Morning report (Minimalist)
14
Morning Report Dr. Aasems Jacob
-
Upload
aasems-jacob -
Category
Health & Medicine
-
view
13 -
download
2
Transcript of Morning report (Minimalist)

Morning Report
Dr. Aasems Jacob

Patient Profile
23 year old AA male presented to outpatient clinic with
• Back pain• Fatigue X 3months

History of Present Illness
• Lower back pain– 5/10 intensity– No radiation– No lower extremity weakness– No bowel/bladder incontinence
• Non productive cough with intermittent fever• Decreased appetite

• Denies – trauma– loss of weight– diarrhea– hemoptysis– rashes– lymph node enlargement– cold intolerance

Past medical and surgical history
• Negative HIV 2 years ago• PPD positive 3 years ago- not followed up
• Father with diabetes and hypertension• Uncle who died of tuberculosis when patient
was a child
Family Medical history

Personal and Social history
• 1-2 beers on weekends• 1 cigar/day x quit 5 months ago• No illicit drug use• Multiple sexual partners in past 1 year
• Spent past 2 years in a homeless shelter in New Orleans
• Unemployed

Review of systems
• Negative except for the symptoms mentioned in HPI

Physical Examination
• Vitals – 100.4ᴼF– Pulse 88/’– BP 119/80– SpO2 98% in room air
• No pallor, icterus• 2x2 cm Rt. supraclavicular node• Tenderness over L2 vertebra• No kypho-scoliosis

• Chest– Bilateral lower rib tenderness– Clear on auscultation
• Abdomen– No hepatosplenomegaly
• Neurological– Straight leg raising test negative– Power 5/5 in all limbs ; Reflexes normal– No sensory loss

Investigations
• CBC, U/A, BMP, LFT, S.Creat: Normal• Serum electrophoresis: negative• Chest X-ray: Negative• Awaiting PPD, blood culture

• CT showed multiple lytic osseous lesions in ribs and L2 spine with invasion into posterior soft tissues
• MRI- Rt. Paravertebral mass at L2 destroying pedicles and transverse process. Reactive inflammatory changes in psoas muscle
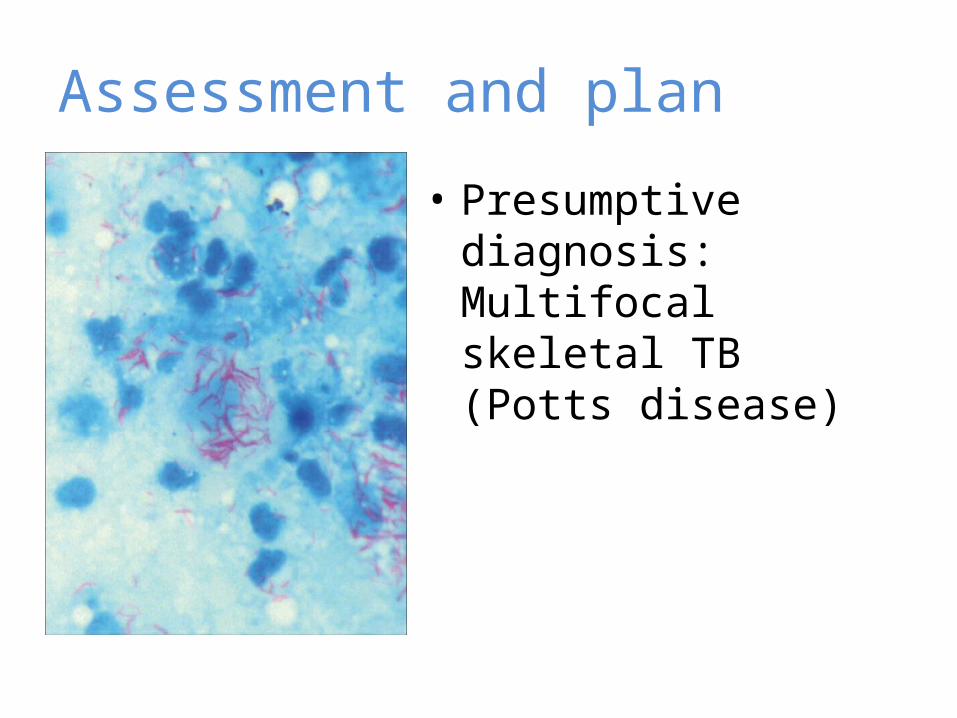
Assessment and plan
• Presumptive diagnosis: Multifocal skeletal TB (Potts disease)

Assessment and plans1. HIV, RPR2. Bone scan3. FNAC supraclavicular lymph node, CT biopsy
lumbar mass4. Fentanyl IV 50µg bolus every 3 hrs5. Empiric treatment with • INH (5mg/kg)• Rifampin (10mg/kg) • Pyrazinamide (15-30mg/kg) • Ethambutol (15-25mg/kg)

Summary• 23 year old AAM• lower back pain and fatigue x 3months• history of non productive cough, fever and loss of
appetite for 3 months• Chronic smoker quit 6 months back• Unemployed and lives in homeless shelter• R. supraclavicular lymph node, bilateral lower rib
tenderness and tenderness over L2. • Paravertebral mass at L2 with inflammatory
changes in psoas muscle in MRI