Motorcyclist “biker couples”: A descriptive analysis of orthopaedic and non-orthopaedic injuries
5
Motorcyclist ‘‘biker couples’’: A descriptive analysis of orthopaedic and non-orthopaedic injuries Joshua Murphy, John Nyland *, Jacob Lantry, Craig Roberts Department of Orthopaedic Surgery, University of Louisville, 210 East Gray St., Suite 1003, Louisville, KY 40202, United States Introduction Two individuals on the same motorcycle, one in the driving position and one in the passenger seat just behind the driver, are a common sight on the road. Accordingly the phenomenon of the ‘‘biker couple’’ also has become more commonly encountered in emergency departments. Although several reports have documen- ted motorcyclist injury patterns, 5–7,12,27,31 there are limited data to our knowledge on the orthopaedic and non-orthopaedic injury patterns of two individuals (driver and passenger) riding on the same motorcycle. 10,19,21 Scapular fractures are relatively uncommon injuries accounting for only 1% of fractures overall, 2 and representing between 0.8 and 2.9% of fractures in multiple trauma patients. 26,28 Eighty-eight percent of scapular fractures occur because of high-energy mechanisms during motor vehicle collisions. 20 Because of the high-energy nature of most scapular fractures, between 80 and 95% of these patients sustain associated injuries. 1,4,9,11,15,23,24,29 The purpose of this descriptive study was to identify the orthopaedic and non-orthopaedic injury patterns of patients who were involved in biker couple (driver and passenger) to compare differences among individuals who had scapular frac- tures. Materials and methods A retrospective review was performed of a Level I Trauma Institute Registry. A medical research institutional review board approved this study. The registry enabled a search of trauma patients admitted between 1993 and 2006 (14 years). All patients had been evaluated and admitted by a general surgery trauma service for at least a 48 h period, or had died in the emergency department following evaluation. Motorcycle accidents were identified by ICD-9 external cause of injury codes (E-codes E810–E825). A decimal and a digit follow the three-digit codes, with a ‘‘2’’ designating a driver and a ‘‘3’’ designating a passenger. During the 14-year study period 996 motorcycle drivers and 91 passengers were entered into the registry. Forty-five pairs of drivers and passengers presenting within 24 h of each other were identified. The medical records of these individuals were then Injury, Int. J. Care Injured 40 (2009) 1195–1199 ARTICLE INFO Article history: Accepted 16 March 2009 Keywords: Scapula Fractures Motor vehicle trauma Closed head injuries ABSTRACT The term ‘‘biker couple’’ is becoming an increasingly common site in emergency departments. The purpose of this study was to identify orthopaedic and non-orthopaedic injury patterns among this unique patient group. A 14-year (1993–2006) retrospective review of a Level I Trauma Institute Registry was performed. Patient demographic and injury data were obtained from 21 confirmed biker couples (n = 42). Nineteen of 21 biker couple pairs (90.5%) included a male driver and a female passenger. Drivers were more likely to have a positive blood alcohol concentration/toxicology test. Drivers had a greater incidence of scapular and rib fractures than passengers. Both drivers and passengers who sustained scapular fractures had a greater incidence of clavicle, rib, pelvis, and fibula fractures. Drivers with scapular fractures had a greater incidence of thoracic spine fractures, while passengers with scapular fractures had a greater incidence of arm–forearm–wrist–hand, femur, tibia, and foot–ankle fractures. Overall, biker couple drivers and passengers did not differ for head injury, pulmonary system, road rash, aortic injury or visceral injury. Both drivers and passengers with scapular fractures had a greater incidence of head injuries, and passengers had a greater incidence of pulmonary system, visceral injury and road rash. Both drivers and passengers who were not wearing a helmet had a greater incidence of head injuries. Unhelmeted drivers were more likely to sustain head injury than passengers. When a scapular fracture was present both drivers and passengers had a greater incidence of head injuries. Prospective investigations are needed to better delineate the precise mechanisms for these injury patterns. ß 2009 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +1 502 852 2782; fax: +1 502 852 7227. E-mail address: [email protected] (J. Nyland). Contents lists available at ScienceDirect Injury journal homepage: www.elsevier.com/locate/injury 0020–1383/$ – see front matter ß 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.injury.2009.03.015
-
Upload
joshua-murphy -
Category
Documents
-
view
212 -
download
0
Transcript of Motorcyclist “biker couples”: A descriptive analysis of orthopaedic and non-orthopaedic injuries

Injury, Int. J. Care Injured 40 (2009) 1195–1199
Motorcyclist ‘‘biker couples’’: A descriptive analysis of orthopaedicand non-orthopaedic injuries
Joshua Murphy, John Nyland *, Jacob Lantry, Craig Roberts
Department of Orthopaedic Surgery, University of Louisville, 210 East Gray St., Suite 1003, Louisville, KY 40202, United States
A R T I C L E I N F O
Article history:
Accepted 16 March 2009
Keywords:
Scapula
Fractures
Motor vehicle trauma
Closed head injuries
A B S T R A C T
The term ‘‘biker couple’’ is becoming an increasingly common site in emergency departments. The
purpose of this study was to identify orthopaedic and non-orthopaedic injury patterns among this
unique patient group. A 14-year (1993–2006) retrospective review of a Level I Trauma Institute Registry
was performed. Patient demographic and injury data were obtained from 21 confirmed biker couples
(n = 42). Nineteen of 21 biker couple pairs (90.5%) included a male driver and a female passenger. Drivers
were more likely to have a positive blood alcohol concentration/toxicology test. Drivers had a greater
incidence of scapular and rib fractures than passengers. Both drivers and passengers who sustained
scapular fractures had a greater incidence of clavicle, rib, pelvis, and fibula fractures. Drivers with
scapular fractures had a greater incidence of thoracic spine fractures, while passengers with scapular
fractures had a greater incidence of arm–forearm–wrist–hand, femur, tibia, and foot–ankle fractures.
Overall, biker couple drivers and passengers did not differ for head injury, pulmonary system, road rash,
aortic injury or visceral injury. Both drivers and passengers with scapular fractures had a greater
incidence of head injuries, and passengers had a greater incidence of pulmonary system, visceral injury
and road rash. Both drivers and passengers who were not wearing a helmet had a greater incidence of
head injuries. Unhelmeted drivers were more likely to sustain head injury than passengers. When a
scapular fracture was present both drivers and passengers had a greater incidence of head injuries.
Prospective investigations are needed to better delineate the precise mechanisms for these injury
patterns.
� 2009 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
journa l homepage: www.e lsevier .com/ locate / in jury
Introduction
Two individuals on the same motorcycle, one in the drivingposition and one in the passenger seat just behind the driver, are acommon sight on the road. Accordingly the phenomenon of the‘‘biker couple’’ also has become more commonly encountered inemergency departments. Although several reports have documen-ted motorcyclist injury patterns,5–7,12,27,31 there are limited data toour knowledge on the orthopaedic and non-orthopaedic injurypatterns of two individuals (driver and passenger) riding on thesame motorcycle.10,19,21
Scapular fractures are relatively uncommon injuries accountingfor only 1% of fractures overall,2 and representing between 0.8 and2.9% of fractures in multiple trauma patients.26,28 Eighty-eightpercent of scapular fractures occur because of high-energymechanisms during motor vehicle collisions.20 Because of thehigh-energy nature of most scapular fractures, between 80 and95% of these patients sustain associated injuries.1,4,9,11,15,23,24,29
* Corresponding author. Tel.: +1 502 852 2782; fax: +1 502 852 7227.
E-mail address: [email protected] (J. Nyland).
0020–1383/$ – see front matter � 2009 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2009.03.015
The purpose of this descriptive study was to identify theorthopaedic and non-orthopaedic injury patterns of patientswho were involved in biker couple (driver and passenger) tocompare differences among individuals who had scapular frac-tures.
Materials and methods
A retrospective review was performed of a Level I TraumaInstitute Registry. A medical research institutional review boardapproved this study. The registry enabled a search of traumapatients admitted between 1993 and 2006 (14 years). All patientshad been evaluated and admitted by a general surgery traumaservice for at least a 48 h period, or had died in the emergencydepartment following evaluation. Motorcycle accidents wereidentified by ICD-9 external cause of injury codes (E-codesE810–E825). A decimal and a digit follow the three-digit codes,with a ‘‘2’’ designating a driver and a ‘‘3’’ designating a passenger.During the 14-year study period 996 motorcycle drivers and 91passengers were entered into the registry. Forty-five pairs ofdrivers and passengers presenting within 24 h of each other wereidentified. The medical records of these individuals were then

Table 2Overall biker couple driver and passenger orthopaedic injuries.
Drivers
(n = 21)
Passengers
(n = 21)
x2 statistic p
Arm–forearm–wrist–hand 3 (14.3%) 7 (33.3%) 2.1 0.28
Scapula 16 (76.2%) 6 (28.6%) 9.5 0.005*
Rib 12 (57.1%) 5 (23.8%) 4.8 0.05*
Drivers
(n = 21)
Passengers
(n = 21)
Fisher’s exact
test (x2 statistic)
p
Clavicle 5 (23.8%) 3 (14.3%) 0.6 0.70
Cervical spine 2 (9.5%) 1 (4.8%) 0.4 0.99
Thoracic spine 5 (23.8%) 1 (4.8%) 3.1 0.18
Pelvis 5 (23.8%) 2 (9.5%) 1.5 0.41
Femur 3 (14.3%) 4 (19%) 0.2 0.99
Tibia 3 (14.3%) 5 (23.8%) 0.6 0.70
Fibula 5 (23.8%) 3 (14.3%) 0.6 0.70
Foot–ankle 4 (19%) 5 (23.8%) 0.1 0.99
* p < 0.05.
Table 3Overall biker couple driver and passenger non-orthopaedic injuries.
Drivers
(n = 21)
Passengers
(n = 21)
x2 statistic p
Head injury 10 (47.6%) 10 (47.6%) 0.0 0.99
Pulmonary system 5 (23.8%) 6 (28.6%) 0.12 0.99
Road rash 3 (14.3%) 8 (38.1%) 3.1 0.16
Drivers
(n = 21)
Passengers
(n = 21)
Fisher’s exact
test (x2 statistic)
p
Aorta 1 (4.8%) 1 (4.8%) 0.0 0.99
Viscera 1 (4.8%) 5 (23.8%) 3.1 0.18
Table 4Overall biker couple head injury incidence vs. helmet use.
Drivers (n = 21)* Passengers (n = 21)**
Head injury No head injury Head injury No head injury
Helmet 2 9 2 6
No helmet 8 2 8 5
* Odds ratio = 18.0, x2 = 8.03, p = 0.009.** Odds ratio = 4.8, x2 = 2.7, p = 0.18. Overall x2 = 9.8, p = 0.002.
J. Murphy et al. / Injury, Int. J. Care Injured 40 (2009) 1195–11991196
cross-checked to verify that they were on the same motorcycle atthe time of their accident. Twenty-four pairs of drivers andpassengers were excluded from the study because it could not beconfirmed that they were on the same motorcycle at the time of theaccident. Twenty-one biker couple pairs (n = 42) were verified,meeting our study inclusion criteria. Injury and demographic dataincluding age, gender, blood alcohol concentration/toxicologytesting, mean hospital days, Injury Severity Score, Glasgow ComaScale score, mortality, helmet usage, orthopaedic, and non-orthopaedic injuries were obtained from the registry and patientmedical records.
Orthopaedic injuries included fractures to the humerus, radius,ulna, hand–wrist, clavicle, scapula, cervical spine, thoracic spine,ribs, pelvis, femur, tibia, fibula, and foot–ankle. Head injuriesincluded closed head injuries, skull fractures, and intracranialbleeding. For statistical analysis purposes the arm–forearm–wrist–hand was calculated as a single factor. Overall comparisons of bikercouple drivers and passengers were made using chi-square (x2) orFisher’s exact tests (when the criteria for appropriate x2 test usewere not reached). Odds ratios were also calculated for head injuryincidence. An alpha level of p � 0.05 was selected to indicatestatistical significance.
Results
The mean time difference between arrival of the biker coupledriver and passenger to the emergency department was 10.2 min(range = 0–62). Nineteen of the 21 (90.5%) biker couples included amale driver and a female passenger. There was also one father–sonpair and one pair with a female driver and a male passenger. Fifty-seven percent of the biker couples were male–female pairs sharingthe same last name. Drivers were more likely to have a positiveblood alcohol concentration/toxicology test, and the only deathoccurred in the passenger group. Patient age, length of hospitalisa-tion, Injury Severity Score, and Glasgow Coma Scale scores wereessentially the same between drivers and passengers (Table 1).
The couple with the female driver produced the only deathwhereby the passenger exanguinated during surgical repair of anintra-thoracic aortic injury. Overall, drivers displayed a greaterincidence of scapula and rib fractures than passengers (Table 2).Overall, non-orthopaedic injury incidence including head injuries,pulmonary contusions, aortic injuries, visceral injuries and roadrash were also similar between drivers and passengers (Table 3).
Head injury and helmet use percentages were also comparedbetween biker couple drivers and passengers (Table 4). Overallthere was an increased incidence of head injury in both bikercouple drivers and passengers who were not wearing a helmet.When analysed by their position on the motorcycle an increasedincidence of head injury was statistically significant for unhel-meted drivers, while the increased incidence in unhelmetedpassengers displayed a trend, but did not reach statisticalsignificance. Unhelmeted drivers were more likely than passengersto sustain head injuries.
Both drivers and passengers with scapular fractures had agreater incidence of clavicle, rib, pelvis, and fibula fractures(Table 5). Passengers with scapular fractures had a greaterincidence of arm–forearm–wrist–hand, femur, tibia, and foot–ankle fractures. Both drivers and passengers with scapular
Table 1Patient demographics.
Mean patient age
in years (range)
Male:female
ratio
% Positive blood alcohol
concentration/toxicology
Drivers (n = 21) 44 (21–59) 20:1 57.1
Passengers (n = 21) 41 (17–57) 2:19 33.3
fractures had a greater incidence of head and pulmonary systeminjuries (Table 6). Passengers with scapular fractures had a greaterincidence of visceral injuries and road rash.
Discussion
Markogiannakis et al.14 in a study of 730 consecutive patientswho were injured in motor vehicle accidents in Greece (motorcy-clists = 60.8%) reported that injuries were most commonly locatedat the craniocerebral, upper and lower extremity, and thoracicregions. Our study supports these findings, with almost half(47.6%) of the biker couple drivers and passengers sustaining ahead injury and the generally high incidence of extremityfractures. Peek et al.18 reported that lower extremity injuries
Mean number of days
hospitalised (range)
Mean injury severity
score (range)
Mean Glasgow
coma scale (range)
Deaths (%)
11 (1–30) 18 (12–34) 13.9 (3–15) 0
10 (1–34) 19 (12–29) 13.9 (3–15) 4.8
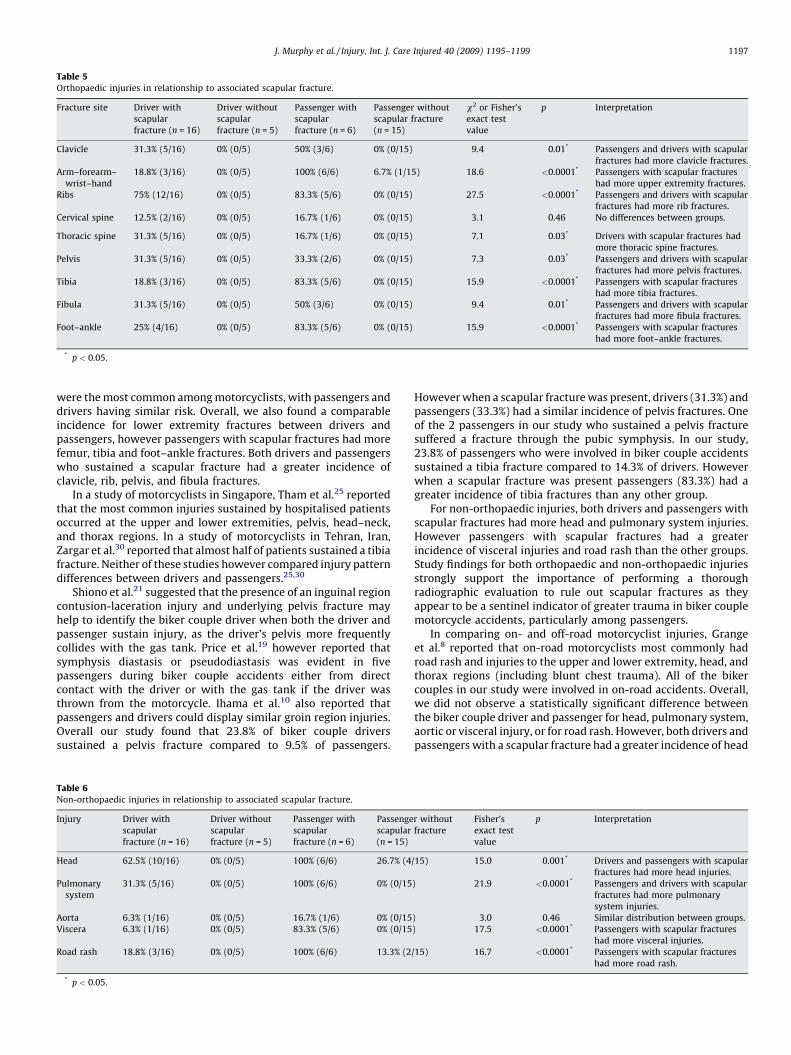
Table 5Orthopaedic injuries in relationship to associated scapular fracture.
Fracture site Driver with
scapular
fracture (n = 16)
Driver without
scapular
fracture (n = 5)
Passenger with
scapular
fracture (n = 6)
Passenger without
scapular fracture
(n = 15)
x2 or Fisher’s
exact test
value
p Interpretation
Clavicle 31.3% (5/16) 0% (0/5) 50% (3/6) 0% (0/15) 9.4 0.01* Passengers and drivers with scapular
fractures had more clavicle fractures.
Arm–forearm–
wrist–hand
18.8% (3/16) 0% (0/5) 100% (6/6) 6.7% (1/15) 18.6 <0.0001* Passengers with scapular fractures
had more upper extremity fractures.
Ribs 75% (12/16) 0% (0/5) 83.3% (5/6) 0% (0/15) 27.5 <0.0001* Passengers and drivers with scapular
fractures had more rib fractures.
Cervical spine 12.5% (2/16) 0% (0/5) 16.7% (1/6) 0% (0/15) 3.1 0.46 No differences between groups.
Thoracic spine 31.3% (5/16) 0% (0/5) 16.7% (1/6) 0% (0/15) 7.1 0.03* Drivers with scapular fractures had
more thoracic spine fractures.
Pelvis 31.3% (5/16) 0% (0/5) 33.3% (2/6) 0% (0/15) 7.3 0.03* Passengers and drivers with scapular
fractures had more pelvis fractures.
Tibia 18.8% (3/16) 0% (0/5) 83.3% (5/6) 0% (0/15) 15.9 <0.0001* Passengers with scapular fractures
had more tibia fractures.
Fibula 31.3% (5/16) 0% (0/5) 50% (3/6) 0% (0/15) 9.4 0.01* Passengers and drivers with scapular
fractures had more fibula fractures.
Foot–ankle 25% (4/16) 0% (0/5) 83.3% (5/6) 0% (0/15) 15.9 <0.0001* Passengers with scapular fractures
had more foot–ankle fractures.
* p < 0.05.
J. Murphy et al. / Injury, Int. J. Care Injured 40 (2009) 1195–1199 1197
were the most common among motorcyclists, with passengers anddrivers having similar risk. Overall, we also found a comparableincidence for lower extremity fractures between drivers andpassengers, however passengers with scapular fractures had morefemur, tibia and foot–ankle fractures. Both drivers and passengerswho sustained a scapular fracture had a greater incidence ofclavicle, rib, pelvis, and fibula fractures.
In a study of motorcyclists in Singapore, Tham et al.25 reportedthat the most common injuries sustained by hospitalised patientsoccurred at the upper and lower extremities, pelvis, head–neck,and thorax regions. In a study of motorcyclists in Tehran, Iran,Zargar et al.30 reported that almost half of patients sustained a tibiafracture. Neither of these studies however compared injury patterndifferences between drivers and passengers.25,30
Shiono et al.21 suggested that the presence of an inguinal regioncontusion-laceration injury and underlying pelvis fracture mayhelp to identify the biker couple driver when both the driver andpassenger sustain injury, as the driver’s pelvis more frequentlycollides with the gas tank. Price et al.19 however reported thatsymphysis diastasis or pseudodiastasis was evident in fivepassengers during biker couple accidents either from directcontact with the driver or with the gas tank if the driver wasthrown from the motorcycle. Ihama et al.10 also reported thatpassengers and drivers could display similar groin region injuries.Overall our study found that 23.8% of biker couple driverssustained a pelvis fracture compared to 9.5% of passengers.
Table 6Non-orthopaedic injuries in relationship to associated scapular fracture.
Injury Driver with
scapular
fracture (n = 16)
Driver without
scapular
fracture (n = 5)
Passenger with
scapular
fracture (n = 6)
Passenge
scapular
(n = 15)
Head 62.5% (10/16) 0% (0/5) 100% (6/6) 26.7% (4
Pulmonary
system
31.3% (5/16) 0% (0/5) 100% (6/6) 0% (0/15
Aorta 6.3% (1/16) 0% (0/5) 16.7% (1/6) 0% (0/15
Viscera 6.3% (1/16) 0% (0/5) 83.3% (5/6) 0% (0/15
Road rash 18.8% (3/16) 0% (0/5) 100% (6/6) 13.3% (2
* p < 0.05.
However when a scapular fracture was present, drivers (31.3%) andpassengers (33.3%) had a similar incidence of pelvis fractures. Oneof the 2 passengers in our study who sustained a pelvis fracturesuffered a fracture through the pubic symphysis. In our study,23.8% of passengers who were involved in biker couple accidentssustained a tibia fracture compared to 14.3% of drivers. Howeverwhen a scapular fracture was present passengers (83.3%) had agreater incidence of tibia fractures than any other group.
For non-orthopaedic injuries, both drivers and passengers withscapular fractures had more head and pulmonary system injuries.However passengers with scapular fractures had a greaterincidence of visceral injuries and road rash than the other groups.Study findings for both orthopaedic and non-orthopaedic injuriesstrongly support the importance of performing a thoroughradiographic evaluation to rule out scapular fractures as theyappear to be a sentinel indicator of greater trauma in biker couplemotorcycle accidents, particularly among passengers.
In comparing on- and off-road motorcyclist injuries, Grangeet al.8 reported that on-road motorcyclists most commonly hadroad rash and injuries to the upper and lower extremity, head, andthorax regions (including blunt chest trauma). All of the bikercouples in our study were involved in on-road accidents. Overall,we did not observe a statistically significant difference betweenthe biker couple driver and passenger for head, pulmonary system,aortic or visceral injury, or for road rash. However, both drivers andpassengers with a scapular fracture had a greater incidence of head
r without
fracture
Fisher’s
exact test
value
p Interpretation
/15) 15.0 0.001* Drivers and passengers with scapular
fractures had more head injuries.
) 21.9 <0.0001* Passengers and drivers with scapular
fractures had more pulmonary
system injuries.
) 3.0 0.46 Similar distribution between groups.
) 17.5 <0.0001* Passengers with scapular fractures
had more visceral injuries.
/15) 16.7 <0.0001* Passengers with scapular fractures
had more road rash.

J. Murphy et al. / Injury, Int. J. Care Injured 40 (2009) 1195–11991198
injury and pulmonary system injuries, while passengers had agreater incidence of visceral injury and road rash.
Jeffers et al.12 reported that motorcycle accident passengersmade up 4.1% of individuals who did not sustain a foot injury, andonly 1.9% of those who did surmising that drivers had morefractures because they instinctively extend their leg on the side ofthe leaning motorcycle, placing the initial impact on the foot.12 Ourstudy found a similar overall incidence of foot–ankle fracturesbetween drivers and passengers, however when a scapular fracturewas present, passengers displayed a greater foot–ankle fractureincidence.
Bried et al.3 reported that 22% of individuals who were injuredin motorcycle accidents were passengers, however an injurycomparison with drivers was not performed. In their study, 75% ofmotorcyclists were not wearing a helmet and 24% were intoxicatedat the time of injury. They reported that lack of helmet useincreased head injury risk, increased time in the intensive careunit, and increased injury severity. Fractures most commonlyoccurred at the skull, ribs, pelvis, tibia, and feet.3 Our study foundthat biker couple drivers and passengers had a similar incidence ofhead injury, however unhelmeted drivers were more likely tosustain a head injury. We found a reduced head injury incidence forboth the biker couple driver (80% vs. 18%) and passenger (61.5% vs.25%) with helmet use.
To our knowledge this is the first study that has describedorthopaedic and non-orthopaedic injury incidence among bikercouples. Additionally, to our knowledge this represents the firststudy that has evaluated the orthopaedic and non-orthopaedicinjury incidence of biker couples based on the presence of ascapular fracture. Previous studies have reported that as manyas 50% of individuals with motor vehicle accident inducedscapular fractures also had thoracic injuries, 44–53.6% had ribfractures, 26% had clavicle fractures, 16–66% had pneumo- orhemothorax injuries, 20% had cerebral contusions, 24% had skullfractures, 53% had pulmonary contusions, 12.5% had brachialplexus injuries, 12.5% had upper extremity vascular injury, 44–50% had ipsilateral upper extremity injury, and 10% had spinefractures.1,10,15–17,22,26
This study provides new information about the orthopaedic andnon-orthopaedic injuries sustained by biker couples. With thisinformation prospective studies can be designed that focus moredirectly on comprehensive documentation of biker couple injurypatterns and accident mechanisms in addition to evaluating long-term accident-related patient disability levels.
This study has several limitations. The registry did notidentify individuals who sustained minor injuries, or those whodied at the accident scene. Additionally, very limited or noinformation was provided regarding the use of protective jackets,trousers, gloves, footwear, etc. More detail regarding the accidentvictim’s attire at the time of the motorcycle accident would helpto determine their injury prevention or severity reductionefficacy. Lastly, patients admitted to a Level I Trauma Institutemay not reflect the overall patient population, but rather amixture of individuals who had either sustained their injurieslocally or who had been transferred in from surrounding regionsto receive specialised care.13 Therefore these study findings maynot generalize directly to all institutions. Also, our report whileproviding confirmed identification of orthopaedic and non-orthopaedic injuries among this patient group does not delineatethe seriousness or grade for each reported injury. This may beparticularly important as multiple region scapular fractures arereportedly associated with more centrifugal injury mechanismsand single region scapular fractures with more centripedal injurymechanisms with the scapula as the center of force.24 Thegreatest study limitation however was the small sample size.Future studies of the scapular fracture relationship to motorcycle
accident-related trauma may benefit from a more detailedassessment of scapular fracture patterns in addition to a largersample size.
Conclusions
Overall scapular and rib fracture incidence was more commonamong the driver than the passenger in biker couple motorcycleaccidents. When a scapular fracture was present however, bothdrivers and passengers had a greater incidence of clavicle, rib,pelvis, and fibula fractures. Drivers with scapular fractures had agreater incidence of thoracic spine fractures, while passengerswith scapular fractures had a greater incidence of arm–forearm–wrist–hand, femur, tibia, and foot–ankle fractures. Overall, bikercouple drivers and passengers did not differ for head injury,pulmonary system, road rash, aortic injury or visceral injury. Whena scapular fracture was present however both drivers andpassengers had a greater incidence of head injuries, and passengershad a greater incidence of pulmonary system, visceral injury androad rash.
References
1. Armstrong CP, Van Der Spuy J. The fractured scapula: Importance and manage-ment based on a series of 62 patients. Injury 1984;15:324–9.
2. Baldwin KD, Ohman-Strickland P, Mehta S, Hume E. Scapula fractures: a markerfor concomitant injury? A retrospective review of data in the national traumadatabase. J Trauma 2008;65:430–5.
3. Bried J, Cordasco F, Volz R. Medical and economic parameters of motorcycle-induced trauma. Clin Orthop 1987;223:252–6.
4. Brown CV, Velmahos G, Wang D, et al. Association of scapular fractures andblunt thoracic aortic injury: fact or fiction? Am Surg 2005;71:54–7.
5. Craig G, Sleet R, Wood S. Lower limb injuries in motorcycle accidents. Injury1983;15:163–6.
6. de Peretti F, Cambas P, Hovorka I, et al. Motorcycle petrol tanks and their role insevere pelvic injuries. Injury 1994;25:223–5.
7. Drysdale W, Kraus J, Franti C. Injury patterns in motorcycle collisions. J Trauma1975;15:99–115.
8. Grange J, Corbett S, Cotton A. Street bikes versus dirt bikes: a comparison ofinjuries among motorcyclists presenting to a regional trauma center. J Trauma2004;57:591–4.
9. Ideberg R, Grevsten S, Larsson S. Epidemiology of scapular fractures: Incidenceand classification of 338 fractures. Acta Orthop Scand 1995;66:395–7.
10. Ihama Y, Fuke C, Miyazaki T. A two-rider motorcycle accident involving injuriesaround groin area in both the driver and the passenger. Legal Med 2007;9:274–7.
11. Imatani RJ. Fractures of the scapula: a review of 53 fractures. J Trauma1975;15:473–8.
12. Jeffers RF, Tan B, Nicolopoulos C, et al. Prevalence and patterns of foot injuriesfollowing motorcycle trauma. J Orthop Trauma 2004;18:87–91.
13. Lowenstein S. Trauma registries: tarnished gold. Ann Emerg Med 1996;27:389–91.
14. Markogiannakis H, Sanidas E, Messaris E, et al. Motor vehicle trauma: analysisof injury profiles by road-user category. Emerg Med J 2006;23:27–31.
15. McGahan JP, Rab GT, Dublin A. Fractures of the scapula. J Trauma 1980;20:880–3.
16. McGinnis M, Denton JR. Fractures of the scapula: a retrospective study of 40fractured scapulae. J Trauma 1989;29:1488–93.
17. McLennan JG, Ungersma J. Pneumothorax complicating fracture of the scapula. JBone Joint Surg Am 1982;64:598–9.
18. Peek C, Braver E, Shen H, Kraus J. Lower extremity injuries from motorcyclecrashes: a common cause of preventable injury. J Trauma 1994;37:358–64.
19. Price N, Ragoowansi R, Bircher M. Pelvic ring diastasis and pseudo-diastasis inmotorcycle pillion passengers. Injury 1996;27:441–4.
20. Scavenius M, Sloth C. Fractures of the scapula. Acta Orthop Belg 1996;62:129–32.
21. Shiono H, Akane A, Matsubara K, et al. Identification of the driver in two-ridermotorcycle accidents Inguinal contusion-laceration as an indication of thedriver. Am J For Med Pathol 1990;11:190–2.
22. Stephans NC, Morgan AJB, Corvo P, Bernstein BA. Significance of scapularfracture in blunt trauma patients. Ann Emer Med 1995;25:439–42.
23. Tadros AMA, Lunsjo K, Czechowski J, Abu-Zidan FM. Causes of delayed diagnosisof scapular fractures. Injury 2008;39:314–8.
24. Tadros AMA, Lunsjo K, Czechowski J, Abu-Zidan FM. Multiple-region scapularfractures had more severe chest injury than single-region fractures: a prospec-tive study of 107 blunt trauma patients. J Trauma 2007;63:889–93.
25. Tham K, Seow E, Lau G. Pattern of injuries in helmeted motorcyclists inSingapore. Emerg Med J 2004;21:478–82.

J. Murphy et al. / Injury, Int. J. Care Injured 40 (2009) 1195–1199 1199
26. Thompson DA, Flynn TC, Miller PW, Fisher RP. The significance of scapularfractures. J Trauma 1985;25:974–7.
27. Varley G, Spencer-Jones R, Thomas P. Injury patterns in motorcycle road racers:experience on the Isle of Man. Injury 1993;24:443–6.
28. Veysi VT, Mittal R, Agarwal S, Dosani A, Giannoudis PV. Multiple trauma andscapular fractures: so what? J Trauma 2003;55:1145–7.
29. Weening B, Walton C, Cole PA, Alanezi K, Hanson BP, Bhandari M. Lowermortality in patients with scapular fractures. J Trauma 2005;59:1477–81.
30. Zargar M, Khaji A, Karbaksh M. Pattern of motorcycle-related injuries in Tehran,1999 to 2000: a study in 6 hospitals. East Mediterr Health J 2006;12:81–7.
31. Zettas J, Zettas P, Thanasophon B. Injury patterns in motorcycle accidents. JTrauma 1979;19:833–6.