIGGIINNAALL PPAAPPEERR
Mucinous adenocarcinoma of the colon – a histochemical study
M. IONILĂ1), CL. MĂRGĂRITESCU2), D. PIRICI3), S. S. MOGOANTĂ4)
1)PhD student in Histology 2)Department of Pathology 3)Department of Histology 4)Department of Surgery
University of Medicine and Pharmacy of Craiova
Abstract Colorectal carcinoma is a major cause of cancer associated with a high rate of morbidity and mortality in the western world. One of the pathologic features considered to be important for prognostic is mucin production. Many authors confirmed that colon carcinomas with high mucin content tend to re-occur locally and carry a poor prognosis. For histochemical evaluation of mucin content, we investigated 149 patients who underwent surgical resection of sporadic colon adenocarcinomas, all over a 5-year period. For histological classification we used the WHO recommendation (2000) and to be more accurate we sub-classified mucinous adenocarcinomas by morphometrical analysis in three categories: pure mucinous, with extracellular mucin more than 80% of the tumoral volume; mixed type, with 50–80% extracellular mucin; and mixed type with less than 50% extracellular mucin. For histochemical investigation, we used stains such as: mucicarmine, PAS/Alcian Blue and High Iron Diamine/Alcian Blue. Our study proved the predominance of mixed mucinous adenocarcinomas with less than 50% extracellular mucin, followed by the pure mucinous type. From the biochemical composition’s point of view, the predominant cases were those with acidic mucins, especially in pure mucinous adenocarcinomas (>90%), while those with mixtures of acidic and neutral mucins were present in 62% of the cases. In addition, our study showed the prevalence of sialomucins over sulphomucins (68%), particularly in pure mucinous adenocarcinomas (77%). Clinical pure mucinous forms were detected mainly in advanced stages, but in terms of lymph node metastasis rate, they were secondary after mixed type with 50–80% extracellular mucin. Keywords: colon adenocarcinoma, mucins, histochemistry.
Introduction
Colorectal cancer (CRC) is the fourth most commonly diagnosed malignant disease worldwide, with over one million new cases and approximately 500 000 deaths each year [1].
Over time there have been investigated a number of morphoclinic parameters with prognostic value in colon cancer, such as: tumor resection margins, histologic size, lesional topography, obstruction and perforation, lymph node involvement, lymphatic vessel invasion, blood vessel invasion [2]. These studies have resulted in 2000, after the Consensus Conference of the Colorectal Working Group of the American Joint Committee on Cancer Prognostic Factors (AJCC) [3, 4] in determining the establishment of four categories of prognostic factors with clear implications in treatment planning and survival estimation for these patients.
One of the histological features of colorectal cancers with important impact on prognosis and therapeutic management of these patients is tumor cells’ mucin production. According to WHO, digestive tract tumor classification [5], mucinous adenocarcinoma (MA) is a subtype of colorectal adenocarcinoma with more than 50% of the lesion composed of mucin. Most authors agree that patients with MA in terms of its presence at a
more advanced stage of disease also have a poorer prognosis than those with other types of carcinoma [6, 7]. Also, it is considered that because of these differences in colorectal MA, the lesional topography and its presentation stage would rather be responsible for their survival, than the histological type [6]. However, it seems that MAs are heterogeneous tumors with respect to their clinicopathological and molecular features [8].
For these reasons, the purpose of our study was to clarify the clinicopathological characteristics of colon MA in the population of Dolj County, especially in what it regards the histochemical types of mucin components.
Materials and Methods
A series of 149 consecutive cases of mucinous colorectal carcinomas (only surgical resections), retrieved from the Pathology department’s files between 2006–2010 were studied.
Only MA were included in this study and they were divided into the following groups based on mucin content, morphometric analysis on transverse sections of surgical specimens: (i) pure mucinous with extra-cellular mucin more than 80% of the tumoral area (PMA); (ii) mixed type with 50–80% extracellular
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

M. Ionilă et al.
784
mucin (MMA); and (iii) mixed type with less than 50% extracellular mucin (mMA). Sections from normal colon were taken as controls.
Representative transverse section fragments were fixed in 10% neutral buffered formalin, and processed for paraffin inclusion. 2–3 µm thick sections were cut for routine HE (Hematoxylin–Eosin) staining.
PAS (Periodic Acid Schiff) and mucicarmine were performed for general staining of mucins, PAS/AB (Periodic Acid Schiff/Alcian Blue), HID (High Iron Diamine) were done for determining the nature of mucins (as neutral and acidic), and a HID/AB (High Iron Diamine/Alcian Blue) staining was done to differentiate between sulphomucins and sialomucins [9, 10].
Mucin content of the investigated cases was estimated by morphometric assessment as the area occupied by mucin present on transverse section slides of the surgical specimens specifically stained and using the NIS elements image analysis software (Nikon, Apidrag, Bucharest). Briefly, this was achieved by investigating the lesions with a 4× objective (tissue scanned from the surface to the depth of the lesion), and from one end to the other, for about 20 microscopic fields.
From the pathological report, slides and clinical record, the following items were retrieved: age, gender, location, size (T), stage (TNM), microscopic features, degree of differentiation, depth of tumor invasion and lymph node status.
Tumors were classified and staged according to the sixth edition of the TNM Classification of the American Joint Committee on Cancer [11]. Tumors were grades 1–3 depending on the degree of gland formation: >70%, grade 1 (well differentiated), 30–70%, grade 2 (moderate differentiation), and <30%, grade 3 (poor differentiation).
The relationship between mucinous content and various clinicopathologic features was tested by chi-square test. Statistics and graph plotting were done in Microsoft Excel 2003.
Results
Epidemiologic characteristics
Regarding mucin content in our casuistry, the predominant form was the mMA type with 50% extra-cellular mucin (52.5%), followed by the PMA (32%) and MMA (15.5%).
In what it regarded the clinicopathologic features studied in parallel, we observed that regardless of the mucin content, MA prevailed in the fifth decade of life, especially in men (with men/female ratio about 1.4:1 in PMA), and in the right colon as lesion topography. The PMA and MMA developed with a somewhat higher percentage in the right colon (with 1.66 value of right/ left colon ratio in PMA and 1.55 for MMA type). Also, these MA subtypes were diagnosed in advanced stages
of disease (52% and respective 56.5% in pTNM stage III); the PMA cases having at least the muscularis propria invaded at the time of diagnosis. The lymph node metastasis was present in 43% of all investigated cases, with the highest percentage recorded for MMA type (56.5%), followed by PMA (46%).
Microscopic characteristics
In PMA, the carcinomatous proliferation had one of the following aspects:
▪ Acini-like structures floating in lakes of mucus, consisting in clumps of carcinomatous cells with pyknotic nuclei and eosinophilic cytoplasm (Figure 1a). Sometimes inside of these carcinomatous proliferations, we could identify the presence of glandular lumens and even a solid or cribriform pattern.
▪ Uni- or multilayered cords of flat carcinomatous cell delimiting lakes of mucus with varying shapes and sizes (Figure 1b). Often, this limiting malignant epithelium was detached and found floating in lakes of mucus.
▪ Isolated carcinoma cells floating in lakes of mucus (Figure 1c). Only in three cases, some of these carcinoma cells following intracellular mucus accumulation have adopted a particular morphology of “signet ring” (Figure 1d).
In the other types of MA (MMA and mMA), in addition to the above issues there were present aspects of conventional adenocarcinoma with various degrees of differentiation. According with this degree of differentiation, the prevalent types were well and moderate differentiated forms (45% and respective 40%); the poor differentiated type being present only in PMA.
Histochemical characteristics
PAS/AA stain highlighted the overwhelming prevalence of cases of MA with a mixed secretion of acid and neutral mucins (>61%), (Figure 1, e and f). A qualitative assessment of these cases revealed the peculiar prevalence of acid mucins (>80% for MMA and for mMA cases).
Regarding the MA subtype, we found that in PMA and MMA acid mucins were prevalent (>90%, respective >58%) (Figure 2, a and b), while in mMA there was a balance between the two types of excreted mucins (Figure 2c).
HID/AB stain revealed the overwhelming prevalence of MA with mixed secretion of sulpho-mucins and sialomucins (>70%) (Figure 2d). A qualitative assessment indicated a prevalence of sialomucins (>72% for mixed MA).
According to histological subtype we found that in PMA prevailed sialomucins (>82% of cases) (Figure 2e), in mMA there was a slight prevalence of sulphomucins (>57%) (Figure 2f), and in MMA there was a balance between sialomucins and sulphomucins.
Also, we noticed the presence of intracellular mucus,

Mucinous adenocarcinoma of the colon – a histochemical study
785
especially in mMA cases where the PAS/AA stain revealed the prevalence of acid mucins (Figure 3a), while the HID/AB stain highlighted the predominance of sialomucins. Usually, the sulphomucins were observed in mMA cases with the least degree of malignancy (Figure 3b).
Results of statistical investigations
In PMA, we observed a statistically significant difference between mucin content on different age groups, χ²(12, N=36) = 38.56, p=0.00012. There are significant differences between the mucin content of the IV–Vth decade of life, where mixed mucins prevailed, followed by far by sialomucins. In the VI–VIIth decades sialomucins where predominating, followed closely by mixed mucins (sialo- and sulphomucins).
The presence of sialo- and sulphomucins was significantly different depending on the degree of differ-entiation χ²(4, N=48) = 11.21, p=0.02423. Thus, we observed a decrease of sulphomucins and an increase in the amount of mixed mucins (sialo- and sulphomucins) with decreasing degree of tumor differentiation.
The presence of lymphatic metastasis was significantly different depending on: (1) the degree of differentiation χ²(4, N=48) = 35.81, p=3.2×10-7, the number of metastases increasing with decreasing degree of differentiation (Figure 3c); (2) pTNM staging χ²(6, N=48) = 28.21, p=1.3×10-7, the number of metastases increasing with the stage of disease; (3) the
stage of tumor invasion, χ²(3, N=48) = 27.34, p=5×10-6, the number of metastases increasing with the depth of invasion.
In mMA, we noticed a difference in the mucin content (acid/neutral mucins) for different age groups [χ²(8, N=16), p=4.4×10-38], between the III–VIIIth decades of life predominating mixed acid/neutral mucins, followed by neutral mucins, the trend being of an increase until the Vth decade, followed by a proportional decrease to the VIII–IXth decades of life. In addition, we observed a difference in the sulphatated or non-sulphatated mucin content for different age groupes [χ²(10, N=14), p=2.7×10-57], between III–VIIIth decades of life predominating the mixed sulpho-/ sialomucins, followed by sulphomucins, the trend being of an increase between the III–VIth decades, followed by a decrease towards very higher ages. Also, significant differences were obtained between the type of acid vs. neutral mucin content for different staging of neoplastic disease pTNM [χ²(6, N=78) = 37.79, p=0.00016] (Figure 3d) and for different depths of invasion [χ²(3, N=78) = 28.81, p=6.6×10-8].
Moreover, the sialo- and sulphomucins content was different for different in mMA with invasion stages, the mixed mucins prevailing especially in advanced stages of neoplasia. In addition, we also noted a relatively equal level of sialo- and sulphomucins in N0 and N1 stages, but in N2 stage the mixed mucins were predominating (Student t-test, p<0.05].
(a) (b)
(c) (d)Figure 1 – Colon mucinous adenocarcinoma: (a) Acini-like structures floating in lakes of mucus, HE stain, ×200; (b) Uni- and multilayered cords of flat carcinomatous cells delimiting lakes of mucus with detaching cells, HE stain, ×100; (c) Isolated carcinoma cells floating in lakes of mucus, HE stain, ×100; (d) Carcinoma cells with the “signet ring” morphology, HE stain, ×200.
M. Ionilă et al.
786
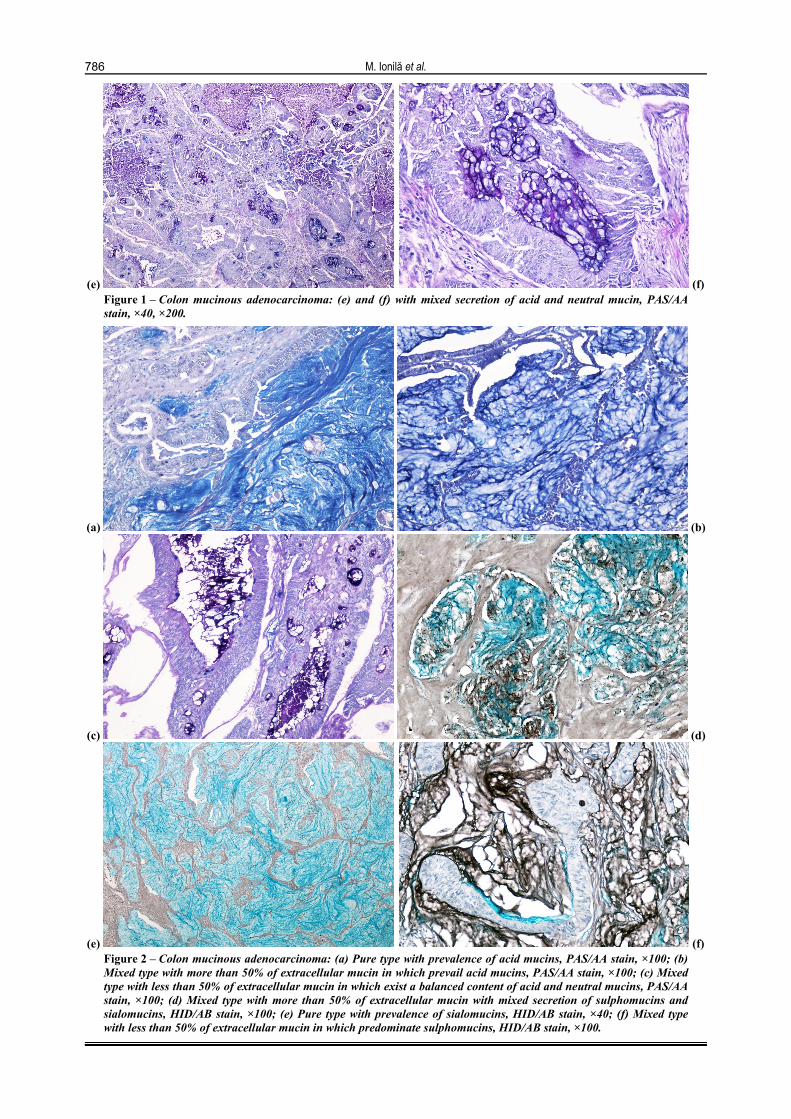
(e) (f)Figure 1 – Colon mucinous adenocarcinoma: (e) and (f) with mixed secretion of acid and neutral mucin, PAS/AA stain, ×40, ×200.
(a) (b)
(c) (d)
(e) (f)Figure 2 – Colon mucinous adenocarcinoma: (a) Pure type with prevalence of acid mucins, PAS/AA stain, ×100; (b) Mixed type with more than 50% of extracellular mucin in which prevail acid mucins, PAS/AA stain, ×100; (c) Mixed type with less than 50% of extracellular mucin in which exist a balanced content of acid and neutral mucins, PAS/AA stain, ×100; (d) Mixed type with more than 50% of extracellular mucin with mixed secretion of sulphomucins and sialomucins, HID/AB stain, ×100; (e) Pure type with prevalence of sialomucins, HID/AB stain, ×40; (f) Mixed type with less than 50% of extracellular mucin in which predominate sulphomucins, HID/AB stain, ×100.
Mucinous adenocarcinoma of the colon – a histochemical study
787
(a) (b)
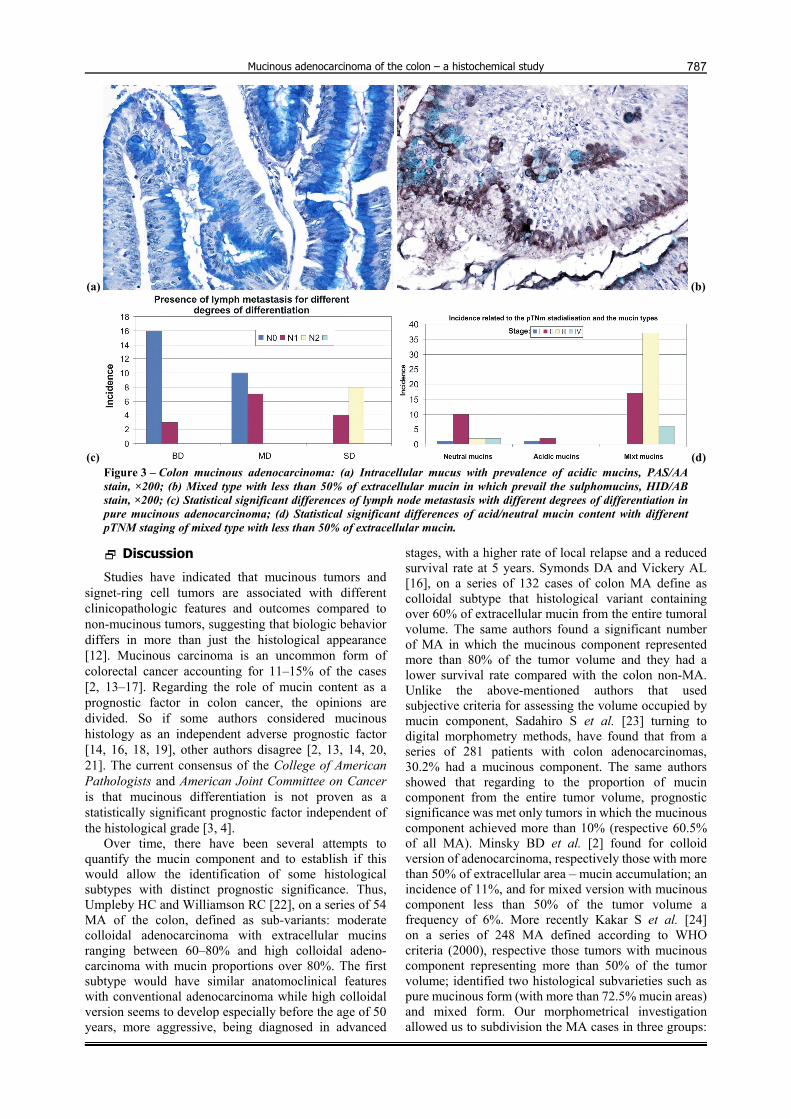
(c) (d)Figure 3 – Colon mucinous adenocarcinoma: (a) Intracellular mucus with prevalence of acidic mucins, PAS/AA stain, ×200; (b) Mixed type with less than 50% of extracellular mucin in which prevail the sulphomucins, HID/AB stain, ×200; (c) Statistical significant differences of lymph node metastasis with different degrees of differentiation in pure mucinous adenocarcinoma; (d) Statistical significant differences of acid/neutral mucin content with different pTNM staging of mixed type with less than 50% of extracellular mucin.
Discussion
Studies have indicated that mucinous tumors and signet-ring cell tumors are associated with different clinicopathologic features and outcomes compared to non-mucinous tumors, suggesting that biologic behavior differs in more than just the histological appearance [12]. Mucinous carcinoma is an uncommon form of colorectal cancer accounting for 11–15% of the cases [2, 13–17]. Regarding the role of mucin content as a prognostic factor in colon cancer, the opinions are divided. So if some authors considered mucinous histology as an independent adverse prognostic factor [14, 16, 18, 19], other authors disagree [2, 13, 14, 20, 21]. The current consensus of the College of American Pathologists and American Joint Committee on Cancer is that mucinous differentiation is not proven as a statistically significant prognostic factor independent of the histological grade [3, 4].
Over time, there have been several attempts to quantify the mucin component and to establish if this would allow the identification of some histological subtypes with distinct prognostic significance. Thus, Umpleby HC and Williamson RC [22], on a series of 54 MA of the colon, defined as sub-variants: moderate colloidal adenocarcinoma with extracellular mucins ranging between 60–80% and high colloidal adeno-carcinoma with mucin proportions over 80%. The first subtype would have similar anatomoclinical features with conventional adenocarcinoma while high colloidal version seems to develop especially before the age of 50 years, more aggressive, being diagnosed in advanced
stages, with a higher rate of local relapse and a reduced survival rate at 5 years. Symonds DA and Vickery AL [16], on a series of 132 cases of colon MA define as colloidal subtype that histological variant containing over 60% of extracellular mucin from the entire tumoral volume. The same authors found a significant number of MA in which the mucinous component represented more than 80% of the tumor volume and they had a lower survival rate compared with the colon non-MA. Unlike the above-mentioned authors that used subjective criteria for assessing the volume occupied by mucin component, Sadahiro S et al. [23] turning to digital morphometry methods, have found that from a series of 281 patients with colon adenocarcinomas, 30.2% had a mucinous component. The same authors showed that regarding to the proportion of mucin component from the entire tumor volume, prognostic significance was met only tumors in which the mucinous component achieved more than 10% (respective 60.5% of all MA). Minsky BD et al. [2] found for colloid version of adenocarcinoma, respectively those with more than 50% of extracellular area – mucin accumulation; an incidence of 11%, and for mixed version with mucinous component less than 50% of the tumor volume a frequency of 6%. More recently Kakar S et al. [24] on a series of 248 MA defined according to WHO criteria (2000), respective those tumors with mucinous component representing more than 50% of the tumor volume; identified two histological subvarieties such as pure mucinous form (with more than 72.5% mucin areas) and mixed form. Our morphometrical investigation allowed us to subdivision the MA cases in three groups:

M. Ionilă et al.
788
pure mucinous with extracellular mucin more than 80% of the tumoral area (PMA), mixed type with 50–80% extracellular mucin (MMA), and mixed type with less than 50% extracellular mucin (mMA). According to this, in our casuistry predominated the mMA type (52.5%), followed by the PMA (32%) and MMA (15.5%).
Regarding the biochemical mucin type in our casuistry, we recorded the prevalence of mixed mucin, both acid and neutral types (about 62% of cases), the acid mucins being the predominant type, especially in PMA form (>90% of these cases). Moreover, in mMA cases we recorded differences between mucin content in acid/neutral mucins for different age groups. Thus between the III–VIIIth decades of life prevailed mixed mucins, followed by neutral mucins, this trend remaining high until the Vth decade, followed by a proportional decrease to the VIIIth and IXth decades of life.
Regarding the acid mucin subtypes, our study revealed the prevalence of sialomucins (68% of all cases investigated), being best represented in PMA subtype (77% of these cases). In PMA there was a statistically significant difference between different age groups, with the prevalence of mixed mucins (sialo- and sulphomucins), followed by sialomucins in the IV–Vth decade of life, while in the VI–VIIth decade of life predominated sialomucins, followed by mixed mucins. In addition, we have recorded low levels of sulpho-mucins and an increase in the amount of mixed mucins (sulpho-/sialomucins) with decreasing degree of tumor differentiation. For the mMA histological types, we recorded that between the III–VIIIth decades of life prevailed mixed mucins followed by sulphomucins, the trend being ascending between decades III–VIth, then there was a decreasing tendency with the increasing age. Significant differences were also obtained between the types of mucin content (acid versus neutral), for different neoplastic disease staging (pTNM) and depths of invasion.
Studies have shown that in normal colorectal mucosa there is a mixture of acid and neutral mucin, the neutral one predominating especially in the ascending and transverse segments [25–27]. Regarding the type of acid mucin present in normal colon mucosa, it was proved the existence of both sulpho- and sialomucin, the first type being prevalent [25–27]. It was showed that there are differences in the composition of mucin in goblet cells in various segments of the colon [26, 27], and also at different levels of the glands themselves [25, 26].
Furthermore, in 1969, Filipe MI [28] introduce the term of “transitional mucosa” to describe a type of abnormal colic mucosa present adjacent to colon adeno-carcinoma, in which goblet cells have an excess of sialomucins, the sulphomucins being under-represented or even being absent [28]. Other studies have addressed this “transitional mucosa” and various authors have obtained somewhat conflicting results regarding the abnormal profile of sialo- and sulphomucins content of goblet cells at this level [29–32]. Further controversy arose about the nature and potential clinical applications of this “transitional mucosa” [33]. This acid mucinous
profile of mucosal goblet cells adjacent to carcinomas is similar to the mucosecretion pattern of fetal intestine, proving a putative reversion of these colon mucosa regions to an embryonic stage that may characterize early stages of carcinogenesis at this level, increasing the chance of early colon cancer detection [34].
Similar to our study, the vast majority of histo-chemical studies carried out for colon MA indicate the presence of acid and neutral mucins mixed secretions with the prevalence of acidic ones, and of these, sialomucins being best represented [34–42].
In our study, the PMA and MMA histological forms were diagnosed especially in stage III pTNM (52% and respective 56.5%), 100% of PMA cases being in T3–T4 stages and 56.5% of MMA cases were metastatic in locoregional lymph nodes. Many studies conducted on colon MA have shown that it tends to be rather local invasive, with local dissemination and peritoneal seeding, the hematogenous dissemination not being a characteristic feature for this type of cancer [43–46]. Predisposition for this type of lymph node metastasis can be explained by the blockade of the local anti-tumoral immune response by increased secretion of mucopolysaccharides, which would facilitate pericolic tissue invasion and the infiltration into lymphatic vessels and lymph nodes [47]. More recently, Goi T et al. [48] and Chen JS et al. [49] suggested that there are two different subtypes of mucinous colorectal carcinoma with different prognostics (tubolopapillary and muco-cellular). The muco-cellular type appears to have a higher rate of venous invasion, lymph node metastasis, liver metastasis, peritoneal dissemination and to occur in more advanced stages (III–IV) than tubolopapillary type. In addition, other authors suggest that variations related to survival of patients with colon adenocarcinoma was due not so much to carcinoma histological type, but especially to differences in tumor topography and stage at diagnosis [4, 7, 44].
Conclusions
Our study proved the prevalence of MA cases with mixed acid and neutral mucin content, with acid mucin being more represented especially in the PMA. Subsequent, from the acid mucins group sialomucins prevailed. The PMA and MMA were diagnosed in advance stages (III–IV pTNM), and with a higher rate of lymph node metastasis.
References [1] Parkin DM, Bray F, Ferlay J, Pisani P, Global cancer
statistics, 2002, CA Cancer J Clin, 2005, 55(2):74–108. [2] Minsky BD, Mies C, Rich TA, Recht A, Chaffey JT, Colloid
carcinoma of the colon and rectum, Cancer, 1987, 60(12):3103–3112.
[3] Compton C, Fenoglio-Preiser CM, Pettigrew N, Fielding LP, American Joint Committee on Cancer Prognostic Factors Consensus Conference: Colorectal Working Group, Cancer, 2000, 88(7):1739–1757.
[4] Compton CC, Fielding LP, Burgart LJ, Conley B, Cooper HS, Hamilton SR, Hammond ME, Henson DE, Hutter RV, Nagle RB, Nielsen ML, Sargent DJ, Taylor CR, Welton M, Willett C, Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999, Arch Pathol Lab Med, 2000, 124(7):979–994.
Mucinous adenocarcinoma of the colon – a histochemical study
789[5] Hamilton SR, Rubio CA, Vogelstein B et al., Carcinoma of
the colon and rectum. In: Hamilton SR, Aaltonen LA (eds), Pathology and genetics of tumours of the digestive system, World Health Organization Classification of Tumours, IARC Press, Lyon, 2000, 103–143.
[6] Yamamoto S, Mochizuki H, Hase K, Yamamoto T, Ohkusa Y, Yokoyama S, Ushitani Y, Tamakuma S, Assessment of clinicopathologic features of colorectal mucinous adeno-carcinoma, Am J Surg, 1993, 166(3):257–261.
[7] Wu CS, Tung SY, Chen PC, Kuo YC, Clinicopathological study of colorectal mucinous carcinoma in Taiwan: a multivariate analysis, J Gastroenterol Hepatol, 1996, 11(1):77–81.
[8] Perez RO, Bresciani BH, Bresciani C, Proscurshim I, Kiss D, Gama-Rodrigues J, Pereira DD, Rawet V, Cecconnello I, Habr-Gama A, Mucinous colorectal adenocarcinoma: influence of mucin expression (Muc1, 2 and 5) on clinico-pathological features and prognosis, Int J Colorectal Dis, 2008, 23(8):757–765.
[9] Spicer SS, Diamine methods for differentialing muco-substances histochemically, J Histochem Cytochem, 1965, 13:211–234.
[10] Filipe MI, Lake BD, Histochemistry in Pathology, Churchill Livingstone, Edinburgh, 1983, 312.
[11] Green FL, Balch CM, Fleming ID, Fritz AG, Balch CM, Haller DG, Morrow M (eds), AJCC Cancer Staging Manual, 6th edition, Springer, Berlin–Heidelberg–New York, 2002.
[12] Kang H, O’Connell JB, Maggard MA, Sack J, Ko CY, A 10-year outcomes evaluation of mucinous and signet-ring cell carcinoma of the colon and rectum, Dis Colon Rectum, 2005, 48(6):1161–1168.
[13] Green JB, Timmcke AE, Mitchell WT, Hicks TC, Gathright JB Jr, Ray JE, Mucinous carcinoma – just another colon cancer? Dis Colon Rectum, 1993, 36(1):49–54.
[14] Secco GB, Fardelli R, Campora E, Lapertosa G, Gentile R, Zoli S, Prior C, Primary mucinous adenocarcinomas and signet-ring cell carcinomas of colon and rectum, Oncology, 1994, 51(1):30–34.
[15] Consorti F, Lorenzotti A, Midiri G, Di Paola M, Prognostic significance of mucinous carcinoma of colon and rectum: a prospective case-control study, J Surg Oncol, 2000, 73(2):70–74.
[16] Symonds DA, Vickery AL, Mucinous carcinoma of the colon and rectum, Cancer, 1976, 37(4):1891–1900.
[17] Nozoe T, Anai H, Nasu S, Sugimachi K, Clinicopathologic characteristics of mucinous carcinoma of the colon and rectum, J Surg Oncol, 2000, 75(2):103–107.
[18] Suma KS, Nirmala V, Mucinous component in colorectal carcinoma – prognostic significance: a study in a south Indian population, J Surg Oncol, 1992, 51(1):60–64.
[19] Connelly JH, Robey-Cafferty SS, Cleary KR, Mucinous carcinomas of the colon and rectum. An analysis of 62 stage B and C lesions, Arch Pathol Lab Med, 1991, 115(10):1022–1025.
[20] Enríquez JM, Díez M, Tobaruela E, Lozano O, Domínguez P, González A, Mugüerza JM, Ratia T, Clinical, histopatho-logical, cytogenetic and prognostic differences between mucinous and nonmucinous colorectal adenocarcinomas, Rev Esp Enferm Dig, 1998, 90(8):563–572.
[21] Messerini L, Ciantelli M, Baglioni S, Palomba A, Zampi G, Papi L, Prognostic significance of microsatellite instability in sporadic mucinous colorectal cancers, Hum Pathol, 1999, 30(6):629–634.
[22] Umpleby HC, Williamson RC, Carcinoma of the large bowel in the first four decades, Br J Surg, 1984, 71(4):272–277.
[23] Sadahiro S, Ohmura T, Saito T, Akatsuka S, An assessment of the mucous component in carcinoma of the colon and rectum, Cancer, 1989, 64(5):1113–1116.
[24] Kakar S, Aksoy S, Burgart LJ, Smyrk TC, Mucinous carcinoma of the colon: correlation of loss of mismatch repair enzymes with clinicopathologic features and survival, Mod Pathol, 2004, 17(6):696–700.
[25] Filipe MI, Branfoot AC, Mucin histochemistry of the colon. In: Morson BC (ed), Current topics in Pathology, Springer, Berlin–Heidelberg–New York, 1976, 143–178.
[26] Filipe MI, Mucins in the human gastrointestinal epithelium: a review, Invest Cell Pathol, 1979, 2(3):195–216.
[27] Shamsuddin AM, Phelps PC, Trump BF, Human large intestinal epithelium: light microscopy, histochemistry, and ultrastructure, Hum Pathol, 1982, 13(9):790–803.
[28] Filipe MI, Value of histochemical reactions for muco-substances in the diagnosis of certain pathological conditions of the colon and rectum, Gut, 1969, 10(7):577–586.
[29] Isaacson P, Attwood PR, Failure to demonstrate specificity of the morphological and histochemical changes in mucosa adjacent to colonic carcinoma (transitional mucosa), J Clin Pathol, 1979, 32(3):214–218.
[30] Franzin G, Grigioni WF, Dina R, Scarpa A, Zamboni G, Mucin secretion and morphological changes of the mucosa in non-neoplastic diseases of the colon, Histopathology, 1983, 7(5):707–718.
[31] Branfoot AC, Filipe MI, Letter to the Editor. Failure to demonstrate specificity of the morphological and histochemical changes in mucosa adjacent to colonic carcinoma, J Clin Pathol, 1979, 32(8):852.
[32] Filipe MI, Correspondence. ‘Transitional mucosa’, Histo-pathology, 1984, 8(4):707.
[33] Williams GT, Transitional mucosa of the large intestine, Histopathology, 1985, 9(11):1237–1243.
[34] Filipe MI, Bancroft AC, Abnormal patterns of mucus secretion in apparently normal mucosa of large intestine with carcinoma, Cancer, 1974, 34(2):262–290.
[35] Dawson PA, Patel J, Filipe MI, Variations in sialomucins in the mucosa of the large intestine in malignancy: a quantimet and statistical analysis, Histochem J, 1978, 10(5):559–572.
[36] Mughal S, Filipe MI, Histogenesis of malignant transformation
in the colonic epithelium. A detailed study on semi-thin sections, Acta Gastroenterol Belg, 1978, 41(5–6):215–225.
[37] Rogers CM, Cooke KB, Filipe MI, Sialic acids of human large bowel mucosa: o-acylated variants in normal and malignant states, Gut, 1978, 19(7):587–592.
[38] Shamsuddin AK, Mucinous colloid adenocarcinoma of colon in Fischer-344 rats. Light microscopy, histochemistry and ultrastructure, J Submicrosc Cytol, 1984, 16(4):697–704.
[39] Listinsky CM, Riddell RH, Patterns of mucin secretion in neoplastic and non-neoplastic diseases of the colon, Hum Pathol, 1981, 12(10):923–929.
[40] Colacchio TA, Chabot JA, Zimmerman BW, Differential mucin staining in colorectal neoplasms. Potential clinical application, Am J Surg, 1984, 147(5):666–669.
[41] Greaves P, Filipe Mi, Abbas S, Ormerod MG, Sialomucins and carcinoembryonic antigen in the evolution of colorectal cancer, Histopathology, 1984, 8(5):825–834.
[42] Lev R, Lance P, Camara P, Histochemical and morphologic studies of mucosa bordering rectosigmoid carcinomas: comparisons with normal, diseased, and malignant colonic epithelium, Hum Pathol, 1985, 16(2):151–161.
[43] Kanemitsu Y, Kato T, Hirai T, Yasui K, Morimoto T, Shimizu Y, Kodera Y, Yamamura Y, Survival after curative resection for mucinous adenocarcinoma of the colorectum, Dis Colon Rectum, 2003, 46(2):160–167.
[44] Du W, Mah JT, Lee J, Sankila R, Sankaranarayanan R, Chia KS, Incidence and survival of mucinous adeno-carcinoma of the colorectum: a population-based study from an Asian country, Dis Colon Rectum, 2004, 47(1):78–85.
[45] Longo R, Morabito A, Carillio G, Lanzi G, Castellana MA, Amici S, Fanelli M, Gattuso D, Multiorganic dissemination of a colorectal signet ring cell carcinoma with fulminant clinical course, Int J Gastrointest Cancer, 2006, 37(1):49–54.
[46] Song W, Wu SJ, He YL, Cai SR, Zhang CH, Zhang XH, Zhan WH, Clinicopathologic features and survival of patients with colorectal mucinous, signet-ring cell or non-mucinous adenocarcinoma: experience at an institution in southern China, Chin Med J (Engl), 2009, 122(13):1486–1491.
[47] Sugarbaker PH, Mucinous colorectal carcinoma, J Surg Oncol, 2001, 77(4):282–283.

M. Ionilă et al.
790
[48] Goi T, Obata S, Inoue T, Fujioka M, Hirono Y, Katayama K, Yamaguchi A, Clinicopathological study of the colorectal mucinous carcinomas, Int Surg, 2006, 91(6):352–357.
[49] Chen JS, Hsieh PS, Chiang JM, Yeh CY, Tsai WS, Tang R, Changchien CR, Wu RC, Clinical outcome of signet ring cell carcinoma and mucinous adenocarcinoma of the colon, Chang Gung Med J, 2010, 33(1):51–57.
Corresponding author Claudiu Mărgăritescu, Associate Professor, MD, PhD, Department of Pathology, Faculty of Dentistry, University of Medicine and Pharmacy of Craiova, 2–4 Petru Rareş Street, 200349 Craiova, Romania; Phone +40740–152 550, e-mail: [email protected] Received: June 10th, 2011
Accepted: August 15th, 2011


















