MSFSPAIN Simplified and Expanded Admission Criteria in Upper Nile, South Sudan: MSF’s experience.
20
MSFSPAIN Simplified and Expanded Admission Criteria in Upper Nile, South Sudan: MSF’s experience
-
Upload
daisy-summers -
Category
Documents
-
view
233 -
download
3
Transcript of MSFSPAIN Simplified and Expanded Admission Criteria in Upper Nile, South Sudan: MSF’s experience.

MSFSPAIN
Simplified and Expanded Admission Criteria in Upper Nile, South Sudan: MSF’s experience

Structure of the session
1. Why only MUAC for admission and discharge2. MSF Nutrition simplified and expanded
protocol3. Kodok project , outcomes and challenges4. Conclusions/Discussion
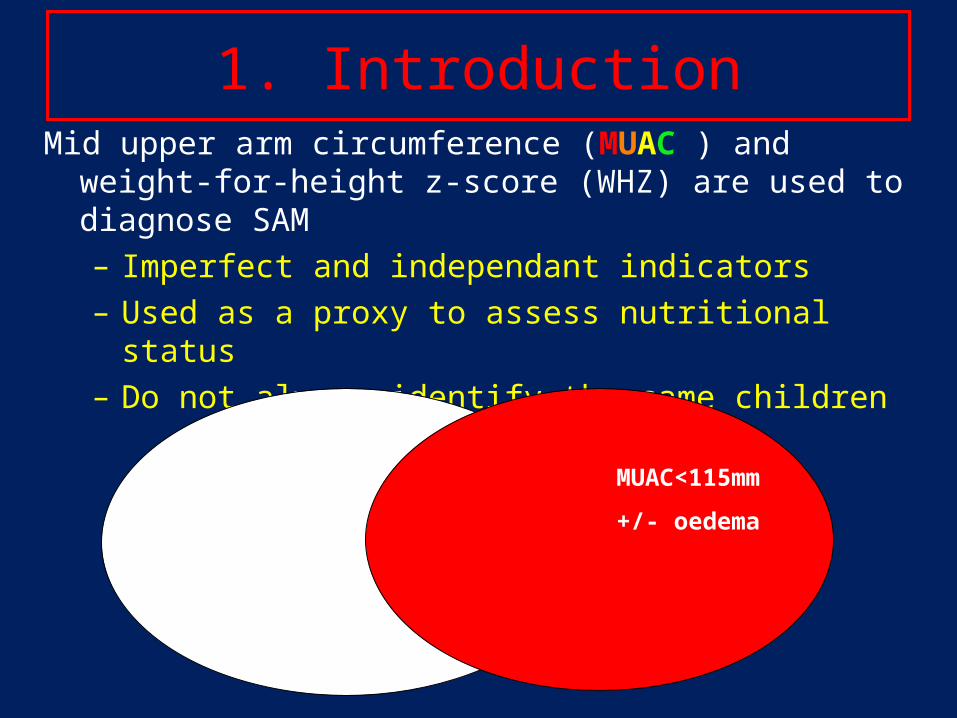
1. IntroductionMid upper arm circumference (MUAC ) and weight-for-height z-
score (WHZ) are used to diagnose SAM– Imperfect and independant indicators – Used as a proxy to assess nutritional status– Do not always identify the same children
W/H <-3 SD
+/- oedema
MUAC<115mm
+/- oedema

Low MUAC vs low WHZ
• MUAC and WHZ do not identify the same children
• WHZ is influenced by body shape and proportions: Regional effect– WHZ seems
• Overestimate malnutrition in long-limbed population• Underestimate malnutrition in short-limbed population
This is likely to alter the link between WHZ and survival.

MUAC the best index to assess the risk of death
• Age Effect
– MUAC grows continuously with age, and when a fixed cut-off is used for identifying SAM children, more young children are selected than with an index adjusted for height such as WHZ.
– As younger children have a higher mortality, this improves the selection of a high risk group.
• Muscle mass relationship
– Survival is linked to fat stores during starvation and muscle mass during infections Link MUAC and survival
• Cahill GF Jr (2006) Fuel metabolism in starvation. Annu. Rev. Nutr. 26,1-22. • Heymsfield SB, McManus C, Stevens V, et al. (1982) Muscle mass: reliable indicator of protein-energy malnutrition severity and outcome. Am. J. Clin. Nutr.35, 1192-1199.
Andre Briend – Use MUAC for severe acute malnutrition

MUAC the best index to assess the risk of death
•Neither MUAC nor WHZ reveal themselves to be ideal predictors of mortality.•MUAC appears to show consistently better predictive power. MUAC is the best anthropometric predictor of mortality currently available.•The use of both WFH and MUAC together does not appear to increase the predictive power over MUAC alone.
Tamsin Walters (ENN) and Victoria Sibson (SCUK)

MSF Holland in BentiuRetrospective analyses 2012
-MUAC < 115mm would comprise 25.8% of the case load -MUAC ≤120mm would cover 53.2 % of the case load-MUAC < 125mm would include 81.1% of case load
MUAC < 115: 25,8%
MUAC < 120: 53,2%
MUAC < 125: 81,1%

WHY ONLY MUAC FOR ADMISSION
• Faster and easier to use than WHZ in emergencies
• Better detection of younger children at high risk of death
• Facilitates coverage• More adapted to community

WHY ONLY MUAC FOR DISCHARGE
• Easier to use than WHZ in CMAM• Avoid to discharge children who are still
malnourished (compared to 15% weight gain old criteria)

WHO RECOMMENDATIOINS
• WHO Nutrition Expert Advisory Group (NUGAG) guideline recommends in 2013
• Per cent weight gain should no longer be used as a discharge criterion in nutrition programs
• Children admitted under one criterion are discharged under that same criterion

Followed up of MUAC gain in Burkina Faso program (2007 – 2011)
It is possible to use MUAC as criterion for identification of cases, their follow up and discharge
Goossens S, Bekele Y, Yun O, Harczi G, Ouannes M, et al. (2012) Mid-Upper Arm Circumference Based Nutrition Programming: Evidence for a New Approach in Regions with High Burden of Acute Malnutrition. PLoS ONE 7(11): e49320. doi:10.1371/journal.pone.0049320
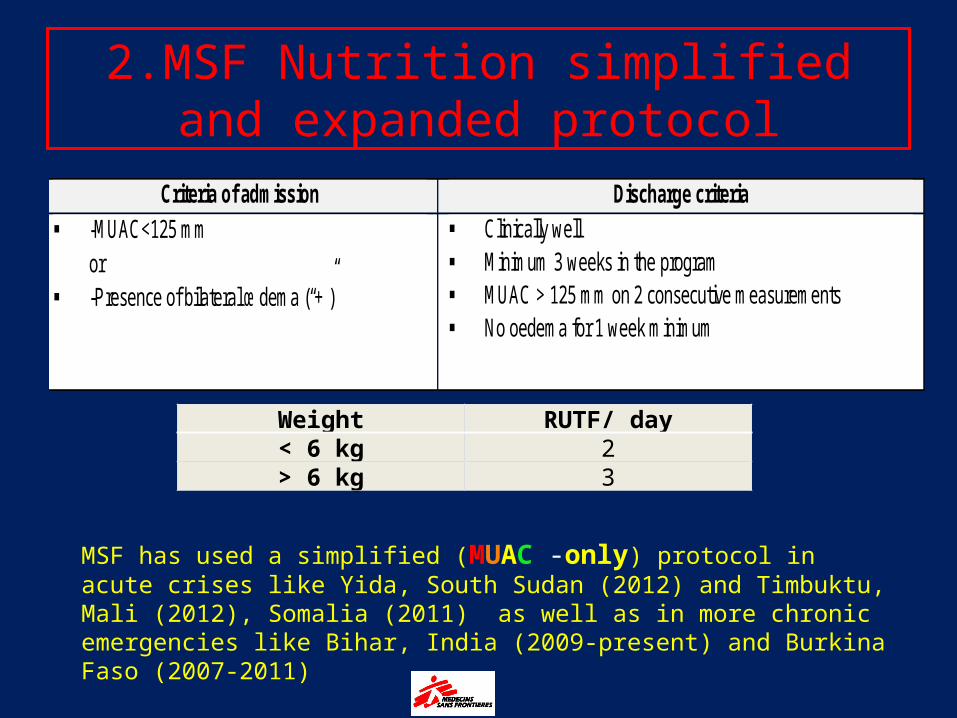
2.MSF Nutrition simplified and expanded protocol
Weight RUTF/ day< 6 kg 2> 6 kg 3
Criteria of admission Discharge criteria
-MUAC<125 mm or
-Presence of bilateral œdema (“+”)
Clinically well Minimum 3 weeks in the program MUAC > 125 mm on 2 consecutive measurements No oedema for 1 week minimum
MSF has used a simplified (MUAC -only) protocol in acute crises like Yida, South Sudan (2012) and Timbuktu, Mali (2012), Somalia (2011) as well as in more chronic emergencies like Bihar, India (2009-present) and Burkina Faso (2007-2011)
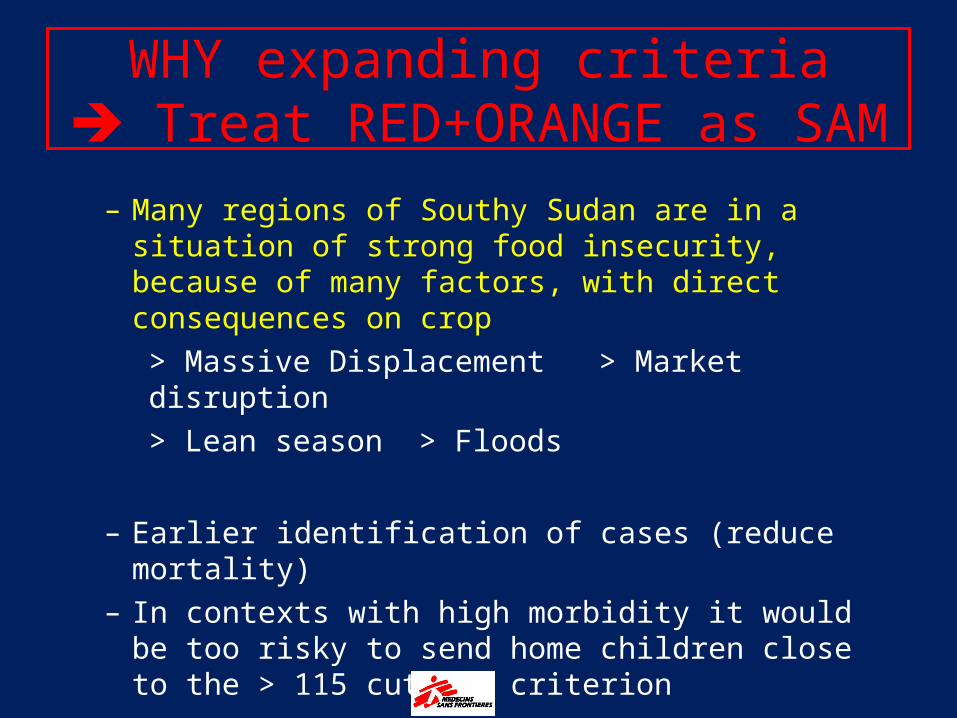
– Many regions of Southy Sudan are in a situation of strong food insecurity, because of many factors, with direct consequences on crop
> Massive Displacement > Market disruption> Lean season > Floods
– Earlier identification of cases (reduce mortality)– In contexts with high morbidity it would be too risky to
send home children close to the > 115 cut off criterion
WHY expanding criteria Treat RED+ORANGE as SAM

Food insecurity
Upper Nile 332.500 481.600 97.900
IPC outlook toAugust 2014
Food Insecurity FSMS Report April 2014

FOOD INSECURITY DEPLACEMENTS 03-04/2014
Food Insecurity FSMS Report April 2014
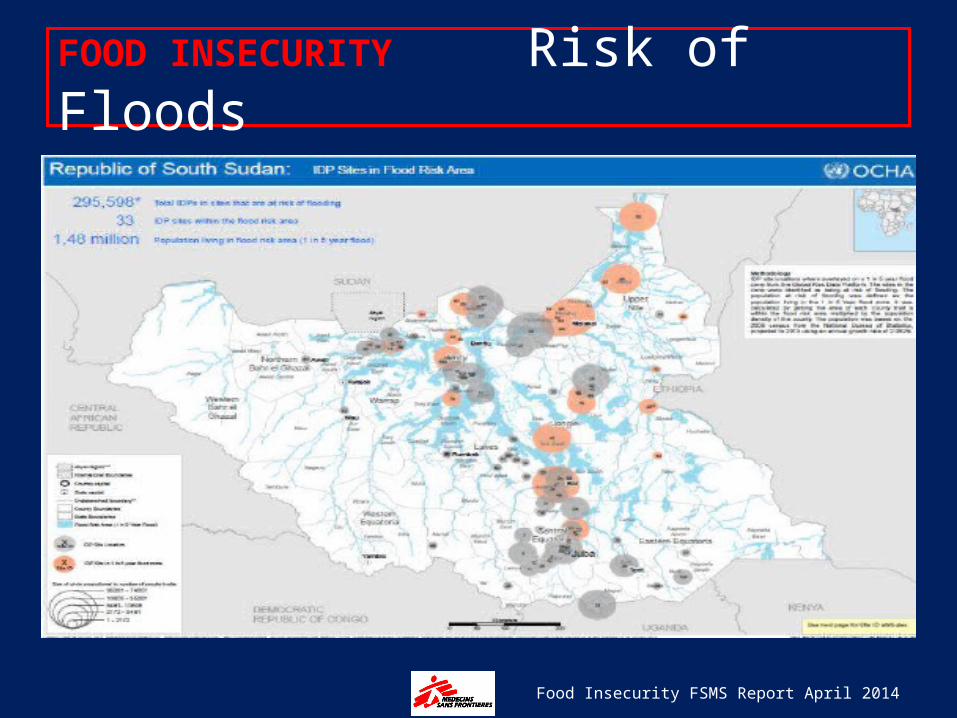
FOOD INSECURITY Risk of Floods
Food Insecurity FSMS Report April 2014

3. KODOK PROJECT
POPULATION
• KODOK 20.000 - 30.000• LUL 10.000 - 15.000• WAU SCHILUK 40.000 - 50.000

LUL KODOK
WAU SCHILUK Admissions 2.206Discharge 1.333Cured 45%Defaulters 54%Deaths 1%
KODOK PROJECT

• CHALLENGES
– Reinforcement of activities at Community level (recruitment of 50 CHW)
– In Wao Schilluk • from 2 to 6 days/week ATFC
KODOK PROJECT
4. DISCUSSION• Use of MUAC as single criteria of admission and/or discharge:
– Benefit/Risks– Costs– Which concrete implications for different stakeholders?
• MoH• NGOs• UN agencies
• Which is the best MUAC cut off for admission and discharge? – 120 vs 125? According to context