Montreal canda chest 2015( Diaphragm Ultrasound)
31
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
538 -
download
3
Transcript of Montreal canda chest 2015( Diaphragm Ultrasound)
Role of Sonography in
RICU
Gamal Rabie Agmy, MD, FCCP Professor of chest Diseases, Assiut University
High Frequency
• High frequency (5-10 MHz)
greater resolution
less penetration
• Shallow structures

Low Frequency
• Low frequency (2-3.5 MHz)
greater penetration
less resolution
• Deep structures
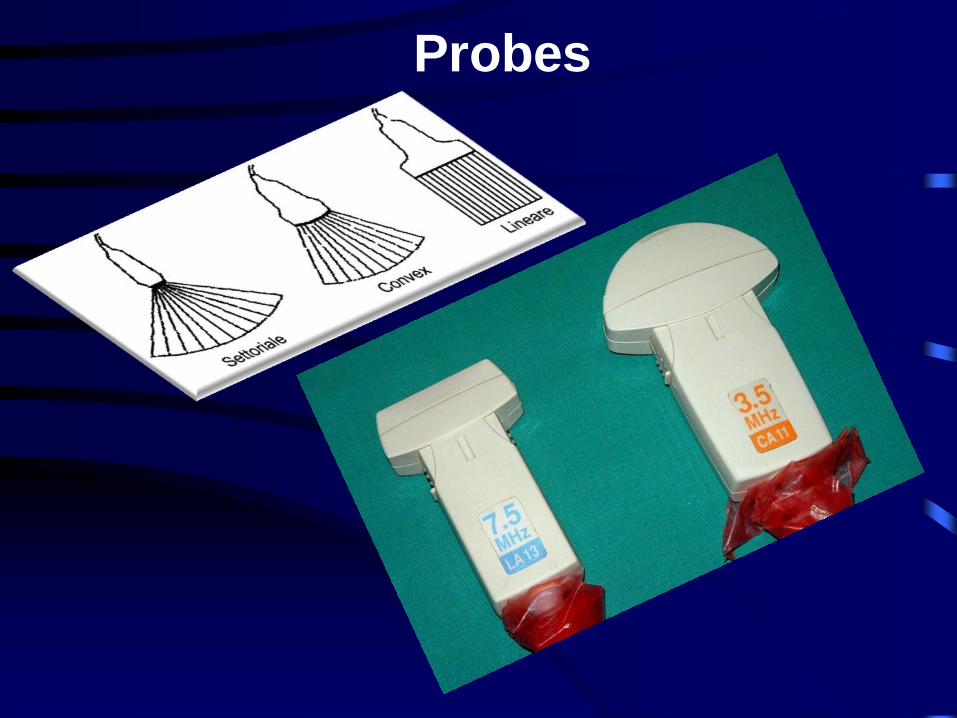
Probes

A common language: Color Coding
Black Grey White

Diaphragm Ultrasound as a
Novel Guide of Weaning from
Invasive Ventilation
Gamal Agmy , MD , FCCP Professor of Chest Diseases and respiratory ICU,
Assiut University, Assiut , Egypt

I have no Conflict of Interest


• Difficulties in weaning from
mechanical ventilation are
encountered in approximately 20%
of patients, and more than 40% of
the time passed in the intensive
care unit is spent to try to wean off
from mechanical ventilation
• Several indexes have been employed to assess the patient's ability to recover spontaneous breathing.
• Variables such as minute ventilation (Ve), maximum
inspiratory pressure (PImax), breathing frequency, rapid shallow breathing index (RSBI, i.e., respiratory
frequency/tidal volume), tracheal airway occlusion
pressure 0.1 s (P 0.1), P0.1/ PImax >0.3, P0.1Xf/VT<300 , a combined index named CROP
(compliance, rate, O2, pressure index) >13, IWI>25 and CORE >8 have been used in common clinical
practice
• Among the numerous parameters used
in clinical practice, the rapid shallow
breathing index is one of the most
accurate.

Objective
• The diaphragm thickeness
Fraction (DTF) measured by
ultrasound was evaluated as a
weaning predictor compared
with the rapid shallow breathing
index.

• A prospective study included 78 patients
with COPD exacerbation.
• All patients were ventilated in pressure
support through endotracheal tube.
• During spontaneous breathing trial (SBT),
the right diaphragm was visualized in the
zone of apposition using a 7.5 MHz linear
ultrasound probe.
• The equipment used were ultrasound
apparatus (ALOKA – Prosound – SSD –
3500SV)

Diaphragm Thickness (DT)
• High frequency transducer 7.5
MHz
• Anterior axillary line
• Sagittal image at the intercostal
space between the 7th/8th , 8th /9th
ribs
• Visualization of both the pleural
and peritoneal membranes at all
times while imaging the diaphragm
for thickness measurements.
• Zone of apposition


DTF was calculated as percentage
from the following formula:
T end-inspiration − T end-expiration
T end-expiration
DTF was measured during deep
inspiration and forced expiration

• The rapid shallow breathing index
(RSBI) was calculated.
• Weaning failure was defined as the
inability to maintain spontaneous
breathing for at least 48 h, without
any form of ventilatory support.

• A significant difference between
DTF at deep inspiration and forced
expiration was observed both in
patients who succeeded SBT and
patients who failed.

• DTF was significantly different between
patients who failed and patients who
succeeded SBT.
• A cutoff value of a DTF >40% was
associated with a successful SBT with a
sensitivity of 88%, a specificity of 92%, a
positive predictive value (PPV) of 95%, and
a negative predictive value (NPV) of 82%.
• On the other hand , RSBI <105 had
a sensitivity of 95%, a specificity of
90%, a PPV of 96%, and a NPV of
92% for determining SBT success.
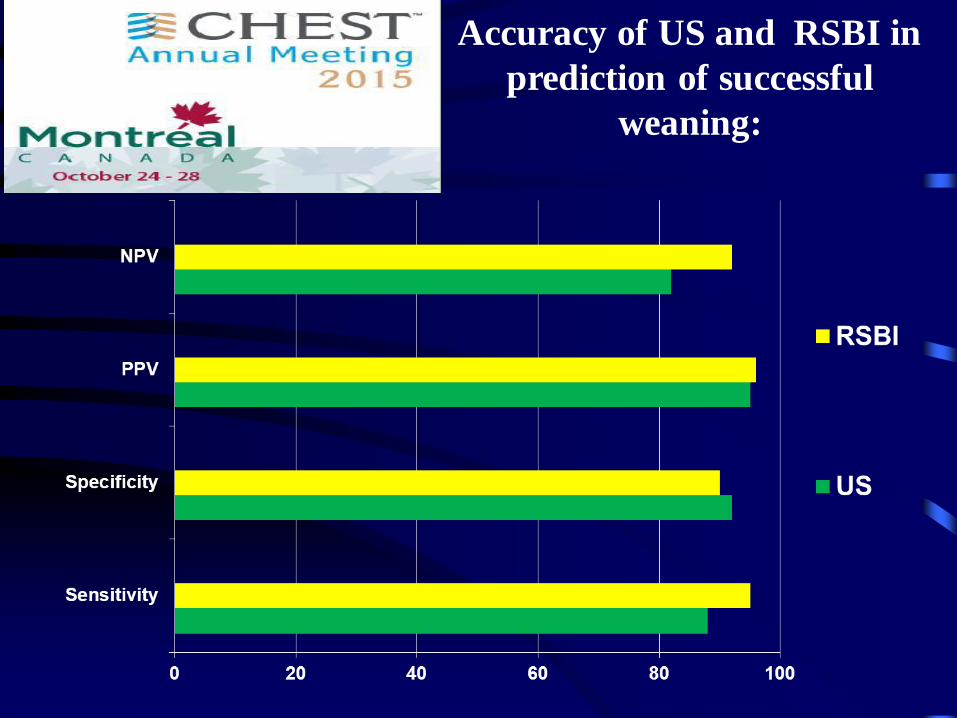
Accuracy of US and RSBI in
prediction of successful
weaning:

• DTF assessed by ultrasound is an
excellent predictor of weaning
outcome in COPD patients
undergoing mechanical ventilation.