MSK & Orthopaedic Quality Drive Programme Philip Lunts Head of Service Improvement Executive Lead...
12
MSK & Orthopaedic Quality Drive Programme Philip Lunts Head of Service Improvement Executive Lead for Programme Ali Mehdi Head of Orthopaedic Service Clinical Lead for Programme
-
Upload
meredith-hopkins -
Category
Documents
-
view
215 -
download
0
Transcript of MSK & Orthopaedic Quality Drive Programme Philip Lunts Head of Service Improvement Executive Lead...

MSK & Orthopaedic Quality Drive Programme
Philip LuntsHead of Service Improvement
Executive Lead for Programme
Ali MehdiHead of Orthopaedic
ServiceClinical Lead for
Programme
The two work-strands from the MSK Project that have had the greatest impact for Borders Patients:
• Work-strand 4: Hip fracture care pathway
• Work-strand 5: Demand & Capacity Modelling (DCAQ)

Work-strand 4: Hip #Clinical Leads: Drs Antrobus & Bennison
1.Frail Elderly Care bundle within acute care
• Plan: to trial use of daily “single question in delirium” (SQID)
• Aim: the earlier identification of patients who have developed delirium during their hospital admission.
• This allows for earlier investigation and treatment of delirium, leading to improved patient experience, reduced symptoms and complications and shorter hospital length of stay
• Method: Nursing staff place “SQID” sticker in notes daily and answer question “Is this person more confused than yesterday”. All patients over the age of 65 should be included.
• If answer is “Yes” – nursing staff inform the ward medical staff. Medical staff then carry out AMT / 4AT / start delirium bundle as appropriate

1. Care bundle: Frail Elderly
Comprehensive Geriatric Assessment
Medication review / analgesia
Avoid / treat delirium
Refer all patients for geriatric assessment on admission
Refer to “blue sheet” / UPR for geriatrician management plan
All patients mobilized day of surgery to chair
All patients reviewed by physiotherapist by day 1 post opo Mobility / balance / gait / falls risk
OT assessment starts day 1 post admission.
Social work input as required Complete nutritional / pressure area
assessment on admission
Analgesia as per preop. bundle.oGive regularlyoReview regularly
Review all medications as per polypharmacy protocol:
oValid indication?oSymptomatic relief?oVital hormone replacement?oHigh risk combination?oPoorly tolerated?oNNT for benefit vs risks
Document reasons for changes in UPREnsure appropriate VTE prophylaxis prescribed
Complete AMT and 4AT on admissionDaily SQiD
o“Is this patient more confused than yesterday”?
Start delirium bundle when identified (sticker)Identify and treat causesReorientate patient regularlyEncourage mobilityCheck hearing aids / spectaclesAvoid constipationMaintain sleep pattern / fluid intakeProvide carers with delirium leaflet / explanationDo not
oCatheterizeoSedate routinely / restrainoArgue with the patient
Reduce falls risk Assess bone health Plan dischargeOn admission
oTake accurate falls history including risk factorsoComplete nursing admission falls assessment
Take action to reduce identified risksComplete active standTreat postural hypotension if present
oIncrease oral fluidsoTEDSoReview medication
Document visual acuityDocument AMT / 4ATIf urinary incontinence present:
oMSUoPost void bladder scanoBladder chart
Prescribe and give vitamin D stat dose – colecalciferol 100,000 units orally
o**check if peanut allergy**If patient is over 80 years old start bone protection:
oCalcium and vitamin D / alendronateoRefer osteoporosis service if contraindications (eg renal impairment)
If under 80 years old request DEXA scanComplete bone health risk factor checklist (on “blue sheet”)
oIf high risk start bone protection whilst results awaitedoIf low risk await DEXA result before starting treatment
Set EDD on admissionInform patient and carers of date and any changes to this during admissionRefer to PT / OT on admissionRefer to social work as soon as need identifiedAfter first DME review
oUpdate EDD and anticipated place of dischargeoPlace patient on community waiting list if appropriate
All patients discussed at daily MDT board round (update plan / EDD)Day before
oEnsure IDL completedoBook transportoEnsure equipment / care ready
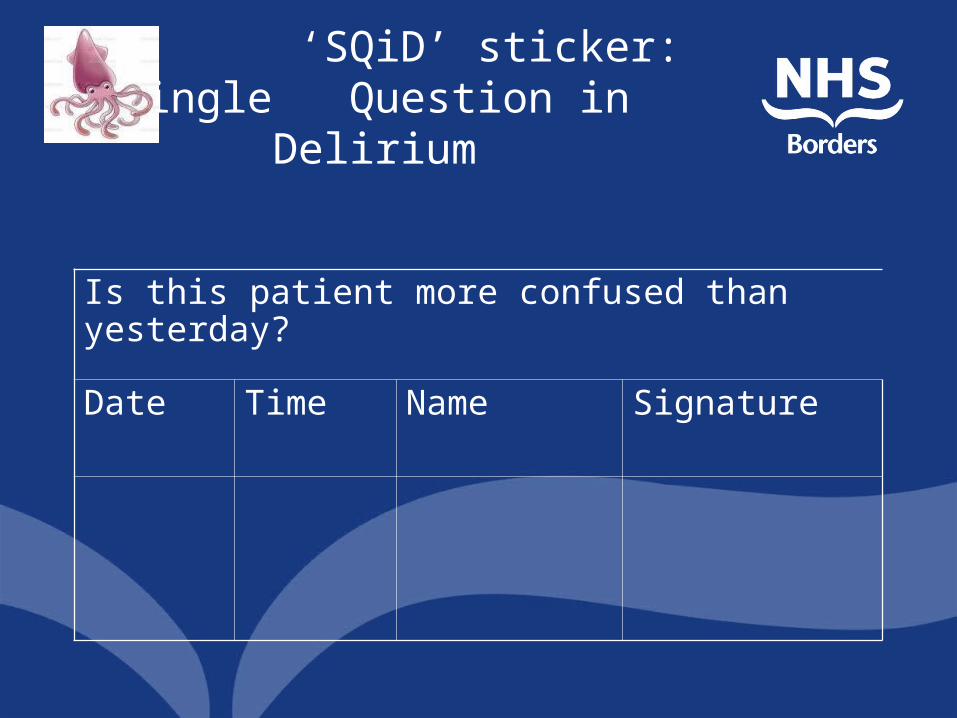
‘SQiD’ sticker: Single Question in Delirium
Is this patient more confused than yesterday?
Date Time Name Signature

2. Care bundle: anaesthetic
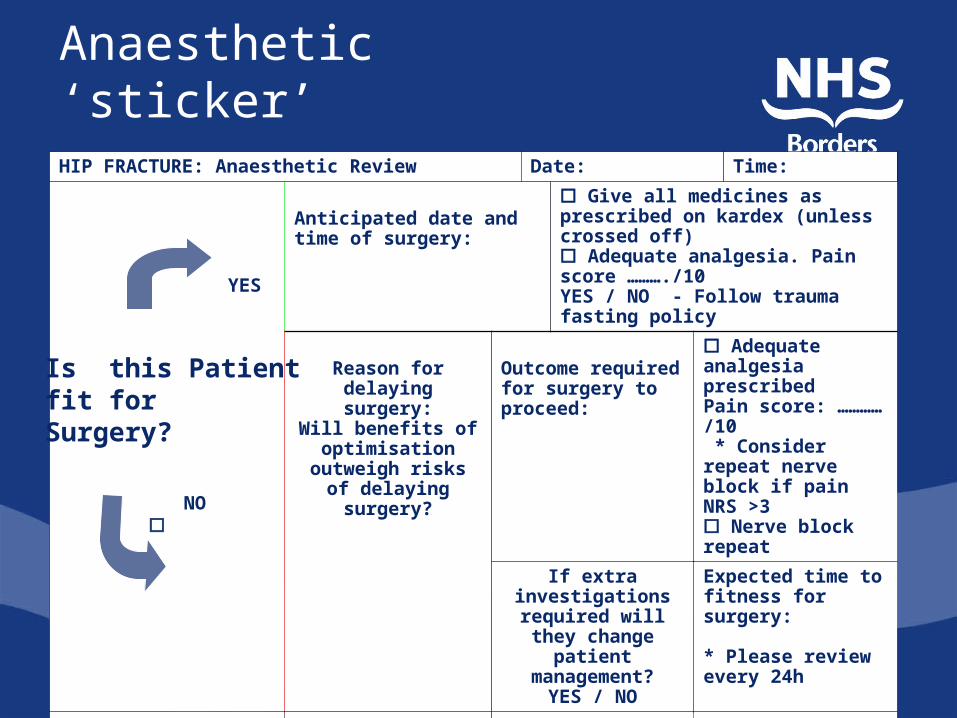
Anaesthetic ‘sticker’
YES
IS PATIENT FIT FOR
SURGERY?
HIP FRACTURE: Anaesthetic Review Date: Time:
Anticipated date and time of surgery:
Give all medicines as prescribed on kardex (unless crossed off) Adequate analgesia. Pain score ………./10YES / NO - Follow trauma fasting policy
Reason for delaying surgery:
Will benefits of optimisation
outweigh risks of delaying surgery?
Outcome required for surgery to proceed:
Adequate analgesia prescribedPain score: ………… /10 * Consider repeat nerve block if pain NRS >3 Nerve block repeat
If extra investigations
required will they change patient management?
YES / NO
Expected time to fitness for surgery:
* Please review every 24h
Signed: Print name:
NO
YES
Is this Patient fit for Surgery?

Using Demand and Capacity• Established predicted demand and capacity
required• Developed ongoing DCAQ modelling tool – updated
weekly• Weekly ‘huddle’ – all ortho consultants plus
booking managers - review– last week actual against predicted (and reasons)– Last week theatre start times– This week planned against required– Outpatient clinic actual against predicted (NEW!)
Impact• Excellent engagement with clinicians• Shared ownership and solution of
problems • competition – gold star of the week!
Next Steps•Establish similar process for OPD•Model demand from OPD vs capacity in real-time

Virtual Fracture Clinic
•Virtual Trauma Meeting set up – avoids need for additional staffing for service•Direct Discharge recently commenced. Direct discharge of: Paediatric Clavicle
5th Metacarpal5th MetatarsalMallet fingerRadial headTorus/buckle Ankle injury
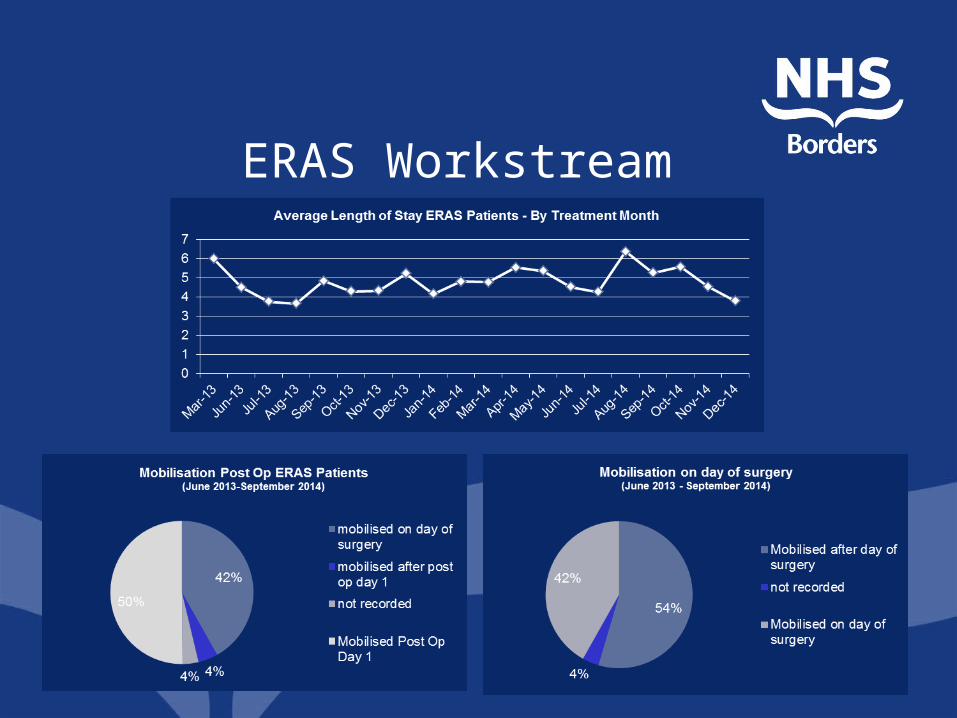
ERAS Workstream