Morning Report 7/7/2010 Pahresah Roomiany. Factor V Leiden Prothrombin gene mutation Protein C/S...
11
Morning Report 7/7/2010 Pahresah Roomiany
-
Upload
aubrie-small -
Category
Documents
-
view
221 -
download
4
Transcript of Morning Report 7/7/2010 Pahresah Roomiany. Factor V Leiden Prothrombin gene mutation Protein C/S...

Morning Report7/7/2010
Pahresah Roomiany

Factor V Leiden Prothrombin gene mutation Protein C/S deficiency Antithrombin deficiency Malignancy Antiphospholipid Ab syndrome Myeloproliferative disorders Paroxysmal nocturnal hemoglobinuria Nephrotic syndrome Multiple myeloma HIV/AIDS

2008 WHO diagnostic criteria 6
Polycythemia vera Essential thrombocythemia Primary myelofibrosis
Major criteria 1
Hgb >18.5 g dl-1 (men)>16.5 g dl-1 (women)orHgb>17 g dl-1 (men),or>15 g dl-1 (women)if associated with a sustainedincrease of 2 g dl-1 from baselinethat cannot be attributed tocorrection of iron deficiencyorElevated red cell mass>25% above mean normalpredicted value
1 Platelet count 450 109 l-1 1
Megakaryocyte proliferationand atypia accompanied by eitherreticulin and/or collagen fibrosis,orIn the absence of reticulin fibrosis,the megakaryocyte changes mustbe accompanied by increasedmarrow cellularity, granulocyticproliferation and often decreasederythropoiesis (i.e. pre-fibrotic PMF).
2Presence of JAK2V617For similar mutation
2
Megakaryocyte proliferation withlarge and mature morphology.No or little granulocyte or erythroidProliferation.
2Not meeting WHO criteria for CML,PV, MDS, or other myeloid neoplasm
3
Not meeting WHO criteria for CML, PV,PMF, MDS or other myeloid neoplasm
3
Demonstration of JAK2V617For other clonal markerorno evidence of reactive marrow fibrosis
4
Demonstration of JAK2V617For other clonal markerorno evidence of reactive thrombocytosis
Minor criteria 1 BM trilineage myeloproliferation 1 Leukoerythroblastosis
2 Subnormal serum Epo level 2 Increased serum LDH
3 EEC growth 3 Anemia
4 Palpable splenomegaly

Relative: due to decreased plasma volume
Secondary: # of erythrocytes increased. Physiologically appropriate:
High altitude COPD R to L shunts Carboxyhemoglobinemia Cobalt ingestion
Physiologically inappropriate: Renal vascular disease Hepatic tumors Renal cysts, transplant, RCC Pheochromocytoma
Polycythemia vera: myeloproliferative disease

Increased production of RBCs and often wbc and platelets due to neoplastic disorder of hematopoetic stem cells.
Peak incidence in 6th/7th decades Often found on routine blood counts Slight male predominance

“vasomotor” symptoms Hyperviscosity: HA, dizziness,
tinnitus, blurred vision
Thrombosis: transient visual disturbance (amaurosis, ocular migraine), Budd-chiari, erythromelalgia
Bleeding: easy bruising, epistaxis, GI bleed
Pruritus 2/2 to histamine release from basophils
PUD, gout (increased cell turnover)

Proposed criteria for PV
Major criteria
Hemoglobin >18.5 g/dL in men, 16.5 g/dL in women or other evidence of increased red cell volume*
Presence of JAK2 617V>F or other functionally similar mutation such as JAK2 exon 12 mutation
Minor criteria
Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) with prominent erythroid, granulocytic, and megakaryocytic proliferation
Serum erythropoietin level below the reference range for normal
Endogenous erythroid colony formation in vitro
Suspect in patients with elevated RBC mass or elevated H/h with an arterial O2>92%,
splenomegaly, thrombocytosis +/- leukocytosis, thrombotic complications, erythromelalgia or
pruritus.

Phlebotomy: goal Hct <45% in men, <42% in women.
Microcytic anemia can cause increase in whole blood viscosity
Low dose ASA: decrease risk of cardiac event
Hydroxyurea: for high risk patients Allopurinol for gout, H2
blocker/antihistamine for pruritus JAK-2 inhibitors are showing positive
treatment response in clinical trials5

Arterial, venous thrombosis Evolution to AML due to cytotoxic agents (1-
2%, a 100-fold increase in incidence in adult pop by age)
Remission with standard chemotherapy is low 15-20% develop myeloid metaplasia
Replacement of marrow by fibrotic tissue Movement of hematopoiesis into spleen and liver
with worsening pancytopenia Gout Budd-chiari Syndrome

Hepatic venous outflow obstruction
Most cases of BCS in west are associated with MPD
Tx with TIPS, balloon angioplasty2
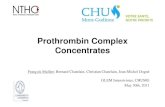
High incidence of rethrombosis and graft failure in PV3 Fluoroscopic image of transjugular
intrahepatic portosystemic shunt (TIPS) in progress. A catheter has been passed into the
hepatic vein and a guidewire was passed into a portal vein branch. A stent has yet to
be placed over the wire.

1. Spivak, J. (2010). Narrative Review: thrombocytosis, polycythemia vera and JAK2 mutations: the phenotypic mimicry of chronic myeloproliferation. Ann Intern Med. 152:300-306.
2. Cruz, E. et.al. (2005).High incidence of recurrence and hematologic events following liver transplantation for budd-chiari syndrome. Clin transplant. 16: 501-506.
3. Buzas, C. (2009). Budd-chiari syndrome secondary to polycythemia vera. J Gastrointestin Liver Dis. 18: 363-366.
4. Rossi, D. (2007). Usefulness of JAK2V617F mutation in distinguishing idiopathic erythrocytosis from polycythemia vera. Leuk Res. 31: 97-101.
5. Finazzi, G. Barbui, T. (2008). Evidence and expertise in the management of polycythemia vera and essential thrombocythemia. Leukemia. 22: 1494-1502.
6. Tefferi, A and Vardiman JW. (2008) Classification and diagnosis of myeloproliferative neoplasms: The 2008 World Health Organization criteria and point-of-care diagnostic algorithms. Leukemia.
7. Kasper et.al. (16th Ed) Harrisons Principles of Internal Medicine.