Motion: Be it resolved that BLBLIs can be used for infections ......2018/05/04 · Motion: Be it...
28
Motion: Be it resolved that BLBLIs can be used for infections caused by Gram-negative bacilli (GNB) carrying ESBL and Amp-C Arguing in favour: Gerald A. Evans MD FRCPC FAMMI Chair, Division of Infectious Diseases Professor of Medicine, Queen’s University AMMI-CACMID Annual Conference 2018 Vancouver, BC
Transcript of Motion: Be it resolved that BLBLIs can be used for infections ......2018/05/04 · Motion: Be it...

Motion:Be it resolved that BLBLIs can be used for infections caused by Gram-negative bacilli (GNB) carrying ESBL and Amp-C
Arguing in favour:Gerald A. Evans MD FRCPC FAMMIChair, Division of Infectious Diseases
Professor of Medicine, Queen’s University
AMMI-CACMID Annual Conference 2018Vancouver, BC

Disclosures – GA EvansRelationships with commercial interests:•
Speakers Bureau/Honoraria: • NoneConsulting Fees: • Reformulary®Financial disclosures • – None
Grants/Research Support: • CIHRPotential for conflict(s) of interest:•
I have received support from • Public Health Ontario, Ontario MOHLTCTravel accommodation • – Sunovion Pharma & AMMI Canada

AmpC Beta lactamases – Ambler Class C• Found in extended-spectrum cephalosporin-resistant Gram-negative bacteria
• Commonly encoded on the chromosome of SPICE/SPACE group GNBs e.g. CMY-2, FOX-5, ACT-1• Able to hydrolyse cephamycins• Their expression is usually inducible, leading to hyperexpression • Hyperexpressed AmpC type β-lactamases may also be carried on plasmids
• In contrast to ESBLs, AmpC BLs are not inhibited by β-lactamase inhibitors
• BLBLIs should NOT be used to treat pathogens expressing AmpC BLs

Extended Spectrum Beta-Lactamases – Ambler Class A• Convey resistance to penicillins and cephalosporins including 3rd
generation cephalosporins (CTX-M)• Major – TEM, SHV, CTX-M
• Heterogenous group with close to 1000 different ESBLs1
• Expressed by many Enterobacteriaceae• TEM – E. coli, K. pneumoniae and others – some are resistant to CA & sulbactam• SHV – Predominately K. pneumoniae• CTX-M – E. coli, Salmonella enterica serovars and others (90 subtypes)
• Varyingly inhibited by beta lactamase inhibitors• MIC determinations for BLBLI can vary upward of 4 dilutions by BMD2
• PTZ breakpoints differ CLSI ≤8 mg/L vs. EUCAST ≤16 mg/L
1. Liakopoulos A et al Forny Microbiol 2016;7:13742. CLSI 2015 1st ed, CLSI Guideline M52 Clin Lab Std Instit Wayne, PA

Let’s address the elephant in the room…

O1121 The MERINO Trial: piperacillin-tazobactam versus meropenem for the definitive treatment of bloodstream infections caused by third-generation cephalosporin non-susceptible Escherichia coli or Klebsiella spp.: an international multi-centre open-label non-inferiority randomised controlled trial
Patrick Harris*1 2 16, Paul Tambyah3 4, David Lye3 5, Yin Mo4, Tau Hong Lee5, Mesut Yilmaz6, Thamer Alenazi7, Yaseen Arabi7, Marco Falcone8, Matteo Bassetti9, Elda Righi9, Benjamin Rogers10, Souha S. Kanj11, Hasan Bhally12, Jonathan Iredell13 14, Marc Mendelson15, Tom Boyles15, David Looke16 17, Spiros Miyakis18 19, Genevieve Walls20, Mohammed Al Khmais21, Ahmed Mohamed Wadie Hassan Zikri21, Amy Crowe22, Paul Ingram23 24, Nick Daneman25, Paul Griffin17 26 27, Eugene Athan28, Penelope Lorenc29, Peter Baker30, Anton Peleg31 32, Tiffany Harris-Brown33, David Paterson33 34
1University of Queensland, UQ Centre for Clinical Research, Brisbane, Australia, 2Royal Brisbane and Women's Hospital, Department of microbiology, Pathology Queensland, Brisbane, Australia, 3National University of Singapore, Yong Loo Lin School of Medicine, Singapore, Singapore, 4National University Hospital Singapore, Department of Infectious Diseases, Singapore, Singapore, 5Tan Tock Seng Hospital, Department of Infectious Diseases, Singapore, Singapore, 6Istanbul Medipol University, Department of Infectious Diseases and Clinical Microbiology, Istanbul, Turkey, 7King Abdulaziz Medical City, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, 8Sapienza University of Rome, Department of Public Health and Infectious Diseases, Roma, Italy, 9University of Udine and Santa Maria Misericordia Hospital, Department of Medicine , Gorizia, Italy, 10Monash University, Centre for Inflammatory Diseases, Clayton, Australia, 11American University of Beirut, Department of Internal Medicine, Division of Infectious Diseases, Beirut, Lebanon, 12North Shore Hospital, Department of Medicine and Infectious Diseases, Auckland, New Zealand, 13The University of Sydney, Marie Bashir Institute for Infectious Disease and Biosecurity, Sydney, Australia, 14Westmead Hospital, Centre for Infectious Diseases and Microbiology, Westmead, Australia, 15University of Cape Town, Division of Infectious Diseases & HIV Medicine, Department of Medicine, Groote Schuur Hospital, Cape Town, South Africa, 16Princess Alexandra Hospital, Infection Management Services, Woolloongabba, Australia, 17The University of Queensland, Saint Lucia, Australia, 18University of Wollongong, School of Medicine & Illawarra Health and Medical Research Institute, Wollongong, Australia, 19Wollongong Hospital, Department of Infectious Diseases, Wollongong, Australia, 20Middlemore Hospital, Department of Infectious Diseases, Auckland, New Zealand, 21King Fahad Specialist Hospital - Dammam, اااااا, Saudi Arabia, 22St. Vincent's Hospital Melbourne, Department of Infectious Diseases Department of Microbiology, Melbourne, Australia, 23The University of Western Australia, School of Pathology and Laboratory Medicine , Crawley, Australia, 24Fiona Stanley Hospital, Department of Infectious Diseases , Murdoch, Australia, 25University of Toronto Scarborough, Sunnybrook Health Sciences Centre, Toronto, Canada, 26Mater Hospital Brisbane, Department of Medicine and Infectious Diseases, Brisbane, Australia, 27QIMR Berghofer Medical Research Institute, Brisbane City, Australia, 28Barwon Health and Deakin University, Department of Infectious Diseases, Geelong, Australia, 29The University of Queensland, UQ Centre for Clinical Research , Herston, Australia, 30University of Queensland, School of Public Health, Herston, Australia, 31Monash University, Infection & Immunity Program, Biomedicine Discovery Institute & Department of Microbiology, Clayton, Australia, 32Monash University, Department of Infectious Diseases, Alfred Hospital and Central Clinical School, Clayton, Australia, 33The University of Queensland, UQ Centre for Clinical Research, Herston, Australia, 34Royal Brisbane & Women's Hospital, Department of Infectious Diseases, Herston, Australia
Background: Escherichia coli or Klebsiella pneumoniae may express extended-spectrum β-lactamases (ESBLs) mediating resistance to third-generation cephalosporins (3GCs). Whether piperacillin-tazobactam is effective carbapenem-sparing therapy for bloodstream infection (BSI) caused by these organisms is uncertain. We aimed to test this concept in a randomised controlled trial (RCT) (ACTRN12615000403538; NCT02176122).
Harris P et al Abstract O1121 28th ECCMID April 2018, Madrid, Spain

The MERINO StudyAdult patients from 32 sites in 9 countries with • BSI caused by 3GC non-susceptible, piperacillin-tazobactam susceptible, E. coli or K. pneumoniaeResults•
23/187 (12.3%) patients randomized to piperacillin• -tazobactam met the primary outcome of mortality at 30 days7/191 (3.7%) randomized to meropenem•Risk difference 8.6%, (95% CI 3.4% to 14.5%)•RR 3.4, (95% CI 1.5 to 7.6; p=0.002)•
Harris P et al Abstract O1121 28th ECCMID April 2018, Madrid, Spain

Issues with MERINO
• They changed their terminology from ESBL to “3rd gen cephalosporin
resistant” which suggests they could not prove that the isolates were all
ESBL
• There may be many AmpC or other mechanisms
• 21% of E. coli are AmpC carriers in Singapore2
• What if those are the 20% that are failing?
• The predominant contributing centre for the study was Singapore (40.6%)
• Does a study that is weighted so heavily to one location translate everywhere else if
enzyme and MIC distributions differ?
• A previous study suggested high rates of CTX-M-1 group in Singapore2 with higher
MICs to BLBLI than CTX-M-9 group1 which is predominant elsewhere in the world1
• Lower rates of SHV and TEM in Singapore2
Sources: 1. Tärnberg et al Eur J Clin Microbiol Infect Dis 2011;30:981–987
2. Sheng WH et al AAC 2013;57:2981–2988

blaCTX-M-9, and blaCTX-M-14 in CTX-M-producing E. coli isolatesthat might be involved in both the spread and expression of thesegenes in Enterobacteriaceae resistance (15). The spread ofblaCTX-M-15 was essentially caused by the clonal expansion of E. coliisolates belonging to the international pandemic ST131 clone (18,19), and these strains have been reported to occur in healthy peo-ple as a part of the commensal flora (20). Our results show theemergence of CTX-M genes (blaCTX-M-14 and blaCTX-M-15) acrossdifferent species, including primarily E. coli and Klebsiella and
Enterobacter spp. The dissemination of blaCTX-M genes in Entero-bacteriaceae species suggests that the diffusion of epidemic plas-mids carrying blaCTX-M already has taken place and plays an im-portant role in the spread of this gene in the Asia-Pacific region.More epidemiological studies are necessary to elucidate this point.
SHV-12 was the dominant SHV type for both ESBL-producingE. coli and K. pneumoniae isolates in various countries, such as inIndia, Taiwan, and Philippines. TEM-52- and SHV-12-producingstrains have been found in hospitals in Europe (18), as well as in in
TABLE 2 (Continued)
Bacterial species
!-Lactamase combination or single !-lactamase (no. of isolates)
Community-associated IAI ("48 h) Hospital-associated IAI (!48 h)
K. oxytoca with an ertapenemMIC of "0.5 #g/ml (n $ 5)
CTX-M-14 % DHA-1 (1)CTX-M-14 (1)CTX-M-15 (2)CTX-M-22 (1)
Other species with ertapenemMICs of &0.5 #g/mla (n $ 9)
SHV-12 % NDM-1 (1) CTX-M-15 % ACT/MIR % NDM-1 (1)CTX-M-15 % NDM-1 (1) CTX-M-15 % DHA-1 % NDM-1 (1)DHA-1 % NDM-1 (1) CMY-2 % DHA-1 % NDM-1 (1)
CMY-2 (2)SHV-12 (1)
Other species with ertapenemMICs of "0.5 #g/mla (n $ 6)
CTX-M-14 (1) CTX-M-15 (2)CTX-M-15 (2) CTX-M-24 (1)
a Other species included C. freundii (5), P. mirabilis (3), M. morganii (2), E. aerogenes (2), E. asburiae (1), P. vulgaris (1), and P. rettgeri (1).
TABLE 3 Geographic distribution of various !-lactamases among Enterobacteriaceae causing intra-abdominal infections in different countries
!-Lactamase (no. of isolates)
No. of isolates from indicated country exhibiting !-lactamase
Australia China India MalaysiaNewZealand Philippines Singapore
SouthKorea Taiwan Thailand Vietnam
ESBL (651) 2 66 347 29 9 52 31 41 51 16 7SHV (59) 0 2 16 2 1 13 4 4 15 2 0
SHV-12 (40) 0 2 7 2 1 11 1 3 12 1 0Others (19) 0 0 9 0 0 2 3 1 3 1 0
TEM (4) 0 0 0 0 0 1 0 2 1 0 0CTX-M (588) 2 64 331 27 8 38 27 35 35 14 7
CTX-M-14 (77) 0 33 0 1 1 2 4 15 18 3 0CTX-M-15 (428) 2 10 323 17 6 26 18 8 9 5 4Others (83) 0 21 8 9 1 10 5 12 8 6 3
AmpC (196) 2 2 109 1 7 16 8 9 37 1 4CMY (110) 0 0 85 0 1 0 1 4 17 0 2
CMY-2 (102) 0 0 80 0 1 0 1 1 17 0 2Others (8) 0 0 5 0 0 0 0 3 0 0 0
DHA-1 (46) 0 2 13 1 0 13 4 1 11 0 1ACT/MIR (40) 2 0 11 0 6 3 3 4 9 1 1
Carbapenemase (79) 2 0 73 0 0 4 0 0 0 0 0KPC (0) 0 0 0 0 0 0 0 0 0 0 0NDM (65) 0 0 65 0 0 0 0 0 0 0 0
NDM-1 (62) 0 0 62 0 0 0 0 0 0 0 0NDM-4 (2) 0 0 2 0 0 0 0 0 0 0 0NDM-6 (1) 0 0 1 0 0 0 0 0 0 0 0
IMP (7) 2 0 1 0 0 4 0 0 0 0 0IMP-26 (6) 2 0 0 0 0 4 0 0 0 0 0IMP-1 (1) 0 0 1 0 0 0 0 0 0 0 0
OXA (7) 0 0 7 0 0 0 0 0 0 0 0OXA-181 (7) 0 0 7 0 0 0 0 0 0 0 0
Sheng et al.
2986 aac.asm.org Antimicrobial Agents and Chemotherapy
on April 29, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
Source: Sheng WH et al AAC 2013;57:2981–2988
GNB Isolates in Asia-Pacific Region

BLBLIs and CTX-M SusceptibilityTABLE2.!-LactamMICsforK.ascorbata,K.cryocrescens,K.georgiana,andE.colilaboratorystrainsproducingrepresentative
CTX-Menzymes
!-Lactam
MIC("g/ml)
LaboratoryE.colistrainsproducing:Kluyverastrainsproducing:
CTX-M-3(77) a CTX-M-15(77) CTX-M-4(40) CTX-M-5(20) CTX-M-9(14) CTX-M-16(14) CTX-M-14(15) CTX-M-27(15) CTX-M-18(74) CTX-M-19(74) CTX-M-8(17) KLUA b(45) KLUG-1 c(78) KLUC-1 d(33)
Amoxicillin#512#512#512 e#128 e#2,048#512#512#512#512#512#5128464Amoxicillin$CLA f128328328884128128160.51%0.5Ticarcillin#512#512128#128#512#512#512#512#512#512#5126416128Ticarcillin$CLA64321281616168256256320.12511Piperacillin512#512256#128256256256256#512#51222%1Piperacillin$TZP g242122221680.1250.25%1Cephalothin#512#512
5125125121,024#512#512#512848Cefuroxime#512#512512512512512512#512#5124416Cefotaxime512512512#12816161616644160.060.250.06Cefotaxime$CLA22
0.060.060.50.50.060.06%0.06
Cefpirome5125122224
80.12%0.06Cefepime12864
0.511644%0.030.12%0.06Ceftazidime32256216181821281%0.030.12%0.06Ceftazidime$CLA22
0.250.250.5160.06%0.06%0.06
Aztreonam1286432128484864480.060.060.06Aztreonam$CLA
0.060.060.250.120.12
Moxalactam0.510.52
%0.060.03Cefoxitin2416
44410.061Imipenem0.250.250.5
0.250.250.250.1250.060.06aReferencenumbersaregiveninparentheses.bModalMICsfor12K.ascorbatastrains.cMICsforK.cryocrescens.dMICsforK.georgiana.eMICofampicillin.fCLA,clavulanateatafixedconcentrationof2"g/ml.gTZB,tazobactamatafixedconcentrationof4"g/ml.
VOL. 48, 2004 MINIREVIEW 9
on April 29, 2018 by guesthttp://aac.asm.org/
Downloaded from
Tärnberg et al Eur J Clin Microbiol Infect Dis 2011;30:981–987

Issues with MERINO
There is no breakdown of source besides the fact that 60% are urinary•
Is it possible that the mortality is equivalent for some infections but not others as shown in •
previous observational studies?
There is no breakdown of MIC for success and failure.•
If there is a MIC below which things are equivalent it might allow us to drop the breakpoint •
for P-T and still use it in low MIC infections
There was equipoise at the second interim analysis, but suddenly at the 3rd •
there was huge signal
So, what the hell happened between 2•
nd
and 3
rd
interim analyses?
“Even if you can’t use for BSI, it doesn’t mean you can’t use it when there isn’t a BSI” – Dr. Jennifer Grant April 2018
Harris P et al Abstract O1121 28
th
ECCMID April 2018, Madrid, Spain

So setting aside BSI & MERINO
Low MICs
Higher dose BLBLI
Cont. infusion
Transition to BLBLI
Use better BLI
Verify ESBL type
Pathogen issues
Source of BSI
Severity of illness
ANTIMICROBIAL RESISTANCE • CID 2017:64 (1 April) • 973
and gene acquisitions occur and what the predisposing host and environmental factors are.
A number of cephamycins are commercially available includ-ing cefoxitin, cefotetan, cefmetazole, flomoxef, and moxalactam. Unfortunately, clinical data evaluating cephamycins for ESBL infections are scarce, and data comparing the relative efficacy of the various cephamycins are virtually nonexistent. Existing observational studies comparing cephamycins and carbapen-ems are plagued by the inherent limitations of observational studies—most notably confounding by indication—as well as small sample sizes (Table 2) [15–20]. Only 1 of these studies showed improved outcomes among ESBL-infected patients
treated with carbapenems compared with cephamycins, while the others could not detect differences [18] (Table 3). Optimal dosing regimens and achievable target attainment for various cephamycin minimum inhibitory concentrations (MICs) need to be explored [21].
We believe that cephamycins may be useful agents in the treatment of nonsevere ESBL-producing infections from uri-nary sources. Given the limited data on nonurinary sources and severe infections, it is the opinion of the authors that the use of cephamycins for severe ESBL infections and those originating outside of the urinary tract should be avoided until more data are available.
CEFEPIME
Cefepime is an oxyimino-cephalosporin agent with enhanced stability against degradation by β-lactamases. The current European Committee on Antimicrobial Susceptibility Testing (EUCAST) and Clinical and Laboratory Standards Institute (CLSI) susceptibility breakpoints for cefepime are 1 µg/mL and 8 µg/mL (accounting for drug dosing), respectively [22, 23]. There is concern that the current CLSI cefepime breakpoint leaves some ESBL enzymes in the susceptible range (ie, “hidden resistance)” [24].
Concerns about the diminished efficacy of cefepime for the treatment of ESBL infections with higher bacterial inoc-ulums (eg, intra-abdominal infections, pneumonia, osteoar-ticular infections) have tempered enthusiasm for the use of cefepime for this indication. This so called “inoculum effect,” in which drug MICs increase dramatically in the presence of an increased bacterial load despite apparent initial susceptibility, has been observed in both in vitro and animal studies [25–31]. Highlighting one experience, Burgess and colleagues evaluated cefepime and meropenem against standard- and high-inoculum ESBL Klebsiella pneumoniae infections [32]. Each of these antibi-otics maintained bactericidal activity against standard inoculums but at high inoculums, in contrast to meropenem, cefepime was unable to sustain bactericidal activity against ESBL producers. In this same series of experiments, both agents maintained >99% killing of high-inoculum non-ESBL infections over a 24-hour observation period. The contribution of the inoculum effect toward treatment failures has not been the subject of com-prehensive clinical review.
Apart from the inoculum effect, an alternative explanation for poor outcomes associated with cefepime therapy relates to failure to meet necessary pharmacodynamic targets due to inadequate dosing and/or interval schedules [33]. A target of 50% free cepha-losporin drug concentration greater than the drug MIC (fT > MIC) has been identified as the quantitative exposure necessary for effective cephalosporin bactericidal activity [34]. Monte Carlo simulation is a mathematical tool that may be applied to integrat-ing multiple pharmacokinetic/pharmacodynamic (PK/PD) vari-ables to estimate the probability of target attainment for specific
Table 1. Potentially Favorable Circumstances for Noncarbapenem- β-Lactams in the Treatment of Extended-Spectrum β-Lactamase Infections
• What if noncarbapenem β-lactam minimum inhibitory concentrations are low?
• What if high-dose, frequent-interval βL-βLIs or cefepime is administered?
• What if extended-infusion noncarbapenem β-lactams are administered?• If carbapenem antibiotics are administered when the burden of bacteria
is highest, can therapy be transitioned to a noncarbapenem after a short period of time?
• If a βL-βLI is administered, does the type of β-lactamase inhibitor matter (eg, tazobactam, sulbactam, clavulanic acid, or avibactam)?
• Does it matter if the ESBL resistance mechanism is a blaTEM type, blaCTX-M type, or blaSHV type?
• Does the genus or species of the ESBL producer matter?• Does the source of bacteremia and if source control measures were taken
matter?• Should the severity of illness determine if a carbapenem or noncarbape-
nem agent is administered?
Abbreviations: βL-βLI, β-lactam–β-lactamase inhibitor; ESBL, extended-spectrum β-lactamase.
Table 2. Select Limitations of Existing Observational Studies Comparing Noncarbapenem β-Lactam Antibiotics and Carbapenems for the Treatment of Extended-Spectrum β-Lactamase Infections
• Inconsistent criteria for extended-spectrum β-lactamase production• Confounding by indication (ie, ill-appearing patients more likely to receive
the more “aggressive” therapy, ie, carbapenems)• Differences in outcomes definitions• Delays in initiating appropriate antibiotic therapy• Classification issues for patients initially receiving empiric noncarbapenem
β-lactam therapy, then transitioned to carbapenem therapy• Large proportions of patients receiving combination antibiotic therapy• Often single-center experiences• Sample sizes limit sufficient power to detect differences between treat-
ment approaches, if such differences exist• Insufficient subgroups for analysis (eg, proportion of Escherichia coli vs
Klebsiella pneumoniae, proportion of blaCTX-M vs blaSHV)• Disproportionate numbers of patients with low-inoculum and high-inocu-
lum infections• Differences in antibiotic susceptibility criteria utilized• Differences in local epidemiology of in vitro activity of noncarbapenem
β-lactams• Insufficient data on dosing regimens
• Insufficient data on clinical outcomes with extended-infusion β-lactam therapy
Downloaded from https://academic.oup.com/cid/article-abstract/64/7/972/2957271by Douglas Library useron 13 February 2018
Tamma & Rodriguez-BaňoClin Infect Dis 2017:64

ESBL GNB Infections commonly seen in practice
Urinary Tract
Biliary Tract
Wounds
BSI

ANTIMICROBIAL RESISTANCE • CID 2017:64 (1 April) • 977
Table 5.
Observa
tional S
tudies E
valuatin
g Clinic
al Outco
mes of P
atients w
ith Exten
ded-Spe
ctrum β
-Lactam
ase Bac
teremia
Compari
ng Treat
ment wi
th β-Lac
tam–β-L
actamas
e Inhibi
tors ver
sus Carb
apenem
s
Study
βL-βLI
Carbap
enem
Organis
m(s)
ESBL C
riteria a
nd βL-βL
I MIC
Distribu
tion, µg
/mLSou
rces of B
acterem
iaICU
Admissio
n at
Infectio
n Onse
tClin
ical Out
comes (
βL-βLI
vs carba
penems
)Sele
ct Limit
ationsa
Kang et
al [49]
n = 36
n = 78
Escheri
chia
coli (68
%),
Klebsiel
la pneu
-mon
iae (32%
)Not pro
vided
Sources
: not pr
ovided
Not pro
vided
Mortali
ty at 30
d: 22%
vs 27%
(ns)
Baselin
e compa
risons n
ot provi
ded
Rodrigu
ez-Baň
o et al
[47]
Empiric
cohort:
n =
72Defi
nitive co
hort:
n = 54
Empiric
coh
ort:
n = 31
Definitiv
e coh
ort:
n = 120
E. coli (
100%)
Molecu
lar detec
tionMIC
s: ≤1 (2
9%), 2
(23%), 4
(11%), 8
(17%), 16
(20%)
Source:
urinary
or biliar
y (70%
)13%
Mortali
ty at 30
d in
empiric
cohort:
10% vs
19% (ns
)Mo
rtality a
t 30 d in
defin-
itive coh
ort: 9%
vs 17%
(ns)
General
izability
to patie
nts infe
cted wit
h ESBL
bloodstr
eam infe
ctions f
rom hig
h-inocu
lum
sources
, elevate
d pipera
cillin MI
Cs, and
severe
infectio
ns not c
lear
Harris e
t al [50]
n = 24
(100%
4.5 g pe
r dose
PTZ)
n = 23
E. coli (
86%)
K. pneu
moniae
(14%)
Cefotax
ime
nonsus
ceptible
MICs: ≤
4 (71%
) and 8
(29%)
Sources
: urinary
(47%),
bilia
ry (9%)
15%Mo
rtality a
t 30 d: 8
% vs
17% (ns
)Mo
re immun
ocompr
omised
patient
s in car
bape-
nem gro
up, gen
eralizab
ility to p
atients
infected
with
ESBL
bloodstr
eam infe
ctions f
rom hig
h-in-
oculum
sources
, elevate
d pipera
cillin MI
Cs, and
sev
ere infe
ctions n
ot clear
Ofer-Fri
edman
et al [8]
n = 10
(dosing
regimen
s not
describ
ed)
n = 69
E. coli (
53%),
K. pneu
moniae
(28%), Pr
oteus
mirabilis
(19%)
Disk diff
usion
MICs: m
edian 8
Sources
: pneum
onia
(34%), sk
in and s
oft tiss
ue (28%
), biliary
(17%
), intra-a
bdomin
al (9%
)
>50%
Mortali
ty at 30
d: 60%
vs 34%
(P = .10
)Mo
rtality a
t 90 d: 8
0% vs
48% (P =
.03)
Endpoin
t of 90-
d morta
lity may
not be
represe
nta-tive
of morta
lity due
to poor
antibiot
ic treatm
ent cho
ices; do
sing not
describ
ed
Tamma
et al
[51]n =
103 (40
% rece
ived 4.5
g per
dose PT
Z)
n = 110
K. pneu
moniae
(68%), E.
coli
(31%), P.
mirabi-
lis (1%
)
Disk diff
usion
MICs: 2
(1%), 4
(39%),
8 (46%
), 16 (14
%)
Sources
: cathet
er (46%
), urin
ary (21%
), intra-a
b-dom
inal (17
%) bilia
ry (9%
), pneum
onia (9%
)
34%Mo
rtality a
t 14 d: 1
7% vs
8% (P <
.05)
Mortali
ty at 30
d: 26%
vs 11%
(P < .01
)
Only ~4
0% rec
eived 4.
5 g eve
ry 6 h; n
o patien
ts rece
ived ext
ended-i
nfusion
therapy
Ng et a
l [53]
Empiric
cohort:
n =
97 (~10
0%
4.5 g)
Empiric
coh
ort:
n = 57
E. coli (
67%),
K. pneu
moniae
(33%)
Resista
nce to
third-gen
eration
cephalo
sporins
MICs: n
ot provi
ded
Sources
: cathet
er (4%),
urin
ary (59%
), biliary
(9%
), pneum
onia (9%
), intra
-abdomi
nal (5%
)
9%Mo
rtality a
t 30 d: 3
1% vs
30% (ns
)PTZ
MIC d
istributi
on not p
rovided
; unclea
r what
proportio
n of infe
ctions w
ere due
to ESBL
prod
ucers
Gutiérre
z- Gut
iérrez
et al [52
]
Empiric c
ohort:
n = 170
(65%
received
4.5 g
per dos
e PTZ)
Definitiv
e cohort
: n =
92(83%
receive
d 4.5
g per do
se PTZ
)
Empiric
coh
ort:
n = 195
Definitiv
e coh
ort:
n = 509
E. coli (
73%),
K. pneu
moniae
(19%)
Elevated
cephalo
sporin
MICs w
ith molec
ular
confirm
ation of
~30%
of c
ohort
MICs: n
ot provi
ded
Sources
: urinary
(45%),
bilia
ry (12%
)11%
Mortali
ty at 30
d in
empiric
cohort:
18% vs
20% (ns
)Mo
rtality a
t 30 d in
defin-
itive coh
ort: 10%
vs 14%
(ns)
General
izability
to patie
nts infe
cted wit
h ESBL
bloodstr
eam infe
ctions f
rom hig
h-inocu
lum
sources
, elevate
d pipera
cillin MI
Cs, and
severe
infectio
ns not c
lear
Abbrevi
ations:
βL-βLI, β
-lactam
–β-lacta
mase in
hibitor;
ESBL,
extend
ed-spec
trum β-la
ctamase
; ICU, i
ntensive
care un
it; MIC,
minimu
m inhibi
tory con
centrat
ion; ns,
not sig
nificant;
PTZ, pip
eracillin-
tazobac
tam.
a Small s
ample s
ize, res
idual co
nfoundin
g, and c
onfound
ing by i
ndicatio
n are lim
itations
for all
include
d studie
s.
Downloaded from https://academic.oup.com/cid/article-abstract/64/7/972/2957271by Douglas Library useron 13 February 2018
Tamma & Rodriguez-Baňo Clin Infect Dis 2017:64

• 13 studies reporting empiric therapy with BLBLI vs. carbapenem for BSI• Mortality
• Carbapenem - 22.1%; BLBLI - 20.5%• RR 1.05 (CI 0.83-1.37, p=0.241)
• 7 studies reporting definitive therapy • Mortality
• RR 0.62 (CI 0.25-1.52, p<0.001)
Muhammed et al OFID 2017;4:ofx099, https://doi.org/10.1093/ofid/ofx099
Open Forum Infectious Diseases
BL/BLIs vs Carbapenems for ESBL-PE BSI • OFID • 1
Open Forum Infectious Diseases®
Comparison Between Carbapenems and β-Lactam/β-Lactamase Inhibitors in the Treatment for Bloodstream Infections Caused by Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae: A Systematic Review and Meta-AnalysisMaged Muhammed, Myrto Eleni Flokas, Marios Detsis, Michail Alevizakos, and Eleftherios Mylonakis
Infectious Diseases Division, Warren Alpert Medical School of Brown University, Rhode Island Hospital, Providence
Background. Carbapenems are widely used for the management of bloodstream infections (BSIs) caused by extended-spectrum β-lactamase-producing Enterobacteriaceae (ESBL-PE). However, the wide use of carbapenems has been associated with carbapen-em-resistant Enterobacteriaceae development.
Methods. We searched the PubMed and Scopus databases (last search date was on June 1, 2016) looking for studies that reported mortality in adult patients with ESBL-PE BSIs that were treated with carbapenems or β-lactam/β-lactamase inhibitors (BL/BLIs).
Results. Fourteen studies reported mortality data in adult patients with ESBL-PE BSI that were treated with carbapenems or BL/BLIs. Among them, 13 studies reported extractable data on empiric therapy, with no statistically significant difference in mortality of patients with ESBL-PE BSI that were treated empirically with carbapenems (22.1%; 121 of 547), compared with those that received empiric BL/BLIs (20.5%; 109 of 531; relative risk [RR], 1.05; 95% confidence interval [CI], 0.83–1.37; I2 = 20.7%; P = .241). In addi-tion, 7 studies reported data on definitive therapy. In total, 767 patients (79.3%) received carbapenems and 199 patients (20.6%) received BL/BLIs as definitive therapy, and there was again no statistically significant difference (RR, 0.62; 95% CI, 0.25–1.52; I2 = 84.6%; P < .001). Regarding specific pathogens, the use of empiric BL/BLIs in patients with BSI due to ESBL-Escherichia coli was not associated with a statistically significant difference in mortality (RR, 1.014; 95% CI, 0.491–2.095; I2 = 62.5%; P = .046), compared with the use of empiric carbapenems.
Conclusions. These data do not support the wide use of carbapenems as empiric therapy, and BL/BLIs might be effective agents for initial/empiric therapy for patients with BSI caused by likely ESBL-PE, and especially ESBL-E coli.
Keywords. β-lactam/β-lactamase inhibitor (BL/BLIs); bloodstream infection (BSI); carbapenems; extended-spectrum β-lacta-mase (ESBL).
The incidence of infections caused by extended-spectrum β-lactamase-producing Enterobacteriaceae (ESBL-PE) is increasing [1–3], and, according to a 2013 report from the US Centers of Disease Control and Prevention, 19% of healthcare-re-lated Enterobacteriaceae infections are caused by ESBL-PE [4]. Bloodstream infections (BSI) caused by ESBL-PE, in particular,
are associated with high mortality, prolonged hospital stay, and increased hospital costs [5, 6], and for these infections, carbap-enems are currently considered the first-line therapy [5, 7, 8]. However, the use of carbapenems has been linked to the devel-opment of carbapenem-resistant Enterobacteriaceae [8]. The efficacy of β-lactam/β-lactamase inhibitor (BL/BLIs) combina-tions, such as piperacillin/tazobactam, in ESBL-PE BSI treat-ment is reported, but it is controversial [9, 10]. We conducted a systematic review and meta-analysis to compare the empiric use of BL/BLIs with that of carbapenems for ESBL-PE BSI.
METHODS
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11].
Data Source and Searches
A systematic search of the PubMed and Scopus databases was conducted (last day of access: June 1, 2016), using the terms
M A J O R A R T I C L E
© The Author 2017. Published by Oxford University Press on behalf of Infectious Diseases Society of America. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs licence (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any medium, provided the original work is not altered or transformed in any way, and that the work is properly cited. For commercial re-use, please contact [email protected]: 10.1093/ofid/ofx099
Received 12 January 2017; editorial decision 3 May 2017; accepted 10 May 2017.Correspondence: E. Mylonakis, MD, PhD, FIDSA, Dean’s Professor of Medical Science
(Medicine, and Molecular Microbiology and Immunology), Chief Infectious Diseases Division, Warren Alpert Medical School of Brown University, Rhode Island Hospital, 593 Eddy Street, POB, 3rd Floor, Suite 328/330, Providence, RI 02903 ([email protected]).
Downloaded from https://academic.oup.com/ofid/article-abstract/4/2/ofx099/3828264by gueston 29 April 2018

8 Studies with unconfirmed BLBLI Susceptible Isolates
4 studies with confirmed BLBLI Susceptible Isolates
BL/BLIs vs Carbapenems for ESBL-PE BSI • OFID • 5
Study
Gutiérrez-Gutiérrez et al (2009)
Chaubey et al (2004)
Cheng et al (2006)
Gudiol et al (2007)
Kang et al (2009)
Lee et al (2005)
Metan et al (2005)
Ng et al (2012)
Qureshi et al (2007)
Rodriguez-Bano et al (2004)
To et al (2008)
Tumbarello et al (2002)
Overall (I-squared = 20.7%, p = 0.241)
.00741 1351
ID RR (95% CI)
1.13 (0.74, 1.74) 39/195 30/170
6/16 4.91
30.83
0/10
10/39 0/4 0.85
2/5 3/6 2.62
21/78 8/36 10.53
4/24 1/13 1.25
7/22 5/7 7.30
17/57 29/94 21.06
0/8 1/4
1/28
121/544
4/33
109/529
1.85
3.53
100.00
14/47 15/74 11.21
6/31 7/72 4.05
0.12 (0.01, 1.91)
2.63 (0.18, 38.30)
0.80 (0.21, 3.05)
1.21 (0.59, 2.47)
2.17 (0.27, 17.43)
0.45 (0.21, 0.96)
0.97 (0.59, 1.59)
0.19 (0.01, 3.75)
1.99 (0.73, 5.44)
1.47 (0.78, 2.76)
0.29 (0.03, 2.49)
1.05 (0.83, 1.33)
Events,
Treatment Control Weight
Events, %
Figure 2. Forest plot of included studies. Relative risk (RR) of mortality among patients with extended-spectrum β-lactamase-producing Enterobacteriaceae bloodstream infections that were treated with empiric carbapenems versus empiric β-lactam/β-lactamase inhibitors. Abbreviation: CI, confidence interval.
Study
Gudiol et al (2007)
Metan et al (2005)
Rodriguez-Bano et al (2004)
To et al (2008)
Overall (I-squared = 62.5%, p = 0.046)
.184 5.441
ID RR (95% CI)
17.18
28.22
0.80 (0.21, 3.05)
0.45 (0.21, 0.96)
23.061.99 (0.73, 5.44)
31.541.47 (0.78, 2.76)
100.001.01 (0.49, 2.10)
Weight
%
NOTE: Weights are from random effects analysis
Figure 3. Forest plot of included studies. Relative risk (RR) of mortality of patients with extended-spectrum β-lactamase Escherichia coli bloodstream infections that were treated with empiric carbapenems versus empiric β-lactam/β-lactamase inhibitors. Abbreviation: CI, confidence interval.
Downloaded from https://academic.oup.com/ofid/article-abstract/4/2/ofx099/3828264by gueston 29 April 2018
Muhammed et al OFID 2017;4:ofx099, https://doi.org/10.1093/ofid/ofx099
Favours BLBLIFavours Carbapenem

BLBLI MIC/Source of Infection MattersA single centre retrospective observational study Australia 2012• -2013 of 92 patients
79/92 (85.9%) • E. coli13/92 (14.1%) • K. pneumoniae
Definitive therapy in 47 patients•BLBLI n=24•Carbapenem n=23•
Urinary source 47%, biliary source 9%•ICU admission • – 15%No difference in mortality (8% vs. 17% NS)•
Harris et al Antimicrob Resist Infect Control (2015) 4:14-24
day where the patients did not fulfil SIRS criteria(as defined above). Patients were assumed to haveresolution of SIRS on the date of discharge (if theydid not have resolution of SIRS previously using theabove criteria). Patients who died were included inthe analysis, and defined as never having resolutionof SIRS. Where daily white cell count values weremissing, the value was imputed by calculating themidpoint difference between the adjacent day values.Patients for whom SIRS criteria could not beascertained due to missing data were excludedfrom this part of the analysis.
2. All-cause mortality at 30 days post initial positiveblood culture.
3. Identification of a carbapenem or piperacillin-tazobactam resistant isolate in subsequent 30 daysor identification of Clostridium difficile infection.
4. Microbiological relapse (positive blood culture >72 hafter initiation of definitive therapy and up to 30 days)with same organism as original initial blood culture.
5. Length of hospital stay post first positive blood culture.Patients who died were excluded from this analysis.
Microbiological testingBlood cultures were inoculated into BacT/Alert bottles(BioMerieux; Marcy-L’Étiole, France) and incubated forup to 5 days. Positive cultures were sub-cultured and iden-tified to species level by standard laboratory methods, in-cluding MALDI-TOF (Bruker Daltoniks GmHB; Bremen,Germany) and Vitek2 (BioMerieux). Susceptibility testingwas performed using Vitek2 microbroth dilution accord-ing to EUCAST interpretative standards [23]. Phenotypictesting or molecular methods were not routinely used toconfirm ESBL or plasmid-mediated AmpC beta-lactamaseproduction. Antibiotic reporting was at the discretion ofthe duty microbiologist at the time of the bloodstream
infection. All positive blood cultures reported within the30-day follow-up period were also recorded.
Statistical analysisCategorical data were presented as proportions and scaledata using median and interquartile ranges. Patients whoreceived carbapenems or BLBLIs as definitive monother-apy were identified and compared. Groups given othernon-carbapenem or non-BLBLI therapy and combinationtherapy were excluded. Survival curves for mortality, daysto resolution of SIRS, and length of hospital stay werepresented using Kaplan-Meier curves. Cox proportionalhazards regression was used to assess potential con-founders identified a priori (age, acquisition status, Pittbacteraemia score, ICU admission, organism, and whetheror not the patient had received appropriate empiricaltherapy). Potential confounders were included in the finalregression model if they caused a change in the main ef-fect (hazard ratio according to definitive treatment) by 5%or more when included in bivariate analysis with definitivetreatment. Statistical analysis was performed using Stata(StataCorp; Texas, USA).
Table 1 Susceptibility profiles of E. coli or K. pneumoniae isolated from blood cultures with resistance to ceftriaxoneduring study periodSusceptibility category Antimicrobial agent tested
E. coli AMP AMC TZP CXM CRO CTX CAZ FEP FOX IPM MEM ETP LVX CIP SXT GEN AMK
R (%) 100 60 0 100 100 100 96 0 11 0 0 0 71 71 59 35 0
I (%) 0 0 0 0 0 0 4 4 20 0 0 0 0 3 0 0 3
S (%) 0 40 100 0 0 0 0 96 68 100 100 100 29 27 41 65 97
Total tested 79 73 79 79 79 79 79 79 79 79 79 79 79 79 79 79 79
K. pneumoniae
R (%) 100 45 0 100 100 100 100 92 0 0 0 0 15 30 85 31 0
I (%) 0 0 0 0 0 0 0 8 8 0 0 0 0 40 0 0 0
S (%) 0 55 100 0 0 0 0 0 92 100 100 100 85 30 15 69 100
Total tested 13 11 13 13 13 13 13 13 13 13 13 13 13 10 13 13 13
R = resistant, I = intermediate, S = susceptible; AMP = ampicillin, AMC = amoxicillin-clavulanate, TZP = piperacillin-tazobactam, CXM = cefuroxime, CRO = ceftriaxone,CTX = cefotaxime, CAZ = ceftazidime, FEP = cefepime, FOX = cefoxitin, IMP = imipenem, MEM=meropenem, ETP = ertapenem, LVX = levofloxacin, CIP = ciprofloxacin,SXT = trimethoprim-sulphamethoxazole, GEN = gentamicin, AMK = amikacin.
Table 2 MIC distributions for cefotaxime-resistant andpiperacillin-tazobactam susceptible E. coli and K.pneumoniae from blood culture isolates tested by Vitek2AMC MIC N (%) FOX MIC N (%) TZP MIC N (%)
4 19 (21.8) <=4 60 (72.3) <=4 65 (70.7)
8 19.0 (21.8) 8 6 (7.2) 8.0 27.0 (29.3)
16 32 (36.8) 16 8 (9.6) - -
> = 32 17 (19.5) 32 9 (10.8) - -
- - > = 64 9 (10.8) - -
Total 87 83 92
AMC = amoxicillin-clavulanate, FOX = cefoxitin, TZP = piperacillin-tazobactam.
Harris et al. Antimicrobial Resistance and Infection Control (2015) 4:14 Page 4 of 10

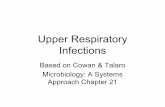
BLBLI MIC/Source of Infection MattersRetrospective cohort study of •empiric therapy of ESBL GNB BSI at single centre US 2007-14PTZ (n=103)•
61% received 3.375 g q6h•39% received 4.5 g q6h•
Carbapenem (n=110)•Meropenem (88%)•Imipenem• -cilastatin (4%)Ertapenem (8%)•
Primary outcome • – 14-day mortality ICU admission • – 34%
Sources•Central line• -associated – 46%Urinary • – 21%Intra• -abdominal – 17%Pneumonia • – 9%Biliary • – 9%
Tamma et al CID 2015;60:1391-1325
0%
10%
20%
30%
40%
50%
2 mg/L 4 mg/L 8 mg/L 16 mg/L
From: Tamma et al Clin Infect Dis. 2015;60(9):1319-1325
Carbapenem
PTZ
• 14-day mortality
• Adjusted HR for empiric
PTZ – 1.92 (CI 1.07-3.45,
p=0.03)
• Increased mortality
associated with:
• High Pitt bacteremia score
• ICU admission day one
• Empiric PTZ use
BLBLI MIC/Source of Infection Matters

ESBL GNB non-BSI InfectionsRetrospective study from India• 1
522 infections due to ESBL• -producing E. coli & K. pneumoniae287 (55%) were UTI•
Clinical success rates similar (p=0.15)•79.6% non• -carbapenem therapy (80% was cefoperazone-sulbactam)85.7% carbapenem therapy•
Retrospective review examining CLSI PTZ breakpoints• 2
6/6 patients with UTI due to • E. coli, Klebsiella sp. successfully treated with BLBLI therapy independent of PTZ MICIf PTZ MIC ≤16 mg/L, 10/11 (91%) patients with non• -UTI ESBL GNB infections were successfully treated with BLBLIIf PTZ >16 mg/L, only 1/5 (20% were successfully treated with BLBLI•
Trivedi M et al J 1. Assoc Physicians India 2012;60:28-30Gavin PJ et al AAC 2006;50:22442. -47

ESBL GNB UTIKorean RCT comparing PTZ vs. Ertapenem (vs. • cefipime) x 10-14 days for HCA UTI
23/33 PTZ (10 not tested) & 33/33 Ertapenem subjects had CTX• -M+66 subjects randomized to PTZ and ertapenem treatment groups•
Assignment to the cefepime treatment group was stopped because of an unexpectedly high •treatment failure rate
PTZ MICs between 4• -16 mg/L
two deaths. While the MIC of cefepime was 1 μg/mL or2 μg/mL, the successful cases all had an MIC of 2 μg/mL.The genotype was predominantly CTX-M-9, but one casewas detected as SHV-2. The genotype did not appear tosignificantly affect the success of treatment. In addition,age and Charlson comorbidity index did not seem to bedirectly related to clinical success. All mortality cases oc-curred under conditions of septic shock.In the PTZ group, treatment was successful except in
two cases (Table 4). In most cases, the MIC was 16 μg/mLand accounted for 72.7% of the total. Although the clinicaloutcome was satisfactory in most cases of 16 μg/mL MIC,all failure and mortality cases were in the 16 μg/mL MICgroup. Ten samples were lost during transport or over thecourse of the experiment. CTX-M-14, CTX-M-15, andCTX-M-27 were frequently observed. The genotypes ofthe mortality cases were CTX-M-15 or CTX-M-27.Similar to cefepime, the genotype seemed to be irrele-vant with respect to clinical outcome. Deaths tended to
be associated with septic shock with high Charlson co-morbidity index and high MIC.
DiscussionThis is the first randomized study comparing the efficacyof PTZ, cefepime, and ertapenem. Although the samplesize was small, results from the study showed that PTZwas as effective as ertapenem for the treatment ofESBL-EC UTI. Clinical and microbiological response toPTZ treatment was estimated to be 94%. Unexpectedly,the efficacy of cefepime was only 33.3%, suggesting thatcefepime is not an appropriate therapeutic alternativefor ESBL-EC UTI.ESBLs might be inhibited by beta-lactamase inhibitors;
thus, it is theoretically attractive to use BLBLI combina-tions to treat ESBL infections. In fact, a large, multicen-ter, prospective observational study has reported thatoutcomes using BLBLIs were comparable to those withcarbapenem in the treatment of ESBL-EC blood stream
Table 2 Demographic characteristics of study subjectsPiperacillin/tazobactam(N = 33)
Cefepime(N = 6)
Ertapenem(N = 33)
p-value
Age 68.8 ± 14.4 75.3 ± 6.6 65.2 ± 16.9 0.281
Female 30 (90.9) 3 (50.0) 26 (78.8) 0.049
Comorbidity, n (%)
Ischemic heart disease 0 (0) 0 (0) 1 (3.0) 1.000
Diabetes mellitus 12 (36.4) 1 (16.7) 15 (45.5) 0.474
Cerebrovascular accident 5 (15.2) 1 (16.7) 2 (6.1) 0.420
Dementia 3 (9.1) 0 (0) 2 (6.1) 1.000
Hemiplegia 2 (6.1) 0 (0) 2 (6.1) 1.000
Congestive heart failure 5 (15.2) 1 (16.7) 1 (3.0) 0.230
COPD 1 (3.0) 0 (0) 1 (3.0) 1.000
Chronic kidney disease 2 (6.1) 0 (0) 2 (6.1) 1.000
Liver cirrhosis 2 (6.1) 0 (0) 4 (12.1) 0.809
Solid tumor 6 (18.2) 1 (16.7) 7 (21.2) 1.000
Lymphoma 1 (3.0) 0 (0) 2 (6.1) 1.000
None 12 (36.4) 2 (33.3) 12 (36.4) 1.000
Charlson comorbidity index 4.7 ± 3.0 4.7 ± 1.0 4.5 ± 3.0 0.951
Bacteremia, n (%) 9 (27.3) 0 (0) 7 (21.2) 0.477
Septic shock, n (%) 9 (24.2) 2 (33.3) 11 (33.3) 0.928
APACH II score 12.9 ± 2.9 16.5 ± 6.4 16.6 ± 5.6 0.298
Table 3 Clinical and microbiological outcomes according to the antibiotic groupsPiperacillin/tazobactam(N = 33)
Cefepime(N = 6)
Ertapenem(N = 33)
p-value
Clinical success, n (%) 31 (93.9) 2 (33.3) 32 (97.0) <0.001
Microbiological success, n (%) 32 (97.0) 2 (33.3) 32 (97.0) <0.001
Clinical and microbiological success, n (%) 31 (93.9) 2 (33.3) 32 (97.0) <0.001
28-days mortality, n (%) 2 (6.1) 2 (33.3) 2 (6.1) 0.108
Seo et al. BMC Infectious Diseases (2017) 17:404 Page 4 of 9
Seo et al BMC Infectious Diseases 2017;17:404

Marion S. Helfand et al. J. Biol. Chem. 2003;278:52724-52729
Chemical structures of class A β-lactamase inhibitors

Does the Beta-lactamase inhibitor matter?Post• -hoc analysis of 6 published prospective cohorts of BSI due to ESBL E.coli Definitive therapy group n=174•
54 patients • – BLBLI (18 PTZ, 36 AMC) 30-Day Mortality – 9.3%120 patients • – Carbapenem (Imip 84, Mero 16, Erta 20) 30-Day Mortality – 16.7%
Empirical therapy group n=103•72 patients • – BLBLI (35 PTZ, 37 AMC)31 patients • – Carbapenem (Imip 22, Mero 8, Erta 1)
After adjusting for propensity score BLBLI (HR for increased mortality = 1.14 •95%CI 0.29-4.40, p=0.84)
Used high• -dose PTZ Most mortality was due to non• -urinary, non-biliary sources of infection
Rodríguez-Baño J et al Clin Infect Dis 2012;54:167–174

Does the GNB & Beta-lactamase inhibitor matter?
Tazobactam has increased activity ESBL• -producing E. coli compared with
ESBL-producing K. pneumoniae isolates1
Ceftolozane• -tazobactam MIC90
E. coli • - 4 mg/L
K. pneumoniae • - >32 mg/L
Sulbactam less effective•
Tazobactam and clavulanate similar efficacy• 2
at day 30 with respect to definitive therapy was as follows: 5.9%
(2/34) for those continuing to receive a BLBLI and 9.4% (3/32)
for those whose regimen was changed to a carbapenem (P 5 .6,
Fisher test); 2 of 6 patients (33.3%) whose treatment was
changed to another antimicrobial died. For patients empirically
treated with carbapenems who continued with carbapenem as
their definitive therapy, mortality was 16.7% (5/30 patients)
(P . .1 for comparison with previous groups); 1 patient whose
therapy changed to a fluoroquinolone died.
We calculated a propensity score for receiving empirical
therapy with a carbapenem by constructing a nonparsimonious
model using logistic regression. From the crude comparison
results of patients empirically treated with BLBLI and carbape-
nems (Table 2), the following variables were introduced into the
model: age, sex, Charlson index, nosocomial acquisition, Pitt
score, neutropenia, cancer, diabetes mellitus, urinary tract dis-
ease, chronic renal insufficiency, source, and presentation with
severe sepsis or shock. The model showed a P value of .53 for
the Hosmer-Lemeshow goodness-of-fit test and an area under
the receiver operating characteristic curve of 0.80, showing good
Table 2. Characteristics of Patients With Bloodstream Infections (BSIs) Caused by Extended-Spectrum b-Lactamase–ProducingEscherichia coli, According to Therapya
Empirical Therapy Cohort Definitive Therapy Cohort
Characteristic BLBLI (n 5 72) Carbapenem (n 5 31) P BLBLI (n 5 54) Carbapenem (n 5 120) P
Age, median y (IQR) 69 (59–80) 60 (52–78) .1b 67 (56–83) 70 (55–78) .3b
Male sex 29 (40.3) 11 (35.5) .6 34 (63) 70 (58.3) .5
Nosocomial acquisition 26 (36.1) 24 (77.4) ,.001 18 (33.3) 67 (55.8) .006
Charlson index, median, (IQR) 2 (1–5) 2 (1–5) .6b 2.5 (1–5) 3 (1–5) .5b
Cancer 21 (31.9) 11 (35.5) .7 15 (27.8) 43 (35.8) .2
Immunosuppression 5 (6.9) 5 (16.1) .1c 3 (5.6) 15 (12.5) .1
Neutropenia 2 (2.8) 3 (9.7) .1c 0 7 (5.8) .1c
Urinary or biliary tract as source 52 (72.2) 18 (58.1) .1 42 (77.8) 79 (65.8) .1
ICU admission 7 (9.9) 2 (6.7) .7c 4 (7.4) 18 (15.4) .1
Severe sepsis or shock at presentation 14 (19.4) 9 (29.0) .2 8 (14.8) 32 (26.7) .08
Pitt score, median (IQR) 1 (0–2) 1 (0–2) .7b 1 (0–2) 1 (1–2) .04b
CTX-M enzyme 57 (80.3) 25 (86.2) .4 43 (82.7) 95 (81.2) .8
Definitive therapy
Carbapenem 32 (44.4) 30 (93.7) ,.001 . . .
BLBLI 34d (47.2) 0 ,.001 . . .
Empirical therapy
Carbapenem . . . 0 30 (25) ,.001
BLBLI . . . 45d (83.3) 38 (31.7) ,.001
Cephalosporins . . . 7 (13) 39 (32.5) .006
Fluoroquinolones . . . 2 (3.7) 13 (10.8) .1c
Appropriate empirical therapy . . . 34 (63) 64 (53.3) .2
Mortality, no. of deaths
Day 7 2 (2.8) 3 (9.7) .1c 1 (1.9) 5 (4.2) .6c
Day 14 7 (9.7) 5 (16.1) .3 3 (5.6) 14 (11.7) .2
Day 30 7 (9.7) 6 (19.4) .1 5 (9.3) 20 (16.7) .1
Hospital stay after BSI , median (IQR), d 12 (8–28) 13 (9–25) .7b 13 (8–22) 13 (10–25) .04b
a Except where otherwise specified, data represent No. (%) of patients. P values were calculated by v2 test, except where otherwise specified. BLBLI, b-lactam/b-lactamase inhibitor association; ICU, intensive care unit; IQR, interquartile range.b Mann-Whitney test.c Fisher test.d The number of patients empirically treated with BLBLI are different in both cohorts because empirical therapy with these drugs was inappropriate in 11 patients inthe Definitive Therapy Cohort, who thus could not be included in the Empirical Therapy Cohort.
Table 3. Mortality at 30 Days in Patients Who Received EmpiricalTherapy With an Active b-Lactam/b-Lactam Inhibitor, According toMinimum Inhibitory Concentration of the Antimicrobial Useda
Antimicrobial
Minimum Inhibitory Concentration, mg/L
#1 2 4 8 16
Piperacillin-tazobactam 0/10 0/8 1/4 2/6 1/7
Amoxicillin-clavulanate . . 1/12 2/25 .
a Data are expressed as No. of patients who died/No. of patients treated.
170 d CID 2012:54 (15 January) d Rodrıguez-Bano et al
Downloaded from https://academic.oup.com/cid/article-abstract/54/2/167/469779by gueston 30 April 2018
1. Farrell DJ et al AAC 2013;57:6305-10
2. Rodríguez-Baño J et al Clin Infect Dis 2012;54:167–174

Inoculum
Effect with
BLBLIs
other four kinds of β–lactam agents against CTX-M-ESBL-producing Escherichia coli.
MethodsEighty non-replicate strains of Escherichia coli, identifiedusing the Vitek 2 system (bioMérieux S.A., Marcy I’Etoile,France), were investigated in this study. The isolates wereselected from a collection of clinical isolates of patientsfrom the First Hospital of China Medical University. ESBLproduction was confirmed phenotypically using double-disc diffusion tests with ceftazidime with/without clavula-nic acid and cefotaxime with/without clavulanic acid.β-lactamases produced by isolates were characterized byPCR gene sequencing, including CTX-M-14, CTX-M-15,CTX-M-22, CTX-M-24 and CTX-M-79 (as reported byour previous study [9]). Escherichia coli ATCC25922 wasused as the quality control strain for susceptibility testing.This study was approved by the Ethics Committee of ourhospital (Approval number, 2013114) and conducted inaccordance with the ethical guidelines of the Declarationof Helsinki.MICs were determined by the broth microdilution
method in accordance with CLSI (2010) recommenda-tions [1]. Susceptibility testing was performed using in-oculum concentrations of approximately 1–5 × 105 CFU/ml (the standard inoculum) and 1–5 × 107 CFU/ml (thehigher inoculum). Inoculum concentrations were esti-mated by optical density measurement and verified byquantitative subculture. An inoculum effect was definedas an eightfold or greater increase in MIC when testedwith the high inoculum [5]. Comparision betweent CTX-M-14-group and other-genotype-group were performedby chi-square test using SPSS16.0. P value of < 0.05 wereconsidered statistically significant. Antimicrobial agentsmeropenem, cefminox, piperacillin/tazobactam (tazobac-tam 4 μg/ml), cefepime, ceftazidime and cefotaxime (ob-tained from the National Institute for the Control ofPharmaceutical and Biological Products) were tested.
ResultsThe strains were isolated from blood (n = 40), urine (n =25), ascites (n = 7), bile (n = 5) and pus (n = 3). The se-quence analysis of lactamase-producing organisms de-tected the ESBL genotypes CTX-M-14 (n = 44), CTX-M-15 (n = 8), CTX-M-22 (n = 12), CTX-M-24 (n = 4) andCTX-M-79 (n = 12). At the standard inoculum, the MICsof cefotaxime were higher than the MICs of cefepime andceftazidime against all CTX-M strains (Table 1). TheMICs of meropenem and cefminox were very low and lessaffected by the inoculum. An inoculum effect on piperacil-lin/tazobactam was observed in only 4 strains, all geno-type CTX-M-14. The MIC50 of ceftazidime was 4 μg/mlat the low inoculum and 35% (28/80) of strains showed aninoculum effect at the high inoculum (all 28 strains weregenotype CTX-M-14). An inoculum effect on cefepimewas observed for 85% (68/80) of isolates, the frequenciesof this inoculum effect, by genotype were CTX-M-14, 40/44; CTX-M-15, 8/8; CTX-M-22, 12/12; CTX-M-24, 4/4;and CTX-M-79, 4/12.
DiscussionThe production of ESBLs is the predominant cause ofresistance to β-lactam antibiotics in gram-negative bac-teria. However, the antimicrobial substrate specificitiesof different phenotypes of ESBLs vary. The commonphenotypes of the ESBL enzymes are TEM, SHV, CTX-M and others. More recently, the CTX-M β-lactamases,which have potent hydrolytic activity against cefotax-ime, have been the most widespread β-lactamases inAsia, especially in China. Therefore, we studied strainscontaining CTX-M-encoded genes to explore their pre-sumptive role as a cause of therapeutic failure. In thisstudy, the isolates contained CTX-M-14, CTX-M-22,CTX-M-15, CTX-M-24 and CTX-M-79 encoding genes.CTX-M-14 is the most common genotype in our area.CTX-M-79 was first reported by Su Fei Tian et al. inour previous study [9].
Table 1 The inoculum effects on six antimicrobial agents for 80 strains of Escherichia coli at standard andhigh-inoculumAntimicrobial agent MIC (μg/ml) at standard and high inoculum Number of strains showing
an inoculum effectEscherichia coliATCC25922Standard inoculum High inoculum
(1–5 × 105 CFU/ml inoculum) (1–5 × 107 CFU/ml inoculum)
Range MIC50 MIC90 Range MIC50 MIC90
Meropenem ≤0.015 ~ 0.06 0.03 0.03 0.03 ~ 0.06 0.03 0.06 0 ≤0.015
Cefminox 0.5 ~ 4 1 2 0.5 ~ 8 2 4 0 2
Piperacillin/tazobactam 4 ~ 32 8 32 8 ~ 256 8 64 4 2
Ceftazidime 1 ~ 32 4 16 8 ~ 128 32 64 28 0.25
Cefepime 4 ~ 32 8 32 32~ > 512 512 >512 68 0.12
Cefotaxime 16 ~ 256 64 256 128~ > 512 512 >512 80 0.12
Wu et al. Annals of Clinical Microbiology and Antimicrobials 2014, 13:45 Page 2 of 4http://www.ann-clinmicrob.com/content/13/1/45
Wu N et al Wu et al. Ann 1. Clin Microbiol Antimicrobials 2014;13:45
Lopez2. -Cerero et al Clin Microbiol Infect 2010;16:132–136
two inhibitor combinations are very similar. Additionally,
when the inoculum was increased 100-fold, amoxycillin and
amoxycillin–clavulanate achieved 99.9% killing at 8 h and
24 h, whereas piperacillin and piperacillin–tazobactam
showed decreases of <1 log10 CFU/mL (Fig. 1).
Studies with ESBL-producing E. coli
Table 2 compares the variations in the MIC values of the
two b-lactam–b-lactamase inhibitors when the bacterial load
of ESBL producers was increased 100-fold. At a high inocu-
lum, a ‡8-fold increase in MIC was found for piperacillin–
tazobactam in broth (mean of 87-fold at the 8 : 1 ratio and
221-fold at 4 mg/L of tazobactam) and in agar (mean of
17-fold (8 : 1) and 168-fold (4 mg/L tazobactam)) with all the
strains. When the inoculum was increased, the MICs of
piperacillin–tazobactam were ‡256 mg/L for 90% (at the
8 : 1 ratio) and 97% (at 4 mg/L of tazobactam) of the strains.
On the other hand, neither combination of amoxycillin–
clavulanate appeared to be affected by a 100-fold inoculum
increase, the MICs increasing <8-fold in all cases with the
broth and agar methods. With the highest inoculum,
six (20%) and seven (23%) strains achieved MIC values
of 16 mg/L for amoxycillin–clavulanate 2 : 1, and 15 (50%) and
16 (53%) strains for amoxycillin–clavulanate 4 : 1, with the
FIG. 1. Time-kill curves of E. coli ATCC 25922
at high inoculum for AMC (a) and PTZ (b);
and time-kill curves of ESBL-producers at
standard inoculum with 8 · AMC MIC (c) and
· 8 PTZ MIC (d), and at high inoculum with
8 · AMC MIC (e) and 8 · PTZ MIC (f). Filled
diamonds, CTX-M-14-producing strain; open
squares, TEM-3-producing strain; open circles,
SHV-12-producing strain; double cross, 2 ·MIC; cross, 4 · MIC; cross, 8 · MIC; broken
line, lower limit of detection.
TABLE 2. MICs of b-lactam–b-lactamase inhibitors for both clinical and transconjugant extended-spectrum b-lactamase-pro-
ducing Escherichia coli strains determined with two bacterial inocula
Type of b-lactamase
MIC (mg/L) of antimicrobial combinations
Amoxycillin–clavulanate Piperacillin–tazobactam
2 : 1 4 : 1 8 : 1 Tazobactam 4 mg/L
S H S H S H S H
CTX-M group 2–16 4–16 4–8 4–16 1–8 16 fi 256 1–4 64–256SHV group 4–16 4–16 4–16 4–16 1–16 64 fi 256 1–8 64–256TEM group 4–8 8–16 4–8 8–16 4–16 64 fi 256 1–4 256
S, standard inoculum for every method according to CLSI guidelines; H, 100-fold standard inoculum.
134 Clinical Microbiology and Infection, Volume 16 Number 2, February 2010 CMI
ª2009 The Authors
Journal Compilation ª2009 European Society of Clinical Microbiology and Infectious Diseases, CMI, 16, 132–136

ConclusionThe data supports the use of BLBLIs in • select infections due to ESBL-producing GNBsHere’s when you can use them:•
The patient is not critically ill 1.
Low inoculum infections: Urinary or Biliary source2.
E.coli 3. is the pathogenIn vitro 4. MIC for piperacillin-tazobactam is ≤4 mg/LIf available, confirmation of ESBL type5.
TEM or SHV • – No worriesCTX• -M – Caution

Why just believe me?1. The decision to use PTZ to treat an infection with an ESBL-GNR requires consideration of
the source of the infection, the severity of the infection, the identity of the organism, the MIC of the organism, and the dosage of antibiotic used
2. PTZ may be effective for treating invasive ESBL-GNR infections in patients who are not critically ill and who have a lower inoculum of infection and a lower MIC (≤2 mg/L)
3. The strongest data supporting the use of a BLBLI for treating infections caused by ESBL-GNR are those from urinary tract infections and biliary tract infections
4. Therapy using BLBLIs appears to be less effective than carbapenem therapy for bloodstream infections due to ESBL-GNR.
5. If PTZ is used for these infections, the laboratory should report MIC data and perform ESBL confirmatory testing to provide clinicians with optimal information for clinical decisions
6. Laboratories that perform ESBL confirmatory testing should consider inclusion of a comment indicating that PTZ therapy may be inadequate for treating blood- stream infections or other serious infections.
Source: Schuetz AN, Reyes S, Tamma PD J Clin Micro 2018;56:1-7

A straight-forward decision for the house…
versus