Molecular and clinical diversity in systemic mastocytosis · Hematology and Oncology ... blastic...
35
Juliana Schwaab Hematology and Oncology University Hospital Mannheim Heidelberg University Germany Molecular and clinical diversity in systemic mastocytosis
Transcript of Molecular and clinical diversity in systemic mastocytosis · Hematology and Oncology ... blastic...

Juliana Schwaab Hematology and Oncology
University Hospital Mannheim Heidelberg University
Germany
Molecular and clinical diversity in systemic
mastocytosis
MDS MDS
CML
aCML
MDS/MPN
PMF
ET
PV
PDGFRA
CEL-NOS
CNL
Systemic Mastocytosis
Blastic plasmacytoid dendritic cell
neoplasm
AML
PDGFRB
MPN-u FGFR1
MDS/ MPN-u
CMML
MPN
Myeloid neoplasms
MLN-eo
MPN-u FGFR1
MDS/MPN -RS-T
JMML
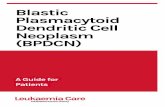
WHO classification 2016: myeloid neoplasms
FGFR1 PCM1-JAK2
B/T-lympho- blastic leukemia
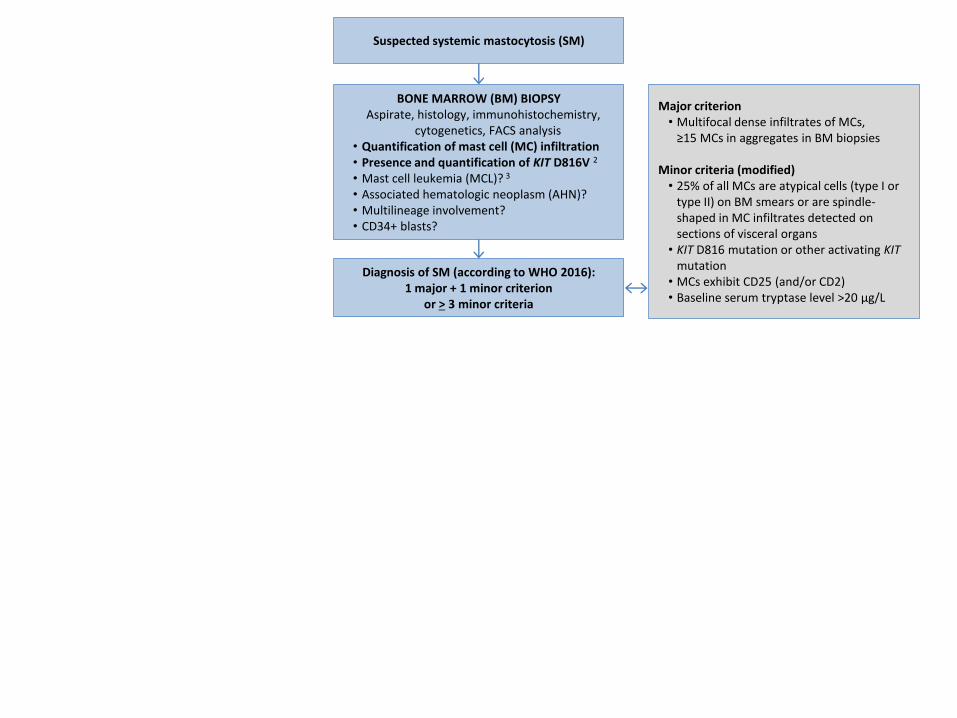
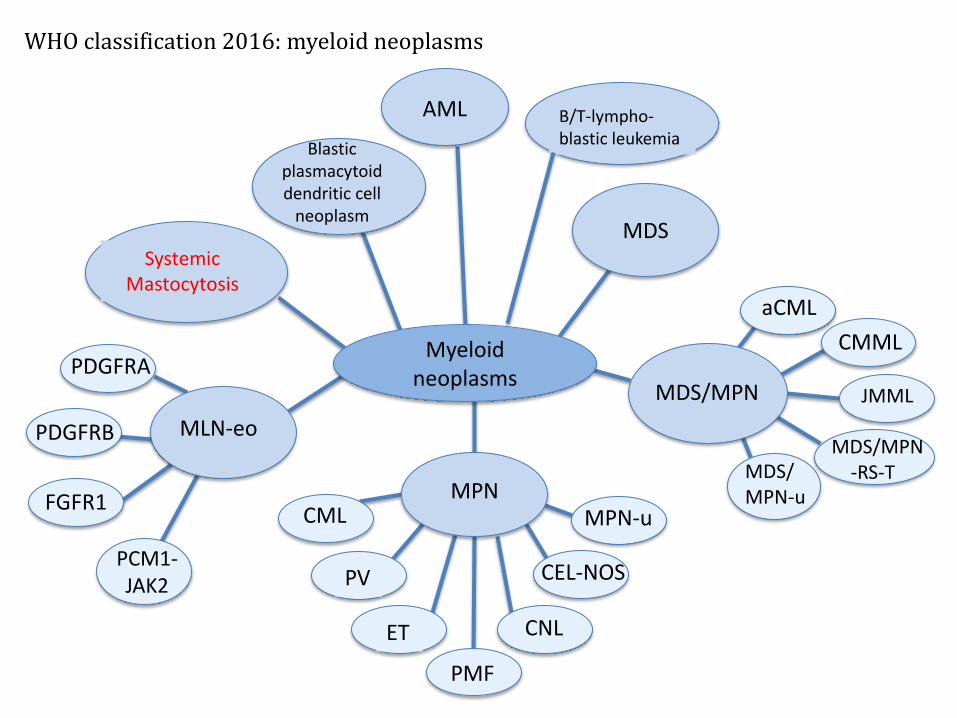
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)

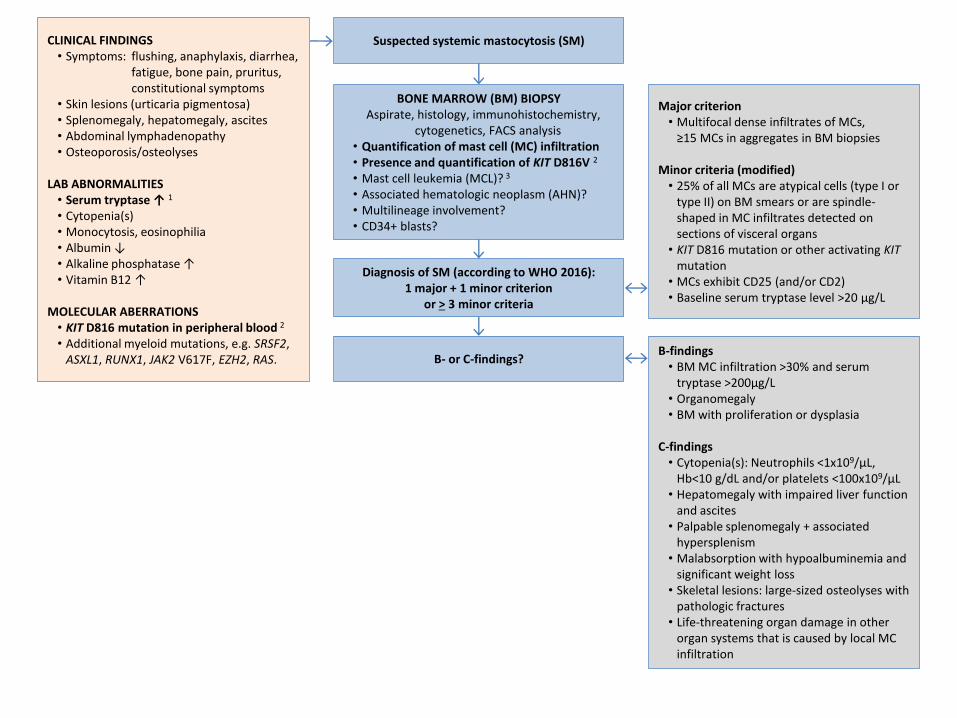
CLINICAL FINDINGS • Symptoms: flushing, anaphylaxis, diarrhea,
fatigue, bone pain, pruritus, constitutional symptoms
• Skin lesions (urticaria pigmentosa) • Splenomegaly, hepatomegaly, ascites • Abdominal lymphadenopathy • Osteoporosis/osteolyses
LAB ABNORMALITIES
• Serum tryptase ↑ 1
• Cytopenia(s) • Monocytosis, eosinophilia • Albumin ↓ • Alkaline phosphatase ↑ • Vitamin B12 ↑
MOLECULAR ABERRATIONS • KIT D816 mutation in peripheral blood 2 • Additional myeloid mutations, e.g. SRSF2,
ASXL1, RUNX1, JAK2 V617F, EZH2, RAS.
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)
CLINICAL FINDINGS • Symptoms: flushing, anaphylaxis, diarrhea,
fatigue, bone pain, pruritus, constitutional symptoms
• Skin lesions (urticaria pigmentosa) • Splenomegaly, hepatomegaly, ascites • Abdominal lymphadenopathy • Osteoporosis/osteolyses
LAB ABNORMALITIES
• Serum tryptase ↑ 1
• Cytopenia(s) • Monocytosis, eosinophilia • Albumin ↓ • Alkaline phosphatase ↑ • Vitamin B12 ↑
MOLECULAR ABERRATIONS • KIT D816 mutation in peripheral blood 2 • Additional myeloid mutations, e.g. SRSF2,
ASXL1, RUNX1, JAK2 V617F, EZH2, RAS.
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)
B- or C-findings? B-findings
• BM MC infiltration >30% and serum tryptase >200µg/L
• Organomegaly • BM with proliferation or dysplasia
C-findings • Cytopenia(s): Neutrophils <1x109/μL,
Hb<10 g/dL and/or platelets <100x109/μL • Hepatomegaly with impaired liver function
and ascites • Palpable splenomegaly + associated
hypersplenism • Malabsorption with hypoalbuminemia and
significant weight loss • Skeletal lesions: large-sized osteolyses with
pathologic fractures • Life-threatening organ damage in other
organ systems that is caused by local MC infiltration

CLINICAL FINDINGS • Symptoms: flushing, anaphylaxis, diarrhea,
fatigue, bone pain, pruritus, constitutional symptoms
• Skin lesions (urticaria pigmentosa) • Splenomegaly, hepatomegaly, ascites • Abdominal lymphadenopathy • Osteoporosis/osteolyses
LAB ABNORMALITIES
• Serum tryptase ↑ 1
• Cytopenia(s) • Monocytosis, eosinophilia • Albumin ↓ • Alkaline phosphatase ↑ • Vitamin B12 ↑
MOLECULAR ABERRATIONS • KIT D816 mutation in peripheral blood 2 • Additional myeloid mutations, e.g. SRSF2,
ASXL1, RUNX1, JAK2 V617F, EZH2, RAS.
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)
B- or C-findings? B-findings
• BM MC infiltration >30% and serum tryptase >200µg/L
• Organomegaly • BM with proliferation or dysplasia
C-findings • Cytopenia(s): Neutrophils <1x109/μL,
Hb<10 g/dL and/or platelets <100x109/μL • Hepatomegaly with impaired liver function
and ascites • Palpable splenomegaly + associated
hypersplenism • Malabsorption with hypoalbuminemia and
significant weight loss • Skeletal lesions: large-sized osteolyses with
pathologic fractures • Life-threatening organ damage in other
organ systems that is caused by local MC infiltration

CLINICAL FINDINGS • Symptoms: flushing, anaphylaxis, diarrhea,
fatigue, bone pain, pruritus, constitutional symptoms
• Skin lesions (urticaria pigmentosa) • Splenomegaly, hepatomegaly, ascites • Abdominal lymphadenopathy • Osteoporosis/osteolyses
LAB ABNORMALITIES
• Serum tryptase ↑ 1
• Cytopenia(s) • Monocytosis, eosinophilia • Albumin ↓ • Alkaline phosphatase ↑ • Vitamin B12 ↑
MOLECULAR ABERRATIONS • KIT D816 mutation in peripheral blood 2 • Additional myeloid mutations, e.g. SRSF2,
ASXL1, RUNX1, JAK2 V617F, EZH2, RAS
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)
B- or C-findings? B-findings
• BM MC infiltration >30% and serum tryptase >200µg/L
• Organomegaly • BM with proliferation or dysplasia
C-findings • Cytopenia(s): Neutrophils <1x109/μL,
Hb<10 g/dL and/or platelets <100x109/μL • Hepatomegaly with impaired liver function
and ascites • Palpable splenomegaly + associated
hypersplenism • Malabsorption with hypoalbuminemia and
significant weight loss • Skeletal lesions: large-sized osteolyses with
pathologic fractures • Life-threatening organ damage in other
organ systems that is caused by local MC infiltration
ISM 0 or 1 B-finding,
No C-finding
SSM At least 2 of 3 B-
findings
MCL ASM C-findings
SM-AHN 4
1,2 An elevated serum tryptase (normal value <11.4µg/L) AND presence of a KIT D816 mutation (KIT D816V in >90% of cases) make diagnosis of SM very likely. 3 MCL is defined by >20% mast cells in BM cytology (not histology!). 4 In the majority of SM-AHN cases , the AHN is also KIT D816V positive and treatment is according to SM. In few cases, SM and AHN may represent two independent diseases and treatment of SM and AHN may differ.

KIT Mutation (Burden) in Patients with Systemic Mastocytosis
The majority (>90%) of patients with systemic mast cell disease express the imatinib resistant Asp816Val (D816V) mutation in the KIT receptor tyrosine kinase.
Erben et al., Ann Hematol. 2014; 93(1):81-8

Lim et al., Blood 2009; 113: 5727–36
ISM: indolent SM ASM: aggressive SM MCL: mast cell leukemia AHD: associated hematologic (non-mast cell lineage) disorder
Survival with SM

CLINICAL FINDINGS • Symptoms: flushing, anaphylaxis, diarrhea,
fatigue, bone pain, pruritus, constitutional symptoms
• Skin lesions (urticaria pigmentosa) • Splenomegaly, hepatomegaly, ascites • Abdominal lymphadenopathy • Osteoporosis/osteolyses
LAB ABNORMALITIES
• Serum tryptase ↑ 1
• Cytopenia(s) • Monocytosis, eosinophilia • Albumin ↓ • Alkaline phosphatase ↑ • Vitamin B12 ↑
MOLECULAR ABERRATIONS • KIT D816 mutation in peripheral blood 2 • Additional myeloid mutations, e.g. SRSF2, ASXL1, RUNX1, JAK2 V617F, EZH2, RAS
BONE MARROW (BM) BIOPSY Aspirate, histology, immunohistochemistry,
cytogenetics, FACS analysis • Quantification of mast cell (MC) infiltration • Presence and quantification of KIT D816V 2
• Mast cell leukemia (MCL)? 3 • Associated hematologic neoplasm (AHN)? • Multilineage involvement? • CD34+ blasts?
Diagnosis of SM (according to WHO 2016): 1 major + 1 minor criterion
or > 3 minor criteria
Major criterion • Multifocal dense infiltrates of MCs,
≥15 MCs in aggregates in BM biopsies
Minor criteria (modified) • 25% of all MCs are atypical cells (type I or
type II) on BM smears or are spindle-shaped in MC infiltrates detected on sections of visceral organs
• KIT D816 mutation or other activating KIT mutation
• MCs exhibit CD25 (and/or CD2) • Baseline serum tryptase level >20 µg/L
Suspected systemic mastocytosis (SM)
B- or C-findings? B-findings
• BM MC infiltration >30% and serum tryptase >200µg/L
• Organomegaly • BM with proliferation or dysplasia
C-findings • Cytopenia(s): Neutrophils <1x109/μL,
Hb<10 g/dL and/or platelets <100x109/μL • Hepatomegaly with impaired liver function
and ascites • Palpable splenomegaly + associated
hypersplenism • Malabsorption with hypoalbuminemia and
significant weight loss • Skeletal lesions: large-sized osteolyses with
pathologic fractures • Life-threatening organ damage in other
organ systems that is caused by local MC infiltration
ISM 0 or 1 B-finding,
No C-finding
SSM At least 2 of 3 B-
findings
MCL ASM C-findings
SM-AHN 4
• H1-/H2-antagonists • MC stabilizers • Leukotriene antagonists • Steroids (topic and/or systemic) • Interferon-alpha (inadequately
controlled symptoms, off-label)
• Midostaurin (SM-AHN, ASM, MCL) • Imatinib (for sensitive KIT mutations only, <1%) • Cladribine (off-label) • Interferon-alpha (off-label) • Hydroxyurea (for the AHN component)
• Allogeneic stem cell transplantation (in eligible patients in best achievable remission)
1,2 An elevated serum tryptase (normal value <11.4µg/L) AND presence of a KIT D816 mutation (KIT D816V in >90% of cases) make diagnosis of SM very likely. 3 MCL is defined by >20% mast cells in BM cytology (not histology!). 4 In the majority of SM-AHN cases , the AHN is also KIT D816V positive and treatment is according to SM. In few cases, SM and AHN may represent two independent diseases and treatment of SM and AHN may differ.

Midostaurin (PKC412, Rydapt®) in advSM
Improvement of:
• Symptoms
• Serum tryptase
• Bone marrow mast cell infiltration
• C-findings (organ dysfunction)
• BUT: no complete remission
Adverse events:
• Nausea
• Vomiting
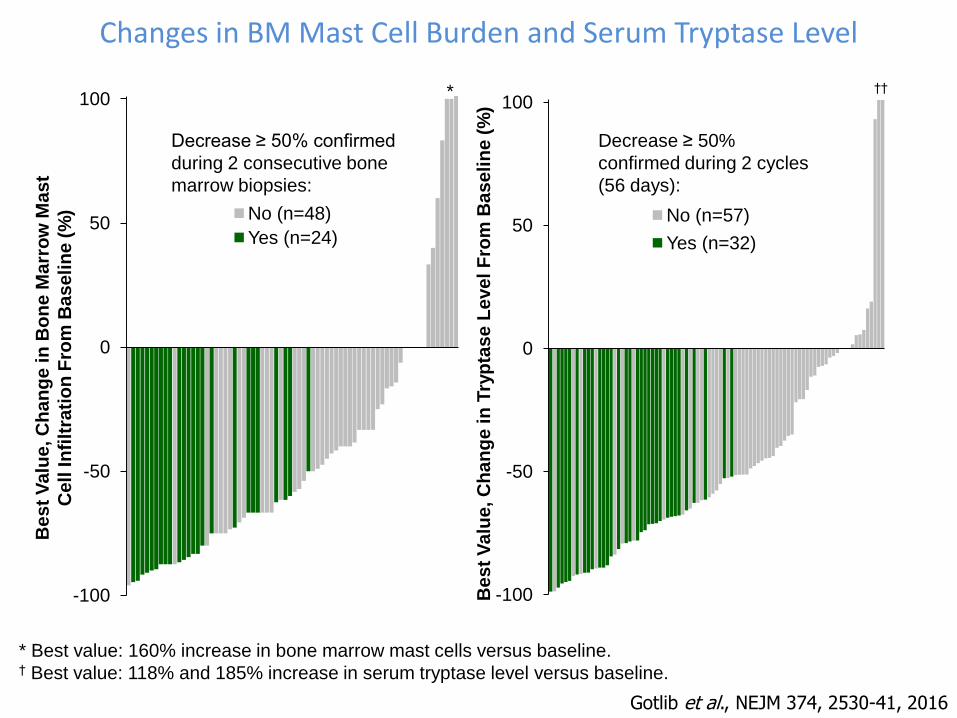
Gotlib et al., NEJM 374, 2530-41, 2016
-100
-50
0
50
100
No (n=57)
Yes (n=32)
Decrease ≥ 50%
confirmed during 2 cycles
(56 days):
Be
st
Va
lue
, C
ha
ng
e in
Try
pta
se
Le
ve
l F
rom
Ba
se
lin
e (
%)
-100
-50
0
50
100
No (n=48)
Yes (n=24)
Be
st
Va
lue
, C
ha
ng
e in
Bo
ne
Ma
rro
w M
as
t
Cell
In
filt
rati
on
Fro
m B
aseli
ne (
%)
Decrease ≥ 50% confirmed
during 2 consecutive bone
marrow biopsies:
†† *
* Best value: 160% increase in bone marrow mast cells versus baseline. † Best value: 118% and 185% increase in serum tryptase level versus baseline.
Changes in BM Mast Cell Burden and Serum Tryptase Level
Gotlib et al., NEJM 374, 2530-41, 2016
-70
-60
-50
-40
-30
-20
-10
0
10
20
30
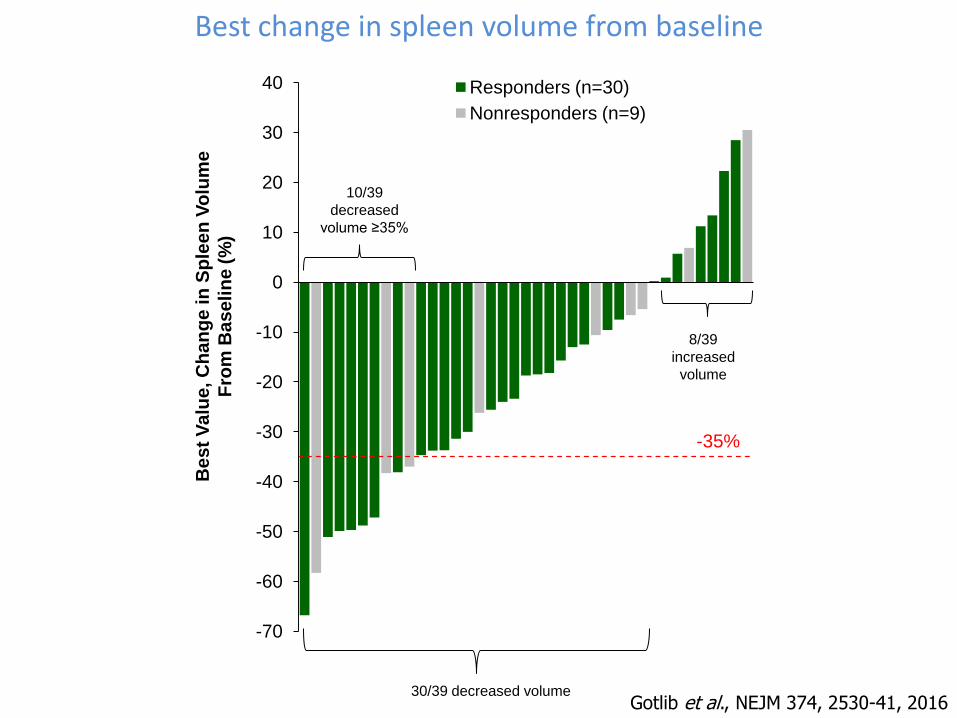
40 Responders (n=30)
Nonresponders (n=9)
Be
st
Va
lue
, C
ha
ng
e in
Sp
lee
n V
olu
me
Fro
m B
as
eli
ne
(%
)
-35%
8/39
increased
volume
10/39
decreased
volume ≥35%
30/39 decreased volume
Best change in spleen volume from baseline
Gotlib et al., NEJM 374, 2530-41, 2016
26
41
50 49 53 56 56 56 59
63 55
59
31
21
19 16
15 11 10 5
8
10
15 13 16
13
8 11
9 11 12
13
10
10 9 4
8 12
4 9 3
8 3 13 10
8
6 13
19 13
19 16
20 13
19 13 12
8 15
11
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12
Pati
en
ts (
%)
Months
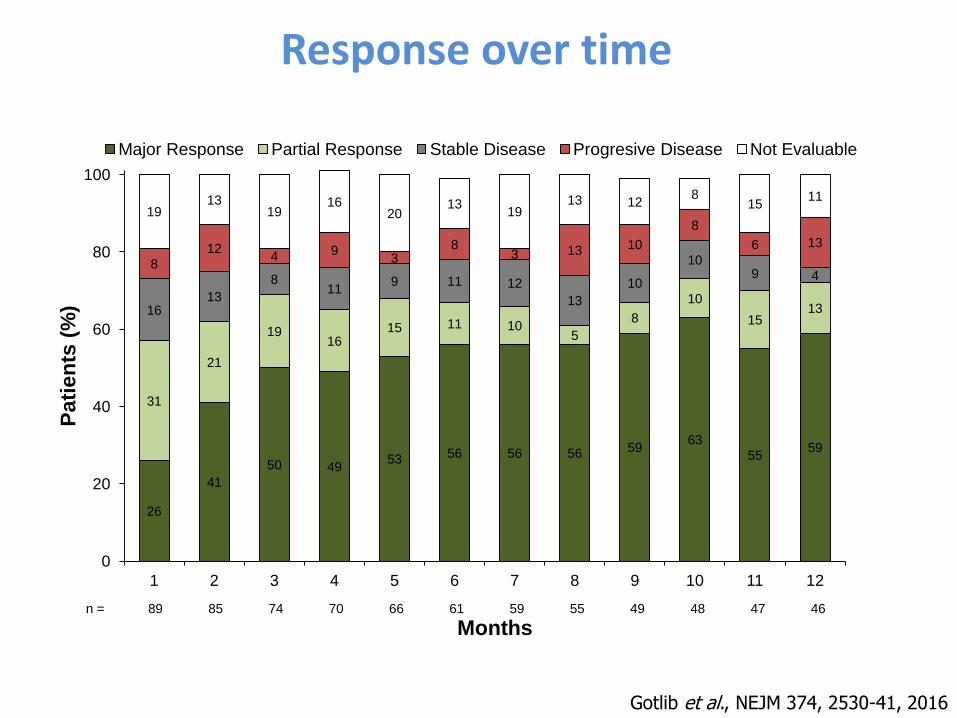
Major Response Partial Response Stable Disease Progresive Disease Not Evaluable
n = 89 85 74 70 66 61 59 55 49 48 47 46
Response over time
Gotlib et al., NEJM 374, 2530-41, 2016
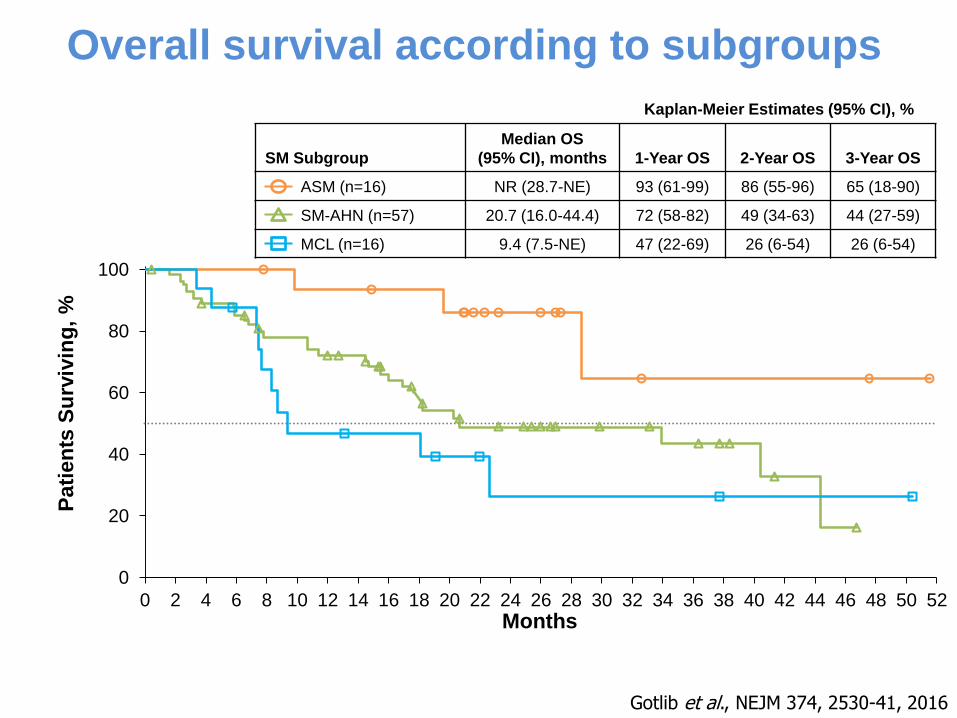
SM Subgroup
Median OS
(95% CI), months 1-Year OS 2-Year OS 3-Year OS
ASM (n=16) NR (28.7-NE) 93 (61-99) 86 (55-96) 65 (18-90)
SM-AHN (n=57) 20.7 (16.0-44.4) 72 (58-82) 49 (34-63) 44 (27-59)
MCL (n=16) 9.4 (7.5-NE) 47 (22-69) 26 (6-54) 26 (6-54)
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52
Pati
en
ts S
urv
ivin
g,
%
Months
Kaplan-Meier Estimates (95% CI), %
Gotlib et al., NEJM 374, 2530-41, 2016
Overall survival according to subgroups

Schwaab et al., Blood 2013; 122:2460–2466; Jawhar et al., Leukemia 2016; 30:136-143
Overall frequency and prognostic impact of mutated genes in 70 advanced KIT D816V+ SM patients
0%
20%
40%
60%
80%
100%
60% of patients had ≥2 mutated genes in addition to KIT D816V
Overall survival in advanced SM depending on mutations in the SRSF2/ASXL1/RUNX1 (S/A/R) panel
S/A/Rneg
S/A/Rpos

Impact of baseline parameters on overall survival
a MCL patients with and without AHN b KIT D816V in peripheral blood
Jawhar et al., Blood 2017, in press
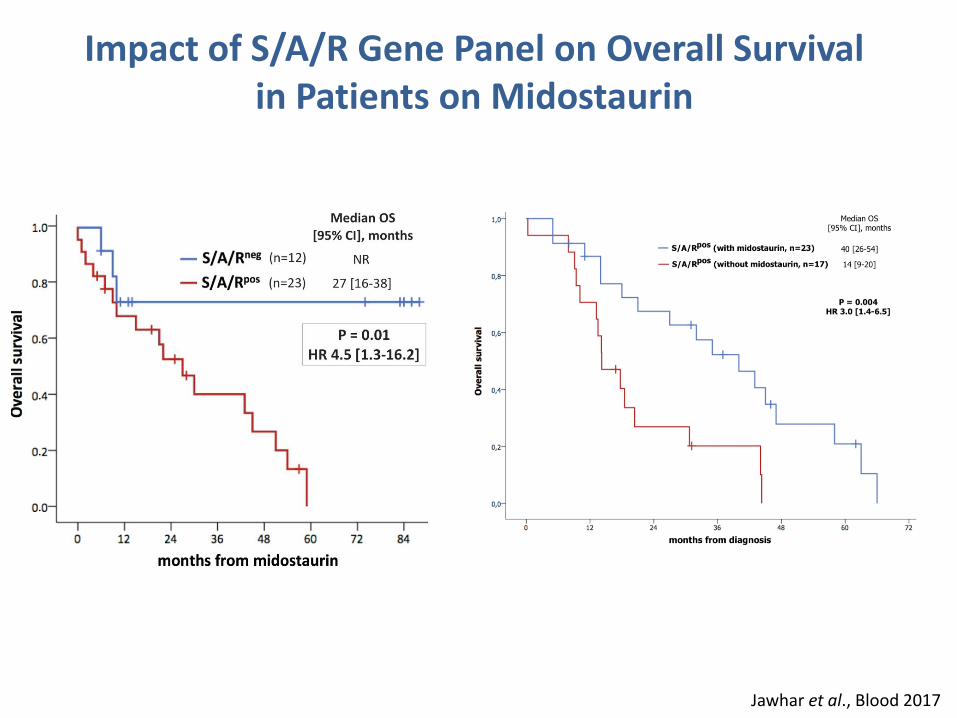
Impact of S/A/R Gene Panel on Overall Survival in Patients on Midostaurin
Jawhar et al., Blood 2017

Univariate and multivariate analyses of on-treatment variables regarding overall survival
b KIT D816V in peripheral blood c AP reduction ≥50% or normalization D Cheson criteria for transfusions e response criteria according to Valent f response criteria according to IWG-MRT & ECNM consensus criteria
Jawhar et al., Blood 2017, in press

Overall survival in advanced SM
Jawhar et al., Haematologica 2017

Mast cell leukemia: characteristics and impact of S/A/Rmut on overall survival
• Cytoreductive therapy: 25/28 (89%)
• Midostaurin (n=23) and/or cladribine (n=12)
• Median overall survival: 17 months (95% CI, 10-24)
• Age: median 67 years (45–82)
• BM MC infiltration: median 65% (20–95)
• Serum tryptase: median 520 µg/L (157-1854)
• KIT D816V in 68%, D816H/Y in 21%
• KIT D816V AB in PB: median 43% (20–98)
• Additional mutations in 68%, S/A/Rpos in 52%
• Hb <10g/dL and/or platelets <100x109/L in 93%
• MCL-AHN: 20/28 (71%)
• Secondary MCL: 12/28 (43%)

Systemic mastocytosis is not adequately diagnosed and subtyped
Jawhar et al., European Journal of Clinical Investigation, 2016
Initial diagnosis n=65
Diagnosis of SM by bone marrow histology, KIT D816V and tryptase
n=65
Correct subclassification
41/50, 82%
Incorrect sublassification (missed AHN)
9/50, 18%
Systemic mastocytosis 50/65, 77%
Inconsistent diagnosis
15/65, 23%
• MDS/MPNu • PMF • HES • B-cell lymphoma • ITP • Reactive
Median interval between bone marrow biopsies 6 months (range 1-48)
KIT mutation analysis in 26% of patients
performed or recommended
Quantification of mast cell infiltration in 66% of patients

Diagnosis in SM- Summary
• Underdiagnosed!!! – by clinicians AND pathologists
• Watch out for advSM:
MDS/MPN, MDS, MPN
± monocytosis ± eosinophilia
Splenomegaly ± elevated AP ± ascites ± diarrhea
LDH frequently normal
´AML´: eosinophilia, elevated serum tryptase, lack of response to chemotherapy
• Serum tryptase
• KIT D816V
• Bone marrow histology (tryptase, CD117, CD25)

Treatment in SM- Summary
• Symptomatic treatment in indolent phase disease
• Cytoreductive treatment in advanced phase disease
• Midostaurin (Rydapt®)
• Other KIT Inhibitors (Blu 285, DCC 2618)
• Cladribine
• Allogeneic stem cell transplantation in best achievable remission
Diagnosis and treatment of systemic mastocytosis
Mast cell burden
Tryptase KIT allele burden
SM

Diagnosis and treatment of SM with monocytosis
Mast cell burden
Tryptase Monocytes KIT allele burden
CMML + ISM
Mast cell burden
Tryptase Monocytes KIT allele burden
SM-CMML
Mast cell burden
Tryptase Monocytes KIT allele burden
SM-CMML
KIT inhibitor Cladribine
Hydroxyurea Azacytidine

Clinical case
Triple-negative primary myelofibrosis
Leukocytes 32 x 109/l
Monocytes 2.4 x 109/l
Eosinophils 1.3 x 109/l
Hemoglobin 11g/dl
Platelets 210 x 109/l
Spleen 2180 ccm3
Bone marrow Hypercellular
fibrosis grade 2
LDH 280U/l
AP 580U/l
Tryptase 350µg/l
Mutations Negative for JAK2 V617F, CALR,
MPL
Treatment No response on ruxolitinib
2x20mg/day

Clinical case
Triple-negative primary myelofibrosis
Leukocytes 32 x 109/l
Monocytes 2.4 x 109/l
Eosinophils 1.3 x 109/l
Hemoglobin 11g/dl
Platelets 210 x 109/l
Spleen 2180 ccm3
Bone marrow Hypercellular
fibrosis grade 2
LDH 280U/l
AP 580U/l
Tryptase 350µg/l
Mutations Negative for JAK2 V617F, CALR,
MPL
Treatment No response on ruxolitinib
2x20mg/day

Clinical case
Triple-negative primary myelofibrosis
Leukocytes 32 x 109/l
Monocytes 2.4 x 109/l
Eosinophils 1.3 x 109/l
Hemoglobin 11g/dl
Platelets 210 x 109/l
Spleen 2180 ccm3
Bone marrow Hypercellular
fibrosis grade 2
LDH 280U/l
AP 580U/l
Tryptase 350µg/l
Mutations Negative for JAK2 V617F, CALR,
MPL
Treatment No response on ruxolitinib
2x20mg/day

Clinical case
Leukocytes 32 x 109/l
Monocytes 2.4 x 109/l
Eosinophils 1.3 x 109/l
Hemoglobin 11g/dl
Platelets 210 x 109/l
Spleen 2180 ccm3
Bone marrow Hypercellular
fibrosis grade 2
LDH 280U/l
AP 580U/l
Tryptase 350µg/l
Mutations Negative for JAK2 V617F, CALR,
MPL
Treatment No response on ruxolitinib
2x20mg/day

Clinical case
Multimutated aggressive systemic mastocytosis
Leukocytes 32 x 109/l
Monocytes 2.4 x 109/l
Eosinophils 1.3 x 109/l
Hemoglobin 11g/dl
Platelets 210 x 109/l
Spleen 2180 ccm3
Bone marrow 40% mast cell infiltration
fibrosis grade 2
LDH 280U/l
AP 580U/l
Tryptase 350µg/l
Mutations Positive for KIT D816V, SRSF2,
ASXL1, RUNX1, TET2
Treatment Midostaurin, cladribine,
allogeneic SCT

In advanced SM
and myelofibrosis,
midostaurin and
ruxolitinib,
respectively, must
navigate complex
mutational
landscapes while
trying to impact
similar disease-
related burdens.
Gotlib J., Blood 130, 98-100, 2017

Thank you
Mannheim Mohamad Jawhar Georgia Metzgeroth Nicole Naumann Alice Fabarius Wolf-Karsten Hofmann Andreas Reiter
München (MLL) Claudia Haferlach Manja Meggendorfer Torsten Haferlach
Salisbury, UK Nicholas C.P. Cross
Freiburg Annette Schmitt-Gräff
München, LMU Hans-Peter Horny
Wien Peter Valent
Jena Thomas Ernst Andreas Hochhaus
Deutsche MPN-Studiengruppe
Salzburg Karl Sotlar

• SM vs. SM-AHN?
SM-AHN underdiagnosed
Survival: normal vs. median survival <5 years
• What is AHN?
Multilineage KITmut involvement
Two independent clones, e.g. CMML, JAK2 V617F, del(5q), etc.
• How important is subtyping of AHN?
e.g. MDS/MPN, CMML, MPN, CEL etc.
Mutation profile is more important than phenotype
• MCL vs. MCL-AHN
KITmut mast cells vs. multimutated multilineage stem cell disease
• SM-AML
Blasts may be KITmut negative
SM-AHN

Jawhar et al., Leukemia 2015; 29:1115-1122
TET2
KIT
ASXL1 TET2
ASXL1 TET2
KIT
• KIT D816V alone was not identified in a single colony.
• In contrast, colonies with additional mutations were frequent.
• Mutations in TET2, SRSF2 or ASXL1 precede KIT D816V.
• KIT D816V is a strong phenotype modifier.
Molecular profiling of myeloid progenitor cells in multi-mutated advanced SM patients