
Morphometric Analysis of Proximal End of the Tibia fileProximal End Morphometry of the Tibia Ahmad...
5
THIEME 82 Original Article Morphometric Analysis of Proximal End of the Tibia Nadia Ahmad 1 Deepa Singh 1 Aksh Dubey 1 S. L. Jethani 1 1 Department of Anatomy, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India Address for correspondence Deepa Singh, MBBS, MD (Anat), Department of Anatomy, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India (e-mail: [email protected]). Background Total knee arthroplasty and unicompartmental knee arthroplasty are frequently done procedures for the treatment of various forms of arthritis and knee injuries. The knee prosthesis, which is used for these procedures, requires adequate sizing specific to the population. Morphometric parameters of upper end of the tibia can be used to guide treatment and monitor outcome of total knee replacement surgeries. Information regarding morphometry of upper end of the tibia is important as it provides reliable method of assessing knee deformity. This article assesses differ- ent morphometric parameters of condylar and intercondylar surface of the tibia and to compile the results, analyze, and formulate a baseline data for future studies with relevance to Indian population. Materials and Methods The study group comprised of 60 adult human dry and processed tibia of both sides which are grossly normal and complete, obtained from the Department of Anatomy, Himalayan Institute of Medical Sciences. Morphometric measurements of the medial condyle, lateral condyle, and intercondylar area of tibia were recorded with vernier calipers with a least count of 0.01 mm. The dimensions were summarized as mean ± standard deviation. A p-value of < 0.05 was considered significant. Result Mediolateral and anteroposterior length were 66.33 and 42.52 mm, respectively. Conclusion Anatomical profile of tibial condyle for Indians is smaller, hence high- lighting the need for sizing of prosthesis specific to the population in question. Abstract Keywords ► morphometry ► proximal end of tibia ► tibial condyles Natl J Clin Anat 2019;8:82–86 DOI https://doi.org/ 10.1055/s-0039-1688529 ISSN 2277-4025. ©2019 Society of Clinical Anatomists Introduction The knee joint is a complex synovial joint which plays an important role in adjusting the center of body mass and posture, requiring a great range of movement in three dimensions together with the ability to withstand high forces. It is essential for everyday activities such as standing, walking, and climbing stairs and is also the main joint involved in running, jumping, kicking, and changing directions. Interactions between the articular surfaces, the passive stabilizers, and the muscles that cross the joint are responsible for maintaining range of mobility and stability at the same time. 1 The proximal end of the tibia articulates with the distal end of the femur (tibiofemoral articulation), this plays a key role in transmission of body weight from the femur above to the talus below and is hence irreplaceable in day-to-day functioning. The knee joint is commonly affected by different forms of arthritis such as inflammatory and posttraumatic arthritis among which osteoarthritis is the most common pathological condition that may require interventional procedures such as total knee arthroplasty (TKA) or unilateral knee arthroplasty (UKA). 2 TKA is a precision surgery, that requires an accurate soft tissue balancing and resection of bone thickness equal to the thickness of the prosthetic component implanted, so that the flexion–extension spacing are equal. This would allow joint stability throughout the range of motion. Selection of the prosthesis, accurate sizing, and proper placement of Published online: 26.06.2019
Transcript of Morphometric Analysis of Proximal End of the Tibia fileProximal End Morphometry of the Tibia Ahmad...

THIEME
82 Original Article
Morphometric Analysis of Proximal End of the TibiaNadia Ahmad1 Deepa Singh1 Aksh Dubey1 S. L. Jethani1
1Department of Anatomy, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India
Address for correspondence Deepa Singh, MBBS, MD (Anat), Department of Anatomy, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India (e-mail: [email protected]).
Background Total knee arthroplasty and unicompartmental knee arthroplasty are frequently done procedures for the treatment of various forms of arthritis and knee injuries. The knee prosthesis, which is used for these procedures, requires adequate sizing specific to the population. Morphometric parameters of upper end of the tibia can be used to guide treatment and monitor outcome of total knee replacement surgeries. Information regarding morphometry of upper end of the tibia is important as it provides reliable method of assessing knee deformity. This article assesses differ-ent morphometric parameters of condylar and intercondylar surface of the tibia and to compile the results, analyze, and formulate a baseline data for future studies with relevance to Indian population.Materials and Methods The study group comprised of 60 adult human dry and processed tibia of both sides which are grossly normal and complete, obtained from the Department of Anatomy, Himalayan Institute of Medical Sciences. Morphometric measurements of the medial condyle, lateral condyle, and intercondylar area of tibia were recorded with vernier calipers with a least count of 0.01 mm. The dimensions were summarized as mean ± standard deviation. A p-value of < 0.05 was considered significant.Result Mediolateral and anteroposterior length were 66.33 and 42.52 mm, respectively.Conclusion Anatomical profile of tibial condyle for Indians is smaller, hence high-lighting the need for sizing of prosthesis specific to the population in question.
Abstract
Keywords ►morphometry ►proximal end of tibia ► tibial condyles
Natl J Clin Anat 2019;8:82–86
DOI https://doi.org/ 10.1055/s-0039-1688529 ISSN 2277-4025.
©2019 Society of Clinical Anatomists
IntroductionThe knee joint is a complex synovial joint which plays an important role in adjusting the center of body mass and posture, requiring a great range of movement in three dimensions together with the ability to withstand high forces. It is essential for everyday activities such as standing, walking, and climbing stairs and is also the main joint involved in running, jumping, kicking, and changing directions. Interactions between the articular surfaces, the passive stabilizers, and the muscles that cross the joint are responsible for maintaining range of mobility and stability at the same time.1
The proximal end of the tibia articulates with the distal end of the femur (tibiofemoral articulation), this plays a key
role in transmission of body weight from the femur above to the talus below and is hence irreplaceable in day-to-day functioning.
The knee joint is commonly affected by different forms of arthritis such as inflammatory and posttraumatic arthritis among which osteoarthritis is the most common pathological condition that may require interventional procedures such as total knee arthroplasty (TKA) or unilateral knee arthroplasty (UKA).2
TKA is a precision surgery, that requires an accurate soft tissue balancing and resection of bone thickness equal to the thickness of the prosthetic component implanted, so that the flexion–extension spacing are equal. This would allow joint stability throughout the range of motion. Selection of the prosthesis, accurate sizing, and proper placement of
Published online: 26.06.2019
83Proximal End Morphometry of the Tibia Ahmad et al.
National Journal of Clinical Anatomy Vol. 8 No. 2/2019
the components determine the success of this procedure. The anteroposterior (AP) dimension of the prosthesis is important in maintaining the flexion–extension spacing, while the mediolateral length (ML) determines the ade-quate coverage of the resected bone surface, and tension-free wound closure.3 Maximal implant coverage on the resected bone surface would reduce the stress applied to the bone implant interface which has been found to be a factor con-tributing to long-term survivorship in TKA.4 An insufficient tibial coverage can lead to tibial implant collapse because of the load being transferred to the cancellous bone instead of the cortical bone.5
UKA has currently emerged as a favorable option for the treatment of unicompartmental arthritis of the knee in elderly patients, more commonly involving the medial compartment. This is so because osteoarthritis of the knee usually affects the medial compartment of the tibiofemoral articulation and it may later involve the lateral compart-ment.6 Advantages of UKA are shorter rehabilitation time, greater postoperative range of motion, and preservation of the proprioceptive function of the cruciate ligaments over TKA. However, studies have shown better outcome for TKA as compared with UKA.7 Indians and Chinese, as a part of the Asian subpopulation, have a smaller build and stature as compared with the Western population. Since there is a large variability in the anthropometry of different populations of the world, the prosthesis that are currently available in the market are best suited for the Western and Caucasian popu-lation. In that case, it is quite likely that ethnic groups such as Indians may be at risk of component oversizing in both UKA and TKA with most of the commercially available prosthesis.8
There have been very few studies on the anthropometry of the proximal tibia in the Indian population. Thus, we aimed to measure the various morphometric dimensions of condylar and intercondylar areas of the proximal end of the tibia and the results obtained from this study would provide valuable data on the average dimensions that would serve as guidelines for designing a suitable tibial component of total knee prosthesis for the Indian population.
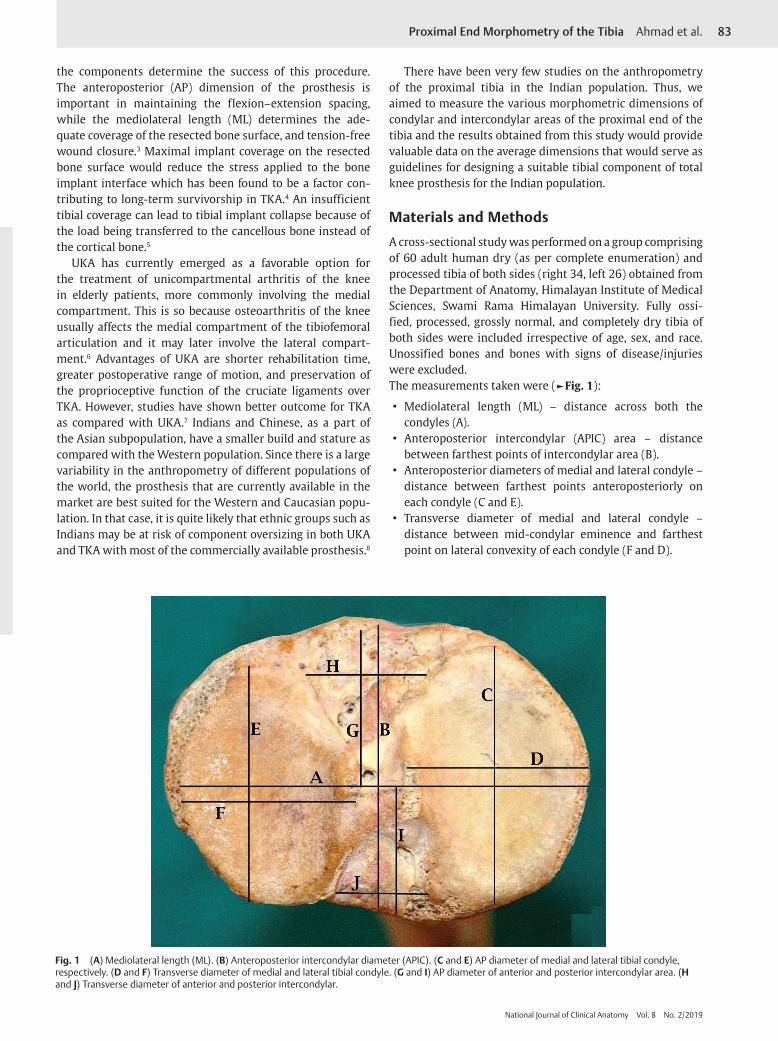
Materials and MethodsA cross-sectional study was performed on a group comprising of 60 adult human dry (as per complete enumeration) and processed tibia of both sides (right 34, left 26) obtained from the Department of Anatomy, Himalayan Institute of Medical Sciences, Swami Rama Himalayan University. Fully ossi-fied, processed, grossly normal, and completely dry tibia of both sides were included irrespective of age, sex, and race. Unossified bones and bones with signs of disease/injuries were excluded.The measurements taken were (►Fig. 1):
• Mediolateral length (ML) – distance across both the condyles (A).
• Anteroposterior intercondylar (APIC) area – distance between farthest points of intercondylar area (B).
• Anteroposterior diameters of medial and lateral condyle – distance between farthest points anteroposteriorly on each condyle (C and E).
• Transverse diameter of medial and lateral condyle – distance between mid-condylar eminence and farthest point on lateral convexity of each condyle (F and D).
Fig. 1 (A) Mediolateral length (ML). (B) Anteroposterior intercondylar diameter (APIC). (C and E) AP diameter of medial and lateral tibial condyle, respectively. (D and F) Transverse diameter of medial and lateral tibial condyle. (G and I) AP diameter of anterior and posterior intercondylar area. (H and J) Transverse diameter of anterior and posterior intercondylar.
84 Proximal End Morphometry of the Tibia Ahmad et al.
National Journal of Clinical Anatomy Vol. 8 No. 2/2019
• Intercondylar (IC) region was further divided into anterior and posterior areas
i. AP diameter of anterior and posterior IC region – distance from mid-point of IC eminence to farthest point anteriorly and posteriorly respectively (G and I).
ii. Transverse diameter of anterior and posterior IC region – maximum transverse distance in the IC region anteriorly and posteriorly (H and J).
All the measurements were taken with the help of vernier calipers. Aspect ratio (ML/AP × 100) was also calculated. Statistical analysis was performed using Student’s t-test by using SPSS for Windows (version 20.0, SPSS). The dimensions were summarized as mean ± standard deviation. A p-value of < 0.05 was considered statistically significant.
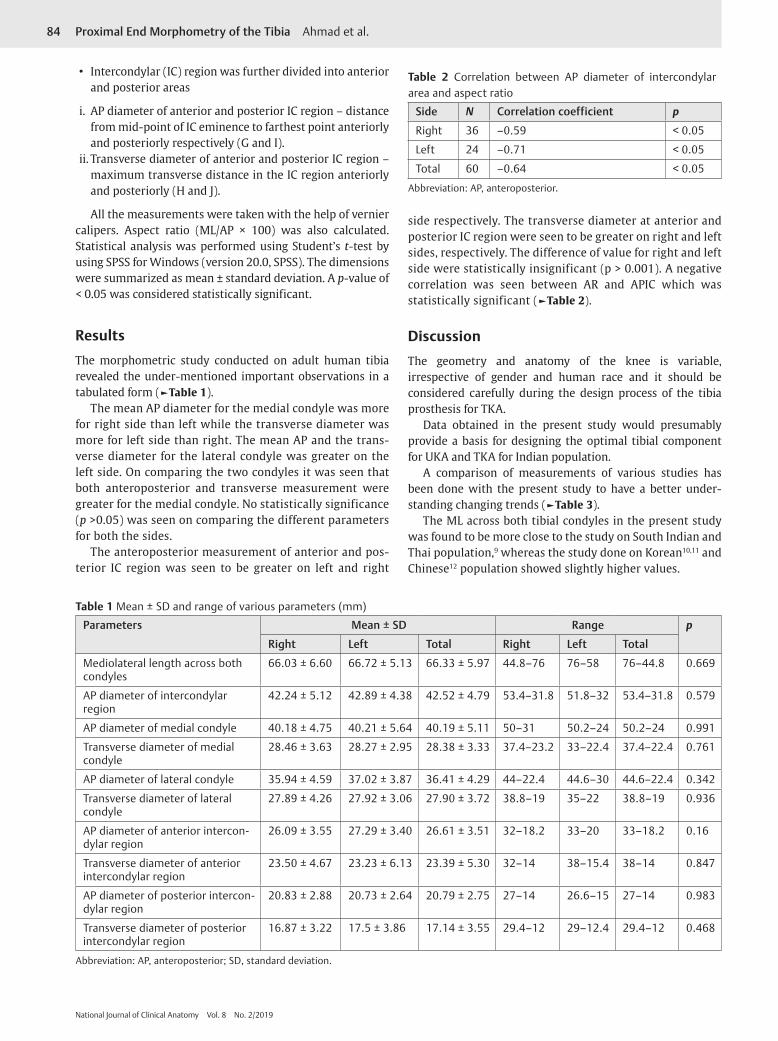
ResultsThe morphometric study conducted on adult human tibia revealed the under-mentioned important observations in a tabulated form (►Table 1).
The mean AP diameter for the medial condyle was more for right side than left while the transverse diameter was more for left side than right. The mean AP and the trans-verse diameter for the lateral condyle was greater on the left side. On comparing the two condyles it was seen that both anteroposterior and transverse measurement were greater for the medial condyle. No statistically significance (p >0.05) was seen on comparing the different parameters for both the sides.
The anteroposterior measurement of anterior and pos-terior IC region was seen to be greater on left and right
side respectively. The transverse diameter at anterior and posterior IC region were seen to be greater on right and left sides, respectively. The difference of value for right and left side were statistically insignificant (p > 0.001). A negative correlation was seen between AR and APIC which was statistically significant (►Table 2).
DiscussionThe geometry and anatomy of the knee is variable, irrespective of gender and human race and it should be considered carefully during the design process of the tibia prosthesis for TKA.
Data obtained in the present study would presumably provide a basis for designing the optimal tibial component for UKA and TKA for Indian population.
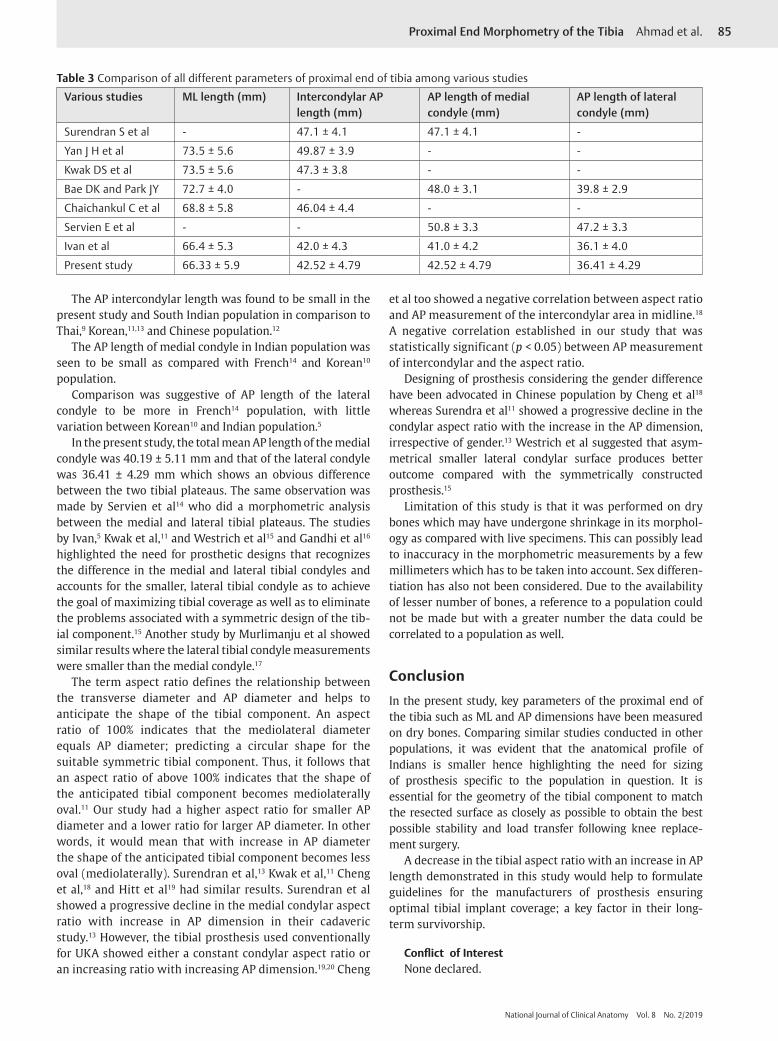
A comparison of measurements of various studies has been done with the present study to have a better under-standing changing trends (►Table 3).
The ML across both tibial condyles in the present study was found to be more close to the study on South Indian and Thai population,9 whereas the study done on Korean10,11 and Chinese12 population showed slightly higher values.
Table 1 Mean ± SD and range of various parameters (mm)
Parameters Mean ± SD Range p
Right Left Total Right Left Total
Mediolateral length across both condyles
66.03 ± 6.60 66.72 ± 5.13 66.33 ± 5.97 44.8–76 76–58 76–44.8 0.669
AP diameter of intercondylar region
42.24 ± 5.12 42.89 ± 4.38 42.52 ± 4.79 53.4–31.8 51.8–32 53.4–31.8 0.579
AP diameter of medial condyle 40.18 ± 4.75 40.21 ± 5.64 40.19 ± 5.11 50–31 50.2–24 50.2–24 0.991
Transverse diameter of medial condyle
28.46 ± 3.63 28.27 ± 2.95 28.38 ± 3.33 37.4–23.2 33–22.4 37.4–22.4 0.761
AP diameter of lateral condyle 35.94 ± 4.59 37.02 ± 3.87 36.41 ± 4.29 44–22.4 44.6–30 44.6–22.4 0.342
Transverse diameter of lateral condyle
27.89 ± 4.26 27.92 ± 3.06 27.90 ± 3.72 38.8–19 35–22 38.8–19 0.936
AP diameter of anterior intercon-dylar region
26.09 ± 3.55 27.29 ± 3.40 26.61 ± 3.51 32–18.2 33–20 33–18.2 0.16
Transverse diameter of anterior intercondylar region
23.50 ± 4.67 23.23 ± 6.13 23.39 ± 5.30 32–14 38–15.4 38–14 0.847
AP diameter of posterior intercon-dylar region
20.83 ± 2.88 20.73 ± 2.64 20.79 ± 2.75 27–14 26.6–15 27–14 0.983
Transverse diameter of posterior intercondylar region
16.87 ± 3.22 17.5 ± 3.86 17.14 ± 3.55 29.4–12 29–12.4 29.4–12 0.468
Abbreviation: AP, anteroposterior; SD, standard deviation.
Table 2 Correlation between AP diameter of intercondylar area and aspect ratio
Side N Correlation coefficient p
Right 36 –0.59 < 0.05
Left 24 –0.71 < 0.05
Total 60 –0.64 < 0.05
Abbreviation: AP, anteroposterior.
85Proximal End Morphometry of the Tibia Ahmad et al.
National Journal of Clinical Anatomy Vol. 8 No. 2/2019
et al too showed a negative correlation between aspect ratio and AP measurement of the intercondylar area in midline.18 A negative correlation established in our study that was statistically significant (p < 0.05) between AP measurement of intercondylar and the aspect ratio.
Designing of prosthesis considering the gender difference have been advocated in Chinese population by Cheng et al18 whereas Surendra et al11 showed a progressive decline in the condylar aspect ratio with the increase in the AP dimension, irrespective of gender.13 Westrich et al suggested that asym-metrical smaller lateral condylar surface produces better outcome compared with the symmetrically constructed prosthesis.15
Limitation of this study is that it was performed on dry bones which may have undergone shrinkage in its morphol-ogy as compared with live specimens. This can possibly lead to inaccuracy in the morphometric measurements by a few millimeters which has to be taken into account. Sex differen-tiation has also not been considered. Due to the availability of lesser number of bones, a reference to a population could not be made but with a greater number the data could be correlated to a population as well.
ConclusionIn the present study, key parameters of the proximal end of the tibia such as ML and AP dimensions have been measured on dry bones. Comparing similar studies conducted in other populations, it was evident that the anatomical profile of Indians is smaller hence highlighting the need for sizing of prosthesis specific to the population in question. It is essential for the geometry of the tibial component to match the resected surface as closely as possible to obtain the best possible stability and load transfer following knee replace-ment surgery.
A decrease in the tibial aspect ratio with an increase in AP length demonstrated in this study would help to formulate guidelines for the manufacturers of prosthesis ensuring optimal tibial implant coverage; a key factor in their long-term survivorship.
Conflict of InterestNone declared.
The AP intercondylar length was found to be small in the present study and South Indian population in comparison to Thai,9 Korean,11,13 and Chinese population.12
The AP length of medial condyle in Indian population was seen to be small as compared with French14 and Korean10 population.
Comparison was suggestive of AP length of the lateral condyle to be more in French14 population, with little variation between Korean10 and Indian population.5
In the present study, the total mean AP length of the medial condyle was 40.19 ± 5.11 mm and that of the lateral condyle was 36.41 ± 4.29 mm which shows an obvious difference between the two tibial plateaus. The same observation was made by Servien et al14 who did a morphometric analysis between the medial and lateral tibial plateaus. The studies by Ivan,5 Kwak et al,11 and Westrich et al15 and Gandhi et al16 highlighted the need for prosthetic designs that recognizes the difference in the medial and lateral tibial condyles and accounts for the smaller, lateral tibial condyle as to achieve the goal of maximizing tibial coverage as well as to eliminate the problems associated with a symmetric design of the tib-ial component.15 Another study by Murlimanju et al showed similar results where the lateral tibial condyle measurements were smaller than the medial condyle.17
The term aspect ratio defines the relationship between the transverse diameter and AP diameter and helps to anticipate the shape of the tibial component. An aspect ratio of 100% indicates that the mediolateral diameter equals AP diameter; predicting a circular shape for the suitable symmetric tibial component. Thus, it follows that an aspect ratio of above 100% indicates that the shape of the anticipated tibial component becomes mediolaterally oval.11 Our study had a higher aspect ratio for smaller AP diameter and a lower ratio for larger AP diameter. In other words, it would mean that with increase in AP diameter the shape of the anticipated tibial component becomes less oval (mediolaterally). Surendran et al,13 Kwak et al,11 Cheng et al,18 and Hitt et al19 had similar results. Surendran et al showed a progressive decline in the medial condylar aspect ratio with increase in AP dimension in their cadaveric study.13 However, the tibial prosthesis used conventionally for UKA showed either a constant condylar aspect ratio or an increasing ratio with increasing AP dimension.19,20 Cheng
Table 3 Comparison of all different parameters of proximal end of tibia among various studies
Various studies ML length (mm) Intercondylar AP length (mm)
AP length of medial condyle (mm)
AP length of lateral condyle (mm)
Surendran S et al - 47.1 ± 4.1 47.1 ± 4.1 -
Yan J H et al 73.5 ± 5.6 49.87 ± 3.9 - -
Kwak DS et al 73.5 ± 5.6 47.3 ± 3.8 - -
Bae DK and Park JY 72.7 ± 4.0 - 48.0 ± 3.1 39.8 ± 2.9
Chaichankul C et al 68.8 ± 5.8 46.04 ± 4.4 - -
Servien E et al - - 50.8 ± 3.3 47.2 ± 3.3
Ivan et al 66.4 ± 5.3 42.0 ± 4.3 41.0 ± 4.2 36.1 ± 4.0
Present study 66.33 ± 5.9 42.52 ± 4.79 42.52 ± 4.79 36.41 ± 4.29

86 Proximal End Morphometry of the Tibia Ahmad et al.
National Journal of Clinical Anatomy Vol. 8 No. 2/2019
References
1 Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anato-my. South Asian Edition. 6th ed. New Delhi: Wolters Kluwer; 2010:520–665
2 Senck S, Gusenbauer C, Frelat MA, McGlynn G, Weber GW, Kastner J. Covariation between shape and bone microstructure in the proximal tibia in humans. iCT Conference. 2014:321-328
3 Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty 2000;15(1):79–85
4 Insall JN, Clarke HD. Historic development, classification and characteristics of knee prosthesis. In: Fitz W, Scott RD, Scott WN, eds. Unicompartmental Total Knee Arthroplasty. Insall and Scott Surgery of the Knee. 4th ed. Vol. 2. Philadelphia
5 Ivan AS. Morphometric Study of Proximal End of Tibia; 2014:75. Available at: http://www.rguhs.ac.in/cdc/onlinecdc/uploads/01_M010_25888.doc. Accessed April 10, 2019
6 Carr A, Keyes G, Miller R, O’Connor J, Goodfellow J. Medial uni-compartmental arthroplasty. A survival study of the Oxford meniscal knee. Clin Orthop Relat Res 1993;(295):205–213
7 Koeck FX, Beckmann J, Luring C, Rath B, Grifka J, Basad E. Evaluation of implant position and knee alignment after patient-specific unicompartmental knee arthroplasty. Knee 2011;18(5):294–299
8 Crockarell JR Jr, Guyton JL. Arthroplasty of the knee. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics. 11th ed. Vol. 1. Philadelphia: Mosby Elsevier; 2008:256–257
9 Chaichankul C, Tanavalee A, Itiravivong P. Anthropometric measurements of knee joints in Thai population: correlation to the sizing of current knee prostheses. Knee 2011;18(1):5–10
10 Bae DK, Park JY. The study of anatomical measurement of proximal tibia and fitness of tibial prosthesis in total knee arthroplasty. J Korean Orthop Assoc 2000;35(1):57–64
11 Kwak DS, Surendran S, Pengatteeri YH, et al. Morphome-try of the proximal tibia to design the tibial component of total knee arthroplasty for the Korean population. Knee 2007;14(4):295–300
12 Yan JH, Yu B, Luo JW, Zuo LJ, Hua LQ, Zuo XH. 3D digitalization of the proximal tibia and its significance on designing the tib-ial component of total knee arthroplasty. Chinese Journal of Clinical Anatomy. 2010;28(2):138
13 Surendran S, Kwak DS, Lee UY, et al. Anthropometry of the medial tibial condyle to design the tibial component for unicondylar knee arthroplasty for the Korean population. Knee Surg Sports Traumatol Arthrosc 2007;15(4):436–442
14 Servien E, Saffarini M, Lustig S, Chomel S, Neyret P. Lateral ver-sus medial tibial plateau: morphometric analysis and adapt-ability with current tibial component design. Knee Surg Sports Traumatol Arthrosc 2008;16(12):1141–1145
15 Westrich GH, Haas SB, Insall JN, Frachie A. Resection specimen analysis of proximal tibial anatomy based on 100 total knee arthroplasty specimens. J Arthroplasty 1995;10(1):47–51
16 Gandhi S, Singla RK, Kullar JS, Suri RK, Mehta V. Mor-phometric analysis of upper end of tibia. J Clin Diagn Res 2014;8(8):AC10–AC13
17 Murlimanju VK, Purushothama C, Srivastava A, et al. Ana-tomical morphometry of the tibial plateau in South Indian population. Ital J Anat Embryol 2016;121(3):258–264
18 Cheng FB, Ji XF, Lai Y, et al. Three dimensional morphometry of the knee to design the total knee arthroplasty for Chinese population. Knee 2009;16(5):341–347
19 Hitt K, Shurman JR II, Greene K, et al. Anthropometric mea-surements of the human knee: correlation to the sizing of current knee arthroplasty systems. J Bone Joint Surg Am 2003;85-A(Suppl 4):115–122
20 Fitzpatrick C, FitzPatrick D, Lee J, Auger D. Statistical design of unicompartmental tibial implants and comparison with cur-rent devices. Knee 2007;14(2):138–144


















