
MRI signal intensity based B-Spline nonrigid registration for pre- and intraoperative imaging during...
7
Original Research MRI Signal Intensity Based B-Spline Nonrigid Registration for Pre- and Intraoperative Imaging During Prostate Brachytherapy Sota Oguro, MD, 1,2 Junichi Tokuda, PhD, 1 Haytham Elhawary, PhD, 1 Steven Haker, PhD, 1 Ron Kikinis, MD, 1 Clare M.C. Tempany, MD, 1 and Nobuhiko Hata, PhD 1 * Purpose: To apply an intensity-based nonrigid registra- tion algorithm to MRI-guided prostate brachytherapy clin- ical data and to assess its accuracy. Materials and Methods: A nonrigid registration of preop- erative MRI to intraoperative MRI images was carried out in 16 cases using a Basis-Spline algorithm in a retrospec- tive manner. The registration was assessed qualitatively by experts’ visual inspection and quantitatively by meas- uring the Dice similarity coefficient (DSC) for total gland (TG), central gland (CG), and peripheral zone (PZ), the mutual information (MI) metric, and the fiducial registra- tion error (FRE) between corresponding anatomical land- marks for both the nonrigid and a rigid registration method. Results: All 16 cases were successfully registered in less than 5 min. After the nonrigid registration, DSC values for TG, CG, PZ were 0.91, 0.89, 0.79, respectively, the MI metric was 0.19 6 0.07 and FRE presented a value of 2.3 6 1.8 mm. All the metrics were significantly better than in the case of rigid registration, as determined by one-sided t-tests. Conclusion: The intensity-based nonrigid registration method using clinical data was demonstrated to be feasible and showed statistically improved metrics when compare to only rigid registration. The method is a valuable tool to integrate pre- and intraoperative images for brachytherapy. Key Words: prostate brachytherapy; signal intensity- based nonrigid registration; B-Spline J. Magn. Reson. Imaging 2009;30:1052–1058. V C 2009 Wiley-Liss, Inc. MRI-GUIDED BRACHYTHERAPY is a method to treat localized prostate cancer (1–3). It enables treatment planning on site through its delineation of prostate substructures and surrounding tissue, especially when using an endorectal (ER) coil. D’Amico et al and Landis et al demonstrated the feasibility of this approach by performing 248 cases of MRI-guided prostate brachytherapy using a 0.5 Tesla (T) open- configuration MRI scanner, and comparing the clinical outcomes with other forms of brachytherapy (4,5). Their study reported that MR-guided prostate brachy- therapy presented fewer complications and a better quality of life than when using ultrasound for image guidance. One of the drawbacks of the MR-guided procedure, however, is that the open-configuration 0.5T scanner had significantly lower field strength and less gradient performance than standard high- field scanner cylindrical magnets, resulting in a lower signal-to-noise ratio and low contrast and resolution. Image registration between preoperative MRI obtained in a high-field scanner and intraoperative images used for guidance in the open magnet can help con- tribute information from the diagnostic scan into the procedure (6). Once registration is performed at the beginning of the procedure, the fused image is useful to better comprehend the prostate substructures and suspi- cious foci that would otherwise be more difficult to detect using intraoperative MRI alone. Hirose et al found that a significant prostate shape change occurred between preoperative 1.5T ER coil images and intraoperative 0.5T imaging due to postural change from a supine to lithotomy position and the absence of an ER coil at 0.5T. In particular, in the preoperative images, the prostate gland appeared to have a smaller anterior–posterior dimension and wider transverse dimension than in the intraoperative images. Furthermore, the shape change of the periph- eral zone was greater than that of the central gland between pre- and intraoperative images (7). Nonrigid registration, as opposed to rigid registra- tion is, therefore, necessary to compensate for the deformation of the prostate between pre- and intra- operative imaging. Bharatha et al reported nonrigid 1 Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA. 2 Department of Diagnostic Radiology, Keio University School of Medicine, Shinjuku-ku, Tokyo, Japan. Contract grant sponsor: NIH; Contract grant numbers: 5U41RR019703, 5P01CA067165, 1R01CA111288, 5U54EB005149, 5R01CA109246, 3P41RR013218. Part of this study was funded by Intelligent Surgical Instruments Project of METI, Japan. *Address reprint requests to: N.H., Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, 75 Francis Street Boston, MA 02115. E-mail: [email protected] Received March 31, 2009; Accepted August 13, 2009. DOI 10.1002/jmri.21955 Published online in Wiley InterScience (www.interscience.wiley.com). JOURNAL OF MAGNETIC RESONANCE IMAGING 30:1052–1058 (2009) V C 2009 Wiley-Liss, Inc. 1052
-
Upload
sota-oguro -
Category
Documents
-
view
212 -
download
0
Transcript of MRI signal intensity based B-Spline nonrigid registration for pre- and intraoperative imaging during...

Original Research
MRI Signal Intensity Based B-Spline NonrigidRegistration for Pre- and Intraoperative ImagingDuring Prostate Brachytherapy
Sota Oguro, MD,1,2 Junichi Tokuda, PhD,1 Haytham Elhawary, PhD,1 Steven Haker, PhD,1
Ron Kikinis, MD,1 Clare M.C. Tempany, MD,1 and Nobuhiko Hata, PhD1*
Purpose: To apply an intensity-based nonrigid registra-tion algorithm to MRI-guided prostate brachytherapy clin-ical data and to assess its accuracy.
Materials and Methods: A nonrigid registration of preop-erative MRI to intraoperative MRI images was carried outin 16 cases using a Basis-Spline algorithm in a retrospec-tive manner. The registration was assessed qualitativelyby experts’ visual inspection and quantitatively by meas-uring the Dice similarity coefficient (DSC) for total gland(TG), central gland (CG), and peripheral zone (PZ), themutual information (MI) metric, and the fiducial registra-tion error (FRE) between corresponding anatomical land-marks for both the nonrigid and a rigid registrationmethod.
Results: All 16 cases were successfully registered in lessthan 5 min. After the nonrigid registration, DSC valuesfor TG, CG, PZ were 0.91, 0.89, 0.79, respectively, the MImetric was �0.19 6 0.07 and FRE presented a value of2.3 6 1.8 mm. All the metrics were significantly betterthan in the case of rigid registration, as determined byone-sided t-tests.
Conclusion: The intensity-based nonrigid registrationmethod using clinical data was demonstrated to be feasibleand showed statistically improved metrics when compareto only rigid registration. The method is a valuable tool tointegrate pre- and intraoperative images for brachytherapy.
Key Words: prostate brachytherapy; signal intensity-based nonrigid registration; B-SplineJ. Magn. Reson. Imaging 2009;30:1052–1058.VC 2009 Wiley-Liss, Inc.
MRI-GUIDED BRACHYTHERAPY is a method to treatlocalized prostate cancer (1–3). It enables treatmentplanning on site through its delineation of prostatesubstructures and surrounding tissue, especiallywhen using an endorectal (ER) coil. D’Amico et al andLandis et al demonstrated the feasibility of thisapproach by performing 248 cases of MRI-guidedprostate brachytherapy using a 0.5 Tesla (T) open-configuration MRI scanner, and comparing the clinicaloutcomes with other forms of brachytherapy (4,5).Their study reported that MR-guided prostate brachy-therapy presented fewer complications and a betterquality of life than when using ultrasound for imageguidance. One of the drawbacks of the MR-guidedprocedure, however, is that the open-configuration0.5T scanner had significantly lower field strengthand less gradient performance than standard high-field scanner cylindrical magnets, resulting in a lowersignal-to-noise ratio and low contrast and resolution.Image registration between preoperative MRI obtainedin a high-field scanner and intraoperative imagesused for guidance in the open magnet can help con-tribute information from the diagnostic scan into theprocedure (6).
Once registration is performed at the beginning ofthe procedure, the fused image is useful to bettercomprehend the prostate substructures and suspi-cious foci that would otherwise be more difficult todetect using intraoperative MRI alone. Hirose et alfound that a significant prostate shape changeoccurred between preoperative 1.5T ER coil imagesand intraoperative 0.5T imaging due to posturalchange from a supine to lithotomy position and theabsence of an ER coil at 0.5T. In particular, in thepreoperative images, the prostate gland appeared tohave a smaller anterior–posterior dimension andwider transverse dimension than in the intraoperativeimages. Furthermore, the shape change of the periph-eral zone was greater than that of the central glandbetween pre- and intraoperative images (7).
Nonrigid registration, as opposed to rigid registra-tion is, therefore, necessary to compensate for thedeformation of the prostate between pre- and intra-operative imaging. Bharatha et al reported nonrigid
1Department of Radiology, Brigham and Women’s Hospital, HarvardMedical School, Boston, Massachusetts, USA.2Department of Diagnostic Radiology, Keio University School ofMedicine, Shinjuku-ku, Tokyo, Japan.
Contract grant sponsor: NIH; Contract grant numbers:5U41RR019703, 5P01CA067165, 1R01CA111288, 5U54EB005149,5R01CA109246, 3P41RR013218. Part of this study was funded byIntelligent Surgical Instruments Project of METI, Japan.
*Address reprint requests to: N.H., Department of Radiology, Brighamand Women’s Hospital, Harvard Medical School, 75 Francis StreetBoston, MA 02115. E-mail: [email protected]
Received March 31, 2009; Accepted August 13, 2009.
DOI 10.1002/jmri.21955Published online in Wiley InterScience (www.interscience.wiley.com).
JOURNAL OF MAGNETIC RESONANCE IMAGING 30:1052–1058 (2009)
VC 2009 Wiley-Liss, Inc. 1052

registration of ER coil-based 1.5T preoperative MRIwith 0.5T intraoperative images using segmented datasets. The results from this study indicated that themethod was feasible and significantly improved theaccuracy of registration when compared to its rigidcounterpart (8,9). The method, however, requiresmanual segmentation of the prostate as a preprocess-ing step, which can introduce intra- and interobservervariability. Furthermore, the manual segmentationstep considerably prolongs the registration process,which impacts the procedure time of the brachyther-apy intervention. Intensity-based nonrigid registrationwhich does not require manual segmentation wouldallow the mapping of high-resolution images to theintraoperative ones in less time. In response to thisneed, Wang et al used such an approach to effectivelytrack anatomical variations within CT images (10).While intensity-based registration was documented inthis study, the method was tested in phantom trialsand only a few clinical data sets, and was not testedfor MR images.
Our objective is to test and validate the feasibility ofintensity-based nonrigid registration between preoper-ative MRI and intraoperative MRI obtained duringMRI-guided brachytherapy of the prostate. Specifi-cally, we tested the accuracy of the intensity-basedregistration method using a 1.5T preoperative MRItaken with an ER coil and a 0.5T intraoperative MRItaken without the ER coil.
MATERIALS AND METHODS
Patient Selection and Imaging Protocols
This study included 16 men (mean age, 63.4 years;range, 54 to 72 years) who were randomly selectedfrom MRI-guided prostate brachytherapy proceduresperformed at our institution between December 1998and August 2002. Informed consent was obtained ineach case after description of the nature of the proce-dures. The entry criteria for patients into the MRI-guided brachytherapy program at the institution hasbeen described elsewhere (1). All patients underwentpreoperative 1.5T MRI using an ER coil with integrated
pelvic phased multi-coil array (Signa LX, GE Health-care, Milwaukee, WI). The ER coil was a receive-onlycoil mounted inside a latex balloon with a diameter of4–6 cm when inflated inside the patient’s rectum. Thepatients were placed in the supine position in theclosed-bore magnet for the imaging examination thatincluded T2-weighted fast spin echo (FSE) images (rep-etition time/echo time [TR/TE] of 4050/135 ms; fieldof view of 12 cm, section thickness of 0.3 cm, sectiongap of 0 cm, matrix of 256 � 256, 3 signal averages).Typical acquisition times were 5–6 min.
Intraoperative imaging was performed in the open-configuration 0.5T MR scanner (Signa SP, GE Health-care, Milwaukee, WI) (11). Each patient was placed inthe lithotomy position to facilitate prostate brachy-therapy by means of a perineal template. The tem-plate was fixed in place by a rectal obturator (2-cm di-ameter). T2-weighted FSE images (TR/TE 6400/100ms, field of view of 24 cm, section thickness of 0.5cm, section gap of 0 cm, matrix 256 � 256, 2 signalaverages) were acquired in the scanner using a flexi-ble external pelvic wrap-round coil, with typical acqui-sition times of 6 min. An example of pre- and intra-operative images is presented in Figure 1.
Image Registration
We used the 3D Slicer (http://www.slicer.org/) andImageJ (http://rsbweb.nih.gov/ij/) software packagesfor image registration. Both are free open source soft-ware for visualization and image-based computing. Aspecific module for 3D Slicer has been developed toautomate the process of rigid and then nonrigid regis-tration of image data sets. A rigid registration stepwas necessary before applying nonrigid registration,to center the pre- and intraoperative image seriesaround the prostate.
The nonrigid registration was done using a B-Splinemethod, a well-known nonrigid registration method(12). This method works by placing a uniformly spacedthree dimensional (3D) grid over the volume to be regis-tered, the lattice points of which act as control pointsfor the displacement of tissue. Displacement of each
Figure 1. a,b: An example ofpreoperative axial T2-weightedimage using an endorectal coilin a 1.5T closed bore scanner(a), and intraoperative axialT2-weighted image in a low-field 0.5T interventional scan-ner (b).
Intensity-Based Nonrigid Registration 1053

control point results in a deformation of the region sur-rounding the point, in a way that makes the overall de-formation as smooth as possible. The displacement iseasily calculated using cubic polynomials. For ourapplication, we used a lattice with 5 � 5 � 5 controlpoints. For our 3D application, this allowed for 125 � 3¼ 375 degrees of freedom in the determination of the B-Spline registration. This choice in the number of con-trol points was made based on experimenting with trialcases; we found that a 5 � 5 � 5 grid provided a reason-able amount of control and acceptable processing time.To guide the registration, a measure of image similaritybased on mutual information (MI) was used (13). Infor-mally, this similarity measure is maximized when theinformation in one image volume ‘‘best explains’’ the in-formation content of the other. This measure has a pre-cise meaning within the field of information theory. TheB-Spline registration algorithm thus adjusts the con-trol points until the resulting deformation aligns theimage volumes in a way that maximizes the informa-tion–theoretic similarity between them.
The registration method involved the followingsteps: (i) both images were cropped for size using theImageJ software to make the field of view the same oneach image, (ii) the 1.5T preoperative images were rig-idly registered with the 0.5T intraoperative imagesusing the corresponding function in 3D Slicer, and(iii) the 1.5T images were nonrigidly registered withthe 0.5T images using the nonrigid B-Spline registra-tion module in 3D Slicer. We then measured therequired processing time and core computation timefor the registration procedure.
Accuracy Assessment
The volume of the prostate gland in the preoperativeMRI was measured using 3D Slicer and the distribu-tion of the prostate volume was compared with similarstudies previously reported in the literature (14–16).
Evaluating the accuracy of a registration method isdifficult because there is no gold standard with whichto compare it. Therefore, accuracy or validation of thenonrigid registration method was evaluated both qual-itatively and quantitatively in several different ways toinclude both local and global measures of registrationsuccess. A qualitative measure included a checker-board comparison between the registered image data-sets. Quantitative methods involved a 3D registrationerror map based on contour alignment between data-sets using Hausdorff distance (HD). We also obtainedthe Dice similarity coefficient (DSC) between the seg-mented registered prostate images, measured the MIvalue of the images before and after registration, andfinally calculated fiducial registration error (FRE)among common anatomical landmarks.
The registered images from the two data sets weremerged for comparison in a checkerboard pattern, toqualitatively evaluate the difference between the pre-and intraoperative images (17,18). The contour of thetotal gland (TG), central gland (CG), and peripheralzone (PZ) of the prostate were drawn by an experiencedradiologist (S.O.) under the supervision of a seniorradiologist (C.T.). The radiologists then assessed the
continuity of the contours of the different regions of theprostate gland in the checkerboard images.
A 3D distance map indicating the HD were createdto assess the accuracy of registration across the pros-tate gland surface, and investigate if the registeredimages correctly separate the prostate gland from thesurrounding critical structure so that the radiationdose to the gland does not damage those surroundingstructures. A similar assessment were performed inthe related study (19). The HD between two imageswere measured by extracting the edges of the seg-mented prostate from the intraoperative MR imagesand from the registered preoperative MR images andcalculating the distance from each point on the con-tour to the nearest point on the contour of the regis-tered prostate (20). Perfect alignment between con-tours will give a HD of zero at every point.
The DSC was calculated to evaluate the coincidencebetween the segmented registered preoperative pros-tate volume and the segmented intraoperative one(8,21,22). The DSC is clinically relevant to MRI-guidedbrachytherapy because the standard radiation plan inthe brachytherapy suggests higher dose on the pe-ripheral zone to avoid overdose to urethra causing uri-nary complications (23). Thus, having a correct volu-metric map of peripheral zone in the fused (registered)images, i.e. higher value in DSC, enables more accu-rate and safer dose planning in the brachytherapy.For two images with segmented volumes (voxels) S1and S2, the DSC is defined as the ratio of the volumeof their intersection to their total volume as,
DSC ¼ 2 � Volume ðS1 \ S2ÞVolume ðS1Þ þ Volume ðS2Þ
where Volume (S1) and Volume (S2) represent the vol-umes of the segmented tissue region in each image andVolume (S1\S2) is the volume of the intersectionbetween the two. The DSC has a value of 1 for perfectagreement of S1 and S2, and 0 when there is no over-lap. A DSC value greater than 0.7 has been reported toindicate good match between two regions in assessingimage segmentation (24). In our study, the DSC valueswere calculated between different substructures of theprostate in the preoperative images and those samestructures in the intraoperative images, first using onlyrigid registration and then using both rigid followed bynonrigid registration. The DSC values calculated inboth cases were quantified and compared to measureany improvement. To this end, the radiologists seg-mented TG, CG, and PZ in all images for each data set.
Calculating the MI value of the images before andafter registration gives another measure of imagealignment. In this study, we used the implementationby Mattes et al to calculate the MI values to evaluatethe similarity between the registered datasets (25,26).The MI value is negative and a smaller value indicatesbetter similarity.
The validation using FRE consists of identifyingwell-defined corresponding anatomical features onregistered images and measuring the 3D distancebetween them. The FRE is more directly linked to theaccuracy of dose planning in the substructure of the
1054 Oguro et al.
prostate. Based on a related study, it was decided toverify the registration accuracy of the urethra (27). Itis internal to the prostate, and passes through theprostate from base to apex. We selected the urethra atthe level of the verumontanum, where the ejaculatoryduct opens into the urethra (28,29). Perfect agreementcorresponds to an FRE of 0 mm. Unlike DSC, FREtells the level of accuracy in a more intuitive mannerusing the metric system, in millimeters.
Summary statistics include the mean and standarddeviation of the DSC values for TG, CG, PZ, MI, andFRE with and without nonrigid image registrationwere applied. A one-sided paired t-test was then per-formed to analyze the DSC values MI and FRE to seeif the proposed nonrigid registration method signifi-cantly improved the level of image matching betweenpre- and intraoperative images compared with rigidregistration.
In addition, a grid motion model was made to esti-mate the local deformation of the prostatic tissue dur-ing registration. A volume made of 3D grid lines wasconstructed, and then the same deformable transformcalculated in step 3 of the nonrigid registrationmethod was applied to the grid lines. Finally, thedeformed grid lines were superimposed on thedeformed preoperative image, and the anteroposterior(AP) distances of the deformed grid lines wereassessed providing a 3D deformation vector field ofthe registered prostate image.
RESULTS
Processing time for the registration, including prepro-cessing, was less than 5 min. The mean core compu-tation time for nonrigid registration in 3D Slicer was
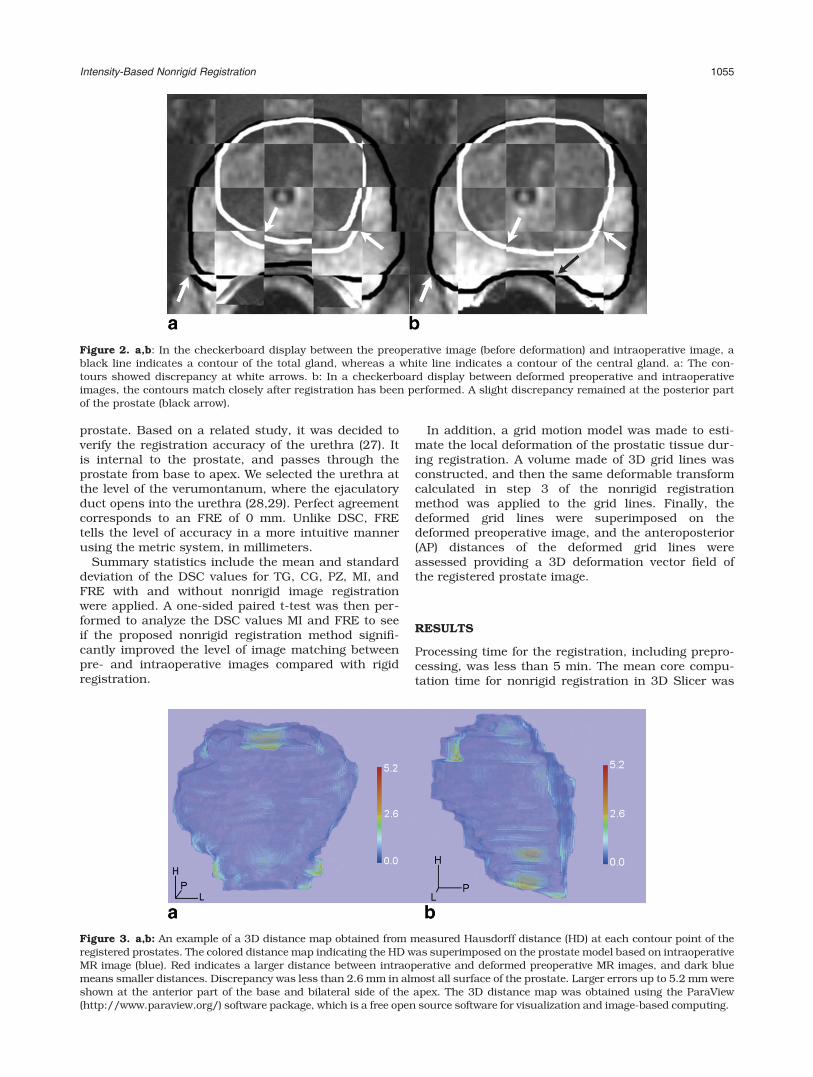
Figure 2. a,b: In the checkerboard display between the preoperative image (before deformation) and intraoperative image, ablack line indicates a contour of the total gland, whereas a white line indicates a contour of the central gland. a: The con-tours showed discrepancy at white arrows. b: In a checkerboard display between deformed preoperative and intraoperativeimages, the contours match closely after registration has been performed. A slight discrepancy remained at the posterior partof the prostate (black arrow).
Figure 3. a,b: An example of a 3D distance map obtained from measured Hausdorff distance (HD) at each contour point of theregistered prostates. The colored distance map indicating the HD was superimposed on the prostate model based on intraoperativeMR image (blue). Red indicates a larger distance between intraoperative and deformed preoperative MR images, and dark bluemeans smaller distances. Discrepancy was less than 2.6 mm in almost all surface of the prostate. Larger errors up to 5.2 mm wereshown at the anterior part of the base and bilateral side of the apex. The 3D distance map was obtained using the ParaView(http://www.paraview.org/) software package, which is a free open source software for visualization and image-based computing.
Intensity-Based Nonrigid Registration 1055
24.3 s (range, 15–51 s) on a mid-end scientific com-puter (CPU, XEON 4 � 2.8 GHz; RAM memory, 8 GB).The mean prostatic volume measured in preoperativeMRI was 40.0 mL (range, 21.0–107.5 mL), which issimilar to that found in other studies (14–16). Figure2 illustrates the checkerboard images and the pros-tate images before and after nonrigid registration wasperformed. The checkerboard display shows improvedmatching of TG, CG, and PZ structures. Figure 3shows a 3D distance map indicating the HD at eachcontour point that is a measure of the magnitude ofmisalignment of the contours of the registered pros-tates. Larger errors were shown at the anterior part ofthe base and bilateral side of the apex (Figure 3).
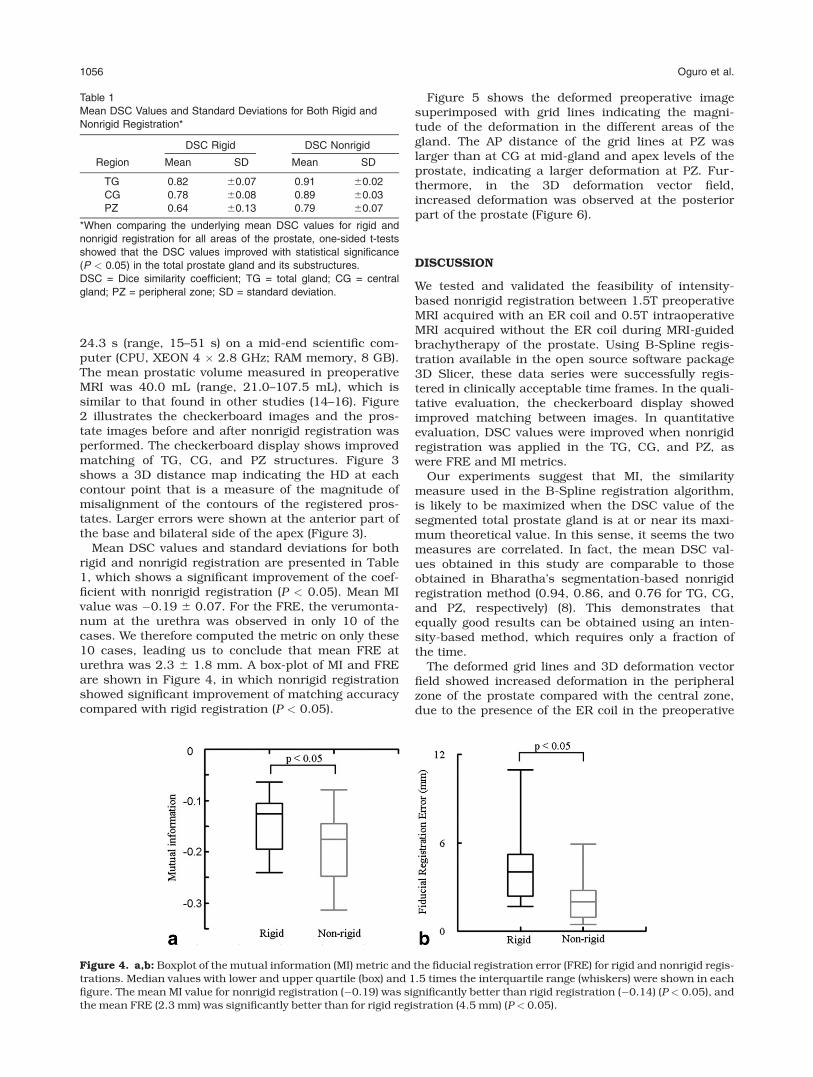
Mean DSC values and standard deviations for bothrigid and nonrigid registration are presented in Table1, which shows a significant improvement of the coef-ficient with nonrigid registration (P < 0.05). Mean MIvalue was �0.19 6 0.07. For the FRE, the verumonta-num at the urethra was observed in only 10 of thecases. We therefore computed the metric on only these10 cases, leading us to conclude that mean FRE aturethra was 2.3 6 1.8 mm. A box-plot of MI and FREare shown in Figure 4, in which nonrigid registrationshowed significant improvement of matching accuracycompared with rigid registration (P < 0.05).
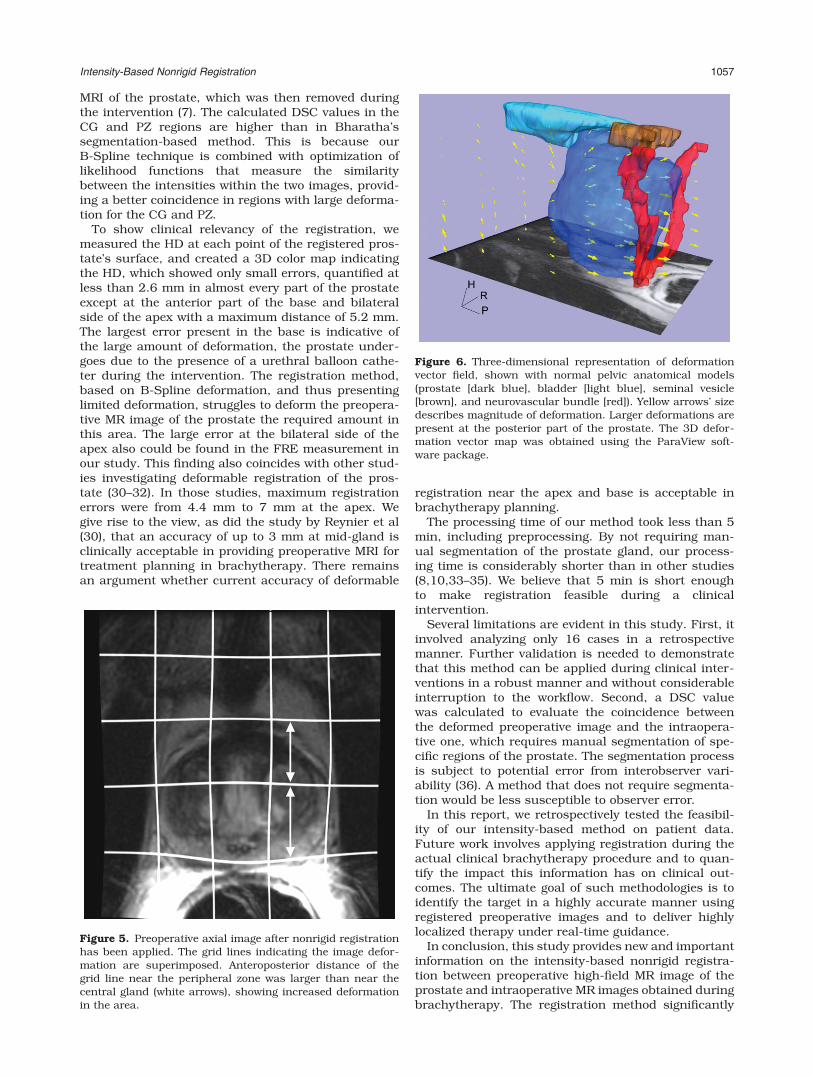
Figure 5 shows the deformed preoperative imagesuperimposed with grid lines indicating the magni-tude of the deformation in the different areas of thegland. The AP distance of the grid lines at PZ waslarger than at CG at mid-gland and apex levels of theprostate, indicating a larger deformation at PZ. Fur-thermore, in the 3D deformation vector field,increased deformation was observed at the posteriorpart of the prostate (Figure 6).
DISCUSSION
We tested and validated the feasibility of intensity-based nonrigid registration between 1.5T preoperativeMRI acquired with an ER coil and 0.5T intraoperativeMRI acquired without the ER coil during MRI-guidedbrachytherapy of the prostate. Using B-Spline regis-tration available in the open source software package3D Slicer, these data series were successfully regis-tered in clinically acceptable time frames. In the quali-tative evaluation, the checkerboard display showedimproved matching between images. In quantitativeevaluation, DSC values were improved when nonrigidregistration was applied in the TG, CG, and PZ, aswere FRE and MI metrics.
Our experiments suggest that MI, the similaritymeasure used in the B-Spline registration algorithm,is likely to be maximized when the DSC value of thesegmented total prostate gland is at or near its maxi-mum theoretical value. In this sense, it seems the twomeasures are correlated. In fact, the mean DSC val-ues obtained in this study are comparable to thoseobtained in Bharatha’s segmentation-based nonrigidregistration method (0.94, 0.86, and 0.76 for TG, CG,and PZ, respectively) (8). This demonstrates thatequally good results can be obtained using an inten-sity-based method, which requires only a fraction ofthe time.
The deformed grid lines and 3D deformation vectorfield showed increased deformation in the peripheralzone of the prostate compared with the central zone,due to the presence of the ER coil in the preoperative
Table 1
Mean DSC Values and Standard Deviations for Both Rigid and
Nonrigid Registration*
Region
DSC Rigid DSC Nonrigid
Mean SD Mean SD
TG 0.82 60.07 0.91 60.02
CG 0.78 60.08 0.89 60.03
PZ 0.64 60.13 0.79 60.07
*When comparing the underlying mean DSC values for rigid and
nonrigid registration for all areas of the prostate, one-sided t-tests
showed that the DSC values improved with statistical significance
(P < 0.05) in the total prostate gland and its substructures.
DSC = Dice similarity coefficient; TG = total gland; CG = central
gland; PZ = peripheral zone; SD = standard deviation.
Figure 4. a,b: Boxplot of the mutual information (MI) metric and the fiducial registration error (FRE) for rigid and nonrigid regis-trations. Median values with lower and upper quartile (box) and 1.5 times the interquartile range (whiskers) were shown in eachfigure. The mean MI value for nonrigid registration (�0.19) was significantly better than rigid registration (�0.14) (P < 0.05), andthe mean FRE (2.3 mm) was significantly better than for rigid registration (4.5 mm) (P < 0.05).
1056 Oguro et al.
MRI of the prostate, which was then removed duringthe intervention (7). The calculated DSC values in theCG and PZ regions are higher than in Bharatha’ssegmentation-based method. This is because ourB-Spline technique is combined with optimization oflikelihood functions that measure the similaritybetween the intensities within the two images, provid-ing a better coincidence in regions with large deforma-tion for the CG and PZ.
To show clinical relevancy of the registration, wemeasured the HD at each point of the registered pros-tate’s surface, and created a 3D color map indicatingthe HD, which showed only small errors, quantified atless than 2.6 mm in almost every part of the prostateexcept at the anterior part of the base and bilateralside of the apex with a maximum distance of 5.2 mm.The largest error present in the base is indicative ofthe large amount of deformation, the prostate under-goes due to the presence of a urethral balloon cathe-ter during the intervention. The registration method,based on B-Spline deformation, and thus presentinglimited deformation, struggles to deform the preopera-tive MR image of the prostate the required amount inthis area. The large error at the bilateral side of theapex also could be found in the FRE measurement inour study. This finding also coincides with other stud-ies investigating deformable registration of the pros-tate (30–32). In those studies, maximum registrationerrors were from 4.4 mm to 7 mm at the apex. Wegive rise to the view, as did the study by Reynier et al(30), that an accuracy of up to 3 mm at mid-gland isclinically acceptable in providing preoperative MRI fortreatment planning in brachytherapy. There remainsan argument whether current accuracy of deformable
registration near the apex and base is acceptable inbrachytherapy planning.
The processing time of our method took less than 5min, including preprocessing. By not requiring man-ual segmentation of the prostate gland, our process-ing time is considerably shorter than in other studies(8,10,33–35). We believe that 5 min is short enoughto make registration feasible during a clinicalintervention.
Several limitations are evident in this study. First, itinvolved analyzing only 16 cases in a retrospectivemanner. Further validation is needed to demonstratethat this method can be applied during clinical inter-ventions in a robust manner and without considerableinterruption to the workflow. Second, a DSC valuewas calculated to evaluate the coincidence betweenthe deformed preoperative image and the intraopera-tive one, which requires manual segmentation of spe-cific regions of the prostate. The segmentation processis subject to potential error from interobserver vari-ability (36). A method that does not require segmenta-tion would be less susceptible to observer error.
In this report, we retrospectively tested the feasibil-ity of our intensity-based method on patient data.Future work involves applying registration during theactual clinical brachytherapy procedure and to quan-tify the impact this information has on clinical out-comes. The ultimate goal of such methodologies is toidentify the target in a highly accurate manner usingregistered preoperative images and to deliver highlylocalized therapy under real-time guidance.
In conclusion, this study provides new and importantinformation on the intensity-based nonrigid registra-tion between preoperative high-field MR image of theprostate and intraoperative MR images obtained duringbrachytherapy. The registration method significantly
Figure 5. Preoperative axial image after nonrigid registrationhas been applied. The grid lines indicating the image defor-mation are superimposed. Anteroposterior distance of thegrid line near the peripheral zone was larger than near thecentral gland (white arrows), showing increased deformationin the area.
Figure 6. Three-dimensional representation of deformationvector field, shown with normal pelvic anatomical models(prostate [dark blue], bladder [light blue], seminal vesicle[brown], and neurovascular bundle [red]). Yellow arrows’ sizedescribes magnitude of deformation. Larger deformations arepresent at the posterior part of the prostate. The 3D defor-mation vector map was obtained using the ParaView soft-ware package.
Intensity-Based Nonrigid Registration 1057

improved the matching between images and could beperformed within a clinically acceptable time frame.
ACKNOWLEDGMENTS
The authors acknowledge advisory comments fromDr. Sachio Kuribayashi, Department of Radiology,Keio University School of Medicine. The contents ofthis study are solely the responsibility of the authorsand do not necessarily represent the official views ofthe NIH.
REFERENCES
1. D’Amico AV, Cormack R, Tempany CM, et al. Real-time magneticresonance image-guided interstitial brachytherapy in the treat-ment of select patients with clinically localized prostate cancer.Int J Radiat Oncol Biol Phys 1998;42:507–515.
2. Van Gellekom MPR, Moerland MA, Battermann JJ, LagendijkJJW. MRI-guided prostate brachytherapy with single needlemethod - a planning study. Radiother Oncol 2004;71:327–332.
3. Zangos S, Eichler K, Thalhammer A, et al. MR-guided interven-tions of the prostate gland. Minim Invasive Ther Allied Technol2007;16:222–229.
4. D’Amico AV, Cormack R, Kumar S, Tempany CM. Real-time mag-netic resonance imaging-guided brachytherapy in the treatmentof selected patients with clinically localized prostate cancer.J Endourol 2000;14:367–370.
5. Landis DM, Schultz D, Cormack R, et al. Acute urinary retentionafter magnetic resonance image-guided prostate brachytherapywith and without neoadjuvant external beam radiotherapy. Urol-ogy 2005;65:750–754.
6. Tempany C, Straus S, Hata N, Haker S. MR-guided prostateinterventions. J Magn Reson Imaging 2008;27:356–367.
7. Hirose M, Bharatha A, Hata N, et al. Quantitative MR imagingassessment of prostate gland deformation before and during MRimaging-guided brachytherapy. Acad Radiol 2002;9:906–912.
8. Bharatha A, Hirose M, Hata N, et al. Evaluation of three-dimen-sional finite element-based deformable registration of pre- andintraoperative prostate imaging. Med Phys 2001;28:2551–2560.
9. d’Aische AD, De Craene M, Haker S, et al. Improved non-rigidregistration of prostate MRI. Med Image Comput Comput AssistInterv Miccai 2004;7(Pt 1):845–852.
10. Wang H, Dong L, Lii MF, et al. Implementation and validation of athree-dimensional deformable registration algorithm for targetedprostate cancer radiotherapy. Int J Radiat Oncol Biol Phys 2005;61:725–735.
11. Schenck JF, Jolesz FA, Roemer PB, et al. Superconducting open-configuration MR imaging system for image-guided therapy. Radi-ology 1995;195:805–814.
12. Rueckert D, Sonoda LI, Hayes C, Hill DLG, Leach MO, HawkesDJ. Nonrigid registration using free-form deformations: applica-tion to breast MR images. IEEE Trans Med Imaging 1999;18:712–721.
13. Wells WM III, Viola P, Atsumi H, Nakajima S, Kikinis R. Multi-modal volume registration by maximization of mutual informa-tion. Med Image Anal 1996;1:35–51.
14. Jeong CW, Park HK, Hong SK, Byun SS, Lee HJ, Lee SE. Com-parison of prostate volume measured by transrectal ultrasonogra-phy and MRI with the actual prostate volume measured afterradical prostatectomy. Urol Int 2008;81:179–185.
15. Mir MC, Planas J, Raventos CX, et al. Is there a relationshipbetween prostate volume and Gleason score?BJU Int 2008;102:563–565.
16. Brock KK, Sharpe MB, Dawson LA, Kim SM, Jaffray DA. Accu-racy of finite element model-based multi-organ deformable imageregistration. Med Phys 2005;32:1647–1659.
17. El Naqa I, Yang D, Apte A, et al. Concurrent multimodality imagesegmentation by active contours for radiotherapy treatment plan-ning. Med Phys 2007;34:4738–4749.
18. Schreibmann E, Xing L. Narrow band deformable registration ofprostate magnetic resonance imaging, magnetic resonance spec-troscopic imaging, and computed tomography studies. Int JRadiat Oncol Biol Phys 2005;62:595–605.
19. Smith WL, Lewis C, Bauman G, et al. Prostate volume contour-ing: a 3D analysis of segmentation using 3DTRUS, CT, and MR.Int J Radiat Oncol Biol Phys 2007;67:1238–1247.
20. Mount DM, Netanyahu NS, Le Moigne J. Efficient algorithms forrobust feature matching. Pattern Recognit 1999;32:17–38.
21. Dice LR. Measures of the amount of ecologic association betweenSpecies. Ecology 1945;26:297–302.
22. Alterovitz R, Goldberg K, Pouliot J, et al. Registration of MR pros-tate images with biomechanical modeling and nonlinear parame-ter estimation. Med Phys 2006;33:446–454.
23. Nag S, Beyer D, Friedland J, Grimm P, Nath R. American Brachy-therapy Society (ABS) recommendations for transperineal perma-nent brachytherapy of prostate cancer. Int J Radiat Oncol BiolPhys 1999;44:789–799.
24. Zou KH, Warfield SK, Bharatha A, et al. Statistical validation ofimage segmentation quality based on a spatial overlap index -Scientific reports. Acad Radiol 2004;11:178–189.
25. Chao M, Li T, Schreibmann E, Koong A, Xing L. Automated con-tour mapping with a regional deformable model. Int J RadiatOncol Biol Phys 2008;70:599–608.
26. Mattes D, Haynor D, Vesselle H, Lewellyn TK, Eubank W. Non-rigid multimodality image registration. Proc SPIE 2001;4322:1609–1620.
27. Fuller DB, Jin H, Koziol JA, Feng AC. CT-ultrasound fusion pros-tate brachytherapy: a dynamic dosimetry feedback and improve-ment method. A report of 54 consecutive cases. Brachytherapy2005;4:207–216.
28. Hricak H, Dooms GC, McNeal JE, et al. MR imaging of the pros-tate gland: normal anatomy. AJR Am J Roentgenol 1987;148:51–58.
29. Curran S, Akin O, Agildere AM, Zhang J, Hricak H, Rademaker J.Endorectal MRI of prostatic and periprostatic cystic lesions andtheir mimics. AJR Am J Roentgenol 2007;188:1373–1379.
30. Reynier C, Troccaz J, Fourneret P, et al. MRI/TRUS data fusionfor prostate brachytherapy. Preliminary results. Med Phys 2004;31:1568–1575.
31. Susil RC, Menard C, Krieger A, et al. Transrectal prostate biopsyand fiducial marker placement in a standard 1.5T magnetic reso-nance imaging scanner. J Urol 2006;175:113–120.
32. Fuller DB, Jin H. Computed tomography-ultrasound fusionbrachytherapy: description and evolution of the technique.Brachytherapy 2007;6:272–279.
33. Foskey M, Davis B, Goyal L, et al. Large deformation three-dimensional image registration in image-guided radiation ther-apy. Phys Med Biol 2005;50:5869–5892.
34. Wu X, Dibiase SJ, Gullapalli R, Yu CX. Deformable image regis-tration for the use of magnetic resonance spectroscopy in pros-tate treatment planning. Int J Radiat Oncol Biol Phys 2004;58:1577–1583.
35. Fei B, Kemper C, Wilson DL. A comparative study of warping andrigid body registration for the prostate and pelvic MR volumes.Comput Med Imaging Graph 2003;27:267–281.
36. Fiorino C, Reni M, Bolognesi A, Cattaneo GM, Calandrino R.Intra- and inter-observer variability in contouring prostate andseminal vesicles: implications for conformal treatment planning.Radiother Oncol 1998;47:285–292.
1058 Oguro et al.


















