Morbidity of Women Who Give Birth

of 14
Transcript of Morbidity of Women Who Give Birth
-
7/23/2019 Morbidity of Women Who Give Birth
1/14
National VitalStatistics ReportsVolume64,Number4 May20,2015
Maternal
Morbidity
for
Vaginal
and
Cesarean
Deliveries,According toPreviousCesareanHistory:NewDataFromtheBirthCertificate,2013
bySallyC.Curtin,M.A.,NationalCenter forHealthStatistics;KimberlyD.Gregory,M.D.,M.P.H.,Cedars-SinaiMedicalCenter;LisaM.Korst,M.D.,Ph.D.,ChildbirthResearchAssociates,LLC;andSayeedhaF.G.Uddin,M.D.,M.P.H.,NationalCenter forHealthStatistics
600
525.1
Vaginal birthNoprevious cesarean
Primary cesarean Vaginal birthPreviouscesarean (VBAC)
Repeat cesarean
Rateper100,0
00livebirths
0
100
200
300
400
500
167.1
366.8
468.7
49.2 43.8
88.9
6.3 11.9
67.551.1
143.1
64.6
383.1
131.4
270.3
Maternal transfusion Ruptured uterus1 Unplanned hysterectomy1 ICU admission
1Difference in rates between primary cesarean and VBAC is not statistically significant.NOTES: The birth certificate reporting area represented 90% of all U.S. births in 2013. ICU is intensive care unit.SOURCE: CDC/NCHS, National Vital Statistics System.
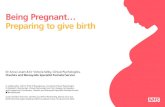
Figure1.Maternalmorbidity,bymethodofdeliveryandpreviouscesareanhistory:41-stateandDistrictofColumbiareportingarea,2013
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESCenters for Disease Control and Prevention
National Center for Health StatisticsNational Vital Statistics System
-
7/23/2019 Morbidity of Women Who Give Birth
2/14
2 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
Abstract
ObjectivesThisreportpresentsrecentfindingsfor2013onfourmaternal morbidities associated with labor and deliverymaternaltransfusion, ruptured uterus, unplanned hysterectomy, and intensivecareunit(ICU)admissionthatarecollectedonbirthcertificates fora41-stateandDistrictofColumbia reportingarea,which represents90%ofallbirths in theUnitedStates.
MethodsRates
of
maternal
morbidity
(per
100,000
live
births)
by
maternalageandraceandethnicityarepresentedbycurrentmethodofdelivery(vaginalorcesarean)andpreviouscesareanhistory.Totalrates are also presented by current method of delivery, previouscesareanhistory,andwhethera trialof laborwasattempted.
ResultsRates
of
maternal
morbidity
were
higher
for
cesarean
thanvaginaldeliveriesratesoftransfusion(525.1per100,000)andICUadmission(383.1)werehighest forprimarycesareandeliveries,while rates of ruptured uterus (88.9) and unplanned hysterectomy(143.1)werehighest for repeat cesareandeliveries.Higher ratesofmaternalmorbidityforcesareancomparedwithvaginaldeliverieswerefound fornearlyallmaternalagegroupsand forwomenofallraces
and
ethnicities.
Women
with
no
previous
cesarean
delivery
who
had
vaginaldeliverieshadlowerratesforallmaternalmorbiditiescomparedwith those who had cesarean deliveries. Women with a previouscesarean delivery who labored and had vaginal birth generally hadlowerratesformostof themorbidities,butfailedtrialsof laborweregenerally associated with higher morbidity than scheduled repeatcesareandeliveries,especially forruptureduterus,whichwasseventimeshigher(495.4per100,000comparedwith65.6).
Keywords:transfusionruptureduterusICUadmissiontrialoflabor
Introduction
Maternal morbidity was defined recently by the World HealthOrganizationasanyhealthconditionattributedtoand/oraggravatedby pregnancy and childbirth that has a negative impact on thewomans wellbeing (1). These morbidities can have short- andlong-termhealthimplicationsforthemotherandthenewbornandcanlengthen hospital stays and increase health care costs (2). Recentresearch has shown that severe maternal morbidity is increasing inCalifornia, partly due to worsening trends in underlying maternalhealthincreased obesity, diabetes, and hypertension, both beforeand during pregnancy (3). Other clinical factors that have beenassociatedwith therise inmaternalmorbidityare the increaseduseofcesareandeliveryandinductionandaugmentationoflabor(4,5).A
demographic
contributor
to
rising
maternal
morbidity
has
been
the
increasing
proportion
of
births
to
older
women,
who
tend
to
have
more health issues and more labor interventions than youngerwomen (6,7). Racial and ethnic disparities persist in maternalmorbidity,withnon-Hispanicblackwomen inparticularhavinghigherrates,evenafterother factorsare taken intoaccount(8).
Another predictor of maternal morbidity is previous cesareanhistoryresearchhasgenerallyshownthatforwomenwithapreviousbirth, those with a history of previous cesarean delivery are at anincreasedriskofmaternalmorbidity(911).This increasedmorbiditypersistedevenwhenotherrelevantdemographicandhealthriskfactorsweretakenintoaccount(9).Inparticular,issuesinvolvingtheplacenta
(placenta previa and accreta, and placental abruption) are morecommoninwomenwithpreviouscesareandeliveries(10).Additionally,the risk of many serious maternal morbidities has been shown toincreaseprogressivelyasthenumberofpreviouscesareandeliveriesincreased (12).
Given the lower morbidity for vaginal compared with cesareandeliveries,attemptingatrialoflaborisrecommendedformostwomenwithnopreviouscesareanaswellasforlow-riskwomenwithapreviouscesarean
delivery
(13).
However,
although
successful
attempts
at
a
trial
of laboraftercesarean(i.e., leadingtoavaginalbirthaftercesarean[VBAC]) result in lower morbidity than planned repeat procedures,failed trialsof labor result in increasedmorbidity (14).Forexample,although rare, rates of ruptured uterus are higher among womenattemptingatrialoflaborafterapreviouscesareanthanamongwomenwithelectiverepeatprocedures(15).Theattempttoavoidsuchmorbiditiesmayhavecontributed to thedecliningpercentageofwomenwithpreviouscesareandeliveriesattemptinga trialof laborover thelast2decades(16).
Dataonmaternalmorbidityareavailableforthefirsttimeforbirthsregisteredusingthe2003revisionoftheU.S.StandardCertificateof
Live
Birth.
Items
capturing
maternal
morbidity
were
added
to
the
birthcertificatetoestablishanationalsurveillancesystemtomonitorthese
morbidities. Maternal morbidity data are available for 41 states thatadopted the 2003 revised birth certificates as of January 1, 2013,representing90%ofallbirthsintheUnitedStatesin2013;completenationaldatafromallofthestatesareexpectedtobeavailablefordatayear2015.
Thisreportfocusesontheincidenceoffourmaternalmorbiditiesreportedonthebirthcertificate:maternaltransfusion,ruptureduterus,unplannedhysterectomy,andICUadmission,allofwhichareusuallyassociatedwithseverecomplicationsoflaborordelivery.Theratesarecompared between vaginal and cesarean deliveries by whether themotherhadapreviouscesareandeliveryandbywhetheratrialoflabor
was
attempted.
This
stratified
analysis
is
possible
with
birth
certificate
databecausetheyarebasedonlargeandalmostcompletecountsofbirth records.
Methods
Data used in this analysis are from the birth certificate andbasedon100%ofbirthsregisteredinthe41statesandtheDistrictofColumbia(D.C.)thathad implemented the2003revisionofthebirthcertificateasofJanuary1,2013.The41statesare:Alaska,California,Colorado, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa,Kansas,Kentucky,Louisiana,Maryland,Massachusetts,Michigan,Min
nesota,
Mississippi,
Missouri,
Montana,
Nebraska,
Nevada,
New
Hampshire,
New
Mexico,
New
York
(including
New
York
City),
North
Carolina,
NorthDakota,Ohio,Oklahoma,Oregon,Pennsylvania,SouthCarolina,SouthDakota,Tennessee,Texas,Utah,Vermont,Virginia,Washington,Wisconsin,andWyoming.
Thebirthsinthe41-stateandD.C.reportingarearepresent90%ofallbirths intheUnitedStates in2013butarenotgeneralizabletothe entire United States in 2013. Some differences between thereportingareaandtheUnitedStatesarenotable,particularlyintheraceandHispanicorigindistributions.BirthstoHispanicwomenandnon-Hispanic black women are slightly overrepresented (23.2% in thereportingareacomparedwith23.1%inthenationforHispanicwomen;
-
7/23/2019 Morbidity of Women Who Give Birth
3/14
3NationalVitalStatisticsReports,Vol.64No.4,May20,2015
15.1% compared with 15.0% for non-Hispanic black women), whilebirths toAmerican IndianorAlaskaNativewomen(AIAN)andAsianorPacific Islander(API)womenareslightlyunderrepresented(0.9%comparedwith1.0%forAIANwomen;6.3%comparedwith6.5%forAPIwomen);seeTableDoftheUserGuidetothe2013NatalityPublicUseFile(17).Whilethesedifferencesaresmall,theyarestatisticallysignificant.Bycomparison,almostnostatisticallysignificantdifferenceswereobservedbetween the reportingareaand theUnitedStates inmaternal
age,
marital
status,
and
infant
characteristics.
Although
not
basedonbirthsfromall50states,thesebirthcertificatedataprovidea large number of births to examine rare events such as maternalmorbiditybymethodofdeliveryandhistoryofcesareandelivery.
The2003 revisionof theU.S.StandardCertificateofLiveBirthaddedtheitemofmaternalmorbidity.Theinstructionsforthisitemaretocheckallthatapplyofthefollowingmorbidities:maternaltransfusion,third- orfourth-degreeperineallaceration,ruptureduterus,unplannedhysterectomy,admissiontointensivecareunit(ICU),unplannedoperating room procedure following delivery, or none of the above. Thesourceofthisinformationisrecommendedtobeinthemedicalrecord(18).
Two
of
the
six
listed
morbidities
were
not
included
in
this
report.Third- orfourth-degreeperineallacerationswasnotincludedbecause
this condition almost always occurs in vaginal births (99%), and ananalysisbymethodofdeliveryisnotappropriate.Unplannedoperatingroomprocedurewasnotincludedbecausethedefinitionisconsideredambiguous.Thefourmorbidities inthisreportareusuallyassociatedwithseverematernalmorbidityitscauses (i.e., ruptureduterus)aswellasitstreatments(maternaltransfusion,unplannedhysterectomy,andICUadmission).Transfusionsaremostoftenadministeredtotreatsevereanemiaandhemorrhaging(19).Unplannedhysterectomiesaremost often performed to treat hemorrhaging (4). Some of the mostcommonreasonsforICUadmissionarepregnancy-relatedhypertensive disease, hemorrhaging, cardiac disease, and infections (20).
Records
for
states
in
the
reporting
area
with
missing
information
on
maternalmorbiditynumbered22,064 (of3,548,525births),or0.6%.Informationonwhetherawomanhadapreviouscesareanandthe
numberofpreviouscesareanswasobtainedfromtheRiskfactorsinthis
pregnancy
item
on
the
birth
certificate.
Missing
records
for
this
item
numbered18,956(of3,548,525births),or0.5%.InformationonmethodofdeliverywasobtainedfromtheMethodofdeliveryitemonthebirthcertificate.The three categories ofvaginalbirthsvaginal/spontaneous, vaginal/forceps,andvaginal/vacuumwerecombinedforatotalvaginalbirthscategory.Whilenotexplicitlyrecordedonthebirthcertificate,bytheirverynature,allvaginalbirthsareassumedtohavehadasuccessfultrialoflabor.Ifacesareanbirthwasindicated,thenthequestion,Ifcesarean,wasatrialoflaborattempted,wasusedtoobtaininformationontrialof
labor
for
these
births.
Records
with
missing
information
for
trial
of
labor
numbered34,094(of1,165,708birthsincesareandeliveries),or2.9%ofcesareandeliveries.
Thetermstrialoflaborandlaborareusedinterchangeablyinthis report. Inaddition, the terms cesareandeliverieswithouta trialoflaborandscheduledcesareandeliveriesareusedinterchangeably.
RaceandHispanicoriginarereportedindependentlyonthebirthcertificate. This report includes data for single-race, non-Hispanicwhite, single-race, non-Hispanic black, single-race, non-HispanicAsian,andHispanicbirths.DetailedinformationonNativeHawaiian
orOtherPacificIslander,AIAN,andmultiple-racebirthsisnotshownbecauseofthesmallnumbersofbirthsforthesegroupsinthisreportingarea.Detailedresults forHispanicsubgroupsarealsonotshown.
Ratesandpercentagesinthisreportarecomputedbysubtractingthenotstatedvaluesfromthetotallivebirthstoobtainthedenominators.Allmaternalmorbidityratesinthisreportareper100,000livebirths.Ratesinthisreportarecomputedonlywhenthenumberofcasesofaspecifiedmorbidity(thenumerator)isgreaterthanorequalto20,but
some
of
the
rates
in
this
report
are
based
on
cases
numbering
between20and99.Therandomvariabilityofthesesmallnumbersisusually greater in terms of percentage than for larger numbers ofevents.Alldifferencesbetweengroupsdiscussed in thisreportweretested for statistical significance, but caution should be used whenevaluatingratesbasedonfewerthan100events.ThestatisticaltestsusedarebasedonthePoissondistributionwhenthenumberofeventsis fewer than 100, and the normal distribution when the number ofeventsis100orgreater.SeeUserGuidetothe2010NatalityPublicUseFile(21)formoredetailonthesignificancetestingandexamplesofcomputations.
Results
Overallfindings
Maternaltransfusionwasthemostcommonofthefourmorbidities
(280.4 per 100,000), followed by ICU admission (154.8),unplanned hysterectomy (40.7), and ruptured uterus (26.1(Table1).
Women having vaginal deliveries with no previous cesarean
deliveryhad the lowest rates forall fourmorbidities(Figure1). Womenwithprimarycesareandeliverieshadthehighestratesof
transfusion(525.1)andICUadmission(383.1),whilemotherswith
repeat
cesarean
deliveries
had
the
highest
rates
of
ruptured
uterus(88.9)andunplannedhysterectomy (143.1).
WomenwithVBACdeliverieshadlowerratesofallfourmaternalmorbidities compared with women with repeat cesarean deliveries,and lower ratesof transfusionand ICUadmissionscomparedwithprimarycesareandeliveries.
Maternalage
Variationinmaternalmorbiditybymaternalageispartlyassociated with differences by age in rates of cesarean delivery andpreviouscesareanhistory(TableA.)Forexample,thetotalcesareanrateforwomenaged3554(43.0per100births)isnearlytwicethat
of
women
under
age
20
(21.8),
while
the
primary
cesarean
rate
isabout50%higher(29.4comparedwith19.9).About9of10women
withapreviouscesareanhaverepeatproceduresforallagegroups,but thepercentage isslightlyhigherforwomenaged3554 thanforyoungerwomen.Alargerproportionofoldermothershavealsohadapreviouscesarean.Table1containsratesofmaternalmorbiditybymaternalageforallbirths,aswellasratesbymethodofdeliveryandpreviouscesareanhistory.
Total
rates
of
transfusion
(316.3)
and
ICU
admission
(156.4)
by
maternalagewerehigherforteenagedmothersthanformothers
-
7/23/2019 Morbidity of Women Who Give Birth
4/14
4 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
aged 2034 (262.4 and 135.5, respectively), and highest formothersaged3554 (355.5and252.8,respectively)(Table1).
Totalratesofruptureduterusandunplannedhysterectomygenerally increased with maternal age, with a greater increase forunplannedhysterectomytherateforwomenaged3554(103.8)wasmorethan10timestherateforwomenunderage20(10.1).
Womenunderage20
The
rate
of
transfusion
was
almost
three
times
higher
for
births
inprimarycesareandeliveries(645.4per100,000)thanforvaginalbirthswithnopreviouscesarean(226.9).
The
rate
of
ICU
admission
was
seven
times
higher
for
women
havingprimarycesareandeliveries(496.6)thanforwomenhavingvaginalbirthswithnopreviouscesarean (68.5).
Casesofruptureduterusandunplannedhysterectomyforwomenunderage20weretoofewinnumbertoexaminedifferencesbymethodofdeliveryandpreviouscesareanhistory.
Womenaged2034and3554
Maternal transfusionsweremorecommon formotherswithpri
mary
and
repeat
cesarean
deliveries
and
VBAC
deliveries
than
for
motherswithvaginalbirthswithnopreviouscesarean. Amongthemethod-of-deliverygroupsforwhichdatawereavail
able,ratesofruptureduteruswerehighestforrepeatcesareans(90.6forwomenaged2034and83.1forwomenaged3554),and lowestforvaginalbirthswithnopreviouscesarean(5.7 forwomenaged2034and11.2 forwomenaged3554).
Womenwithvaginalbirthswithnopreviouscesareanhadlowerratesofunplannedhysterectomy thanwomenwhohadprimaryorrepeatcesareanbirths.Ratesofunplannedhysterectomywerehigher
for
repeat
cesarean
deliveries
than
for
primary
cesarean
deliveries.
WomenwithvaginaldeliverieswithnopreviouscesareanhadthelowestICUadmissionrates(58.9forwomenaged2034and97.3forwomenaged3554).Womenwithprimarycesareandeliverieshad higher rates of ICU admission than women with repeatcesareandeliveries(344.3comparedwith231.3,respectively,forwomenaged2034;502.2comparedwith397.1forwomenaged3554).
RaceandethnicityVariationinmaternalmorbiditybymaternalraceandethnicityis
partly associated with differences by race and ethnicity in rates ofcesarean delivery and previous cesarean history (TableA). Forexample, non-Hispanic white women had the lowest total cesareanrate(31.8per100births)andthehighestpercentageofwomenwithnopreviouscesarean(86.3).Hispanicwomenhadthelowestprimarycesareanrate(21.1),butthehighestproportionofwomenwithtwoormoreprevious cesareandeliveries (5.7%).Table2contains rates ofmaternalmorbiditybymaternalraceandethnicityforallbirthsaswellasratesbymethodofdeliveryandpreviouscesareanhistory.DuetoinsufficientcasesinsomeinstancesforbirthsinVBACdeliveriesandtonon-HispanicAsianwomen,rateswerenotcomputed forsomeof
the
morbidities
by
race
and
ethnicity.
Non-Hispanicblackwomenhad thehighestratesof transfusion(332.3)and ICUadmission (239.5)amongall racialandethnicgroups.
Non-Hispanicblack(39.2)andnon-HispanicAsian(32.1)womenhad thehighestratesof ruptureduterus.
Forcategorieswithsufficientcases tocompute rates,maternal
morbiditywashigherforwomenwhohadcesareandeliveriesthantheir counterparts who had vaginal deliveries with no previouscesarean forallof theracialandethnicgroups.
Inmost instances,ratesofruptureduterusandunplannedhys
terectomy were higher for repeat cesarean deliveries than for
TableA.Total,primary,andrepeatcesareanratesandpreviouscesareanhistory,bymaternalageandraceandethnicity:41-stateandDistrictofColumbiareportingarea,2013
Previous
cesarean
history
Total Primary Repeat
cesarean
cesarean
cesarean
Two
or
Maternal
age
and
race
and
ethnicity
Number
rate1 rate2 rate3 Total
None
One
more
Per100births
Allbirths4 . . . . . . . . . . . . . . . . . . . 3,548,525 32.6 22.8 89.4 100.0 85.4 10.3 4.4
Maternalage(years):
Under
20
. . . . . . . . . . . . . . . . .
248,842
21.8
19.9
89.5
100.0
97.3
2.5
0.2
2034 . . . . . . . . . . . . . . . . . . . 2,758,010 31.5 21.9 89.3 100.0 85.8 10.1 4.2
3554
. . . . . . . . . . . . . . . . . . .
541,673
43.0
29.4
89.9
100.0
77.7
14.9
7.4
Maternal
race
and
ethnicity:
Non-Hispanicwhite. . . . . . . . . . . . . 1,880,350 31.8 22.6 89.1 100.0 86.3 10.0 3.7
Non-Hispanic
black
. . . . . . . . . . . . .
511,132
35.9
25.7
89.0
100.0
84.0
10.7
5.3
Non-HispanicAsia n . . . . . . . . . . . . . 206,651 33.9 24.6 89.4 100.0 85.6 12.0 2.4
Hispanic
. . . . . . . . . . . . . . . . . .
818,006
32.3
21.1
90.4
100.0
83.9
10.4
5.7
1Numberofbirthsbycesareandeliveryper100 totalbirths.2Number
of
births
by
cesarean
delivery
per
100
births
to
women
with
no
previous
cesarean
delivery.
3Number
of
births
by
cesarean
delivery
per
100
births
to
women
with
a
previous
cesarean
delivery.
4Includesbirthswith raceandethnicitynotstated.
NOTES:
Race
and
Hispanic
origin
are
reported
separately
on
the
birth
certificate.
Race
categories
are
consistent
with
1997
Office
of
Management
and
Budget
standards;
see
Methods.
Data
by
race
are
non-Hispanic
and
exclude
mothers
reporting
multiple
races.
Reporting
area
includes
Alaska,
California,
Colorado,
Delaware,
District
of
Columbia,
Florida,
Georgia,
Idaho,
Illinois,
Indiana,
Iowa,
Kansas,
Kentucky,
Louisiana,
Maryland,
Massachusetts,
Michigan,
Minnesota,
Mississippi,
Missouri,
Montana,
Nebraska,
Nevada,
New
Hampshire,
New
Mexico,
New
York,
North
Carolina,
North
Dakota,Ohio,Oklahoma,Oregon,Pennsylvania,SouthCarolina,SouthDakota,Tennessee,Texas,Utah,Vermont,Virginia,Washington,Wisconsin,andWyoming.
-
7/23/2019 Morbidity of Women Who Give Birth
5/14
5NationalVitalStatisticsReports,Vol.64No.4,May20,2015
primarycesareandeliveriesfortheracialandethnicgroups.Theexceptions were ruptured uterus for Hispanic women (44.4 forprimarycomparedwith51.2forrepeatcesarean,notsignificantlydifferent) and unplanned hysterectomy for non-Hispanic Asianwomen (110.9 for primary compared with 124.5 for repeatcesarean,notsignificantlydifferent).
RatesofICUadmissionwerehigherforprimarycesareandeliveriesthanforrepeatcesareandeliveriesforallracialandethnicgroups.
Trialof laborandmethodofdelivery
Another importantconsideration inexamining ratesofmaternalmorbidity by previous cesarean history is whether a womanattempted a trial of labor with her current delivery. Rates of trial oflabor and trial-of-labor success rates differ markedly by previouscesarean
history
(Table
B
and
Figure
2).
Almost
9
of
10
women
with
nohistoryofapreviouscesareanattemptatrialof labor(87%),andthevastmajorityaresuccessful(89%).Incontrast,only1in5womenwhohadonepreviouscesareanattemptatrialoflaboraftercesarean(20%), although 70% of these are successful. Less than 1 in 10women
with
a
history
of
two
or
more
previous
cesarean
deliveries
attemptedatrialoflabor(7%),withaboutone-halfoftheseresultinginsuccessfulvaginaldeliveries(51%).
Womenwithnopreviouscesareandelivery
Table3andFigure3presentmaternalmorbidityratesforwomenwith no previous cesarean delivery by whether a trial of labor wasattemptedandwhether the laborresulted inavaginaldelivery.
Womenwhoattemptedatrialoflaborandhadasuccessfulvaginaldeliveryhadlowerratesforallofthemorbiditiescomparedwithwomenwhohadcesareandeliveries,eitherwithorwithoutlabor.
Women
with
cesarean
deliveries
who
did
not
labor
had
higherratesofICUadmission(420.6per100,000)thanwomenwhohad
failedtrialsoflabor(318.4),butlowerratesofmaternaltransfusion(486.9comparedwith600.9,respectively).
Theratesofruptureduterusandunplannedhysterectomywerenotstatisticallydifferentbywhetheratrialoflaborwasattemptedfor women who had cesarean deliveries with no history of apreviouscesarean.
Women
with
a
previous
cesarean
Table4andFigure4presentmaternalmorbidityratesforwomenwithapreviouscesareandeliverybywhethertheyattemptedatrialoflaborandwhether this laborultimately resulted inaVBACdelivery.
Womenwhoattemptedatrialoflaboraftercesareanandhadasuccessful VBAC delivery had lower rates of transfusion,unplannedhysterectomy,andICUadmissionthandidwomenwithcesareandeliverieswithoutlabor.RatesofruptureduteruswerenotsignificantlydifferentbetweensuccessfulVBACbirths (43.8per100,000)andcesareanbirths (65.6)withouta trialof labor.
WomenwithsuccessfultrialsoflaborresultinginVBACdeliverieshad lowerrates forallof themorbiditiescomparedwithwomen
who
had
failed
trials
of
labor
resulting
in
repeat
cesarean
deliveries.
Womenwhohadfailedtrialsoflaborresultinginrepeatcesareandeliverieshadhigherratesforthreeofthemorbiditiescomparedwith women with repeat cesareans without labor (transfusion,ruptureduterus,and ICUadmission).Thegreatestdifference inrateswasforruptureduterustherateforwomenwithfailedtrialsof
labor
(495.4
per
100,000)
was
more
than
seven
times
higher
thanforwomenwithrepeatcesareandeliverieswhodidnotlabor(65.6).
Discussion
This report presents recent data from the birth certificate onmaternalmorbidityassociatedwithlaboranddelivery.Thedatausedin this analysis from the 41-state and D.C. reporting area in 2013represent 90% of all U.S. births, and complete national data onmaternal morbidity are expected with the 2015 data year. Theestimatesofmaternalmorbidityfromthisstudymaynotbenationallyrepresentative, because births to Hispanic and non-Hispanic blackwomen are slightly overrepresented. Findings from the birth certificate data are generally consistent with previous research, althoughsome new findings for which previous research is not available arealsopresented.
Findings
from
the
birth
certificate
compared
withotherstudies
The findings in this study that womenwithcesarean deliverieshavemoremorbiditythanwomenwithvaginaldeliveriesisconsistentwith many other studies (25,9,12). History of a previous cesareanhas been generally associated with increased morbidity (911) andwas found in thisstudy forruptureduterusandunplannedhysterectomy, which had higher rates for repeat compared with primarycesareandeliveries.Giventhispattern,thehigherratesoftransfusionand ICU admission for primary cesareans compared with repeatcesareanswassomewhatunexpected.However,amulticenterU.S.
TableB.Methodofdeliveryand trialof labor,bypreviouscesareanhistory:41-stateandDistrictofColumbiareportingarea,2013
Previous
cesarean
history
Two or
Trial
of
labor
and
method
of
delivery
Total
None
One
more
Allb i r t h s . . . . . . . . . . . . . . . . . . . . 100.0 100.0 100.0 100.0
Successful
trial
of
laborvaginal
deliveries
(includesVBAC1) . . . . . . . . . . . . . . 67.8 77.6 13.8 3.5
Failed trialof laborcesareandelivery . . . . 8.5 9.1 5.8 3.3
No
trial
of
laborcesarean
delivery
. . . . . .
23.7
13.3
80.4
93.2
Successratewhen trialof
labor
is
attempted2. . . . . . . . . . . . . .
88.8
89.5
70.4
51.4
1Vaginalbirthaftercesarean.2Percentage
of
vaginal
births
when
a
trial
of
labor
is
attempted.
NOTE:Reportingarea includesAlaska,California,Colorado,Delaware,DistrictofColumbia,Florida,Georgia, Idaho, Illinois, Indiana, Iowa,Kansas,Kentucky,Louisiana,Maryland,Massachusetts,Michigan,Minnesota,Mississippi,Missouri,Montana,Nebraska,Nevada,NewHampshire,
New
Mexico,
New
York,
North
Carolina,
North
Dakota,
Ohio,
Oklahoma,
Oregon,
Pennsylvania,
South
Carolina,
South
Dakota,
Tennessee,
Texas,
Utah,
Vermont,
Virginia,
Washington,
Wisconsin,
and
Wyoming.
-
7/23/2019 Morbidity of Women Who Give Birth
6/14
6 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
studythatfocusedspecificallyontransfusionsforwomenundergoing
cesarean
delivery
also
found
an
increased
incidence
in
primarycomparedwith repeatcesareandeliveries(19).The findings for ICU
admission
are
new,
with
no
other
large
U.S.
studies
available
that
examine this specifically by method of delivery and previouscesareanhistory.
Oldermothersandnon-Hispanicblackmothershavehigherratesof maternal morbidity, but this reflects, to some extent, their highercesarean rates. However, these groups generally have higher morbidity,evenwhenotherrelevant factorsareconsidered(9).Althoughratescouldnotbecomputedforsomegroupsduetoinsufficientcases,theelevatedmorbidityforcesareancomparedwithvaginaldeliverieswas generally found in all age groups and for all racial and ethnicgroups.
For
women
with
no
history
of
previous
cesarean,
morbidity
was
always lower forvaginalbirthscomparedwithwomenwithbirthsbycesareandeliveries,eitherwithorwithout labor.Resultsweremixedfor primary cesarean deliveries by whether a trial of labor wasattemptedfailed trials of labor were associated with elevatedmorbidityfortransfusionsrelativetocesareandeliverieswithoutlabor,butassociatedwithlowerratesofICUadmission.Becausemostwomenwithnopreviouscesareanattempt labor(almost9of10),thosewithscheduledcesareandeliveriesaremorelikelytohaveunderlyinghealthconditions or problematic pregnanciesmore preeclampsia, pluralgestations,
malpresentations,
and
suspected
macrosomic
fetuses
(weighing more than 4,000 grams)while a very small percentage
have elective procedures (22,23). Admission to the ICU has been
shown
to
be
associated
with
both
underlying
maternal
health
(chieflyhypertensive and cardiac issues) as well as issues associated with
labor
and
delivery
(hemorrhaging
and
infection)
(20).
Forwomenwithapreviouscesareandelivery,successfulVBACdeliveriesweregenerallyassociatedwithlowermorbiditythanscheduledrepeatprocedures(withtheexceptionofruptureduterus,whichwas not significantly different). However, failed trials of labor wereassociatedwithincreasedratesforthreeofthemorbiditiescomparedwithscheduledrepeatprocedures,whichisconsistentwithmanyotherstudies(2427)andespeciallytrueforruptureduterus.Attemptingatrialoflaborwiththecurrentdeliveryafterapreviouscesareandeliveryisaconsistentpredictorof ruptureduterus (15,27,28),although thismorbidity isstillveryrare.
Dataqualityofhealth information frombirthcertificates
Medicalandhealth informationhavebeen traditionallyunderreportedonthebirthcertificate(29,30).TheNationalCenterforHealthStatistics(NCHS) fieldeda recentvaliditystudybasedondata fromthe2003 revision thatdidnot includematernalmorbiditydue to therarityofsomeoftheitems(31).Otherrelevantmedicalitems(methodofdelivery,numberofpreviouscesareandeliveries,andtrialoflabor)were
included
in
the
NCHS
validity
study
conducted
in
two
states.
Theprimarymeasurementofdataquality forcheckbox items in the
NOTES: Total trial of labor is Vaginal plus CesareanFailed trial of labor. The birth certificate reporting area represented 90% of all U.S. births in 2013.SOURCE: CDC/NCHS, National Vital Statistics System.
0 20 40 60
Percent
80 100
CesareanNo trial of laborCesareanFailed trial of laborVaginal
Two or more 4 3 93
One 14 6 80
None 78 9 13
Number of previouscesarean deliveries
Total trial of labor = 87%
Total trial of labor = 20%
Total trial of labor = 7%
Figure2.Trialof laborandmethodofdelivery,bynumberofpreviouscesareandeliveries:41-stateandDistrictofColumbiareportingarea,2013
-
7/23/2019 Morbidity of Women Who Give Birth
7/14
7NationalVitalStatisticsReports,Vol.64No.4,May20,2015
quality report was sensitivity, or the true positive rate. This is
measured
as
the
percentage
of
birth
records
for
which
a
specific
item
was reported when it was indicated on the medical record. Formethodofdelivery, thisstudy foundhighsensitivity,above90%, forvaginalandcesareandeliveriesinbothstates.Fortheitemsmotherhadapreviouscesareandeliveryand trialof labor,onestatehadsubstantial sensitivity, between 75.0% and 89.9%, and the otherstate had moderate sensitivity, between 60.0% and 74.9%. Thenumberofpreviouscesareandeliveriesisnotacheckboxitem,butacontinuous variable. The exact agreement between the birth certificateandthemedicalrecord(theprimaryqualitymeasure)wasabove90%
in
both
states.
Asanaggregatecomparison,twoofthematernalmorbidities in
this
report,
maternal
transfusions
and
unplanned
hysterectomy,
are
also
included
to
some
extent
on
the
Center
for
Disease
Control
and
Preventions(CDCs)listofseverematernalmorbidityindicators(32).Thesedataarecollectedfromanationallyrepresentativesurveybasedon International Classification of Diseases, Ninth Revision, ClinicalModification(ICD9CM)codesfromhospitaldischargerecordsintheUnitedStates.Theirestimateofmaternaltransfusionsforthelatestdatayear,20102011,was117per10,000deliveries(or1,170per100,000)comparedwithabout280per100,000forbirthcertificatedatain2013.Theirestimateofhysterectomywas9per10,000deliveries(or90per100,000),comparedwithabout41per100,000forbirthcertificatedata.Notethatthedefinitionsandmethodofascertainmentofthesemorbidities
differbetween the twodatasources,whichcould, inpart,explain these
discrepancies.
For
example,
the
CDC
indicator
for
hysterectomy
does
not
differentiate the procedure according to whether it was planned orunplanned,whereas the itemonthebirthcertificate isspecificabout itsbeing unplanned.However, given that these hysterectomies are performedatthetimeofdelivery,themajorityareemergentandunplanned(33). Despite the limitations, this comparison of the severe maternalmortalityindicatorsandthebirthcertificatedatasuggestsunderreportingof thesemorbiditieson thebirthcertificate.Thedifferentials inmorbidityamong groups featured in this report are generally consistent with theliterature,buttheoverall levelsaremost likelyunderestimated.
No
large-scale,
recent
studies
exist
to
use
as
comparisons
for
ruptureduterusandICUadmission,andpreviousestimatesofruptured
uterus
vary
widely
(34).
Problems
in
identifying
ruptured
uterus
with
ICD9CM
codes
have
been
documented
and
may
extend
to
birth
certificate data as well (35). In particular, ICD9CM codes do notdistinguish between a ruptured uterus and a less serious condition,uterinedehiscence.Astudythatcomparesbirthcertificateentrieswiththemedicalrecordwouldbenecessarytoascertainwhetherthisissuealsoexists forbirthcertificatedata.
Maternalmorbiditiesarerarebut importantmaternalhealth issues,andtheyaredifficulttoexaminewithmostsamplesurveydata.Studiesthatassessthevalidityofthebirthcertificatedataareneeded.Itishopedthatthesefindingswillinformresearchersandcliniciansaswellassuggestavenuesoffurtherresearchusingthesenewdata.
1Difference in rates between Primary cesareanFailed trial of labor and Primary cesareanNo trial of labor is not statistically significant.NOTES: The birth certificate reporting area represented 90% of all U.S. births in 2013. ICU is intensive care unit.SOURCE: CDC/NCHS, National Vital Statistics System.
Rateper100,0
00livebirths
0
100
200
300
400
500
600
700 Primary cesareanFailed trial of labor Primary cesareanNo trial of laborVaginal
ICU admissionUnplanned hysterectomy1Ruptured uterus1Maternal transfusion
167.1
600.9
486.9
55.0 46.5
11.9
70.4 66.6 64.6
318.4
420.6
6.3
Figure3.Maternalmorbidityforwomenwithnopreviouscesareandelivery,bymethodofdeliveryand trialof labor:41-stateandDistrictofColumbiareportingarea,2013
-
7/23/2019 Morbidity of Women Who Give Birth
8/14
8 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
References
1.
Firoz
T,
Chou
D,
von
Dadelszen
P,
Agrawal
P,
Vanderkruik
R,
Tunalp
O,
et
al.
Measuring
maternal
health:
Focus
on
maternal
morbidity.
Bull
World
Health
Organ
91:7946.
2013.
2.
Callaghan
WM,
Creanga
AA,
Kuklina
EV.
Severe
maternal
morbidity
among
delivery
and
postpartum
hospitalizations
in
the
United
States.
Obstet
Gynecol
120(5):102936.
2012.
3.
Fridman
M,
Korst
LM,
Chow
J,
Lawton
E,
Mitchell
C,
Gregory
KD.
TrendsinmaternalmorbiditybeforeandduringpregnancyinCalifornia.Am
J
Public
Health
104
Suppl
1:S4957.
2014.
4.
Bateman
BT,
Mhyre
JM,
Callaghan
WM,
Kuklina
EV.
Peripartum
hysterectomy
in
the
United
States:
Nationwide
14
year
experience.
Am
J
Obstet
Gynecol
206(1):63.e18.
2012.
5.
Kramer
MS,
Dahhou
M,
Vallerand
D,
Liston
R,
Joseph
KS.
Risk
factors
for
postpartum
hemorrhage:
Can
we
explain
the
recent
temporal
increase?
J
Obstet
Gynaecol
Can
33(8):8109.
2011.
6. OstermanMJK,MartinJA,CurtinSC,etal.Newlyreleaseddatafromthe
revised
U.S.
birth
certificate,
2011.
National
vital
statistics
reports;
vol
62
no
4.
Hyattsville,
MD:
National
Center
for
Health
Statistics.
2013.
7.
Martin
JA,
Hamilton
BE,
Osterman
MJK,
et
al.
Births:
Final
data
for
2013.
National
vital
statistics
reports;
vol
64
no
1.
Hyattsville,
MD:
National
Center
for
Health
Statistics.
2015.
8.
Creanga
AA,
Bateman
BT,
Kuklina
EV,
Callaghan
WM.
Racial
and
ethnic
disparities
in
severe
maternal
morbidity:
A
multistate
analysis,
20082010.
Am
J
Obstet
Gynecol
210(5):435.e18.
2014.
9. Gray KE, Wallace ER, Nelson KR, Reed SD, Schiff MA. Population-based
study
of
risk
factors
for
severe
maternal
morbidity.
Paediatr
Perinat
Epidemiol
26(6):50614.
2012.
10.
Daltveit
AK,
Tollnes
MC,
Pihlstrm
H,
Irgens
LM.
Cesarean
delivery
and
subsequent
pregnancies.
Obstet
Gynecol
111(6):132734.
2008.
11.
Galyean
AM,
Lagrew
DC,
Bush
MC,
Kurtzman
JT.
Previous
cesarean
section
and
the
risk
of
postpartum
maternal
complications
and
adverse
neonatal
outcomes
in
future
pregnancies.
J
Perinatol
29(11):72630.
2009.12.
Marshall
NE,
Fu
R,
Guise
JM.
Impact
of
multiple
cesarean
deliveries
on
maternal
morbidity:
A
systematic
review.
Am
J
Obstet
Gynecol
205(3):262.e18.
2011.
13.
American
College
of
Obstetricians
and
Gynecologists.
Vaginal
birth
after
previous
cesarean
delivery.
Practice
bulletin
no
115:114.
2010
(reaffirmed
2013).
14. Lydon-RochelleMT,CahillAG,SpongCY.Birthafterpreviouscesareandelivery:
Short-term
maternal
outcomes.
Semin
Perinatol
34(4):24957.
2010.
15.
Spong
CY,
Landon
MB,
Gilbert
S,
Rouse
DJ,
Leveno
KJ,
Varner
MW,
et
al.
Risk
of
uterine
rupture
and
adverse
perinatal
outcome
at
term
after
cesarean
delivery.
Obstet
Gynecol
110(4):8017.
2007.
1Difference in rates between VBAC and Repeat cesareanNo trial of labor is not statistically significant.2Difference in rates between Repeat cesareanFailed trial of labor and Repeat cesareanNo trial of labor is not statistically significant.NOTES: The birth certificate reporting area represented 90% of all U.S. births in 2013. ICU is intensive care unit.SOURCE: CDC/NCHS, National Vital Statistics System.
Rateper100,0
00livebirths
ICU admissionUnplanned hysterectomy2Ruptured uterus1Maternal transfusion0
200
400
600
800 Repeat cesareanFailed trial of labor
Repeat cesareanNo trial of labor
Vaginal birthPreviouscesarean (VBAC)
366.8
731.4
458.0
43.8
495.4
65.651.1
158.7143.9
131.4
356.0
265.3
Figure4.Maternalmorbidityforwomenwithapreviouscesareandelivery,bymethodofdeliveryand trialof labor:41-stateandDistrictofColumbiareportingarea,2013
-
7/23/2019 Morbidity of Women Who Give Birth
9/14
9NationalVitalStatisticsReports,Vol.64No.4,May20,2015
16.
Uddin
SF,
Simon
AE.
Rates
and
success
rates
of
trial
of
labor
after
cesarean delivery in the United States, 19902009. Matern ChildHealthJ17(7):130914.2013.
17.
National
Center
for
Health
Statistics.
User
guide
to
the
2013
natality
public
use
file.
Available
from:
ftp://ftp.cdc.gov/pub/Health_Statistics/
NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdf .
18.
National
Center
for
Health
Statistics.
Guide
to
completing
the
facility
worksheets
for
the
certificate
of
live
birth
and
report
of
fetal
death
(2003
revision).
2006.
Available
from:
http://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdf.
19.
Rouse
DJ,
MacPherson
C,
Landon
M,
Varner
MW,
Leveno
KJ,
Moawad
AH,
et
al.
Blood
transfusion
and
cesarean
delivery.
Obstet
Gynecol
108(4):8917.
2006.
20.
Wanderer
JP,
Leffert
LR,
Mhyre
JM,
Kuklina
EV,
Callaghan
WM,
Bateman
BT.
Epidemiology
of
obstetric-related
ICU
admissions
in
Maryland:
19992008.
Crit
Care
Med
41(8):184452.
21.
National
Center
for
Health
Statistics.
User
guide
to
the
2010
natality
public use file. Available from: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdf .
22.
Boyle
A,
Reddy
UM,
Landy
HJ,
Huang
CC,
Driggers
RW,
Laughon
SK.
Primary
cesarean
delivery
in
the
United
States.
Obstet
Gynecol
122(1):3340.
2013.
23.
Barber
EL,
Lundsberg
LS,
Belanger
K,
Pettker
CM,
Funai
EF,
Illuzzi
JL.Indications
contributing
to
the
increasing
cesarean
delivery
rate.
Obstet
Gynecol118(1):2938.2011.24.
National
Institutes
of
Health.
National
Institutes
of
Health
Consensus
Development
Conference
statement:
Vaginal
birth
after
cesarean:
New
insights;
March
810,
2010.
Obstet
Gynecol,
115(6):127995.
2010.
25.
Macones
GA,
Peipert
J,
Nelson
DB,
Odibo
A,
Stevens
EJ,
Stamilio
DM,
et
al.
Maternal
complications
with
vaginal
birth
after
cesarean
delivery:
A
multicenter
study.
Am
J
Obstet
Gynecol
193(5):165662.
2005.
26. HibbardJU, Ismail MA, WangY,TeC,KarrisonT, Ismail MA.Failedvaginal
birth
after
a
cesarean
section:
How
risky
is
it?
I.
Maternal
morbidity.
Am
J
Obstet
Gynecol
184(7):136571;
discussion
13713.
2001.
27.
Landon
MB,
Hauth
JC,
Leveno
KJ,
Spong
CY,
Leindecker
S,
VarnerMW,
et
al.
Maternal
and
perinatal
outcomes
associated
with
a
trial
of
labor
after
prior
cesarean
delivery.
N
Engl
J
Med
351(25):25819.
2004.
28. McMahonMJ,LutherER,BowesWAJr,OlshanAF.Comparisonofatrial
of
labor
with
an
elective
second
cesarean
section.
N
Engl
J
Med
335(10):68995.
1996.
29.
Piper
JM,
Mitchel
EF
Jr,
Snowden
M,
Hall
C,
Adams
M,
Taylor
P.
Validation
of
1989
Tennessee
birth
certificates
using
maternal
and
newborn
hospital
records.
Am
J
Epidemiol
137(7):75868.
1993.
30.
Buescher
PA,
Taylor
KP,
Davis
MH,
Bowling
JM.
The
quality
of
the
new
birthcertificatedata:Avalidationstudy inNorthCarolina.AmJPublicHealth
83(8):11635.
1993.
31.
Martin
JA,
Wilson
EC,
Osterman
MJK,
et
al.
Assessing
the
quality
of
medical
and
health
data
from
the
2003
birth
certificate
revision:
Results
from
two
states.
National
vital
statistics
reports;
vol
62
no
2.
Hyattsville,
MD:
National
Center
for
Health
Statistics.
2013.
32.
CDC.
Severe
maternal
morbidity
in
the
United
States.
Available
from:
http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/
SevereMaternalMorbidity.html.
33. Shellhaas
CS,
Gilbert
S,
Landon
MB,
Varner
MW,
Leveno
KJ,
Hauth
JC,
et
al.
The
frequency
and
complication
rates
of
hysterectomy
accompanying cesarean delivery. Obstet Gynecol 114(2 Pt 1):2249.2009.
34. Guise
JM,
Berlin
M,
McDonagh
M,
Osterweil
P,
Chan
B,
Helfand
M.
Safety of vaginal birth after cesarean: A systematic review. ObstetGynecol
103(3):4209.
2004.
35.
CDC.
Use
of
hospital
discharge
data
to
monitor
uterine
rupture
Massachusetts,
19901997.
MMWR
49(12),
2458.
2000.
ListofDetailedTables
1.
Maternal
morbidity,
by
previous
cesarean
history,
method
of
delivery,
and
age
of
mother,:
41-state
and
District
of
Columbia
reporting
area,
2013
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10
2.
Maternal
morbidity,
by
previous
cesarean
history,
method
of
delivery,
and
race
and
Hispanic
origin
of
mother:
41-state
and
District
of
Columbia
reporting
area,
2013
. . . . . . . . . . . . . . . .
11
3.
Maternal
morbidity
for
women
with
no
previous
cesarean
delivery,
by
method
of
delivery
and
trial
of
labor:
41-state
and
District
of
Columbia
reporting
area,
2013
. . . . . . . . . . . . . . . . . . . . . . .
12
4.
Maternal
morbidity
for
women
with
a
previous
cesarean
delivery,
by method of delivery and trial of labor: 41-state and District ofColumbiareportingarea,2013. . . . . . . . . . . . . . . . . . . . . . . 13
ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlhttp://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.htmlftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2010.pdfhttp://www.cdc.gov/nchs/data/dvs/guidetocompletefacilitywks.pdfftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/natality/UserGuide2013.pdf -
7/23/2019 Morbidity of Women Who Give Birth
10/14
10 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
Table1.Maternalmorbidity,reportingarea,2013
[Ratesarenumberof livebirthswith
bypreviouscesareanhistory,methodofdelivery,
specifiedmorbidityper100,000 livebirths inspecifiedgroup]
andageofmother:41-stateandDistrictofColumbia
Age(years)andmaternalmorbidityAll
births
Previouscesareanhistoryandmethodofdelivery
Withoutpreviouscesareandelivery Withpreviouscesareandelivery
Vaginal Primarycesarean VBAC1 Repeatcesarean
2All
ages
Totalnumber . . . . . . . . . . . . . . . . Notstated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Under
age
20
Totalnumber . . . . . . . . . . . . . . . . Notstated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Aged2034
Totalnumber . . . . . . . . . . . . . . . . Notstated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . Unplanned
hysterectomy
. . . . . . . .
Admission to intensivecareunit. . . .
Aged3554
Totalnumber . . . . . . . . . . . . . . . . Notstated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
3,548,52522,064
9,888922
1,4375,460
280.426.140.7
154.8
248,8421,327
316.311.7 10.1
156.4
2,758,01016,566
262.424.531.2
135.5
541,6734,171
355.541.1
103.8252.8
2,322,3203,863
3,875146 277
1,497
167.16.3
11.964.6
192,901289
226.9* *
68.5
1,834,9402,965
157.85.79.4
58.9
294,479609
186.111.231.697.3
Number
of
686,1941,558
3,595337 462
2,623
Rate
525.149.267.5
383.1
Number
of
47,823100
Rate
645.4* *
496.6
Numberof
515,5361,086
Rate
489.345.350.5
344.3
Numberof
122,835372
Rate
628.873.5
158.4502.2
births
births
births
births
54,933140
20124 2872
366.843.851.1
131.4
7121
** **
42,02198
333.9*
50.1
109.7
12,20041
468.8**
213.8
464,3801,154
2,171412 663
1,252
468.788.9
143.1270.3
6,04310
480.7* **
349,709813
462.090.6
114.4
231.3
108,628331
489.483.1
239.2397.1
*
Figure
does
not
meet
standards
of
reliability
or
precision;
based
on
fewer
than
20
births
in
the
numerator.
1Vaginalbirthaftercesarean;98%ofvaginalbirthswere towomenwithnopreviouscesarean,while2%wereVBAC.Forsomegroups,maternalmorbiditycaseswere too few(less than20) forVBACto
show
rates
by
age
category.
2
Includes
births
with
previous
cesarean
history,
method
of
delivery,
or
maternal
morbidity
not
stated.
3Noresponse reported formaternalmorbidity item; includesbirths toresidentsofstatesusing the2003U.S.StandardCertificateofLiveBirthbutoccurring instatesusing the1989U.S.StandardCertificateofLiveBirth (0.3%).
NOTE:
Reporting
area
includes
Alaska,
California,
Colorado,
Delaware,
District
of
Columbia,
Florida,
Georgia,
Idaho,
Illinois,
Indiana,
Iowa,
Kansas,
Kentucky,
Louisiana,
Maryland,
Massachusetts,
Michigan,
Minnesota,
Mississippi,
Missouri,
Montana,
Nebraska,
Nevada,
New
Hampshire,
New
Mexico,
New
York,
North
Carolina,
North
Dakota,
Ohio,
Oklahoma,
Oregon,
Pennsylvania,
South
Carolina,
South
Dakota,
Tennessee,
Texas,
Utah,
Vermont,
Virginia,
Washington,
Wisconsin,
and
Wyoming.
-
7/23/2019 Morbidity of Women Who Give Birth
11/14
NationalVitalStatisticsReports,Vol.64No.4,May20,2015 11
Table2.Maternalmorbidity,bypreviouscesareanhistory,methodofdelivery,andDistrictofColumbiareportingarea,2013
[Ratesarenumberof livebirthswithspecifiedmorbidityper100,000 livebirths inspecifiedgroup]
andraceandHispanicoriginofmother:41-state
Raceand
andHispanicoriginmaternalmorbidity
Allbirths
Previouscesareanhistoryandmethodofdelivery
Withoutpreviouscesareandelivery Withpreviouscesareandelivery
Vaginal Primarycesarean VBAC1 Repeatcesarean
2All
races
Totalnumber . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Non-Hispanicwhite
Totalnumber . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Non-Hispanicblack
Totalnumber . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . .
Unplanned
hysterectomy
. . . . . . . .Admission to intensivecareunit. . . .
Non-HispanicAsian
Totalnumber . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . .
Condition reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
Hispanic
Totalnumber . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . .
Condition
reported:
Maternal transfusion. . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . Admission to intensivecareunit. . . .
3,548,52522,064
9,888922
1,4375,460
280.426.140.7
154.8
1,880,3505,590
276.724.338.9
120.1
511,1323,474
332.339.2
46.1239.5
206,651743
251.632.147.6
150.6
818,0062,234
247.120.340.1
182.0
2,322,3203,863
3,875146 277
1,497
167.16.3
11.964.6
1,250,4261,826
172.54.7
11.847.7
316,9721,042
156.410.1
13.080.7
133,109312
155.1**
67.8
539,552478
150.86.9
11.392.8
Number
of
686,1941,558
3,595337 462
2,623
Rate
525.149.267.5
383.1
Numberof
365,751730
Rate
532.044.965.2
309.8
Numberof
109,553474
Rate
584.967.8
59.6572.1
Numberof
43,385117
Rate
487.750.8
110.9367.5
Numberof
144,342185
Rate
453.044.465.2
428.0
births
births
births
births
births
54,933140
20124 2872
366.843.851.1
131.4
28,17450
334.2**
88.9
8,99559
402.9*
**
3,16410
****
12,67620
331.9**
173.8
464,3801,154
2,171412663
1,252
468.788.9
143.1270.3
230,594514
421.695.6
140.8215.1
72,924368
704.3118.5
165.4436.9
26,58469
335.7113.1124.5211.2
119,360160
419.551.2
139.3286.9
*
Figure
does
not
meet
standards
of
reliability
or
precision;
based
on
fewer
than
20
births
in
the
numerator.
1Vaginalbirthaftercesarean;98%ofvaginalbirthswere towomenwithnopreviouscesarean,while2%wereVBAC.Forsomegroups,maternalmorbiditycaseswere too few(less than20) forVBACto
show
rates
by
racial
and
ethnic
categories.
2Includesbirthswithpreviouscesareanhistory,methodofdelivery,maternalmorbidity, or raceandethnicitynotstated.3Noresponse reported formaternalmorbidity item; includesbirths toresidentsofstatesusing the2003U.S.StandardCertificateofLiveBirthbutoccurring instatesusing the1989U.S.StandardCertificateofLiveBirth (0.3%).
NOTE:Reportingarea includesAlaska,California,Colorado,Delaware,DistrictofColumbia,Florida,Georgia, Idaho, Illinois, Indiana, Iowa,Kansas,Kentucky,Louisiana,Maryland,Massachusetts,Michigan,
Minnesota,
Mississippi,
Missouri,
Montana,
Nebraska,
Nevada,
New
Hampshire,
New
Mexico,
New
York,
North
Carolina,
North
Dakota,
Ohio,
Oklahoma,
Oregon,
Pennsylvania,
South
Carolina,
South
Dakota,
Tennessee,
Texas,
Utah,
Vermont,
Virginia,
Washington,
Wisconsin,
and
Wyoming.
-
7/23/2019 Morbidity of Women Who Give Birth
12/14
12 NationalVitalStatisticsReports,Vol.64No.4,May20,2015
Table3.District
[Ratesare
Maternalmorbidity forwomenwithnopreviouscesareandelivery,ofColumbiareportingarea,2013
numberof livebirthswithspecifiedmorbidityper100,000 livebirths inspecifiedgroup]
bymethodofdeliveryandtrialof labor:41-stateand
Trialof labor
Attempted None
MaternalmorbiditySuccessful,
vaginalFailed,
primarycesareanPrimary
cesarean
Total1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . Notstated2 . . . . . . . . . . . . . . . . . . . . . . . . .
Condition reported:Maternal transfusion. . . . . . . . . . . . . . . . . . Ruptureduterus . . . . . . . . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . . . . . . . . Admission to intensivecareunit. . . . . . . . . . .
2,322,3203,863
167.16.3
11.9 64.6
273,120528
600.955.070.4
318.4
398,736705
486.946.566.6
420.6
1Includesbirthswithmaternalmorbiditynotstated.2Noresponse reported formaternalmorbidity item; includesbirths toresidentsofstatesusing the2003U.S.CertificateofLiveBirth (0.3%).
NOTE:Reportingarea includesAlaska,California,Colorado,Delaware,DistrictofColumbia,Florida,Georgia,Michigan,
Minnesota,
Mississippi,
Missouri,
Montana,
Nebraska,
Nevada,
New
Hampshire,
New
Mexico,
New
Carolina,
South
Dakota,
Tennessee,
Texas,
Utah,
Vermont,
Virginia,
Washington,
Wisconsin,
and
Wyoming.
StandardCertificateofLiveBirthbutoccurring instatesusing the1989U.S.Standard
Idaho, Illinois, Indiana, Iowa,Kansas,Kentucky,Louisiana,Maryland,Massachusetts,York,
North
Carolina,
North
Dakota,
Ohio,
Oklahoma,
Oregon,
Pennsylvania,
South
-
7/23/2019 Morbidity of Women Who Give Birth
13/14
NationalVitalStatisticsReports,Vol.64No.4,May20,2015 13
Table4.District
[Ratesare
MaternalmorbidityforwomenwithapreviousofColumbiareportingarea,2013
numberof livebirthswithspecifiedmorbidityper100,000 live
cesareandelivery,
births inspecifiedgroup]
bymethodofdeliveryand trialof labor:41-stateand
Trialof labor
Attempted None
MaternalmorbiditySuccessful,
VBAC1Failed,
repeatcesareanRepeat
cesarean
Total2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . Not stated3 . . . . . . . . . . . . . . . . . . . . . . . . .
Condition reported:Maternal transfusion . . . . . . . . . . . . . . . . . . Ruptured uterus . . . . . . . . . . . . . . . . . . . . Unplannedhysterectomy . . . . . . . . . . . . . . . Admission to intensivecareunit. . . . . . . . . . .
54,933140
366.843.851.1
131.4
25,92686
731.4495.4158.7356.0
432,547928
458.065.6
143.9265.3
1Vaginalbirthaftercesarean.2Includesbirthswithmaternalmorbiditynotstated.3No
response
reported
for
maternal
morbidity
item;
includes
births
to
residents
of
states
using
the
2003
U.S.
CertificateofLiveBirth (0.3%).
NOTE:Reportingarea includesAlaska,California,Colorado,Delaware,DistrictofColumbia,Florida,Georgia,Michigan,Minnesota,Mississippi,Missouri,Montana,Nebraska,Nevada,NewHampshire,NewMexico,NewCarolina,
South
Dakota,
Tennessee,
Texas,
Utah,
Vermont,
Virginia,
Washington,
Wisconsin,
and
Wyoming.
Standard
Certificate
of
Live
Birth
but
occurring
in
states
using
the
1989
U.S.
Standard
Idaho, Illinois, Indiana, Iowa,Kansas,Kentucky,Louisiana,Maryland,Massachusetts,York,NorthCarolina,NorthDakota,Ohio,Oklahoma,Oregon,Pennsylvania,South
-
7/23/2019 Morbidity of Women Who Give Birth
14/14
NationalVitalStatisticsReports,Vol.64No.4,May20,2015
U.S.DEPARTMENTOF
HEALTH&HUMANSERVICES
Centers forDiseaseControlandPreventionNationalCenter forHealthStatistics3311ToledoRoad,Room5419Hyattsville,MD207822064
FIRSTCLASSMAIL
POSTAGE&FEESPAID
CDC/NCHS
PERMIT
NO.
G-284
OFFICIALBUSINESSPENALTYFORPRIVATEUSE,$300
FormoreNCHSNVSRs,visit:http://www.cdc.gov/nchs/products/nvsr.htm.
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Overall findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Maternal age . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Race and ethnicity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Trial of labor and method of delivery . . . . . . . . . . . . . . . . . . . . . 5
Discussion
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Findings from thebirthcertificatecomparedwithotherstudies. . . . . . 5
Dataqualityofhealth information frombirthcertificates . . . . . . . . . . 6
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
List of Detailed Tables. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Acknowledgments
This report was prepared under the general direction of Delton Atkinson, Director of the Division of Vital Statistics (DVS), and Amy M. Branum, Chief of the Reproductive Statistics Branch (RSB). Joyce A. Martin, RSB LeadStatistician, provided helpful suggestions for the analysis in this report.Sharon E. Kirmeyer provided content review. This report was edited andproduced by NCHS Office of Information Services, Information Design andPublishing Staff: Jane Sudol edited the report; typesetting was done byJacqueline M. Davis; and graphics were produced by Odell Eldridge(contractor).
Suggestedcitation
CurtinSC,GregoryKD,KorstLM,UddinSFG.
Maternalmorbidityforvaginalandcesarean
deliveries,according topreviouscesarean
history:Newdatafromthebirthcertificate,
2013.Nationalvitalstatisticsreports;vol64
no4.Hyattsville,MD:NationalCenter for
HealthStatistics.2015.
Copyright information
Allmaterialappearing in thisreport is inthepublicdomainandmaybereproducedorcopiedwithoutpermission;citationas tosource,however, isappreciated.
NationalCenterforHealthStatistics
CharlesJ.Rothwell,M.S.,M.B.A.,Director
NathanielSchenker,Ph.D.,DeputyDirector
JenniferH.Madans,Ph.D.,AssociateDirectorfor
Science
DivisionofVitalStatistics
DeltonAtkinson,M.P.H.,M.P.H.,P.M.P.,Director
Fore-mailupdatesonNCHSpublicationreleases,subscribeonlineat:http://www.cdc.gov/nchs/govdelivery.htm.
Forquestionsorgeneral informationaboutNCHS:Tel:1800CDCINFO(18002324636)TTY:18882326348
Internet:http://www.cdc.gov/nchsOnlinerequest form:http://www.cdc.gov/info
DHHSPublicationNo.20151120CS255967
http://www.cdc.gov/nchs/products/nvsr.htmhttp://www.cdc.gov/nchs/govdelivery.htmhttp://www.cdc.gov/nchshttp://www.cdc.gov/infohttp://www.cdc.gov/nchs/products/nvsr.htmhttp://www.cdc.gov/nchs/govdelivery.htmhttp://www.cdc.gov/nchshttp://www.cdc.gov/info