Monitored Anaesthesia Care in the Elderlylibrary.tasmc.org.il/...Monitored Anaesthesia Care in the...
25
Dr\/ic\i/ A nTi^i c "^o^'^oino^cca-. 25ÍÓI. -177-500 KCVItW MKII^Lt n7O-229X/D8AX!OW3d77/S48.XW o 2008 Adis Doto infottnaikon BV. All rights Monitored Anaesthesia Care in the Elderly Guidelines and Recommendations Margaret Ekstein,^'^ Doron Gavish^-^ Tiberiu Ezrf^ and Avi A. 1 Department of Anesthesia and Critical Care Medicine, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel 2 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel 3 Department of Anesthesia, Wolfson Hospital, Holon, Israel 4 Post-Anesthesia Care Unit, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel Contents Abstract 478 1. Age-Related Physiological Changes in the Elderly 479 1.1 Changes in Organ Systems 479 1.1.1 Cardiac System 479 1.1.2 Pulmanory Function 480 1.1.3 Hepatic Function 480 1.1.4 Renal Function 480 1.1.5 Nervous System 481 1.1.6 Endocrine System 481 1.2 Pharmacodynamics 482 1.3 Pharmacokinetics 482 2. Patient Preparation 485 2.1 Preoperative Fasting 485 2.2 Long-Term Medications 485 2.3 Preoperative Testing 486 3. Patient-Specific Monitoring 486 4. Assessment of the Level of Sedation 487 5. Specific Agents, Doses and Reiated Risks for Medications Used for Monitored Anaesthesia Care (MAC) 487 5.1 Sedatives/Anxioiytics/Hypnotics 487 5.1.1 Benzodiazepines 487 5.1.2 Barbiturates 488 5.1.3 Propofol 488 5.1.4 Dexmedetomidine 489 5.2 Anaigesics 489 5.2.1 Remifentanil 489 5.2.2 Fentanyl and Alfentanil 489 5.2.3 Tramadol 490 5.2.4 NSAiDs and Cyclo-Oxygenase-2 inhibitors 490 5.3 Multimodal Analgesic Regimens 491 5.4 Drug Antagonists 491 5.4.1 Flumazenil 491 5.4.2 Naioxone 492 6. Specific Procedures Performed Under MAC 492
Transcript of Monitored Anaesthesia Care in the Elderlylibrary.tasmc.org.il/...Monitored Anaesthesia Care in the...

Dr\/ic\i/ A nTi^i c "^o^'^oino^cca-. 25ÍÓI. -177-500KCVItW MKII^Lt n7O-229X/D8AX!OW3d77/S48.XW
o 2008 Adis Doto infottnaikon BV. All rights
Monitored Anaesthesia Care inthe ElderlyGuidelines and Recommendations
Margaret Ekstein,^'^ Doron Gavish^-^ Tiberiu Ezrf^ and Avi A.
1 Department of Anesthesia and Critical Care Medicine, Tel Aviv Sourasky Medical Center,Tel Aviv, Israel
2 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel3 Department of Anesthesia, Wolfson Hospital, Holon, Israel4 Post-Anesthesia Care Unit, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
ContentsAbstract 478
1. Age-Related Physiological Changes in the Elderly 4791.1 Changes in Organ Systems 479
1.1.1 Cardiac System 4791.1.2 Pulmanory Function 4801.1.3 Hepatic Function 4801.1.4 Renal Function 4801.1.5 Nervous System 4811.1.6 Endocrine System 481
1.2 Pharmacodynamics 4821.3 Pharmacokinetics 482
2. Patient Preparation 4852.1 Preoperative Fasting 4852.2 Long-Term Medications 4852.3 Preoperative Testing 486
3. Patient-Specific Monitoring 4864. Assessment of the Level of Sedation 4875. Specific Agents, Doses and Reiated Risks for Medications Used for Monitored Anaesthesia
Care (MAC) 4875.1 Sedatives/Anxioiytics/Hypnotics 487
5.1.1 Benzodiazepines 4875.1.2 Barbiturates 4885.1.3 Propofol 4885.1.4 Dexmedetomidine 489
5.2 Anaigesics 4895.2.1 Remifentanil 4895.2.2 Fentanyl and Alfentanil 4895.2.3 Tramadol 4905.2.4 NSAiDs and Cyclo-Oxygenase-2 inhibitors 490
5.3 Multimodal Analgesic Regimens 4915.4 Drug Antagonists 491
5.4.1 Flumazenil 4915.4.2 Naioxone 492
6. Specific Procedures Performed Under MAC 492

478 Ekstein et al.
6.1 Oral or Dental Surgery 4926.2 Ophthalmology 4926.3 Plastic Surgery 4926.4 Interventional Radiology and Gastroenterology Procedures 4926.5 Awake Vascular and Neurasurgical Procedures 493
7. Potential Complications Associated with MAC in the Elderly 4937.1 Haemodynamic 4937.2 Airway and Respiratory 4937.3 Neurological 494
7.3.1 Delirium 4947.3.2 Postoperative Cognitive Dysfunction 494
7.4 Prolonged Hospitai Stay 4947.5 Closed Claims-Reiated Data 494
8. Postoperative Pain Control in the Elderly after MAC 4949. Discharge Criteria for the Elderly after MAC 495
10. Summary and Conclusion 495
AbstrOCt As the number of elderly patients undergoing surgery continues to rise, il isimportant to consider anaesthetic options that minimize physiological stress inthese patients. Monitored anaesthesia care (MAC), or sedation and monitoringduring surgery. Is an attractive option for certain common procedures. However,those administering MAC must consider the normal decline in functional reservein patients aged >70 years. This includes loss of normal compensation for thestress of hypovolaemia, decreased peripheral vascular resistance, altered mentalstatus and reduced response to hypoxia and hypercarbia associated with theperioperative and sedated state in this population. In addition, vigilance is neces-sary to identify co-morbid states, which increase in incidence with age and oftenpresent atypically. Elderly patients have increased sensitivity to all sedatives andopioids (doubled by age 80 years, quadrupled by age 90 years with benzodiaze-pines). As a result of changes in body composition, as well as senescence of renaland hepatic function, the time to onset and offset of even short-acting sedativeswill be prolonged. There is also extreme variability in the response to sedativesamong these patients.
Anaesthetic dosing should be in smaller increments in the elderly, bolusesreduced by half and infusions reduced by as much as two-thirds. Caution must beexercised through full monitoring of inlra-operative and postoperative mentalstatus, oxygénation and perfusion states. Pain is best treated using smaller doses ina multimodal regimen, the aim being to reduce adverse effects while ensuringadequate pain relief. In this way, a huge range of procedures can be safelyperformed in our aging population with expectations for a full and early return tobaseline functional status.
As life expectancy increases, the number of eld- five Americans will be aged >65 years, and 21% oferly patients undergoing surgical procedures contin- them will undergo surgery cacb year.''' Tlie fastestues to increase. Approximately 15% of tbe Western growing sector of the elderly population is tbe sub-population and about 25% of surgical patients are group aged >85 years.t-^ While the incidence ofcurrently aged >65 years. By the year 2030, one in intra-operative adverse events (primarily cardio-
© 2008 Aclis Data infcNmatkxi BV. All rights reseived. DnjQS Aging 2008; 25 (6)

Monitored Anaesthesia Care in the Elderiy 479
vascular) increases linearly with agep^ the availableevidence indicates that age itself is not the primarypredictor of perioperative mortality; rather, the exis-tence of co-morbid states, the site of surgery and thesetting of an emergency procedure are the importantfactors that predict outcome.'" ^
Monitored anaesthesia care (MAC) is care givenby an anaesthesiologist during surgery and consistsof monitoring with or without sedation. It is often asupplement to local anaesthesia provided by tbesurgeon. In this setting, the patient breathes sponta-neously and is arousable. comfortable and coopera-live. MAC is an alternative to general or regionalanaestbesia (spinal, epidural or major nerve block).Studies show cognitive decline in elderly patientsafter general anaesthesia, which may suggest thatMAC would be a better cboice for the elderly.' ^ Arecent study that specifically addressed tbe correla-tion between anaesthesia management and 1-yearmortality rate after major surgery with general an-aesthesia found that the cumulative time of deephypnosis as well as intra-operative hypotensionwere independent predictors of increased mor-tality.'^l Thus, the primary goal of MAC is to mini-mize the effects of anaesthesia on cardiovascular,pulmonary and neurological systems in the surgicalpatient while maintaining an unaltered functionalstatus.
There are also economic considerations that en-courage surgical procedures to be performed usinglocal anaesthesia with MAC, where feasible. Proce-dures may be located in a day surgery area of ahospital, outpatient surgical centres or at a doctor'soffice. Since many of these procedures are currentlybeing performed on patients aged >65 years usingMAC, there is a need to assess specific risk factorsand offer recommendations for the safe administra-tion of MAC in the elderly population.
In this article we review specific age-related is-sues regarding perioperative care of the elderly.These include the physiological and pharmacologi-cal changes associated with senescence, and theimpact of co-existing diseases in the elderly whentailoring anaesthetic techniques to such patients. Wealso review anaesthetic medications and monitoring
requirements for the safe performance of MAC inthe elderly. Finally, we discuss potential complica-tions, management of postoperative pain and readi-ness for discharge after the administration of MACin elderly patients.
1. Age-Related Physiological Changesin [he Elderly
1.1 Changes in Organ Systems
The process of natural aging causes a progressivedecline in the structure and physiological function ofall human beings. This process is probably causedby progressive damage by reactive free oxygen radi-cals to DNA and protein structure^'' and is asso-ciated with decreased function and reserve even in'bealtby' people aged >70 years. In addition tonatural decline, the incidence of eo-existing diseaseincreases with age.
/. Ï. / Cardiac SystetnAging brings about increased fibrosis ofthe myo-
cardium. There is preserved systolic function butimpaired diastolic filling ofthe left ventricle. Dias-tolic filling is more dependent on atriai contraction.Because tbe prevalence of atriai fibrillation in-creases witb age (the condition affects approximate-ly 5% of all patients aged >65 years), elderly pa-tients often have further compromise of ventricularfilling secondary to loss of atriai systole. Understress, such as that occurring during MAC and sur-gery, the heart has a reduced chronotropic and ino-tropic response to catecholamines and limited maxi-mal aerobic capacity. As a result, elderly patients aremostly dependent on preload to increase cardiacoutput during stress. Progressive ventricular byper-trophy develops in response to increased afterload.Ventricular hypertrophy increases both wall stressand myocardial oxygen demand and makes the ven-tricle more prone to ischaemia.
Although intrinsic contractility and resting cardi-ae output are unaltered with aging, the practicaleffect of ventricular hypertrophy and stiffening isthat the heart has limited ability lo adjust stroke
^ There is also an overall increase in left
' 2iX)8 Adis Data Information BV. All rights reserved. Drugs Aging 2008; 25 (6)

480 Ekstein et al.
atrial size with age that is thought to be secondary tothe chronic effect of reduced left ventricular com-pliance. Degenerative changes of the conductionsystem can also lead to heart block.' ^
In addition to normal cardiovascular aging, theincidence of coronary heart disease over a 10-yearfollow-up of adults aged >65 years was 39.6 in menand 22.3 in women per 1000 person-years; the inci-dence of congestive heart failure increased 9% witheach year over age 65.''°' Because normal physicalactivity declines and metaholic demands are re-duced, cardiovascular disease is not always recog-nized in the elderly and the clinical manifestationsare frequently atypical.f"' A history of cardiac dis-ease, cardiac risk factors, reduced exercise toleranceand type of surgery are predictors of perioperativerisk. Currently, guidelines for preoperative riskstratification and preparation are similar, whetherthe procedure is performed under MAC, regional orgeneral anaesthesia.
/. 1.2 Pulmonary FunctionThe pulmonary system also undergoes age-relat-
ed changes in hoth mechanics and control mechan-isms, independently of co-morbid disease processes.With aging, the thorax becomes stiffer.''^' This maynot be evident in the sedentary patient, but reducedchest wall compliance increases the work of breath-ing and reduces maximal minute ventilation.''^^ Be-cause of a decrease in elastic lung recoil, the closingvolume increases to such a degree that by age 65years it exceeds functional residual capacity.f'' ' In-spiratory and expiratory functional reserves de-crease with aging, normal ciliary function is de-creased and cough is reduced. Finally, matching ofventilation and perfusion is compromised.''•'' Thelatter process increases the alveolar-arterial oxygengradient and decreases resting oxygen partial pres-sure.
Sensation and the motor function required forswallowing are diminished. Airway protective re-flexes are weaker in the aged, which increases therisk of pulmonary aspiration of gastric content. Thisis a particular concern when the level of conscious-ness is depressed by sedatives, as often happens inpatients under MAC. There is also a decreased re-
sponse to hypoxaemia and hypercarbia.^'*' In thesetting of sedation with opioids or benzodiazepines.there are more episodes of apnoea or periodicbreathing. Oxygen supplementation and monitoringare therefore essential.
The risk of perioperative mortality in patientswith postoperative pneumonia is 20%.'"^ The oddsratio is 1.56 for patients of all ages undergoinggeneral anaesthesia compared with MAC or spinalanaesthesia, and 5.63 for patients aged >80 yearscompared with patients aged <50 years. History ofimpaired sensorium or permanent neurological defi-cit and dependent functional status are additionalrisk factors.
The risk of other pulmonary complications(bronchospasm, respiratory failure, atelectasis or ex-acerbation of underlying chronic lung disease) isapparently unrelated to age. It could be expected thatMAC. when applicable, would enable early detec-tion of exacerbation of pulmonary conditions inpatients with chronic lung disease. Importantly, ar-terial blood gases are less reliable predictors ofpulmonary risk in such individuals than clinicalfindings and exercise tolerance.
J. 1.3 Hepatic FunctionLiver blood flow falls by about 35% between
young adulthood and old age, and liver size by about25-50%. Serum and biliary cholesterol appear toincrease, predisposing elderly people to coronarydisease and gallstones. All of these point to an age-related decrease in biotransformation of manyanaesthetics and sedatives, especially those withlarge first-pass effects. Most intravenous anaesthcl-ics are metabolized primarily by the liver (with theprominent exception of remifentanii}. Hepatic hloodflow may be further compromised during sedation ifblood pressure (BP) falls because of the sedativesadministered, or if there is significant blood loss.Ordinarily, liver function tests are intact but ihe liverfunctional reserve is
1.1.4 Renal FunctionAnatomic abnormalities in the aging kidney in-
clude a decrease in kidney size, glomerular sclero-sis, altered tubular structure and an altered pattern ofvaseular flow. These anatomic abnormalities are
® 2008 Adis Data Inrormation BV. All rights reserved. Drugs Aging 2008; 25 C6)

Monitored Anaesthesia Care in the Elderly 481
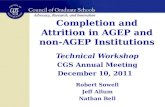
associated with renal functional abnormalities, in-cluding decreased renal blood flow and glomerularriltraiion rate (GFR) [figure 1 ]. Altered renal tubularfunction, including impaired handling of water, so-dium, acid and glucose, may also be present. Im-paired endocrine function, manifested by cbanges inihc renin-angiotensin system, vitamin D metabolismand anlidiuretic hormone responsiveness, is alsopresent. It bas been argued tbal hypertension, whichis frequently encountered in tbe elderly, is an impor-tant factor in the development and progression ofrenal insufficiency in tbe elderly.^-°'
The water content of tbe body declines witb age.Fluid intake is frequently reduced in senescencebecause of a reduced sensation of thirst. Tbe com-bined effects of water depletion, reduced barorecep-tor sensitivity and reduced cardiac reserve increasetbe risk for ortbostatic bypotension in tbe eldcrlyJ^'^This is partly responsible for the increased frequen-cy of perioperative cardiovascular instability ob-served in tbese patients.
1.1.5 Nervous System
Independently of any co-morbid process, bothilie central and peripheral nervous systems are af-fected by aging.' - ^ Loss of cortical grey matterbegins in middle age, resulting in cerebral atro-phy.'-•*' At tbe level of the neuron, tbe complexity ofneuronal connections decreases, tbe synthesis ofncurotransmilters decreases and tbe enzymes re-sponsible for tbeir postsynaptic degradation in-crease. While cerebral metabolism, blood flow and
250-1
50 60 70Age (y)
Fig. 1. Changes ¡n creatinine clearance and blood creatinine byage (reproduced from Shater,'^'' with permission).
autoregulation generally remain intact, neuronalloss and the deficiency of neurotransmitters limit tbeability of tbe older brain to integrate multiple neuralinputs. Functionally, spinal cord reflexes changeand proprioception is reduced. Tbere are also impor-tant decreases in bypoxic and bypercarbic drive.'-^'Declines in visual and auditory function furtbercomplicate tbe ability of tbe nervous system to ac-quire and process information. Tbis combination ofchanges can limit tbe ability of the older patient tounderstand and process information during MACand in the perioperative period. These cbanges areprobably important contributors to drug toxicily andpostoperative delirium.
Aging is also associated with neuronal loss in tbeautonomie nervous system. Botb sympatbetic andparasy m pathetic ganglia lose neurons, and fibrosisof pcripberal sympatbetic neurons occurs. This peri-pberal neuronal adrcnergic loss Is associated withimpairment of cardiovascular reflexesJ^^^
Numerous neurotransmitter systems are alteredwith aging. For example, dopamine uptake sites,transporters and levels are reduced. Cortical cholin-ergic activity also decreases, a finding of particularsignificance since failure of cholinergic neurotrans-mission is a central feature of Alzheimer's dis-ease.'-^' Slow reaction time and cognitive processingmanifest cognitive impairment. There is an inverserelationship between age and speed of motor per-formance. Tbe more complex tbe task, the slowertbe response. Tbis is caused by slow central process-ing of information. There is a deterioration in 'fluid'intelligence, i.e. the ability to respond to novel envi-ronmental events. Short-term memory is also affect-ed.f' ^ Cognitive and sensory difficulties frequentlyjeopardize obtaining informed consent from frailelderly paiients. Dementia, depression, hearing dif-ficulties and prior stroke may all interfere with theability to make independent decisions.'-^^ Tbeymight also hamper communication during MAC.
/. 1.6 Endocrine System
Impairment of glucose tolerance is a commonfeature of human aging. Diabetes mellitus is presentin 20.9% of people aged >65 years in the USJ^ ' Inaddition, a state of glucose intolerance (fasting glu-
; 2008 Adis Data Infcirmatian BV. All rights reswved. Drugs Aging 2008: 25 (6)

482 Ehtein el al.
cose between 100 and 125 mg/dL or blood glucosebetween 140 and 200 mg/dL after a 2-hour glucosetolerance lest) is present in 40% of people agedbetween 40 and 74 years, and is probably morecommon in people aged >75 years. With age, thereare changes in body composition, including a de-cline in fat-free mass and a decline in physicalactivity. Tbere is a reduction in insulin sensitivity inmuscle and fat and initially a hyperinsulin state,vfhich tapers off as pancreatic ß cells lose function.Thus, witb age, tbere is reduced sensitivity andavailability of insulin.f^°' Presentation of diabetes isatypical in the elderly, leading to a delay in diag-nosis, treatment and occurrence of severe secondaryvascular affects. Mortality risk is also bigh in hospi-talized elderly patients witb diabetes.'- ' Diagnosisis based on tbe same fasting and post-glucose loadlevels, but treatment in the elderly should betargeted to a bigber blood glucose level because oftbe increased incidence of bypoglycaemic events inelderiy patients witb diabetes treated witb oral anti-byperglycaemic agents.
As part of normal aging, secretion of thyrotropin-releasing hormone from tbe hypothalamus is re-duced; however, tbyroid-stimulating bormone(TSH) levels remain normal or in the low normalrange, levothyroxine sodium {T4) levels are normal,and Iiothyronine (T3) levels may be only slightlylow.f- J Tbere is some evidence for decreased tissuesensitivity (but not pituitary sensitivity) to tbyroidbormone. Tbyroid dysfunction is more common intbe elderly. Hypotbyroidism, defined as TSH >10 U/mL, is present in 5% of patients aged >60 years,compared witb 0.1% of patients aged <22 yearsJ^^lIts presentation is atypical and symptoms (tiredness,weakness, loss of appetite, etc.) are often misinter-preted as being related to advanced age or other co-morbidities rather than to a correctable tbyroid dys-function.'^-' Hypotbyroidism is associated with aworse cardiovascular status. Older patients requireless tbyroid replacement therapy than their youngercounterparts. Urgent surgery should not be post-poned because of mild or moderate hypotbyroidism;however, tbe anaesthetic doses used in sucb casessbould take into account the further reduction in
metabolic rate. Tbere is no consensus on tbyroidfunction screening recommendations. In addition tothyroid disease, poor health status is associated withlower T3 levels (secondary to reduction in conver-sion of T4 to T3), increased reverse T3 and de-creased TSH levels as part of tbe effect of chronicillness on tbe bypothalamic-pituitary axis. Serumreplacement is not helpful in tbese patients. Hyper-thyroidism in tbe elderly is often subclinical andpresents as 'apatbetic' hypertbyroidism. A bigb in-dex of suspicion is required as treatment can im-prove cognitive status significantly.
1.2 Pharmacodynamics
Aging often results in different responses to thesame effect-site drug concentration wben comparedwitb younger individuals.f "*' By using continuousEEG analysis during incremental dosing of seda-tives, it is possible to correlate the blood concentra-tion of a drug witb its effect on tbe EEG in volun-teers of different ages. In tbis way it has beendemonstrated that the brains of elderly people aremore sensitive to midazolam, - ''' opioids^^ ' and pro-pofol. ' In addition, the sensitivity of ß-adrc-noceptors, especially in tbe beart, to agonists andantagonists, is reduced.
1.3 Pharmacokinetics
Changes in body composition with age can affectdrug disposition in different ways. Increases in bodyfat and decreases in lean body mass and total btxlywater content, as well as relative cbanges in proteinconstituents, affect drug pbarmacokinetics. Mostsedatives follow a multi-compartment pharmacokin-etic model. With aging, tbe central compartment issmaller because of decreased body water and tbepeak concentration after a bolus dose migbt bebigber tban expected. On the otber band, becausefatty stores are increased, there might be prolongeddrug effects.'-" With aging, the circulatory level ofalbumin decreases while tbat of aj-aeid glycoprote-in increases.'-" Tbus, medications that bind to albu-min, e.g. diazepam, have an increased circulatingfree fraction and a smaller initial dose is needed:clearance may be increased. On the other band.
© 2G06 Adb Dota Information BV, All rights reserved. Drugs Aging 20O8. 25 (6)

Monitored Anaesthesia Care in the Elderly 483
Neonata
2 3 4 5 6 7 8 9 10 20 30 40 50 60 70 80 90 100
Age (y)
• ' " 'an' Chiid AduH ElderH K >+• H
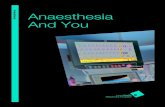
Fig. 2. Changes in pharmacokinetics with age. HalNiife {H) and both clearance and maintenance dosing rate of a drug vary with age. Thevalues are calculated from data for creatinine. tVi is expressed as a Iraction of the average value for a typical 55-year-old adult patient; thedosage regimen is calculated assuming that the desired average piateau unbound concentration of the drug (that is then eliminated entirelyby renal excretion with a clearance equal to the glomerular filtration rate) remains constant throughout iife. Elimination is slow in the neonatebecause of poor renal function but improves rapidly thereafter. Although bodyweight and, therefore, voiume of distribution change onlyslightiy beyond 30 years ol age, Ib is ionger in the aged, because renal function and, therefore, ciearance progressively diminish. By 95years of aga, tv¡ is twice the typical adult value (reproduced from Rowland and Tozer.i'*' with permission).
medications that bind to ai-acid glycoprotein have aleduccd free fraction causing reduced potency aswell as reduced clearance. In addition, quahtativechanges may occur in circulating proteins, therebyreducing tbe binding effectiveness of these proteins.Co-administered drugs may interfere with the abilityt)f anaesthetic agents to bind to these proteins, lead-ing to exaggerated clinical effects of the anaestheticdrugs. Decreased hepatic mass, hepatic blood Howand microsomal demethylation pathway activitywill result in greater bioavailability of agents withhigh hepatic clearance, e.g. alfentanil and propofol.An age-related reduction in creatinine clearance de-lays the offset of certain medications and their activemetabolites (figure 2). Tbis is seen after prolongedinfusions of midazolam in patients witb reducedrenal function.'^'
In addition, because of the huge range in baselinehealth status, there is great variability and unpredict-ability in the response of an elderly patient to anygiven dose.l- '' Medications must, therefore, be givenin small increments and titrated to effect. Important-ly, time lo peak effect is delayed and ample timemust be allowed to elapse before repeat dosing. This
will avoid unnecessary over-^sedatioti as well as ex-aggerated, undesirable adverse effects, which areknown to be more frequent in this population.
In summary, when dosing elderly individuals forsedation, it is important to consider the followingfive factors. First, changes in body compositionaffect drug volume of distribution and peak concen-tration. Secondly, because there is often a delaybetween delivery of a medication and its arrival atthe effect site, a delay in onset of effect should beanticipated. Thirdly, because clearance may be re-duced, infusion rates should be reduced to maintainthe desired peak concentration, and a delay in theoffset of effect should be anticipated. Fourthly, thereis a profound increase in sensitivity to all sedatives,hypnotics and opioids in elderly patients {octogenar-ians are twice as sensitive to opioids, benzodiaze-pines and propofol) and reduced reserve for com-pensating for respiratory and cardiovascular adverseeffects. Fifthly, variability of response to drugs in-creases witb age. Finally, as an example, in patientsaged 90 years, midazolam dose should be reducedby 75% for a colonoscopy and a delay in the offsetof effect should be expected^^^^ (table I).
200Ö Adis Data Irttormafion BV. All rights resefved. Drugs Aging 2008; 25 (6)

484 Ekstdn et ai
.>• o-9 E
fill
C3 Q. (D O)
Q. 11 .JC g ,
l > . gS? - >c « (0 ~
cï o c
'D. 'Q.¿ID to c
Ê i
ë "-g s.£ o (D
d O 3.
0) • -10 03
03
.S en
CVJ
Q .
l!i3 CD "D
e 3 i
Ilipll(3-g s 2 3 E 5• " - Q . 03 "CJ c
c £o Q)
59
a EÔ.O a T i " c - ^ § = *CO Q.Z -D 3 tD E S: .9
E g
o E <D
II œ ï Sîî J) 2 * oÜ ë ^ = .9?
.Sî 9 o =i: 5; 'S -c« w o) to «3 £ g>en a «J X tf) a . c
d± E ^
c a .Eto w c-5 £ S
lit.£ 03 2
fl 03 C3.9 S "5
03 .=jo fo
c p s cf o> 03Q s o o s i
S s-e S ä> oCO -D Q. CO T3 E
m Ec 03
< ce
&o 6X) E Q.
E
:!.l O
?Ö
g3
äo
© 2008 Adis Dalo Informatton BV. AH rights reservect. Drjos Aglng 2008; 25 C6)

Monitored Anaesthesia Care in the Elderly 485
o S
ft
ce pj â< s:
s S
5 &
CO • :
s? •—
1 1 :§
m a; i «
5 .s.E A
= to
0) OC
m £
to o
eu in
E 5
> ^
c tu 3Ï 2
es
o O A• 5 > Q . • -
to mII 3 —
UJ S £Ü 2 o< a. E
2. Patient Preparation
Clinicians should provide both patients and theirattendants with written instructions on preoperativefasting, medications, anaesthesia and postoperativecare.
2.1 Preoperative Fasting
Pulmonary aspiration of gastric contents is con-sidered to be a potential life-threaten ing complica-tion of anaesthesia. Patients should fast prior toanaesthesia to allow sufficient time for gastric emp-tying. Long-term prospective studies and retrospec-tive reviews have shown that the incidence of signif-icant clinical aspiration is 1.4-6/100 000 anaesthet-ics for elective general surgery.'"* ' No data areavailable as to the risk and incidence of pulmonaryaspiration associated with MAC. Risk factors foraspiration under general anaesthesia include a highAmerican Society of Anesthesiologists (ASA) phys-ical status score, difficult airway management, in-creased gastric volume and acidity, increased intra-abdominal pressure, gastro-oesophageal reflux, im-paired consciousness and extreme age.'"* ! The re-commended fasting period is 6 hours after solidfood, including milk, and 2 hours after clear liquids.When discussing fasting with the patient, it is impor-tant to be very specific as to what are 'clear liquids'.
2.2 Long-Term Medications
Patients must take necessary medications such asantihypertensive, cardiac, antiepileptic and asthmamedications with sips of water on the day of surgery.People with diabetes should continue taking oralantihyperglycaemic agents until the evening beforesurgery. Blood glucose levels must be checked andinsulin should be administered on the morning priorto surgery. Aspirin (acetylsalicylic acid) should bestopped 1 week before surgery if the dose is > 100mg/day. Anticoagulation with coumadin (warfarin)should be managed perioperatively according to therisk to the patient for thromboembolism andoperative bleeding. If the patient is at high risk ofthromboembolism (e.g. had a venous embolie eventwithin 3 months, has a mechanical cardiac mitral
2008 Adls Data Information BV. All rights reserved. Drugs Aging 2008; 25 C6)

486 Ekstein et al.
valve), coumadin should be stopped 4 days beforesurgery and intravenous heparin or low-molecular-weight heparin (LMWH) started 2 days before sur-gery. Intravenous heparin should be stopped 5 hoursbefore surgery and LMWH 12 hours before surgery.Coumadin and bridging anticoagulant should be re-sumed 12 hours after surgery, as long as there is nopostoperative active bleeding. If the patient is al lowrisk for thromboembolism (>3 months after acutevenous embolie event or atrial fibrillation withoutprior stroke), coumadin should be stopped 4 daysbefore surgery and resumed after surgery, while alsousing LMWH or subcutaneous heparin starting 12hours postoperatively until oral anticoagulationreaches the therapeutic range. If the surgical risk ofbleeding is low (e.g. gynaecological or orthopaedicprocedures), coumadin may be continued at a lowerthan usual dose, starting 4 days preoperatively, andaiming for an international normalized ratio of1.5-1.8.1^«]
Percutaneous coronary revascularization withstents requires prophylaxis with dual antiplatelettherapy: aspirin plus clopidogrel. Because perioper-ative stent thrombosis can be catastrophic, it is bestto delay surgery for 6-8 weeks after placement of abare metal stent and 12 months after placement of adrug-eluting stent. If surgery cannot be delayed andthere is significant risk of surgical bleeding,clopidogrel sbould be stopped 5-10 days beforesurgery, a bridging sbort-acting antiplatelet agentshould be used and clopidogrel should be restartedas soon as possible after surgery.i"' '
Tbe risks of withdrawal seem to justify continua-tion of selective serotonin reuptake inhibitors inpatients who are mentally stable.f™l Antidepressantsare often used by patients with neurodegenerativedisorders to help states of depressed mood, appetiteloss, insomnia, fatigue, irritability and agitation. Tri-cyclic antidepressants may cause ortbostatic hypo-tension and cardiac arrhythmias, especially in largedoses and during anaesthesia. Benzixiiazepines arethe most frequently prescribed psychotropic drugsin the elderly; however, they can cause confusion,sedation and ataxia, and are associated with an in-creased risk of falls and bone fractures. Antipsy-
cbotics have been shown to induce parkinsoniansymptoms in over 30% of all patients.'^'^ Tbe inci-dence increases with older age, pre-existing extra-pyramida! signs and with use of a drug such ashaloperidol.
Patients taking medications for Parkinson's dis-ease are very difficult to monitor as the adverseeffects of the drugs, such as lethargy, decreasedcognitive function and dyskinesia. are similar to themanifestations of the disease itself '''
Caution is needed when using NSAIDs in pa-tients aged >70 years because of possible adverseeffects (higher incidence of hyperkalaemia, renalfailure and gastrointestinal bleeding with a highmortality rate), especially in patients with pre-ex-isting renal failure.f - ^
2.3 Preoperative Testing
Preoperative laboratory tests are performed aspart of the preoperative assessment regardless of thetype of anaesthesia. Current recommendations arethat healthy elderly patients (aged >60 years) shouldbe routinely tested for haemoglobin and haemato-crit, glucose, blood urea nitrogen and creatinine.12-lead ECG and chest radiograph (where needed)abnormalities.''' "''"*' ASA classification and surgicalrisk are independent predictors of in-hospital ad-verse postoperative outcomes. Selective testing, asindicated by bistory and physical examination(which will determine the degree of co-morbidityand risk), is indieated;f''•''' such testing sbould includecoagulation studies.
3. Patient-Specific Monitoring
Basic monitoring recommended by the ASA forprocedures performed under MAC include ECG.BP, respiratory rate and pulse oximetry. However,the extent of monitoring should consider the pa-tient's condition and degree of invasiveness of thesurgical procedure and should not be minimizedsimply because tbe patient is 'awake'. Tbere is theadded value of an 'awake' patient's subjective feed-back of distress. This added value depends on thedegree of wakefulness, cooperation and reliability ofthe patient's J' ^
@ 2008 Adis Data lnto<matk>n BV. M\ rights reserved. Dnjos Aging 2006; 25 (a)

Monitored Anaesthesia Care in the Elderly 487
Importantly, qualified anaesthesia personnelmust be present in the room throughout the conductof all MAC. During all anaesthetics, the patient'soxygénation, ventilation and circulation should hecontinually evaluated. Pulse oximetry must be usedto ensure adequate oxygénation. Assessment ofqualitative clinical signs of ventilation, such as chestexcursion, auscultation of breath sounds or the pres-ence of exhaled carbon dioxide, is necessary in allcases where deep sedation is used. The ASA prac-tice guidelines for sedation and analgesia by non-anaesthesiologisLs further recommends followingIhc patient's response to verbal contact.'^''
Intra-operatively, all patients should be connect-ed to an ECG for continuous assessment of rate,rhythm and ST analysis. Use of two leads, typicallyleads II and V5, of an ECG, has been shown to havea high sensitivity for detection of myocardial ischae-mia. Circulatory evaluation by at least one of thefollowing is also essential: palpation of the pulse,monitoring of a tracing of intra-arterial pressure orpiclhysmography-associated oximetry.'^^l
4. Assessment of the Level of Sedotion
Scdalion is currently assessed by two scoringsystems:1. The Ramsay scale assigns a score of 1-6, basedon the clinical assessment of the level of sedation,evaluating response to sound, verbal commands ortactile stimulation by the anaesthetist. Scores l~3apply to arousable patients: 1 = anxious, agitated,restless; 2 = awake, but cooperative, tranquil, orien-lated; 3 = responds to verbal commands only. Scores4-6 apply to sleeping patients and are graded ac-cording to the response to a loud noise or a glabellarlap: 4 = brisk response; 5 = sluggish response; 6 = noresponse.'•'' • î
2. The sedation visual analogue scale (VAS) is asimple method of assessment in which a stimulatedpatient is asked how sedated he/she feels on a scalefrom I to 10. Patients differ considerably in theiriibility to reliably self-rate their sedation level usingIhe VAS.'^l
Sudden meaningful depression of vital signs,such as slow respiratory rate, low heart rate or BP,
are clinical signals of sedation-induced central de-pression that warrant quick medical and/or pharma-cological responses.
5. Specific Agents, Doses and RelatedRisks for Medications Used for MonitoredAnaesthesia Care (MAC)
The spectrum of medication used during MACincludes sedative/hypnotic/anxiolytic drugs to mini-mize the stress associated with the milieu of theoperating room, drugs with amnesic properties toreduce recall of intra-operative events and analgesicmedication to minimize patient discomfort from sur-gery (table I). Single- or multi-drug protocols mustbe tailored individually to the patient.
5,1 Sedatives/Anxiolytics/Hypnotics
5.1.1 BenzodiazepinosBenzodiazepines are commonly employed be-
cause of tbeir anxiolytic and amnesic effects.Among them, midazolam is a better alternative todiazepam because of its short half-life; it is alsowater soluble and causes no pain on injection.'^'^Midazolam is associated with good intra-operativeamnesia and sedation compared with propofol, butis also associated with a slower recovery time ofpsychomotor function.' - ^ Its onset of action is be-tween 2 and 2.5 minutes. Midazolam is metabolizedby the liver cytochrome P450 system to activehydroxymidazolam and inactive metabolites, whichare then secreted in the urine. Us half-life in adultvolunteers is between 1.5 and 3.5 hours, but tbis canbe prolonged after continuous infusions in very illpatients and in patients with decreased renal func-tion.'^'^ Small intravenous repetitive doses are re-commended to minimize deep/prolonged sedation.Of note, elderly patients are extremely sensitive tothe respiratory and cardiovascular effects of intrave-nous midazolam.'*^' On rare occasions (<1%), pa-tients treated with midazolam can develop paradoxi-cal reactions characterized by restlessness and agita-tion. This reaction can be reversed by small doses offlumazenil (0.1-0.5 mg),'^''-^' without reversing Ihe
' 2008 Adis Data Information BV. Ali rights reserved. Dnigs Aging 2008:25 <6)

488 Ekslein et ai
amnesic and sedative effects of the benzodiazepinereceptor agonist.
5.1.2 Barbiturates
Barbiturates have been used in the past for seda-tion during MAC.'^''! The most commonly used in-travenous barbiturates were methohexital and thio-pental sodium.' ^1 Methohexital 2.5 mg in a bolus isequivalent to propofol 5 mg for patient-controlledsedation in the elderlyJ* '! Methohexital provides anexcellent steady level of intra-operative sedationwhen administered via an infusion pumpJ™'
Of note, propofol has now fully replaced use ofbarbiturates in MAC.
5.1.3 Propofol
Propofol is a fast-acting intravenous sedative-hypnotic agent that rapidly and reliably reduces thelevel of consciousness.t^'l It is also associated with aquick and smooth recovery; adult patients typicallyregain consciousness within 8 minutes from cessa-tion of administration of propofol. The drug is safelyadministered in patients with kidney and liver fail-ure and may be useful in patients who have devel-oped tolerance to benzodiazepines. Careful titrationis mandatory as respiratory depression is always apotential danger because of significant decreases intidal and minute volumes; there is also a risk ofapnoea at higher than sedative doses and reductionsin both hypercarbic and hypoxic ventilatory re-sponses can f '
The cardiovascular effects of bradycardia, de-creased systemic vascular resistance and reducedcardiac output are mildly significant in patients re-ceiving low (sedative dose) rates of propofot infu-sions (table 11).'' ^ Time to peak effect is slightlyprolonged because of the pharmacokinetics of pro-pofol in the elderly. Recovery, although rapid, afterdiscontinuation of an infusion is significantly longerin elderly patients secondary to their increased sen-sitivity to propofol.''•'^ The blood propofol concen-tration required for 50% of patients aged 25 years tolose consciousness is twice that of patients aged 75years (figure 3). - ' The effect of propofol on systolicBP is also exaggerated in the elderly.''^! A smalldose of midazolam increases sedation, amnesia andanxiolysis when administered immediately prior tothe propofol infusion as part of sedation technique(table I).f ^ Some studies suggest that propofol(20 mg) possesses anti-emetic properties, with ashorter post-anaesthesia care unit stay and a greaterdegree of patient satisfaction.'"' ^ Pain on injection isthe most common adverse effect of propofol, fol-lowed by excitatory phenomena and involuntarymovements. Pain on injection can be minimized bypre-mixture of lidocaine (lignocaine) with the pro-pofol solution.' ^J Table II shows the age-relatedfrequency of unwanted adverse effects in propofol-sedated patients undergoing endoscopie proce-dures. '' ^
Table II. Frequency (%) ot unwanted adverse effects in propofol-sedaîed patients undergoing endoscopie procedures according to agegroup (reproduced from Heuss et al.,f ' with permission)
Adverse effect Cohort
age <70 y (n = 2534) age 70-85 y (n = 1167) age >85 y (n = 318) p-Values vs <70 y
Emergency interventions^
iV atropine administration
SaO2 decreased by >5%''
MAP decreased by >257o
SBP decreased to <90 mmHg
HB decreased by >20%
HR decreased to <50 bpm
0.3
0.1
2.0
6.8
32.817.4
13.53.4
0.3
0 ^
3 29.4
29.010.914.8
4.6
0.3
0.3
4.7
12.330.211.0
13.95.7
NS
NS
0.004
<0.0010.61
<0.0010.525
0.06a Includes Esmarch's manoeuvre, mask ventilation and/or placement of a nasopharyngeal airway.
b Oxygen 2 l_/min or more was continuously administered via a nasal probe.
bpm = beats per minute; HR = heart raie; IV - intravenous; MAP = mean arterial pressure; NS = not significant; SaO2 = arterial bloodoxygen saturation; SBP = systolic blood pressure.
® 2008 Adis Dafa Intormafion BV, Aii rights reserved. Drugs Agino 2008; 25 (6)

Monitored Anaesthesia Care in the Elderly 489
160-1
150-
140-
130-_120-§110-S 100-o^ 90-I 80-e 70-
60-
50-
40-
30-
20-
• Mean total doseO Mean dose needed to
begin endoscopy
10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85
Age (y)
Fig. 3. Influence ol age on the dose of propofol required duringmonitored anaesthesia care {reproduced from Heuss et al. , ' " ' withpermission).
5.1.4 Dexmedetomidine
Dexinedetomidine is a potent and highly selec-tive a2-adrenoceptor agonist with hypnosedativeand anaesthetic-sparing properties.l^^-^ ' It may beuseful for elderly patients undergoing cataract sur-gery under regional anaesthesia because it reducesintra-ocuiar pressure perioperativelyj^'^ as well asfor vascular surgery (carotid endarterectomy, peri-pheral revascularization), neurosurgery (awakecraniotomy), general surgery, plastic surgery and tosupplement regional or local anaesthesia. Dexmede-iomidinc decreases anxiety, sympathoadrenal res-ponse and postoperative opioid analgesic require-ments.' ''•^ '
5.2 Analgesics
Opioids can be used to supplement propofol andkical anaesthetics but migbt produce respiratory de-gression and a longer time-to-bome readiness.' ^• ''i
5.2. ] Remlfentanil
Remifentanil is a higbly potent opioid with arapid onset of effect and a short duration of actiondue to its rapid hydrolysis by esterases in blood andtissues.l"- ' Its terminal half-life in adults ranges from10 to 21 minutes. The rapid onset and short duration(if action of remifentanil make it well suited forliti'ation of dose (by changing infusion rate) to the
desired effect. Although remifentanil can produceopioid-related adverse effects, its rapid eliminationreduces the duration of these undesirable effects.'"^'An important consideration arising from its rapidclearance is the necessity for providing post-operative pain relief. In the elderly, the peak concen-tration of remifentanil is similar to that of youngerindividuals after an initial bolus, but takes slightlylonger to be reached because of slower equilibrationbetween blood and effect-site concentrations. On theother hand, because of increased sensitivity to thesedative effects of the drug in the elderly (approxi-mately double by EEG modelling), only half anadult bolus should be given. Since clearance ofremifentanil in the elderly is 66% ofthat in youngerpeople and the increased sensitivity ofthe elderly tothe drug means that only half the usual amountneeds to be administered, maintenance infusionsshould be run at about one-third the rate used inyounger individuals. ^^^
In younger adults, remifentanil provides com-parable intra-operative conditions to propofol seda-tion; however, it is associated with greater respira-tory depression, more episodes of desaturation andlonger time-to-home readiness. 1 - ' A study of se-dation of elderly patients (with significant co-mor-bid disease) during carotid endarterectomy under acervical plexus block showed that despite similarsedative effects, remifentanil 0.05 ^g/kg/min causedmore adverse respiratory effects than propofol I mg/kg/hour.'^''' Thus» propofol in elderly patients wasfound to be superior to remifentani! when used in thestated doses. Specific studies using other dosageregimens in this age group are lacking; nevertheless,remifentanil infusions should be used cautiously forsedation in the elderly.
5.2.2 Fentanyl and Alfentanil
Fentanyl, a synthetic opioid, is the most com-monly employed opioid for MAC. Even in smallboluses (25-50 p.g), it can cause respiratory depres-sion when combined with otber sedatives. Recoveryis significantly faster with alfentanil, another syn-thetic opioid, but young adult patients receivingalfentanil have a higher incidence of adverse events(chest wall rigidity, apnoea and laryngospasm) than
2008 Adis DcrtQ Intormcrtlon BV. All rights reserved. Drugs Aging 2008; 25 (6)

490 Ekstein et al.
those receiving fentanyl.t ^^ There are no consistentage-related changes in the pharmacokinetics of fen-tanyl or alfentanil. The decreased dose necessary forolder patients represents the increased sensitivity ofthese patients to opioids.' ' ' Along with the in-creased sensitivity to sedation, there is an increasedincidence of respiratory depression. In a retrospec-tive analysis of 8855 hospitalized patients who re-ceived opioids, patients aged 61-70 years had 2.8times the risk, those aged 71-80 years had 5.4 timesthe risk and those aged >80 years had 8.7 times therisk of significant respiratory depression, as com-pared with adults aged <45 years.'^' Conversely, therisk of nausea and vomiting decreased with age.Alfentanil given hy a pharmacokinetic-based targetcontrolled infusion for extracorporeal shock wavelithotripsy provided good analgesia with little seda-tion in a range of ages up to 77 years.^^" Respiratorydepression was uncommon, hut supplementary oxy-gen was recommended.
5,2.3 TramadoiTramadol is a centrally acting analgesic lacking
some of the adverse effects associated with otheranalgesic agents. Its dual mechanism of action in-cludes a weak affinity for the ^.-opioid receptor aswell as inhibition of the neuronal reuptake of nore-pinephrine and serotonin.' -^
Tramadol is rapidly absorbed and peak serumconcentrations are attained about 2 hours after oralingestion.Í"' It has an elimination half-life of 6.3hours and is poorly bound (20%) to plasma pro-teins.' "*' Tramadol is indicated for the managementof mcxlerate to moderately severe pain and the usualdose is 50-100 mg every 4-6 hours, as needed.f "*'Slowly titrating the dose was effective in signifi-cantly reducing adverse effects, such as vomiting(reduced by 60%) and nausea (reduced by 38%).that may have led to discontinuation at higher initialdoses.' •''' *' The maximum dosage of tramadolshould not exceed 4(K) mg/day or 1(X) mg/dose, andpatients aged >75 years should not receive morethan 300 mg/day.l ' ' In patients with a creatinineclearance <30 niL/min. the dosing interval should beincreased to every 12 hours and the total dose shouldnot exceed 200 mg/day. Patients with liver cirrhosis
should not receive more than 50 mg of tramadolevery 12 hours.
Overall, tramadol has demonstrated safety andefficacy and has a low abuse potential. A slowintravenous infusion of 50-75 mg before the end ofsurgery would provide good analgesia for 4-6 hourspostoperatively. It augments analgesia when parace-tamol (acetaminophen) is insufficient. Comparedwith traditional NSAIDs, tramadol lacks seriousgastrointestinal or renal toxicity, which are majorconcerns in elderly patients. Even though the newcyclo-oxygenase (C0X)-2 specific NSAIDs maydemonstrate greater gastrointestinal safety ihan theolder NSAIDs, tramadol has a superior renal safetyprofile. It may also be used to augment or replaceNSAIDs and has an advantage over opioids becauseit is associated with less respiratory depression.
5.2.4 NSAIDs and Cycio-Oxygenas9-2 InhibitcrsNSAIDs non-selectively inhibit COX-1, leading
to gastrointestinal and renal toxicity, and COX-2.leading to anti-inflammatory effects. NSAIDs arcadvantageous for perioperative management of painbecause they do not produce opioid-relatcd adverseeffects and have a sparing effect on opioids both interms of tbe amount required and adverse effects.They are one of the most commonly prescribedmedications worldwide as they are effective forchronic and acute pain.'"' For example, ketorolac. apotent parenterally active NSAID, has been usedboth as a sole analgesic and as a supplement topropofoi sedation during local anaesthesia. Intrave-nous ketoroiac 1 mg/kg up to a total dose of 60 mg(equipotent to 10 mg of morphine) is associated witha decreased incidence of pruritus, nausea and vomit-ing in the intra- and postoperative periods comparedwith opioids.'^^'
Selective COX-2 inhibitors appear to have anti-inflammatory and analgesic properties similar tothose of conventional, non-selective NSAIDs, butcause less gastrointestinal toxicity. COX-2 inbibi-tors thus may be safer than non-selective NSAIDsfor elderly patients, especially for those with a his-tory of gastrointestinal ulcers, since gastroduodenalulcération and bleeding is more common and has ahigher mortality rate in patients aged >70
© 2008 Adls Data Information BV. AH rlgt^ reserved. Drugs Agmg 2008:25 (6)

Monitored Anaesthesia Care in the Elderly 491
Age was shown to be an independent predisposingfactor for gastrointestinal bleeding, with the riskincreasing significantly in individuals aged >65years and increasing further in those aged >75 years.Indeed, bleeding incidence and mortality are dis-linctly higher in elderly patients.' ^^ Importantly,rofecoxib was withdrawn from the market in Sep-tember 2004 after preliminary results of the VIGOR(Vioxx Gastrointestinal Outcomes Research)irial' '™' showed five times the incidence of non-fatalmyocardial infarctions in the rofecoxib group com-piu-ed with the naproxen group.''*"' The risk ofcardiovascular and cerebro vascular events with oth-er COX-2 inhibitors, and with NSAIDs in general, isundergoing evaluation and their use for long post-operative periods or in patients with cardiovascularrisk factors should be implemented cautiously.
In addition, there are many reports of hyper-kalaemia and worsening renal failure in patientsgiven NSAIDs, specifically when given in conjunc-tion with ACE inhibitors, with or without diure-tics.'"^ '"**' Patients who have a history of congestiveheart failure (CHF) or, less commonly, hyperten-sion, may be managed for these conditions with acombination of an ACE inhibitor (or an angiotensinII lype 1 reeepior antagonist [angiotensin receptorblocker]) and a diuretic. Such patients should notreceive NSAIDs or COX inhibitors perioperative-ly [102] QpiR js dependent on renal blood fiow. affer-L-nt arteriolar vasodilation by prostaglandins andefferent arteriolar vasoconstriction by angiotensin.If both prostaglandins and angiotensin are inhibited(by NSAID analgesics or by long-term treatmentwith ACE inhibitors, respectively), renal blood flowmust increase to maintain normal GFR. Patientswho are volume depleted, have cardiomyopathy.renovascular disease or who are aged >75 years,luck the ability to make this compensation in renalblood How necessary lo maintain GFR, meaningrenal failure will ensue.'"^^' In addition, a case con-irol study showed a significant increase in the risk ofCHF in patients who recently (within the previousweek) .started NSAIDs other than aspirin.I'^'^' Therisk was higher in patients with known cardiac dis-
ease, and was correlated to the dose of the NSAIDgiven.
In summary, a recent review recommendedagainst using NSAIDs in patients with GFR <30mL/min, the US FDA has recommended not usingprescription NSAIDs in patients who have had re-cent cardiac revascularization procedures, and it isprudent to use the lowest possible effective dose inelderly patients because all adverse effects are dosedependent.'^^'05]
5.3 Multimodal Analgesic Regimens
As a result of the shift to office or outpatientsurgery, use of multimodal analgesic regimens,based on addition of non-opioid analgesics (e.g.local anaesthetics, NSAIDs, paracetamol, ketamine,a2-adrenoceptor agonists) to opioid analgesics, hasincreased. The opioid-sparing effects of these com-pounds reduce nausea, vomiting, constipation, urin-ary retention, respiratory depression, sedation andenhance postoperative pain relief.'"^^
5.4 Drug Antagonists
All types of drug antagonists should be used onlyand exclusively when reversal is mandatory andpatients should remain under medical observationfor twice the antagonist half-life in order to preventunobserved relapse of the untoward reversed phe-nomenon.
5.4.1 Flumazenil
Flumazenil, a 1.4-imidazobenzodiazepine. is aspecific benzodiazepine receptor antagonist that isindicated for use when the effect of a benzodiaze-pine must be quickly attenuated or terminated. Al-though flumazenil has a short elimination half-lifeof about 1 hour, an intravenous dose of up to 1 mg issufficient to attain and maintain the desired level ofconsciousness for 2 hours after conscious-to-moder-ate sedation induced by benzodiazepines inadults.'"'^•'^''l Small incremental doses of intrave-nous flumazenil 0.2 mg facilitate early recoverywithout adverse effects.'"^' Currently, the proveneffective dose of fiumazenil is up to 0.5 mg in the
¿' 2008 Adis Data Information BV. All rights reserved. Drugs Aging 2008: 25 (ó)

492 Ekslein et al.
" ' and in this clinical setting, true re-seda-tion does not occur.
5.4.2 Naloxon&Naioxone is an opioid receptor antagonist with a
rapid onset, short duration of effect and an elimina-tion half-life of 1-1.5 hours. Naioxone 0.1-0.5 mg(maximum 2 mg) administered slowly restores ade-quate ventilation in patients who have received ex-cessive doses of opioid analgesics.'"'^
6. Specific Procedures PerformedUnder MAC
A great variety of surgical procedures can beperformed under MAC. A comprehensive, althoughnot complete list, is provided by Smith and Tay-lor.f" ^ Studies specifically addressing sedation pro-tocols for selected procedures are reviewed in sec-lions 6.1-6.5.
6.1 Oral or Dental Surgery
Pharmacological strategies used in outpatientdental settings must specifically consider preserva-tion of protective upper airway reflexes. Intravenousmidazolam/fentanyl sedation, with or without pro-pofol, for dento-alveolar surgery provided stableintra-operative haemodynamics in elderly patientswith coronary artery disease.'"•'^ NSAIDs could beadministered to such patients at =50% of the adultdose.
Ó.2 Ophthalmology
Patients undergoing eye surgery are a challengeto the anaesthesiologist because of the increasedincidence of multiple systemic diseases in this pa-tient group. Low-dose (0.15 mg) oral clonidine aspre-medication before intra-ocular surgery under re-trobulbar anaesthesia appears to be comparable withuse of dexmedetomidine I M-g/kg over 10 minutes,followed by 0.1-0.7 [xg/kg/hour intravenous infu-sion, or to intravenous midazolam 20 |ig/kg fol-lowed by intravenous 0.5-mg boluses as required,for increasing patient comfort, offering haemodyna-mic stability and reducing BP response to periopera-tive stress.i^^"'*' These investigators also concluded
that dexmedetomidine alone was not suitable forsedation in patients undergoing cataract surgery be-cause of accompanying cardiovascular depressionand delayed recovery room discharge.
6.3 Plastic Surgery
In common with eye surgery, face-lifts and otherplastic surgery on the face and neck limit the anaes-thesiologist's access to the airway. Therefore, pres-ervation of a patent airway and effective spontan-eous ventilation are of utmost importance and neces-sitate careful drug titration to avoid deep sedation inthis setting. Abeles and Segueira'"^' recommendedusing propofol and fentanyl in standard doses inpatients aged between 25 and 65 years undergoingplastic surgeries. Doses must be adjusted in olderindividuals for conscious sedation.
Ó.4 Interventional Radiology andGastroenteroiogy Procedures
In some interventional radiology and gastroenter-oiogy procedures (e.g. gastroscopy), the anaesthesi-ologist and the interventionist compete for access tothe airway. Avoidance of deep sedation is crucialunder such circumstances to avoid hypoxaemia undairway obstruction. Administration of sedation andanalgesia in inlerventional radiology and gastroen-teroiogy suites is often necessary during painfuldiagnostic and some intravenous therapeutic proce-dures. For pre-emptive analgesia, oral paracetamolor an NSAID can be administered followed by tilra-tion of small doses of midazolam alone or combinedwith an opioid (e.g. intravenous midazolam l-mgand fentanyl 25-|lg boluses in incremental doses).Larger doses may be necessary during painful pro-cedures such as hepatobiliary intervention or uterinefibroid embolization.'"*' Use of dexmcdelomidincfor colonoscopy is considered unacceptable becauseof adverse effects such as haemodynamic instabilityand longer than desired sedation effect.
For patients aged >65 years with co-existing car-diac or respiratory illness undergoing other types ofprocedure (e.g. drainage of intra-abdominal collec-tion, nephrostomy insertion, trans-jugular hepaticbiopsy or anterograde ureteric stent insertion).
© 2008 Adis Data Intotmation BV. All rights feserved. I>UQS Aging 2008; 25 (6)

Monitored Anaesthesia Care in the Elderly 493
Skehan and Malone'"'' used fentanyl and midazo-lam that were administered in one to five steps (A.B, C, D, E) until the patient was drowsy and tran-quil: A, fentanyl 1 |lg/kg; B, midazolam 10-35 |lg/kg; C, repeat dose in A; D, repeat half dose in B; andE, midazolam 1- lo 2-mg boluses. Using this proto-col, sedation, analgesia and amnesia were achievedwithout patients becoming apnoeic, but increasedinspired oxygen concentration was necessary in partof the cohort.
6.5 Awake Vascular andNeurosurgical Procedures
Carotid endarterectomy (CEA) procedures aremore frequently undertaken under MAC or localanaesthesia alone to allow monitoring for inadver-tent brain ischaemia. The properties of dexmede-tomidine that result in titratable sedation and sympa-thetic modulation suit such conditions and providean acceptable alternative but provide no superiorityto standard techniques for sedation during awakeCEA performed under regional anaesthesia.
Anaesthetic techniques for awake craniotomyhave been evolving over the years and include localanaesthesia with mild sedation. Neurosurgical pro-cedures for tumour resection in eloquent brain areas(involving either speech or motor areas) and move-ment disorders are performed with the patient awakeand cooperative so that neurological status can bemonitored. Propofol sedation by infusion (1-1.5mg/kg/hour) or in small boluses is delivered at thetime of local anaesthesia infiltration and duringplacement of pins for the head holder. Both fentanylby bolus and remifentanil by infusion have beenused with equal success in conjunction with pro-pofol in younger individuals.'"^1 In the study byBerkenstadt and Ram,'"* ' propofol 100 )Xg/kg/minand remifentanil 0.01 |ig/kg/min for brain tumourremoval was found to be safe. The most commoncomplication was nausea and vomiting. Dexmede-tomidine 0.5 |ig/kg over 20 minutes followed by aninfusion of 0.01-1 jig/kg/min has also been usedsuccessfully.''-°'
7. Potential Complications Associatedwith MAC in the Elderly
Many elderly patients present to surgery withmultiple pre-existing morbidities that may induce ahigher risk of perioperative adverse events than ispresent in younger patients. Elevated ASA physicalstatus, history of ventricular arrhythmia, angina, hy-pertension, previous myocardial infarction, severebronchopulmonary disease, asthma, obesity andsmoking are predictors for perioperative complica-tions.''^'' Cardiovascular events are the most fre-quent intra-operative events, which are more preva-lent among the elderly. The incidence of intra-operative adverse events among elderly patients hasbeen found to be higher in ear. nose and throat,dental, urological. orthopaedic and ophthalmic sur-geries.'-'' Intra-operative arterial pressure should bemaintained within 20% of the best estimate of pre-operative arterial pressure. In those patients inwhom there is no contraindication, perioperative ß-adrenergic blockade may be of value. '~*^
7.1 Haemodynamic
Cardiovascular (risk factors: hypertension, is-chaemic heart disease, low cardiopulmonary reserveand compensatory incapacity) events are the mostfrequent intra-operative events in patients aged >65years.I'^J Overdose was found to be the primarycause of anaesthesia-related cardiac arrest anddeath, mostly in patients with spinal anaesthesia.'' "*^These events may occur during or after MAC ad-ministration.
7.2 Airway and Respiratory
The potential for compromising the respiratorysystem results from depression of oesophageal andlaryngeal reñexes, upper airway obstruction anddepression of central hypercarbic and hypoxic venti-latory responses.''-^' The patient must be carefullyand continuously monitored for all of these condi-tions and maximum airway patency preserved in theelderly.
> 2008 Adis DcilQ Information BV. All rights reserved. Drugs Aging 2008; 25 (ô)

494 Ekstein cl at.
7.3 Neurological
7.3.1 DeliriumDepending on the type of surgery. 10-50% of
older surgical patients develop aeute eonfusion.f' ^^Often, delirium is the only manifestation of seriousevents, such as myocardial infaretion, hypoxaemiaor sepsis.t' ^^ The risk factors for emergence deliri-um in an elderly but otherwise healthy patient areuse of preoperative henzodiazepines and surgery oflong duration.f'' ' Meperidine (pethidine) was con-sistently associated with an increased risk of deliri-um or cognitive decline in elderly patients, and otheropioids can also generate such occurrences on occa-sion. ' ^^ Titrated holus treatment of physostigmine0.2 mg, up to a maximum of 2.5 mg. accompaniedby close ECG monitoring, is a useful interventionfor preventing this undesired event (WeinbroumAA, unpublished data).
7.3.2 Postoperative Cognitive DysfunctionPostoperative cognitive dysfunction (POCD) is a
decline in cognitive function for weeks or monthsafter surgery. The subtle nature of this adverse eventmeans neuropsychological testing is necessary forits detection. Interpretation of the literature onPOCD is difficult because of numerous method-ological limitations, particularly the different defini-tions of POCD used and the lack of data fromcontrol groups.
The risk of POCD increases with age and thecomplexity of surgery; there is a very low incidenceassociated with minor surgery.i- ' Regional anaesthe-sia does not seem to reduce the incidence of POCD.
7.4 Prolonged Hospital Stay
In a study assessing predictors of prolonged post-operative hospital stay after ambulatory surgery,6301 individuals received MAC, 586 received localanaesthesia. 484 received regional anaesthesia and157 patients received a long-term pain block.'' ^^The mean age of patients receiving MAC was 67 ±16 years. Factors associated with prolonged staywere length and type of surgery, undesired eventssuch as excessive pain, nausea and vomiting, dizzi-
ness and cardiovascular events, and underlying eon-ditions such as CHF.
7.5 Closed Claims-Reiated Data
Analysis of closed-claims reports associated withMAC showed a high severity of patient injury and aliability profile similar to claims associated withgeneral anaesthesia, but a significantly smaller pro-portion of regional anaesthesia claims.''-^"' The mostcommon severe injury was severe respiratory de-pression resulting in death or brain damage in asso-ciation with drugs used during sedation. Of a total of121 claims for MAC patients, 26% were aged >70years and 63% were female. Elective eye, head,neck and face surgeries and endoscopies were pre-ponderant. Respiratory depression due to an abso-lute or relative overdose of sedative/hypnotic/anai-gesic agents was responsible for 25 MAC-relatedclaims (21%). Propofol was used in half of the cases,either alone or in combination with a benzodiaze-pine and/or an opioid. A combination of a benzo-diazepine and an opioid was used in seven cases ofdeath or brain damage. Although most patients weremonitored with pulse oximetry and 20% had bothpulse oximetry and capnography in use at the time ofthe event, nearly half of the claims were judged aspreventable by additional (or better) monitoring.Contributing factors to the serious incidents weredistraction due to loud music in the operating room,inattention to monitors, monitor alarms off. poorlyfunctioning pulse oximeters in sick patients, delay inresuscitation due to prone position (as during use ofa magnetic resonance imaging scanner) and poorresuscitation technique.
8. Postoperative Pain Control in ttieElderly after MAC
Given the expanding role of ambulatory surgeryand the need to facilitate earlier hospilal discharges,improving postoperative pain control (table III) hasbecome an increasingly important issue for allanaestbesiologists. Inadequately treated pain is amajor cause of unanticipated hospital admissionafter ambulatory surgery. Use of drug combinationsmay provide improved analgesia with fewer adverse
@ 2006 Adis Data Information BV. All rights reserved. Dfugs Agir>g 2008; 25 C6)

Monitored Anaesthesia Care in the Elderly 495
Table III. Analgesics commonly used for postoperative pain (reproduced with modifications from Zuccala et a l . , ' ' ^ with permission)
Drugs Maximum dailydose (mg)
Route Comments
NSAIDs or non-opioldsParacetamol (acetaminophen)
Dipyrone
Didofenac
T ramadol
Etodolac
Opioids
Buprenorphine
1000-1500
1000-2000
75
150
50-75
2100
0,4
PO/IV/PR
PO/IV/IM
PO
IM
Slow IV infusion
PO
IV
Morphine 30-40 IV
Not recommended in liver insufficiency
Possible allergy; slow infusion Is recommended; notrecommended in CRF
Nausea; start before end of surgery
Long-term use may affect stomach and kidney
Partial opioid receptor agonist. Rare psychomimetic effects;respiratory depression rare; PCA usefulStandard analgesic, IV bolus/infusion/PCA is optimal.Respiratory depression
CRF = chronic renal failure; IM = intramuscular; IV = intraver)ous; PCA = patient-controlled analgesia; PO = oral; PR = per rectum.
effects. The aim of any analgesic technique shouldbe to lower pain scores, facilitate earlier mobiliza-tion and reduce perioperative complications.t'^'' Theinitial treatment could include opioids, such as intra-venous morphine (up to 4 mg) or buprenorphine(0.4 mg), in divided doses, within the first post-operative 30-45 minutes, in order to achieve steady-state plasma concentrations and avoid drug accumu-iaiion while obtaining sufficient pain control (Wein-broum AA, unpublished data). Addition of NSAIDs,such as ketorolac 30-60 mg parenterally or intrave-nous lornoxicam 5-6 mg or tramadol 50-60 mg, isuseful since this may reduce opioid consumption.With the exception of tramadol, such treatment alsoleads to a reduction in postoperative nausea andvomiting, and all improve ventilation. Use of meper-idine should he discouraged because of the possibili-ty of toxic metabolite normeperidine-associated ad-verse effects.''-'1 Ketamine, given at a dose of250-350 |lg/kg intravenously concomitantly withmorphine 0.7-1 mg by bolus, can be used as anadjuvant drug for postoperative analgesia in in-pa-
9. Discharge Criteria for the Elderlyafter MAC
Recovery is a continual process, the early stagesof which overlap wilh the end of intra-operativecare. Patients cannot be considered fully recovered
until they have returned to their preoperative physio-logical state. Various scoring systems for evaluatingpatients' physical condition in the immediate post-operative period have been created and thereaftersimplified, and some arc based on physiologicalparameters rating patients' emergence from surgeryand anaesthesia.^'""'-'-^' Table IV sets out detaileddischarge criteria proposed by Marshall andChung.f' * ' Korttilat'"^ has also formulated guide-lines for safe discharge after ambulatory surgery.According to this author, the patient should havestable vital signs for at least 1 hour and be fullyoriented, able to dress, and able to walk unassisted.The patient should also have no postoperative nau-sea or vomiting, excessive pain or bleeding; havebeen discharged by both the anaesthetist and thesurgeon (or their designates); have written instruc-tions for home (including a contact phone, place andperson); and have a responsible adult caring for hitnor her over the first 24 hours. Before discharge, painmust be minimal or non-existent, effectively con-trollable by oral analgesics and its Ux:ation/type/intensity consistent with the anticipated discomfort.
10. Summary and Conclusion
The following key points summarize concernsregarding the elderly when undergoing proceduresunder MAC;
2008 Adte Data Intormotton BV, All hghts reserved. DnJOS Aging 2008; 25 (6)

496 Ekstein el al.
Table IV. Poslanaesthesia Discharge Scoring System (PADS) fordelermining home readiness (reproduced from Marshall and
' with permission)
1. Vital signs
Must be stable and consistent with age and preoperative baseline
BP/HR within 20% of preoperative baseline
BP/HR 20-40% of preoperative baseline
BP/HR >40% of preoperative baseline
2. Activity level
Patient must ambulate at preoperative level
steady gait, no dizziness, or meets preoperative level
requires assistance
unable to ambulate
3. Nausea and vomiting
Minimal nausea and vomiting
minimal, successfully treated with oral medication
moderate, successfully treated witti IM medication
severe, continues after repeated treatment
4. Pain
Pain acceptable to ttie patient
yes
no
21
0
2
1
1
2
1
0
2
1
5. Surgical bleeding
Bieeding consistent with expected blood loss for the procedure
minimal, not requiring dressing change 2
moderate, requiring one to two dressing changes 1
severe, requiring more than three dressing changes 0
Discharge minimal total score â9
BP = blood pressure; HR = heart rate; IM = intramuscular.
The physiology of aging is associated with aprogressive loss of functional reserve in all organsystems.
The extent and onset of these changes are highlyvariable from person to person, independently ofchronological age.
The elderly are more sensitive to anaestheticagents than young patients, even if healthy. Thus,less medication is usually required to achieve thedesired clinical effect, and drug effect is oftenprolonged.
The greatest concern of the elderly patient is tomaintain independence. Therefore, the most im-portant outcome and the overall objective of theperioperative care of this population is lo speedrecovery, avoid functional decline and provideearly home discharge.
• Surgical risk in patients aged >65 years dependsprimarily on the following factors: (i) age:(ii) physiological status, particularly mental;(iii) co-existing diseases (ASA class); (iv) type oíprocedure; and (v) whether the intervention iselective or urgent.
• When preoperatively evaluating a geriatric pa-tient, there should be a high index of suspicionfor disease processes commonly associated withaging.
• Prior to surgery, it is important to assess thedegree of functional reserve of specific, pertinentorgan systems as well as the patient as a whole.
• Routine testing based on age alone is currentlynot indicated. Instead, the patient should be se-lectively assessed on the basis of the history andphysical examination and the specific surgicalprocedure.
• Evidence-based data suggest that preoperativeco-morbid disease is a detetminant of post-operative complications. Anaesthetic care shouldbe tailored to co-morbid diseases and the require-ments of the surgical procedure.
• Pre- and postoperative management of cardiacand pulmonary problems in the elderly is ofparticular importance in the prevention of mor-bidity and mortality.
• MAC is an anaesthetized condition; all monitor-ing required hy the patient's status and surgicalprocedure are to be maintained.
• Important postoperative issues when caring forthe elderly include cognitive dysfunction andperioperative delirium.
• Pain is poorly accepted by the elderly; its optimalcontrol speeds recovery and the patient's inde-pendence and home discharge.
Acknowledgements
No sources of funding were used lo assist in the prcparu-lion of this review. The authors have no conOicts of interestthat are directly relevant to the content of this review.
References1. t..iu LL. Wicncr-Kronish JP. Perioperative anesthesia issues in
ihe elderly. Crit Care Clin 2003; 19: 641-56
® 2008 Adis Data Ir^formotion BV. All rights reserved. Drugs Aging 2006; 25 (6)

Monitored Anaesthesia Care in the Elderly 497
2. Jin F. Chung F. Minimizing perioperalive adverse events in Iheelderly. Br J Anaesih 2001: 87: 608-24
3. Chung F, Mezei G. Tong D. Pre-existing medical conditions aspredictors of adverse events in day-case surgery. Br J Anaesth1999:83: 262-70
4. Bufaiari A. Ferri M. Cao P, el a!. Surgical care in octogenarians.BrJSurg 1996:83: 1783-7
5. Muravchjck S. The elderly outpatient: curreni anesthetic impli-cations. CurrOpin Anacsihesiol 2002; 13: 621-5
6. Monk TG. Saini V. Weldon BC. et al. Anesthetic managementand one-year mortality after noncardiac surgery. Anesih Analg2005: 100:4-10
7. Bonnefoy M, Drai J, Kostka T. Antioxidants to slow aging, factsand perspectives. Presse Med 2002; 31: 1174-84
8. Folkow B, Svanborg A. Physiology of cardiovascular aging.Physiol Rev 1993; 73: 725-64
9. Mackstaller LL. Alpert JS. Atrial fibrillation: a review of mech-anism, etiology, and therapy. Clin Cardiol 1997; 20: 640-50
10. Arnold AM. Incidence ofcardiovasculardisease in older Ameri-cans: the cardiovascular health study. J Am Geriatr Soc 2005;53: 211-8
11. Bangalore S. Comparison of heart rate reserve versus 85% ofage-predicted maximum hean rate as a measure of chrono-Iropic response in patients undergoing dobutamine stress echo-cardiography. Am J Caidiol 2006; 97: 742-7
12. Wahba WM. Influence of aging on lung function: clinical sig-nificance of changes from age twenty. Anesth Analg 1983; 62:764-76
13. Fowler RW. Ageing and lung function. Age Ageing 1985; 14:209-15
14. Pontoppidan H. Geffin B, Lowenstein E. Acute respiratoryfailure in the adult: 1. N Engl J Med 1972; 287: 690-8
15. Kitamura H. Sawa T. Ikezono E. Postoperative hypoxemia: Ihecontribution of age to the maldistribution of venlilation. Anes-thesiology 1972; 36: 244-52
16. Cerveri I, Zoia MC, Fanfulla F, el al. Reference values ofarterial oxygen tension in ihe middie-aged and elderly. Am JRespir Crit Care Med 1995; 152:934-41
17. Arozullah AM. Khuri SF. Henderson WG. el al. Developmentand validation of mullifactorial risk index for predicting post-operative pneumonia after major noncardiac surgery. AnnIntern Med 2001; 135: 847-57
18. Wynne H. Drug metabolism and ageing. J Br Menopause Soc2005; 11:51-6
19. Schmucker DL. Aging and [he liver: an update. J Gerontol BiolSei Med Sei 1998; 53: B315-20
20. Meyer BR. Renal function in aging. J Am Geriatric Soc 1989;37: 791-800
21. Shafer SL. The pharmacology of anesthetic drugs in elderlypatients. Anesthesio! Clin North Am 2000; 18: 1-29
22. Tumheim K. Drug dosage in the elderly: is it rational? DrugsAging 1998: 13:357-9
23. Morris JC, McManus DQ. The neurology of aging: normalversus pathologic changes. Geriatrics 1991; 46: 47-8. 51-4
24. Creasey H. Rapoporl SI. The aging human brain. Ann Neurol1985; 17: 2-!0
25. Peterson DD. Pack Al. Silage DA, ei al. Effects of aging onvenlilatory and occlusion pressure responses to hypoxia andhypercarbia. Am Rev Resp Dis 1981: 124: 387-91
26. Phillips PA. Hod.sman GP. Jobnsion CI. Neuroendocrine mech-anisms and cardiovascular homeostasis in the elderly. Cardi-ovasc Drugs Ther 1991; 4 Suppl. 6: 1209-13
27. Francis PT, Palmer AM. The cholinergic hypothesis ofAlzheimer's disease: a review of progress. J Neurol NeurosurgPsychiatry 1999:66: 137^7
28. Crosby G. Culley DJ. Anesthesia, the aging brain, and tbesurgical patient [refresher course outline]. Can J Anaestb 2003;50: R12
29. John AD. Sieber FE. Age associated issues: geriatrics. Anes-tbesiol Clin North Am 2004: 22: 45-58
30. Rizvi AA. Management of diabetes in older adults. Am J MedSei 2007: 333: 35-Í7
31. Rosenlhal MJ. Fajardo M. Gilmore S. Hospiialization and mor-lalily of diabetes in older adults. Diabetes Care 1998; 212:231-5
32. Weissel M. Disturbances of thyroid function in the elderly.Wien Klin Wocbenschr 2006; 118: 16-20
33. Habra M. Sarlis NJ. Thyroid and aging. Rev Endocr MelabDisord 200.5:6: 145-54
34. Andrea H. Hartmul D. Lowenthal DT. Pharmacokinetic andpharmacodynamic changes in the elderly: clinical implica-tions. Clin Pharmacokinei 1998: 35: 49-54
35. Jacobs JR. Reves JG, Marty J. ei al. Aging increa.ses pharmaco-dynamic sensitivity to the hypnotic effects of midazolam.Anesih Analg 1995; 80: 143-8
36. Minto CF. Scbnider TW, Egan TD. et al. Influence of age andgender on the pharmacokinetics and pharmacodynamics ofremifcnianil: I. Model development. Anesthesiology 1997; 86:10-23
37. Scbnider TW. Minto CF. Shafer SL. et al. The influence of ageon propofol pharmacodynamics. Anesthesiology 1999; 90:1502-16
38. Rowland M. Tozer TN. Clinical pharmacokinetics: conceptsand applications. 3rd ed. Media (PA): Lippincott Williams &Wilkins, 1993: 235
39. Bell GD. Spickett GP. Reeve PA. et al. Intravenous midazolamfor upper gastrointestinal endoscopy: a study of 800 consecu-tive cases relating dose to age and sex of patient. Br J ClinPharmacol 1987:23:241-3
40. Cressey DM.Claydon P, BhaskaranNCetal. Effect of midazo-lam pretreatment on induction dose requirements of propofolin combination wiib fentanyl in younger and older adults.Anaesthesia 2001; 56: 108-13
41. Klotz U. Effect of age on pharmacokinetics and pharmaco-dynamics in man. Int J Clin Pharmacol Ther 1998; 36: 581-5
42. Fredmar B. Lahav M. Zobar E. et al. The effeci of midazolampremedication on mental and psychomotor recovery in geriai-ric patients undergoing brief surgical procedures. Anesth Ana-lg 1999:89: 1161-6
43. Heuss LT. Schnieper P. Drewe J. et al. Safely of propofol forconscious sedation during endoscopie procedures in high-riskpatienis: a prospective, coninilled study. Am J Ga.stroenterol2003:98: I75I-7
44. Jorden VS. Pousman RM, Sanford MM, et al. Dexmede-tomidine overdose in the perioperative setting. Ann Pharma-cother 2004: 38: 803-7
45. Arain SR. Ebert TJ. Tbe efficacy, side effects, and recoverycbaracteristicsofdexmedeiomidine versus propofol when usedfor intraoperative sedation. Anesth Analg 2002; 93: 461-6
46. Albashemi JA. Dexmedelomidine vs midazolam for moniloredanesthesia care during cataract surgery. Br J Anaestb 2006; 96:722-6
47. Scarlett M. Crawford-Sykes A, Nelson M. Preoperative slarva-lion and pulmonary aspiralion: new perspectives and guide-lines. West Indian Med J 2002; 31: 241-3
® 2006 Adis Dcrto tntormcitlon BV. All rights resefved. Drugs Aging 2008; 25 (6>

498 Ekstein et al-
48. Ansell J. Hirsh J, Dalen J. el al. Managing oral anticoagulanltherapy. Chesl 2001: 119: 22S-38S
49. Brilakis ES. Banerjee S, Berger PB. Perioperative managementof palienls with coronary stems. J Am Coll Cardiol 2007; 49:2145-50
50. Huyse FJ. Touw DJ. van Schijndel RS. et al. Psychotropic drugsand the perioperative period; a proposal Tor guideline in elec-tive surgery. Psychosomalics 2(X)6: 47: 8-22
51. Bunon DA. Nicholson G, Hall GM. Anesthesia in elderly pa-tients with neurodegeneralive disorders. Drugs Aging 2004;21:229-42
52. Jones AG. Hunter JM. Anesthesia in the elderly: special consid-erations. Drugs Aging 1996; 9: 319-31
53. Roizen M. Foss J, Fisher S. Preoperative evaluation. In: MillerRD. editor. Anesthesia. 5th ed. New York: Churchill Living-stone. 2000: 855-6
54. Velanovich V. The value of routine preoperative laboratorytesting in predicting the postoperative complications: a multi-variaie analysis. Surgery 1991; 109: 236-43
55. Dzankic S, Pastor D. Gonzales C, et al. The prevalence andpredictive value of abnormal preoperative laboratory tests inelderly surgical patients. Anesth Analg 2001: 93: 301-8
56. Buhre W, Rossaint R, Perioperative management and monitor-ing in anaesthesia. Lancet 2003; 362; 1839-46
57. Practice guidelines for sedation and analgesia by non-anesthesi-ologists: an updated report by the American Society of Anes-thesiologisu Task Force on Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology 2002: 96: [004-17
58. Ramsay MA, Savege TM. Simpson BR. et al. Conlrolled seda-tion with alphaxalone-alphadolone. BMJ 1974: 2; 656-9
59. Schulte-Tamburen AM. Scheier J. Briegel J. et al. Comparisonof five sedation scoring systems by means of auditory evokedpotentials. Intensive Care Med 1999; 25: 377-82
60. Carlsson AM, Assessment of chronic pain: aspects of the relia-bility and validity of the visual analogue scale. Pain 1983; 16:87-101
61. White PF. Vasconez LO. Mathes SA. et al. Comparison ofmidazolam and diazepam for sedation during plastic surgery,Plast Reconstr Surg 1988; 81: 703-12
62. White PF, Negus JB. Sedative infusions during local and region-al anesthesia: a comparison of midazolam and propofol. J ClinAnesth 1991:3:32-9
63. Zomorodi K, Donner A, Somma J, et al. Population phamiaco-kinetics of midazolam administered by target controlled infu-sion for sedation following coronary artery bypass grafting.Anesthesiology 1998: 89: 1418-29
64. Ronald I. Rational use of benzodiazepines in the elderly. DrugsAging 1994:4: 9-20
65. Thurston TA. Williams CG, Foshee SL. Reversal of a paradoxi-cal reaction of midazolam with flumazenil. Anesth Analg1996: 83: 192
66. Weinbroum AA, Glick A. Belhassen B. Rumazenil is innocu-ous in a paroxysmal supraventritular tachycardia and radiofre-quency ablation: a paediatric case report and review of theliterature. Paediatr Anaesth 2003; 13: 349-54
67. Kain ZN, A first-pass cost analysis of propofol versus barbitu-rates for children undergoing magnetic resonance imaging.Anesth Analg 1994; 79: 1102-6
68. Helge E. Clinically important drug interactions with intravenousanesthetics in older patients. Drugs Aging 2003: 20: 969-80
69. Hamid SK. McCann N. MtArdle L. et al. Comparison ofpatient-control led sedation with either methohexitone or pro-pofol, BrJ Anaesth 1996: 77: 727-30
70. Cohen M, Comparison of recovery of propofol and methohex-ital sedation using an infusion pump, Anesth Prog 1996; 43:9-13
71. Bryson HM. Propofol: an update of its use in anesthesia andconscious sedation. Drugs 1995; 50: 513-59
72. Dodds C, General anaesthesia: practical recommendations andrecent advances. Drugs 1999: 58: 453-67
73. Heuss LT, Schnieper P. Drewe J. et al. Conscious sedation withpropofol in elderly patients: a prospective evaluation. AlimentPharmacol Ther 2003: 17: 1493-501
74. Kreuer S. Schreiber JU. Bruhn J. et al. Impact of patient age onpropofol consumption during propofol-remifentanil anaesthe-sia. Eur J Anaesthesiol 2005: 22: 123-8
75. SchniderTW. Minto CF. Shafer SL. et al. The influence of agcon propofol pharmacodynamics, Anesthesiology 1999; 90:1502-16
76. Kazama T. Ikeda K. Morita K. et al. Comparison of the effect-site k(eO)s cf propofol for blood pressure and EEG bispectralindex in elderly and younger patients. Anesthesiology 1999;90: 1517-27
77. Taylor E, Ghouri AF, White PF, Midazolam in combinationwith propofol for sedation during local anesthesia. J ClinAnesth 1992; 4: 213-6
78. Gajraj NM. Nathanson MH. Preventing pain during injection ofpropofol: the optimal dose of lidocaine. J Clin Anesth 1996; 8:575-7
79. Levanen J. Makela ML. Dexmedetomidine premedication atten-uates ketamine induced cardiostimulatory effects andpostanesihetic delirium. Anesthesiology 1995; 82: 1117-25
80. Ben-Abraham R. Ogorek D. Weinbroum AA, Dexmede-tomidine: a promising agent for anesthesia and perioperativecare, Isr Med Assoc J 2000; 2: 793-6
81. Virkkila M. Dexmedetomidine as intramuscular premedicationfor day-case cataract surgery: a comparative study ofdexmedetomidine. midazolam and placebo. Anaesthesia 1994:49: 853-8
82. Jakkola ML, Dexmedetomidine premedication before intrave-nous regional anesthesia in minor outpatient hand surgery,J Clin Anesth 1994; 6: 204-11
83. Smith I, Avramov MN. A comparison of propofol and remi-fentanil during monitored anesthesia care. J Clin Anesth 1997:9: 148-54
84. Holas A. Remifentanil, propofo! or both for conscious sedationduring eye surgery under regional anesthesia, Eur J Anaes-thesiol 1999; 16: 741-8
85. Rosow C. Remifentanil; a unique opioid analgesic. Anesthesiol-ogy 1993; 79: 875-6
86. Avramov MN, Smith 1, White PF, Interactions between tnidazo-lam and remifentanil during monitored anesthesia care. Anes-thesiology 1996: 85: 1283-9
87. Krenn H. Deusch E. Jellinek H. et al, Remifentanil or propofolfor sedation during carotid endarterectomy under cer\'icalplexus block. Br J Anaesth 2002: 89: 637-40
88. Cooper GM. O'Connor M, Mark J. et al. Effect of alfentanil andfentanyl on recovery from brief anaesthesia. Br J Anaesth1983; 35 Suppl, 2: 179S-82S
89. Scott JC. Stanski DR, Decreased fentanyl and alfentanil doserequirements with age; a simultaneous pharmacokinetic andpharmacodynamic evaluation, J Phannacol Exp Ther 1987;240: 159-66
90. Cepeda MS, Farrar JT. Baumgarten M, et íü. Side effects ofopioids during short-term administration: effect of age, gender,and race, CliÜ Pharmacol Ther 2003; 74: 102-12
© 2008 Adis Data Informotton BV. All rl^its reserved. Drugs Aging 200S: 25 (6)

Monitored Anaesthesia Care in the Elderly 499
91. Irwin MG. Campbell RC. Lun TS, el a!. Patient maintainedalfentanil target-conlro!led infusion for analgesia during ex-iracorporeal shock wave lilhotripsy. Can J Anaeslh 1996; 43:919-24
92. Raffa RB. Friderichs E, Reimann W, el ai. Opioid and non-opioid components independenlly contribute lo the mechanismof action of tramadol. an "atypical" opioid analgesic. J Pharma-col Exp Ther 1992: 260: 27.1-85
93. Kalz WA. Pharmacology and clinical experience with tnunadolin osieoanhritis. r>n]gs 1996; 52 Suppl. 3: 39-47
W, Ortho-McNeil Pharmaceutical. Ultram® (tramadol hydrochlo-ride lahlets). In: Physicians' desk reference. .'Í3rd ed. Montvale(NJ): Medical Economics Company. 1999: 2254-7
95. Ruoff GE. Slowing the initial litralion rale of tramadol improveslolerability. Pharmacotherapy 1999; 19: 88-9.Í
96. Pétrone D. Kamin M. Olson W. Slowing the tiiration rate oftramado! HCl reduces ihe incidence of discontinuation due tonau.sea and/or vomiting: a double-blind randomized trial.J Ciin Pharm Ther 1999: 24: 115-23
47- Rahme E. Marenlelte MA. Kong SX. et al. Use of NSAIDs.COX-2 inhibitors, and acetaminophen and associatedcoprescriptionsofgastroproteciive agents in an elderly popula-tion. Arthritis Rheum 2002: 47: 595-602
98. Ramirez-Rui?. M. Smith I, While PF. Use of analgesics duringpropofol sedation: a comparison of IceEorolac, dezocine. andfentanyl. } Clin Anaesth 1995: 7: 481-5
99. Zullo A. Hassan C. Campo SM, et al. Bleeding peptic ulcer inthe elderly: risk factors and prevention strategies. Drugs Aging2007: 24 (10): 815-28
100. Bombardier C, Laine L, Reicin A. et al. Comparison of uppergastroinlesiinal toxicily of rofecoxih and naproxen in paiientswith rheumatoid arthritis: the VIGOR Study Group. N Engl JMed 2000: 343: 1520-8
101. StillmanMJ. Siillman MT. Appropriate use of NSAIDs: consid-ering cardiovascular risk in the elderly. Geriatrics 2007; 62:16-21
102. Jolohe OMP. Nephro toxicily in ihe elderiy due lo co-prescrip-tion of ACE inhibitors and NSAIDs, J R Soc Med 2001; 94:657-8
KB. Adhiyaman V, Asghar M, Oke A. et al. Nephrotoxicity in theetdcriy due lo co-pre.scription of angiotensin convertingenzyme inhibitors and nonsteroidal ami-inflammatory drugs.J R S o t Med 2001:94: 512-4
KM. Ruiz JG, Lowenthal DT. NSAIDs and nephrotoxicity in theelderiy. Geriatr Nephrol Urol 1997; 7: 51-7
105. Stillman MJ. Siillman MT. Choosing nonselective NSAIDs andselective COX-2 inhibitors in the elderly: a clinical use path-way. Geriatrics 2007: 62: 26-34
106. While PE. The changing role of non-opioid analgesic techniquesin ihe management of postoperative pain. Aneslh Anaig 2005:101 Supp!. 5: S5-22
107. Brogden RN. Goa KL. Elumazenil: a preliminary review of itsbenzodiazepine antagonist properties, intrinsic activity andtherapeutic use. Drugs 1988; 35: 448-67
108. Wcinhroum AA. Flaishon R. Sorkine P. et al. A risk-benefitassessment of flumazenii in the management of benzodiaze-pine overdose. Drug Saf 1997: 17: 181-96
1(19. McKay AC, McKinny MS. Clark RS. Effects of flumazenil onmidazolam-induced amnesia. Br J Anaesth 1990: 65: 190-6
110, Weinbroum AA, Szold O. Ogorek D. et al. The midazolam-induced paradox phenomenon is reversible by flumazenil;epidemiology, patient characteristics and review of Ihe litera-ture. Eur J Anaesthesiol 2001; 18; 789-97
111. John.son A. BengLsson M, Soderiind K, et al. Influence ofinirathecal morphine and naloxcme intervention on post-operative ventiiaiory regulation in elderly patients. ActaAnaesthesiol Scand 1992; 36: 436-44
112. Smith I. Taylor E. Monitored anesthesia care. Inl AnesihesiolGin 1994:32:99-112
113. Cilio JE, Einn R. Hemodynamics in elderiy coronary arterydisease patients undergoing propofol sedation. J Oral Maxil-lufat Surg 2006; 64: 1338-42
114. Weindler J, Kiefer RT. Rippa A, et al. Low-dose oral clonidineas premedication before intraocular surgery in relrobulbaranesthesia. Eur J Ophlhalmol 2000: 10: 248-56
115. Abeles G, Segueira M. The combined use of propofol andfentanyl for outpatient intravenous conscious sedation. I>erma-lolSurg 1999:25:559-62
116. Michael L. Lenox PH. Sedation and analgesia in intervenlionalradiology department. J Vase lnterv Radiol 2003; 14: 1119-28
117. Skehan SJ. Malone DE. Sedation and analgesia in adult patients:evaluaiion of staged-dose system based on body weight for usein abdominal inierventional radiology. Radiology 2000; 216:653-9
118. Manninen PH, Balki M, Lukiito K. ei al. Patient satisfactionwith awake craniotomy for tumor surgery: a comparison ofremifentanil and fenianyl in conjunction with propofol. AnesthAnalg2OO6; 102:237-42
119. Berkenstadi J, Ram Z. Monitored anesthesia care in awakecraniotomy for brain tumor surgery. Isr Med Asscx: J 2001 ; 3:297-300
120. Mack PF, Perrine K. Kobylarz E. et al. Dexmedetomidine andneurocognitive testing in awake cranioiomy. J NeurosurgAnesthesiol 2004; 16:20-5
121. Forrest JB, Rehder K. Cahalan MK. et al. Mullicenter study ofgeneral anesthesia: predictors of severe perioperative adverseoutcomes. Anesthesiology 1992; 76: 3-15
i 22. Howelt SSJ. Sear J W, Foex P. Hypertension, hypertensive hear!disease and perioperative cardiac risk. Br J Anaesth 2004; 92;570-83
123. Chung E, Mezei G. Adverse events in ambulatory surgery: acomparison between elderly and younger patients. Can JAnaesth 1999; 46: 309-12
124. Biboulet P, Aubas P. Dubourdieu J, ei al. Fatal and non fatalcardiac anests related to anesthesia. Can J Anaeslh 2001; 48:326-32
125. Nishino T, Takizawa K, Yokokawa N, et al. Depression of theswallowing reflex during sedation and/or relative analgesiaproduced by inhalation of 50% nitrous oxide in oxygen. Anes-ihesiology 1987; 67; 995-8
126. Fong HK. Sands LP, Leung JM. The role of posioperativeanalgesia in delirium and cognitive decline in elderly patients;a systematic review. Anesth Analg 2006; 102: 1255-66
127. Zuccala G. Cocchi A. Gambassi G. et al. Postsurgical complica-tions in older patienis: ihe role of pharmacological interven-tion. Drugs Aging 1994; 5: 419-30
128. Lepouse C. Lauther CA, Liu L. Emergence delirium in adults inposi anesthesia care unit. Br J Anaesth 2006; 96: 747-53
129. Chung E, Mezei G. Factors contributing to prolonged slay afterambulatory surgery. Anesth Analg 1999; 89: 1352-9
130. Bhananker SM. Posner KL, Cheney FW, el al. Injuiy andliability a.*isociaied wiih monitored anesthesia care: a closedclaims analysis. Anesthesiology 2006; 104: 228-34
131. Joshi GP. Postoperative pain management. Inl Anesthesiol Clin1994; 32; 113-26
•• 2D08 Adis Data Intofmatlon BV. All rights feserved. DnjQS Aging 2006; 25 (6)

500 ÍH et al.
132. Weinbroum AA, A single smalt dose of postoperative ketamineprovides rapid and sustained improvement in morphine anal-gesia in the presence Df tiiorphine-resistant pain. Anesth Atialg2003: 96: 789-95
133. Aldrete JA, The post anaesthesia recovery score revisited [let-ter], J Clin Anesth 1995: 7: 89-91
134. Aldrete JA, Post-anesthetic recovery score [tetter]. J Am CollSurg 2007: 205 (5): e3-4
135. Gawande AA. Kwaan MR. Regenbogen SE. el at. An Apgarscore for surgery, J Am Coll Surg 2007: 204: 201-8
136. Marshall S. Chung F. Assessment of "home readiness": dis-charge criteria and postdischarge complicaiions, Curr OpinAnaesthesiol 1997: 10: 445-50
137. Korttiia K, Recovery from outpatient anaesthesia, factors affect-ing outcome. Anaesthesia 1995: 50 Suppt.: 22-8
Correspondence: Dr Avi A. Weinbroiim, Professor of Anes-thesiology and Critical Care Medicine, Director, Post-Anes-thesia Care Unit, Tel Aviv Sourasky Medical Center,6 Weizman Street, Tel Aviv 64239, Israel.E-mail: [email protected]
© 2008 Adls Data Infomiaiton BV, AJI rights reserved. :25 (¿)