
Monika Equit · Heike Sambach Justine Niemczyk · Alexander ...
21
Monika Equit · Heike Sambach Justine Niemczyk · Alexander von Gontard Urinary and Fecal Incontinence A Training Program for Children and Adolescents
Transcript of Monika Equit · Heike Sambach Justine Niemczyk · Alexander ...

Monika Equit · Heike Sambach Justine Niemczyk · Alexander von Gontard
Urinary and Fecal Incontinence
A Training Program for Children and Adolescents

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Urinary and Fecal Incontinence

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Urinary and Fecal Incontinence
A Training Program for Children and Adolescents
Monika EquitHeike SambachJustine NiemczykAlexander von Gontard

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Library of Congress Cataloging-in-Publication Datais available via the Library of Congress Marc Database
National Library of Canada Cataloguing in Publication DataLibrary and Archives Canada Cataloguing in PublicationEquit, Monika, 1978– [Ausscheidungsstörungen bei Kindern und Jugendlichen. English] Urinary and fecal incontinence: a training program for children and adolescents/Monika Equit, Heike Sambach, Justine Niemczyk, Alexander von Gontard.
Translation of: Ausscheidungsstörungen bei Kindern und Jugendlichen. Includes bibliographical references. Issued in print and elec-tronic formats.
ISBN 978-0-88937-460-7 (pbk.), ISBN 978-1-61676-460-9 (pdf), ISBN 978-1-61334-460-6 (epub)
1. Urinary incontinence in children. 2. Urinary incontinence in children Treatment. 3. Fecal incontinence in children. 4. Fecal inconti-nence in children Treatment. I. Gontard, Alexander von, author. II. Sambach, Heike, author. III. Niemczyk, Justine, author. IV. Title. V. Title: Ausscheidungsstörungen bei Kindern und Jugendlichen. English
RJ476.I6E6813 2014 618.92’62 C2014-902523-8 C2014-902524-6
English translation prepared by Octavia Harrison with assistance of Alexander von Gontard, Monika Equit, and Justine Niemczyk.
© 2015 by Hogrefe Publishinghttp://www.hogrefe.com
PUBLISHING OFFICESUSA: Hogrefe Publishing, 38 Chauncy Street, Suite 1002, Boston, MA 02111 Phone (866) 823-4726, Fax (617) 354-6875; E-mail [email protected]: Hogrefe Publishing, Merkelstr. 3, 37085 Göttingen, Germany Phone +49 551 99950-0, Fax +49 551 99950-425; E-mail [email protected]
SALES & DISTRIBUTIONUSA: Hogrefe Publishing, Customer Services Department, 30 Amberwood Parkway, Ashland, OH 44805 Phone (800) 228-3749, Fax (419) 281-6883; E-mail [email protected]: Hogrefe Publishing c/o Marston Book Services Ltd, 160 Eastern Ave., Milton Park, Abingdon, OX14 4SB,
UK Phone +44 1235 465577, Fax +44 1235 465556; E-mail [email protected]: Hogrefe Publishing, Merkelstr. 3, 37085 Göttingen, Germany Phone +49 551 99950-0, Fax +49 551 99950-425; E-mail [email protected]
OTHER OFFICESCANADA: Hogrefe Publishing, 660 Eglinton Ave. East, Suite 119–514, Toronto, Ontario, M4G 2K2SWITZERLAND: Hogrefe Publishing, Länggass-Strasse 76, CH-3000 Bern 9
Should the print edition of this book contain a CD/DVD, then all material/worksheets included on the CD/DVD have been included in this e-book edition.
Copyright InformationThe e-book, including all its individual chapters, is protected under international copyright law. The unauthorized use or distribution of copyrighted or proprietary content is illegal and could subject the purchaser to substantial damages. The user agrees to recognize and up-hold the copyright.
License AgreementThe purchaser is granted a single, nontransferable license for the personal use of the e-book and all related files. Making copies or print-outs and storing a backup copy of the e-book on another device is permitted for private, personal use only.
Other than as stated in this License Agreement, you may not copy, print, modify, remove, delete, augment, add to, publish, transmit, sell, resell, create derivative works from, or in any way exploit any of the e-book’s content, in whole or in part, and you may not aid or permit others to do so. You shall not: (1) rent, assign, timeshare, distribute, or transfer all or part of the e-book or any rights granted by this License Agreement to any other person; (2) duplicate the e-book, except for reasonable backup copies; (3) remove any proprietary or copyright notices, digital watermarks, labels, or other marks from the e-book or its contents; (4) transfer or sublicense title to the e-book to any other party.
These conditions are also applicable to any audio or other files belonging to the e-book.
Cover illustration: Daniel Kleimenhagen, Designer AGD
Format: PDFISBNs 978-0-88937-460-7 (print), 978-1-61676-460-9 (pdf), 978-1-61334-460-6 (epub)http://dx.doi.org/10.1027/00460-000

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Table of Contents
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1 Theoretical Background
Chapter 1: Incontinence During Childhood and Adolescence . . . . . . . . . . . . . . . . . . . . . . . . . 51.1 Nocturnal Enuresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.1.1 Definition and Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.1.2 Subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.1.3 Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.1.4 Differential Diagnoses and Comorbid Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.1.5 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.2 Daytime Urinary Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101.2.1 Definition and Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101.2.2 Subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101.2.3 Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111.2.4 Differential Diagnoses and Comorbid Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.2.5 Comorbid Psychological Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.2.6 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1.3 Fecal Incontinence (Encopresis) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.1 Definition and Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.2 Subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.3 Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151.3.4 Differential Diagnoses and Comorbid Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161.3.5 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Chapter 2: Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.1 Standard Diagnostic Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
2.1.1 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.1.2 Development and Family History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.1.3 The 48-Hour Bladder Diary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.1.4 Physical Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.1.5 Sonography/Urine Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2.2 Extended Assessment for Complex Elimination Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . 232.2.1 Uroflowmetry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.2.2 Bacteriology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.2.3 Further Pediatric and Urologic Diagnostic Steps . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2.3 Psychological Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Chapter 3: Treatment of Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.1 General Treatment Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.2 Treatment of Fecal Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25

vi
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Table of Contents
3.3 Treatment of Daytime Urinary Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263.3.1 Urge Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263.3.2 Voiding Postponement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273.3.3 Dysfunctional Voiding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
3.4 Treatment of Nocturnal Enuresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273.5 Urotherapy as a Treatment for Complex Elimination Disorders . . . . . . . . . . . . . . . . . . . . . . 28
3.5.1 Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293.5.2 Scientific Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2 Therapy Manual
Chapter 4: Description and Structure of the Manual . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.1 Development of the Manual . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.2 Formal Aspects of the Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 344.3 Contents of the Sessions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 354.4 Including the Parents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364.5 Application as Individual Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364.6 Application to Adolescents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Chapter 5: Conducting the Individual Sessions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395.1 Bladder Training Session 1: Introduction, Defining Problems and Goals . . . . . . . . . . . . . . . 395.2 Bladder Training Session 2: Anatomy and Physiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 465.3 Bladder Training Session 3: Pathophysiology of Wetting and Coping With Stress . . . . . . . . 505.4 Bladder Training Session 4: Drinking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.5 Bladder Training Session 5: Going to the Toilet, Hygiene, and Constipation . . . . . . . . . . . . 595.6 Bladder Training Session 6: Emotions, Body and Bladder Perception . . . . . . . . . . . . . . . . . 635.7 Bladder Training Session 7: Knowledge Check, Goal Analysis, Outlook . . . . . . . . . . . . . . . 675.8 Bowel Training Session 1: Problem and Goal Analysis, Pathophysiology
of Fecal Incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 705.9 Bowel Training Session 2: Diet and Exercise . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Chapter 6: Evaluation of the Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 796.1 Sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 796.2 Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 796.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 806.4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 816.5 Final Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Preface
Elimination disorders are common and stressful disorders for children and adolescents. Addition-ally, they are often associated with comorbid psy-chological disorders. Elimination disorders include nocturnal enuresis (nighttime wetting), daytime urinary incontinence (functional urinary incon-tinence) and soiling (fecal incontinence or en-copresis). With specific evidence-based treatment methods, most children and adolescents can be treated successfully. These standard treatments, described in detail by von Gontard and Nevéus (2006), should be applied first. But there is a group of children and adolescents who do not respond to standard treatment and do not achieve conti-nence. Generally, these children are affected by complex elimination disorders. What does this term comprise?
On the one hand, these are children suffering from multiple elimination disorders (any combination of nocturnal enuresis, daytime urinary incontinence, fecal incontinence, and constipation). On the other hand, these children are often affected by comor-bid psychological disorders: 20–30% of children with nocturnal enuresis, 20–40% of those with day-time urinary incontinence, and 30–50% of children with fecal incontinence have at least one other psy-chological disorder (von Gontard, Baeyens, van Hoecke, Warzak, & Bachmann, 2011). These in-clude predominantly externalizing disorders as at-tention deficit hyperactivity disorder (ADHD) or conduct disorders. If these disorders remain unno-ticed or untreated, the compliance of the children as well as the treatment success will be decreased (Crimmins, Rathburn, & Husman, 2003).
Furthermore, subgroups of children without obvi-ous risk factors is also more difficult to treat and more likely to encounter a relapse or have con-tinuous incontinence as was shown in popula-tion-based longitudinal studies (Heron, Joinson, Croudace, & von Gontard, 2008). These relapses and persistent trajectories with continuing incon-tinence might be due to genetic and other congen-
ital factors. These chronically incontinent patients usually exhibit these problems from early age on-wards into adolescence and even adulthood. In these cases, incontinence is often associated with psychological strain, low self-esteem, hopeless-ness, and resignation. Moreover, problematic fa-milial interaction can impede the treatment. Par-ents often show higher treatment motivation than children. These problematic parent–child relation-ships can result in oppositional behavior of the children and in escalating conflicts. On the other hand, some parents think they have made mistakes in their childrearing; they feel responsible for their children’s incontinence and have feelings of guilt. Sometimes parents also see the incontinence as a deliberate provocation and react with punishment, which leads to further dysfunctional interactions.
All these groups of children have in common that they are resistant to standard treatment. This is es-pecially stressful for children but also for parents. Therapy resistance despite of correct treatment is perceived as a personal failure. This manual was developed for these children. The aim was to offer an efficient and structured treatment within a lim-ited number of sessions. The aim is to encourage children to actively restart their treatment and not to give up. Parents and children show a high ac-ceptance of this clear and manageable therapy pro-gram consisting of 7–9 afternoon sessions.
The treatment described in this manual can be conducted in an outpatient setting. Inpatient or day-care treatment is not necessary for most chil-dren with elimination disorders. This way, the children stay in their social environment and train their newly acquired skills at home. The group training is meant to motivate children and adoles-cents and to invigorate them for a new “round” of treatment. Additionally, new opportunities and perspectives can evolve. Thereby, children learn to take responsibility for their elimination disor-ders themselves and not to transfer it to their par-ents. Parents are informed and supported, but they

viii
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Preface
are not the main recipients of the treatment. They do learn, however, to return the commitment and responsibility needed for therapeutic success to their children.
Many different components are combined in the group training, e. g., provision of information, psy-choeducation, relaxation and body perception tech-niques, changing dysfunctional cognitions, and other elements of cognitive behavioral therapy. Therefore, it is far more than a mere training. The group format offers considerable advantages. Chil-dren learn that problems with incontinence are more common than they have thought. They see other children as also being affected by inconti-nence or as suffering from even more severe dis-orders. They learn to modify their own subjective views. They develop new coping strategies to-gether with the other children in the group train-ing. To avoid feelings of shame and embarrass-ment, the groups should be homogeneous regarding age and gender. Some of the training components have been adapted to the treatment of adolescents. If group training is not possible due to organiza-tional or other reasons, the components can be of-fered in individual sessions as well. In individual treatment, a selection of components of the train-ing can suffice.
This manual has been developed over the course of many years at the specialized outpatient depart-ment for elimination disorders at Saarland Univer-sity Hospital, Germany (Department of Child and Adolescent Psychiatry and Psychotherapy). Heike Sambach, a pediatric nurse and urotherapist, be-came aware of the need for special group training for children with therapy resistance. With great in-
novation, passion to experiment, and dedication she laid the foundation for this manual. In mutual cooperation, our group of authors further devel-oped and completed the manual, which is there-fore the result of creative teamwork.
The manual is aimed at pediatricians, specialists of child and adolescent psychiatry, psychologists, nurses, urotherapists, and all other professionals treating children and adolescents with elimination disorders. The training program was designed to be of fun for the children (as well as the thera-pists). It should, therefore, be carried out in a re-laxed and humorous way. The components of this manual are designed to be appealing and attrac-tive for children and adolescents.
We would like to express our gratitude to all the children, adolescents, and parents who gave us many insights over the years – and still do so every day. We wish to thank the editors of the Hogrefe publishing company, who responded very posi-tively to our proposal of creating this manual and have assisted us throughout the whole process. Our thanks also go to Dr. Manfred Vogtmeier, Ms. Alice Velivassis, Mr. Robert Dimbleby, Ms. Juliane Mun-son, and our translator Octavia Harrison.
We would be very pleased if our approaches were integrated extensively in all settings treating in-continent children and adolescents.
June 2014 Monika Equit Heike Sambach Justine Niemczyk Alexander von Gontard

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Introduction
Nocturnal wetting (nocturnal enuresis), daytime wetting (functional urinary incontinence), and fecal incontinence (encopresis) are categorized as elim-ination disorders. Elimination disorders are het-erogeneous in their clinical signs and symptoms, i. e., many different kinds and subtypes can be dis-tinguished. They are also heterogeneous with re-gard to their etiology. On the one hand, genetic factors can predominate (as in nocturnal enuresis). On the other hand, environmental factors can be more important (as in voiding postponement). And finally, they differ regarding type of treatment – in order to be effective, therapy has to be specific to each type of incontinence, which requires an exact diagnosis.
In contrast to many other disorders in child and adolescent psychiatry and psychotherapy, elimi-nation disorders can be treated quite effectively, resulting in high success rates. Most elimination disorders are functional in their pathogenesis, i. e., not caused by organic factors. Although psycho-logical disorders can co-occur, the etiology of elimination disorders is not mainly psychogenic, as previously assumed, i. e., they are not due to in-trapsychological or interpersonal conflicts and stressors. They are caused by a multivariate etiol-ogy with genetic dispositions, which are modu-lated by environmental factors. The aim of the treatment is always the achievement of continence, i. e., becoming completely dry or free from soil-ing. If children and adolescents become continent, there will be an improvement of psychological distress, self-esteem, and even behavioral symp-toms.
In order to attain this goal, simple but specific symptom-oriented treatment approaches are the most successful. These include counseling and components of cognitive behavioral therapy. When indicated, they can be combined with pharmaco-therapy. Neither surgical interventions nor long-term psychotherapy are needed in most cases.
Another advantage is that in almost all cases out-patient therapy is possible – inpatient or day-care treatments are usually not necessary. According to our experience, they are needed only in excep-tional cases and are mostly indicated by comorbid psychological disorders but not by elimination dis-orders themselves.
In summary, with exact diagnosis and specific therapy most incontinent children and adolescents can be treated well in an individual outpatient set-ting combined with parental counseling. Elimina-tion disorders treated that way can be considered “simple” disorders. Standard treatments for these uncomplicated disorders are described in detail in von Gontard and Nevéus (2006) and in von Gon-tard (2012a, 2012b). At our specialized outpatient clinic, we can witness every day that incontinence can be treated successfully through short and spe-cific interventions – much to the relief of children and their parents.
Unfortunately, in some children and adolescents treatment is not so successful. Despite optimal di-agnosis and specific therapy, they will not respond to standard treatments. These are so-called com-plex elimination disorders. The program presented in this manual is aimed at children and adolescents who do not respond adequately to standard treat-ment. Besides therapy resistance, these complex elimination disorders are often characterized by comorbidities, i. e., they often coexist with other psychological disorders. These difficult-to-treat children and adolescents have often been neglected in the past because their treatment resistance some-times leads to feelings of frustration and incompe-tence in therapists and doctors. Sometimes unnec-essary and ineffective treatments, such as inpatient treatment, nonindicated medication, or a pause in therapy are suggested.
This manual makes new therapy options available. It presents new topics and introduces a group for-

2
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Introduction
mat for therapy. The group setting gives children the opportunity to a step out of their isolation and to share their experiences with others. The follow-ing structure was chosen for this manual: The first part gives a short overview of the current state of research on elimination disorders. For even more detailed information, readers are referred to the literature on standard therapy (von Gontard & Nevéus, 2006; von Gontard, 2012a, 2012b). The second part is dedicated to the description of the group therapy itself. Following general informa-
tion on indication and procedures, every session is described in detail in a practical and clinically relevant way. There are 7 bladder training sessions for children with enuresis and urinary inconti-nence and 2 additional bowel training sessions for children with fecal incontinence (encopresis) and/ or constipation.
The materials for the group therapy can be printed out (see Appendix).

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
1 Theoretical Background

This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Chapter 1Incontinence During Childhood and Adolescence
1.1 Nocturnal Enuresis
1.1.1 DefinitionandClassification
According to both classification systems ICD-10 (WHO, 1993) and DSM-5 (APA, 2013), enuresis is defined as an involuntary voiding of urine in in-appropriate places from the age of 5 years on-wards after ruling out organic causes. According to the diagnostic criteria of ICD-10, wetting oc-curs at least either twice a month (age 5–7) or once a month (age > 7) for at least 3 consecutive months. According to DSM-5, wetting occurs twice a week or leads to social incapacitation for at least 3 con-secutive months.
According to the classification of the International Children’s Continence Society (ICCS), which is the gold standard in national and international re-search, enuresis (or nocturnal enuresis) is defined as any kind of wetting in discrete amounts while asleep (i. e., also during daytime naps) – indepen-dent of possible comorbid symptoms or assumed causes (Austin et al., 2014; Nevéus et al., 2006).
A minimum age of 5 years, a duration of 3 months, and a frequency of once per month is also required (Austin et al., 2014).
1.1.2 Subtypes
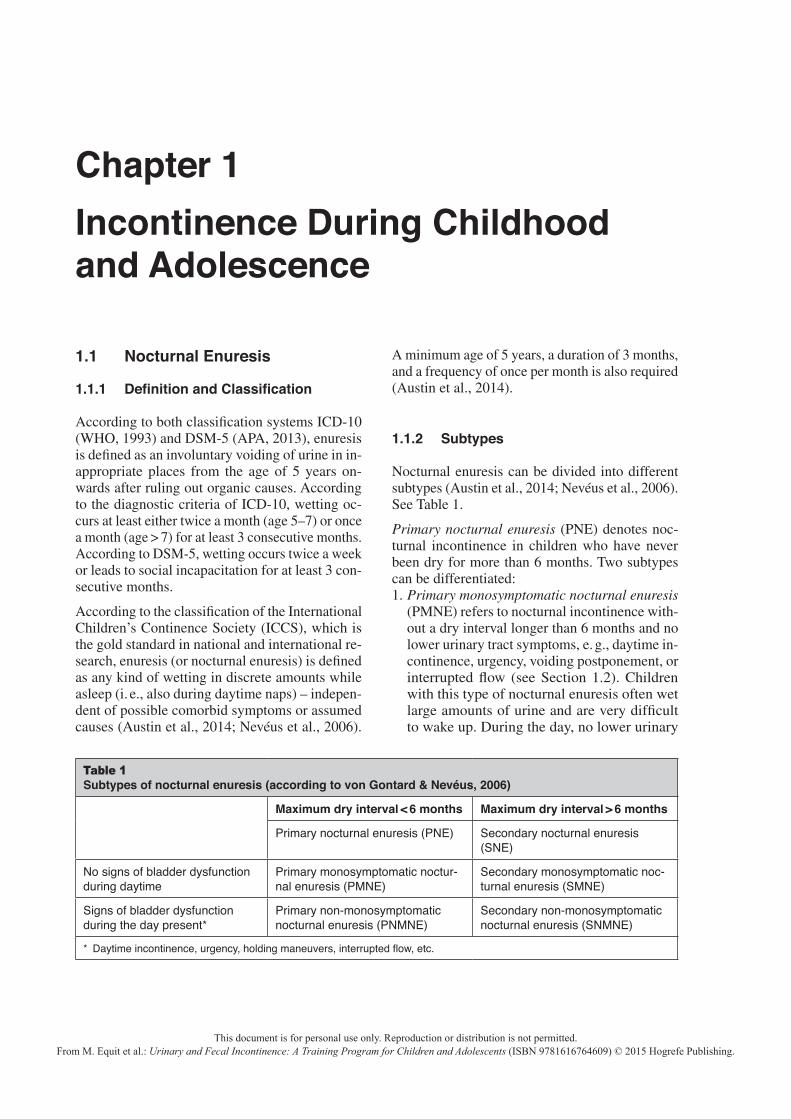
Nocturnal enuresis can be divided into different subtypes (Austin et al., 2014; Nevéus et al., 2006). See Table 1.
Primary nocturnal enuresis (PNE) denotes noc-turnal incontinence in children who have never been dry for more than 6 months. Two subtypes can be differentiated:1. Primary monosymptomatic nocturnal enuresis
(PMNE) refers to nocturnal incontinence with-out a dry interval longer than 6 months and no lower urinary tract symptoms, e. g., daytime in-continence, urgency, voiding postponement, or interrupted flow (see Section 1.2). Children with this type of nocturnal enuresis often wet large amounts of urine and are very difficult to wake up. During the day, no lower urinary
Table 1Subtypes of nocturnal enuresis (according to von Gontard & Nevéus, 2006)
Maximum dry interval < 6 months Maximum dry interval > 6 months
Primary nocturnal enuresis (PNE) Secondary nocturnal enuresis (SNE)
No signs of bladder dysfunction during daytime
Primary monosymptomatic noctur-nal enuresis (PMNE)
Secondary monosymptomatic noc-turnal enuresis (SMNE)
Signs of bladder dysfunction during the day present*
Primary non-monosymptomatic nocturnal enuresis (PNMNE)
Secondary non-monosymptomatic nocturnal enuresis (SNMNE)
* Daytime incontinence, urgency, holding maneuvers, interrupted flow, etc.

Chapter 16
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
tract abnormalities exist. The micturition fre-quency is normal (4–7 times a day) and the amount of urine during daytime is appropriate for age. No urgency is present; the children do not show holding maneuvers, they can empty their bladder without any problems, and they do not soil.
2. Primary non-monosymptomatic nocturnal enure-sis (PNMNE) refers to nocturnal incontinence without a dry interval longer than 6 months with disturbances of bladder function. For instance, these children can show urgency, voiding post-ponement, or interrupted flow.
Children with secondary nocturnal enuresis wet during the night after a dry period of at least 6 months. Again, two subtypes are differentiated:1. Secondary monosymptomatic nocturnal enure-
sis (SMNE) is defined as nocturnal incontinence after a dry period of at least 6 months without any signs of bladder dysfunction.
2. Secondary non-monosymptomatic nocturnal en-uresis (SNMNE) describes nocturnal inconti-nence after a dry period of at least 6 months with signs of bladder dysfunction – as in PNMNE.
The differentiation between monosymptomatic and non-monosymptomatic is more relevant for treat-ment. Disturbances of bladder function have to be treated first. Treatment is the same in primary as in secondary types. However, children with second-ary nocturnal enuresis have a higher risk for comor-bid psychological disorders, which, if necessary, have to be treated in addition to the incontinence.
1.1.3 Prevalence
Nocturnal enuresis occurs 2–3 more often than daytime urinary incontinence. The sex ratio is 1.5:1 to 2:1 (boys to girls). Depending on defini-tion, prevalence rates are 43.2% in 3-year-old chil-dren and 20.2% in 4-year-old children. However, enuresis is not a formal diagnosis at this age (not until age 5 according to ICD-10, DSM-5, and ICCS). Of 5-year-old children, 15.7% are affected, of the 6-year-olds 13.1%. The prevalence rate de-creases to 2.5% in children between 7 and 10 years of age. In adolescence, 1–2% still wet during the night and in adulthood 0.3–1.7%. Here the high
rate of spontaneous remission of nocturnal enure-sis of approximately 13% per year becomes ap-parent (Hellström, Hanson, Hansson, Hjälmås, & Jodal, 1990; von Gontard & Nevéus, 2006). Ac-cording to the large epidemiological Avon Longi-tudinal Study of Parent and Children (ALSPAC, Golding, Pembrey, & Jones, 2001), at the age of 7 ½ years 15.5% (of 8,269 children) wet during the night (Butler, Golding, Northstone, & AL-SPAC Team, 2005). Most of these children wet ap-proximately once a week (82.9%). According to DSM-IV, 2.6% fulfilled the criteria for nocturnal enuresis, thus wetted at least twice a week. In their study of 2,856 children with a mean age of 7.3 years, Sureshkumar and colleagues (2009) found a prevalence rate for nocturnal enuresis of 18.2%. Of these children, 12.6% had nocturnal en-uresis with a frequency of 1–6 times per month, 3.6% of them wet every night. In an epidemiolog-ical study by two of the authors with 2,079 pre-schoolers (mean age of 6 years), a prevalence rate of 9.5% for nocturnal enuresis was found (Equit, Klein, Braun-Bither, Gräber, & von Gontard, 2013). Of these children, 2.7% wetted during the day at least once a month. In another population-based study of 1,391 6-year-old children, 13.4% showed daytime or nighttime wetting: 9.1% wetted at night and 4.4% during the day (von Gontard, Moritz, Thome-Granz, & Freitag, 2011).
In general, PNE occurs more often than SNE, but until the age of 7, SNE appears as often as PNE (5.2%; Fergusson, Horwood, & Shannon, 1986). SNE occurs the most often at the age of 7 (5.1%). Further epidemiological studies show that mono-symptomatic nocturnal enuresis (MNE) occurs twice as often (68.5%) as non-monosymptomatic nocturnal enuresis (NMNE, 31.5%; Butler, Heron, & ALSPAC Team, 2006).
1.1.4 Differential Diagnoses and Comorbid Disorders
1.1.4.1 Psychological Differential Diagnoses
Many children wet during the night without any psychological disorder. If additional psychologi-cal disorders exist, they are classified separately.

Incontinence During Childhood and Adolescence 7
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
Therefore, in general, the focus is more on iden-tifying possible comorbid disorders. These should be diagnosed and treated in addition to the incon-tinence (see Section 1.1.4.2) – not on a differen-tial diagnosis per se. However, the same possible organic causes as in daytime urinary incontinence have to be ruled out (see Section 1.2.4).
1.1.4.2 Comorbid Psychological DisordersChildren with incontinence often have high psy-chological stress and reduced self-esteem. Subjec-tive distress, however, is often a consequence of incontinence and improves with successful treat-ment of incontinence (Hägglöf, Andren, Berg-ström, Marklund, & Wendelius, 1996). These sub-clinical symptoms usually do not need additional treatment.
Manifest psychological comorbid disorders, how-ever, should not be overlooked. Epidemiological studies have shown increased rates of 20–40% of psychological comorbidities in incontinent chil-dren (von Gontard, Baeyens, et al., 2011). Higher rates of up to 70% can be found in selected clin-ical populations, especially in children and ado-lescents referred to psychiatric clinics. In one clinical study, 40% of all children with nocturnal enuresis or daytime urinary incontinence had at least one further psychiatric diagnosis according to ICD-10 (von Gontard, Plück, Berner, & Lehm-kuhl, 1999). Van Hoecke and colleagues (2006) compared children with nocturnal enuresis with nonwetting children and found significantly higher values for the incontinent children concerning ex-ternalizing and internalizing behavior as measured with the Child Behavior Checklist (CBCL; Achen-bach, 1991). Furthermore, the total score of psy-chological symptoms as well as the subscale at-tention problems were increased for these children. In the ALSPAC, Joinson and colleagues (2007) examined frequencies of psychological problems in children with nocturnal enuresis, in children with combined daytime and nighttime wetting, and in continent children. There were significant differences in parental reports of psychological symptoms (such as anxiety, depressive symptoms, attention and behavioral disorders) between the three groups with a higher risk for wetting chil-dren. Moreover, children with combined wetting
had a higher risk of externalizing behavior prob-lems compared to children with nocturnal enure-sis only. In an epidemiological study of 2,079 pre-school children, associations between nocturnal enuresis and anxious and depressive symptoms could be shown (Equit, Klein, et al., 2013). Of the children with nocturnal enuresis 17.8% were af-fected by clinically relevant anxious and depres-sive symptoms compared to 12% of the continent children. No significant differences, however, were shown between children with daytime urinary in-continence and continent children.
The most common comorbid disorder of noctur-nal enuresis is the attention deficit hyperactivity disorder (ADHD). Of the children with ADHD 20.9% also wet at night (Robson, Jackson, Black-hurst, & Leung, 1997). In contrast, in an epide-miological study with 1,136 children between 8 and–11 years old, 12.5% of the children with nocturnal enuresis additionally fulfilled the cri-teria for ADHD in comparison to only 3.6% of children without nocturnal enuresis (Shreeram, He, Kalaydjian, Brothers, & Merikangas, 2009). Comparably high prevalence rates of 10% in chil-dren with ADHD combined with nocturnal en-uresis in primary care and up to 30% in tertiary care are described by Baeyens, Roeyers, D’Hase, and colleagues (2006).
In a population-based study by von Gontard, Moritz, and colleagues (2011), the association be-tween nocturnal enuresis and ADHD symptoms was analyzed. Nocturnal enuresis did not repre-sent a risk factor for ADHD symptoms if other fac-tors, such as developmental problems and psycho-social risk factors (e. g., divorce of parents), were controlled for.
Children with nocturnal enuresis and ADHD are more difficult to treat, show lower compliance, and have lower success rates in therapies that require compliance. For instance, children with ADHD more often refuse to get up at night during alarm treatment than children with nocturnal en-uresis without ADHD (Baeyens, Roeyers, Demey-ere, et al., 2005; Crimmins et al., 2003).
In a study by von Gontard, Plück, and colleagues (1999), the rate of comorbid disorders with PNE was 20%. Children who only wet at night without

Chapter 18
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
symptoms of bladder dysfunction showed a very low rate (10%) of comorbid psychological disor-ders. Children with MNE were thus not more dis-turbed than nonwetting children. In children with signs of bladder dysfunction, such as urgency, the rate of psychological disorders was increased. Similar results have been published by Zink, Fre-itag, & von Gontard (2008), who examined 166 children between 5 and 16 years of age with day-time urinary incontinence and/or nocturnal en-uresis. Overall, the rate of externalizing behavior problems was twice as high as the rate of internal-izing symptoms. Children with daytime urinary incontinence showed significantly more external-izing behavior problems as well as comorbid psy-chological disorders than children with nocturnal enuresis only. Children with MNE had the lowest comorbidity. Children, who had been dry before and have relapsed, had a much higher risk for co-morbid disorders. In one study, the rate of ICD-10 diagnoses was about 75% in children with second-ary nocturnal enuresis (von Gontard, Plück, et al., 1999). These children especially need further as-sessment and therapy in addition to the treatment of nocturnal enuresis. Furthermore, many clinical and epidemiological studies indicate that the rate of stressful life events is significantly increased in children with SNE, particularly preceding the re-lapse. Parental separation/divorce was described as an especially stressful event in the life of chil-dren (Järvelin, Moilanen, Vikeväninen-Tervonen, & Huttunen, 1990).
1.1.5 Etiology
1.1.5.1 GeneticsNocturnal enuresis can be considered a genetically determined maturation disorder of the central ner-vous system. The genetic predisposition is the same in primary and secondary enuresis. Genet-ics can be regarded as the most important etiolog-ical factor for the development of nocturnal enure-sis, which has been shown by formal as well as molecular genetic analyses (von Gontard, Scha-umburg, Hollmann, Eiberg, & Rittig, 2001). Em-pirical family studies show that 60–80% of all children with nocturnal enuresis have relatives with wetting problems. The prevalence of enure-
sis in children is 44% if one parent was affected and 77% if both parents were affected (Bakwin, 1961, 1973).
In epidemiological studies, a positive family his-tory was described as the most important etiolog-ical factor of enuresis. The attainment of dryness was delayed by 1.5 years if at least two first-de-gree relatives had wetted. Furthermore, children have a 3–4 time higher risk for relapse if they at-tain dryness after age 5 (Fergusson et al., 1986). The risk of nocturnal enuresis increases 5–7 times for 7-year-old children and 11.3 times if one par-ent or both have a history of enuresis (Järvelin, Vikevärnen-Tervonen, Moilanen, & Huttunen, 1988).
Twin studies compared concordance rates of mono- and dizygotic twins and showed significantly higher rates for monozygotic (46–68%) compared to di-zygotic twins (19–36%) (Bakwin, 1973). Segre-gation analyses showed an autosomal dominant mode of inheritance with reduced penetration of 90% in 44% of the cases. This means that only one parent with possible enuresis genes would be suf-ficient to induce enuresis in a child (dominant in-heritance; Arnell et al., 1997). Reduced penetra-tion means that if the relevant gene exists, only 90% actually develop enuresis. In contrast, in only one third of the cases enuresis develops sporadi-cally, i. e., no relatives are incontinent or have been affected by wetting. Linkage studies have identified different ‘loci’ on chromosomes 4, 8, 12, 13, and 22, on which possible genes for noc-turnal enuresis could be localized (von Gontard, Schaumburg, et al., 2001).
Thus, nocturnal enuresis is a predominantly ge-netic disorder influenced by environmental fac-tors. The environmental impact is less in PNE as genetic factors lead directly to wetting (delay in getting dry). Children with SNE have an increased genetic disposition for relapse, which is activated by environmental conditions, e. g., stressful life events or psychological disorders.
1.1.5.2 Neurobiological ResultsNeurobiological findings are comparable in PNE and SNE. Unspecific signs for involvement of the central nervous system are lower birth weight,

Incontinence During Childhood and Adolescence 9
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
lower body length, and delayed bone age. In one third of all children fine neurologic coordination disorders (soft-signs) were found that additionally emphasize the involvement of the central nervous system. Children with nocturnal enuresis show slower motor performance (von Gontard, Freitag, Seifen, Prukop, & Röhling, 2006) and exhibit a slightly higher rate of abnormalities in early acous-tic evoked potentials (Freitag, Seifen, Pukrop, & von Gontard, 2006).
In sleep studies with EEG monitoring, children with nocturnal enuresis revealed no abnormalities. Wetting is not an equivalent of dreaming, as wet-ting rarely occurs in rapid eye movement (REM) phases. Instead, wetting is independent of sleep stage and occurs in every non-REM phase (non-dreaming phase). However, the majority of wet-ting episodes occur in the first third of the night (Nevéus, Läckgren, et al., 2000).
Neurobiological factors of nocturnal enuresis are not located in the cerebral cortex, as measured by EEG, but in deeper brain structures. A full blad-der can lead to wetting during the night if the mic-turition reflex is not inhibited (Nevéus, Läckgren, et al., 2000). This function, i. e., the inhibition of the micturition reflex, is mediated by the pontine micturition center in the brainstem. Additionally, wetting occurs when sensations of the full blad-der are not registered and do not lead to arousal, which is regulated by the locus coeruleus. Both structures are anatomically close and functionally connected.
Many parents of children with nocturnal enuresis report difficulties in waking their children up, which could be demonstrated in standardized wak-ing trials. Wolfish, Pivik, & Busby (1997) showed that only 9% of enuretic children could be woken up by acoustic stimuli of up to 120 decibel.
1.1.5.3 Neuroendocrinological ResultsMany children with PNE or SNE have increased urine production (polyuria) during the night as well as a shift of the circadian day-night rhythm of the antidiuretic hormone (ADH). Due to in-creased production of urine, the capacity of the bladder can be exceeded so that wetting results if the children do not awake (Nevéus, Läckgren,
et al., 2000). The amount of urine is regulated by ADH leading to a decreased production of urine. Usually, during daytime less ADH is secreted so that more urine is produced. During the night, ADH secretion increases, whereby less and more concentrated urine is produced. For some children with nocturnal enuresis, ADH secretion is the same during night and day (i. e., leading to noc-turnal polyuria). Therefore, changes of the day-night rhythm can be associated with nocturnal en-uresis (Norgaard, Pedersen, & Djurhuus, 1985; Rittig, Knudsen, Norgaard, Pedersen, & Djurhuus, 1989). These ADH hypotheses of enuresis do not apply to all children as many wetting children do not have polyuria. Other children are dry during the night despite polyuria because they wake up and go to the toilet. Furthermore, polyuria does not explain why children do not wake up during the night or do not suppress the micturition reflex (Hunsballe et al., 1995; Mattson, 1994; Nevéus, 2011).
In summary, polyuria does indeed increase the risk of nocturnal enuresis, but it is not the main cause. Arousal difficulty or the lacking suppression of the micturition reflex are also needed to explain the pathophysiology of nocturnal enuresis. Poly-uria and variations of ADH can therefore be con-sidered additional aspects of general maturation delay of the central nervous system.
1.1.5.4 Psychosocial FactorsTwo longitudinal Swiss studies of the 1950s and 1960s showed that potty training does not have an impact on becoming dry during the night. In the 1950s, 96% of all parents began potty train-ing before their child reached the age of 1 year; in the 1970s training shifted to the median age of 19–21 months due to different child-rearing prac-tices and the availability of disposable diapers. However, these differences did not have an impact on becoming dry during the night (Bloom, Seeley, Ritchey, & McGuire, 1993; Largo, Molinari, von Siebenthal, & Wolfensberger, 1996). In a longitu-dinal study of more than 8,000 children, Joinson et al. (2009) could demonstrate that children who began potty training at the age of two took longer to get dry during the day and had more relapses in bladder control during the day compared to chil-

Chapter 110
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
dren who began potty training with 15–24 months of age. However, no differences were found be-tween these groups concerning the age of conti-nence at night.
Psychosocial risks (e. g., stressful life events, ex-isting psychiatric disorders) can trigger a relapse. Enuresis can lead to high psychological stress and decrease self-esteem. After successful therapy, subclinical psychological signs decrease. How-ever, problems in self-esteem can reinforce al-ready existent psychological disorders. Also, psy-chosocial risks and wetting can coexist without any causal relation, i. e., by chance. In a study by Sureshkumar and colleagues (2009) of 2,856 Aus-tralian children, associations were demonstrated between the existence of emotional stressors and mild nocturnal enuresis.
Children with PMNE do not exhibit a highly in-creased rate of psychological disorders or psycho-social risk factors. These results support the pre-dominantly genetic-biologic etiology of PMNE. For children with PNMNE, emotional and behav-ioral symptoms are more common compared to healthy children or children with PMNE, however, these symptoms are less common than in children with daytime urinary incontinence (Zink et al., 2008). Butler and colleagues (2006) compared children with MNE and NMNE in respect to ab-normalities in micturition, voiding frequency, etc., but also in respect to psychological variables such as social anxiety, general anxiety, unhappiness/de-pression, and ADHD. Although the rates of psy-chological disturbances were higher in the group of children with NMNE, no statistically signifi-cant differences could be shown.
The rate of stressful life events and preceding psy-chiatric disorders is increased in children with SNE and can function as a trigger for relapse. There are two main peaks for relapse: in infancy (2–3 years) and at preschool age (5–6 years). The most important life event was the separation or di-vorce of the parents (Järvelin et al., 1990). Fergus-son and colleagues (1990) demonstrated that the risk for SNE was increased in children who were exposed to four or more stressful life events in a year. In one study, 75% of children with second-ary enuresis had a comorbid psychological dis-order. Additionally, 62% of the parents reported
stressful life events, such as a separation or di-vorce, in the environment of 19% of the children (von Gontard, Plück, et al., 1999).
1.2 Daytime Urinary Incontinence
1.2.1 DefinitionandClassification
According to the recommendation of the Interna-tional Children’s Continence Society (ICCS), the term functional daytime urinary incontinence (or daytime incontinence) should be used for children who wet during the day after ruling out organic causes (Nevéus et al., 2006; Austin et al., 2014). This implies that a disorder of the bladder func-tion is present resulting in involuntary passing of urine at an inappropriate place and time. Organic (i. e., not functional) urinary incontinence can be caused, for instance, by malformation (structural) or a disorder of bladder innervation (neurogenic). The term functional implies that no organic blad-der dysfunction exists. Additionally, a duration of 3 months, a frequency of once per month, and a minimum age of 5 years is required for a diagno-sis (Austin et al., 2014).
1.2.2 Subtypes
In functional daytime urinary incontinence, three common and several rare types can be differenti-ated. First we will describe the three common types urge incontinence, voiding postponement, and dys-functional voiding:1. Urinary incontinence with urgency is described
as urge incontinence (overactive bladder). In most cases, it is due to genetic factors with an inherent dysfunction of the filling phase of the bladder. The bladder contracts spontaneously during the filling phase, which often leads to ur-gency and frequent micturitions (up to 20 times a day) with small amounts of urine. These con-tractions are not adequately inhibited by the central nervous system. The children try to sup-press the urge by using holding maneuvers (e. g., pressing legs together, sitting on the heel, etc.).
2. Urinary incontinence in voiding postponement is an acquired disorder. It is characterized by postponing micturition habitually, so that wet-

Incontinence During Childhood and Adolescence 11
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
ting during daytime occurs despite holding ma-neuvers. The most important sign for this type is infrequent micturitions (less than 5 times a day). Children postpone micturition in typical situations, e. g., at school, during play, or while watching TV. The longer the voiding postpone-ment persists, the stronger the urgency gets. These children use similar holding maneuvers as those with urge incontinence. Finally, when micturition cannot be postponed any longer, wetting occurs.
3. Dysfunctional voiding is defined by a lack of re-laxation and paradox contraction of the urethral sphincter during micturition (i. e., it is a disor-der of the emptying phase). It is an acquired co-ordinative dysfunction between detrusor and sphincter. The sphincter contracts during mic-turition instead of relaxing. The detrusor, there-fore, pushes against the activated sphincter in order to achieve emptying. Children with dys-functional voiding cannot urinate spontaneously. They need to strain to initiate micturition. As a result, the stream of urine is interrupted. When these main symptoms occur (straining, inter-rupted voiding), further assessment with uro-flowmetry and EMG is indicated, as the risk of medical complications is the highest in this type of daytime urinary incontinence (Chase, Aus-tin, Hoebeke, & McKenna, 2010).
Rare types of daytime urinary incontinence include:1. Stress incontinence is characterized by urine
leakage during an increase of intra-abdominal pressure, e. g., when coughing or sneezing. Stress incontinence is rare in childhood but typical in adult women. The amounts of urine leakage are usually small.
2. Giggle incontinence is characterized by com-plete bladder emptying while laughing. The amounts of urine are very large. This disorder is inherited.
3. Underactive bladder (formerly lazy bladder syndrome) represents a rare type of daytime uri-nary incontinence. The detrusor is decompen-sated so that the bladder cannot spontaneously be emptied completely and high volumes of re-sidual urine remain. Micturition is interrupted and abdominal pressure is needed to achieve bladder emptying.
4. Vaginal reflux is a rare subtype in girls.
1.2.3 Prevalence
The prevalence rates of different subtypes of day-time urinary incontinence have not been studied in detail. The gender ratio is relatively balanced (1.5:1 for girls to boys). Sixteen percent to 47% of 3-year-old children and 2–12% of 4-year-old children wet during daytime, i. e., before the defi-nitional age of the disorder. With increasing age, 25% of 5-year-olds, 2.9% of 6-year-olds, 3.6% of 7-year-olds, 4.0% of 8-year-olds, 3.0% of 10-year-old children, and less than 1% of adolescents are affected. The rate of daytime urinary incontinence increases in late adulthood, 12–18% of the 25– 64-year-olds wet and 9–23% of the over 65-year-olds (von Gontard & Nevéus, 2006).
One epidemiological study showed a prevalence rate of 7.7% of daytime urinary incontinence in 7.5-year-old children (Joinson, Heron, von Gon-tard & the ALSPAC team, 2006). In the same AL-SPAC with 10,819 children, the prevalence rate of daytime urinary incontinence for the age of 4.5 years was about 15.5% and decreased to 4.9% at the age of 9.5 years (Swithinbank, Heron, von Gontard, & Abrams, 2010). In the same ALSPAC, Heron and colleagues (2008) identified four tra-jectories of daytime wetting. Of all children 86% attained bladder control during daytime already at the age of 4.5 years and did not wet in later years. In 6.9% of the children, the attainment of bladder control during daytime was delayed. They still wetted at the age of 4.5 years. Wetting, however, decreased successively and disappeared at the age of 9.5 years. Daytime wetting persisted in 3.7% until the age of 9.5 years. Finally, 3.2% of the children experienced a relapse at the age of 6.5 years after a period of continence. Both of the latter trajectories are clinically relevant (i. e., the continuous wetters and the relapsers) – these chil-dren need special therapeutic attention. Suresh-kumar and colleagues (2000) reported prevalence rates of 16.9% of daytime urinary incontinence in 7.3-year-old Australian children. According an epidemiological study of one of the authors and colleagues, 4.4% of 6-year-old preschoolers wet during daytime (von Gontard, Moritz, et al., 2011).
There are hardly any prevalence rates available for the subtypes of daytime urinary incontinence. Urge

Chapter 112
This document is for personal use only. Reproduction or distribution is not permitted.From M. Equit et al.: Urinary and Fecal Incontinence: A Training Program for Children and Adolescents (ISBN 9781616764609) © 2015 Hogrefe Publishing.
incontinence occurs most often in girls. Voiding postponement is as common as urge incontinence, and in clinical studies more boys than girls are affected. Based on ALSPAC data, von Gontard, Heron, & Joinson (2009) analyzed the associa-tions of daytime wetting and voiding frequency. The children’s median of age was 77 months. Of the 8,475 examined children, 10.4% still wetted during daytime. Of these children 35.7% went to the toilet less than 5 times per day (voiding post-ponement), 61.5% had 5–9 micturitions a day, and 2.8% went to the toilet 10 times or more per day (urgency). Prevalence rates for dysfunctional void-ing range from 4.2–31% in clinical samples, how-ever, no population-based dates exist (Hjälmås, 1995; Hoang-Böhm, Jüneman, Köhrmann, Zend-ler, & Alken, 1999; Hoebeke, van Laecke, van Camp, Raes, & Vande Walle, 2001).
1.2.4 Differential Diagnoses and Comorbid Disorders
Children with daytime urinary incontinence have higher rates of somatic disorders than children with nocturnal enuresis only. Therefore, the as-sessment and treatment of the underlying organic disorder is necessary. It is especially important to avoid lasting kidney damage from recurring infec-tions of the lower urinary tract.
The following causes of urinary incontinence can be differentiated:• structural (i. e., malformation and abnormalities
of the urinary tract);• neurogenic (i. e., dysfunction of the innervation
of the bladder); and• other physical diseases (i. e., diseases which re-
sult in an increased urine production, such as diabetes insipidus or mellitus, or urinary tract infections).
In structural urinary incontinence malformations of the urinary tract exist, which require urological or surgical assessment. Malformations include those of the kidneys (renal agenesis: the complete missing of a kidney; double kidneys, renal pelvis distension) or malformations of the ureter (e. g., megaureter – enlarged ureter).
Vesicoureteral reflux (VUR, urine flowing back from the bladder through the ureter up to the kid-neys) is a common differential diagnosis which can also be caused by increased bladder pressure (as in voiding postponement or dysfunctional void-ing). In severe types of VUR, the renal pelvis is in-volved. In mild types, urinary tract infections can occur. VUR must always be assessed radiograph-ically and should be referred to pediatric urologists or nephrologists. Mild types are treated conserva-tively with an antibiotic prophylaxis (long-term an-tibiotics), severe types often require surgery.
The urethra can be affected by malformations such as posterior urethral valves, but a stenosis of the urethra has to be considered as well. Furthermore, abnormal outlets of the urethra have to be excluded in boys (hypospadias, epispadias).
In neurogenic urinary incontinence the innerva-tion of the bladder is disturbed (e. g., in spina bi-fida occulta). Individuals with spina bifida, a mal-formation of the vertebral arches, can show neural deficits of the lower extremities as well as of the bladder.
Other rare neurogenic causes of incontinence are the tethered cord syndrome and tumors of the spi-nal cord. Therefore, the spine, asymmetries of the buttocks and lower extremities, reflex differences, and sensitivity deficits of the lower extremities should always be examined thoroughly. Urinary incontinence can rarely be due to other underlying diseases, such as diabetes mellitus or diabetes in-sipidus (lack of ADH). Another neurologic condi-tion that can cause incontinence is sacral agenesis.
1.2.5 Comorbid Psychological Disorders
Children with daytime urinary incontinence have an increased rate of comorbid psychological dis-orders (von Gontard, Baeyens, et al., 2011). Join-sen, Heron, von Gontard, & ALSPAC team (2006) found increased rates for ADHD (24.8%), oppo-sitional behavior (10.9%), and conduct problems (11.8%). In an epidemiological study of 1,391 pre-school children, von Gontard, Moritz, and col-leagues (2011) found a specific association of day-time wetting and ADHD. However, the risk for


















