Molecular Diagnostic Algorithms in Hepatocellular Carcinoma: Dead-End Street or Light at the End of...
5
knowledge of CRC in IBD. First, they demonstrated how patients with LEC significantly drive CRC risk in an IBD population despite being a small proportion of the pop- ulation. They highlighted the importance of chronic colonic inflammation as the key biologic risk factor for CRC in IBD, because both UC and CD patients with >10 years of disease and >50% of the colon involved had a similar and elevated risks of CRC. They demonstrated that an impor- tant proportion of HGD/cancers will have occurred at the time screening begins, highlighting limitations of current guidelines. Finally, they reported a reduction in CRC risk associated with thiopurine use. We look forward to addi- tional studies to provide a better understanding of this latter observation, because there are insufficient data at this time to reliably explain the mechanism for the observed reduction in risk. Until then, we propose current guidelines from the American Gastroenterological Association should not change (remain grade insufficient) on the potential chemopreventive effect of thiopurines on IBD-associated CRC. FERNANDO S. VELAYOS Division of Gastroenterology and Hepatology, University of California, San Francisco, San Francisco, California THOMAS A. ULLMAN The Dr Henry D. Janowitz Division of Gastroenterology, The Mount Sinai Medical Center, New York, New York References 1. Rutter M, Saunders B, Wilkinson K, et al. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroen- terology 2004;126:451–459. 2. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation is a risk factor for progression to colorectal neoplasia in ulcerative colitis: a cohort study. Gastroenterology 2007;133: 1099–1105. 3. Soderlund S, Brandt L, Lapidus A, et al. Decreasing time-trends of colorectal cancer in a large cohort of patients with inflammatory bowel disease. Gastroenterology 2009;136:1561–1567. 4. Jess T, Simonsen J, Jorgensen KT, et al. Decreasing risk of colorectal cancer in patients with inflammatory bowel disease over 30 years. Gastroenterology 2012;143:375–381. 5. Ekbom A, Helmick C, Zack M, et al. Ulcerative colitis and colorec- tal cancer. A population-based study. N Engl J Med 1990; 323:1228–1233. 6. Farraye FA, Odze RD, Eaden J, et al. AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology 2010;138:738–745. 7. Pinczowski D, Ekbom A, Baron J, et al. Risk factors for colorectal cancer in patients with ulcerative colitis: a case-control study. Gastroenterology 1994;107:117–120. 8. Velayos FS, Terdiman JP, Walsh JM. Effect of 5-aminosalicylate use on colorectal cancer and dysplasia risk: a systematic review and metaanalysis of observational studies. Am J Gastroenterol 2005; 100:1345–1353. 9. Beaugerie L, Brousse N, Bouvier AM, et al. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: a prospective observational cohort study. Lancet 2009; 374:1617– 1625. 10. Beaugerie L, Svrcek M, Seksik P, et al. Risk of colorectal high- grade dysplasia and cancer in a prospective observational cohort of patients with inflammatory bowel disease. Gastroenter- ology 2013;145:166–175. 11. Matula S, Croog V, Itzkowitz S, et al. Chemoprevention of colorectal neoplasia in ulcerative colitis: the effect of 6-mercaptopurine. Clin Gastroenterol Hepatol 2005;3:1015–1021. 12. Velayos FS, Loftus EV Jr, Jess T, et al. Predictive and protective factors associated with colorectal cancer in ulcerative colitis: a case- control study. Gastroenterology 2006;130:1941–1949. 13. Farraye FA, Odze RD, Eaden J, et al. AGA technical review on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology 2010;138:746–774. 14. Winther KV, Jess T, Langholz E, et al. Long-term risk of cancer in ulcerative colitis: a population-based cohort study from Copenhagen County. Clin Gastroenterol Hepatol 2004;2:1088–1095. 15. Jess T, Loftus EV Jr, Velayos FS, et al. Risk of intestinal cancer in inflammatory bowel disease: a population-based study from Olmsted County, Minnesota. Gastroenterology 2006;130:1039–1046. Reprint requests Address requests for reprints to: Fernando S. Velayos, MD, University of California, San Francisco, Division of Gastroenterology, Department of Medicine, 2330 Post Street, Suite 610, San Francisco, California 94115. e-mail: [email protected]; fax: 415-502-2249. Conflicts of interest The authors disclose no conflicts. © 2013 by the AGA Institute 0016-5085/$36.00 http://dx.doi.org/10.1053/j.gastro.2013.05.023 Molecular Diagnostic Algorithms in Hepatocellular Carcinoma: Dead-End Street or Light at the End of the Tunnel? See “A hepatocellular carcinoma 5-gene score associated with survival of patients after liver resection,” by Nault JC, de Reyniès A, Villanueva A, et al, on page 176. H epatocellular carcinoma (HCC) is one of the most frequent and deadliest cancers worldwide. 1,2 Despite its enormous clinical relevance, therapeutic options have remained limited. 3–5 No curative, systemic treatment exists to date and only limited lifespan extension can be reached by established palliative therapy, despite increased treatment options over the last years (eg, local ablative technologies, transarterial chemoembolization [TACE], sorafenib, endoradiotherapy). 3–10 Curative approaches mainly reside on surgery, that is, partial liver resection or transplantation (LTX). 3–8 Unfortunately, in Western countries only a minority of HCC patients is eligible for Editorials, continued 49
Transcript of Molecular Diagnostic Algorithms in Hepatocellular Carcinoma: Dead-End Street or Light at the End of...
Editorials, continued
knowledge of CRC in IBD. First, they demonstrated howpatients with LEC significantly drive CRC risk in an IBDpopulation despite being a small proportion of the pop-ulation. They highlighted the importance of chroniccolonic inflammation as the key biologic risk factor for CRCin IBD, because both UC and CDpatients with>10 years ofdisease and >50% of the colon involved had a similar andelevated risks of CRC. They demonstrated that an impor-tant proportion of HGD/cancers will have occurred at thetime screening begins, highlighting limitations of currentguidelines. Finally, they reported a reduction in CRC riskassociated with thiopurine use. We look forward to addi-tional studies to provide a better understanding of thislatter observation, because there are insufficient data at thistime to reliably explain the mechanism for the observedreduction in risk. Until then, we propose current guidelinesfrom the American Gastroenterological Association shouldnot change (remain grade insufficient) on the potentialchemopreventive effect of thiopurines on IBD-associatedCRC.
FERNANDO S. VELAYOSDivision of Gastroenterology and Hepatology, Universityof California, San Francisco, San Francisco, California
THOMAS A. ULLMANThe Dr Henry D. Janowitz Division of Gastroenterology,The Mount Sinai Medical Center, New York, New York
References
1. Rutter M, Saunders B, Wilkinson K, et al. Severity of inflammation isa risk factor for colorectal neoplasia in ulcerative colitis. Gastroen-terology 2004;126:451–459.
2. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammationis a risk factor for progression to colorectal neoplasia inulcerative colitis: a cohort study. Gastroenterology 2007;133:1099–1105.
3. Soderlund S, Brandt L, Lapidus A, et al. Decreasing time-trends ofcolorectal cancer in a large cohort of patients with inflammatorybowel disease. Gastroenterology 2009;136:1561–1567.
4. Jess T, Simonsen J, Jorgensen KT, et al. Decreasing risk of colorectalcancer in patients with inflammatory bowel disease over 30 years.Gastroenterology 2012;143:375–381.
5. Ekbom A, Helmick C, Zack M, et al. Ulcerative colitis and colorec-tal cancer. A population-based study. N Engl J Med 1990;323:1228–1233.
6. Farraye FA, Odze RD, Eaden J, et al. AGA medical position statementon the diagnosis and management of colorectal neoplasiain inflammatory bowel disease. Gastroenterology 2010;138:738–745.
7. Pinczowski D, Ekbom A, Baron J, et al. Risk factors for colorectalcancer in patients with ulcerative colitis: a case-control study.Gastroenterology 1994;107:117–120.
8. Velayos FS, Terdiman JP, Walsh JM. Effect of 5-aminosalicylate useon colorectal cancer and dysplasia risk: a systematic review andmetaanalysis of observational studies. Am J Gastroenterol 2005;100:1345–1353.
9. Beaugerie L, Brousse N, Bouvier AM, et al. Lymphoproliferativedisorders in patients receiving thiopurines for inflammatory boweldisease: a prospective observational cohort study. Lancet 2009;374:1617–1625.
10. Beaugerie L, Svrcek M, Seksik P, et al. Risk of colorectal high-grade dysplasia and cancer in a prospective observationalcohort of patients with inflammatory bowel disease. Gastroenter-ology 2013;145:166–175.
11. Matula S, Croog V, Itzkowitz S, et al. Chemoprevention of colorectalneoplasia in ulcerative colitis: the effect of 6-mercaptopurine. ClinGastroenterol Hepatol 2005;3:1015–1021.
12. Velayos FS, Loftus EV Jr, Jess T, et al. Predictive and protectivefactors associated with colorectal cancer in ulcerative colitis: a case-control study. Gastroenterology 2006;130:1941–1949.
13. Farraye FA, Odze RD, Eaden J, et al. AGA technical review on thediagnosis and management of colorectal neoplasia in inflammatorybowel disease. Gastroenterology 2010;138:746–774.
14. Winther KV, Jess T, Langholz E, et al. Long-term risk of cancerin ulcerative colitis: a population-based cohort study fromCopenhagen County. Clin Gastroenterol Hepatol 2004;2:1088–1095.
15. Jess T, Loftus EV Jr, Velayos FS, et al. Risk of intestinalcancer in inflammatory bowel disease: a population-based study fromOlmsted County, Minnesota. Gastroenterology 2006;130:1039–1046.
Reprint requestsAddress requests for reprints to: Fernando S. Velayos, MD, University
of California, San Francisco, Division of Gastroenterology, Department ofMedicine, 2330 Post Street, Suite 610, San Francisco, California 94115.e-mail: [email protected]; fax: 415-502-2249.
Conflicts of interestThe authors disclose no conflicts.
© 2013 by the AGA Institute0016-5085/$36.00
http://dx.doi.org/10.1053/j.gastro.2013.05.023
Molecular Diagnostic Algorithms in Hepatocellular Carcinoma: Dead-EndStreet or Light at the End of the Tunnel?
See “A hepatocellular carcinoma 5-gene scoreassociated with survival of patients after liverresection,” by Nault JC, de Reyniès A, VillanuevaA, et al, on page 176.
epatocellular carcinoma (HCC) is one of the most1,2
Hfrequent and deadliest cancers worldwide. Despiteits enormous clinical relevance, therapeutic options have
remained limited.3–5 No curative, systemic treatmentexists to date and only limited lifespan extension can bereached by established palliative therapy, despite increasedtreatment options over the last years (eg, local ablativetechnologies, transarterial chemoembolization [TACE],sorafenib, endoradiotherapy).3–10 Curative approachesmainly reside on surgery, that is, partial liver resection ortransplantation (LTX).3–8 Unfortunately, in Westerncountries only a minority of HCC patients is eligible for
49

Editorials, continued
curative treatment owing to late diagnosis and the factthat about 80% of these HCC patients have confoundingsevere fibrosis or cirrhosis, with advanced cirrhosis beinga contraindication for partial liver resection. Furthermore,organ donor shortage, abstinence from cadaveric LTX,and extensive effort and costs are significant limitationsfor LTX as a numerically relevant HCC treatment.6,7
In terms of surgical treatment strategy of HCC, someprogress has been achieved in recent years. For example,neoadjuvant treatment (bridging TACE) is meanwhileapplied to most HCC patients on the waiting list for LTX.Sequential approaches (resection and subsequent LTX incase of recurrence) are performed by some centers. In somecases, LTX or resection have been performed after down-staging by TACE.7 Currently, clinical trials are assessingthe potential of sorafenib in adjuvant and neoadjuvanttreatment.8 Although these approaches are lagging behindthe significant progress in many other cancers (eg, breastand colorectal cancer), they indicate that multimodalstrategies have entered the field of curative HCC treat-ment. Are we up to it? How are we going to identifypatients who may benefit?
To further improve curative strategies in HCC, validprognostic and predictive diagnostic algorithms arerequired. Unfortunately, the latter are lacking for HCCowing to the limited clinical need of prognostic andpredictive algorithms until now, because currently thechoice of therapeutic options does not depend on prog-nostic subtyping of HCC. As a consequence, in the absen-ce of differential therapeutic approaches, there is noprediction, and without predictive impact, prognosticinformation hardly matters. A second, important aspect isthe presence of multiple confounding factors: Accompa-nying liver morbidity limits therapeutic options butalso affects survival after resection; in patients witholigonodular tumors (especially in chronic hepatitis B), itis frequently impossible to distinguish intrahepaticmetastases from independent tumorigenic processes.8,9
Furthermore, in case of LTX, prognosis mostly dependson transplantation- rather than tumor-related factors.6,7
However, the problem lies even deeper: Three basicdiagnostic principles are pivotal for the development ofsubsequent prognostic and predictive algorithms and poseproblems in HCC. First, exact tumor typing is based onmorphology in all relevant cancers, but HCC represents theonly important exception, in which typing evenbefore specific treatment can be performed solely byimaging.11 Therefore, a significant percentage of mistyping(eg, intrahepatic cholangiocarcinomas and mixed HCC-cholangiocarcinomas) may occur and novel subtypingapproaches are hard to implement. Second, tumor stagingin HCC is done by imaging and on resection and explantspecimens by pathomorphologic evaluation, and there issufficient evidence demonstrating relevant mis-stagingsolely by imaging. Third, assessment of tumor
50
aggressiveness is conventionally performed by morpho-logic grading, which in most cases represents an indepen-dent prognostic parameter. In HCC, the power of gradingis limited by the lack of an internationally accepted anduniformly implemented grading scheme. Mostly, thehistorical and time-honored Edmondson-Steiner gradingsystem12 is applied, but data supporting its independentprognostic impact are relatively weak. Thus, newapproaches and methodologies are needed to developindependent prognostic and predictive tools that mayfinally assist the clinical decision-making process. In thisregard, a lot of hope is concentrated on the field ofmolecular markers/algorithms derived from recentsequencing and profiling approaches. Promising exampleshave been described in other tumor types, such as expres-sion based algorithms for neoadjuvant treatment of breastcancer, which have been commercialized and have enteredroutine diagnostics successfully.13 In recent years,numerous molecular classifiers have been publishedfor HCC, but several shortcomings have prohibited theirtranslation into application, such as lack of reproducibility,independent confirmation, or applicability for the wholespectrum of HCCs, improper definition of parameters, ortechnical impossibility of transferring the assays into real-world diagnostics. Because the cited breast cancer algo-rithms are inevitably based on sophisticated morphologicand clinical assessment, which is complemented but notreplaced by them, successful algorithms for moleculartyping in HCC should follow the same path. Thus, theyrequire meticulous validation of the underlying collectivesand detailed comparison and combination with existing(morphologic) parameters, no matter how imperfect theymay be. Reciprocally, new molecular algorithms may teachus a new look at existing morphologic classifiers and theway to improve them. The path to success is combinationand co-evolution and not replacement.
The outlined aspects have to be respected when devel-oping rational prognostic/predictive algorithms in HCCand certainly make the job much harder compared withother tumor types when it comes to the composition ofrelevant collectives, planning of clinical trials, and trans-lation into diagnostic reality. But what can we do?Should we surrender to depression? Certainly not. And thefirst step would be to determine independent classicaland molecular prognostic parameters (and combinationsthereof) that distinguish highly from less aggressive HCCsin the setting of surgical treatment and explore themwhether they represent meaningful discriminators for newtherapeutic questions.
This issue has been tackled by the paper of Nault et al.14
In this elegant study, the authors aimed at identifyinga robust molecular signature able to accurately predict theclinical outcome of HCC patients who underwent curativesurgical resection.14 For this purpose, a large collection ofhuman HCC samples from patients undergoing curative

Editorials, continued
resection (training cohort) was analyzed by microarrayprofiling. A panel of 5 genes (including TAF9, RAMP3,HN1, KRT19, and RAN) showed the strongest prognosticrelevance and was selected for further analysis.14 Inparticular, the authors constructed a 5-genes score usingthe coefficient and regression formula of the multivariateCox model from the training cohort. The 5-genes score wasfurther validated in an independent, large cohort. Of note,the 5-genes score was associated with disease-specificsurvival both in the training and in the validationcohort, and was found to be significantly more accuratein predicting the patients’ prognosis when comparedwith known gene expression signatures.14 Indeed, itshowed its superiority to predict the patients’ prognosiswhen compared with the published G3,15 the prolifera-tive,16 the metastasis,17 and the hypoxia signatures,18
which were all shown to be good predictors of HCCpatients’ prognosis.15–18 Also, the 5-genes score accuratelypredicted overall survival and was associated with earlytumor recurrence both in the training and the validationcohort and precisely predicted the risk of death after tumorrelapse.14 Furthermore, it was associated with disease-specific survival independent of clinical and pathologicfeatures and was able to determine the prognosis of HCCpatients when associated with the 2 most relevant clinicaland pathologic variables, the Barcelona Clinic Liver Cancerclassification system and tumorous microvascular inva-sion.14 The prognostic performance of the 5-genes signa-ture covered different HCC etiologies as it was furthervalidated in an independent collective of European and USpatients with hepatitis C, cirrhosis, and HCC, and Asianpatients with HCC in chronic hepatitis B. Finally, the 5-gene score further increased its prognostic accuracy whencombined with the expression pattern from the adjacentnon-tumor tissue that was previously reported to correlatewith patient survival.19
The work by Nault et al14 has potential for imple-mentation into clinical management of HCC in manyaspects. Their 5-genes score may be broadly applicable inthe clinical setting because its validation in large cohortsof HCC patients characterized by different risk factors/etiologies seems to limit possible geographical and lifestyleinfluences. In general, differential decisions for LTX versuspartial resection or no surgical treatment at all and neo-adjuvant (eg, TACE? Chemotherapy? Sorafenib?) andadjuvant protocols linked to resection seem to be poten-tial applications.
In particular, owing to its high predictive accuracy, thescore may be able to stratify the risk of relapse and tumor-related death before a decision of liver resection is made.In difficult “borderline” cases, the molecular score mayidentify patients carrying tumors with good molecularprognostic parameters that may still benefit from resec-tion and HCC patients with poor prognostic parametersfor whom resection is unlikely to improve the outcome.
Also, in terms of LTX, the 5-genes score could be testedfor extending the Milan criteria for tumors >5 cm, oridentify tumors with poor prognostic molecular parame-ters that should be excluded from LTX or submitted tomore aggressive neo-adjuvant approaches. Furthermore,the 5 genes identified belong to different signaling path-ways, whose inhibition might likely reduce the risk ofearly tumor recurrence after surgery and survival afterrecurrence.
Although the data are solid and the 5-genes score maylead to a useful, robust predictive tool, there are someobvious actions to be taken. To gain international accep-tance, independent validation of this prognostic algo-rithm by a different group with a qualified collectivewould be helpful for international acceptance and pavingthe way into guidelines.
As outlined, prognosis assessment is a valuable first step,but per se is of little clinical help, if it has no impact ontherapeutic decision making. Because there is no validatedtherapeutic alternative for the group of HCCs with betteror worse prognosis, there is no chance of directly claimingclinical impact. Therefore, it is mandatory to decide onroutine or trial-based questions that may benefit from thisalgorithm and prospectively demonstrate the value indifferential therapeutic decision making. The proposedalgorithm has a realistic chance to survive at least some ofthese tests, but then the true work will start. In the battlefor clinically relevant tumor biomarkers, the graveyards arehuge and full of strong and highly cited candidates,whereas the group of survivors is very small and manypromising candidates have been killed quite late. Why?
� None of these treatment options is currently part ofguideline based processes in HCC. The implementa-tion depends on trials, which raises several issues suchas integration into trial protocols, financing, testingmode, and so on.
� Bias and applicability: The current algorithm has beendeveloped on the basis of resection specimens, whichamong the spectrum of HCCs are biased towardbetter/earlier stages of HCC. This is well addressed bythe authors,14 but in the long run, stage-independentprognostic markers are highly preferable; therefore,testing this algorithm for its prognostic impact inhigher (inoperable/progressed) stages of HCCs seemsto be mandatory. Also, other questions such asrecurrence risk after LTX or prognostic relevance innon-surgically treated patients may be addressed.
� Technology adaptation: Expression profiling is ahelpful exploratory technology, but it is diffi-cult—although not impossible—to transfer it intoclinical diagnostic practice. This has been in factachieved with extensive effort and in the frame ofpredictive testing in mammary carcinoma.13
51

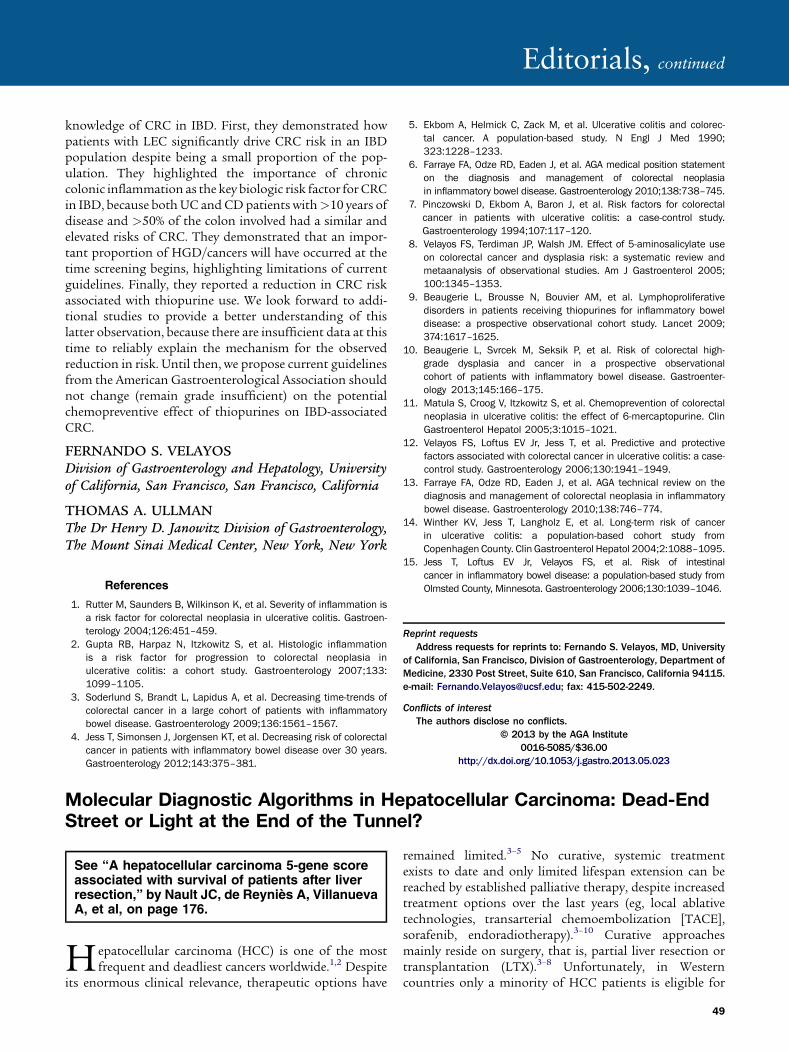
Figure 1. Challenges and fatesof predictive and prognostictissue markers.
Editorials, continued
� Furthermore, to exactly define a discriminative algo-rithm based on 5 independently regulated parametersis methodically highly demanding and more difficultand vulnerable compared with single marker assays.The final diagnostic test has to be as robust aspossible or to be transferred to more robust tech-nologies (fluorescence in situ hybridization, immu-nohistochemistry). It makes a lot of sense to work onfurther simplification/robustness even if it may be atsome expense of the diagnostic power.
� Transfer the technology for application in clinicalmaterial: For the foreseeable future, the relevantclinical material will remain to be small biopsymaterial (because decisions have to be madebefore operation) or other formalin-fixed, paraffin-embedded specimens (because the type of clinicalmaterial for the foreseeable future). It has to beproven that the algorithm and a derived testingprocedure properly function on these materials andthat analytical results are representative.
� Broad implementation: Assays have little chance tobecome accepted in clinical routine if they can beperformed only in a few, highly specialized centersindependent of refunding strategies. Long-lastingsuccess is only achieved if the test can adapted tothe routine diagnostic constellation.
In the end, daily clinical practice will decide on the fateof diagnostic algorithms and changes of treatment
52
strategies may influence their usefulness (Figure 1). So it isa long and winding road ahead, but we may have wit-nessed the first step.
PETER SCHIRMACHERPathologisches Institut, Universität Heidelberg,Heidelberg, Germany
DIEGO F. CALVISIInstitut für Pathologie, Universitätsmedizin Greifswald,Greifswald, Germany
References
1. El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011;365:1118–1127.
2. McGlynn KA, London WT. The global epidemiology of hepatocellularcarcinoma: present and future. Clin Liver Dis 2011;15:223–243.
3. Bruix J, Sherman M. Management of hepatocellular carcinoma: anupdate. Hepatology 2011;53:1020–1022.
4. de Lope CR, Tremosini S, Forner A, et al. Management of HCC.J Hepatol 2012;56(Suppl 1):S75–S87.
5. Mazzaferro V, Chun YS, Poon RT, et al. Liver transplantation forhepatocellular carcinoma. Ann Surg Oncol 2008;15:1001–1007.
6. Melloul E, Lesurtel M, Carr BI, et al. Developments in liver trans-plantation for hepatocellular carcinoma. Semin Oncol 2012;39:510–521.
7. Padhya KT, Marrero JA, Singal AG. Recent advances in the treatmentof hepatocellular carcinoma. Curr Opin Gastroenterol 2013;29:285–292.
8. Maluccio M, Covey A. Recent progress in understanding, diagnosing,and treating hepatocellular carcinoma. CA Cancer J Clin 2012;62:394–399.

Editorials, continued
9. Llovet JM, Bruix J. Molecular targeted therapies in hepatocellularcarcinoma. Hepatology 2008;48:1312–1327.
10. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advancedhepatocellular carcinoma. N Engl J Med 2008;359:378–390.
11. Kudo M. Diagnostic imaging of hepatocellular carcinoma: recentprogress. Oncology 2011;81(Suppl 1):73–85.
12. Edmondson HA, Steiner PE. Primary carcinoma of the liver:a study of 100 cases among 48,900 necropsies. Cancer 1954;7:462–503.
13. Arpino G, Generali D, Sapino A, et al. Gene expression profiling inbreast cancer: a clinical perspective. Breast 2013;22:109–120.
14. Nault JC, de Reyniès A, Villanueva A, et al. A hepatocellular carci-noma 5-gene score associated with survival of patients after liverresection. Gastroenterology 2013;145:176–187.
15. Boyault S, Rickman DS, de Reyniès A, et al. Transcriptome classifi-cation of HCC is related to gene alterations and to new therapeutictargets. Hepatology 2007;45:42–52.
16. Lee JS, Chu IS, Heo J, et al. Classification and prediction of survivalin hepatocellular carcinoma by gene expression profiling. Hepatology2004;40:667–676.
17. Roessler S, Jia HL, Budhu A, et al. A unique metastasis genesignature enables prediction of tumor relapse in early-stage hepa-tocellular carcinoma patients. Cancer Res 2010;70:10202–10212.
18. van Malenstein H, Gevaert O, Libbrecht L, et al. A seven-gene setassociated with chronic hypoxia of prognostic importance in hepa-tocellular carcinoma. Clin Cancer Res 2010;16:4278–4288.
19. Hoshida Y, Villanueva A, Kobayashi M, et al. Gene expression in fixedtissues and outcome in hepatocellular carcinoma. N Engl J Med2008;359:1995–2004.
Reprint requestsAddress requests for reprints to: Peter Schirmacher, MD,
Pathologisches Institut, Universität Heidelberg, Im Neuenheimer Feld224, 69120 Heidelberg, Germany. e-mail: [email protected]; fax: þ49 0622156-5251; or Diego Calvisi, MD, Institut fürPathologie, Universitätsmedizin Greifswald, Friedrich-Löffler-Strasse23e, 17489 Greifswald, Germany. e-mail: [email protected]; fax: þ49 3834865704.
Conflicts of interestThe authors disclose no conflicts.
© 2013 by the AGA Institute0016-5085/$36.00
http://dx.doi.org/10.1053/j.gastro.2013.05.026
Primary Liver Carcinomas Can Originate From Different Cell Types: A NewLevel of Complexity in Hepatocarcinogenesis
See “Modeling pathogenesis of primary livercancer in lineage-specific mouse cell types,” byHolczbauer Á, Factor VM, Andersen JB, et al, onpage 221.
rimary liver carcinomas (PLC) in adults comprise
Phepatocellular carcinoma (HCC) and cholangio-carcinoma (CCA), 2 morphologically, genomically, andclinically very heterogeneous tumors with dismal clinicaloutcomes.1 For a long time, it has been the prevailing viewthat hepatocytes represent the target cell for oncogenictransformation in HCC and cholangiocytes in CCA.However, work over the past decade has suggested that, inaddition to hepatocytes and cholangiocytes, PLC may bederived from adult liver stem/progenitor cells.2Liver progenitor cells (HPC) are bipotent; they expressboth hepatocellular and cholangiocyte markers and candifferentiate into mature hepatocytes and cholangiocytes.3
First evidence that human HCC could be derived fromHPC was provided by the team of Snorri Thorgeirsson in2006.4 They showed that human HCCs can be separatedaccording to their gene expression profiles into tumors witha hepatocyte-like and fetal hepatoblast (HB)/HPC signature.The team of Scott Lowe5 by using a new generation of HCCmosaic mouse models, provided functional evidence in thesame year that oncogenic transformation of bipotential HPCcould give rise to liver carcinomas that reflect many featuresof human HCC. More recently, gene expression profilingstrongly supported that several subtypes of human HCCcould be derived from malignantly transformed liver stem/
progenitor cells,6,7 and that in human PLC there isa continuum between intrahepatic CCA, mixed tumors withphenotypes of HCC and CCA, and pure HCC with orwithout progenitor features.1,8 Collectively, these datastrongly support that PLC can derive from liver stem/progenitor cells. However, an unanswered question is towhat extent dedifferentiation of malignantly transformeddifferentiated liver cells (hepatocytes and cholangiocytes)may contribute to the observed stem/progenitor cellexpression signatures in PLC. For example, recent data byFan et al9 suggest that a simultaneous activation of NOTCHand AKT signaling may drive hepatocytes into a chol-angiocellular differentiation and trigger the growth of CCA.
In this issue of GASTROENTEROLOGY, Holczbaueret al10 describe a systematic, side-by-side comparison of livertumorigenesis after controlled oncogenic transformation ofadult hepatocytes (AH), HB, and HPC. The respective celltypes were isolated at high purity and subjected to lentiviraltransduction with vectors encoding oncogenic H-ras andSV40LT. The authors thoroughly analyzed cancer stem cellproperties (CD133 expression, sphere formation andgrowth) and characterized the tumorigenic potential of all3 H-ras/SV40 transduced lineages, showing that the cancerstem cell properties and tumorigenesis were higher in HPC-than in HB- and AH-derived tumors. Interestingly, all 3lineages gave rise to tumors with varying HCC and CCAcontent. However, AH-derived tumors showed mostly HCC,HB-derived tumors mostly CCA, and HPC-derived tumorsmostly anaplastic histopathology, suggesting that tumorcells may have undergone epithelial to mesenchymal tran-sition (Figure 1).
53